pitutary part 1
TRANSCRIPT

Dr.prakash shendeMD ( MEDICINE) CCDCONSULTANT DIABETOGOLIST & CARDIOLOGIST THYROID SPECIALISTASSISTANT PROFESSOR DR.D Y P H PIMPRI
Introduction Diseases of the hypothalamus and pituitary are rare,
Annual incidence is ∼1:50000
The anterior pituitary is "master gland"
The anterior pituitary gland produces six major hormones:
(1) prolactin (PRL),
(2) growth hormone (GH),
(3) adrenocorticotropin hormone (ACTH),
(4) luteinizing hormone (LH),
(5) follicle-stimulating hormone (FSH), and
(6) thyroid-stimulating hormone (TSH)


FUNCTIONAL ANATOMY The pituitary gland is enclosed in the sella turcica and
bridged over by a fold of dura mater called the diaphragma sellae, with the sphenoidal air sinuses below and the optic chiasm above.
The cavernous sinuses are lateral to the pituitary fossaand contain the 3rd, 4th and 6th cranial nerves and the internal carotid arteries.
The gland is composed of two lobes, anterior and posterior, and is connected to the hypothalamus by the infundibular stalk, which has portal vessels carrying blood from the median eminence of the hypothalamus to the anterior lobe and nerve fibres to the posterior lobe.

CLASSIFICATION OF DISEASES OF THE PITUITARY AND HYPOTHALAMUS
Hormone excess-
Anterior pituitary-
ProlactinomaAcromegalyCushing's diseaseRare TSH-, LH- and FSHomas
Secondary - Disconnection hyperprolactinaemia
Hypothalamus and posterior pituitary –
Syndrome of inappropriate antidiuretic hormone

Hormone deficiency –
Anterior pituitary- Hypopituitarism
secondary - e.g. GnRH deficiency (Kallmann'ssyndrome)
Hypothalamus and posterior pituitary - Cranial diabetes insipidus
Hormone resistance –
Growth hormone resistance (Laron dwarfism) Nephrogenic diabetes insipidus
Non-functioning tumours-
Pituitary adenomaCraniopharyngiomaMetastatic tumours

Hypothalamic and Anterior Pituitary Insufficiency
Hypopituitarism results from impaired production of one or more of the anterior pituitary trophichormones.
Reduced pituitary function can result from inherited disorders; more commonly, it is acquired and reflects the mass effects of tumors or the consequences of inflammation or vascular damage.

Etiology of Hypopituitarism - Development/structuralTranscription factor defectPituitary dysplasia/aplasiaCongenital CNS mass, encephalocelePrimary empty sellaCongenital hypothalamic disorders (septo-optic dysplasia, Prader-Willi syndrome, Laurence-Moon-Biedl
syndrome, Kallmann syndrome) TraumaticSurgical resectionRadiation damageHead injuries NeoplasticPituitary adenomaParasellar mass (meningioma, germinoma, ependymoma, glioma)Rathke's cystCraniopharyngiomaHypothalamic hamartoma, gangliocytomaPituitary metastases (breast, lung, colon carcinoma)Lymphoma and leukemiaMeningioma Infiltrative/inflammatoryLymphocytic hypophysitisHemochromatosisSarcoidosisHistiocytosis XGranulomatous hypophysitis

Infiltrative/inflammatoryLymphocytic hypophysitisHemochromatosisSarcoidosisHistiocytosis XGranulomatous hypophysitis
VascularPituitary apoplexyPregnancy-related (infarction with diabetes; postpartum necrosis)Sickle cell diseaseArteritis
InfectionsFungal (histoplasmosis)Parasitic (toxoplasmosis)TuberculosisPneumocystis carinii
Kallmann Syndrome = Defective hypothalamic gonadotropin-releasing hormone (GnRH) synthesis & associated with anosmia or hyposmia due to olfactory bulb agenesis or hypoplasia
The syndrome may also be associated with color blindness, optic atrophy, nerve deafness, cleft palate, renal abnormalities, cryptorchidism, and neurologic abnormalities such as mirror movements.
Defects in the KAL gene, which maps to chromosome Xp22.3
Bardet-Biedl Syndrome- rare genetically heterogeneous disorder characterized by mental retardation, renal abnormalities, obesity, and hexadactyly, brachydactyly, or syndactyly.
Central diabetes insipidus may or may not be associated. GnRH deficiency occurs in 75% of males and half of affected females.

