pioneers in global health_30 years of history in the hospital clínic de barcelona
TRANSCRIPT

Pioneers in Global Health
Years of History in the Hospital Clínic de Barcelona

30 Years of History in the Hospital Clínic de Barcelona
Pioneers in Global Health
The beginning of the Tropical Medicine Unit at the Hospital Clínic
From Barcelona to Tanzania: research takes off
The work in Mozambique in the nineteen nineties
The research boom in CISM and the creation of CRESIB
The Tropical Medicine and International Health Department and the challenge of the new wave of immigration
The Barcelona Institute for Global Health, taking science one step further
Acknowledgements
P. 15
P. 31
P. 45
P. 67
P. 85
P. 101
P. 117
Introduction
Prologue
P. 9
P. 7

7
F or those of us involved in the day-to-day work at Bar-celona’s Hospital Clínic, looking back and reflecting on the challenges taken on by this institution over the years is a good way of ensuring that we continue to follow the right path. The decisions taken, however difficult they may have been or however risky they may appear in retrospect, have made this hospital a centre of excellence based on a strong conviction that training and research are essential ingredients
for improving healthcare. Tropical medicine and international health is one of the specialties our hospital has become well known for both in this country and abroad. Even now, over a hundred years later, it is important to remember that the Hospital Clínic was founded to attend to the needs of the most vulnerable groups in our society. As the city grew, prosperity in- creased and the diseases treated at the hospital were the same as those found in most developed countries. The need to extend the limits of our knowledge and find new directions led us, in the nineteen eighties, to confront diseases which at that time primarily affected people in faraway places, but which have now become part of our daily lives. A new era brought new challenges. At the start of the age of globalisation, Spain was just starting to build a democratic society and to move out into the world with confidence. It was no coincidence there-fore that it was around the same time—in 1984— that the Tropical Medi- cine Unit was founded. Although other institutes and hospitals were already working in this field in other parts of Europe, especially in countries that had close links to ex-colonies, for the Hospital Clínic the idea of developing its own expertise and taking on the challenges posed by global health was a logi-
Prologue Pedro Luis Alonso Head of the Tropical Medicine and Inter-national Health Department at the Hospital Clínic de Barcelona
Josep Maria Piqué Director General of the Hospital Clínic de Barcelona

98
Acal extension of the commitment made by its founders to serve society’s most vulnerable populations. What appeared at the time to be an unusual choice and a somewhat marginal addition to the hospital’s traditional departments, has over the years become an ever more relevant field. And the marked increase in numbers of travellers and immigrants has not been the only reason for this change. A number of other factors have intervened in the success of these thirty years. The first of these has been the hospital’s capacity to offer quality care to patients with diseases that are uncommon in Spain and often clinically complex. The second component of this success has been the work undertak-en to train new generations of specialists, both at the hospital and at the Uni-versity of Barcelona. As this is a university hospital committed to the highest academic quality, it was logical that the first chair in international health was created in the Faculty of Medicine. The third ingredient was the effort to find new answers through research, which in turn led to the creation of the Man-hiça Health Research Centre (CISM) and the Barcelona Centre for Interna-tional Health Research (CRESIB). Lastly, this hospital has always striven to apply its vision, values and action to real world challenges and tried to have a real impact where the problems are most acute. For this reason, our work has focussed not only on our local context but also on places further afield, primarily in Tanzania, Mozambique, Morocco and Bolivia. The following pages describe the road travelled from the time the new Tropical Medicine Unit at the hospital started treating its first patients to its transformation into a Tropical Medicine and Internation-al Health Department and the recent foundation of the Barcelona Institute for Global Health (ISGlobal). This institution is a response to the challenges posed by global health. It is made up of a staff of two hundred people who work in different areas, ranging from research into the molecular basis of dis-eases and their geographical distribution to the development of new vaccines and preventive strategies. The aim is that the knowledge generated by this work will be translated into real improvements in the medical care of patients and will shape new public health policies. In a globalised world, the success of the endeavours described in this book spur us on to further reduce the huge gap in health equity that gives rise to neglected diseases and deprives many margin-alised people of adequate, quality healthcare.
A huge map of the world hanging on the wall is the first thing that catches your eye when you enter rooms 63 and 64 in the Hospital Clínic on Carrer Roselló. A map and a calendar are essential tools in any trop-ical medicine specialist’s consulting room. The day we visited the hospital when researching this book in early summer 2014, the doctors had seen twenty two patients, mostly Catalans returning from abroad, one with a possible case of malaria.
Three decades have passed since Dr Manuel Corachan started seeing his first patients in the Hospital Clínic. The raison d’être of this service is as strong today as it was then, but the global context is very different. Today, diseases travel at the speed of a plane and can spread to an-other country in a matter of hours. Health problems once only endemic in one part of the world have now become common in others. The globalisation of diseases is reflected in the changes in the terms used to describe this field of work. Thirty years ago, tropical medicine was the most common term. A legacy of Europe’s colonial past, it is no longer used today except in medical contexts or in the name of certain institutions such as the department at the Hospital Clínic. Later, during the nineteen nineties the expression international health gained in popularity when it became clear that diseases did not respect borders. More recently, global health has become the preferred option in both academia and scien-tific research as well as in the area of international aid policy. All three terms are used in this book, with greater emphasis on one or another de-pending on the historical context. The following chapters describe the main events in these thirty years of progress made in global health in the Hospital Clínic,
Introduction

1110
first and foremost in healthcare. What started out as a Tropical Medicine Unit has evolved to become the Tropical Medicine and International Health Department. Similarly, the small travel advice service that opened its doors in the eighties has grown over the years to become a modern Travel Clinic (SAVI). In research, the Epidemiology and Biostatistics Unit was created in the Hospital Clínic in 1992 and the Manhiça Health Research Centre (CISM) was set up four years later. The creation of CISM marked a turning point that eventually led to the foundation of the Barcelona Centre for International Health Research (CRESIB) in 2006. The most recent leap forward was taken in 2010 with the creation of the Barcelona Institute for Global Health, of which CRESIB is now an integral part. Malaria vaccine clinical trials in Mozambique and research into better treatments for patients with chronic Chagas disease in Bolivia are just two examples of the large volume of research carried out in Barcelona and parts of the world where these diseases are endemic. The papers published over the years have earned the Hospital Clínic an inter-national reputation for its contribution to the scientific and medical advances made in the field of global health. In addition, as a result of its work in Africa and Latin America, the hospital has become a strategic partner of the Spanish Agency for International Development Cooperation (AECID). Throughout this journey, the longstanding relation- ship between the hospital and the University of Barcelona’s Faculty of Medicine has continued to flourish. The events in this story came about mainly because of the vision of the people who have played leading roles. Among them are Manuel Corachan, founder of the Tropical Medicine Unit (who was later joined by Joaquim Gascon and Clara Menéndez), and Pedro Alonso, the first person to work in the Epidemiology and Biostatistics Unit. All these doctors were pioneers, people who chose to follow unusual paths. Working together, on the basis of common interests and similar experiences of studying and working abroad, they succeeded over the years in building a solid team and making the Tropical Medicine and International Health Department an in-novative and cutting edge facility. In the Hospital Clínic they found an ideal home. They found fertile ground where they could put down roots, where they could grow and develop their ideas with the support of people who could
recognise the potential of a specialty which, at that time, appeared to be marginal—people like Dr Joan Rodés, the former director general of the hospital.There have been many others who, through their commit-
ment, hard work and expertise, have also made a contribution and left their mark. They have played important roles in Barcelona and elsewhere, some by treating patients and others by contributing to the effort to find answers to the many questions that arise in consulting rooms and laboratories. The leitmotif running through the whole story is the indissoluble link between healthcare, training and research—the three pil-lars of the work carried out in global health at the Hospital Clínic. These three components are found time and time again, both in Barcelona and elsewhere. This book was born of a desire to celebrate the jour-ney travelled thus far and the achievements attained along the way. It is a story that has never been written before and the task was undertaken in spite of the risks inherent in any attempt to look back and write a history.
The Hospital Clínic, founded in 1906, is located in the Eixample neighbourhood of Barcelona. © Hospital Clínic de Barcelona
12
The intention was not to write a summary of activities, but rather to trace the steps and weave the story from the memories and anecdotes of some of the people who have travelled different parts of the journey. Finally, we would like to conclude this introduction by thanking the more than fifty people interviewed, who have shared their time and their memories and without whom the book would not have been possible. Many of them are still involved in this important work, in Barcelona and elsewhere, and some have moved on to new ventures. What most of them have in common is that they have shown an almost moving commitment to their task, a passion for their work, for medicine, research and science, for finding answers to the major problems facing global health, and finally, a passion for contributing through their work to making the world a better place.

The beginning of the Tropical Medicine Unit at the Hospital Clínic

17 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
It might be a chance encounter, a defining moment, a fortuitous event; the beginnings of a sto-ry can often be traced back to a small but important past event, to something that happened long ago that acted as a catalyst for what was to come. For Ma-nuel Corachan, it was the trips he made as a teenager during the nineteen fifties that sparked
his interest in pursuing a career in the field of tropical medicine. Encouraged by his grandmother, he left his hometown of Bar-celona during the summer holidays and went to stay with family friends in France. There he met several doctors who had travelled and lived in Africa, a continent largely unknown to most Spanish people at the time, except for the few who were missionaries or lived in the Spanish colony of Equatorial Guinea.
Those encounters made a deep impression on the visiting teen-ager, as a whole new world opened up before his eyes. Now retired and enjoying the peace of his house in Massanes, Girona, Manuel looks back on those times and reflects: “listening to those doctors talking I realised that tropical medicine was an academic disci-pline just like any other specialty. I understood how—even with very few resources—one could have a huge impact on people’s lives. And I heard how in other countries people were already pub-lishing scientific papers in highly credible journals, while here in Spain the only thing we ever heard about was the DOMUND”.1
Tropical medicine, formerly known as colonial medicine, was a spe-cialty born of the need for the European powers to protect their armies and other personnel living and working in their colonies at a time when diseases like malaria, yellow fever and sleeping sickness represented an even greater threat to the colonial pro-jects than wars.2 It was not for nothing that Rudyard Kipling once famously described Africa as “the white man’s grave”.3 The more the colonial territories grew, the more military and administrative personnel were needed, and their governments were responsible for their health and wellbeing. In 1898, the Englishman Patrick Manson, the “Father of Tropical Medicine”, wrote the first text-book on tropical diseases. Indeed, the end of the nineteenth centu-ry was an era of important discoveries, a time when scientists first identified the microbes, parasites and vectors that cause diseases
1 DOMUND is the Spanish acronym for World Mission Sunday, the day set aside every year by the Catholic Church worldwide to raise funds for the church’s missionary activities.2 Deborah J. 2012. Networks in tropical medicine: internationa-lism, colonialism, and the rise of a medical specialty, 1890-1930. Stanford University Press. p.123 Idem, p.13
Background
On the previous double-page spread, from left to right: Clara Menéndez, Manuel Corachan, Pedro Alonso and Joaquim Gascon talk about their memories and experiences of the last thirty years.
Photographs on pages 14-15, 30-31, 44-45, 66-67, 84-85 and 100-101 © Borja Ballbé

1918 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
Manuel Corachan worked for five years at a hospital in Mwanza, Tanzania. © Manuel Corachan archive
4 Pérez Abadía C., Sabaté Caselles F.Revistas Españolas de Medicina Tropical, en Medicina, ideología e Historia en España (siglos xvi-xxi), coordinated by R. Campos, L. Montiel, R. Huertas. Spanish Na-tional Research Council, p. 462.
5 Idem, p.461-3
Doctor Schweitzer’s reply from Gabon to the letter Manuel Corachan wrote in 1963. © Manuel Corachan archive
Manuel Corachan still treasures the letter and stamped envelope from Gabon. © Manuel Corachan archive
such as trypanosomiasis and malaria. A growing community of European scientists saw the colonial expansion as an opportunity for new research that would help advance the emerging discipline, with the microscope as one of the most important tools.
While Great Britain, Belgium, France, Germany and Portugal were setting up research institutes and schools of tropical med-icine, and doctors in those countries were starting to publish pa-pers in specialised journals, Spain was facing up to the loss of its last insular colonies in America and the Philippines, with all that that entailed. With no large colonial territory for field research ex-cept Equatorial Guinea, the contribution Spain was able to make to the field of tropical medicine on an international level was limited compared to its European competitors. Furthermore, the country remained on the margins of the main international networks be-ing set up by scientists and doctors from different countries. Of the few Spanish journals that sprung up during that period, the only one comparable to the European publications of the time was Medicina de los Países Cálidos, a bimonthly journal edited by Gusta-vo Pittaluga, which only survived eight years, from 1928 till 1936.4
The Italian-born Gustavo Pittaluga was one of the most important scientists in Spain in the field of tropical medicine during the first half of the last century. He undertook a series of studies on malaria in Spain between 1902 and 1903 and led expeditions to the Spanish territories on the gulf of Guinea to study sleeping sickness in 1909. He was appointed professor of parasitology and tropical patholo-gy at the University of Madrid and made several failed attempts to establish a Tropical Medicine Institute in Malaga or Granada. At a conference held at the Barcelona Academy of Medicine, Pi- ttaluga proposed setting up a tropical medicine clinic and research centre outside Barcelona, but this project also failed to get off the ground due to a lack of funding. In recognition of his interna-tional renown, Pittaluga was asked to organise the Third Inter-national Congress on Malaria in Madrid in October 1936.5 How-ever, with the start of the Spanish Civil War the event, like many others, was postponed and Pittaluga subsequently had to go into exile. The end of the war in 1939 marked the beginning of a for-ty year-long dictatorship in Spain stifling progress in many areas. The country became even more isolated from the advances made in the rest of Europe in the treatment of tropical diseases and from training and research initiatives in the field of tropical medicine.
It was in this context of na-tional censorship and isolation in all areas, including science, that the teenage Manuel Cora-chan made his summer visits to France and discovered the world of tropical medicine. Re-membering the final year of his medical degree at the Universi-ty of Barcelona in 1963, he says: “I knew I wanted to specialise in tropical medicine and go abroad. But there wasn’t anyone who could help me in Spain. So I wrote a letter to Doctor Al-bert Schweitzer, a Swiss theolo- gian and missionary who lived
and worked in Gabon. I asked him for advice. And this man, win-ner of the Nobel Peace prize, was humble enough to reply in his own handwriting to a medical student from Barcelona who said he wanted to go to the tropics”. Still amazed by that response, Ma-nuel has kept both the letter written over fifty years ago and the envelope it came in bearing a stamp from Gabon. He followed Dr Schweitzer’s advice: upon finishing his degree he spent two years working in a rural hospital in Switzerland and then attended a course on Tropical Medicine in Amsterdam. From there he went to a hospital in Ghana where he had to do “a bit of everything”. Following a short stay in Barcelona, his second job was on the shores of Lake Victoria, where between 1973 and 1978 he worked for Medicus Mundi International in a hospital in Mwanza, Tanza-nia. His third and last post abroad before finally returning to Bar-celona was in Papua New Guinea, where he taught and worked as a doctor in a hospital in the capital city of Port Moresby.
During the time Manuel trained and worked in Europe and Afri-ca, important developments had started to take place in Barcelo-na. These changes would eventually help him to find an environ-ment more open to his vision of establishing a tropical medicine unit at the Hospital Clínic.

