plaque disclosing agents
TRANSCRIPT

PLAQUE DISCLOSING
AGENTS

CONTENTSI. DEFINITION OF PLAQUE
II. DENTAL PLAQUE: A HOST-ASSOCIATED BIOFILM
III. SIGNIFICANCE OF PLAQUE IN DEVELOPMENT OF PERIODONTAL DISEASE
IV. IDENTIFICATION OF DENTAL PLAQUE
V. DEFINITION OF DISCLOSING AGENT
VI. HISTORY
VII. UTILITY
VIII. IDEAL PROPERTIES
IX. COMPOSITION
X. MECHANISM OF ACTION
XI. DYES USED AS DISCLOSING AGENT
XII. METHOD OF APPLICATION
XIII. APPLIED ASPECTS
XIV. CONCLUSION
XV. REFERENCES2

1. WHO (1978):
Dental plaque is defined as a specific but highly variable
structural entity resulting from sequential colonization
and growth of micro organisms on the surfaces of teeth
and restoration consisting of micro organisms of various
strains and species are embedded in the extra cellular
matrix, composed of bacterial metabolic products and
substance from serum, saliva and blood.
3
I. DEFINITION OF DENTAL PLAQUE

2. Bradshaw and Marsh (1999):
Dental plaque is a microbial biofilm, a diverse microbial
community found on the tooth surface embedded in a
matrix of polymers of bacterial and salivary origin.
4Dumitrescu AL. Etiology and Pathogenesis of Periodontal disease: Springer –
Verlag Berlin Heidelberg, 2010.

II. DENTAL PLAQUE: A HOST-ASSOCIATED BIOFILM
Dental plaque is a host-associated biofilm. The significance of the biofilm environment has been increasingly recognized because the environment itself may alter properties of microorganisms. The biofilm community is initially formed through bacterial interactions with the tooth and then through physical and physiologic interactions among different species within the microbial mass. Furthermore, the bacteria found in the plaque biofilm are strongly influenced by external environmental factors that may be host mediated.
5Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders Co.2002.

Macroscopically,
Classified as Supragingival & Subgingival plaque, based on its position of the tooth surface.
Marginal plaque – The supragingival plaque in direct contact with the gingival margin. Holds prime importance in the development of gingivitis.
6Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders Co.2002.
III. SIGNIFICANCE OF PLAQUE IN DEVELOPMENT OF PERIODONTAL DISEASE
• Once the biofilm has formed, the species composition at a
site is characterized by a degree of stability or balance
among the component species, despite regular minor
environmental stresses following, for example, periodic oral
hygiene, food intake or diurnal changes in saliva flow.
Importantly, this stability (termed microbial homeostasis) is
not due to any biological indifference among the resident
organisms, but is due to a dynamic balance imposed by
numerous microbial interactions.
7Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders Co.2002.

8
• Bacteria respond to environmental change, and,
microbial homeostasis can break down if a key
parameter exceeds the threshold that is compatible
with community stability.
• A consequence of homeostasis breakdown is re-
organization of the structure and composition of the
microbial community, with previous species that
were only minor components becoming more
competitive under the new conditions, and, as a
result, more dominant. Such a change in community
composition and activity can predispose a site to
disease.
Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders Co.2002.
IV. IDENTIFICATION OF DENTAL PLAQUE
9
• Elimination of bacterial plaque from tooth surfaces is
essential for maintaining dental health (Loe et al 1965,
1971, Lovdal et al 1958, 1961, Suomi et al 1969, 1971,
Greene and Vermillion 1971).
• It is often difficult, however, to convince patients about the
importance of performing thorough oral hygiene.
• Patient motivation, therefore, represents an important
aspect in improving oral hygiene.
Lang et al 1972. A fluorescent plaque disclosing agent. J. Periodont.Res. 7: 59-
67.
The use of agents which stain and disclose bacterial plaque in situ is generally thought to enhance motivation by enabling the patient to detect deposits on the teeth and to control the efficacy of his oral hygiene techniques.
Home care aids: 1. Tooth brushing methods
2. Dentifrices(ShoPlaq , PlaqueHD)
may contain plaque disclosing agent that permits dental plaque observation.
Staining of bacterial plaque aids in efficient plaque removal teaches the significance of plaque in periodontal disease.
Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3 10

