pilot study of waterpipe tobacco smoking among us muslim college students
TRANSCRIPT

ORI GIN AL PA PER
Pilot Study of Waterpipe Tobacco Smoking Among USMuslim College Students
Cynthia L. Arfken • Wahiba Abu-Ras • Sameera Ahmed
� Springer Science+Business Media New York 2014
Abstract Waterpipe smoking is common among the young in Muslim-majority countries
despite recent Islamic rulings on tobacco. US Muslim college students, especially immi-
grants, may be at high risk for smoking, but information is lacking. In this pilot study,
respondent-driven sampling was used to sample 156 Muslim college students. Waterpipe
smoking was common (44.3 %). Leading motivations to smoke were social and perceived
low tobacco harm. Independent risk factors among the Muslim students were perception
that friends and other students smoked, and ever drank alcohol. Personal belief that
waterpipe smoking is prohibited in Islam was not significant. This pilot suggests that
Muslim students are at high risk for waterpipe smoking and more definitive studies are
needed.
Keywords Waterpipe smoking � Muslim � College students � Religiosity � Social
influences
Introduction
Waterpipe smoking (also known as Hookah) is centuries-old nicotine delivery system from
the Middle East and South Asia. Unlike cigarette smoking, waterpipe smoking often occurs
in a social context where the waterpipe is shared with family or friends. Waterpipe use is
C. L. Arfken (&) � S. AhmedDepartment of Psychiatry and Behavioral Neurosciences, Wayne State University, 3901 ChryslerService Drive, Ste 1B, Rm 156, Detroit, MI 48201, USAe-mail: [email protected]
W. Abu-RasSchool of Social Work, Adelphi University, Garden City, NY, USA
S. AhmedFamily and Youth Institute, Canton, MI, USA
123
J Relig HealthDOI 10.1007/s10943-014-9871-x

on the increase worldwide (Maziak 2011), particularly among young people residing in
Muslim-majority countries (Akl et al. 2011). In the USA, waterpipe smoking is growing in
popularity among college students with a lifetime prevalence ranging from 15 to 48 %
(Grekin and Ayna 2012; Eissenberg et al. 2008; Primack et al. 2008; Sutfin et al. 2011).
The high prevalence in Muslim-majority countries and recent increase in the USA is a
health concern as waterpipe smoking has been associated with harmful effects from both
the acute and chronic exposure to tobacco smoke (Akl et al. 2010). These harmful effects
include lung cancer, respiratory illness, and low birth weight. Other diseases may also be
associated with its use, but establishing the link to waterpipe smoking is complicated
because people who engage in waterpipe smoking are also more likely to smoke cigarettes
(Eissenberg et al. 2008; Smith et al. 2011) and/or drink alcohol (Jarrett et al. 2012; Sutfin
et al. 2011).
To address the growing epidemic of waterpipe smoking, effective interventions are
needed. These interventions, in turn, can be tailored based upon reported motivations for
waterpipe smoking, and the identification of risk and protective factors for it. Such
interventions have to be sensitive to religious affiliation to be effective. Currently, there is
a lack of information about motivations and risk factors for waterpipe smoking among
Muslim college students in the USA
In Muslim-majority countries, there is a high exposure to tobacco from cigarettes and
waterpipe smoking (Eriksen et al. 2012). To reduce the harmful effects, tobacco use has
been declared prohibited by many Islamic scholars due to Islam’s injunction to avoid
harming oneself (El Awa 2004, 2008). However, one study in rural Egypt found men more
likely to believe cigarette smoking was prohibited than waterpipe smoking (Singh et al.
2012). Although it is only one study, it suggests the need to clarify these rulings as well as
increase awareness of the negative health effects of waterpipe smoking among Muslims.
A recent review of waterpipe smoking among US college students highlighted that Arab
American students had a higher prevalence than other students (Grekin and Ayna 2012).
The higher prevalence among Arab American students may reflect cultural acceptance of
waterpipe smoking or even viewing the practice as part of their cultural identify. However,
it is also possible that the higher prevalence is due to other factors. Arab American students
differ by religious affiliation (i.e., there are Christian Arab American students and Muslim
Arab American students) and nativity (i.e., there are Arab Americans students born in the
USA and Arab American students born in other countries). If there is a difference in
prevalence by nativity, the difference in prevalence may be due to differences in accul-
turation between groups of immigrant Arab American students. However, the review and
original articles did not provide information on religious affiliation, nativity, or accultur-
ation among immigrant students that may inform public health interventions.