2120 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
One significant event was the foundation of Medicus Mundi in Spain, an organisation that had been set up in Germany in 1963. In the same year, Salva-dor Cortadellas—a Spanish doctor interested in the health of people in less well developed countries—together with the gynaecologist Francisco Abel, set up a medical-missionary
association. On hearing about the work of Medicus Mundi, these two doctors decided to integrate the new Spanish association into the German based network and established a Spanish branch of Medicus Mundi at the end of 1963. The organisation gradually extended its presence to different Spanish provinces and initiated activities that today fall under the umbrella of aid and development.
In the second half of the nineteen sixties, following the foun-dation of Medicus Mundi, a growing number of Spanish health professionals were interested in going abroad to provide health-care in less well developed countries. This situation made obvi-ous the significant deficiency in Spain of information about trop-ical medicine and the lack of training in this specialty. As Vicenç Cararach, another Hospital Clínic doctor who was also very in-volved in the work of Medicus Mundi explains: “We started to send health professionals— doctors and nurses—and we saw they weren’t trained in tropical diseases because these weren’t includ-ed in the curriculum of the medical degree. The State National School of Public Health had organised some courses on malar-ia. But their focus was on parasitology and microbiology and, in any case, those courses were not running at that time. Spain had a small colony in Equatorial Guinea where there was malar-ia and other diseases, such as trypanosomiasis, but there weren’t any courses for people who wanted to work in such places and Medicus Mundi didn’t want to send inexperienced people.”
The beginnings of international aid in Spain
“When I was national secretary and Dr Salvador Cortadellas was president of the organi-sation” says Vicenç Cararach, “we began to entertain the idea of starting up a training course in Tropical Medicine. I was a teacher and I was working here in the Hospital Clínic. So I went to see Dr Agustín Pumarola, Professor of Microbiology and
Parasitology, the dean and the vice-dean to ask for their permission to run a tropical medicine course at the University of Barcelona. And that is how the first course in tropical medicine came about. It was held in the Faculty of Medicine and organised by Medicus Mundi.” The course ran for many years and especially Professor María Teresa Jiménez de Anta and Dr Jordi Mas gave it their full support. It was the start of what, forty years later, has become the University of Barcelona’s Master of Global Health programme.
Vicenç Cararach explains how the course “from the start, had a significant clinical component”. Manuel Corachan proposed a syllabus that not only included an overview of tropical diseases from the point of view of microbiology and epidemiology, but also focussed on the clinical aspects of how to treat a patient. In 1971, we set up the first course as best we could and we invited the professors of the faculty to teach the parts of their subject that were related to tropical medicine. However, as the classes were very theoretical we soon asked for help from European schools, specifically the one in Antwerp, and as soon as we could we re- placed the professors with professionals who had worked in tropi-cal countries and who had relevant experience.”
Manuel Corachan taught on the course as often as his job in Tan-zania would allow him to and, for a time, was the course director. Seeing what had happened in other European countries, he fore-saw that with the changing political context and gradual open-ing up of Spain, the number of travellers and migrant workers, until then almost non-existent, would soon grow. As a result, he warned, the prevalence of imported diseases would also increase, making it ever more necessary to have a health service specialised in tropical medicine.
The first training courses in tropical medicine
2322 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
On his return to Barcelona from Tanzania in 1978, Manuel com- municated his viewpoint to the Catalan Government’s Health De-partment. But it was not till five years later that the authorities were finally convinced of the need to set up a specialist tropical medicine unit in the Hospital Clínic.
“We began to see aid workers returning with tropical diseases; they had to go to tropical medicine schools in other parts of Eu-rope when it became obvious that nobody here could treat them,” explains Vicenç Cararach. “We also thought that there should be a clinic where students could observe real cases, and not just study the theory. In a city like Barcelona and a country like Spain, there was a need for a tropical medicine school and a hospital unit for treating patients. So we insisted on this. Representing Medi-cus Mundi and the Hospital Clínic, I went together with Dr Lluís Salleras to see Dr Josep Laporte, the Catalan Government’s Minister of Health, to propose the establishment of a tropical medicine unit.”
In June 1984, the first steps were finally taken when Manuel Cora-chan was given the job of setting up the Tropical Medicine Unit within the Infectious Diseases Department of the Hospital Clínic.
It is often the case that the start of an innovative activi-ty is not easy and the case of the Tropical Medicine Unit was no exception to the rule. Looking back on the last three decades, Manuel emphasis-es that it was in those early years that he faced the greatest challenge. In spite of the sup-
port of the hospital directors, he met a certain degree of resist-ance from his peers, who were cynical about the idea of setting up the unit. They questioned its use. “What is it for?” they asked. According to them these tropical diseases were already being treat-ed. “One has to have first-hand experience of these diseases, one has to have treated them in the field”, Manuel says. “However some peo-ple did not see the need to have someone with that experience.”
The greatest challenge was convincing the medical community that, far from being “missionary’s medicine”, tropical medicine was in fact an academic discipline using diagnostic tools and lab-
The creation of the Tropical Medicine Unit
oratories just like any other. “Many of my colleagues had an im-age of my time in Africa as a missionary surrounded by starving children covered with flies. There was so much ignorance. They could never have even dreamt that the hospital where I worked in Tanzania had 600 beds and a laboratory, that I could order ra-diographs, that I diagnosed on the basis of imaging, that I took decisions… They thought that I was there [in the Hospital Clínic] as a missionary, they almost believed that I was treating patients with an amulet. Their attitude began to change when they saw that tropical diseases not only affected immigrants and that I was not just a missionary, but that many Spaniards also got these diseases, and that some of them were gravely ill!”
The other institution that treated tropical diseases in Barcelona at that time was the former Drassanes Diagnostic Centre headed up by Dr José Luis Bada, which today has become the Tropical Medicine and International Health Unit, Primary Health Care Drassanes Centre.
Initially Manuel Corachan’s position in the hospital was that of attending physician but the following year, in 1985, he was made Head of Section when the unit became a Section of the Infec-tious Diseases Department. “Before the unit was created” he says, “they used to see what they thought were isolated cases. My first presentation at a clinical meeting with colleagues at the hospital was very indicative of what the unit was achieving. First I talked about the twelve cases of malaria that had been diagnosed in the five years before the unit was established and the very high mor-tality rate, with a fatal outcome in four or five cases. Then I pre-sented the sixty cases I had treated over the first year and a half since the unit started, with no deaths. We had had three cases in intensive care, but all three patients had been saved. This was de-finitive proof of the need for specialised care. There were many other diseases that had never been diagnosed before the unit ex-isted, such as schistosomiasis. I began to show how there were certain problems that were not diseases themselves but rather symptoms of something else, such as anaemia and cardiac insuffi-ciency, both of which can be caused by intestinal parasitosis. With all this evidence we showed staff from other departments and hospitals that these diseases were becoming more common here. They were becoming more visible.”
“Where have you been? has become an essential part of the interrogation of a patient. In these days of fast and frequent travel there is no infection

2524 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
endemic to one part of the world which may not appear in another (…). It is essential for the European medical student to know something of the diseases which may be brought to him from the outside.”6
These prophetic words, written by the visionary Brian Mae-graith, had already appeared in a paper entitled “Unde venis?” (‘Where do you come from?’) published by the medical journal The Lancet in 1963. The man who would become one of the fa-thers of global health gave Manuel Corachan a copy of the article in October 1983, warning him that Spain would follow the steps of other European countries. “When you have set up the clinic, don’t forget about the travellers”, Brian Maegraith told Manuel. A piece of advice that turned out to be true. “Unde venis?” became Manuel’s mantra.
By then, the first immigrants from Africa coming to Catalonia had started to settle in the Maresme area north of Barcelona and the Tropical Medicine Section was seeing an increasing num-ber of travellers, especially by the end of the 1980s when there was a boom in international tourism. They were seeing more and more patients coming back from a trip with diseases that could have been prevented, people who had gone away without any pre-travel information or advice. This was not the norm in other European countries.
As a result of the cases he was seeing, Manuel Corachan un-dertook a study to demonstrate the need for a travellers’ advice service. With the help of sev-eral travel agencies, one of his assistants interviewed trav-ellers at the check-in area of Barcelona-El Prat airport. He asked them where they were
travelling to and what preventive measures they had taken. The re-search showed that, although vaccination centres existed, there were no services providing people with pre-travel advice. “We saw how many people were travelling without the appropriate vaccines and had not received any pre-travel advice”, Manuel explains. “They hadn’t received any information. They had not been told things like ‘Where you are going there are many health problems for which there are no vaccines or treatment but these can be prevented by
The travellers’ advice service
6 Maegraith B. Unde venis?, The Lancet, 23rd February 1963.
The question “unde venis?” became Manuel Corachan’s mantra. © Manuel Corachan archive
2726 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
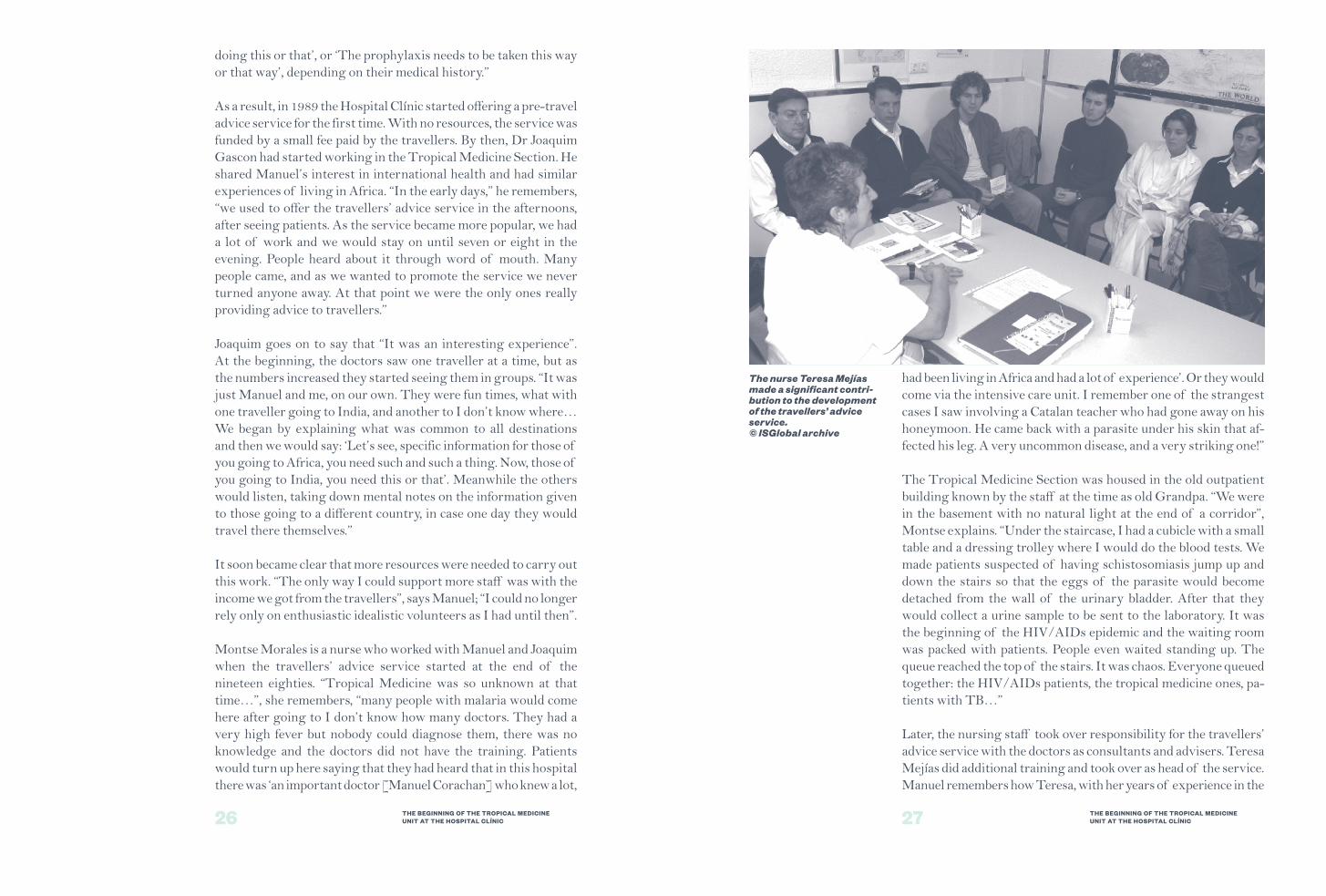
The nurse Teresa Mejías made a significant contri-bution to the development of the travellers’ advice service. © ISGlobal archive
doing this or that’, or ‘The prophylaxis needs to be taken this way or that way’, depending on their medical history.”
As a result, in 1989 the Hospital Clínic started offering a pre-travel advice service for the first time. With no resources, the service was funded by a small fee paid by the travellers. By then, Dr Joaquim Gascon had started working in the Tropical Medicine Section. He shared Manuel’s interest in international health and had similar experiences of living in Africa. “In the early days,” he remembers, “we used to offer the travellers’ advice service in the afternoons, after seeing patients. As the service became more popular, we had a lot of work and we would stay on until seven or eight in the evening. People heard about it through word of mouth. Many people came, and as we wanted to promote the service we never turned anyone away. At that point we were the only ones really providing advice to travellers.”
Joaquim goes on to say that “It was an interesting experience”. At the beginning, the doctors saw one traveller at a time, but as the numbers increased they started seeing them in groups. “It was just Manuel and me, on our own. They were fun times, what with one traveller going to India, and another to I don’t know where… We began by explaining what was common to all destinations and then we would say: ‘Let’s see, specific information for those of you going to Africa, you need such and such a thing. Now, those of you going to India, you need this or that’. Meanwhile the others would listen, taking down mental notes on the information given to those going to a different country, in case one day they would travel there themselves.”
It soon became clear that more resources were needed to carry out this work. “The only way I could support more staff was with the income we got from the travellers”, says Manuel; “I could no longer rely only on enthusiastic idealistic volunteers as I had until then”.
Montse Morales is a nurse who worked with Manuel and Joaquim when the travellers’ advice service started at the end of the nineteen eighties. “Tropical Medicine was so unknown at that time…”, she remembers, “many people with malaria would come here after going to I don’t know how many doctors. They had a very high fever but nobody could diagnose them, there was no knowledge and the doctors did not have the training. Patients would turn up here saying that they had heard that in this hospital there was ‘an important doctor [Manuel Corachan] who knew a lot,
had been living in Africa and had a lot of experience’. Or they would come via the intensive care unit. I remember one of the strangest cases I saw involving a Catalan teacher who had gone away on his honeymoon. He came back with a parasite under his skin that af-fected his leg. A very uncommon disease, and a very striking one!”
The Tropical Medicine Section was housed in the old outpatient building known by the staff at the time as old Grandpa. “We were in the basement with no natural light at the end of a corridor”, Montse explains. “Under the staircase, I had a cubicle with a small table and a dressing trolley where I would do the blood tests. We made patients suspected of having schistosomiasis jump up and down the stairs so that the eggs of the parasite would become detached from the wall of the urinary bladder. After that they would collect a urine sample to be sent to the laboratory. It was the beginning of the HIV/AIDs epidemic and the waiting room was packed with patients. People even waited standing up. The queue reached the top of the stairs. It was chaos. Everyone queued together: the HIV/AIDs patients, the tropical medicine ones, pa-tients with TB…”
Later, the nursing staff took over responsibility for the travellers’ advice service with the doctors as consultants and advisers. Teresa Mejías did additional training and took over as head of the service. Manuel remembers how Teresa, with her years of experience in the

2928 THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
THE BEGINNING OF THE TROPICAL MEDICINE UNIT AT THE HOSPITAL CLÍNIC
The staff of the Tropical Medicine Section in the mid nineteen nineties. From left to right: Laura Schiaffi (a resident physician), Manuel Corachan, Encarna Caralt (administrative officer), Teresa Mejías and Joaquim Gascon. © Teresa Mejías archive
Psychiatry department, was a great addition to the Tropical Medi-cine Section and gave a great boost to the travellers’ advice service.
Those were the early days—pioneering in Spain—of the work carried out in the field of tropical medicine in the Hospital Clínic. Increasingly, the hospital staff themselves travelled more and more, on holiday or as aid workers, and they would come to Ma-nuel Corachan and Joaquim Gascon for advice about the preventive measures they should take. In this way, the work of the Section became better known within the hospital.
Looking back on those early years, Manuel says: “Many young doctors helped me out selflessly because all they wanted was to learn. Without them, I wouldn’t have been able to deal with the volume of clinical work. It wasn’t until the nineteen nineties that we were officially included in the rotations of medical residents as part of the programme for Internal and Preventive Medicine”.However providing medical care was not the only work undertaken by the Tropical Medicine Section. As has already been mentioned, the leitmotif of this thirty-year-long story has been that health-
care, training and research form an indivisible triangle, with each one feeding from the others. As a result, while he was treating patients, Manuel Corachan also maintained his international contacts and continued teaching at the University of Barcelona, and in Switzer-land, Italy and Tanzania. Together with Joaquim Gascon, he under-took several research projects dealing with schistosomiasis, enter- opathogens and the so-called traveller’s diarrhoea. Whatever was possible with the limited human resources and capacity of the Tropical Medicine Section. It was a taste of what was to come. As will be seen in the following chapters, research in international health grew exponentially during the nineteen nineties, with the establishment of the Epidemiology and Biostatistics Unit and the arrival of Clara Menéndez and Pedro Alonso at the Hospital Clínic.

From Barcelona to Tanzania: research takes off

33 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
There was a defining moment in autumn 1988, when Manuel Corachan attended the Interna-tional Conference for Tropical Medicine and Malaria in Ams- terdam and met Pedro Alonso, a young epidemiologist from Madrid who at the time was working for the British Medical Research Council in Gambia.
This encounter turned out to be a turning point in the script of this story. It did not take either of the two long to see how, with Manuel’s clinical focus and Pedro’s experience in research and ep-idemiology, they complemented each other perfectly.
Shortly after that first meeting, Manuel visited Pedro in Gambia where the epidemiologist was conducting an important study on the use of insecticide-treated nets to prevent malaria, together with his wife, Clara Menéndez, who was working on maternal and child health. Manuel recalls how they both said “wouldn’t it be great if we could work together some day”. They could not have imagined that one day their wish would come true and that they would meet up again in the Hospital Clínic and develop their work in international health to an outstanding level, making it a bench-mark for the rest of Spain.
The Hospital Clínic has long been recognised as an innova- tive and pioneering institution in Spain, and the hospital’s identity is largely defined by its research output. “Biomed-ical research was very strong here before 1936”, explains Joan Rodés, the president of the Au-gust Pi i Sunyer Biomedical Re-
search Institute (IDIBAPS). “The most influential researcher was August Pi i Sunyer, the first doctor ever to give insulin to a European patient. But during the Civil War, many researchers were exiled to other countries and many never returned. The war created an intellectual desert.”
A crucial encounter
The Hospital Clínic and the importance of research

3534 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
Since the nineteen seventies, the hospital has become a centre of excellence in research and healthcare. © Hospital Clínic de Barcelona
Since it was founded, the Hospital Clínic has always been closely linked to the Faculty of Medicine. At the time it was built, the Hospital was one of the city’s grandest buildings. © Hospital Clínic de Barcelona
The creation of the Epidemiology and Biostatistics Unit
The importance of research and international relations resur-faced in the nineteen seventies. In 1973, in the context of grow-ing social and political pressure and protests by students seek-ing greater freedom, the Hospi-tal Clínic underwent a massive change. “We knew that if we did medical research in the hospital, the quality of care would im-prove because we would acquire a critical understanding of the practice of medicine”, explains
Joan Rodés. Historically, the Hospital Clínic was structured around a series of departments each one headed by the professor of the specialty and equipped with its own laboratory, X-ray, etc. “It was madness, but it was the product of history.” He continues: “I will always remember how a few of us used to get together at the Bar El Velódromo on Carrer Muntaner. Most of us had studied in Paris and we said ‘This can’t go on’. In 1971, a very important strike took place and a representative committee of doctors was set up. As a result significant changes were made in the hospital’s organisational structure, bringing it closer to the model used in more advanced European countries at the time. New departments were created and a centralised laboratory and radiology service shared by all. That’s when the concept of research revived. Those of us who had been abroad managed to gain recognition as scientific
doctors, and well, that’s how the big change was achieved”.
One example of the growing importance of research and international relations was the institution of the sabbatical in 1979. Since then four doctors are authorised every year to take sabbatical leave from their work at the Hospital Clínic to do research in a foreign institution.
Joan Rodés was one of the key figures in promoting this initiative: “It was vital for people to leave for a while, for them to see a different kind of medical practice— more scientific, more critical—to really experience what high level research was all about”.
The Hospital Clínic’s research initiatives were further strength-ened by the State Law of Clini-cal Trials, which came into force in 1988. As a result of the new legislation, the Clínic Founda-tion for Biomedical Research was set up to administer all the re-search projects and their funding. A couple of years later, the Insti-
tute of Health Carlos III (the main public body responsible for funding, managing and executing biomedical research in Spain) made it com-pulsory for hospitals to have an Epidemiology Unit if they wanted to receive support from the national Health Research Fund. This gave additional impetus to the Hospital Clínic’s research projects and led, in 1992, to the creation of the Epidemiology and Biostatistics Unit. And it was literally a unit: there was only one position.
By that time, after working in Gambia for several years, Pedro Alonso and Clara Menéndez had returned to Madrid. Pedro ap-plied for the position at the Epidemiology Unit and at the same time coincidence intervened and Clara was recruited for a position in the Tropical Medicine Section directed by Manuel Corachan.
Joan Rodés, at that time the general director of Hospital Clínic, remembers the beginning of the Epidemiology and Biostatistics Unit and says: “In the selection process I chose Pedro because he had a scientific mind. I wanted to promote the concept of the scientist-doctor and there weren’t very many of them in Spain”.
That is how Pedro and Clara came to Hospital Clínic and how the idea of working with Manuel Corachan began to crystallise.
Looking back on her early days at the Tropical Medicine Section, Clara recalls: “I found two people [Manuel and Joaquim] who were making a tremendous effort, working very hard. The number of travellers was already growing and so was the clinical work. They were determined to be recognised within the hospital and within the world of medicine in Barcelona and Catalonia as a whole”.
From the start, in spite of being structurally separate, the staff of the Tropical Medicine Section and of the Epidemiology Unit worked together as a team. The purpose of the Epidemiology Unit was to support the different research projects carried out in the hospital and