Acquired Hypopituitarism = Pituitary Apoplexy- Acute intrapituitary hemorrhagic Damage to the pituitary and surrounding sellar structures. Its occur spontaneously in a preexisting adenoma; post-partum (Sheehan's
syndrome); or in association with diabetes, hypertension, sickle cell anemia, or acute shock.
The hyperplastic enlargement of the pituitary during pregnancy increases the risk for hemorrhage and infarction.
It is an endocrine emergency that may result in severe hypoglycemia, hypotension, central nervous system (CNS) hemorrhage, and death.
Acute symptoms may include severe headache with signs of meningealirritation, bilateral visual changes, ophthalmoplegia, and, in severe cases, cardiovascular collapse and loss of consciousness.
Pituitary computed tomography (CT) or MRI may reveal signs of intratumoralor sellar hemorrhage, with deviation of the pituitary stalk and compression of pituitary tissue.
Patients with no evident visual loss or impaired consciousness can be observed and managed conservatively with high-dose glucocorticoids.
Those with significant or progressive visual loss or loss of consciousness require urgent surgical decompression.
Visual recovery after surgery is inversely correlated with the length of time after the acute event. Therefore, severe ophthalmoplegia or visual deficits are indications for early surgery. Hypopituitarism is very common after apoplexy.

Empty Sella-
A partial or apparently totally empty sella is often an incidental MRI finding.
These patients usually have normal pituitary function, implying that the surrounding rim of pituitary tissue is fully functional.
Hypopituitarism, however, may develop insidiously.
Rarely, small but functional pituitary adenomas may arise within the rim of pituitary tissue, and these are not always visible on MRI

Tests of Pituitary Sufficiency Growth hormone –Test- Insulin tolerance test: Blood Samples- Regular insulin (0.05–0.15 U/kg IV) –
30, 0, 30, 60, 120 min for glucose and GH Interpretation- Glucose < 40 mg/dL;GH should be >3 g/L, Prolactin –TRH test: 200–500 g IV Blood Samples- 0, 20, and 60 min for TSH and PRLInterpretation- Normal prolactin is >2 g/L and increase >200% of
baseline ACTH-Test- Standard ACTH stimulation test: ACTH 1-24 (Cosyntropin),
0.25 sa mg IM or IV mBlood sample - 0, 30, 60 min for cortisol and aldosteroneInterpretation- Normal response is cortisol >21 g/dL anddosterone response of >4 ng/dL above baseline

TSH
Test- Basal thyroid function tests: T4, T3, TS
sample- Basal tests
Interpretation- Low free thyroid hormone levels in the setting of TSH levels that are not appropriately increased

Hypopituitarism: Treatment ACTH-
Hydrocortisone (10–20 mg A.M.; 5–10 mg P.M.)Cortisone acetate (25 mg A.M.; 12.5 mg P.M.)Prednisone (5 mg A.M.; 2.5 mg P.M.)
TSH L-Thyroxine (0.075–0.15 mg daily) FSH/LH male
Testosterone enanthate (200 mg IM every 2 weeks)Testosterone skin patch (5 mg/d)FemalesConjugated estrogen (0.65–1.25 mg qd for 25 days)Progesterone (5–10 mg qd) on days 16–25Estradiol skin patch (0.5 mg, every other day)
For fertility: Menopausal gonadotropins, human chorionic gonadotropinsGH Adults: - Somatotropin (0.1–1.25 mg SC qd)Children: Somatotropin [0.02–0.05 (mg/kg per day)]Vasopressin- Intranasal desmopressin (5–20 g twice daily)Oral 300–600 g qd