Raybin (1943):
A disclosing agent is a solution which when applied on the tooth, makes visible by staining roughness and foreign matter on the tooth.
World English Dictionary:
A disclosing agent is a dye in liquid or tablet form that colors something, especially the teeth to show plaque.
V. DEFINITION OF DISCLOSING AGENT
11Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3
VI. HISTORY
1. Skinner in 1914: First disclosing solution
(Skinner’s iodine solution). Patients' teeth
were disclosed with this solution to
demonstrate "soft accumulations" which
had to be removed by the patient at home.
2. Berwick in 1920: Combination of Brilliant
green – crystal violet.
3. Easlick in 1935: Bismark brown.
4. Raybin in 1943: Gentian violet (non-iodine
dye)e
Cohen et al 1972. A Comparison of Bacterial Plaque Disclosants in Periodontal Disease. J Periodonol.43[6]: 333-338.
12

VII. UTILITY OF DISCLOSING AGENT
a. Diagnosing the dental plaque.
b. Personalized patient instruction and motivation.
c. Self- evaluation by the patient.
d. To evaluate the effectiveness of oral hygiene
maintenance.
e. Preparation of plaque indices.
13Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3

1. Taste: i. Patient comfort.ii. Flavored.iii. Should encourage patient co-operation.
2. Intensity of color:i. Evident contrast to differentiate from surrounding
environment.
3. Duration of Intensity: Retentive – The color should not rinse off with ordinary rinsing methods for the period of time required to complete the instructions or clinical examination.
4. Non-irritating to oral mucosa.
5. Non-allergic.
6. Antiseptic property.
VIII. IDEAL PROPERTIES
14Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3
7. The dye must be capable of adequately
penetrating the plaque deposit.
8. Selective staining efficacy.
9. Water-soluble.
15Skaggs et al.,1991. Plaque Disclosing Compositions. United States Patent: 1-7

IX. COMPOSITION
Pertains to combinations of dyes-
I. FDC Red No. 3(Erythrosin) and FDC Blue No. 1;
II. FD&C Blue No. 2;
III. FD&C Green No.5;
IV. FD&C Blue No. 1 and D&C Yellow No. 5;
V. D. & C. Yellow No. 8 (Fluorescein);
VI. FD&C Red No. 3 and FD&C Green No. 3;
VII. FD&C Red No. 3 and Hercules Green Shade 3;
VIII.FD&C Red No. 40, or Allura Red (0.05%-10%);
IX. FD&C Red No. 22 (eocine)
16Skaggs et al.,1991. Plaque Disclosing Compositions. United States Patent: 1-7
i. Disclosing agents work by changing the color of dental plaque so that it contrasts with the white tooth surface.
ii. Dental plaque has the ability to retain a large number of dye substances which can be used for disclosing purposes. This property is related to interaction, because of the polarity difference between the components of plaque and dyes(Gallagher et al, 1977). The particles are bound to the surface by electrostatic interaction(proteins) and hydrogen bonds(polysaccharides).
Chetrus and Ion 2013. Dental Plaque – classification, formation, and identification.
International Journal of Medical Dentistry.3[2]:139-143.
17
X. MECHANISM OF ACTION

2. Mercurochrome preparations
3. Bismark brown
1. Iodine preparations
5. Erythrosin
4. Merbromin
6. Fast green
8. Two tone solution
9. Basic fuchsin
10. Three tone gel
7. Fluorescein
XI. DYES USED AS DISCLOSING AGENTS
18Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental Research.2[1]:1-3