Motivations for Waterpipe Smoking
Motivations for waterpipe smoking in the general US college student population include
social acceptability and perception that it is less harmful or less addictive than cigarettes
(Eissenberg et al. 2008). Another motivation for waterpipe smoking not explored in US
studies may be cultural identity. One study reported that students of Arab heritage (the
study did not state if they were Muslim or Christian) identified waterpipe smoking as part
of their culture (Roskin and Aveyard 2009). As waterpipe smoking originated from the
Middle East and South Asia, it is possible that students of South Asian heritage would also
identify waterpipe smoking as part of their culture. Thus, potential motivators for Muslim
J Relig Health
123

US college students for waterpipe smoking may include cultural identity. If it is a common
motivation, public health interventions would need to address cultural identification.
Risk and Protective Factors
Identified risk factors for waterpipe smoking include younger age, male gender, white race
(Primack et al. 2013), cigarette smoking and alcohol use (Akl et al. 2011; Jarrett et al.
2012), and family and friends’ waterpipe smoking. In contrast, protective factors against
waterpipe smoking have not been identified. Borrowing from the substance abuse litera-
ture, protective factors against waterpipe smoking may include academic achievement
(Giovino 2002), religiosity (i.e., public actions or personal importance attached to religious
behaviors) (Ford and Hill 2012), and belief that one’s religion prohibits the behavior
(Michalak et al. 2007). Also borrowed from the substance abuse literature, a potential risk
factor for waterpipe smoking is having friends who smoke (Salame et al. 2013). This list of
risk and protective factors is drawn from Bronfenbrenner’s ecological systems theory
(1992) by including the social aspects of family, friends, religious community, and social
environment.
Objectives
The objectives of this study were to determine the prevalence, motivations, and risk/
protective factors for waterpipe smoking among Muslim US college students in a pilot
study as it has never been assessed before. Although waterpipe smoking among Arab
American students (some of whom are Muslims) and Muslim students elsewhere in the
world has been shown to be elevated, there is no information on waterpipe smoking among
Muslim US students. It would also advance our understanding of the association of reli-
gious beliefs and religiosity with waterpipe smoking.
Methods
Participants
Eligible participants were self-identified Muslim undergraduate students who were at least
18 years of age at one Midwestern university. The University is primarily a commuter
campus, located in an urban environment in an area with a large Muslim population. The
number and racial backgrounds of Muslim students at the University are unknown; fur-
thermore, there is no listing of Muslim students at the University from which to sample.
Likewise, there is no national information on characteristics of Muslim college students.
Sampling
Due to the lack of a list of enrolled Muslim students, we turned to a sampling technique
used to recruit samples without traditional sampling frames, namely respondent-driven
sampling. Briefly, respondent-driven sampling was developed to address the challenge of
sampling ‘‘hidden populations’’ of injection drug users (Heckathorn 1997). It has been used
in over 15 countries (Semaan et al. 2009) and online with college students (Wejnert
and Heckathorn 2008). It is based upon social networking with the assumption that if the
J Relig Health
123

chain-referral sampling (such as snowball sampling) was allowed to continue until satu-
ration, all the target population would be included in the final sample. Chain-referral
sampling has a number of known difficulties: A few individuals may be responsible for
most referrals, people with large social networks have a greater pool from which to make
potential referrals and within the chains of referred/referees observations are not inde-
pendent. Respondent-driven sampling differs from chain-referral sampling by restricting
the number of referrals, inverse weighting by size of potential network, and controlling for
dependence between referrals in the analysis. It is extensively used in the HIV literature
and increasingly used in the substance abuse field (e.g., Wang et al. 2007).
Sampling was initiated with officers of Muslim and predominately Muslim student
organizations. The officers were selected for two reasons: We wanted to establish an easily
replicated protocol for future studies and we hoped the officers were respected members of
the Muslim community whose word and referral would be trusted by other Muslim stu-
dents. Prior to participating in the survey, the officers verified they were Muslim. After
completing a 15-min online survey, each officer was emailed a gift certificate and three
codes to pass to other eligible students (i.e., Muslim undergraduate student at the Uni-
versity who was 18 years or older). After each of their coupons was used by an eligible
student to complete the survey, the referring student received another gift certificate
through university email. Sampling continued until 156 students were recruited. Students
were only eligible to participate once. All students indicated that they were Muslim on the
survey. The study was approved by the University Institutional Review Board. Recruitment
occurred from May 2010 to March 2011.
