pkiparkinson’s disease – current research and future developments · pkiparkinson’s disease...
TRANSCRIPT
P ki ’ diParkinson’s disease –Current Research and Future Developments
Shelley JonesShelley JonesLead Clinical Pharmacist
NeurosciencesKing’s College Hospital

Overview
• Introduction to Parkinson’s• Introduction to Parkinson s
• Current Treatment strategies• Current Treatment strategies
• New developments/research• New developments/research
• Non Motor Symptoms• Non Motor Symptoms
• The future• The future

James Parkinson• He noted:
‘Involuntary– Involuntary tremulous motion’–‘A propensity to bendA propensity to bend forwards’–‘The senses andThe senses and intellect are intact’
Parkinson’s Defined• Parkinson’s is:
– A chronic, progressive, neurological degenerative diseaseg
Th t d fi iti i• The contemporary definition is:– ‘Multi-system neurological disorder whichy g
affects cognitive processes, emotion and autonomic function.’

Aetiology of Parkinson’sgy• Incidence of Parkinson’s is 4-20 per 100,000 per year(3)
P l f P ki ’ b 200• Prevalence of Parkinson’s may be up to 200 per 100,000(3i)
Th i t l 120 000 l ith• There are approximately 120,000 people with Parkinson’s in the UK(3ii)
Almost a quarter are in hospital or residential care– Almost a quarter are in hospital or residential care– Almost a third in the community requiring help
Nearly half are independent living in the community– Nearly half are independent, living in the community• Age at onset is 30+, usually 50+(4)

The Cause of Parkinson’s• In most cases, the cause of Parkinson’s is
unknownunknown– Age
• The ageing process is intricately linked toThe ageing process is intricately linked to Parkinson’s, but is not solely responsible
– Genes• Parkinson’s inheritance is rare (5)
– Environment– Genes plus environment

Normal Movement
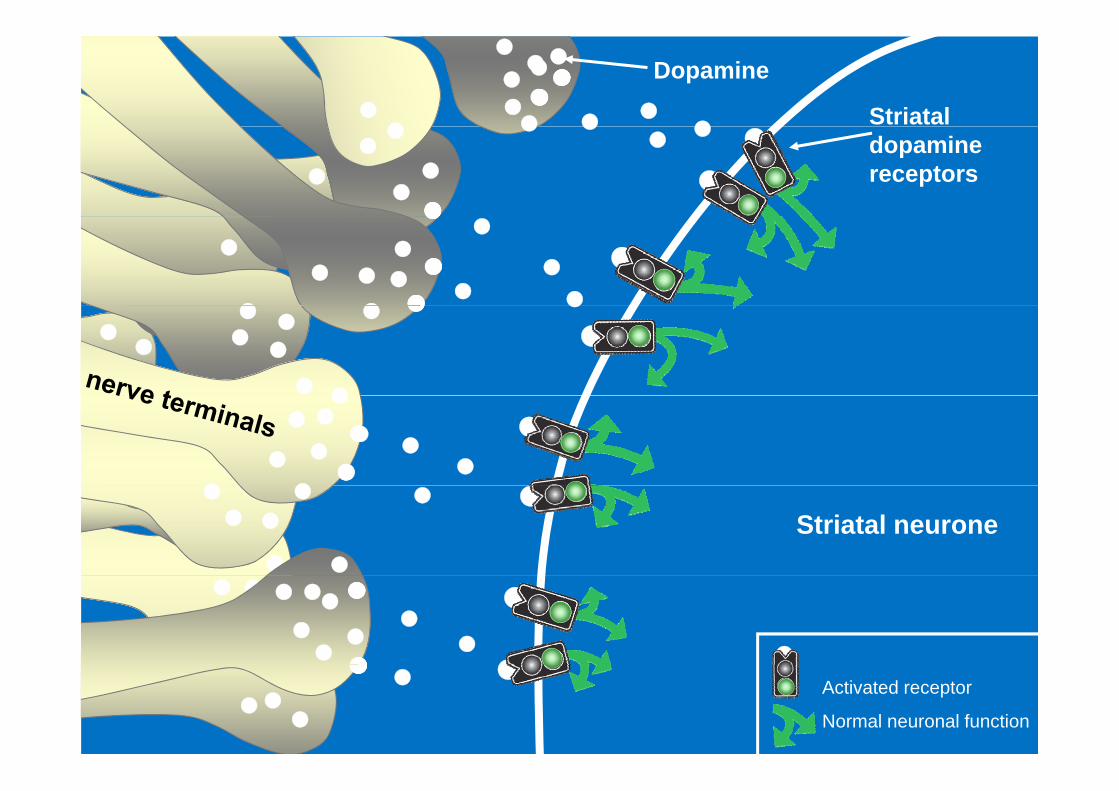
Striatal
Dopamine
dopamine receptors
Striatal neurone
Activated receptor
Normal neuronal function