3736 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
Juan Rodés (on the right, next to Pedro Alonso) has been a driving force behind research in the Hospital Clínic. © Hospital Clínic de Barcelona
The work in Tanzania
Pedro Alonso vaccinates a child during the SPf66 malaria vaccine clinical trial in Tanzania. © Pedro Alonso archive
also to develop its own line of research in the field of international health. “When I started I thought I was going to be here for a couple of years” relates Pedro. Twenty two years later he is still here, with a project on his plate of a magnitude unimaginable back then.
Throughout all these years, “the role of Joan Rodés has been very important”, emphasises Pedro. “It also says a lot about why this hospital is now world class. He leaves you to get on with the job and tries not to ‘micro-manage’. In contrast to the Spanish tradition, he makes room for people to develop. That is an enormous advantage compared to the more traditional scientific bodies in this country”. As history has shown, Joan Rodés’ attitude, also adopted by his successors Raimon Belenes and Josep M. Piqué, has provided es-sential nourishment for the seeds planted in the Tropical Medicine Section and the Epidemiology Unit.
Pedro’s beginnings in his new job at the Hospital Clínic were similar to Manuel Corachan’s many years earlier. “I only had a cubicle”, he remembers. And like Manuel, he did not start from scratch or arrive empty hand-ed. On the contrary, he brought with him a great deal of expe-rience gained from the research
he had done on bed nets in Gambia, a study that had already been published in The Lancet. He also came with the possibility of doing a clinical trial involving a vaccine against malaria.
Indeed, shortly before he accepted the position at the Hospital Clínic, Pedro had been offered the possibility of carrying out an independent evaluation of the malaria vaccine candidate SPf66, a study to be financed by the World Health Organisation. At the pros-pect of such a major opportunity, he did not have to think twice and immediately started looking into possible locations for the study.
“One day I was talking to Manuel Corachan and he mentioned that his team had begun a study on schistosomiasis in São Tomé so we considered the possibility of doing it there”, says Pedro. They travelled to São Tomé together but found that the island did not meet the required conditions for carrying out the vac-cine study. Pedro started looking for an alternative location. He
proposed to Dr Marcel Tanner of the Swiss Tropical Medicine and Public Health Institute the possibility of doing it at the If-akara Research Centre, in Tanzania. Pedro and Marcel had met years before when they studied together on the Public Health in Developing Countries Master’s course at the London School of Hygiene and Tropical Medicine.
Ifakara, a small town in south central Tanzania, was and continues to be a focal point in clinical research, training and healthcare. The town is home to three major institutions: the Ifakara Health Institute, former-ly known as the Ifakara Health Research and Development Centre, the St. Francis Desig-nated Referral Hospital and the Tanzanian Training Centre for International Health.
“I still remember that conversa-tion very well”, says Marcel, cur-rently the director of the Swiss Institute of Tropical Medicine and Public Health. “In those days we didn’t have mobile phones. I re-member I was in a phone booth in the airport talking to Pedro when he said: ‘You are in the Ifakara Centre, would you be interested in doing a study with us on the malaria vaccine?” That marked the beginning of a longstanding relationship between the Hospi-tal Clínic and the Swiss Institute. Apart from a few studies like the
one on schistosomiasis, which had already been started in São Tomé and Mali by the Tropical Medicine Section, it was the first time the Hospital Clínic had ventured abroad to set up such a large-scale re-search project in a country like Tanzania.
“So this led to collaboration on a whole portfolio of work in which we shared our knowledge and expertise and our connections in

3938 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
In Ifakara, from left to right: Pedro Alonso, Camilo Acosta, David Schellenberg, Fidel Font, Rosmarie Hirt, David’s son, Claudia Galindo with her daughter and Beatriz Font Hirt. © Pedro Alonso archive
Africa”, explains Marcel Tanner. “That is how we worked together and the two institutions grew and grew. Our aim was to undertake intervention studies that would have an influence on the health of the population.”
The Hospital Clínic and the Swiss Tropical and Public Health Institute carried out several trials, led by Pedro Alonso, on the malaria vaccine SPf66 developed by the Colombian immunologist Manuel Patarroyo.
“Just three weeks after my arriv-al in Barcelona in 1992”, recalls Pedro Alonso, “I was on my way to Tanzania”. As the initiative in Ifakara began to take shape, the Epidemiology Unit stopped be-ing literally a single unit. Clara Menéndez joined the team in 1994. In the same year, another doctor, Fidel Font, and a nurse Rosmarie Hirt, were the first people to be recruited by the unit to work in Ifakara. Among other tasks they started to prepare the
vaccine trial. Three more doctors soon joined them to work on the trial—Camilo Acosta, Claudia Galindo and David Schellenberg. A year later, two statisticians, Llorenç Quintó and John Aponte, joined the team in Barcelona.
In those days, communication between Barcelona and Ifakara was very different from today, now that we can send an email, Skype someone or call a mobile phone anywhere in the world, however remote, without thinking twice. “We didn’t have email and we had to send faxes”, Pedro explains. “But in Tanzania they didn’t have fax machines at that time and the Hospital Clínic had already got rid of the telex it once used for transplant notifications. So, in order to communicate with Tanzania, I had to go down to the Post Office in the harbour, which was the only place that still had a telex machine, and send the message from there! Later on, we eventually managed to get a telex installed at the Hospital Clínic.”
Although it was only twenty years ago, it seems now like a whole other world. Llorenç Quintó remembers how he used to commu-nicate with Pedro and Clara when they were in Tanzania: “We
would send the message on a certain day of the week, at a cer-tain time when we knew the satellite was in position. We count-ed every word, obviously, because we had to pay for each one”. That was the context in which the first malaria vaccine trial was conducted. The participants were children aged one to five years. The study, which was called KIVAC, lasted two years. “The re-sults were promising and it led to a second trial in infants called INFANVAC”, explains John Aponte, the statistician responsible for analysing the results of those trials. “But the second time, the results led to the conclusion that in that formulation the vaccine was not an effective public health tool for the prevention of malaria.”
“The vaccine trials were the first step towards the many other things we went on to do in Ifakara”, Pedro Alonso says. Before long, other studies were started, such as IRONMAL, a trial led by Clara Menéndez in which Rosmarie Hirt and John Aponte also par-ticipated. “That has turned out to be one of the most important studies we have done in the last twenty years; in fact, it is still cited today”, says Clara. “The IRONMAL study was novel and very important for two reasons”, Pedro explains. “First, it was significant because it highlighted the importance of malaria in infants aged under one year of age at a time when many people thought malaria was not a problem at that age. The other reason is that anaemia is one of the leading causes of death in African children and for years there has been a debate on whether or not it is was safe to administer iron supplementation in malaria- endemic areas. This was the first study to show how many of the cases of anaemia in children under one year old were caused by malaria, how many were due to an iron deficiency, and whether iron supplementation was safe or not in these babies.”
The results, published in The Lancet, showed that it was safe to give prophylactic iron supplements to infants in that age group at the dose established in the study.
These studies helped to consolidate the position of the Epidemi-ology Unit. “We had a very important and growing scientific body of work that had been published in The Lancet and other similar journals, something that very few other departments in Hospi-tal Clínic had achieved at that time”, Clara Menéndez explains. “That was one reason why the work of the Epidemiology Unit was kept going and allowed to expand—because of its scientific output. And that output, in turn, was the magnet that attracted

4140 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
new projects and more funding. The more papers you publish, the more attractive you become. It’s like your photo; it shows what you can do.” As was the case for Pedro, the professional experience Clara had gained during her time in Gambia proved extreme-ly useful when it came to setting up new studies in Tanzania.
IRONMAL was followed by a study on the Intermittent Pre-ventive Treatment of malaria in infants (IPTi), which was also led by Clara Menéndez. The IPTi studied the intermittent ad-ministration of prophylaxis as a method of malaria preven-tion. This study was also very important. The results showed that both malaria and anaemia were reduced in the group of infants who received an antimalarial drug called sufadoxine- pyrimethamine (SP) at the same time routine childhood vacci-nations were administered during the first year of life, and that the prophylactic treatment had no negative effect on the devel-opment of their natural immunity against malaria. It was also significant because distribution costs were reduced considerably by taking advantage of the vaccination programme and, as SP is a low-cost treatment, the cost of the whole intervention was greatly reduced.
Like the vaccine trials, this study has had major repercussions. As will be seen in the following chapters, it was the precursor of several other IPTi studies in Tanzania and other countries, and IPTi has subsequently been approved by the World Health Organisation as a malaria control tool.
The Hospital Clínic staff worked or actively collaborated with the Ifakara Research Centre until the start of the decade of 2000. Although the bulk of this work was research, training and clin-ical care were also key priorities. As can be seen throughout this story, these are the three pillars that provide the foundation of the work carried out in the field of international health, both in Barcelona and elsewhere in places like Ifakara.
As well as providing a wealth of opportunities for research, the work in Ifakara also opened up other possibilities for the Hospital Clínic. One significant outcome was the opportunity to collaborate with the Spanish Agency for International Development Cooperation (AECID) on several development projects financed by the state agency. This collaboration marked the beginning of a long relation-ship between AECID and Hospital Clínic that would later result in much larger joint projects in Mozambique, Morocco and Bolivia.
The activities in Ifakara also provided an opportunity for staff from various different departments in the Hospital Clínic to work together on international health issues as a single team despite belonging to different departments within the hospital. Apart from the staff of the Tropical Medicine Section and the Epide-miology Unit, who travelled frequently to Ifakara or even lived there, professionals from other departments also had the oppor-tunity to travel to Ifakara and to participate in the collaboration, exchange of knowledge and work that took place there.
Doctor Jordi Vila, who is now the head of the Microbiology De-partment in Hospital Clínic, still remembers how he and Joaquim Gascon obtained funds from AECID in the early nineteen nineties to study the aetiology of diarrhoea in children under five at the Ifakara Research Centre. Apart from doing the study itself, he recalls, “we trained professionals and set up a small microbiology laboratory on the site”.
Manuel Corachan and other colleagues also visited Ifakara on several occasions. Among other things, they trained health assis-tants, developed protocols to improve clinical care at the District Referral Hospital, and trained medical staff in the use of ultra-sound equipment and how to interpret thoracic radiographs. This “signified great progress in the diagnostic imaging services at the District Hospital, and it was made possible thanks to Manuel’s contribution”, remembers David Schellenberg, now a professor at the London School of Hygiene and Tropical Medicine.
As David observes, at the heart of the work in Ifakara there was “a critical interaction between the clinical and research skills of Manuel, Pedro and Clara. Their clinical expertise on the one hand, seeing patients, getting a feel for what the main health problems really were in the area, combined on the other hand with their skill in coming up with studies that would address some of the questions and uncertainties that had arisen”.
What was built and achieved in Ifakara was without a doubt a great inspiration for the Hospital Clínic group. One of the biggest gaps in international health has been, and continues to be, the lack of research centres in Africa where the health problems of the continent can be addressed. In contrast to other research cen-tres in Africa, which have remained extensions of the European centres that set them up, the one in Ifakara eventually became an independent entity. Today it is a Tanzanian-registered foundation
4342 FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
FROM BARCELONA TO TANZANIA: RESEARCH TAKES OFF
The large welcome sign at the entrance of the Ifakara Health Institute. © David Davies.
administered by Tanzanians. As Pedro Alonso says: “The expe-rience in Ifakara was key for us; we gave a lot but we also learnt a great deal”. And, as Joaquim Gascon goes on to explain, it helped them to visualise a model that could be replicated elsewhere in the future—a vision that materialised not long after in Mozambique, as described in the next chapter.

The work in Mozambique in the nineteen nineties

47 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
The work in Ifakara was in ef-fect the genesis of what was to come. Inspired by the projects in Ifakara at the height of the expansion of Spanish aid in 1994, AECID decided to sup-port the creation of a research centre in Africa and encouraged the Hospital Clínic staff to take the lead. After several propos-
als had been considered the final decision was to establish a centre in Mozambique. At the time, the Portuguese-speaking country, which was entering a period of reconstruction following an in-tense civil war, was a priority for the Spanish aid agency.
Life for Pedro Alonso, Clara Menéndez and their family already involved a great deal of back and forth between Barcelona and Ifakara. Pedro remembers: “Mozambique was one of the poorest countries in the world; it was far away and we were far away”. And “there were only a few of us!” he emphasises. The Epidemiolo-gy and Biostatistics Unit was still only a few small rooms hidden away in a corner of the Hospital Clínic. To set up a research centre in an African country was no small undertaking. It was a brave step to take, given the unit’s limited resources and the large vol-ume of work already being generated in Tanzania. Manuel Cora-chan and Joaquim Gascon’s priority was to strengthen the clinical work and the travellers’ advice service. Meanwhile “Clara, John Aponte and myself carried all the weight of the scientific work of the Epidemiology Unit”, Pedro says. “We had the vaccine trials in Tanzania, plus the other studies on malaria and anaemia, and at the same time they were suggesting we set up a new structure in another country… Looking back now, it was madness!”
In spite of all this, they decided to take on the task and look into the different options. In 1994, Joaquim Gascon travelled to Mo-zambique with the director of Medicus Mundi to find out more about the country and to look for a location where they could set up a research centre. Accompanied by the Mozambican Ministry of Health, they visited several places in search of a rural area without a large presence of NGOs. Manhiça, a town 80km north of the capital Maputo, was one of the places they visited but as the medical aid organisation Médecins Sans Frontières was already there this option was initially discarded.
The move to Mozambique

4948 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
So they went to check out Montepuez, a rural area north of the country which had great healthcare needs and where there were no NGOs. In the end, the area was also ruled out as a viable site for a research centre because the logistics would have been far too complicated. However, the trip to Montepuez was not in vain as shortly afterwards Medicus Mundi launched a healthcare project (the start of the work AECID is still supporting today in the re-gion) and Manuel Corachan started a study on schistosomiasis.
The following year, Pedro Alonso travelled to Mozambique in a second attempt to find a place suitable for the new research cen-tre. “We were looking for rural areas with a health centre, close to the airport, 150km from Maputo at the most. We needed to make the most of being close to South Africa, where we could obtain supplies”. Among other places, he returned to Manhiça, where by that time Médecins Sans Frontières had closed down its projects. Finally, it was decided that Manhiça was the best choice.
A blend of Portuguese Alentejo architecture and a typical African settlement, Manhiça is a small town located on the main highway, and for many years the only road, connecting the north and south of Mozambique. At that time the country had just emerged from a prolonged period of war that had lasted almost three decades.
Portugal, the poorest of the colonial powers, had done little for the development of its col-onies and a lot to exploit them. In Mozambique the African population was largely exclud-ed from the education system, the administration and busi-ness sector. They faced strong restrictions which prevented
them from getting a job, an education or running a business.7
Following a ten-year struggle for independence, the Mozambican Liberation Front (FRELIMO) took power in 1975. Most of the Portuguese settlers fled in panic to Europe, leaving behind the legacy of a history of exploitation, causing financial disarray and destabilising the few structures that existed.
The political situation in Mozambique
7 Hanlon J. “How the cold war shaped Mozambique today”. Pa-per presented at the conference: Legacies of conflict, decolo-nisation and cold war, London School of Economics IDEAS /IPRI, Lisbon, 28-29 May 2010. 8 Ibidem.
What happened immediately after independence can only be un- derstood within the global geopolitical context of the time. In short, and simplifying a lot, Mozambique became a pawn in the cold war rivalry. For the next sixteen years a war—manipulat-ed and financed by foreign powers—was fought between the FRELIMO government, supported by the soviet bloc, and the op-position Mozambican National Resistance (RENAMO) guerrilla force, set up and supported by Zimbabwe and later South Africa.
The end of the nineteen eighties saw the fall of the Berlin wall, the end of the cold war, and the dismantling of the apartheid regime in South Africa. With these changes, peace finally came to coun-tries like Mozambique, where the estimated number of casualties caused by the civil war is only an approximation of the real figure and is of such magnitude that the reality is hard to comprehend.
A million Mozambicans lost their lives and a third of the popula-tion was displaced. Half of the primary schools and health posts were destroyed or closed down.8 A large number of children lost their childhood when they were forced to become soldiers. And let’s not forget the infamous landmines that were laid up and down the length of the country and which have led to innumera-ble limb amputations, until long after the war ended.
The country’s national infrastructure and social fabric were de-stroyed, and mistrust permeated all areas of personal and public life.
Maputo is a cultural melting pot with over one million inhabitants. The main ethnic groups are Bantu and Portu-guese, but the city is also home to Arab, Chinese and Indian communities. © Hansueli Krapf
5150 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
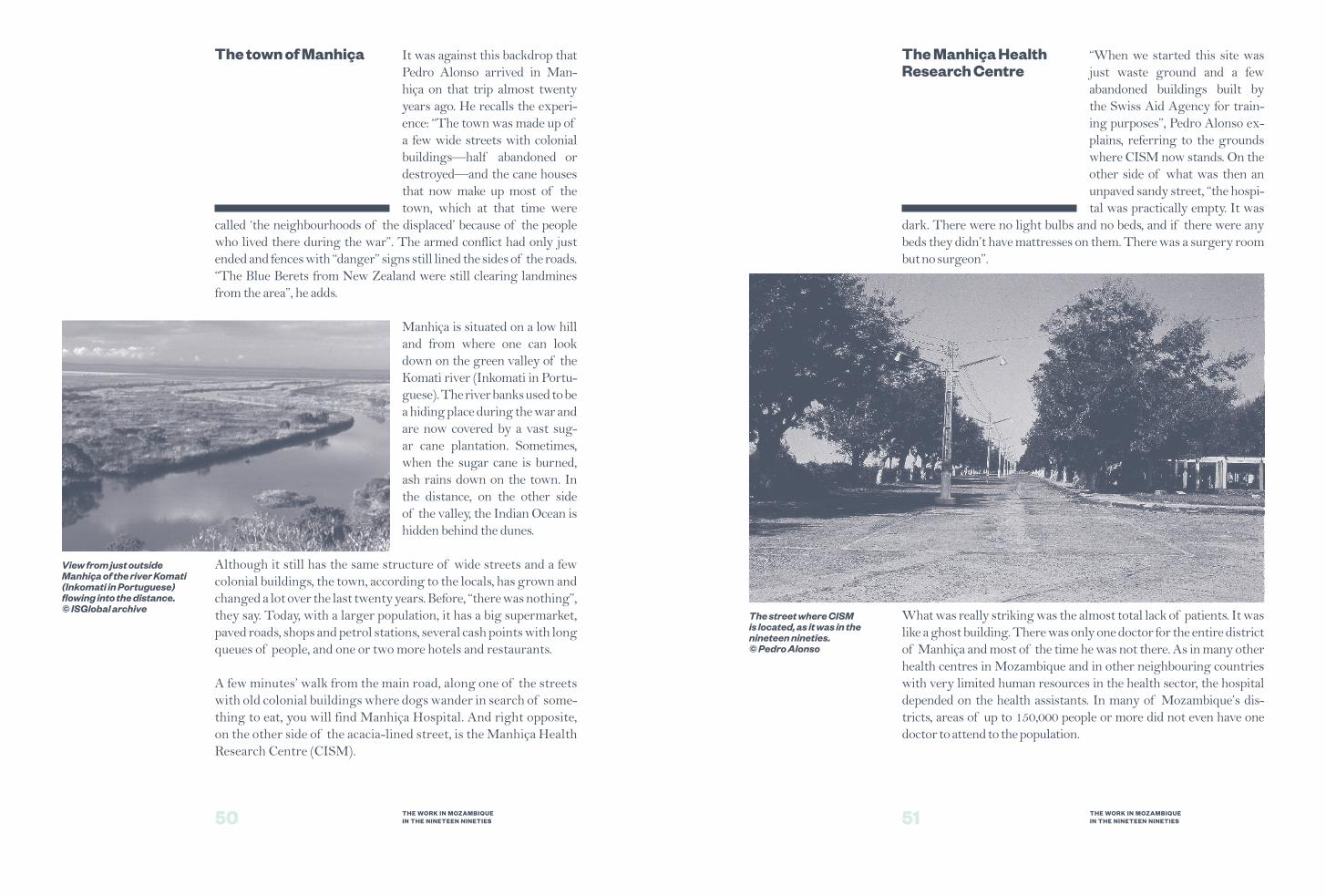
It was against this backdrop that Pedro Alonso arrived in Man-hiça on that trip almost twenty years ago. He recalls the experi-ence: “The town was made up of a few wide streets with colonial buildings—half abandoned or destroyed—and the cane houses that now make up most of the town, which at that time were
called ‘the neighbourhoods of the displaced’ because of the people who lived there during the war”. The armed conflict had only just ended and fences with “danger” signs still lined the sides of the roads. “The Blue Berets from New Zealand were still clearing landmines from the area”, he adds.
Manhiça is situated on a low hill and from where one can look down on the green valley of the Komati river (Inkomati in Portu-guese). The river banks used to be a hiding place during the war and are now covered by a vast sug-ar cane plantation. Sometimes, when the sugar cane is burned, ash rains down on the town. In the distance, on the other side of the valley, the Indian Ocean is hidden behind the dunes.
Although it still has the same structure of wide streets and a few colonial buildings, the town, according to the locals, has grown and changed a lot over the last twenty years. Before, “there was nothing”, they say. Today, with a larger population, it has a big supermarket, paved roads, shops and petrol stations, several cash points with long queues of people, and one or two more hotels and restaurants.
A few minutes’ walk from the main road, along one of the streets with old colonial buildings where dogs wander in search of some-thing to eat, you will find Manhiça Hospital. And right opposite, on the other side of the acacia-lined street, is the Manhiça Health Research Centre (CISM).
View from just outside Manhiça of the river Komati (Inkomati in Portuguese) flowing into the distance. © ISGlobal archive
The town of Manhiça
The street where CISM is located, as it was in the nineteen nineties. © Pedro Alonso
“When we started this site was just waste ground and a few abandoned buildings built by the Swiss Aid Agency for train-ing purposes”, Pedro Alonso ex-plains, referring to the grounds where CISM now stands. On the other side of what was then an unpaved sandy street, “the hospi-tal was practically empty. It was
dark. There were no light bulbs and no beds, and if there were any beds they didn’t have mattresses on them. There was a surgery room but no surgeon”.
What was really striking was the almost total lack of patients. It was like a ghost building. There was only one doctor for the entire district of Manhiça and most of the time he was not there. As in many other health centres in Mozambique and in other neighbouring countries with very limited human resources in the health sector, the hospital depended on the health assistants. In many of Mozambique’s dis-tricts, areas of up to 150,000 people or more did not even have one doctor to attend to the population.
The Manhiça Health Research Centre