Measures
Demographic questions included racial/ethnic heritage, place of birth and parents’ place of
birth (to categorize the student as first generation, second generation, or later generation),
receipt of scholarship (a crude measure of academic achievement), what language they
predominately thought in (a crude measure of acculturation), marital status, and living
arrangement (e.g., alone or with parents/relatives). For social influences, we asked the
students’ perception of the proportion of Muslims in their current neighborhood and in
their high school using categorical responses of ‘‘almost none,’’ ‘‘some but less than
10 %,’’ ‘‘10–30 %,’’ ‘‘30 % but less than 50 %,’’ and ‘‘50 % or more.’’ To measure the size
of their social network, we asked the number of other Muslim undergraduate students at the
University with whom they had reciprocal knowledge of names and social contact in the
past 2 weeks (in person, phone, text, email, or social media).
Individual questions asked about students’ waterpipe smoking, cigarette smoking, use of
cigars, bidi (a small cigarette popular in India) or snuff, and alcohol drinking for the
periods: (1) ever use, (2) past year use, and (3) past 30-day use. Questions also asked how
many other students, Muslim students, and their friends engage in waterpipe smoking with
response options of ‘‘none,’’ ‘‘some,’’ ‘‘most,’’ and ‘‘almost all or all.’’ Parental attitude
toward and history of ever smoking waterpipe were also queried. Motivations for water-
pipe smoking were adapted from alcohol use motivations questions in the College Alcohol
Survey (Wechsler and Nelson 2008) with the addition of two questions (Part of my culture
and Safer than cigarettes).
Questions on Islam’s stance on using alcohol, cigarettes, or waterpipe (anchored
1 = actively encourages and 5 = prohibits) were asked with a lead-in reassuring the
students that it was not a test and we were interested in their beliefs. Religiosity measures
were also included in the survey. Two measures were from the annual US National Survey
J Relig Health
123

of Drug Use and Health (NSDUH) and one from a study on American Muslim physicians
(Abu-Ras 2013). These religiosity measures were selected for analysis as they measure
importance of belief on behavior (My religious beliefs influence how I make decisions in
my life), publicly observed actions (During the past 12 months how many times did you
attend religious services?), and Islamic-specific (In general, to what extent do you adhere
to the practices of Islam?).
Analysis
Respondent-driven sampling requires specialized software to weight by the inverse of the
social network size and control for dependence within referrals (available at www.
respondentdrivensampling.org). More information about the statistical process can be
obtained at the Web site; it is based on Markov chain and biased network theories.
Adjusted population prevalence and 95 % confidence intervals (CI) were obtained along
with adjusted network size and homophily. The latter measure ranges from 1 when
smokers only refer other smokers and nonsmokers only refer nonsmokers to -1 when
smokers only refer nonsmokers and nonsmokers only refer smokers. Ideally, homophily is
close to zero.
For bivariate and multivariate analyses, we used the unweighted sample. Response
frequencies for individual motivations were calculated only for students with a lifetime
history of waterpipe smoking. For the risk and protective factors analyses, results are
summarized as odds ratios (OR) with 95 % CI. As risk factors may be correlated, multi-
variate logistic regression models with stepwise selection of factors significant in bivariate
analyses were used to detect independent associations with waterpipe smoking. As part of
sensitivity analysis, we also used other selection strategies to assess robustness of results.
One selection strategy was entering religiosity measures followed by demographic or
social factors. Analyses were conducted with both the original coded responses and the
responses dichotomized for ordinal questions. For ease of interpretation, the dichotomized
responses are presented here.
Results
Sample Characteristics
The sample was predominately female (67.9 %) and immigrants with 55.8 % being born
outside the USA (Table 1). Self-reported heritage for the students (whether they were
immigrants or native born) was predominately South Asian (46.8 %) and Arab (35.3 %).
Almost all (91 %) of the sample graduated from US high school with about a third
(38.5 %) of the students reporting that they thought exclusively in English. Most of the
sample (82.1 %) lived with their parents and received a scholarship (60.3 %). At the time
of the survey, 70 % of undergraduates at the university received scholarships.
