physiology of performance enhancement
TRANSCRIPT

By Adam McKay
ENG 201
7/2/14
Three Omnipresent Performance Enhancing Methods in American Sports Anabolic-Androgenic Steroids (AAS)
- i.e. testosterone, oxymetholone, stanozolone, etc.
Human Growth Hormone (HGH)
“Blood Doping”- i.e. recombinant human erythropoietin (rHuEPO), autologous and allogeneic blood transfusions, and hemoglobin-based oxygen carriers (HBOC’s)

History of Performance Enhancement Ancient Use – Some historians believe that the Greeks used
experimental herbal concoctions and ate a lot of meat prior to competitions1; ancient Roman gladiators used substances like strychnine and hydromel in order to stave off fatigue and increase speed2.
19th Century Use – Athletes have used stimulants such as strychnine, caffeine, and cocaine since the 1800’s3.
Modern Use – Steroid use has been an acknowledged problem in America since the 1960’s. Blood doping became a major concern in sports after the creation of commercial rHuEPO in 1989. HGH became major concern by 2010.

Stimulants in Sports Amphetamine is the most notorious stimulant in athletics
today
- The MLB is the most infamous institution of amphetamine use
– due to the penalties implemented for amphetamine use, 8-10% of MLB players receive therapeutic use exemptions (TUE’s) in order to use them without penalty (compared to the 4.4% of the general population with symptoms appropriate for amphetamine use3)

Anabolic-Androgenic Steroids (AAS)AAS are probably the most recognized means of performance enhancement, and use has evolved over time in order to escape detectionThese compounds act on one intracellular receptor mostly found in the reproductive tract, but also present in non-reproductive cells in bone, skeletal muscle, the liver, and adipocytes (fat cells)4
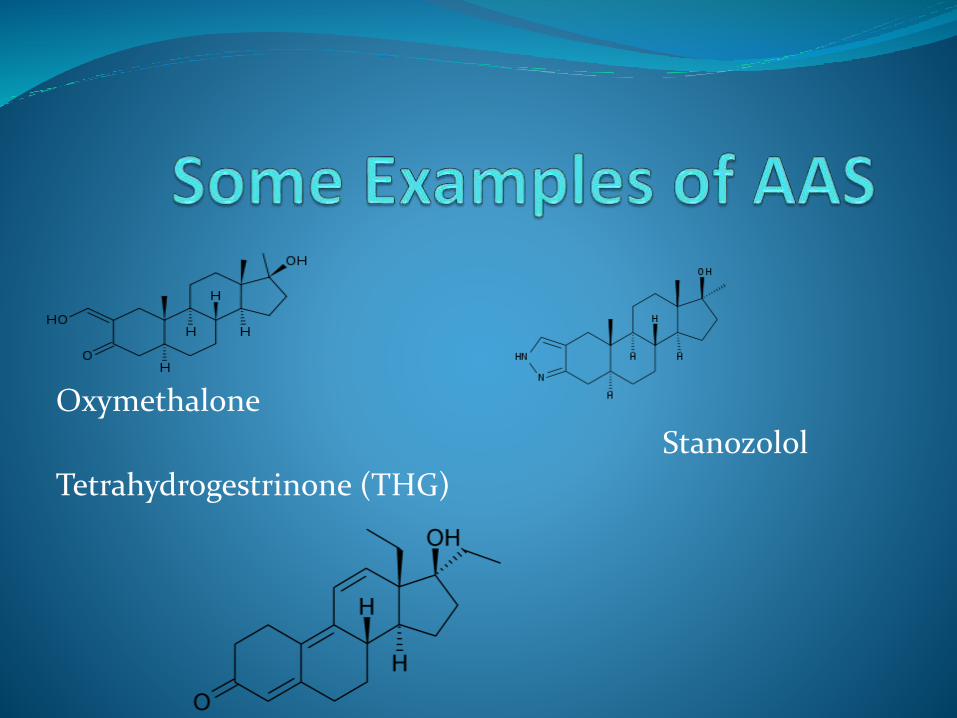
Oxymethalone
Stanozolol
Tetrahydrogestrinone (THG)
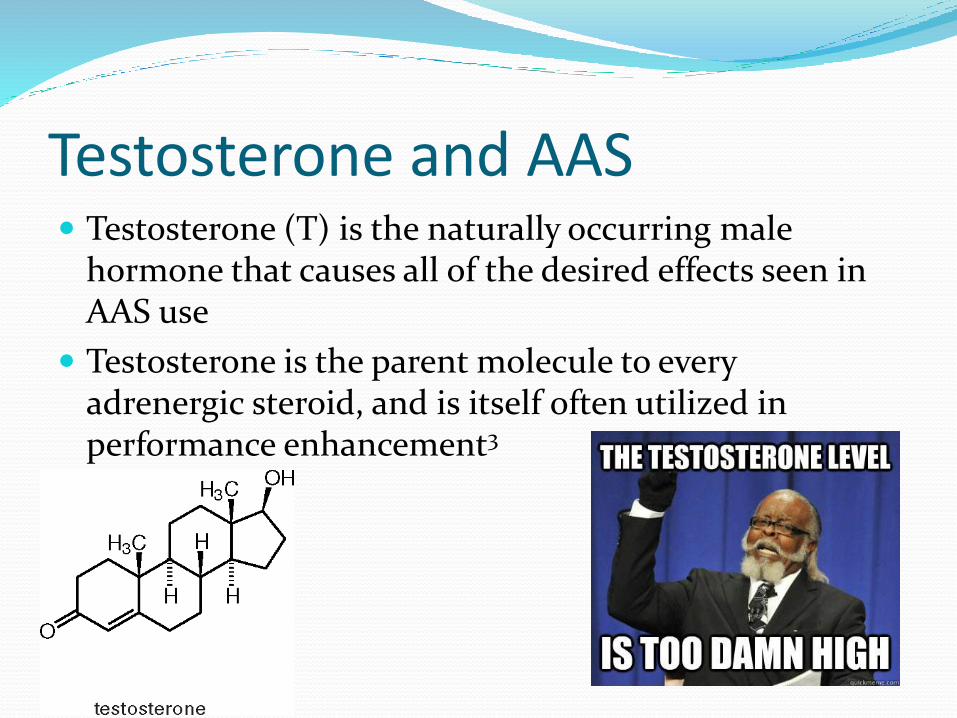
Testosterone and AAS Testosterone (T) is the naturally occurring male
hormone that causes all of the desired effects seen in AAS use
Testosterone is the parent molecule to every adrenergic steroid, and is itself often utilized in performance enhancement3