5352 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
CISM’s laboratories are equipped with the latest technology. © Andalu Vila-San-Juan
“At the beginning, in 1995, the district authorities gave us a small house to live in and offered us a room in the hospital’s administra-tion building. We set up a couple of computers and we were there for the first two years, before we started building what has become CISM”, Pedro Alonso says.
Apart from two signs, little else outside the white walls of CISM provides any hint of what goes on inside. Nobody would guess that what lies behind the front gate is one of the most prestig-ious research centres in Africa. It is hard to believe without see-ing it, but entering CISM is like walking into another world. This impression is not so much due to the design or size of the centre—indeed the garden, the payotas (huts) and the low red and white buildings do not look out of place—but to the work that is done there, to what is concentrated in that relatively small space: world class technology and the experts with the skills needed to make use of it.
Walking into CISM is like going into a universe of microscopes, glass slides, fridges, freezers, demographic and data collection centres, offices, a room for researchers, a payota that houses the canteen, and another that functions as an open air meeting room, as well as several rooms for visitors. The interior of CISM is truly impressive: a striking contrast with the outside world of reddish muddy streets and the statistics that persistently classify Mozam-bique as one of the poorest countries in the world.
Through the lab windows one can watch the technicians in white overalls working away using the latest technology. Their work may involve studying cultures and analysing blood samples to un-derstand who is protected against malaria and who is not, describ-
ing cellular response to HIV, or analysing the serotype of the pneumococcus bacteria that causes pneumonia, to mention just some of the daily activities. This is the place where, over the last thirteen years, doctors and scientists have carried out several malaria vaccine trials that have had massive scientific repercussions on a global scale. This is the centre where it was discovered that chloroquine,
formerly used in Mozambique as a first-line treatment against malaria, was not effective. To-day children are vaccinated against pneumococcus thanks to the results of studies under-taken at CISM. Here, only a few steps from where the tarmac turns into mud and children run around barefoot, extraordi-nary things have been achieved that could not have been fore-seen twenty years ago by the government in Maputo or, many miles further away, by the Hospital Clínic in Barcelona.
The journey travelled from then until now has been one
of steady progress punctuated by huge leaps forward. The aim, which was always clear and always the same since the beginning, was to establish a research centre that would contribute to finding solutions to the main diseases affecting the population. Initially, the focus was on carrying out descriptive epidemiological studies and later it shifted to the development of new tools for the preven-tion, diagnosis and treatment of these diseases.
Pedro Alonso explains: “We didn’t want to be ‘parachute’ re-searchers like many European and American teams, who swoop into a hospital, take samples and go back to the USA or Europe to analyse them. Even though it may be much more expensive to do the work in Manhiça, where keeping the equipment up-to-date and certifying it costs around $100,000 a year … we believe that it is crucial to do the research on the ground. To literally be able to go across the street from where the problem is and use the most advanced technology to try to understand that problem better”. Malaria, the main cause of illness in Mozambique, has been the flagship of CISM until now. Tuberculosis, HIV/AIDS, respiratory infections and diarrhoeal diseases are also very com-mon in Mozambique and have also been priority research topics for the centre.
“And in the vision we have of a research centre”, Pedro contin-ues, “one of our commitments to the community is to provide
On average, CISM has some twenty five studies ongoing at any given time. © Olivia Blanchard

5554 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
medical care. You can’t do research without providing health-care and you can’t provide healthcare without strengthening the human resources. That was something we were very clear about from the start, that training and medical care were in-separable from research”.
Supporting the Manhiça Hospi-tal was, therefore, one of the pri-orities from the start. Together with two other people, Montse Soriano was the first doctor re-cruited from Barcelona to work in Manhiça in 1996. She started working in the hospital along-side two Mozambican doctors. Now living in Berlin, she reflects
back on those years: “I remember my first day very well. The outpa-tient building was empty. There were only a few patients, who had tuberculosis and from their appearance probably HIV/AIDS as well. They were dying. The children’s ward was very small and there were only a few children. There was hardly any staff and we recruited sev-eral nurses. In Mozambique, a small hospital like that was lucky to have even one nurse.”
There were several reasons why people were not going to the hos-pital and that there was no need was definitely not one of them. It was common for people to go to the local healers, or to Maputo. Some sought no medical attention at all until it became an emer-
gency. When patients did even-tually make it as far as the hos-pital they would often find that there was no staff and no drugs or resources, which generated an even greater mistrust in the health system.
“There was still a lot of mistrust in the community”, Montse re-calls. “It wasn’t long since the war had finished and there were still landmines in Manhiça. Peo-ple who had fled to Maputo were returning home. Sometimes we
Montse Soriano walking towards straw-bale houses in 1997. Although these houses made of straw-bale and cane are still found in Manhiça, the town “has changed a lot”, say the locals. © Montse Soriano archive
Healthcare in the Manhiça Hospital
would receive people in the hospital who had suffered severe assaults. One day, a man came in who had been hit on the head with a machete. His wounds were all open and exposed. There was a lot of violence: if someone stole something from the neighbour, they would go and beat him up. One time when I was on call and an injured man came in, an old nurse from the hospital told me: ‘Doctor, don’t forget that not that long ago we were killing one another. We have committed atroci-ties, and that is still inside us’.”
Gradually, more and more patients started to come to the hospital. In a relatively short period, it went from being a ghost hospital to one where the staff would see an average of 125 children a day.
Magdalena Ripinga is one of those people who is not easy to forget, and she has really become an institution in the hospital. She is one of the veteran healthcare assistants and one of the first people to be employed by CISM: she has been there seventeen years. Nowadays she works at the children’s Short Stay Ward where patients are sta-bilised and triaged and either get admitted or return home. When asked about the most common diseases she sees, Magdalena ex-plains: “It depends on the time of year. In the summer, there is a lot
The healthcare assistant Magdalena Ripinga examines a child with malaria at the Short Stay Ward, in Manhiça Hospital. © Olivia Blanchard

5756 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
of diarrhoea, gastroenteritis and malaria. Those are less common in the winter, when we see more respiratory infections and pneumonia”.
“The hospital has changed a lot. When I arrived in 1997, there was only a first aid post and a few small buildings. Adults and chil-dren were seen in the same place”, she relates while getting ready to examine a fifteen-month-old baby who has diarrhoea as a result of malaria. He was treated at another centre but is not improving. “We are going to admit this child into hospital because he lives very far away and could get worse during the trip”, she explains after examining him. “Here, child mortality has gone down a lot. People like this mum are now much better informed about differ-ent diseases and prevention, and they come sooner.”
A paediatrics ward, more rooms for patients, consulting rooms, toilets, a surgical block, a maternity ward are just some of the new structures that over time have been built or rehabilitated thanks to AECID funding administered through CISM and Euro-pean Union funds administered by the Mozambican Minis-try of Health. “When you provide quality care, people make use of the services”, says Pedro Alonso. Today the new build-ing housing the consulting rooms is heaving with people waiting to be seen, something unheard of in those bygone days.
Manhiça Hospital has grown a great deal over the last twenty years. © Olivia Blanchard
As well as getting the Manhiça Hospital up and running, the other priority in 1996 was to do a population census. In Africa, people are often born and they die without ever having existed on any register. “Today they take a census and then they might do it again in ten years’ time. But if you are born after one census and
die before the next, you are never registered. What greater indignity could there be”, exclaims Pedro, “than never to have existed on this earth at all?”
“In the case of Mozambique”, explains Ariel Nhacolo, a demog-rapher at CISM, “during the civil war we didn’t do a census in seventeen years, and before independence, only white Europeans were registered.”
“But if you want to do research and monitor the population in a thorough way, having a census is very important”, Pedro contin-ues. “We did it in three steps. First we defined a geographical area of study. Second, we conducted a census, that is, we registered every case of migration, birth and death within the study area; this is what we call our demographic platform. Third, we registered the cases of disease in this population; this we call the morbidity surveillance platform. The combination of these three elements, a defined geographical area, a population census and disease sur-veillance is a very powerful tool in research. Ours was the first population census of this type to be done ever in Mozambique.”
From the start, CISM teams worked with community leaders to map out the neighbourhoods within the study area. A large num-
ber of people were employed to go out into the community and number the front doors of each house, one by one, and reg-ister all the people living there. “The study area has grown over time”, Pedro explains. “At the beginning, what we now call the ‘old study zone’ included 35,000 people living in an area of 500 km². Not long ago, the
A data centre was one of the first buildings to be renovated in CISM. © Llorenç Quintó archive
The demographic, geographic and morbidity platforms

5958 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
study population was up to 94,000 people and soon the whole dis-trict will be covered and will include 150,000 people.”
Nowadays, when a study requires children from a certain age group and a specific part of the district, researchers can find out who lives where and how old they are practically at the touch of a button. But none of this would be possible without the work of a huge team of people who keep the database up-to-date. These are the staff who go out to number each house, the interviewers who collect the demo-graphic information and the supervisors.
In addition, every week the community leaders keep the demog-raphers informed about any births, deaths, pregnancies or migra-tions that may have happened between the visits of CISM staff to the community. And, clinical data is collected daily from the six health centres in the study area (including Manhiça Hospi-tal). Charfudin Sacoor, Head of the Demography Department at CISM explains: “By the end of the day, in each of the health cen-tres we know how many children were sick, their diagnosis and the result: whether they were admitted, referred to Maputo or re-
turned home. At the end of the month we see the distribution of diseases in Manhiça, infor-mation we later use to plan our research programmes”. For ex-ample, it is possible to see which areas have the highest number of malaria cases and identi-fy the focal points for certain infections. Likewise, since all pregnancies are registered, it
is possible to monitor neonatal mortality in the area, something practically unimaginable anywhere else in the continent.
It is hard to convey how important it is for the entire research programme at CISM to have access to all this continuously up-dated demographic and clinical data. Charfudin describes the Demography Department as “the red carpet of the biggest cat-walks, the one all the research projects have to walk along”.
Every day, Albino Chilaule and other members of CISM’s demographic team go out into the community to update the census information. © Olivia Blanchard
In 1997, this room became the centre’s first laboratory. © Archive Llorenç Quintó.
After the first year of work, in 1997 the time came to start building the research centre it-self including the first labora-tory. The whole structure had to be built from scratch, new staff had to be recruited and trained, and new lab materials had to be bought.
“For quite a while we considered building some small labs in the grounds of the hospital”, ex-plains Pedro Alonso. “But then someone from the Ministry of Health reminded us about the abandoned buildings on the oth-er side of the street”. After the paperwork was sorted out, work started on the buildings. Two rooms were turned into an office
and a data centre, and what would have been a classroom became CISM’s first mini-lab.
“When we first started working in Manhiça”, says the statistician Llorenç Quintó, “getting hold of materials was not as easy as it is now that we have a purchasing department. Before, we had to buy everything in Barcelona. We had to go to the store room at the Hos-pital Clínic and ask whether they had any boxes of this or that size.
We used to ask them to please keep them for us. Then we would put them together, weigh them, measure them, fill them, make up the parcels and send them. All this was done by the statistician or the secretary alike, by the few of us who were based in Barcelona.” By the time Her Majesty Queen Sofia of Spain went to official-ly inaugurate the CISM, there was already a laboratory, a new pavilion, a researcher’s room, a library and a data collection
The construction of the first laboratories at CISM
Over the years, CISM has grown to meet the needs of the research programme. © ISGlobal archive

6160 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
Capacity building and training of staff
Her Majesty Queen Sofía of Spain (in the centre of the photo, next to Montse Soriano) officially inau-gurated the CISM in 1998. © Montse Soriano archive
Lab technician Crisóstomo Messías (on the left) discusses a new study with Hélder Bulo, the laboratory manager at CISM. © Olivia Blanchard
centre. Since then, new labora-tories have been built and out-fitted with new equipment and instruments to meet the needs of the research programme. Existing buildings were used when possible and new ones built when necessary. “As the centre became too small, we extended it. So it has often been like a construction site!” Pedro Alonso says.
A laboratory or hospital can have the best technology in the world, but if there is no one competent to use it, it will be a useless space. So from the most basic training of a new microscopist to the PhD thesis of a doctoral candidate, one of the foundations of the CISM’s work is training and educating technicians and researchers.
The Training Fellowship Programme has been running since the centre opened. The core aims of the programme are capac-ity building and strengthening and it tries to counteract the nega-tive effects of the migration phenomenon known as brain drain. Researchers start out working on CISM projects and can enter a scholarship programme to study at master and doctorate lev-els. Many of them spend time working in the labs in Barcelona, and they always focus on the health issues that are a priority for Mozambique. At the end of the programme, they return to their country to work in the health system or at the University of Mo-zambique. The Hospital Clínic and the University of Barcelona are two major academic partners of Mozambique; in fact many Mozambican researchers have trained in Barcelona and most of their doctorates have been awarded by the university there.
The statistician Llorenç Quintó explains the concept: “we could have just gone there to do a study and once it was finished and published that would have been the end of the story. But in our
vision of aid, development through training is very important. It goes beyond the limits of research”.
Moreover, it must be said that the exchange of knowledge and training has not been a one-way street. “When we talk about the people trained in Manhiça, we often make the mistake of only counting the Mozambicans”, says the director of CISM, Eusébio Macete. But in fact, the training programmes have benefited pro-fessionals from Barcelona and other parts of the world as well as those from Mozambique. “The training of Spanish doctors who do part of their residency or doctorate in Manhiça, and the pres-ence of statisticians who do the analysis of their research over there, has been continuous”, says Llorenç.
To sum up, the foundations of CISM were laid during the sec-ond half of the nineteen nineties. The efforts were focussed on

6362 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
From Sub-Saharan Africa to the Maghreb: the project in Morocco
The maternity ward of the Spanish Hospital of Tetouan became a centre of excellence and a new ambulance service was created. © Susana Oñoro
9 UNDP, Human development report 2011.
the population census and setting up the demographic and mor-bidity surveillance systems, as well as on the construction of the first laboratories. Strong links were forged with the com-munity and the first epidemiological studies were undertaken. The renovation of the hospital, the medical care of patients and the recruitment and training of staff were also essential activi-ties. The training of researchers through master’s and doctor-ate programmes began at that time. From the start, the three essentials—healthcare, training and research—have constituted the backbone of the work.
While all this was happening in Manhiça and the studies and oth-er activities continued in Ifakara, the clinical work in Barcelona also evolved. The number of patients arriving at the Tropical Medicine Section continued to grow and the travellers’ advice service was consolidated.
At the end of the nineteen nineties, Manuel Corachan was elect-ed President of the European Association of Tropical Medicine Schools, an organisation to which the Hospital Clínic had be-longed since the nineteen eighties. In 1998, the same year Her Majesty Queen Sofia of Spain travelled to Mozambique to offi-cially inaugurate the CISM, the Spanish Society of Tropical Med-icine and International Health (SEMTSI) was founded in Spain. The new association was promoted by the Hospital Clínic and Manuel Corachan was the first president.
As if all of the above were not enough, at the turn of the cen-tury something else happened that later came to represent a new milestone in the relation-ship between Hospital Clínic and AECID. The setting was Morocco, where the Hospital Clínic took on the responsibili-ty for renovating the Materni-
ty Department of the Spanish Hospital in Tetouan, a project un-dertaken within the framework of existing bilateral cooperation agreements between the two countries.
The border between Morocco and Spain (and therefore between Africa and Europe) marks the world’s greatest disparity in human development between two countries: the twelve kilometres of the Strait of Gibraltar symbolises the huge gaps that exist in income, health and education, as well as the global inequities.9
The area of maternal, child and reproductive health in Morocco faces two main chal-lenges: to improve the quality of medical care and to reduce inequalities in access to repro-ductive health services. These inequalities are the result of marked socio-economic differ-ences and the disparity between urban and rural environments in Morocco. Neonatal mortality, which accounts for 66% of in-fant mortality, is mainly caused by inadequate care during the birth or postnatal period.
With the Maternity Without Risk programme, between 1999 and 2011, the Maternity Department of the Spanish Hospital of Te-touan became an outstanding maternal and neonatal health centre, where 20,000 babies were delivered, 15,000 prenatal consultations took place and innovative practices were introduced. In addition, maternity waiting homes were built or renovated and an ambu-lance service for obstetric and neonatal emergencies was set up.