1. Iodine preparations
Iodine crystals – 3.3%Potassium iodide – 16%
Zinc iodide -10%Distilled water – 16%
Skinner’s iodine solution
Tincture of iodine – 21%
Distilled water – 15%
Diluted tincture of iodine
19
Plaque deeply brown or black.
Inflamed gingiva dark areas.
Discoloration disappears in a few minutes.
Advantages :
Low cost.
Clinical photography.
Disadvantages :
Patients allergic to iodine.
Objectionable taste.
I. Iodine based solutions
20

2. Mercurochrome preparations
Mercurochrome – 1.5%
Distilled water – 30%
Mercuroc-hrome
solution – 5%
Mercurochrome – 13.5 gmDistilled water – 3 ml
Oil of peppermint – 3 drops
Flavoured mercuroch
r-ome solution
21

3. Bismark Brown (Easlick’s disclosing solution)
Bismark brown – 3 gm Glycerin – 120 ml
Ethyl alcohol – 10 ml
Anise (flavor) – 1 drop
22

4. Merbromin
Merbromin NF – 450 mg Oil of peppermint – 1 drop Distilled water – 100
ml
23

5. Erythrosin
Based on purpose
1. By Rinsing
2. For Direct topical application
3. Tablet or Wafers
24

1. By Rinsing
F.D & C. Red No. 3 or No. 28 – 6 gm
Alcohol - 10 ml
Distilled water - 100 ml
Peppermint Oil - 2 drops
25
2. For Direct topical application
Erythrosine – 0.8 gm
Alcohol - 10 ml
Distilled water - 100 ml
Peppermint Oil - 2 drops
26

3. Tablet or Wafers
F.D & C. Red No. 3 – 15 gm
Sodium chloride – 0.747%
Sodium sucaryl – 0.747%
Calcium stearate – 0.995%
White oil – 1.124%
Flavoring agent – 2.239%
27
28
However, with regular use of the FDC Red No. 3 tablet, it
became abundantly clear that the “pleasing shade of red”
adversely affected the utility of wafer. The plaque
interproximally and at the gingival margin, especially in
the posterior areas, could not easily be seen because of
poor contrast between the gingiva and the stained plaque.
Accordingly, the use of a red disclosing dye reveals that
red is the wrong color since plaque that has been stained
red is extremely difficult to see due to poor contrast with
the oral tissues, especially in the back areas of the mouth
and between the teeth. It should be noted that it is these
precise areas which are the most prevalent sites of caries
and periodontal disease.
Block et al 1973. Dental Plaque Disclosing Agent. United States Patent:1-6.
ADVANTAGES OF ERYTHROSIN RED
1. Fades in brief time.
2. Does not stain dental equipment or clothing
permanently.
3. Does not stain composite type restoratives
permanently.
4. Does not have any known possible effects that
iodine or mercury stains possess.
29
6. Fast Green F. D. & C. Green No. 3 – 5%
7. Fluoroscein F.D. & C. Yellow No. 8. Used with special ultraviolet light source to make the
agents visible.
30
PLAK – LITE:John Forrest 1981 The apparatus consists of a small mains operated lamp
gives off white light
through a dichrotic filter

Introducing 2 drops of Fluorescein – based solution
in patient’s mouth
Patient is asked to swish
Affinity for plaque by the indicator fluid
The light makes it visible as a
greenish yellow glow.31

Following application of the Plak-Lite® solution, the fluorescence remained unchanged for 20 minutes following which it began to fade, and after 2 hours, the fluorescence was completely absent.
The Plak-Lite® system consists of a fluorescent disclosing agent and a light source to make the agent visible. The solution has a light absorbency which lies within the frequencies of 2000-5400 A. The highest peak is at 4800 A and two lower peaks appear at 3250 A and 2900 A (Fig. 1).
The Plak-Lite® lamp transmits light in the frequency range 4200-5600 A.
32Lang et al.,1972. A fluorescent plaque disclosing agent. J. periodont Res.7: 59-67.