Metabolic Effects of AAS AAS have been shown to increase EPO activity in both
mice and humans, in vivo and in vitro
Molinari and Neri showed that the administration of the AAS oxymetholone in eight healthy volunteers increased the concentration of 2,3-diphosphglycerate (2,3-DPG), which has an important role in the binding of hemoglobin to oxygen4

Anabolic Effects of AAS In bone, AAS stimulate osteoblast proliferation, bone
matrix protein production, and the syntheses of growth factor and cytokines4
Steroids and testosterone decrease muscle and protein breakdown while encouraging lipolysis (fat break-down) in part due to their nitrogen-retaining properties

Detecting AAS and Testosterone AAS are typically detected through hyphenated mass
spectrometry, a method that combines chromatographic techniques with spectroscopic techniques to more accurately identify a compound5
Synthetic T is identified through the ratio of T to epitestosterone (E) – an isoform of inactive T only made through natural T and not through synthetic T. The current threshold for the T:E ratio is 33.
Risks and Adverse Effects of Steroids Serious side effects of chronic AAS use include
cholestatic jaundice, peleosis hepatitis, hepatic cancer, masculinization in women and children (acne, deepening voice, clitoral enlargement, etc.), and simultaneously raising low-density lipoproteins (“bad” cholesterol) while lowering high-density lipoproteins (good” cholesterol), among others4

Adverse Effects Cont. Jaundice Peliosis Hepatitis

Benefits of AASAAS have become widely used in the
treatment of muscle wasting disorders, damaged myocardium from heart failure, growth retardation and malnutrition, bone marrow failure syndromes, end-stage renal disease, and angioneurotic edema4

Human Growth Hormone Recently, HGH for performance enhancement in
athletics has become a problem
HGH is a natural occurring hormone, arising from the anterior pituitary, that has a wide swath of uses in the human body – in children it aids in growth and development; while it helps break down fat, build lean muscle, maintain immunity, and repair tissue throughout life6

HGH Structure

HGH in Athletics HGH was listed in the 2010 Prohibited List
HGH use can start as early as adolescence, with a survey showing that 5% of American 10th grade boys had used HGH in the past
A web-based study showed that 25% of AAS users also used HGH6
Detection of HGH Urinalysis is ineffective at detecting HGH, as its
concentrations in urine are less than 1% their conc. in blood
A test was developed that can detect the 22 kDaisoform of the hormone, however, it was found ineffective at detecting HGH in athletes. This could be due to the relatively fast excretion of HGH (24-36 hr)3