6564 THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
THE WORK IN MOZAMBIQUE IN THE NINETEEN NINETIES
Thousands of Moroccan women have received pre-natal care through the Maternity Without Risk programme. © Susana Oñoro
This national programme has contributed to a marked reduction in the maternal mortality rate in Morocco, which went from 300 per 100,000 live births in 1990 to 100 per 100,000 live births in 2010.
As well as the medical activities, and as part of the support offered to the Provincial Health Delegation of Tetouan, several studies have been carried out to investigate the causes of maternal and child mortality, the coverage of an extended immunisation pro-gramme, and barriers of access to maternal health services.
The project in Morocco continued into the first decade of the 21st century. And since 2009, it also included biomedical research in areas that are important for the national health system. Despite the progress made in child health care, acute respiratory infec-tions and diarrhoeas continue to be among the main causes of child mortality in children aged under five years. In this context, as in others, scientific evidence is crucial for the strengthening of national health policies and programmes.
Consequently, the Hospital Clínic—together with the Moroccan Ministry of Health and Ibn Sina University Hospital in Rabat—set up a biomedical research laboratory, the first one to be created within the Moroccan hospital system. This laboratory “is specifi-cally for research and supports the studies undertaken jointly by the Moroccan and Hospital Clínic teams”, explains Enric Grau,
who was in charge of the project in Morocco from 2002 to 2012. In recent years, teams of researchers from Rabat and Barcelona have studied a number of topics, including diarrhoeal diseases and acute respiratory diseases in children under five, the epidemi-ology and aetiology of meningitis in under fifteen year olds, and the epidemiology of mother-to-child transmission of infections and the risk factors involved.
Education and training has also been an essential component of the bilateral cooperation agreements. The aim of this work is to build local capacities and structures in both clinical and re-search settings. Working together with the national institute of health administration, which is part of the Moroccan Ministry of Health, a diploma course in epidemiology and biostatistics was launched. In collaboration with the University of Fez and the Lalla Salma Foundation, the country’s first e-learning plat-form was developed to provide training on the early detection of cervical cancer. Recently, thanks to a collaboration with the Mo-hamed V – Souissi University, two new diploma courses have been launched: one in neonatal resuscitation and the other in obstetric and neonatal emergency care.
Finally, inspired by the model first pioneered in the CISM, a Research Fellowships programme has been implemented in Morocco to offer young researchers an opportunity to devel-op their skills and further their professional careers by entering Master’s or Doctorate programmes at European and Moroccan universities. Once again, the backbone of the work is built on the convergence of medical care, training and research.
None of this would have been possible without the dedication of numerous researchers and professionals from the health sector among others, mainly from Spain and Morocco. Nor could it have been achieved without the support of AECID and the “la Caixa” Foundation.
As we shall see in the next chapter, the activities in Mozambique and Barcelona continued into the decade of 2000. Research took off de-finitively. One could say that the nineteen nineties were the start-er for the main course that was yet to come. The new millennium brought with it a very important chapter in this thirty-year story.

The research boom in CISM and the creation of CRESIB

69 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
The start of the 21st centu-ry saw an explosive increase in activity, with research on international health issues in-creasing exponentially within a brief period. Several factors stimulated this growth. The most important was the rap-id expansion of the research programme in the CISM, Mo-
zambique, with the simultaneous launch of two major studies: a trial of the GlaxoSmithKline (GSK) malaria vaccine and a new Intermittent Preventive Treatment of malaria in infants (IPTi) study. The impact of these two studies was felt not only in CISM - which had to expand its staff from 60 to 250 employees -, but also thousands of miles away in Barcelona, where the Hospital Clínic increased considerably the resources and staff allocated to international health research.
This change of pace was not an isolated phenomenon; the glob-al context favoured the growth of research activity at that time. The Millennium Development Goals—established at the turn of the century—set ambitious targets in areas in which the Trop-ical Medicine Section was already working: malaria and child and maternal health. The creation of the Bill and Melinda Gates Foundation and other philanthropic bodies also helped to firmly establish the priorities of international health on the global po-litical agenda and to underscore the value of innovation and re-search as development tools.
Undoubtedly, the most impor-tant studies in CISM’s histo-ry to date have been the RTS,S vaccine trials led by Pedro Alonso. The story began in 2000 when the Bill and Melin-da Gates Foundation decided to fund the development of the pharmaceutical GSK’s vac-cine and chose the CISM as
a location for phase II studies in children aged between one and five years. In 2001, a pilot study tested the vaccine in 60 children. This was followed by MAL 026, a larger study involving 2,000
A new step in international health
The malaria vaccine trials that made history

7170 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
children. To cover the needs of this work CISM had to recruit new staff, strengthen the De-mography Department and the fieldwork team, and update and improve the microbiology and parasitology laboratories.
Quique Bassat, a paediatrician whose early vocation for trop-ical medicine had brought him to Manhiça during his medical
training, went to CISM in 2003 to help document adverse events and safety issues during the MAL 026 trial. Today, once again living in Manhiça, he looks back on that earlier time: “It took us a month to vaccinate all the children in the study, and then we had to give them another dose a month later, and another one a month after that. Those were the most intense months of my professional life, working with the vaccination team from seven in the morning to eleven at night. It was a massive study. I have never seen such a complex intervention done with the means we had at the time. It was the first large trial of the vaccine and it opened the doors to
the many studies that followed.”
The preliminary results of the vaccine trials had major reper-cussions in the international media. They were front page news in the most important newspapers around the world and the results were published in the The Lancet in 2004. The findings demonstrated that the GSK vaccine had a protection rate against malaria of 30%, and therefore achieved the min-imum efficacy level for a vaccine to be considered useful in the context of public health. This scientific milestone was crucial to the consolidation of the pro-jects in Barcelona and Manhiça. The centre has worked contin-uously for over fourteen years
The first trials of the RTS,S malaria vaccine, produced by the pharmaceutical company GSK, started in Manhiça in 2001. © Bill and Melinda Gates Foundation
The initial results of the vaccine trials appeared in the Vintage Papers from The Lancet , a collection of landmark papers published in the journal. © Pedro Alonso archive
on studies that have been central to the clinical development of this vaccine candidate. Examples include studies on immunity in newborn babies and infants and the first phase III trial, the results of which may open the door to the regulatory approval of what would be the first generation of malaria vaccines in history.
The initial results of the RTS,S vaccine trials made the front page of the New York Times. © Pedro Alonso archive

7372 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
Intermittent preventive treatment for malaria in infants
The other large study which began at almost the same time as the vaccine trials, was the IPTi study led by Clara Menén-dez. Following the success of the IPTi study in Tanzania de-scribed in the second chapter, the BBVA Foundation and the Gates Foundation funded the creation of the IPTi Consortium, to be
coordinated from Barcelona, and a new IPTi study, to be carried out in several research centres including CISM.
The malaria vaccine clinical trials and the IPTi study were the first intervention studies carried out by CISM. Gonzalo Vicente, who went to Manhiça in 2002 to manage the centre, faced the chal-lenge of overseeing the start of these two major studies. “The challenge was to scale up the resources and operations of the centre fourfold, a difficult task because of the logistical difficulties involved in recruiting staff, building and maintaining laboratories and installa-tions, and everything else in a rural area in Africa.”
The intermittent treatment study also had a considerable impact and led to the approval by the World Health Organisation of IPTi as a tool in the fight against malaria. It also further strengthened the capacity of CISM and the Hospital Clínic with the construc-tion of immunology laboratories in both places.
Carlota Dobaño, a pharmacologist with a PhD in immunology, started working in the Epidemiology and Biostatistics Unit of Hospital Clínic in 2002. She was responsible for the immunologic aspects of the IPTi study and oversaw the construction of the new laboratories. Today, she remembers how, during the first two years, she was more of an architect and a logistician than a re-searcher. At that time, CISM only had parasitology and microbi-ology laboratories. The funds allocated to the IPTi study made it possible to build an immunology laboratory and the equipment needed to study molecular biology. This new infrastructure al-lowed the researchers to do more sophisticated analyses, such as investigating how a parasite grows and whether or not it was af-fected by a specific treatment.
Inácio Mandomando (at that time the laboratory manager) and Carlota Dobaño getting ready to show CISM’s new immuno-logy lab to Bill and Melinda Gates in 2003. © ISGlobal archive
The statistician John Aponte (on the left) has worked with Clara Menéndez and Pedro Alonso for almost twenty years. He was one of the first people to be recruited by the Epidemiology Unit at the Hospital Clínic. © ISGlobal archive
7574 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
Changes in the Hospital Clínic
With an immunology laboratory it was also possible to study the presence or absence of antibodies in the samples obtained, that is, to ascertain whether there was an immune response. This marked an important turning point, allowing the researchers to take one step further and study the mechanisms underlying the vaccine’s activity as well as the effect of the drug on the immune system. “The IPTi study led to all the other studies on immunology and molecular bi-ology that have been done since then” says Carlota Dobaño. She still remembers the epic journey involved in taking a flow cytometer, an essential tool in the analysis of cellular immunology: “Over there it’s not the same as being in Barcelona; when you have a problem there’s no technician sitting next to you who can deal with it, you have to go to South Africa”.
At that time, the Epidemiology Unit at Hospital Clínic, headed by Pedro Alonso, was still housed in four rooms at the end of a cor-ridor in the outpatient depart-ment and had no laboratories of its own. On the rare occasions the team needed to do research in Barcelona, they had to turn to other departments for help, as
the researcher Alfredo Mayor did when, during his doctorate years, he borrowed a workbench from the microbiology laboratory.
The RTS,S vaccine trials and the IPTi study in Manhiça changed all of this. At the same time as the new immunology laboratory was be-ing added to CISM, Carlota Dobaño explains how “in Barcelona, we started looking for a place where we could at least put a small lab, be-cause we were soon going to be sending samples from the study [in Manhiça] to Barcelona and we needed to start doing research here. In the end, we were given a room that soon became our first labora-tory at the Hospital Clínic. Laura Puyol and Elisa Serra were the first two people I recruited to work there.”
In the world of scientific research, studies are like a business card. If they are done well and result in papers getting published in high level journals, with a bit of luck they will attract new projects and more funds, and so on and so forth.
“Manhiça nourished Barcelona and vice-versa”, Alfredo Mayor ex-plains. “It was a total synergy. The work done at CISM made the team here grow and as a result we were able to take on more complex studies involving molecular biology, immunology, and things like that. And at the same time, the research we were doing here in Hospi-tal Clínic was helping CISM to grow too.”
As the number of studies grew, the needs of the Epidemiology Unit once again outstripped the space available in the Hospital Clínic and what used to be called Area Six (international health) at the IDIBAPS. More staff were recruited. As Carlota Dobaño explains: “We managed to get another tiny room for culturing cells and par-asites. And not long after, they gave us a slightly larger space. We started getting a foot in the door here and there. Then we moved to a bigger room, although it was still only a single space where we had to do everything. And by that time we were researching malaria, HIV, enteropathogens, respiratory diseases… ”.
However, it was not only the laboratories that had become too small, the administrative systems had also become inadequate. Although the overall number of people at the hospital working on interna-tional health issues was relatively small, the volume of funding of these projects represented a disproportionately high percentage of the Clínic Foundation’s funds. With projects underway in Tanzania, Morocco and Mozambique, there came a time when the foundation’s administrative structures were no longer suitable.
“The financial, logistical and organisational needs of these projects were so different, that the structure was no longer appropriate. It had not been designed for this kind of research”, explains Enric Grau. The Clínic Foundation was set up to manage the national funds for biomedical research within the framework of a teaching hospital like Hospital Clínic. But these other activities, involving multiple donors, funds in different currencies, international travel, and expatriate staff, presented a very different scenario.
As a result, in 2002, a new structure was created within the Clínic Foundation called the International Cooperation Office (OCI), which was set up to administer the financial aspects of the hospital’s aid and development projects.

7776 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
At the same time as the OCI was created in Barcelona and in response to the need to en-sure the long term sustaina-bility of CISM, the idea of the Manhiça Foundation was born in 2002. Drawing up the con-ceptual framework for the new foundation was one of Gonzalo Vicente’s responsibilities. He
describes the task as “a real challenge”, at a time when there were very few foundations in Mozambique. Since CISM had been set up in 1996, the idea had always been to create an independent founda-tion with its own legal personality, and for the Centre to be man-aged by Mozambicans.
It took several more years’ of planning before the Manhiça Foundation was created in 2008, with the Hospital Clínic as one of its board of trustees. In the same year, the Prince of Asturias Foundation awarded CISM its International Aid and Development Prize in recogni-tion of the centre’s work in bi-omedical research, healthcare and training.
“Having a centre like CISM is a great advantage for Mozam-bique”, Eusebio Macete explains. “Its modus operandi differs a great deal from the classical models of aid and development. Precisely, one of the main chal-lenges throughout these years has been to get politicians to see research and the generation of
knowledge as a new form of international cooperation. Another challenge has been the process that has taken CISM from being an aid and development project to becoming an independent Mo-zambican institution responsible for its own decisions and man-agement. The process took several years. And the third major
The creation of the Manhiça Foundation
The Tropical Medicine and International Health Department
challenge has been to generate a critical mass in terms of human resources. Science is not made up of machines. It’s the minds that count, the human capacity. Building that up requires time, invest-ment and long term commitment. In that respect, we have got to where we are thanks to the steady purpose and commitment of AECID, the University of Barcelona and the Hospital Clínic”.
In Barcelona, important struc-tural changes were also taking place in the Hospital Clínic. In 2001, the Tropical Medicine Section split from the Infectious Diseases Department and, to-gether with the Epidemiology Unit, was merged into the Eval-uation, Support and Prevention Unit (UASP). A few years later,
in 2006, the Tropical Medicine Section and the Epidemiology Unit separated from the UASP and merged to become the new Tropical Medicine and International Health Department.
The creation of this new department, a significant milestone in this thirty-year journey, was principally the work of Antoni Trilla, the doctor who headed up the UASP, Manuel Corachan and Pedro Alonso. It was the first department of its kind in a Span-ish hospital and represented a positive step towards consolidat-ing the international health research and healthcare within the Hospital Clínic. Pedro became the head of the department and Joaquim Gascon took over the Tropical Medicine Section (Ma-nuel had retired in 2004).
At around the same time, and also motivated by the desire to bring this type of work to the forefront in the academic world, the Uni-versity of Barcelona made Pedro Alonso a professor in the Facul-ty of Medicine at the University of Barcelona.
Eusébio Macete, current director of CISM, was once a PhD student on the Training Fellowship Programme. © ISGlobal archive

7978 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
As the volume of research at CISM continued to grow and the Manhiça Foundation and the Tropical Medicine and In-ternational Health Department began to take shape, another im-portant event in this story was brought about by the Catalan Government’s decision to pri-oritise research in internation-
al health. In 2006, the Barcelona Centre for International Health Research (CRESIB) was created as part of the government’s CERCA programme (a network of research institutions special-ised in different areas). The new centre was set up as an independ-ent legal entity and the Hospital Clínic, the University of Barcelo-na and the relevant government ministries were represented on its board of trustees. From this point onwards, CRESIB took over re-sponsibility for all the research that had previously been done with-in the framework of IDIBAPS - Clínic Foundation.
The creation of CRESIB, an entity born of political will and a historic opportunity at a unique point in time, marked a turning point in these thirty years. The new institution gave fresh impe-tus and greater visibility to international health research in Bar-celona. It was the only research centre of its kind in Spain and southern Europe, and it became the precursor of the Barcelona Institute for Global Health set up in 2010.
“Research improves the quality of healthcare and attracts fund-ing”, states Dr Marina Geli, who was the Catalan Minister of Health during the presidency of Pasqual Maragall and later José Montilla and the person mainly responsible for the creation of CRESIB. The Catalan Government’s commitment to interna-tional health research took place in a context in which the world, and diseases, were becoming increasingly globalised. The threat of an avian flu pandemic underscored the need for health systems to generate knowledge and be prepared to deal with diseases pre-viously unknown within the country’s borders or to respond to the re-emergence of diseases that had been eradicated years before.
It was a period of significant demographic and social changes in Spain, all of which had an impact on the health system. Starting in1998, immigration flows increased dramatically. In Catalonia alone, the population rose by one million between 1998 and 2008.
The creation of CRESIB
“Our world changed”, Marina Geli says. “We didn’t have enough paediatricians. We had to recruit interpreters and mediators. We had to deal with a huge increase in demand, especially for paedi-atric care. And we had to train professionals, not only to diagnose previously unknown diseases, but also to deal with cultural issues and language problems.”
The Catalan Government drafted and implemented an Action Plan for Immigration to deal with the impact of new arrivals on the health system, and an Action Plan on Research, which responded to the need to rethink how research was done within the health sys-tem. Both plans were instrumental in the creation of CRESIB.
Dr Núria Casamitjana is a teacher at the University of Barcelo-na. During the last decade, she has been one of the foremost ad-vocates for the need for training and research in international health. She has worked on these issues both as vice chancellor of the University of Barcelona and later as the technical director of CRESIB from 2006 to 2011. CRESIB “made it possible for us to bring it all under one roof, to be more coherent; it was like tidy-ing up the house”, she explains. The new institution helped us to achieve greater coordination between all the different activities which, until that time, had been done in a somewhat haphazard way. These included all the research that had previously been car-ried out under the auspices of IDIBAPS or the Clínic Foundation and all the training activities organised by the University of Bar-celona’s Department of Public Health and Preventive Medicine.
CRESIB was an independent legal entity governed by a board of trustees. It had its own mission and vision. After its creation, the volume of research increased significantly. Researchers were able to submit proposals in response to calls for new projects, to attract more funds and to recruit new researchers into their teams. While malaria continued to be the principal focus, new lines of research opened up in other areas, including acute respiratory infections, diarrhoeal diseases, tuberculosis and HIV/AIDS.
Another repercussion of the new situation was the expansion of the scope of the research, with a larger number of multicen-tre studies involving sites outside of Africa. “The move into re-search on Plasmodium vivax malaria was one of the first things that happened as a result of the creation of CRESIB”, explains Nuria Casamitjana. “Until then, the research had been very much focussed on Plasmodium falciparum malaria. The team was