PITUITARY AND (PARA-)SELLAR TUMOURS
Lesion may simply be an incidental discovery during neuroimaging for another indication (e.g. the investigation of cerebrovascular disease).
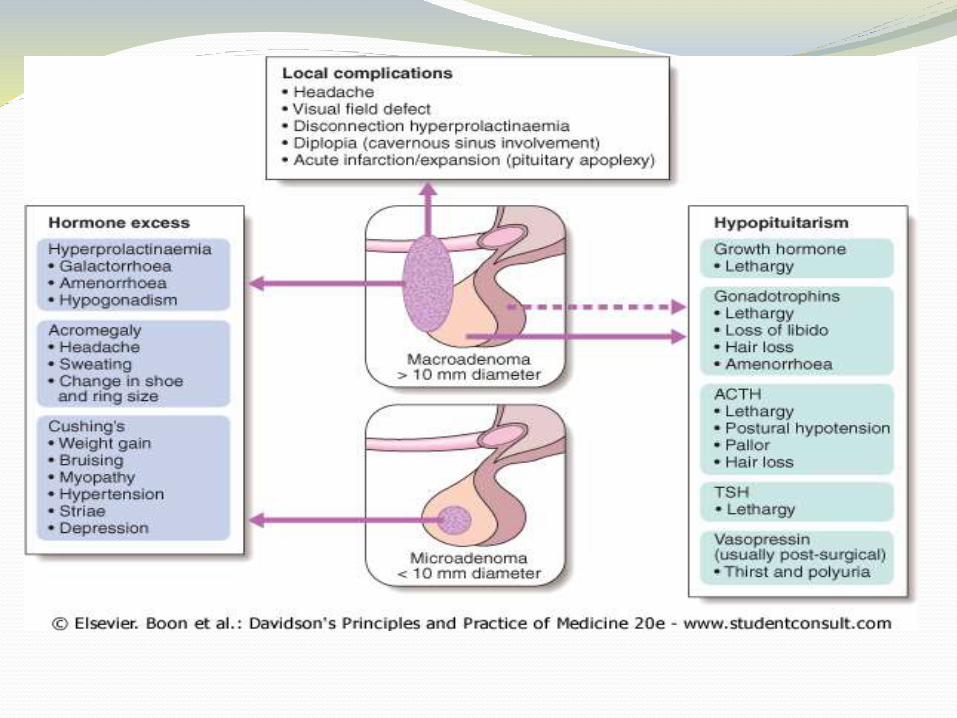
Sellar and para-sellar tumours produce a variety of mass effects, depending on their size and location.
The most common is headache, which is due to stretching of the diaphragma sellae.
Compression of the neural connections between the retina and occipital cortex may lead to a visual field defect. –bitemporal hemianopia or upper quadrantanopia, any type of visual field defect can result from suprasellarextension of a tumour because of compression of the optic nerve (unilateral loss of acuity or scotoma) or the optic tract (homonymous hemianopia).
Lateral extension into the cavernous sinus with subsequent compression of the 3rd, 4th or 6th cranial nerves may cause diplopia and strabismus.

Aetiology and investigations- Majority of intrasellar tumours are pituitary
macroadenomas (most commonly non-functioning adenomas, ) most suprasellar masses are craniopharyngiomas , and para-sellar masses are most commonly meningiomas.
Diagnosis requires surgical biopsy.
All patients with (para-)sellar space-occupying lesions should have pituitary function test
Management If there is evidence of pressure on visual pathways, then
urgent treatment is required.
The chances of recovery of a visual field defect are proportional to the duration of symptoms; full recovery is unlikely if the defect has been present for longer than 4 months.
Serum prolactin is measured before emergency surgery is performed.
If the prolactin is > 5000 mU/l, then the lesion may be a macroprolactinoma and a therapeutic trial of a dopamine agonist for just a few days may successfully shrink the lesion and make surgery unnecessary

SurgeryRadiotherapy Medical Comment
Non-functioning pituitary macroadenoma
1st line 2nd line -
Prolactinoma 2nd line 2nd line 1st lineDopamine agonists
Dopamine agonists usually cause macroadenomas to shrink
Acromegaly 1st line 2nd line 2nd lineSomatostatin analogues Dopamine agonistsGH receptor antagonists
Medical therapy does not reliably cause macroadenomas to shrink
Cushing's disease 1st line 2nd line - Radiotherapy is used in children and to prevent Nelson's syndrome
Craniopharyngioma 1st line 2nd line

Most operations on the pituitary are performed by the trans-sphenoidal approach.
The pituitary fossa is approached via the sphenoid sinus from an incision under the upper lip or through the nose.
Transfrontal surgery via a craniotomy is reserved for suprasellar tumours.
Pituitary function should be retested 4-6 weeks following surgery.
HYPERPROLACTINAEMIA- Hyperprolactinaemia is a common biochemical
abnormality.
The cardinal features are galactorrhoea and hypogonadism.
Galactorrhoea describes lactation without breastfeeding.
Prolactin stimulates milk secretion but not breast development, so that galactorrhoea almost never occurs in men.