Parkinsonian StateParkinsonian State
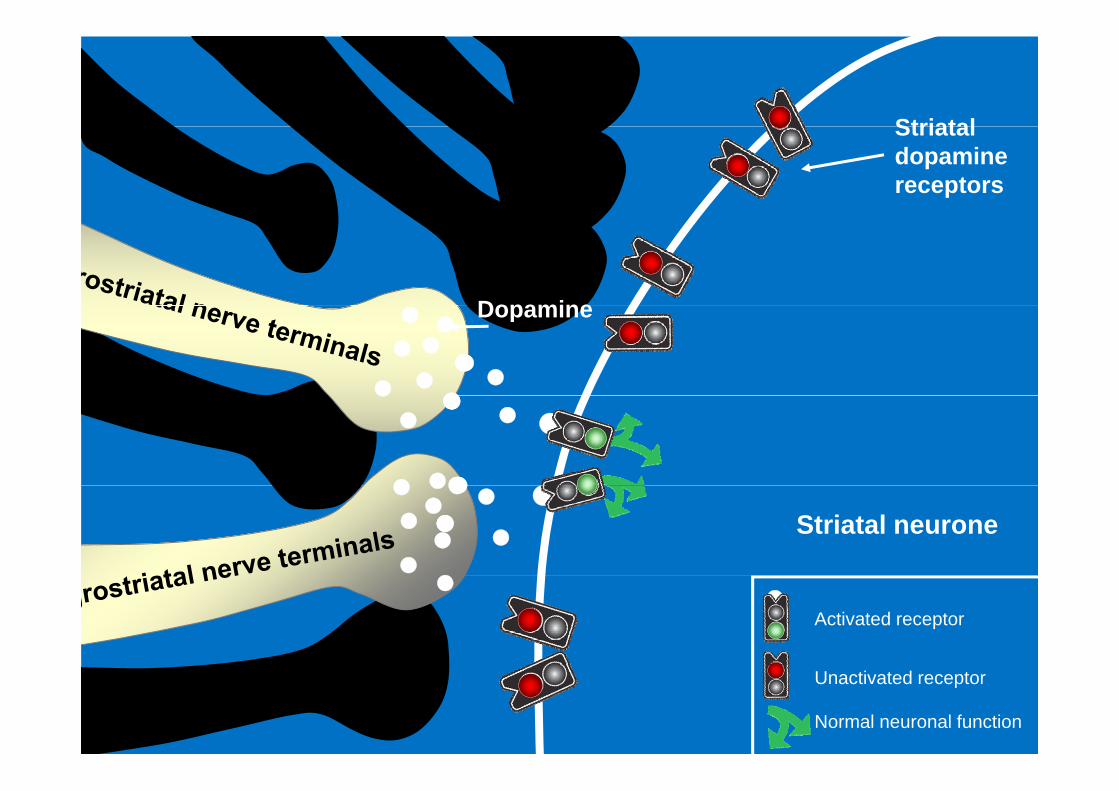
StriatalStriatal dopamine receptors
DopamineDopamine
Striatal neurone
Activated receptor
Unactivated receptor
Normal neuronal function

Diagnosisg• Based on clinical presentation:
– Bradykinesia– RigidityRigidity– Tremor
P t l I t bilit– Postural Instability
The four clinical management stagesg gThere are four stages of management for PD
1. Diagnosis phase2. Maintenance phasep3. Complex phase4 Palliative phase4. Palliative phase
Current Therapeutic strategies
1 dopamine levels in the brain1. dopamine levels in the brain (Sinemet, Madopar)
2. metabolism and breakdown of dopamine in the brain (Selegiline, Rasagiline, Entacapone, Tolcapone)
3 Sti l t d i t3. Stimulate dopamine receptors (Pergolide, Cabergoline, Ropinirole, Rotigotine,
Pramipexole, apomorphine)p p p )
Levodopa Therapyp py• Most effective drug for treating Parkinsons
Disease– E.g. Sinemet, MadoparE.g. Sinemet, Madopar
• Long term use is complicated by significantly disabling fluctuations and g y gdyskinesias
Dyskinesiay• involuntary fidgety movements can include twitches,
jerks twisting or writhing movements or simplejerks, twisting or writhing movements or simple restlessness
• can take the form of rapid dance like movements –pknown as ‘chorea’– loose and floppy muscles and too much movement or dystonia• or dystonia – a sustained involuntary contraction of the muscles causing the
affected part of the body to go into spasm
• Typically occur at the peak of levodopa dose, but can l t th b i i d f th d i t lalso occur at the beginning or end of the dose interval

Long-term challenges:Ch i l dChanges in levodopa response
Obeso et al. 2000

Optimising Levodopa Therapyp g p py• Improve consistency of absorption
– Treatments to improve gastric emptying• E.g Reviewing medications which can slow gastric
t iemptying• Treating constipation
T ki d h b f ft l– Taking doses one hour before or after meals• Use smaller doses more frequently• Consider the use of modified release
preparationsp p

Dopamine agonistsp g• Ergot • Non ergot
– Bromocriptine– Lisuride
– Apomorphine – Ropinirole
– Cabergoline– Pergolide
– Pramipexole– Rotigotine (patch)

Long term challenges: Dopamine agonistsDopamine agonists
• Fibrotic reactions (ergot derived)• Retroperitoneal pleuropulmonary cardiacRetroperitoneal, pleuropulmonary, cardiac
• Neuropsychiatric symptoms• Impulse control disorders
– Compulsive gambling Punding– Punding
• Sudden onset sleep• (?all dopaminergic agents)

Complications of missed/late dosesdoses
• Ability to manage symptoms may be lost– Reduced mobility– Increased risk of aspirationIncreased risk of aspiration
• Can be as serious as neuroleptic li t dmalignant syndrome
– Fevers, confusion• ‘Get it On Time Every Time’

Advancing strategiesg g• Continuous delivery of medication for
continuous, stable blood levels & effect• ExamplesExamples
– Dopamine agonistsR ti ti P t h (N ®)• Rotigotine Patch (Neupro®)
• Controlled release pramipexole/ropinirole• Apomorphine infusion
– Levodopa intestinal gel (Duodopa®)
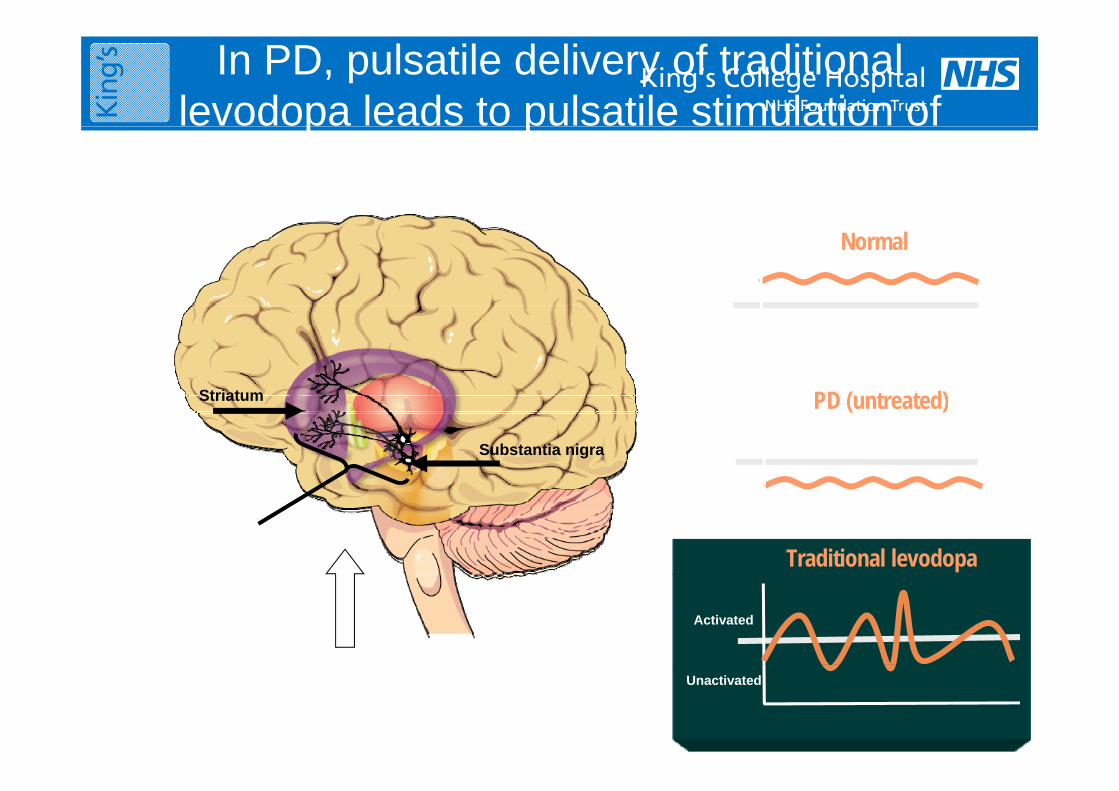
In PD, pulsatile delivery of traditional levodopa leads to pulsatile stimulation of p p
dopamine receptorsDopamine receptor state
Activated
Normalp p
Unactivated
PD ( t t d)Striatum PD (untreated)
Substantia nigra
Striatum
Activated
Traditional levodopaNigrostriatal neuronsdegenerate
Unactivated
Traditional levodopa Activated
Unactivated
Duodopa®p• Continuous infusion of
l d / bid d i i dlevodopa/carbidopa administered with a portable pump directly into h d d j jthe duodenem or upper jejenum
• Surgical procedure for Percutaneous endoscopic gastrostomy tube insertion
• Pump is then programmed to deliver dose at an individualised rate
Surgical Interventiong• Deep Brain Stimulation
– Electrodes in basal ganglia targets
– Contra-indications in cognitive decline/neuropsychiatric problemsdecline/neuropsychiatric problems
• Pallidotomy for severe dyskinesia• Lesional surgery where DBS not possible• Lesional surgery where DBS not possible

The four clinical management stagesg gThere are four stages of management for PD
1. Diagnosis phase2. Maintenance phasep3. Complex phase4 Palliative phase4. Palliative phase

Non-Motor Features of Parkinson’s• Cognitive deficiencies• Depression• Depression • Raised anxiety levels• Olfactory deficiencies (smell and taste)• Olfactory deficiencies (smell and taste)• Sleep disturbance• Fatigue• Fatigue• Pain• Bowel and bladder problems• Bowel and bladder problems• Sexual dysfunction
Depression and Anxietyp y• Depression
– Can affect up to 45% of patientsCan affect up to 45% of patients– Positive results from small studies using dopamine agonists e.g.
pramipexole and ropinirole XL– effects of dopamine stimulation on moodp– Improvement of motor control
– CBT – Cognitive Behavioural Therapy– Antidepressant therapyp py
• AnxietyOften coexists with depression– Often coexists with depression
• Can be responsive to antidepressant therapy (as above)– Can be dopamine dependent
E i tt k h ‘l d i ff’• E.g. panic attacks when ‘levodopa wearing off’
Sleep Dysfunctionp y• Dopamine has a complex role in the sleep/wake
cyclecycle• Insomnia
Diffi lt f lli l– Difficulty falling asleep– Difficulty maintaining sleep
P ibl t t t• Possible treatments– Good sleep hygiene
Slow release levodopa formulation– Slow release levodopa formulation– To improve ‘off’ state symptoms disturbing sleep
– Other agents to improve sleep qualityOther agents to improve sleep quality

Recent/Current Research• Continuous Stimulation
• Neuroprotection• Neuroprotection– Early versus late treatment
• Impact and treatment of NMS• Impact and treatment of NMS– Europar
The Future
• Neurorestoration
• Gene therapyy
N ll t l t ti• Nerve cell transplantation

Parkinson’s diseaseParkinson’s disease
Diagnosis and management in
primary and secondary care
NICE clinical guideline 35
June2006

References(1) Parkinson J, 1817: An Essay on Shaking Palsy, MacmIllan & PDS. London(2) Playfer J, et al. (2001), Parkinson’s Disease in the Older Patient. Arnold, London(3) Clough C et al. (2003), Parkinson’s Disease, Health Press Ltd. Oxford(4) Quinn N. (1997), Parkinson’s Disease: Clinical Features. Balliere’s Clinical
Neurology: 6 (1) 1-16(5) Clarke C (2001) Parkinson’s Disease in Practice Royal Society of Medicine(5) Clarke C. (2001). Parkinson s Disease in Practice. Royal Society of Medicine
Press. London(6) Gelb D, et al. (1999). Diagnostic Criteria for Parkinson’s Disease. Archives of
Neurology 56, pp33-39(7) Hughes A et al (1992). Accuracy of Clinical Diagnosis of Idiopathic Parkinson’s
Disease – a clinico-pathological study of 100 cases. Journal of Neurology, Neurosurgery and Psychiatry 55: pp181-184
(8) Gibb W et al (1988) The relevance of the Lewy body to the pathogenesis of(8) Gibb W et al. (1988). The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson’s Disease. Journal of Neurology, Neurosurgery and Psychiatry 51: pp745-52
(9) Aquilonius S et al; Parkinson’s disease – role of continous dopaminergic ti l ti ESP Bi i Ltd 2012stimulation; ESP Bioscience Ltd; 2012


ELLDOPA trial3%
3%
2%
17%
NEJMNEJM 2004;351:24982004;351:2498

The role of dopaminep• Dopamine acts to oppose acetylcholine• Dopamine inhibitory • Acetylcholine excitatory• Acetylcholine excitatory• Depletion in dopamine results in
hypokinetic disorders such as PD
Parkinson’s Risk Factors• Definite risk factors
– Agef• Highly likely risk factors
– MZ co-twin with early-onset Parkinson’s• Probable risk factors
Positive family history– Positive family history• Possible risk factors
– Herbicides / pesticides– Heavy metalsy– Proximity to industry– Farming communities– Repeated head trauma
P ibl t ti ff t• Possible protective effect– Smoking and dopamine agonists
Signs and Symptomsg y p• Impairment of postural reflexes
– Usually later onset in PD, but earlier onset in Parkinsonism
– Combined with other features, it leads to a high risk of fallshigh risk of falls
• Other features – insidious onset, initially il t l tunilateral symptoms
Management options for specific motor fluctuationsmotor fluctuations
• ‘Wearing off’g– Shorten dosage interval– Pre meal levodopa– Addition of a COMT inhibitor or dopamine agonist– Controlled release levodopa before sleep– Addition of a MOA-B inhibitor
• Early morning dystonia– Late evening or night time dose of controlled release levodopa– Addition of a long acting dopamine agonist
• Dyskinesia– Amantadine at high doses has an antidyskinetic action which may last
t 9 th ith t ff ti P ki ’ t lup to 9 months without affecting Parkinson’s control

Metabolism of L-dopap

Signs and symptoms contg y p• Facial
I i i f bli ki– Impassivity, poverty of blinking• Speech
– Monotonous, hypophonic• Movement
– Decreased manual dexterity, rigid hands & arms ‘frozen shoulder’
• Olfactory abnormalities• Bulbar symptomsBulbar symptoms