8180 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
Once CRESIB had been consolidated, Marina Geli and Joan Rodés (in the photo both to the right of Pedro Alonso) visited CISM. The Catalan Government has played an essential role in supporting international health research in both Spain and Mozambique. © Hospital Clínic de Barcelona
The first CRESIB scientific retreat was held in June 2006 to reflect on and discuss the various lines of research. © ISGlobal archive
Today, CRESIB’s labs occupy almost an entire floor of the CEK building, located next to the Hospital Clínic. © Pau Fabregat
strengthened by the addition of two new researchers: Hernan-do del Portillo, a specialist in the molecular biology of malaria; and Ivo Muller, a malaria epidemiologist working in Papua New Guinea. At the same time a project funded by the CELLEX Foun-dation was also started. These events soon gave rise to new multi-centre studies on Plasmodium vivax malaria in Brazil, India, Gua-temala, Colombia and Papua New Guinea.”
CRESIB also opened up new lines of research in other fields, in-cluding the social sciences and health economics. More new team members were recruited, including the anthropologist Robert Pool, currently at the University of Amsterdam, the sociologist Maria Roura, who studies the viability of HIV/AIDS testing in different epidemiological contexts, and the economist Elisa Si-curi, who is currently studying the cost-benefit relationship of new drugs and vaccines. Another person who joined CRESIB at that time was the epidemiologist Ned Hayes, who came from the Centers for Disease Control and Prevention in the USA. A spe-cialist in arboviral infections such as dengue, Ned made a great contribution to the course on arboviral diseases and the establish-
ment of the new Master of Global Health programme, of which he was director.
“The strategy”, explains Pedro Alonso, “was to concentrate all the international health activities and create a stable, cutting edge in-stitution that would focus on the issues affecting the health of the world’s most disadvantaged people. What was wanted was a cen-tre with roots in the Hospital Clínic and its alma mater, the Uni-versity of Barcelona, that would work to improve medical care, research and training”.
Ultimately, the creation of CRESIB strengthened the capacities of the Barcelona team on all fronts, in terms of funding, person-nel and also square metres. Today, its researchers occupy almost a whole floor of the Esther Koplowitz Centre (CEK), the Clínic Foundation’s biomedical research building, and in addition a whole floor of the building at 132 Carrer Roselló —a far cry from the first small laboratory space occupied by the Epidemiology Unit barely ten years ago.
But the impact and quality of a centre of this kind cannot be meas-ured only in terms of the number of laboratories, amount of staff or the volume of scientific output.
The creation of CRESIB also had a significant impact on training. After gaining accreditation from the University of Barcelona as
one of their medical doctorate programme’s research centres, CRESIB took on a leading role in the area of international health within that programme. Nuria Casamitjana explains how this enhanced the centre’s prestige, “and to be able to do a PhD at an internationally known centre like this one was an added bo-nus for the students”. In fact, the number of PhD students enter-ing the programme increased considerably.
Researchers and students flow back and forth between the centres in Barcelona and Mo-
8382 THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
THE RESEARCH BOOM IN CISM AND THE CREATION OF CRESIB
From left to right: Llorenç Quintó, John Aponte, Santi Pérez-Hoyos, Sergi Sanz and Edgar Ayala discuss statisti-cal methods for the analysis of data from a CRESIB study. © Pau Fabregat
Senior lab technician Alfons Jiménez uses a micros- cope to quantify the number of parasites in a sample of blood infected with Plasmodium falciparum. © Pau Fabregat
zambique. According to Eusebio Macete, “A large number of the PhDs at CRESIB have been done in Manhiça or on issues related to here”.
These years of growth in Manhiça and Barcelona could be lik-ened to a train travelling at high speed at the same time as more railway lines and carriages are added. However, while the changes and developments described in this chapter were very important, they were not the only ones taking place at that time. At the same time as the CISM expanded its research output and the idea of CRESIB started to take shape in Barcelona, a new chapter opened up in the history of the Spanish national health system and the Hospital Clínic’s Tropical Medicine and International Health De-partment. As the next chapter reveals, Spain became a channel for the transmission of Chagas disease, a tropical parasitic infection.

The Tropical Medicine and International Health Department and the challenge of the new wave of immigration

87 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
As a result of economic growth and the availability of jobs (many of which were in the black econ-omy), Spain in the blink of an eye became the country with the fastest growing immigrant population in Europe. In 2000, foreigners represented 2.3% of the registered population. Sev-en years later, this figure had in-creased to 9.9%.10
As has already been mentioned in the previous chapter in the context of the creation of CRESIB, the rapid increase in immigration had a major impact on the country’s health services, and especially on pae-diatric care. The profile of patients in the International Health and Tropical Medicine Department at the Hospital Clínic also started to reflect these demographic changes. In the past the department had mainly treated patients from sub-Saharan Africa and the predominant diseases were malaria, infection with intestinal parasites and schisto-somiasis. Now, the doctors started to see many more people from Latin American countries and a large proportion of these new patients had an illness previously unknown in Spain, a parasitic infection called Chagas disease (or American trypanosomiasis).
Between the end of the nineteen nineties and 2003, over two million people from Latin America came to live in Spain. Joaquim Gascon re-calls the time when they first started to see Bolivian patients who pre-sented with a particular set of symptoms that raised the suspicions of the team.
Since they were aware that Chagas disease is endemic in Bolivia, the doctors started to wonder whether the digestive and cardiovascular symptoms of these new patients might be related to the parasitic in-fection. Some patients even openly expressed their concern about the disease, which in Bolivia is associated with death. “Nobody in Spain knew much about Chagas, and as the surge in immigration was so re-cent, there hadn’t been any cases”, says José Muñoz, one of the doc-tors who works in the department. “As these cases were not resolved in the primary healthcare centres or anywhere else, some of them would eventually end up here.”
“At the same time, the blood bank [at the Hospital Clínic] alerted us that they were seeing Latin American donors who perhaps had Cha-
Chagas, a disease rescued from oblivion
10 Morera Montes J., Alonso Babarro A., Huerga Aramburu H. 2009. Manual de atención al inmigrante. ERGON. P. 351.

8988 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
gas disease” relates Joaquim. “We wanted to see whether we were dealing with isolated cases or whether this was really a public health problem.” To answer this question, the team produced a descriptive analysis of the profile of the patients and of the disease, and three large studies were undertaken. One was carried out by the Catalan Blood Bank, another focussed on the maternity wards of the Hospi-tal Sant Joan de Déu and Hospital Clínic, and the third involved out-patient consultations at the Hospital Clínic and Drassanes Primary Health Care Centre, the two healthcare facilities where most of the cases of imported infectious diseases were treated in Barcelona.
The results of these studies showed that far from being isolated cases, the patients diagnosed with Chagas disease at the Hospital Clínic only represented the tip of the iceberg. As much as 27% of Bolivian moth-ers and 10% of blood donors of Bolivian origin had the disease.
These important studies had a major impact on public health policies. In 2005, the national law regulating blood transfusions was modified to make it obligatory for all donors coming from Latin America to be tested for Chagas. Five years later, a protocol for the control of vertical transmission of the disease was put in place in Catalonia to diagnose pregnant women with the infection so that they and their children could be monitored and treated.
“It was the first time in Spain—a country where Chagas is not endem-ic—that it became necessary to create a local programme to control infection within Spain with a tropical disease from ‘over there’”, says Joaquim Gascon. It was a paradigm shift that required a change in the way of thinking about the problem. “It was not a case of nothing be-ing done here before about this issue; the question of Chagas disease simply never came up!” he adds.
This shift marked the beginning of the significant work relating to Chagas led by the Hospital Clínic, first in Spain and later in Bolivia, an effort that continues today. “We were the first to describe the disease”, says José Muñoz, “and we have acquired the know-how to deal with it. Our common language, our historical and cultural ties and the scale of Latin American immigration into Spain gave us the opportunity to become a leader in this area in Europe.”
Owing to migratory flows, Chagas disease, an infection originally en-demic only in Latin America, is now present in other places, including the USA, Australia, Japan and Europe. Even so, it remains one of the world’s most neglected diseases because it mainly affects people in
Latin America with very low purchasing power. Consequently the dis-ease has never attracted the interest of large pharmaceutical compa-nies looking to invest in the search for new treatments. The only treat-ments that exist—nifurtimox and benznidazole—were developed in the sixties by the veterinary industry. They require a long treatment period and can have serious adverse effects.
Eventually it became necessary at the Hospital Clinic to set aside two days a week exclusively for seeing patients with Chagas. This was not only because of the volume of people who came but also because of the difficulties the patients faced in keeping their appointments, as many of them literally work from dawn to dusk. The immigration from Latin America, and in this case Bolivia, has been predominantly female and this is reflected in the profile of the patients with Chagas who come to the hospital. Most of these women work as cleaners in offices or private homes. Sometimes they start the treatment without telling their employers. However, the side effects of the therapy, which include extensive skin rashes and joint pain, can be so intense—in some cases requiring hospitalisation—that the patient may be unable to work and may even be dismissed as a result.
In Bolivia, the disease is very common. However, “there is still a sig-nificant lack of awareness among the patients who come here, either
Cochabamba, Bolivia’s third largest city, was the site chosen for Hospital Clínic’s pilot project for Chagas patients in 2009. © Juan Millás

9190 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
Elizabeth Posadas explains Chagas disease to a patient in the Tropical Medicine and International Health Depart-ment at the Hospital Clinic. © Archive ISGlobal.
Chagas is transmitted through the faeces of the vinchuca or kissing bug, the insect vector that carries the disease. © Juan Millás
because they have been too scared to seek information or because they lacked the means to do so. In a lot of places in Bolivia, it costs money to do the test”, explains Elizabeth Posadas, an anthropologist who has worked with Chagas patients in the Tropical Medicine and Interna-tional Health Department since 2007.
For many of these patients, the very idea of being diagnosed brings to mind unpleasant images of the method previously used in Bolivia: a kissing bug (Triatoma infestans) would be placed on the patient’s skin until it bit, and then the bug’s faeces was analysed to see whether the person had Chagas disease. In spite of the fact that 60% of those in-fected never develop the disease, people are often anxious and afraid of being diagnosed because of their memories of relatives or friends who died from Chagas. “We try to explain to them that the context is an all-important factor and that things are different here”, Elizabeth says. “The first thing we do is an electrocardiogram or a chest X-ray to see whether or not the heart is affected.”

9392 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
Joaquim Gascon’s team did not limit itself to undertaking stud-ies and treating patients in Bar-celona. Once it had been con-firmed that most of the people who had the disease came from Bolivia, Joaquim got in touch with Faustino Torrico, a doctor and professor of medicine who until 2007 was responsible for
diagnosis and treatment in the National Control Programme of Chagas Disease in Bolivia. Until then, all the work in Bolivia had focussed on controlling the vector and treating newborn babies and pregnant women. However, nothing was being done about the treatment of adults; the lucky ones were diagnosed, but very few were actually treated. The idea of starting up a pilot project in Bo-livia was born as a result of that initial contact.
A healthcare project was designed in 2008 and launched a year lat-er with the financial support of the Catalan Aid and Development Agency (ACCD). The project was based on the protocols used by the Hospital Clínic and by Faustino Torrico and his team in Co-chabamba in Bolivia. María Jesús Pinazo was the doctor respon-sible for starting up the programme: “We began treating people in 2009. The patients felt that they were being well treated just because someone was finally looking after them, because a doc-tor followed up on what was happening to them and they weren’t abandoned once they started the treatment.”
In view of the success of this pilot project, AECID funded the joint project for a period of four years. The Platform for the Integral Care of Patients With Chagas Disease was set up and the pilot project was expanded to bring the health-care programme to six other centres located in the regions of Cochabamba, Chuquisaca and Tarija. Today, several oth-er initiatives have been added, involving healthcare, the train-ing of health professionals and
From Barcelona to Bolivia
From left to right: María Jesús Pinazo, Faustino Torrico, Joaquim Gascon, Lluís Basteiro (at that time ACCD delegate in Bolivia) and Jimmy Pinto (the doctor in charge of the Cercado- Cochabamba centre) at the launch of the Platform in July 2009. © ISGlobal archive
research. Once again, the work is based on the three pillars that define this thirty-year-long story.
The fact that the healthcare protocols are shared between the two countries has greatly facilitated the work on a transnational level. Patients seen by a doctor in one country can have follow-up treat-ment in the other if they travel there or move permanently. And the relatives of the patients treated by the Hospital Clínic in Bar-celona can be referred to any of the six healthcare centres that form part of the programme in Bolivia and vice-versa. “It’s like moving home and keeping the same furniture”, says María Jesús Pinazo. Moreover, as she goes on to explain, “having a network of centres with common healthcare protocols and a solid da-tabase allows us to generate quality, high impact research”. The Platform represents a new healthcare model in Bolivia based on the integration of healthcare and research and is a benchmark for the whole region.
For the staff at Hospital Clínic, it has been fundamental to have had the opportunity to go to the country of origin and gain a better un-derstanding of the context where the disease and those affected come from. Visiting Bolivia has allowed them to improve the health-care in Spain, where 50,000 to 70,000 people with Chagas disease now live. “You can sit behind a desk and treat someone. But, if you don’t come [to Bolivia] and see the reality for yourself, you can’t un-derstand the disease and why people are in the situation they are in. It’s essential to put it in context”, emphasises María Jesús.
In Bolivia there is huge demand for the diagnosis and treatment of Chagas disease. © Andalu Vila-San-Juan

9594 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
At the time she was interviewed for this book, María Jesús was reaching the end of her four years in Bolivia. The first four-year project is also coming to an end and AECID has decided to fund the initiative for a further four years. In anticipation of her return to Barcelona and to the Hospital Clínic, she reflects on what has been achieved to date through the Platform: “For me the most im-portant accomplishment has been to bring the disease out into the open, to end the silence. We no longer talk about a neglected disease of forgotten people. Chagas disease exists, and research is being done.”
There is still a lot to be done. The priorities are: research aimed at finding more reliable diagnostic methods, more effective and easy-to-administer antiparasitic drugs and the development of biomarkers.
In Spain, a national strategy and a vertical transmission control programme have yet to be established. Today, only four autono-mous communities have implemented programmes to control the vertical transmission of Chagas disease.
“Except for the United Kingdom, most of the European countries that have attracted Latin American immigrants over the last two decades have no specific programme in place to treat Chagas dis-ease. Consequently, the Catalan experience is considered by the World Health Organisation to be a benchmark for the rest of the continent”, explains Antoni Plasència, the technical director of CRESIB and former director general of Public Health in Catalo-nia from 2004 to 2011
In the last fifteen years, over a thousand patients have been treated for Chagas disease at the Hospital Clínic. Without a doubt, the emergence of this disease in Spain has had an impact, both on the consulting rooms at the hos-pital and as a public health issue.
However, while Chagas rep-resents a large proportion of the cases seen in recent years, the big-gest clinical challenges faced by the department are not related to this disease. Other challenges, such as complicated cases of malaria
The Hospital Clínic, a centre of excellence for imported diseases
or schistosomiasis, or patients with Japanese encephalitis, can result in sleepless nights for the medical team. Sometimes the doctors are faced with conditions that are difficult to diagnose. Or patients come in and report having had a fever for days and days without any obvi-ous cause. In such cases, the clinical workup can be complex, requir-ing unusual tests and further explorations. As this is a hospital, it is often the last stop for patients with the rarest diseases. As a result, a great deal of work usually has to go into each and every diagnosis.
In June 2014, the department was made a national referral unit by the Spanish National Health System.
“In a centre of excellence like this one”, says José Muñoz, “you have to study diseases you are never going to see. This is something we often discuss with the medical residents, who ask us why they have to study a disease that they will probably never encounter in their practice. Take the case of the Ebola virus, for example. We haven’t yet seen any cases here, but our department has been involved in drafting a proto-col that describes what we must do if, for example, we receive a patient with Ebola haemorrhagic fever from Sierra Leone. Diseases you nev-er see can generate a lot of work because you have to be well informed and up-to-date.”
It is not surprising therefore that an essential requirement for any doctor who wants to work in the Tropical Medicine and Internation-al Health Department is to have first-hand experience of the envi-ronments where the diseases they deal with are found. “The disease is important, but everything that surrounds it is equally or even more important”, explains José Muñoz. “The experience of living and working in Africa or Latin America helps us to understand the con-text of the diseases when the patients explain them to you… When a patient who has schistosomiasis comes in and tells you that they have lived in a part of Senegal or the Ivory Coast that you have vis-ited yourself, a place with a river, where you know the kids swim and women wash clothes, a place where you know people get infected, you immediately know that they may have schistosomiasis… That his-torical memory you can use to recreate the situation is beautiful for the doctor and helps us to provide better care.”
“In this department the doctors understand and share the thirst for knowledge... that curiosity that some people carry inside, the desire to know other places and cultures”, says Mercè Bosch, a forty-eight-year-old Catalan biologist who first came to the department as a pa-