Prevalence of Waterpipe Smoking
Lifetime waterpipe smoking was reported by almost half (44.3 %; 95 % CI 30.3–63.8 %
after adjustment for sampling technique) of the sample; past 30-day waterpipe smoking
was much less common (10.6 %). Lifetime waterpipe smoking was higher than lifetime
J Relig Health
123
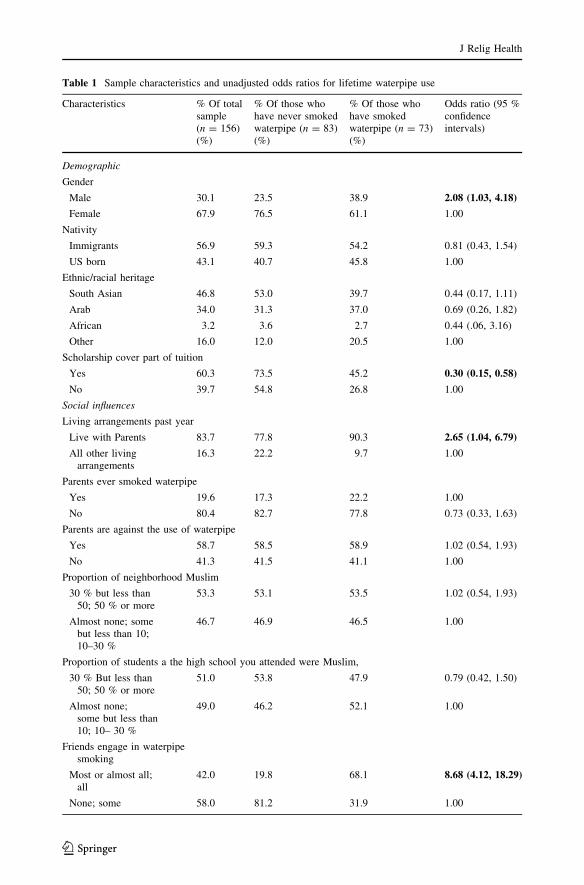
Table 1 Sample characteristics and unadjusted odds ratios for lifetime waterpipe use
Characteristics % Of totalsample(n = 156)(%)
% Of those whohave never smokedwaterpipe (n = 83)(%)
% Of those whohave smokedwaterpipe (n = 73)(%)
Odds ratio (95 %confidenceintervals)
Demographic
Gender
Male 30.1 23.5 38.9 2.08 (1.03, 4.18)
Female 67.9 76.5 61.1 1.00
Nativity
Immigrants 56.9 59.3 54.2 0.81 (0.43, 1.54)
US born 43.1 40.7 45.8 1.00
Ethnic/racial heritage
South Asian 46.8 53.0 39.7 0.44 (0.17, 1.11)
Arab 34.0 31.3 37.0 0.69 (0.26, 1.82)
African 3.2 3.6 2.7 0.44 (.06, 3.16)
Other 16.0 12.0 20.5 1.00
Scholarship cover part of tuition
Yes 60.3 73.5 45.2 0.30 (0.15, 0.58)
No 39.7 54.8 26.8 1.00
Social influences
Living arrangements past year
Live with Parents 83.7 77.8 90.3 2.65 (1.04, 6.79)
All other livingarrangements
16.3 22.2 9.7 1.00
Parents ever smoked waterpipe
Yes 19.6 17.3 22.2 1.00
No 80.4 82.7 77.8 0.73 (0.33, 1.63)
Parents are against the use of waterpipe
Yes 58.7 58.5 58.9 1.02 (0.54, 1.93)
No 41.3 41.5 41.1 1.00
Proportion of neighborhood Muslim
30 % but less than50; 50 % or more
53.3 53.1 53.5 1.02 (0.54, 1.93)
Almost none; somebut less than 10;10–30 %
46.7 46.9 46.5 1.00
Proportion of students a the high school you attended were Muslim,
30 % But less than50; 50 % or more
51.0 53.8 47.9 0.79 (0.42, 1.50)
Almost none;some but less than10; 10– 30 %
49.0 46.2 52.1 1.00
Friends engage in waterpipesmoking
Most or almost all;all
42.0 19.8 68.1 8.68 (4.12, 18.29)
None; some 58.0 81.2 31.9 1.00
J Relig Health
123

alcohol use (9.1 %, 95 % CI 1.8–19.8 %). However, lifetime waterpipe smoking did not
differ from lifetime cigarette use (28.3 %, 95 % CI 13.8–47.7 %) due to the overlapping
95 % CIs. Lifetime history of any tobacco use was 51.3 %. The homophiles were very low
(0.15 for waterpipe smokers and -0.08 for nonsmokers of waterpipe), indicating that
Table 1 continued
Characteristics % Of totalsample(n = 156)(%)
% Of those whohave never smokedwaterpipe (n = 83)(%)
% Of those whohave smokedwaterpipe (n = 73)(%)
Odds ratio (95 %confidenceintervals)
Undergraduate students engage in waterpipe smoking
Most or almost all;all
57.2 43.2 73.2 3.60 (1.81, 7.14)
None; some 42.8 56.8 26.8 1.00
Substance use
Lifetime alcohol use
Yes 8.3 2.4 15.1 7.19 (1.54, 33.60)
No 91.7 97.6 84.9 1.00
Lifetime cigarette use
Yes 22.4 6.0 41.1 3.31 (1.20, 9.15)
No 77.6 94.0 58.9 1.00
Religiosity
During the past 12 months how many times did you attend religious services?