Dangers of HGH Use HGH use creates significant fluid retention, which can
cause feelings of “pins and needles”, carpel tunnel syndrome, and arthralgias
A possibly serious complication of long term HGH use is acromegaly, which often presents with hypertrophic but weaker muscles, hypertension and other cardiac problems, joint pathology, and an increased risk of diabetes and cancer6

Acromegaly

Results of HGH Use Some studies suggest that HGH does not even enhance
performance much at all
The increase in lean body mass associated with HGH comes mostly in the form of fluid retention, and most of those who experience fat loss and muscle gain are those with HGH deficiency to begin with6
However, one study by Meinhardt et al juxtaposed these results with their own data showing that HGH therapy increased sprint capacity by 3.9%3

Blood Doping Three different types of blood doping are primarily
engaged in athletics – the use of rHuEPO, autologous (or rarely allogeneic) blood transfusions, and hemoglobin-based oxygen carriers

Human Recombinant Erythropoeitin The most common form of blood-doping, rHuEPO
must be used consistently (i.e. injections every 2-3 days over a 4 week period) in order to see its full benefits
Many different forms of rHuEPO already exist in the market or are currently being created/researched, including the α-, β-, and ω- isoforms as well as gene-activated and EPO and adeno-associated viral vectors able to deliver the EPO gene7
Blood Transfusions Blood transfusions offer an immediate increase in red
blood cells (RBC’s) and oxygen-carrying capacity
The newly injected RBC’s are exactly like any other RBC’s, and so they are alive for 120 days
The biggest drawback to this method is inconvenience, as the drawn RBC’s must be stored in a container at no more than 4 degrees Celsius in order to survive long enough to be of use7

Hemoglobin-Based Oxygen Carriers HBOC’s are synthesized from hemoglobin taken from
bovine or human sources, which is sterilized, cross-linked, modified, and micro-encapsulated to stabilize the molecule and provide a basis for a range of subsitutes
These compounds have the advantage of causing no toxicity
The major disadvantage of this method is the rapidity of excretion – usually taking place in 12-24 hours7

Detection of Blood Doping Currently there is no accurate way of detecting blood
transfusions directly
HBOC’s are relatively new, and no method of accurately detecting them is around either7
rHuEPO can be detected using a test that involves the use of chemiluminescence and electric fields in order to separate different isoforms of the compound along a gradient3

Adverse Effects of Blood Doping Blood doping increases blood volume within a
constant container, thus increasing viscosity – this has been shown to cause problems ranging from hypertension to increased platelet reactivity to general inflammation
One study described how EPO use needed to be discontinued in breast cancer patients due to an increase in thrombotic events8

Is Blood Doping Worth It? A review by Jules Heuberger et al showed little
scientific evidence that blood doping, particularly with EPO, objectively boosts performance in cycling
Many studies reviewed in this publication were flawed, as many only tested moderately trained cyclists with untrained controls
EPO was found to increase hematocrit and VO2max, but there is no evidence that this improves performance8

Legal and Ethical Concerns Numerous organizations across the globe exist solely
to condemn, prohibit, and discourage the use of performance enhancing drugs in sports
Players can and often are sued when it is discovered that they have been “doping”
The major ethical problem of these drugs comes in the destruction of any sort of fairness – rules are in place for the purpose of leveling the playing field

Bibliography 1) Bowers, L.D. “Athletic Drug Testing," Clinics in Sports Medicine, Apr. 1, 1998 2) Aziz, R.A. “History of Doping," Presented at the WADA Asia Education
Symposium, Aug. 29, 2006 3) Werner, T.C.; Hatton, Caroline “Performance Enhancing Drugs in Sports”
Journal of Chemical Education, 88, 34-41, 2011 4) Shahidi, N. “A Review of the Chemistry, Biological Action, and Clinical
Applications of Anabolic-Androgenic Steroids” Clinical Therapeutics, 23, 2001 5) Patel, K. “Introduction to Hyphenated techniques and their Application in
Pharmacy” Pharmaceutical Methods, 1, 2-13, 2010 6) Birzniece, V.; Nelson, A.; Ho, K. “Growth Hormone and Physical
Performance” Trends in Endocrinology and Metabolism, 22, 2011 7) Ashenden, M. “A Strategy to Deter Blood Doping in Sport” Haematologica,
87, 225-234, 2002 8) Heuberger, J.; Tervaert, J.M.C. “Erythropoeitin Doping in Cycling: Lack of
Evidence for Efficacy and a Negative Risk-Benefit” British Journal of Clinical Pharmacology, 75, 1406-1421, 2012