8. Two Tone solution• F. D. & C. Green No. 3• F. D. & C. Red No.3• Thicker (older) plaque stains Blue.• Thinner (newer) plaque stains Red.
33
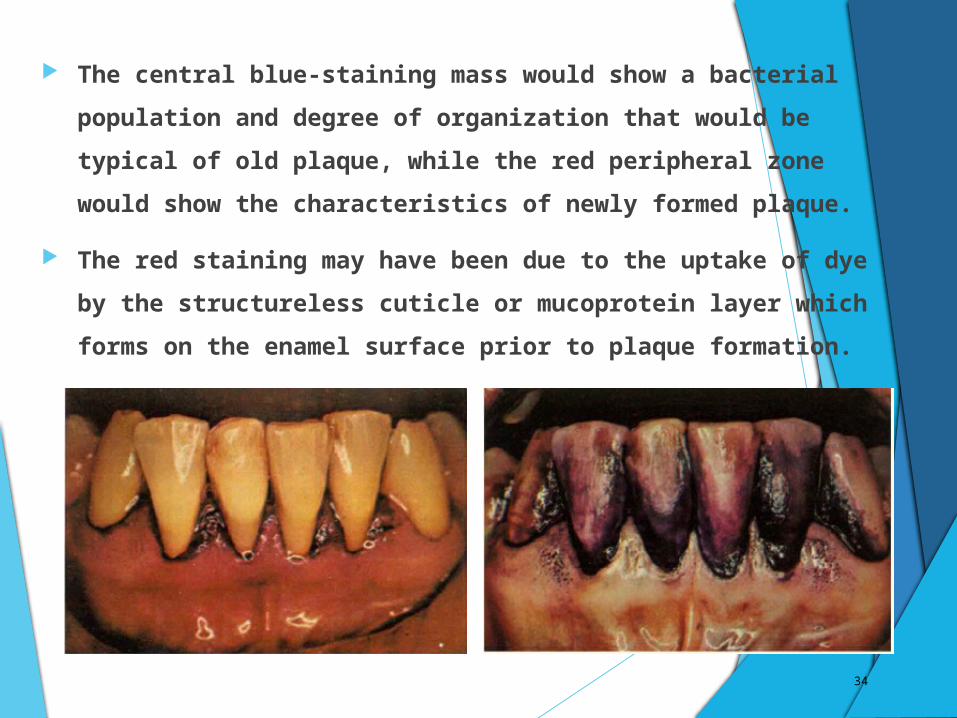
The central blue-staining mass would show a bacterial population and degree of organization that would be typical of old plaque, while the red peripheral zone would show the characteristics of newly formed plaque.
The red staining may have been due to the uptake of dye by the structureless cuticle or mucoprotein layer which forms on the enamel surface prior to plaque formation.
34

35
Blue plaque - clinicaland microscopic features Red plaques
Considerably greater thickness than red plaque.
Extreme thinness - to the extent that sometimesit was hard to obtain sufficient material for examination.
High degree of architectural organization. Cocci,
Low density of organisms.
Rods and/or filaments arranged in parallel rowsforming fan-shaped patterns. Filaments intertwined forming a mesh work.
No evidence of any orderly architecture.
Motility — present in some blue plaques.
No motility.
Spiral organisms and vibrios. No filaments, spiral organisms or vibrios.
Block et al 1973. Dental Plaque Disclosing Agent. United States Patent:1-6.
36
9. Basic Fuchsin• 6 gm• Ethyl alcohol 100 ml - 95 %• Used by adding 2 drops to distilled water in a
dappen dish.
XII. METHODS OF APPLICATION
1. Solution for direct application:
i. Retracting the cheeks and tongue.
ii. Air drying the teeth.
iii. Carrying the solution in cotton pellet or swabs and applying it on the crowns of teeth.
iv. The patient is directed to spread the solution over all surfaces of teeth.
v. The distribution is examined and patient is instructed to rinse off.
37