25 times or more 34.6 34.6 34.7 1.01 (0.52, 1.96)
0; 1–2; 3–5;or 6–24
65.4 65.4 65.3 1.00
In general, to what extent do you adhere to the practices of Islam?
All of the time 28.8 34.6 22.2 0.54 (0.26, 1.11)
Never; rarely;sometimes; mostof the time
71.2 65.4 77.8 1.00
My religious beliefs influence how I make decisions in my life
Strongly agree 59.5 66.7 51.4 0.53 (0.28, 1.02)
Strongly disagree;disagree; agree
40.5 33.3 48.6 1.00
How do you believe your religion views each of the following: waterpipe
Prohibit 26.1 29.6 22.2 0.68 (0.33, 1.41)
Activelyencourages;supports; nostance;discourages
73.9 70.4 77.8 1.00
Frequencies not adjusted using respondent-driven sampling software. Similar results were obtained usingordinal responses for variables with multiple response categories. Statistically significant (at .05 level) oddsratios bolded
J Relig Health
123
referrals were made independent of smoking status. Adjusted mean social network sizes
were higher for ever smokers (11.2) than for never smokers (9.6).
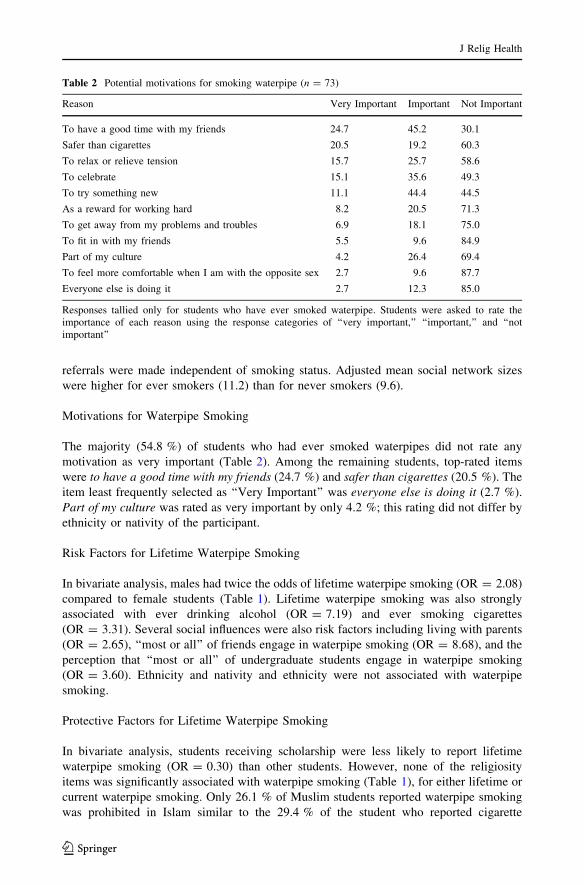
Motivations for Waterpipe Smoking
The majority (54.8 %) of students who had ever smoked waterpipes did not rate any
motivation as very important (Table 2). Among the remaining students, top-rated items
were to have a good time with my friends (24.7 %) and safer than cigarettes (20.5 %). The
item least frequently selected as ‘‘Very Important’’ was everyone else is doing it (2.7 %).
Part of my culture was rated as very important by only 4.2 %; this rating did not differ by
ethnicity or nativity of the participant.
Risk Factors for Lifetime Waterpipe Smoking
In bivariate analysis, males had twice the odds of lifetime waterpipe smoking (OR = 2.08)
compared to female students (Table 1). Lifetime waterpipe smoking was also strongly
associated with ever drinking alcohol (OR = 7.19) and ever smoking cigarettes
(OR = 3.31). Several social influences were also risk factors including living with parents
(OR = 2.65), ‘‘most or all’’ of friends engage in waterpipe smoking (OR = 8.68), and the
perception that ‘‘most or all’’ of undergraduate students engage in waterpipe smoking
(OR = 3.60). Ethnicity and nativity and ethnicity were not associated with waterpipe
smoking.
Protective Factors for Lifetime Waterpipe Smoking
In bivariate analysis, students receiving scholarship were less likely to report lifetime
waterpipe smoking (OR = 0.30) than other students. However, none of the religiosity
items was significantly associated with waterpipe smoking (Table 1), for either lifetime or
current waterpipe smoking. Only 26.1 % of Muslim students reported waterpipe smoking
was prohibited in Islam similar to the 29.4 % of the student who reported cigarette
Table 2 Potential motivations for smoking waterpipe (n = 73)
Reason Very Important Important Not Important
To have a good time with my friends 24.7 45.2 30.1
Safer than cigarettes 20.5 19.2 60.3
To relax or relieve tension 15.7 25.7 58.6
To celebrate 15.1 35.6 49.3
To try something new 11.1 44.4 44.5
As a reward for working hard 8.2 20.5 71.3
To get away from my problems and troubles 6.9 18.1 75.0
To fit in with my friends 5.5 9.6 84.9
Part of my culture 4.2 26.4 69.4
To feel more comfortable when I am with the opposite sex 2.7 9.6 87.7
Everyone else is doing it 2.7 12.3 85.0
Responses tallied only for students who have ever smoked waterpipe. Students were asked to rate theimportance of each reason using the response categories of ‘‘very important,’’ ‘‘important,’’ and ‘‘notimportant’’
J Relig Health
123

smoking was prohibited in Islam. Believing that waterpipe smoking was prohibited in
Islam was not a protective factor against lifetime waterpipe use (OR 0.68, 95 % CI
0.33–1.41), even when analysis was limited to those reporting high religiosity. In
exploratory analysis, the only demographic or substance use variable that was statistically
associated with believing that Islam prohibited waterpipe smoking was reporting that both
parents discourage waterpipe smoking (p \ .001).
Multivariate Analysis
The findings from the bivariate analysis were then examined in multivariate analysis.
Independent risk factors for lifetime waterpipe smoking were (1) ‘‘most or all’’ of friends
engage in waterpipe smoking, (2) ‘‘most or all’’ of undergraduate students engage in
waterpipe smoking, and (3) ever use of alcohol (Table 3). The other risk factors identified
in bivariate analysis were not statistically associated in multivariate analysis. No protective
factors were significant in the multivariate analysis. No protective factors were identified
when we conducted the analyses using current waterpipe smoking. Ethnicity, nativity, male
gender, or where the student lived were not statistically significant independent risk factor
for waterpipe smoking among Muslim college students.
Discussion
In this pilot study, we estimated the prevalence, motivations, and risk/protective factors for
waterpipe smoking among Muslim US college students, a group that potentially could be at
high risk due to elevated prevalence among young people in Muslim-majority countries
and increasingly in the USA. We found that lifetime prevalence of waterpipe smoking was
alarmingly high and that specific religious beliefs on waterpipe and religiosity were not
protective factors. Furthermore, specific motivations for waterpipe use focused more on
social aspects and much less on cultural issues. Finally, although many Islamic scholars
have ruled that tobacco is prohibited in Islam, few of the Muslim students reported that
tobacco, whether in cigarettes or in waterpipes, was prohibited in Islam.
Table 3 Independent risk factors for lifetime waterpipe smoking
Risk factor Adjusted odds ratios(95 % confidence interval)
Alcohol use
Ever 8.03 (1.47–43.81)
Never 1.00
Friends engage in waterpipe smoking
Most; almost all; all 6.62 (3.00–14.6)
None; some 1.00
Undergraduate students engage in waterpipe smoking
Most; almost all; all 2.34 (1.05–5.25)
None; Some 1.00
Variables initially entered into model included variables identified in bivariate analysis as significant(bolded odds ratios in Table 1). Unadjusted for sampling strategy
J Relig Health
123

In this pilot, we found that waterpipe smoking was widespread. Even among students
who rated religious beliefs as very important and believed that tobacco was prohibited by
Islam, waterpipe smoking was found. This result may reflect the highly social context of
smoking where the waterpipe is shared with family and friends. Social influences on
waterpipe smoking have also been found in the general population of US college students
(Eissenberg et al. 2008; Primack et al. 2013; Smith-Simone et al. 2008) and in Muslim-
majority countries for alcohol use (Salame et al. 2013).
Independent of social factors, alcohol use among the Muslim students was a risk factor
for waterpipe smoking. Although our sample did not examine whether alcohol use or
waterpipe smoking occurred first, almost every participant who ever drank alcohol had also
engaged in smoking waterpipe. For that reason, alcohol use was identified as a risk factor
for waterpipe smoking in this sample. However, tailoring anti-smoking interventions to
target alcohol use would miss the majority of Muslim students who ever smoked waterpipe
as they never drank alcohol. In the general student population where alcohol use is much
higher, some studies examined alcohol use and found it a significant risk factor for
waterpipe smoking (Jarrett et al. 2012; Sutfin et al. 2011).
Our pilot findings support that some of the Muslim students appeared misinformed
about the health hazards of waterpipe smoking, a gap also found in the general population
of students (Nuzzo et al. 2012; Primack et al. 2013). Knowledge of harm by itself may not
influence waterpipe smoking (Nuzzo et al. 2012), but it is important to build support for
any restrictions on the behavior similar to what occurred with cigarette smoking.
After controlling for social influences, protective factors against waterpipe smoking
were not identified in this sample. Although some Islamic scholars have declared tobacco
use prohibited, few of the Muslim students in this study reported believing that waterpipe
smoking was prohibited by Islam. In contrast to findings from the study of rural Egyptian
men (Singh et al. 2012), the students in our sample were equally likely to report
waterpipe and cigarette smoking as prohibited. However, it was a minority of the stu-
dents who reported tobacco was prohibited. Even with analysis is restricted to students
who rate religious beliefs as highly important, there was no association between religious
belief on waterpipe smoking and actual waterpipe smoking. This general lack of asso-
ciation was not due to students’ mismarking religiosity questions, as we have previously
reported strong associations between the religiosity measures and alcohol use (Arfken
et al. 2013). Instead, the lack of an association may reflect the social aspects of
waterpipe smoking.
Limitations
Our pilot study was limited by the reliance on self-report without laboratory confirmation
and small sample size. Additionally, the sampling was conducted at one university and
needs replication. It is possible that we never reached Muslim students who had little
interactions with formal student organizations. Finally, the survey was cross-sectional and
cannot address changing motivations or patterns of use.
However, recruitment showed no pattern with the individual’s experience of water-
pipe smoking (i.e., homophiles were near zero), as is desired in respondent-driven
sampling. These low homophiles for waterpipe smoking are in contrast to the higher
homophiles for alcohol use where students who drank tended to recruit their friends who
drank and students who abstained tend to recruit other abstainers (Arfken et al. 2013).
The lack of such a recruitment pattern for waterpipe smoking may reflect greater social
acceptance or less social stigma of the behavior among the Muslim students compared to
J Relig Health
123

alcohol use. If this is true, it would suggest that underreporting of waterpipe smoking
due to stigma was low.
New Contributions to the Literature
Waterpipe smoking was common and independently associated with social influences and
alcohol use in this sample of Muslim predominately immigrant college students. Religious
belief on tobacco, religiosity, ethnicity, and nativity did not significantly impact the
prevalence of waterpipe smoking within the sample of Muslim students. Although a cul-
turally distinct minority in the USA, few Muslim students rated cultural identification as a
motivation for waterpipe smoking. This pilot study shows it is feasible to sample Muslim
college students on tobacco use, but a larger more definitive study is needed to make public
health intervention recommendations.
Acknowledgments This work was supported by a grant from the Institute on Social Policy and Under-standing (www.ispu.org).
References
Abu-Ras, W. (2013). American Muslim physicians’ public role post-9/11 and minority communityempowerment: Serving the underserved. Journal of Immigrant and Refugee Studies, 11, 1–23.
Akl, E. A., Gaddam, S., Gunukula, S. K., Honeine, R., Jaoude, P. A., & Irani, J. (2010). The effects ofwaterpipe tobacco smoking on health outcomes: A systematic review. International Journal of Epi-demiology, 39, 834–857.
Akl, E. A., Gunukula, S. K., Aleem, S., Obeid, R., Jaoude, P. A., Honeine, R., et al. (2011). The prevalenceof waterpipe tobacco smoking among the general and specific populations: A systematic review. BMCPublic Health, 11, 244.
Arfken, C. L., Ahmed, S., & Abu-Ras, W. (2013). Respondent-driven sampling of Muslim undergraduateU.S. college students and alcohol use: Pilot study. Social Psychiatry and Psychiatric Epidemiology, 48,945–953.
Bronfenbrenner, U. (1992). Ecological systems theory. In R. Vasta (Ed.), Six theories of child development:Revised formulations and current issues (pp. 187–249). London, England: Jessica Kingsley Publications.
Eissenberg, T., Ward, K. D., Smith-Simone, S., & Maziak, W. (2008). Waterpipe tobacco smoking on a U.S.college campus: Prevalence and correlates. Journal of Adolescent Health, 42, 526–529.
El Awa, F. (2004). The role of religion in tobacco control interventions. Bulletin of the World HealthOrganization, 82, 894–894.
El Awa, F. (2008). Tobacco control in the eastern Mediterranean region: Overview and way forward.Eastern Mediterranean Health Journal, 14, S123–S131.
Eriksen, M., Mackay, J., & Ross, H. (2012). The tobacco atlas. Atlanta, GA: American Cancer Society.Ford, J. A., & Hill, T. D. (2012). Religiosity and adolescent substance use: Evidence from the National
Survey on Drug Use and Health. Substance Use and Misuse, 47, 787–798.Giovino, G. A. (2002). Epidemiology of tobacco use in the United States. Oncogene, 21, 7326–7340.Grekin, E. R., & Ayna, D. (2012). Waterpipe smoking among college students in the United States: A
review of the literature. Journal of American College Health, 60, 244–249.Heckathorn, D. (1997). Respondent-driven sampling: A new approach to the study of hidden populations.
Social Problems, 44, 174–199.Jarrett, T., Blosnich, J., Tworek, C., & Horn, K. (2012). Hookah use among U.S. college students: Results
from the National College Health Assessment II. Nicotine & Tobacco Research, 14, 1145–1153.Maziak, W. (2011). The global epidemic of waterpipe smoking. Addictive Behaviors, 36, 1–5.Michalak, L., Trocki, K., & Bond, J. (2007). Religion and alcohol in the U.S. National Alcohol Survey: How
important is religion for abstention and drinking? Drug and Alcohol Dependence, 16, 268–280.Nuzzo, E., Shensa, A., Kim, K. H., Fine, M. J., Barnett, T. E., Cook, R., et al. (2012). Associations between
hookah tobacco smoking knowledge and hookah smoking behavior among US college students. HealthEducation Research, 28, 92–100.
J Relig Health
123

Primack, B. A., Shensa, A., Kim, K. H., Carroll, M. V., Hoban, M. T., Leino, E. V., et al. (2013). Waterpipesmoking among U.S. university students. Nicotine & Tobacco Research, 15, 29–35.
Primack, B. A., Sidani, J., Agarwal, A. A., Shadel, W. G., Donny, E. C., & Eissenberg, T. E. (2008).Prevalence of and associations with waterpipe tobacco smoking among U.S. university students.Annals of Behavioral Medicine, 36, 81–86.
Roskin, J., & Aveyard, P. (2009). Canadian and English students’ beliefs about waterpipe smoking: Aqualitative study. BMC Public Health, 9, 10.
Salame, J., Barbour, B., & Salameh, P. (2013). Do personal beliefs and peers affect the practice of alcoholconsumption in university students in Lebanon? Eastern Mediterranean Health Journal, 19, 340–347.
Semaan, S., Santibanez, S., Garfein, R. S., Heckathorn, D. D., & Des Jarlais, D. C. (2009). Ethical andregulatory considerations in HIV prevention studies employing respondent-driven sampling. Interna-tional Journal of Drug Policy, 20, 14–27.
Singh, P. N., Neergaard, J., Job, J. S., El Setouhy, M. E., Israel, E., Mohammed, M. K., et al. (2012).Differences in health and religious beliefs about tobacco use among waterpipe users in the rural malepopulation of Egypt. Journal of Religion and Health, 51, 216–225.
Smith, J. R., Edland, S. D., Novotny, T. E., Hofstetter, C. R., White, M. M., Lindsay, S. P., et al. (2011).Increasing hookah use in California. American Journal of Public Health, 101, 1876.
Smith-Simone, S., Maziak, W., Ward, K. D., & Eissenberg, T. (2008). Waterpipe tobacco smoking:Knowledge, attitudes, beliefs, and behavior in two U.S. samples. Nicotine & Tobacco Research, 10,393–398.
Sutfin, E. L., McCoy, T. P., Reboussin, B. A., Wagoner, K. G., Spangler, J., & Wolfson, M. (2011).Prevalence and correlates of waterpipe tobacco smoking by college students in North Carolina. Drugand Alcohol Dependence, 115, 131–136.
Wang, J., Falck, R. S., Li, L., Rahman, A., & Carlson, R. G. (2007). Respondent-driven sampling in therecruitment of illicit stimulant drug users in a rural setting: Findings and technical issues. AddictiveBehaviors, 32, 924–937.
Wechsler, H., & Nelson, T. (2008). What we have learned from the Harvard School of Public HealthCollege Alcohol Study: Focusing attention on college student alcohol consumption and the environ-mental conditions that promote it. Journal of Studies on Alcohol and Drugs, 69, 481–490.
Wejnert, C., & Heckathorn, D. (2008). Web-based network sampling: Efficiency and efficacy of respondent-driven sampling for online research. Sociological Methods & Research, 37, 105–134.
J Relig Health
123