9796 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
tient in 2013 after a trip to Costa Rica. Tears well up in her eyes when she talks about what travel means to her, how it is one of the driv-ing forces in her life. She emphasises how important it was for her that the doctors treated her with humanity, that they transmitted a feel-ing of calmness and understood her need to travel and see the world. “It’s very important that the doctor is able to calm the patient and doesn’t judge them for wanting to travel to certain places or do cer-tain things. Some doctors might ask, ‘What did you think you were doing? What have you done?’ These ones [the doctors in the depart-ment] know what they are dealing with.”
For another doctor, Antonia Calvo, the department is like a “window onto the world” because of the stories that lie behind each patient. In the intimacy of the consulting room, the immigrant patients share the story of their lives, both the one they left behind and the one they have now. In other cases, the stories reflect the adventures and anec-dotes of returning travellers, who sometimes even come straight from the airport to the hospital.
Among the travellers, malaria has always been one of the most com-mon diseases together with traveller’s diarrhoea, which is the motive for seeking medical attention in 25-30% of cases. Digestive problems caused by giardia and salmonella and skin problems, urine infections and pneumonias are also frequent, as are fevers not due to malaria, usu-ally a symptom of dengue or typhoid fever or acute schistosomiasis.
Fever and diarrhoea were the symptoms Joan Prosper had on his re-turn from a trip to India during the Christmas holidays in 2013 and the reason for his first visit to the Tropical Medicine and Internation-al Health Department in January 2014. Used to travelling to all the corners of the world, this was a trip he and his wife Laia Montoliu will not easily forget. “Because of where we live in the city, I ought to go to a different hospital, but we have always known that there is an excellent tropical medicine department at the Hospital Clínic. As soon as I started feeling unwell after the trip, I went straight there. I didn’t think twice”, Joan recalls. He was diagnosed and treated for an amoebic infection and Laia for giardiasis. A few days later he had a fever again and returned to the Hospital Clínic. This time he was hos-pitalised for a week with hepatitis E infection, another souvenir from his trip to India.
“It gives you a great sense of security”, adds Laia, “to know that we have this service in Barcelona”. And she is surprised the same service
does not exist in other places. “I remember an anecdote from when I attended a congress in Ghana in 2008. Some colleagues from Okla-homa and Melbourne were concerned about getting malaria or other diseases. I told them not to worry. I said that if they did catch some-thing they could go to the tropical medicine clinic when they got home, like the one we have here. One of them looked at me and said ‘Laia, Oklahoma is not Barcelona’ so I presume that they must not have a service like this one over there.”
The care offered to patients return from abroad is important, but the work of the Travel Clinic (SAVI) created in 2008 is equally so. SAVI represents the fruit of the work started by Manuel Corachan and Joaquim Gascon over twenty years ago. On average, 15,000 people come to the clinic every year for information and advice and to get the relevant pre-departure vaccinations. If they need medical attention when they return home, they go straight to the Tropical Medicine and International Health Department, which attends an annual aver-age of 1,200 patients (first visits).
“We have always had tourists”, says Azucena Bardaji, the doctor cur-rently in charge of the Travel Clinic, “but now there are fewer aid workers and especially far fewer missionaries than before”. The cur-rent financial recession in Spain has resulted in a radical change in the profile of the travellers who use this service to get information and vaccinations. Over the last five or six years, there has been a notice-able increase in the number of people who travel for work. Before, work-related travel accounted for only isolated cases. Today, it is not surprising to find many people who travel for professional reasons to countries far beyond the borders of Europe. Some are workers, in the construction industry for example, who have lost their jobs in Spain and found employment in Africa.
Another significant change noted by José Muñoz is that nowadays certain diseases, especially the preventable ones, are not seen so much in the consulting room. This change is partly due to the fact that trav-el has become less hazardous than it was a few years ago. The tour-ist industry has grown so much and become so globalised that it is difficult to find a totally remote and unexplored area where you can-not buy bottled water, for example. But another factor is that it is be-coming more and more ingrained in people’s minds that prevention is better than cure. “We used to see many cases of schistosomiasis, but it seems that the preventive measures advised by services like the Travel Clinic are having a positive effect and people are looking after themselves a bit more”, he adds.

9998 THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
THE TROPICAL MEDICINE AND INTERNATIONAL HEALTH DEPARTMENT AND THE CHALLENGE OF THE NEW WAVE OF IMMIGRATION
From the outset, the Tropical Medicine and International Health Department has worked closely with professionals from other departments in the hos-pital and other local healthcare centres as well as participating in networks and platforms on a na-tional and international level.
Jordi Vila says that his department (Microbiology) and the Trop-ical Medicine Department are “like brothers”. It is a longstanding relationship, “intense and fruitful from the start”. He remembers how the first contact he had with them was in the eighties about some diagnostic methods that were very specific to the field of tropical medicine. At that time, the Microbiology Department did not have the tools that were needed. “They are used for detecting microorganisms that aren’t native to Spain, like the enterotoxigen-ic Escherichia coli bacteria that causes traveller’s diarrhoea”. After conversations with Manuel Corachan and Joaquim Gascon, the Mi-crobiology Department acquired the tools that would allow them to test whether or not a patient’s diarrhoea was caused by E. coli.
Today, the Microbiology Department still plays an important role in the diagnosis of imported diseases, such as malaria, den-gue, Chagas disease and the chikungunya virus, among others. “Not all microbiology departments in Spain have these methods, but we have had to put them in place because they are needed for the Tropical Medicine and International Health Department”, explains Jordi Vila. “It’s an indispensable service in a hospital like ours”, he adds.
Antonia Calvo feels lucky to be able to work in the field of tropical medicine in a hospital that has all the necessary technical infra-structure and staff in different departments who are used to see-ing cases of imported diseases. Certain things she values highly: “Being able to do very complex diagnostic tests and obtain certain foreign drugs in the hospital pharmacy that would be difficult or impossible to find in other hospitals”.
Hospital Clínic has worked closely with Sant Joan de Déu- Barcelona Children’s Hospital over the years. Victoria Fuma-dó is a paediatrician who studied Tropical Medicine at the Uni-versity of Barcelona and worked with Clara Menéndez on the
Collaboration with other departments and healthcare centres
IRONMAL study in Tanzania. At the end of the nineties, when the Hospital Clínic stopped treating children, Victoria was re-sponsible for setting up a specialised Tropical Medicine Unit in Sant Joan de Déu with the Tropical Medicine and International Health Department of the Hospital Clínic as its reference.
On the community level, a working group was established in 2011 with the participation of several family practitioners to create protocols for healthcare and referral from the primary health care centres to the Hospital Clínic.
On a national level, as mentioned earlier, the department played a ma-jor role at the end of the nineties in the creation of the Spanish So-ciety of Tropical Medicine and International Health (SEMTSI) and Manuel Corachan served as the first president of the new organisa-tion. Significant work has also been done with the Spanish Network of Collaborative Research on Tropical Diseases (RICET). On a Eu-ropean level, the department has maintained a longstanding relation-ship with the European Network for Tropical Medicine and Travel Health (TropNet) since it was set up in 1999.