3. Rinsing
i. Few drops of concentrated preparation
ii. Water is added to dilution
iii. Swish and rinse for 1 minute
iv. Examining all the tooth surfaces.
4. Tablets or Wafers
i. After chewing, tablets or wafers are to be swished for around 30 – 60 seconds and then rinsed off.
38

EFFECT
Clean tooth surface do not absorb the colouring agent.
The pellicle and bacterial plaque, if present, absorbs
the agent and are thus, disclosed.
Pellicle stains Relatively thin, clear covering.
Bacterial plaque Darker, thicker and more opaque.
39

1. GC Plaque Indicator Kit(Now out of assortment and is replaced by GC Tri Plaque ID Gel)
APPLIED ASPECTS
40
2. GC Tri Plaque ID Gel
Unique three tone plaque disclosing gel that identifies new, mature and acid producing biofilms.
41

Differentiates among fresh plaque, mature plaque (more than 48 hours old) and strong acid-producing plaque by colour to aid in patient oral hygiene education.
42

Ingredients:
1. Glycerol – 10 – 20%
2. Sucrose – 5 – 10%
3. Ethyl alcohol – 1 – 5%
4. Sodium carboxyl methyl cellulose– 1 – 5%
43

DIRECTIONS FOR USE
1. Apply GC Tri Plaque ID Gel onto the tooth surfaces using a suitable instrument (microbrush, swab or tooth brush).
44

2. Dispense gel into a dish if applying on multiple tooth surfaces. Following this, the patient is instructed to lightly rinse their mouth with water.
45

3. Plaque identification by observing the color of gel.
46

a) A pink or red colour fresh plaque accumulation. b) A blue or purple colour 48hr old mature plaque. c) A light blue colour mature and strong acid-producing plaque.
47

2. Patient is instructed about proper tooth cleaning and thereby remove any remaining plaque and disclosing gel.
CONTRAINDICATION:Patients sensitive or allergic to benzoate preservatives.
48

3. The use of a Disclosing Agent During Resective Periodontal Surgery for Improved Removal of Biofilm
Aim: To clinically evaluate the scaling effectiveness during osseous resective surgery and the potential aid of a disclosing agent during this procedure. The influence on the scaling results induced by the operator awareness of a final supervision was also analyzed.
The surgical treatments – Apically positioned flap with respective osseous surgery – were performed.
49Montevecchi et al.2012. The Open Dentistry Journal(6):46-50.

50
N = 20 N = 20
Operator was informed about the planned post-treatment chromatic
examination by a supervisor. Operator was not previously informed
about the examination.
The chromatic examination was performed using the Phloxine B
disclosing agent. It was applied in a passive manner using sterile swabs
onto the exposed roots, left in situ for 10 seconds and then washed out for an
equal time.
The examination phase was performed just before suturing the flaps.
Teeth % with residual biofilm = (No. of treated teeth with atleast one stained area/total number of
treated teeth)*100
A second chromatic examination was performed to verify the use of
disclosing agent in improving the scaling results.
The stains were cleaned away & flaps were sutured.
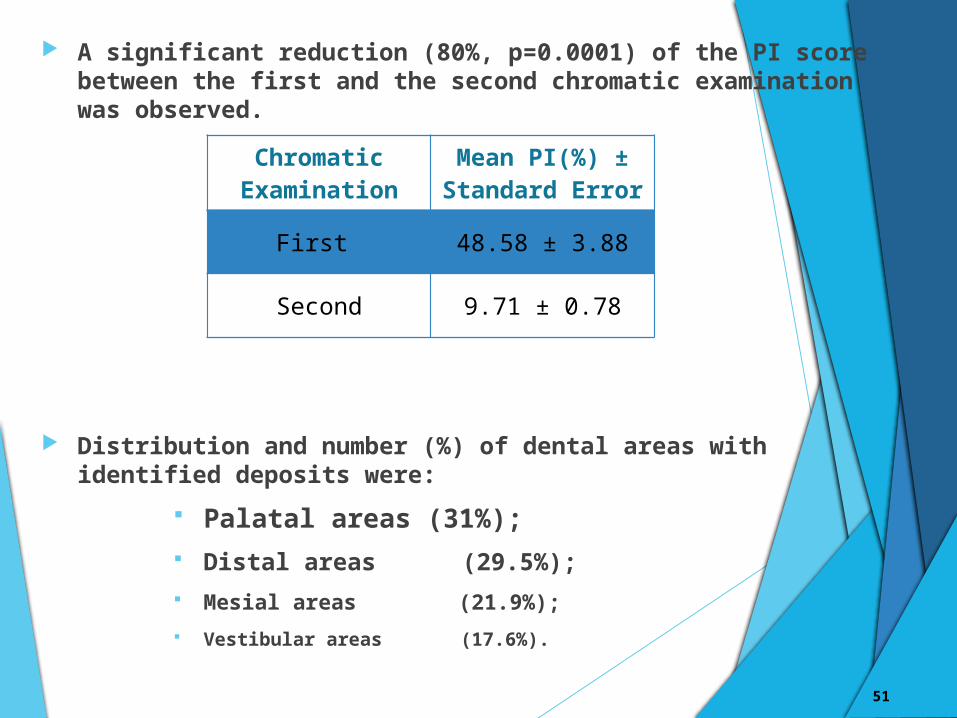
A significant reduction (80%, p=0.0001) of the PI score between the first and the second chromatic examination was observed.
Distribution and number (%) of dental areas with identified deposits were:
Palatal areas (31%); Distal areas (29.5%); Mesial areas (21.9%); Vestibular areas (17.6%).
51
Chromatic Examination
Mean PI(%) ± Standard Error
First 48.58 ± 3.88
Second 9.71 ± 0.78

This finding, associated to the observation that at the first
chromatic examination, the distal and lingual areas
remained more frequently unclean than the vestibular
areas – Suggestive of Accessibility and Visibility are
important limiting factors in determining the quality of
the cleansing outcome.
Interestingly, the use of a disclosing agent during
periodontal resective surgery seems to be instead
effective in improving the scaling and root planing results.
52
XIV. CONCLUSION This study shows that a total removal of root deposits
during an osseous resective surgery is never obtained with conventional instrumentation.
Clinical limitations and visual deficiency could be primarily responsible of the present results. In order to overcome these obstacles, the use of a plaque disclosing agent during resective surgeries seems to be effective.
Through this observation, the post-operative clinical parameters remain to be assessed in order to evaluate the attainable advantages that affect both recovery phases and long-term periodontal health.
Such observations would constitute an interesting starting point for future experimental studies on this subject.
53
XV. REFERENCES1. Newman et al. Carranza’s Clinical Periodontology. ed.3. W.B. Saunders
Co.2002.2. Dumitrescu AL. Etiology and Pathogenesis of Periodontal disease:
Springer – Verlag Berlin Heidelberg, 2010.3. Lang et al 1972. A fluorescent plaque disclosing agent. J. Periodont.Res.
7: 59-67.4. Shefali Sharma 2010. Plaque Disclosing Agent – A Review. J Adv Dental
Research.2[1]:1-35. Cohen et al 1972. A Comparison of Bacterial Plaque Disclosants in
Periodontal Disease. J Periodonol.43[6]: 333-338.6. Skaggs et al.,1991. Plaque Disclosing Compositions. United States
Patent: 1-7.7. Chetrus and Ion 2013. Dental Plaque – classification, formation, and
identification. International Journal of Medical Dentistry.3[2]:139-143.8. Block et al 1973. Dental Plaque Disclosing Agent. United States Patent:1-
6.9. Lang et al.,1972. A fluorescent plaque disclosing agent. J. periodont
Res.7: 59-67.10. Montevecchi et al.2012. The use of a Disclosing Agent During Resective
Periodontal Surgery for Improved Removal of Biofilm. The Open Dentistry Journal(6):46-50.
54

THANK YOU