HYPERPROLACTINAEMIA Physiological Stress (e.g. post-seizure) Pregnancy Lactation Nipple stimulation Sleep Coitus Exercise Baby crying Drugs Dopamine antagonists Antipsychotics (phenothiazines and butyrophenones) Antidepressants Antiemetics (e.g. metoclopramide, domperidone) Dopamine-depleting drugs Reserpine Methyldopa Oestrogens Oral contraceptive pill Pathological Common Disconnection hyperprolactinaemia (e.g. non-functioning
pituitary macroadenoma) Prolactinoma (usually microadenoma) Primary hypothyroidism Polycystic ovarian syndrome Macroprolactinaemia Uncommon Hypothalamic disease Pituitary tumour secreting prolactin and growth hormone Renal failure

Prolactinoma - Most prolactinomas in pre-menopausal women are microadenomas.
In men and post-menopausal women, presentation is often much more insidious and the tumours are almost invariably macroadenomas at the time of diagnosis.
Macroprolactin (or 'big, big prolactin') is prolactinbound to an IgG antibody.
Many prolactin assays do not distinguish macroprolactin from monomeric (i.e. unbound) prolactin.
Identification requires gel filtration chromatography or polyethylene glycol precipitation techniques.
Macroprolactin cannot cross blood vessel walls to reach prolactin receptors in target tissues and so is less likely to cause the classical symptoms of hyperprolactinaemia.

Presentation and Diagnosis- Amenorrhea, galactorrhea, and infertility are the hallmarks
of hyperprolactinemia in women.
If hyperprolactinemia is sustained, vertebral bone mineral density can be reduced.
Patients may also complain of decreased libido, weight gain, and mild hirsutism.
In men with hyperprolactinemia, diminished libido, infertility, or visual loss (from optic nerve compression) are the usual presenting symptoms.
Gonadotropin suppression leads to reduced testosterone, impotence, and oligospermia..
The diagnosis of idiopathic hyperprolactinemia is made by exclusion of known causes of hyperprolactinemia in the setting of a normal pituitary MRI.
Some of these patients may harbor small microadenomasbelow MRI sensitivity (~2 mm).

Investigations -. Pregnancy should be excluded in all women of child-bearing potential. The upper limit of serum prolactin is ∼500 mU/l (∼14 ng/ml). In non-pregnant and non-lactating patients, monomeric prolactin
concentrations of 500-1000 mU/l are likely to be induced by stress or drugs, and a repeat measurement is indicated.
Levels between 1000 and 5000 mU/l are likely to be due to either drugs, a microprolactinoma or 'disconnection' hyperprolactinaemia.
Levels above 5000 mU/l are highly suggestive of a macroprolactinoma, and the higher the level, the bigger the tumour.
Some macroprolactinomas cause levels over 100 000 mU/l. Patients with prolactin excess should have tests of gonadal function
and T4 and TSH measured to exclude primary hypothyroidism causing TRH-induced prolactin excess.
Unless the prolactin falls after withdrawal of relevant drug therapy, a serum prolactin of > 1000 mU/l is an indication for MRI or CT scan of the hypothalamus and pituitary.
Patients with a macroadenoma also need tests for hypopituitarism

Management Medical -Medical Dopamine agonist drugs are first-
line therapy .
In patients with macroadenomas, drugs can only be withdrawn after curative surgery or radiotherapy and under close supervision.
DOPAMINE AGONIST THERAPY: DRUGS USED TO TREAT PROLACTINOMAS-
Bromocriptine 2.5-15 mg/day8-12-hourly
Available for parenteral useShort half-life; useful in treating infertilityProven long-term efficacy Ergotamine-like side-effects (nausea, headache, postural hypotension, constipation)

Cabergoline 250-1000 μg/week2 doses/week Long-actingReported to have fewer ergotamine-like side-effects Limited data on safety in pregnancy
Quinagolide 50-150 μg/dayOnce daily
A non-ergot with few side-effects Untested in pregnancy Surgical - Dopamine agonists not only lower prolactin levels, but
shrink the majority of prolactin-secreting macroadenomas.Thus, surgical decompression is not usually necessary unless the
macroadenoma is cystic.However, in patients who are intolerant of dopamine agonists,
microadenomas can be removed selectively by trans-sphenoidalsurgery with a cure rate of about 80%.
The cure rate for surgery in macroadenomas is lower. Radiotherapy- External irradiation may be required for some
macroadenomas to prevent regrowth if dopamine agonists are stopped