The Barcelona Institute for Global Health, taking science one step further

103 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
In the building across the road from the Tropical Medicine consulting rooms, on corner of Carrer Roselló and Carrer Casanova, we find the Barcelo-na Institute for Global Health (ISGlobal). The foundation of this relatively new institute is the most recent development in this thirty-year-long journey.
With office space on five floors, ISGlobal has brought together the activities of OCI, CRESIB, the training department and the think tank under a single roof.
The term that comes into every conversation and is on everyone’s lips in this building is knowledge translation, a concept that lies at the heart of this new institution. While research, healthcare and training continue to be key elements, with the creation of ISGlobal a new ingredient has been added to the mix: political advocacy and strat-egies aimed at translating scientific evidence into concrete action.
This new component has been added because the scientists’ work usually ends when their results are published; however, the pub-lication of an article does not necessarily have any real impact on public policies or models of action. It is at this stage that the job of the professionals in the think tank team begins; their task is to take the findings a step further and translate the new scientific evidence into practice, ensuring that it is applied to change models of action and policies.
ISGlobal is a creation of modern Barcelona and reflects the reality of a city that has changed mas-sively over the last three decades. It has not only become a top destination for the thousands of tourists who visit each year attracted by its international reputation, it has also become a recognised hub of excellence in the world of biomedicine. The hospitals have improved greatly, the number of research centres has grown and the city is home
The foundation of ISGlobal
Today, Barcelona is an international hub of excellence in biomedicine. © Andalu Vila-San-Juan
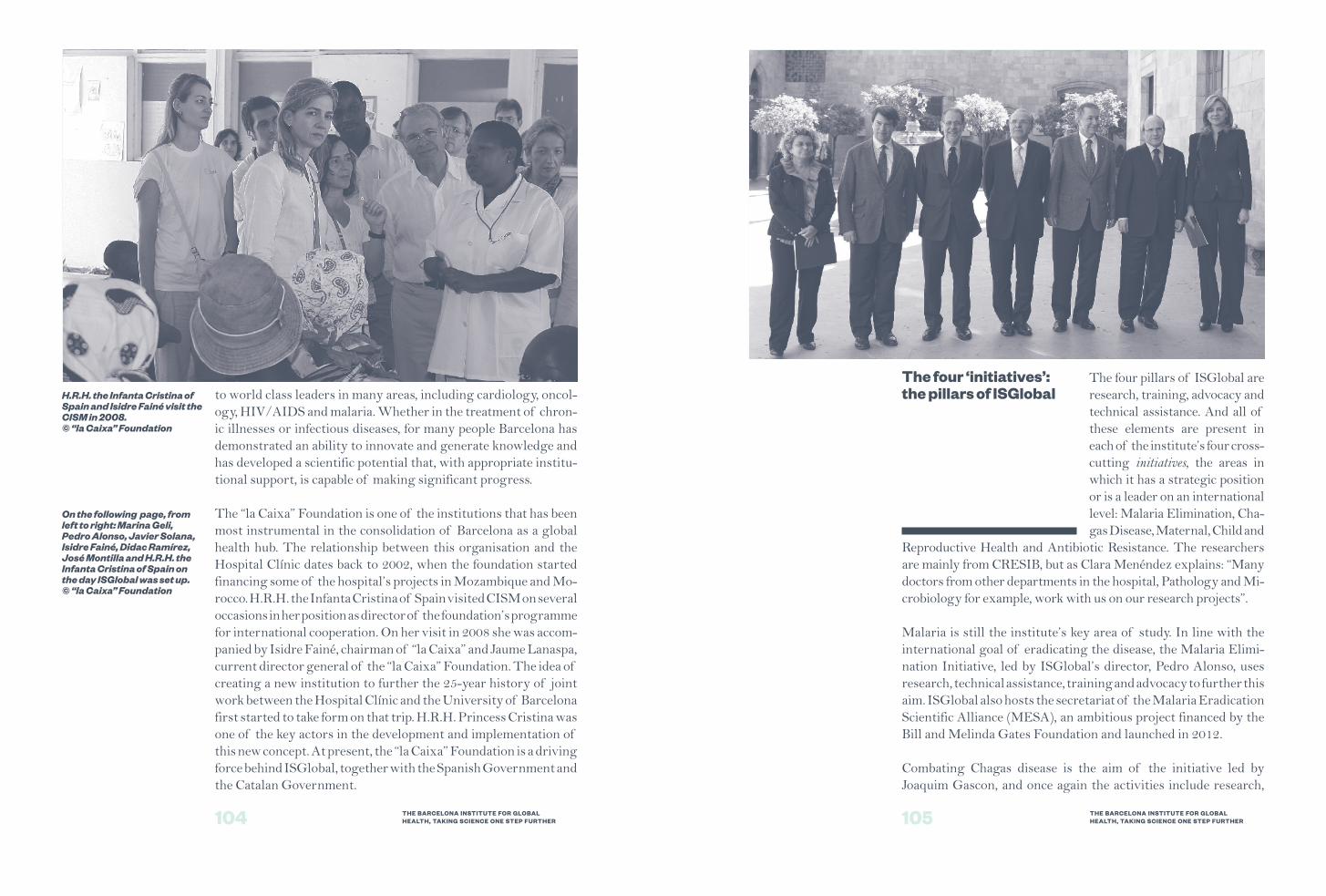
105104 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
H.R.H. the Infanta Cristina of Spain and Isidre Fainé visit the CISM in 2008. © “la Caixa” Foundation
On the following page, from left to right: Marina Geli, Pedro Alonso, Javier Solana, Isidre Fainé, Didac Ramírez, José Montilla and H.R.H. the Infanta Cristina of Spain on the day ISGlobal was set up. © “la Caixa” Foundation
The four ‘initiatives’: the pillars of ISGlobal to world class leaders in many areas, including cardiology, oncol-
ogy, HIV/AIDS and malaria. Whether in the treatment of chron-ic illnesses or infectious diseases, for many people Barcelona has demonstrated an ability to innovate and generate knowledge and has developed a scientific potential that, with appropriate institu-tional support, is capable of making significant progress.
The “la Caixa” Foundation is one of the institutions that has been most instrumental in the consolidation of Barcelona as a global health hub. The relationship between this organisation and the Hospital Clínic dates back to 2002, when the foundation started financing some of the hospital’s projects in Mozambique and Mo-rocco. H.R.H. the Infanta Cristina of Spain visited CISM on several occasions in her position as director of the foundation’s programme for international cooperation. On her visit in 2008 she was accom-panied by Isidre Fainé, chairman of “la Caixa” and Jaume Lanaspa, current director general of the “la Caixa” Foundation. The idea of creating a new institution to further the 25-year history of joint work between the Hospital Clínic and the University of Barcelona first started to take form on that trip. H.R.H. Princess Cristina was one of the key actors in the development and implementation of this new concept. At present, the “la Caixa” Foundation is a driving force behind ISGlobal, together with the Spanish Government and the Catalan Government.
The four pillars of ISGlobal are research, training, advocacy and technical assistance. And all of these elements are present in each of the institute’s four cross- cutting initiatives, the areas in which it has a strategic position or is a leader on an international level: Malaria Elimination, Cha-gas Disease, Maternal, Child and
Reproductive Health and Antibiotic Resistance. The researchers are mainly from CRESIB, but as Clara Menéndez explains: “Many doctors from other departments in the hospital, Pathology and Mi-crobiology for example, work with us on our research projects”.
Malaria is still the institute’s key area of study. In line with the international goal of eradicating the disease, the Malaria Elimi-nation Initiative, led by ISGlobal’s director, Pedro Alonso, uses research, technical assistance, training and advocacy to further this aim. ISGlobal also hosts the secretariat of the Malaria Eradication Scientific Alliance (MESA), an ambitious project financed by the Bill and Melinda Gates Foundation and launched in 2012.
Combating Chagas disease is the aim of the initiative led by Joaquim Gascon, and once again the activities include research,
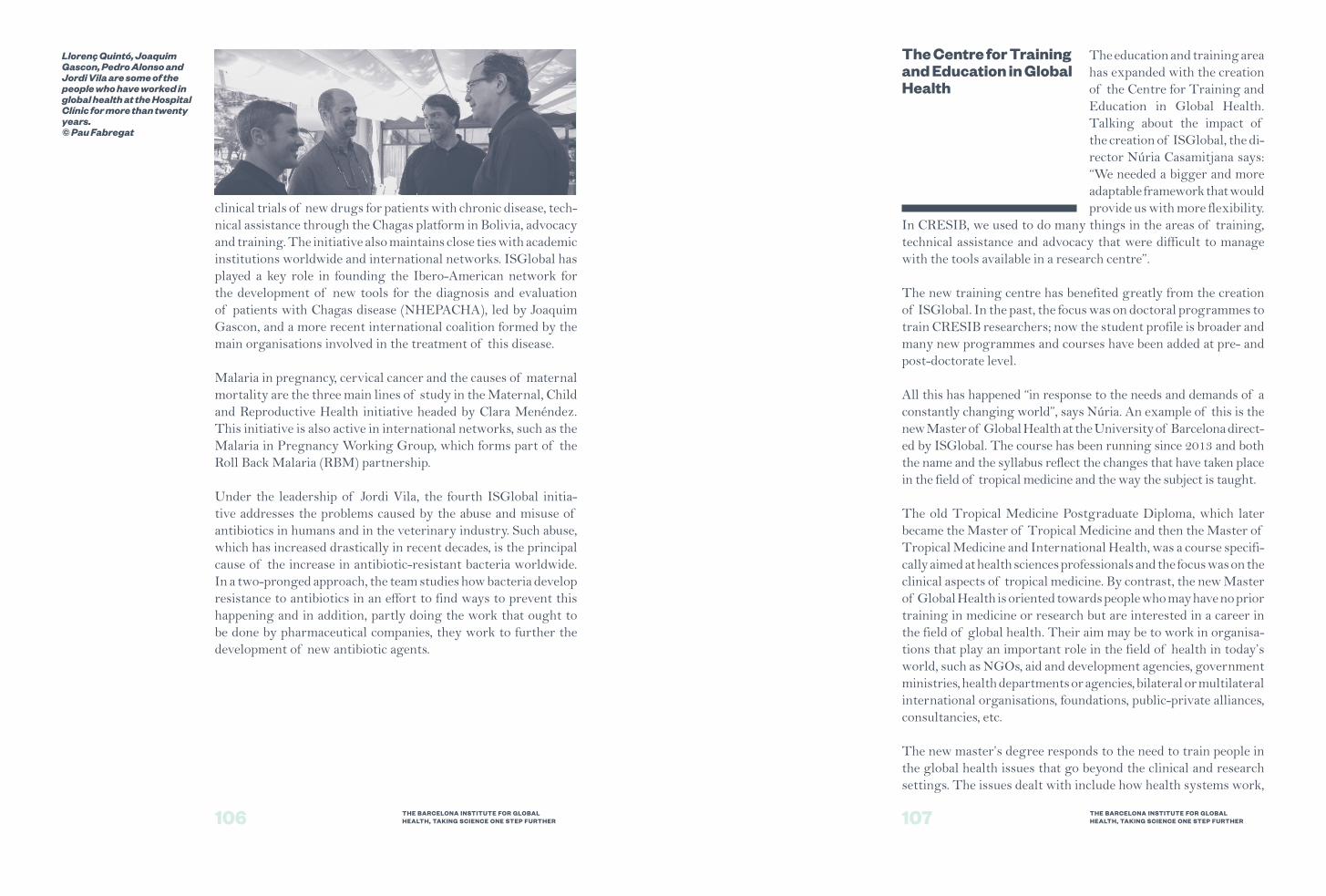
107106 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
The Centre for Training and Education in Global Health
Llorenç Quintó, Joaquim Gascon, Pedro Alonso and Jordi Vila are some of the people who have worked in global health at the Hospital Clínic for more than twenty years. © Pau Fabregat
clinical trials of new drugs for patients with chronic disease, tech-nical assistance through the Chagas platform in Bolivia, advocacy and training. The initiative also maintains close ties with academic institutions worldwide and international networks. ISGlobal has played a key role in founding the Ibero-American network for the development of new tools for the diagnosis and evaluation of patients with Chagas disease (NHEPACHA), led by Joaquim Gascon, and a more recent international coalition formed by the main organisations involved in the treatment of this disease.
Malaria in pregnancy, cervical cancer and the causes of maternal mortality are the three main lines of study in the Maternal, Child and Reproductive Health initiative headed by Clara Menéndez. This initiative is also active in international networks, such as the Malaria in Pregnancy Working Group, which forms part of the Roll Back Malaria (RBM) partnership.
Under the leadership of Jordi Vila, the fourth ISGlobal initia-tive addresses the problems caused by the abuse and misuse of antibiotics in humans and in the veterinary industry. Such abuse, which has increased drastically in recent decades, is the principal cause of the increase in antibiotic-resistant bacteria worldwide. In a two-pronged approach, the team studies how bacteria develop resistance to antibiotics in an effort to find ways to prevent this happening and in addition, partly doing the work that ought to be done by pharmaceutical companies, they work to further the development of new antibiotic agents.
The education and training area has expanded with the creation of the Centre for Training and Education in Global Health. Talking about the impact of the creation of ISGlobal, the di-rector Núria Casamitjana says: “We needed a bigger and more adaptable framework that would provide us with more flexibility.
In CRESIB, we used to do many things in the areas of training, technical assistance and advocacy that were difficult to manage with the tools available in a research centre”.
The new training centre has benefited greatly from the creation of ISGlobal. In the past, the focus was on doctoral programmes to train CRESIB researchers; now the student profile is broader and many new programmes and courses have been added at pre- and post-doctorate level.
All this has happened “in response to the needs and demands of a constantly changing world”, says Núria. An example of this is the new Master of Global Health at the University of Barcelona direct-ed by ISGlobal. The course has been running since 2013 and both the name and the syllabus reflect the changes that have taken place in the field of tropical medicine and the way the subject is taught.
The old Tropical Medicine Postgraduate Diploma, which later became the Master of Tropical Medicine and then the Master of Tropical Medicine and International Health, was a course specifi-cally aimed at health sciences professionals and the focus was on the clinical aspects of tropical medicine. By contrast, the new Master of Global Health is oriented towards people who may have no prior training in medicine or research but are interested in a career in the field of global health. Their aim may be to work in organisa-tions that play an important role in the field of health in today’s world, such as NGOs, aid and development agencies, government ministries, health departments or agencies, bilateral or multilateral international organisations, foundations, public-private alliances, consultancies, etc.
The new master’s degree responds to the need to train people in the global health issues that go beyond the clinical and research settings. The issues dealt with include how health systems work,
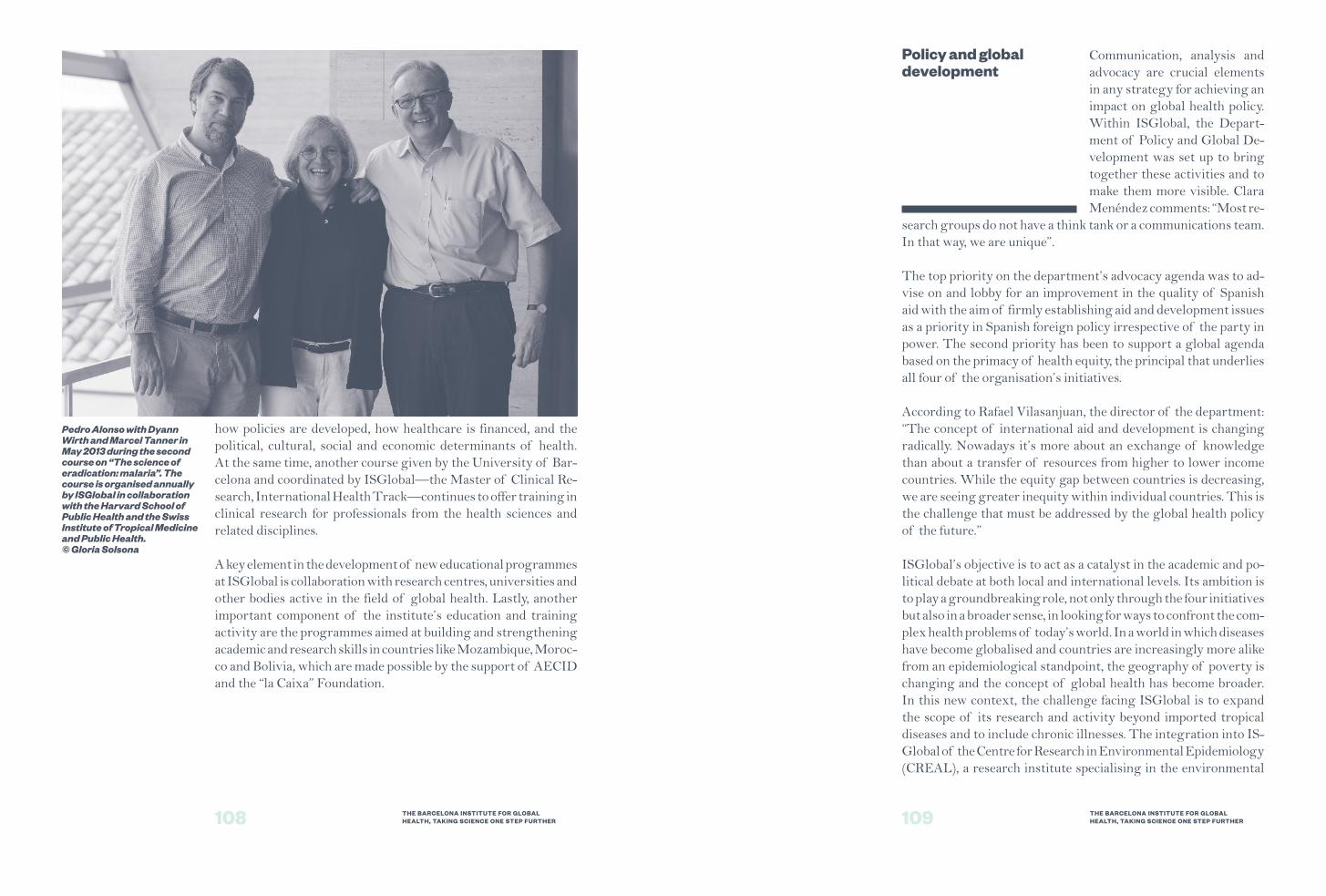
109108 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
Pedro Alonso with Dyann Wirth and Marcel Tanner in May 2013 during the second course on “The science of eradication: malaria”. The course is organised annually by ISGlobal in collaboration with the Harvard School of Public Health and the Swiss Institute of Tropical Medicine and Public Health. © Gloria Solsona
Policy and global development
how policies are developed, how healthcare is financed, and the political, cultural, social and economic determinants of health. At the same time, another course given by the University of Bar-celona and coordinated by ISGlobal—the Master of Clinical Re-search, International Health Track—continues to offer training in clinical research for professionals from the health sciences and related disciplines.
A key element in the development of new educational programmes at ISGlobal is collaboration with research centres, universities and other bodies active in the field of global health. Lastly, another important component of the institute’s education and training activity are the programmes aimed at building and strengthening academic and research skills in countries like Mozambique, Moroc-co and Bolivia, which are made possible by the support of AECID and the “la Caixa” Foundation.
Communication, analysis and advocacy are crucial elements in any strategy for achieving an impact on global health policy. Within ISGlobal, the Depart-ment of Policy and Global De-velopment was set up to bring together these activities and to make them more visible. Clara Menéndez comments: “Most re-
search groups do not have a think tank or a communications team. In that way, we are unique”.
The top priority on the department’s advocacy agenda was to ad-vise on and lobby for an improvement in the quality of Spanish aid with the aim of firmly establishing aid and development issues as a priority in Spanish foreign policy irrespective of the party in power. The second priority has been to support a global agenda based on the primacy of health equity, the principal that underlies all four of the organisation’s initiatives.
According to Rafael Vilasanjuan, the director of the department: “The concept of international aid and development is changing radically. Nowadays it’s more about an exchange of knowledge than about a transfer of resources from higher to lower income countries. While the equity gap between countries is decreasing, we are seeing greater inequity within individual countries. This is the challenge that must be addressed by the global health policy of the future.”
ISGlobal’s objective is to act as a catalyst in the academic and po-litical debate at both local and international levels. Its ambition is to play a groundbreaking role, not only through the four initiatives but also in a broader sense, in looking for ways to confront the com-plex health problems of today’s world. In a world in which diseases have become globalised and countries are increasingly more alike from an epidemiological standpoint, the geography of poverty is changing and the concept of global health has become broader. In this new context, the challenge facing ISGlobal is to expand the scope of its research and activity beyond imported tropical diseases and to include chronic illnesses. The integration into IS-Global of the Centre for Research in Environmental Epidemiology (CREAL), a research institute specialising in the environmental
111110 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
Current and future challenges
A global commitment to people’s health
factors that cause chronic diseases, is currently under way and represents a step in that direction.
Antoni Plasència, the director of CRESIB, reflects on the inter-relation between research and political advocacy: “Although the processes and activities they are involved in are very different, the dialogue between researchers, political scientists and communica-tion professionals is very enriching. And this discussion allows us to extend ISGlobal’s influence on health policies and research agendas”.
ISGlobal has far-reaching ambi-tions and faces tough challeng-es. One important hurdle is the question of financing. In the cur-rent recession, competition for funding between research cen-tres is more intense than ever and state funding has been reduced. ISGlobal currently relies heavi-ly on competitive funding and its
structural funding profile is far from ideal for a centre of this type.
Apart from the impact this imbalance has on the institute’s financial sustainability, it also has an effect on the recruitment and retention of talent. Consequently, diversifying sources of income and obtain-ing new structural funding will undoubtedly be two priorities in the coming years.
Another challenge is to position the centre internationally as a leading provider of education and training and to attract a larger number of students. At present, NGOs in Spain are reducing their staff and the number of postgraduate students is decreasing across all disciplines. According to Núria Casamitjana, this reduction in numbers means that they can no longer rely on the national market. The figures speak for themselves. Of the twenty seven students who have been accepted on next year’s Master of Global Health, only one is Spanish. Finally, another objective in the immediate fu-ture will be to have access to funds and be able to offer scholarships to students from low and middle income countries.
Another important challenge is related to the so-called glass ceiling, a phenomenon regrettably still very prominent throughout all sec-tors and also in the world of research. “In general, there are very
few women in decision making roles and very few women who are in a position to establish research priorities and decide on whether to focus on this issue or that one”, Clara Menéndez says. In her area of expertise—malaria in pregnancy— she is one of the few women working at a high level and the only woman on the international Malaria in Pregnancy consortium. The number of men at senior levels in ISGlobal is also disproportionately high. Most of the researchers in top positions, the directors and the board members are men. By contrast, the bulk of researchers and professionals in technical and administrative roles are women.
Finding ways to change this distribution will not be easy, but steps are already being taken. María José Merino, the person in charge of Human Resources at ISGlobal, explains that a Plan on Gender and Diversity Management has recently been launched as part of the institute’s Strategic Plan for 2014 -2016: “We have started by assessing where we are, and the next step will be to make a proposal for improvement and devise a plan of action”.
As these lines are written in the summer of 2014, thirty years have gone by since the start of this adventure, but only four have passed since the foundation of ISGlobal.
From the seventh floor of the building where several ISGlobal offices are housed, there are mag-
nificent views of Hospital Clínic and the impressive entrance to the Faculty of Medicine. The backdrop is a constant reminder of the ongoing relationship—past and present—between ISGlobal and those two important institutions that gave birth to the institute and this story.
In this critical and historic nexus linking medicine and academia, in a space where it is hard to see where the classrooms end and the consulting rooms begin, the seeds of the first training course and the first consulting room in the Tropical Medicine Unit were planted in the seventies and eighties. Those seeds gave birth to a tree that has given fruits that few could have dreamt of back then. The Tropical Medicine and International Health Department is fully consolidated within the Hospital Clínic. ISGlobal is playing
113112 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
The Faculty of Medicine at the University of Barcelona lies at the heart of the Hospital Clínic. © Hospital Clínic de Barcelona
This longstanding close relationship between the University of Barcelona and the Hospital Clínic has played a vital role throughout these thirty years of work in international health. © Hospital Clínic de Barcelona
in the first division on an inter-national level. The Master of Global Health at the University of Barcelona is fast becoming a benchmark in southern Europe.
The indissoluble link between healthcare, education and train-ing, and research— the common thread running through this story—continues to be as strong as ever. Advocacy, the key to tak-ing science a step further and translating its impact to the po-litical arena, is the ingredient that has been added to the mix in recent years with the creation of ISGlobal.
As the pages of this book have illustrated, these three decades have been marked by turning points, the leadership of a few people and the commitment of many more. Several events have shaped the course of this story and determined the outcome. The foundation of Medicus Mundi and the start of the first training course in Tropical Medicine were important milestones. These were fol-lowed by the arrival of Manuel Corachan at the Hospital Clínic, his crossing of paths with Pedro Alonso and their shared vision. Crucial throughout was the role played by the University of Bar-celona. The creation of CISM and CRESIB opened up new possi-bilities. The story spans the end of the 20th century—the eighties and nineties —and the first decade of the 21st century. With the start of the new century, the climate in Spain, and particularly in Catalonia, was one of increasing political openness and financial prosperity, creating an optimum environment for new initiatives and pushing forward the boundaries of research. And finally, in 2010, with the creation of ISGlobal the story moves on, taking the next great step in a very different political and financial context.
Many people have dedicated their lives, and many still do, to this area of medicine and research. Many people have been motivated by a desire to bridge the yawning gap that excludes millions of people from medical treatments that exist and could save their lives but which are either inaccessible to them or not adapted to their needs.
As always in life, had the circum-stances, the context or the people been different, the story told in this book would also have been different. With the closing of this chapter, and with it the book, a new space opens up for the start of a new story: a new phase of the journey still to be travelled. Never before has there been so much progress in terms of global health as we have seen in the last
ten years. But it is precisely because of this progress that the potential of what remains to be done is even greater. Health indicators are im-proving almost everywhere in the world, even in Africa. Nevertheless, huge challenges lie ahead. More than a billion people on this planet still live in extreme poverty and in very precarious health conditions.
Recent world history is a magnificent testimony to the fact that innovation and medicine continue to be the best investments for achieving a more just future and more balanced global development. The journey travelled over these thirty years since the Hospital Clínic decided to venture beyond its own borders is now driven by new goals and ambitions, while the commitment to creating a more just world based on research, training and healthcare remains as strong as ever.

115114 THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
THE BARCELONA INSTITUTE FOR GLOBAL HEALTH, TAKING SCIENCE ONE STEP FURTHER
ISGlobal’s first team building day held in May 2011. © Pau Fabregat

117
Acknowledgements Thanks to all the people involved in the last thirty years, 28,000 patients have received medical care at the Tropical Medicine and International Health Department at the Hospital Clinic, almost a million patients have been treated at the Manhiça Hospital, in Mozambique, 15,000 patients have been treated for Chagas in Bolivia and 20,000 babies were delivered in Tetouan, Morocco.
In total, 1,076 scientific papers have been published and 53 researchers have successfully defended their doctoral thesis.
We thank all those who were interviewed for the writing of this book:
Pedro Alonso, John Aponte, Pau Balcells, Azucena Bardají, Quique Bassat,Mercè Bosch, Hélder Bulo, Antonia Calvo, Vicenç Cararach,Núria Casamitjana, Albino Chilaule, Manuel Corachan, Carlota Dobaño,Fidel Font, Victoria Fumadó, Alberto García-Basteiro, Joaquim Gascon,Marina Geli, Enric Grau, Ernesto Herrera, Samira Ismael, Cecilia Justino,Eusébio Macete, Maria Maixenchs, Xavier Mas, Alfredo Mayor,Teresa Mejías, Clara Menéndez, Crisóstomo Messías, Pascoal Mocumbi,Laia Montoliu, Montse Morales, Khátia Munguambe, José Muñoz,Ariel Nhacolo, Delino Nhalungo, María Jesús Pinazo, Antoni Plasència,Elizabeth Posadas, Joan Prósper, Llorenç Quintó, Magdalena Ripinga,Joan Rodés,Charfudin Sacoor, David Schellenberg, Elisa Sicuri,Montse Soriano, Elisa Tabangay, Marcel Tanner, Gonzalo Vicente,Jordi Vila and Rafael Vilasanjuan
We would also like to thank all the other people who have directly or indirectly contributed to making this project come together, in particular Àngels Alfonso, Beatriz Fiestas, Pau Rubio, Yolanda Surriel, Raül Toran and Sònia Tomás.
Sadly, some who have collaborated in the work described throughout this book are no longer with us. We wish to remember them here:
Agnès BarbalA gynaecologist at the Maternity of the Spanish Hospital of Tetouan, passed away on the 23rd of August 2000.
Ned HayesAn epidemiologist at CRESIB and ISGlobal, passed away on the 9th of May 2013.
Rosmarie HirtOne of the first people to be recruited by the Hospital Clínic to work in Ifakara (Tanzania), passed away on the 12th of October 2011.
Marcela YñestaA personal assistant to several CRESIB and ISGlobal directors, passed away on the 27th of October 2013

118
Original titlePioneros de la Salud Global: 30 años de historia en el Hospital Clínic de Barcelona© ISGlobal
Author and translatorOlivia Blanchard
Copy editorAnn King
DesignMucho
PrintingLeicrom
With the collaboration of:
30 Years of History in the Hospital Clínic de Barcelona
Pioneers in Global Health
In the nineteen eighties, Spain was just starting to build a new democracy and look beyond its own borders. Cases of tropical disease in this country were the exception. Today, three decades later, people are travelling more than ever and diseases once only encountered in faraway places are making an appearance in our consulting rooms.
The Hospital Clínic de Barcelona pioneered the treatment of tropical diseases in Spain, starting with the creation in 1984 of the Tropical Medicine Unit. Since then, the Hospital has gained a solid reputation in the field, not only in terms of clinical care, but also in training and scientific research.
This book commemorates the Hospital Clínic’s thirty years of work in global health. Through the memories and experiences of the more than fifty people interviewed, the narrative gives an account of the journey travelled so far. The book is a tribute to everything that has been achieved and to all those who have made these achievements possible.
With the collaboration of: