physiological mechanisms - nsdl at niscair:...
TRANSCRIPT

Physiological Mechanisms
Hormonal Control
Dr Smita Bhatia BP-5, II floor,
Shalimar Bagh (West) Delhi 110088
Contact: 27483738 Email: [email protected]
1

Learning objectives
Chemical nature of hormonesTransport of hormonesMechanism of hormone action Hormone interactionsControl of hormone secretionClearance of hormonesMajor endocrine glands, their secretions and disorders
Hypothalamic-hypophyseal axisThyroid glandParathyroid glandsAdrenal glandsPancreatic isletsGonads and placenta ThymusPineal gland
Other endocrine tissues
In addition to other homeostatic mechanisms of the body, one of the two major regulatory systems of the body is the endocrine system (the other being the nervous system). This system comprises the endocrine glands that release their secretions, called hormones, into the blood stream which transports it to the various target organs on which these hormones act to activate, inhibit or, modify certain functions. Hormones are released into the blood stream rather than directly reaching the target organs because these glands have no ducts (ductless glands) to convey their secretions (also because there could be many target organs for a single hormone so it would not be possible to take these secretions to each and every organ by means of ducts).
Why do hormones act on certain specific organs and not on others?
This is due to the presence of receptors in/on the target cell. These receptors are protein, or glycoprotein molecules, which can bind to the hormone. The location of receptors differs within a cell for different types of hormones. These receptors may be present:
• On the cell: For the protein peptide and catecholamine hormones.
• In the cytoplasm of the cell: Steroid hormones (since these hormones can readily enter a cell).
• In the cell nucleus: Thyroid hormones (as these hormones can readily enter the cell because of their lipid soluble nature) where they directly affect the genes.
A specific change occurs after the hormone binds to the receptor (see mechanism of hormone action). The number of receptors on the cell surface is regulated by the concentration of the circulating hormone. If the concentration is very high the number of receptors decreases so
2

that the cell becomes less sensitive to the hormone. This is known as down-regulation. If the concentration of the hormone becomes low, the number of receptors increases to increase the sensitivity of the cell to the hormone. This is known as up-regulation.
C
H
PP
Differences between the two major regulatory systems of the body—the endocrine and the nervous system
Nervous system Endocrine system • Neurotransmitters are released which • Hormones are released which can be
act locally • Act on muscle cells, gland cells and
other neurons • Effect of neurotransmitters occurs
within a short span of time (msec) • Effect lasts for a short time (msec)
carried anywhere in the body • Act on a variety of cells • Effect of hormones may take seconds
to hours to days to occur • Effect may last for a long time (seconds
to days)
Functions of hormones
• Help to regulate the chemical composition and volume of the various components of the body, e.g. plasma, interstitial fluid.
• Help regulate the metabolism and energy balance.
• Help regulate the contraction of smooth and cardiac muscle fibres.
• Help regulate glandular secretion and some immune system activities.
• Control growth and development.
• Regulate the functioning of the reproductive system.
• Help establish circadian rhythms.
• Help regulate the interaction between the environment and the body.
hemical nature of hormones
ormones are of different types:
rotein or peptide hormones. These are made up of amino acids. They are water soluble. eptides are made up of 3 to 49 amino acids. e g. oxytocin and insulin. Protein hormones are
made up of 50 to 200 amino acids e.g., thyroid stimulating hormone (TSH), follicle stimulating hormone (FSH). These are produced as biologically inactive precursor molecules (pre-prohormones) by the rough endoplasmic reticulum of the gland cell. These pre-prohormones are then cleaved into prohormones which are also biologically inactive. Prohormones are then packaged into vesicles as hormones by the Golgi body. These vesicles
3
are stored in the cytoplasm near the plasma membrane from where they are secreted by exocytosis on an appropriate stimulus.
Steroid hormones. These hormones are derived from cholesterol e.g., testosterone, cortisol, progesterone. They are lipid soluble. These are not stored in the cytoplasm but are synthesized from cholesterol when needed and are secreted directly by passing through the plasma membrane as they are lipid soluble.
Biogenic amines. They are derived from amino acids. They are of different types:
• Thyroid hormones and catecholamines. Thyroxine (T4) and triiodothyronine (T3) are secreted by the thyroid gland. Catecholamines include epinephrine and non-epinephrine secreted by the adrenal medulla and dopamine secreted by the hypothalamus and other brain cells. They are all derivatives of the amino acid tyrosine. Thyroxine is synthesized in the thyroid follicles where they are stored with thyroglobulin (a glycoprotein). When needed, thyroxin is released from the thyroglobulin into the blood where it combines with the thyroxin-binding globulin. Catecholamines are stored in the vesicles in the cytoplasm which are released by exocytosis when needed. Catecholamines are water soluble while thyroid hormones are lipid soluble because they are iodinated.
• Histamine secreted by the mast cells is derived from amino acid histidine.
• Serotonin (or 5-hydroxytrptamine, 5-HT) and melatonin. Both are derived from the amino acid tryptophan. Serotonin is secreted by certain brain cells and melatonin is secreted by the pineal gland.
• Eicosanoids. These are different types of hormones derived from the fatty acid arachidonic acid containing 20 carbon atoms. Eicosanoids include prostaglandins (like PGF2α), prostacyclins and leukotrienes. These are water-soluble.
• Nitric oxide. Though it is a gas, it is produced as a hormone as well as a neurotransmitter. It is lipid soluble.
Transport of hormones The secretion, transport and mechanism of action of these hormones depends on their polar or non-polar nature i.e., whether they are water soluble or lipid soluble.
The water-soluble hormones do not need any carrier molecules in the plasma, where they can circulate freely in the aqueous medium. But lipid-soluble hormones cannot be transported as free molecules in the aqueous plasma and are transported by carrier proteins. In addition to transporting these hormones these carrier proteins also,
• Prevent filtration of small lipid hormones through the glomerulus in the kidneys thus increasing their half-life.
• Provide a readily available stock of these hormones circulating in the blood.
4

Mechanism of hormone action
Lipid soluble hormones
Lipid-soluble hormones bind to the receptors present inside the target cells because these hormones can cross the plasma membrane.
Sequence of events of the action of a lipid molecule Lipid hormone is released from the blood into the interstitial space
It crosses the plasma membrane of the cell and binds to specific receptors inside the cell
The hormone-receptor complex turns certain specific genes on or off.
Synthesis of certain specific mRNA (and hence specific
5
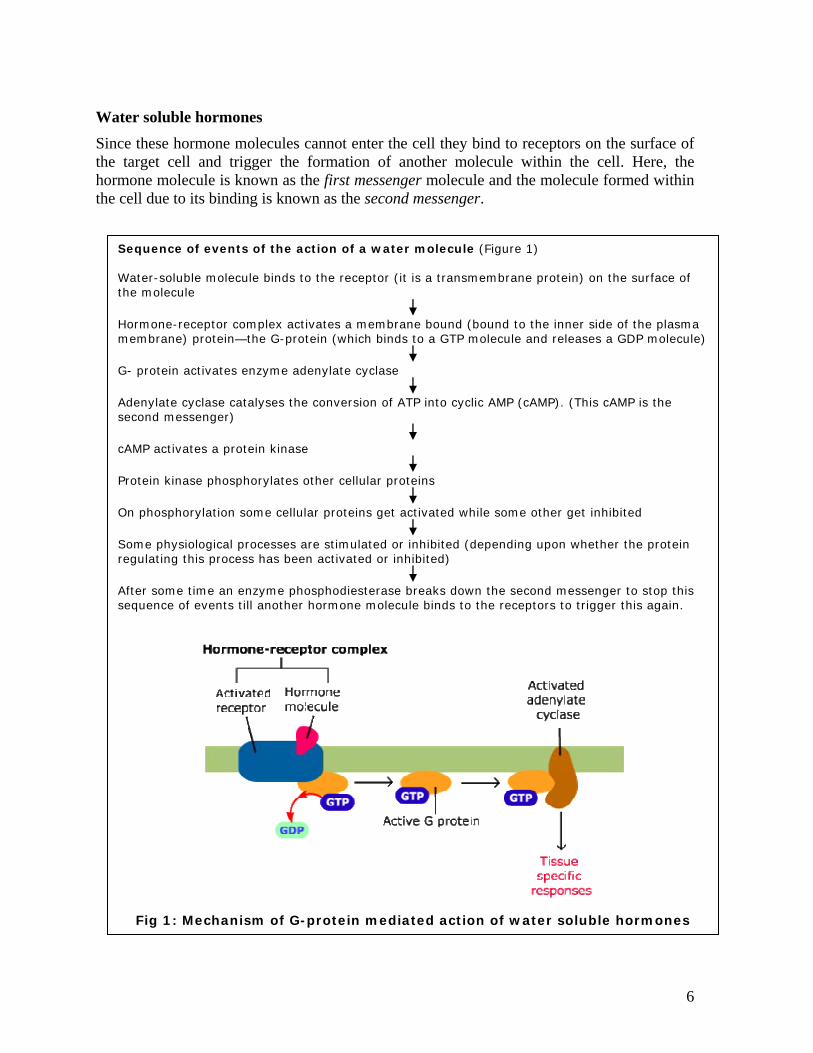
Water soluble hormones Since these hormone molecules cannot enter the cell they bind to receptors on the surface of the target cell and trigger the formation of another molecule within the cell. Here, the hormone molecule is known as the first messenger molecule and the molecule formed within the cell due to its binding is known as the second messenger.
Sequence of events of the action of a water molecule (Figure 1) Water-soluble molecule binds to the receptor (it is a transmembrane protein) on the surface of the molecule
Hormone-receptor complex activates a membrane bound (bound to the inner side of the plasma membrane) protein—the G-protein (which binds to a GTP molecule and releases a GDP molecule)
G- protein activates enzyme adenylate cyclase
Adenylate cyclase catalyses the conversion of ATP into cyclic AMP (cAMP). (This cAMP is the second messenger)
cAMP activates a protein kinase
Protein kinase phosphorylates other cellular proteins
On phosphorylation some cellular proteins get activated while some other get inhibited
Some physiological processes are stimulated or inhibited (depending upon whether the protein regulating this process has been activated or inhibited)
After some time an enzyme phosphodiesterase breaks down the second messenger to stop this sequence of events till another hormone molecule binds to the receptors to trigger this again.
Fig 1: Mechanism of G-protein mediated action of water soluble hormones
6

Different protein kinases exist in different cells or within the same cell, while one type of
protein kinase may stimulate an activity by phosphorylating a protein another protein kinase may inhibit another activity by phosphorylating another protein.
In addition to cAMP, other second messengers include cGMP (cyclic guanosyl monophosphate), inositol phosphate (IP3) and diacyl glycerol (DAG). Nitric oxide which causes vasodilation by stimulating the relaxation of smooth muscle fibres in blood vessels acts by stimulating the formation of cGMP (the secondary messenger) which stimulates the transport of Ca2+ into storage areas of the smooth muscle fibre from the cytosol. When cytosol Ca2+ ion concentration decreases it results in the relaxation of muscle fibres.
Some hormones cause the opening or closing of specific ion-channels in the cell membrane to initiate the entry or exit of certain ions to produce a specific effect (this effect may be produced through the G-protein).
Hormone interactions
The action of a hormone is dependent upon
• Its concentration in the plasma • The number of receptors of the hormone • Interaction with other hormones
In addition to the concentration of the hormone and the number of receptors present a hormone’s interaction with other hormones also affects its effectiveness. The different types of interactions that a hormone can have with other hormones are:
• Permissive effect. When prior exposure to one hormone facilitates the action of another hormone, e.g. exposure of the uterine cells to estrogen and FSH during follicular phase facilitates the action of progesterone during the luteal phase of the menstrual cycle. Exposure to estrogen and FSH also causes the development of receptors for progesterone in the uterine cells.
• Synergistic effect. When the effect of two hormones is greater than their independent effects. Thus, these hormones work together to produce an effect, e.g. both FSH and estrogens are required for the development of an ovarian follicle.
• Antagonistic effect. When the effect of one hormone is opposite to the effect of another hormone, e.g. parathyroid hormone from parathyroid gland increases blood calcium levels while calcitonin from C cells of thyroid reduces blood calcium levels. Normally, antagonistic hormones are not released at the same time because that would be a waste of energy.
Control of hormone secretion
Secretion of a particular hormone can be regulated by three mechanisms:
• By neural control, e.g., release of epinephrine and nor-epinephrine from the adrenal medulla is controlled by the sympathetic nervous system.
7

• By another hormone, e.g. release of thyroxin from the thyroid gland is stimulated by the thyroid stimulating hormone (TSH) from the anterior pituitary.
• Through negative or positive feedback:
Negative feedback
When the secretion of a hormone is inhibited by an effect produced in the target cell, e.g. FSH that stimulates the secretion of estrogen from the ovary is suppressed when estrogen levels reach a particular concentration. The effect produced (secretion of estrogens) by a hormone (FSH from the anterior pituitary) inhibits the secretion of the hormone (FSH) that caused it (Figure 2).
Fig 2: Negative feedback control
FSH from anterior pituitary
Follicles in the ovary are stimulated
Estrogen secretion
Increased levels of estrogen Shows the negative feedback
–
Positive feedback
Secretion of certain hormones is stimulated by the effect that it produces, e.g. oxytocin from the posterior pituitary enhances uterine contractions during parturition (birth of a baby). This causes the baby to descend to the cervix, further stretching the cervix which further stimulates the release of oxytocin. The positive feedback cycle is broken by a sudden change in the events of the cycle, e.g. in case of oxytocin, the cycle breaks when the baby is born.
In addition to the positive and negative feedback regulation of the hormone secretion there are periodic variations in their secretion also. These variations are dependent on seasonal changes, the circadian rhythm (an inherent rhythm), aging, stages of development and sleep, e.g., the levels of growth hormone increase during early stages of sleep and then reduce.
Clearance of hormones
• Binding with tissue. Once a hormone binds to a receptor, it is internalized and the hormone is degraded and the receptors are recycled.
• Metabolic destruction by the tissue, e.g. the water soluble hormones (proteins and catecholamines) are degraded by enzymes in the blood and tissues and excreted by the kidneys.
• Excretion by liver into bile, e.g. the steroid hormones which are conjugated in the liver and secreted ("excereted") into the bile.
• Excreted by the kidneys.
8

Hormones that are bound to plasma proteins have a longer half life.
Half-life of a hormone. The time taken for the levels of a hormone to be reduced to half
of its original concentration is known as its "half-life". Hormones like angiotensin II have
a half-life of less than a minute while others such as the thyroid hormone (bound to
proteins) have a half-life of 1 to 6 days.
9

Major endocrine glands, their secretions and disorders
The major endocrine glands include hypothalamus and pituitary (hypothalamo–hypophyseal system), thyroid, parathyroid, adrenal, pancreas, thymus, pineal gland and the gonads (ovary and testis) (Figure 3).
Pineal
Hypothalamo–hypophyseal system
Thyroid
Thymus
Adrenal
Pancreas
Ovary
Testis
Fig 3: Position of the major endocrine glands in the body
Hypothalamo–hypophyseal axis
For a long time the pituitary gland (hypophysis) was regarded to be the master gland of the body as it secretes hormones that control the secretion of other glands in the body. Then it was discovered that the pituitary itself is regulated by another gland, the hypothalamus, which secretes a set of regulatory hormones that act on the pituitary. Thus this hypothalamo–hypophyseal axis regulates the activity of various glands in the body (Figure 4). H
Hypothalamus
10

It is a part of the brain below the thalamus. It is an important connecting link between the nervous system and the endocrine system because it receives neural inputs from different regions of the brain and influences the secretions of the various hormones in the body through the pituitary gland. It integrates all the sensory inputs received by the brain from the body and acts as a regulatory centre for maintaining body temperature, osmotic balance, heart rate, respiratory rate, etc.
Releasing or inhibiting hormones Control and regulation of hormone
secretion Thyrotropin releasing hormone (TRH) Stimulates thyrotropin (TSH)
Growth hormone releasing hormone
(GHRH)
Stimulates growth hormone release
Growth hormone inhibiting hormone
(GHIH)
Inhibits growth hormone release
Prolactin releasing hormone (PRH) Stimulates prolactin release
Prolactin inhibiting hormone (PIH) or
dopamine
Inhibits prolactin release
Adrenocorticotropic hormone releasing
hormone (CRH)
Stimulates adrenocorticotropic hormone
release
Melanocyte stimulating hormone releasing
hormone (MSHRH)
Stimulates melanocyte stimulating hormone
release
Melanocyte stimulating hormone inhibiting
hormone (MSHIH)
Inhibits melanocyte stimulating hormones
release
11
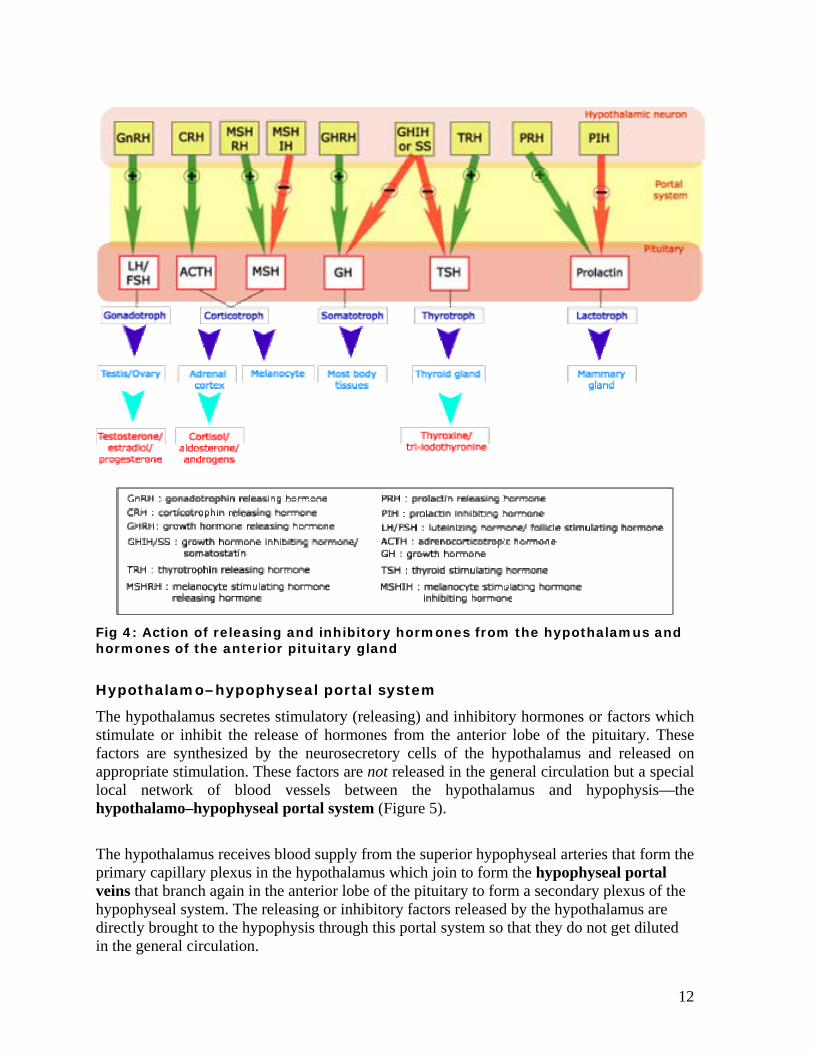
Fig 4: Action of releasing and inhibitory hormones from the hypothalamus and hormones of the anterior pituitary gland
Hypothalamo–hypophyseal portal system
The hypothalamus secretes stimulatory (releasing) and inhibitory hormones or factors which stimulate or inhibit the release of hormones from the anterior lobe of the pituitary. These factors are synthesized by the neurosecretory cells of the hypothalamus and released on appropriate stimulation. These factors are not released in the general circulation but a special local network of blood vessels between the hypothalamus and hypophysis—the hypothalamo–hypophyseal portal system (Figure 5).
The hypothalamus receives blood supply from the superior hypophyseal arteries that form the primary capillary plexus in the hypothalamus which join to form the hypophyseal portal veins that branch again in the anterior lobe of the pituitary to form a secondary plexus of the hypophyseal system. The releasing or inhibitory factors released by the hypothalamus are directly brought to the hypophysis through this portal system so that they do not get diluted in the general circulation.
12

Fig 5: Hypothalamo–hypophyseal portal system
s
e
m
Neurohypophysis
Pars nervosa
Hypophysis (Pituitary)
The hypophysis or pituitary gland is connected to the hypoth
infundibulum.
The pituitary consists of two lobes, the anterior lobe or aden
lobe or neurohypophysis. The adenohypophysis has two part
upper pars tuberalis which forms a covering around the infun
has the lobe like pars nervosa and the infundibulum. During
intermediate lobe called the pars intermedia is present which
its cells get integrated into the pars distalis.
Primary capillary plexus
Pars distalis
Pars tuberalis
Adenohypophysis
Hypophyseal portal veinsInfundibulu
alam
ohy
s, th
dib
emb
is l
Hypothalamu
u
po
e
ul
r
os
Secondary capillary plexus
Median eminenc
s though a stalk, the
physis and the posterior
lower pars distalis and the
um. The neurohypophysis
yonic development a third
t in the adults but some of
13

Somatotroph
It consists of five types of cells that secrete seven types of hormones (Figure 6). These are:
Adenohypophysis
1. Somatotrophs that secrete the growth hormone (GH) or
Corticotroph
Lactotroph
Gonadotroph
Thyrotroph
2. Antidiuretic hormone (ADH) or vasopressin produced by the supraoptic nucleus.
1. Oxytocin
This region of pituitary does not synthesize any hormones. It stores and then secretes two hormones which are synthesized in the neurons of the hypothalamus. There are two sets of neurons in the hypothalamus, the supraoptic nucleus and paraventricular nucleus which synthesize hormones and convey them to the posterior pituitary through the nerve fibres of these neurons. These nerve fibres form the axon terminals in the posterior pituitary where these hormones are stored and released on appropriate stimulation. These two hormones are:
Neurohypophysis Fig 6: Cell types of the adenohypophysis
produced by the paraventricular nucleus.
3. Gonadotrophs secrete the follicle stimulating hormone (FSH) and the luteinizing hormone (LH). These two hormones together are known as gonadotropins because they stimulate the gonads to produce specific hormones.
5. Corticotrophs secrete adrenocorticotrophic hormone (ACTH) which stimulates the adrenal cortex to produce adrenocorticoids (cortisol, corticosterone, and aldosterone). Some corticotrophs are the remnants of the pars intermedia and they secrete the melanocyte stimulating hormone (MSH).
4. Lactotrophs secrete the hormone prolactin.
2. Thyrotrophs that secrete the thyroid stimulating hormone (thyrotropin)
somatotropin
14

Part of pituitary
Principal cell type Hormones Principal actions Target organs
Disorders
Somatotroph Growth
hormone (GH)
Growth of body cells especially of
bones of limbs, stimulates protein
synthesis and inhibits protein
breakdown, stimulates hydrolysis
of fats, retards use of blood
glucose for ATP production
(diabetogenic effect).
General Hyposecretion
Dwarfism—Reduced secretion of GH from the anterior
pituitary results in stunted growth so the person
remains a dwarf. In African Pygmies and Lévi-Lorain
dwarfs, however, the secretion of GH from the
hypothalamo-hypophyseal tract is normal but
Somatomedin C (a mediator of growth hormone
action) levels are low. Levels of GH reduce with age.
Hypersecretion
Gigantism—This occurs due to overactivity of the
somatotrophs or some tumors in this region of the
pituitary causes increased secretion of GH. If this
happens before adolescence (before the closure of
epiphyseal plates) the person is abnormally tall.
If this happens after adolescence the bones become
thicker and the soft tissue continues to grow. In his
condition, called acromegaly, the hands and feet
become greatly enlarged, the lower jaw protrudes
out, the forehead slants forwards, and the tongue
liver and kidneys also become enlarged.
Thyrotroph Thyrotropin or
thyroid
stimulating
hormone
(TSH)
Controls secretion of thyroid
hormones
Thyroid
gland
Adeno-
hypophys
is
Corticotroph Adrenocorticot
ropic hormone
(ACTH)
Controls secretion of adrenal
cortex hormones.
Adrenal
cortex
15

16
Lactotroph Prolactin (PRL) Along with other hormones
stimulates milk production,
participates in control of
reproduction, osmoregulation,
growth and metabolism
Mammary
glands
Follicle
stimulating
hormone
(FSH)
In males, stimulates
spermatogenesis. In females
stimulates growth of ovarian
follicles.
Gonads
Gonadotroph
Luteinizing
hormone (LH)
Or
Interstitial cell
stimulating
hormone
(ICSH)
In females, also causes secretion
of estrogen & proferone and
together with FSH, it triggers
ovulation, stimulates conversion of
ovarian follicles into corpus
luteum.
In males stimulates stimulation of
testosterone from interstitial cells
of Leydig.
Gonads
No hormones are
synthesized here. Its
hormones are
synthesized in
hypothalamus
Oxytocin (OT) Stimulates contraction of uterine
muscles during birth; initiates
ejection of milk.
Uterine
muscles and
mammary
glands
Neuro-
phypophy
sis
Antidiuretic
hormone
(ADH) or
vasopressin
Stimulates reabsorption of water
and reduction in urine output;
stimulates constriction of blood
vessels to increase blood pressure,
reduces sweat secretion from
sweat glands.
Kidney,
blood
vessels,
sweat
glands
Hyposecretion causes diabetes insipidus. Inability
of the posterior pituitary to secrete enough ADH can
be due to head injury, some infections or it may be
congenital. It can result in loss of water from the
body due to the formation of very dilute urine as
enough water is not reabsorbed by the kidney
tubules resulting in severe dehydration.

The thyroid gland is an H-shaped gland that lies over the trachea below the larynx with the right and left lateral lobes on either side of it. The lobes are connected by a mass of tissue, called the isthmus. The gland consists of microscopic spherical sacs called thyroid follicles. These contain a colloid, composed of the glycoprotein thyroglobulin bound to thyroid hormones triiodothyronine (T3) and tetraiodothyronine or thyroxine (T4), which fills most of the thyroid gland.
Thyroid gland
Blue arrow shows parafollicular or C-cells that secrete calcitonin which helps lower calcium levels. These C-cells are actually named for being "clear" (as it is lightly stained). Notice that they are in the interstitium and do not normally touch the follicles.
Source: Courtesy: http://www.kumc.edu/instruction/medicine/anatomy/histoweb/endo/endo.htm ©1996 The University of Kansas
Thyroid gland
Larynx
Trachea
Basement membrane
Colloidal secretion
Cuboidal epithelium
The simple cuboidal epithelium lining the follicles produce the hormones T3 and T4 which are stored in the follicles with a glycoprotein, thyroglobulin. Notice that the thyroid is the only gland to store its hormones extracellularly.
Colloidal secretion
Follicular cell
Parafollicular cells
Blood c
17
apillary

18
Thyroid
cell type
Hormone Principle actions Disorders
Follicular
cells
Triiodothyronine
(T3)
Thyroxine or
tetraiodothyronine
(T4)
Increases basal metabolic
rate, stimulates synthesis
of proteins, increases use
of glucose and fatty acids
for ATP production,
increases heart strength,
accelerates body growth
and contribute to the
development of nervous
system in the embryo.
Hypersecretion is called hyperthyroidism and hyposecretion is called hypothyroidism.
Hyperthyroidism (toxic goiter, thyrotoxicosis or Grave’s disease). Is caused by an
autoimmune disorder where antibodies bind to receptors to TSH mimicking its action in
stimulating the thyroid gland. These antibodies are called thyroid-stimulating
immunoglobulins.
It may also be caused by a tumour in the thyroid tissue. Symptoms of hyperthyroidism
include a high state of excitability, increased sweating, intolerance to heat, weight loss, hand
tremors, psychic disorders and protrusion of the eyeballs in most patients.
Hypothyroidism. There is a reduced secretion of thyroid hormones because of another type
of autoimmune disorder where antibodies destroy the secretory cells. It may also be caused
by a deficiency of iodine as it is needed for the synthesis of thyroid hormones. The gland
enlarges in order to increase the secretion of hormones. This state of enlarged thyroid gland
is called goiter. Hypothyroidism in adults causes myxedema where there is accumulation of
a gel-like fluid in the interstitial spaces. 0ther symptoms include swelling of the face,
bagginess under the eyes, sluggishness, reduced cardiac output, etc.
Hypothyroidism in fetal life, infancy or childhood causes a condition called cretinism. It could
be congenital or caused by iodine deficiency. Symptoms include mental retardation and
improper body growth.
Parafollicular
cells (C-
cells)
Calcitonin (CT)
Lowers blood levels of
ionic Ca2+ and phosphates
by inhibiting bone
resorption by osteoclasts
and stimulates uptake of
calcium and phosphates
into the bone matrix. This
effect is more
predominant in children
than in adults.

Parathyroid glands These are small masses of tissue, partially embedded in the posterior surface of the lateral lobes of the thyroid gland.
Oxyphil cells Chief cells
Parathyroid cells (Chief cell) in string-like arrangement on the right and large, clear oxyphil cells (whose function is unknown) to the left.
Thyroid gland
Larynx
Trachea
Parathyroid glands
Hormone and
source
Principal actions Disorders
Parathyroid
hormone (PTH)
from Chief cells
Increases blood Ca2+ and PO42+ levels.
Increases bone resorption by osteoclasts;
and promotes formation of calcitriol,
which increases rate of dietary Ca2+ and
Mg2+ absorption, decreases the excretion
of calcium from the kidneys.
Hypoparathyroidism occurs when the
parathyroid hormone is not secreted in
adequate amounts. This results in decrease in
Ca2+ ion concentration of blood; very low levels
of calcium result in tetany that could be fatal.
Hyperparathyroidism is increased secretion of
parathyroid hormone and results in an
increased plasma Ca2+ ion concentration due to
increased bone resorption. This results in
weakened bones, depressed peripheral and
central nervous system, muscle weakness,
constipation, lack of appetite and depressed
relaxation of the heart muscle during diastole.
Secondary hyperparathyroidism may be caused
by vitamin D deficiency where there is a
compensatory hyperactivity of the parathyroid
gland.
19

A pair of adrenal (supra-renal) glands are located, one on each side of the spinal cord, above each kidney. Each gland consists of an outer cortex and inner medulla. The cortex has three distinct layers—zona glomerulosa, zona fasciculata and zona reticularis, each secreting different types of steroids. Medulla as groups of large cells which secrete epinephrine and norepinephrine on sympathetic stimulation (that is why adrenal medulla is considered to be an extension of the sympathetic nervous system).
Adrenal glands
Capsule
Adrenal glands
Kidney
Adrenal cortex
Adrenal medulla
Medulla
Zona reticularis
Zona fasciculata
Zona glomerulosa
Source: Courtesy: http://www.kumc.edu/instruction/medicine/anatomy/histoweb/endo/endo.htm ©1996The University of Kansas
20
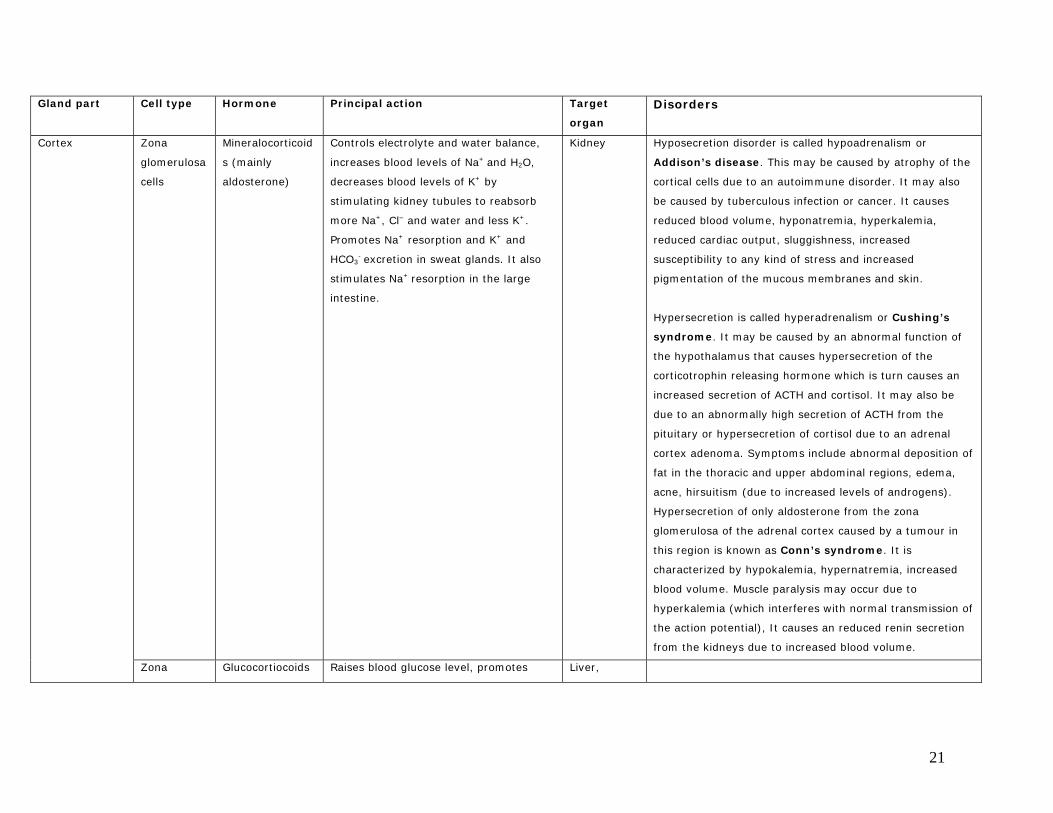
Gland part Cell type Hormone Principal action Target
organ
Disorders
Zona
glomerulosa
cells
Mineralocorticoid
s (mainly
aldosterone)
Controls electrolyte and water balance,
increases blood levels of Na+ and H2O,
decreases blood levels of K+ by
stimulating kidney tubules to reabsorb
more Na+, Cl– and water and less K+.
Promotes Na+ resorption and K+ and
HCO3- excretion in sweat glands. It also
stimulates Na+ resorption in the large
intestine.
Kidney Hyposecretion disorder is called hypoadrenalism or
Addison’s disease. This may be caused by atrophy of the
cortical cells due to an autoimmune disorder. It may also
be caused by tuberculous infection or cancer. It causes
reduced blood volume, hyponatremia, hyperkalemia,
reduced cardiac output, sluggishness, increased
susceptibility to any kind of stress and increased
pigmentation of the mucous membranes and skin.
Hypersecretion is called hyperadrenalism or Cushing’s
syndrome. It may be caused by an abnormal function of
the hypothalamus that causes hypersecretion of the
corticotrophin releasing hormone which is turn causes an
increased secretion of ACTH and cortisol. It may also be
due to an abnormally high secretion of ACTH from the
pituitary or hypersecretion of cortisol due to an adrenal
cortex adenoma. Symptoms include abnormal deposition of
fat in the thoracic and upper abdominal regions, edema,
acne, hirsuitism (due to increased levels of androgens).
Hypersecretion of only aldosterone from the zona
glomerulosa of the adrenal cortex caused by a tumour in
this region is known as Conn’s syndrome. It is
characterized by hypokalemia, hypernatremia, increased
blood volume. Muscle paralysis may occur due to
hyperkalemia (which interferes with normal transmission of
the action potential), It causes an reduced renin secretion
from the kidneys due to increased blood volume.
Cortex
Zona Glucocortiocoids Raises blood glucose level, promotes Liver,
21

fasciculata
cells
Cortisol (main),
corticosterone
gluconeogenesis in the liver and reduces
glucose utilization by cells, reduces
protein stores in all other cells of the
body, except liver cells and plasma,
promotes mobilization of fatty acids from
adipose tissue and enhances oxidation of
fatty acids in the cells, provides general
resistance to long term stress by blocking
inflammatory and allergic responses.
adipocytes
and other
body cells
Zona
reticularis
cells
Androgens
(main), e.g.
dihydroepiandros
terone (DHEA)
and
androstienedione
Assists in early growth of axillary and
pubic hairs in both sexes; in females, it
contributes to libido and is a source of
estrogen after menopause
Gonads Hypersecretion of androgens from the zona reticularis
because of a tumour in this part of the adrenal cortex
causes the adrenogenital syndrome. It causes
masculinization of the body. If it occurs in a female there is
a development of male characteristics such as a beard, a
deeper voice, deposition of proteins in the muscles,
baldness, etc. If it occurs in a prepubertal male it causes
precocious development of secondary sexual characters.
Medulla Chromaffin
cells
Epinephrine
(adrenaline)
Norepinephrine
(nor-adrenaline)
Stimulates elevation of blood glucose by
conversion of liver glycogen to glucose;
raises blood pressure; accelerates the
rate and force of heart beat; causes
constriction of skin and visceral
capillaries; causes dilation of vessels of
heart and skeletal muscles; increases
lipid breakdown, oxygen consumption,
erection of hair, dilation of pupils; initiate
stress response
Skeletal
muscles,
cardiac
muscles,
smooth
muscles,
blood
vessels, fat
cells
22

The pancreas is both an endocrine and exocrine gland. It is a flattened organ, about 12.5–15 cm long, located in the curve of the duodenum. Roughly 99% of pancreatic cells are exocrine present in clusters called acini. Interspersed among them are a group of endocrine cells forming lobules known as pancreatic islets or Islets of Langerhans. These islets contain four types of cells— alpha (α), beta (β), delta (δ), and F cells.
Pancreatic islets
23
Types of cells in the Islet of Langerhans
Alpha cell
Beta cell
F cell
Pancreas
Capillary
Delta cell

24
Cell type Hormone Principal action Target organ Disorders
Alpha cells
(α cells)
Glucagon
Causes lypolysis
• Accelerates breakdown of glycogen into glucose
in liver.
• Promotes conversion of other nutrients, such as
amino acids and lactic acid, into glucose in the
liver (gluconeogenesis).
• Enhances the release of glucose into blood.
Liver adipose
tissue
Beta cells
(β cells)
Insulin • Stimulates glucose transport from blood to
muscles and adipose cells, and stimulates liver
to take up glucose.
• Inhibits gluconeogenesis in the liver.
• Promotes both oxidation and conversion of
glucose into glycogen in liver and muscle cells.
• Inhibits metabolic breakdown of stored glycogen
in liver and muscle cells.
• Promotes synthesis of fats from glucose by
adipose tissue and also inhibits metabolic
breakdown of fat.
• Promotes uptake of amino acids by liver and
muscle cells, and stimulates protein synthesis
while inhibiting protein breakdown.
Liver, muscle,
adipose tissue, and
body cells
Delta cells
(δ cells)
Somatostatin (is a
paracrine agent)
Inhibits secretion of glucagon and insulin; reduces
motility of stomach, duodenum and gall bladder;
reduces secretion and absorption in the digestive
tract.
Pancreas (α and β
cells),
gastrointestinal
tract
F cells Pancreatic
polypeptide
(is a paracrine agent)
Inhibits somatostatin secretion, gall bladder
contraction and secretion of pancreatic digestive
enzymes.
Pancreas, gall
bladder
Hypersecretion of insulin is
called hyperinsulinism. It
may be caused by an
adenoma of an Islet of
Langerhans. It results in
hypoglycemia (reduced
blood glucose levels) which
could be fatal.
Hyposecretion of insulin or
hypoinsulinism causes
diabetes mellitus (Type I).
In Type II diabetes mellitus
the amount of insulin
secreted by pancreatic β
cells is normal but the
response of the cells is not
(insulin resistance).
Diabetes mellitus causes
hyperglycemia, glycosuria
(glucose in urine) polyuria
(increased urine output),
tissue injury, increased
metabolism of fat,
ketoacidosis and depletion
of body proteins.

25
Gonads and placenta
The testis in males and ovaries in females secrete sex hormones during puberty. These hormones are steroids and responsible for controlling various secondary sexual characters during puberty. The placenta also releases some hormones that are responsible for the maintenance and certain changes during pregnancy.
he testis in males and ovaries in females secrete sex hormones during puberty. These hormones are steroids and responsible for controlling various secondary sexual characters during puberty. The placenta also releases some hormones that are responsible for the maintenance and certain changes during pregnancy.
Ovary Testis Placenta
Ovarian follicle Corpus luteum Testis
The Graafian follicle is identified by the large antrum (A) and the cumulus oophorous (arrow) that surrounds the actual oocyte and projects into the antrum.
Source: Courtesy: http://www.kumc.edu/instruction/medicine/anatomy/histoweb/female/female.htm ©1996 The University of Kansas
Progesterone from the corpus luteum maintains the uterus for implantation. Granulosa luteal cells (GL) and theca luteal cells (TL).
Interstitial cells of Leydig
Seminiferous tubule
Sperms in different stages of development

26
Gland type
and part
Hormones Principal action Disorders
Ovary
Ovarian follicle Estrogen (estradiol
and estrone)
Stimulates the development and maintenance
of female sexual characteristics such as high
pitch, female voice and female pattern and
distribution of body hair at puberty.
Together with gonadotropic hormones of the
anterior pituitary gland they also regulate
menstrual cycle and development of
secondary sex organs.
Hypogonadism: when there is reduced estrogen secretion because
of poorly formed ovaries or genetically abnormal ovaries female
eunuchism occurs. The female secondary sexual characteristics fail
to develop and there is a prolonged growth of bones. The ovarian
cycles are irregular or there may be complete amenorrhoea.
Hypersecretion of estrogens: may occur in case of a granulosa cell
tumour which usually occurs after menopause. Symptoms include
hypertrophy of the endometrium and irregular bleeding.
Corpus luteum Progesterone and
estrogen
Progesterone prepares and maintains the
uterine lining for pregnancy, stimulates
mucosal lining of the fallopian tubes to
secrete a nutrient-rich fluid, prevents the
uterine myometrium from undergoing
contractions. Prepares the breast for milk
secretion. Estrogen stimulates uterine lining
for implantation to maintain pregnancy,
prepares the mammary glands for lactation
and regulates oogenesis.
Relaxin Facilitates accommodation of the growing
fetus. Relaxes pubic symphysis and helps
dilate uterine cervix near the end of
pregnancy.
Inhibin Regulates oogenesis by inhibiting FSH and
GnRH secretion.
Testis
Interstitial cells Testosterone Stimulates the descent of testis and male Hypogonadism: where there is a loss of testes or if there is a

27
of Leydig pattern of development (before birth);
stimulates development and maintenance of
male sexual characteristics and expression of
male characteristics such as beard,
moustache and low-pitch voice; stimulates
spermatogenesis, growth spurt, protein
synthesis and muscle development, bone
growth, stimulate secretion of erythropoietin
from the kidneys; increases basal
metabolism.
reduced secretion of GnRH from the hypothalamus (adipose genital
syndrome or Fröhlich’s syndrome or hypothalamic eunuchism). In
the absence of testosterone in an adult some of the secondary
sexual characteristics are lost. In a child these characteristics fail to
develop.
Hypergonadism: refers to an increased secretion of testosterone
due to tumour of Leydig cells. This causes an abnormally increased
muscle growth, reduced height (as the epiphyseal plates close
early) and excessive development of male sexual characteristics.
Sertoli cells Inhibin Regulates spermatogenesis by inhibiting FSH
secretion.
Placenta
Human chorionic
gonadotropin
(HCG)
Stimulates progesterone release from the
corpus luteum and maintains it. It has an
interstitial cell stimulating effect in a male
fetus. Simulates mammary gland growth
during pregnancy. Has weak growth hormone
like effects. Decreases insulin sensitivity and
glucose utilization by the mother’s cells so
that glucose is made available to the fetus. It
also mobilizes fatty acids from mother’s fat
stores.
or
Human placental
lactogen

Thymus
The thymus is located behind the sternum. It consists of two lobes
separated from one another by a connective tissue capsule.
Extensions of this capsule penetrate in the form of septa or
trabeculae to divide each lobe into lobules. Each lobule has a
lighter staining central medulla surrounded by a darkly staining
outer cortex. The cortex contains T cells which proliferate and
mature in the thymus; dendritic cells that assist the maturing T
cells and epithelial cells with long processes form a framework for
the maturing T cells. The medulla consists of more mature T cells,
epithelial cells and macrophages. Clusters of flattened degenerate
epithelial cells are arranged in concentric layers called Hassall’s
(thymic) corpuscles. In infants, the thymus is large but it starts
degenerating after puberty and is almost absent in old age.
Thymus Hormones Princip
Thymosin, thymic humoral factor,
thymic factor, thymopoietin
Promot
matura
lympho
Thymus
Source: http://www.cytochemistry.net/microanatomy/immune_system/lymphoid_tissues.htm© copyright 1998 Gwen V. Childs, Ph.D. URL Address: http://cellbio.utmb.edu/microanatomy/ Gwen V. Childs, Ph.D., WebMistress [email protected]
al action
e the proliferation and
tion of T-cells (derived from
cytes)
28

Pineal gland
It is a small endocrine gland attached to the roof of the third ventricle of the brain at the midline. It is covered by a capsule formed by pia mater and consists of masses of neuroglia and secretory cells called pinealocytes. It secretes the hormone melatonin, which is believed to help in maintaining the biological clock, as it is produced when no light stimulus is present and its production ceases when eye receives light stimulus.
Cerebral cortex
Pineal gland
Hypothalamus
Pituitary
Pineal gland Hormones Principal action
Melatonin Involved with the setting of the
biological clock in the body.
Controls seasonal fertility in some
animals.
Other endocrine tissues
Some tissues other than those described already, contain endocrine cells which secrete hormones. Along with these hormones some growth factors are also produced which stimulate cell growth and division.
29

Production site Hormone or
growth factor
Principal action
Gastrointestinal tract
G-cells of the stomach
Gastrin
Promotes secretion of gastric juice and increases motility
of the stomach.
Glucose-dependent
insulinotropic peptide
(GIP)
Stimulates release of insulin by pancreatic β cells, inhibits
gastric secretion.
Secretin Stimulates secretion of pancreatic juice rich in HCO3– ions
and bile; reduces gastric secretion and motility.
Cholecystokinin
(CCK)
Stimulates secretion of pancreatic juice rich in enzymes,
release of bile from the gall bladder and brings about the
feeling of fullness after eating.
Enteroendocrine cells of
the duodenum
Vasoactive intestinal
polypeptide (VIP)
Inhibits gastric secretion and motility
Oxyntic cells of the
stomach and cells of
the intestine
Ghrelin Stimulates food intake
Liver Angiotensinogen gets
converted to
angiotensin I which
gets converted to
angiotensin II
Causes vasoconstriction, enhances reabsorption of sodium
and chloride ions and water, stimulates the release of
aldosterone from adrenal cortex which further stimulates
reabsorption of sodium and chloride ions from the kidney
tubules. All this results in increased blood volume and
blood pressure.
Erythropoetin (EPO) Increases rate of red blood cell formation. Kidneys
Calcitriol (active
vitamin D)
Aids in the absorption of dietary calcium and phosphorus.
Heart Atrial natriuretic
peptide (ANP)
Decreases blood pressure and blood volume by
stimulating the excretion of Na+ ions from the kidney
tubules.
Adipose tissue Leptin Suppresses appetite, stimulates the release of
corticotropin releasing hormone that decreases food
intake, increases sympathetic activity resulting in an
increased metabolic rate and energy expenditure,
suppresses the release of appetite stimulators from the
hypothalamus.
Submaxillary salivary
gland
Epidermal growth
factor (EGF)
Stimulates proliferation of epithelial cells, fibroblasts,
neurons and astrocytes; suppresses some cancer cells and
30
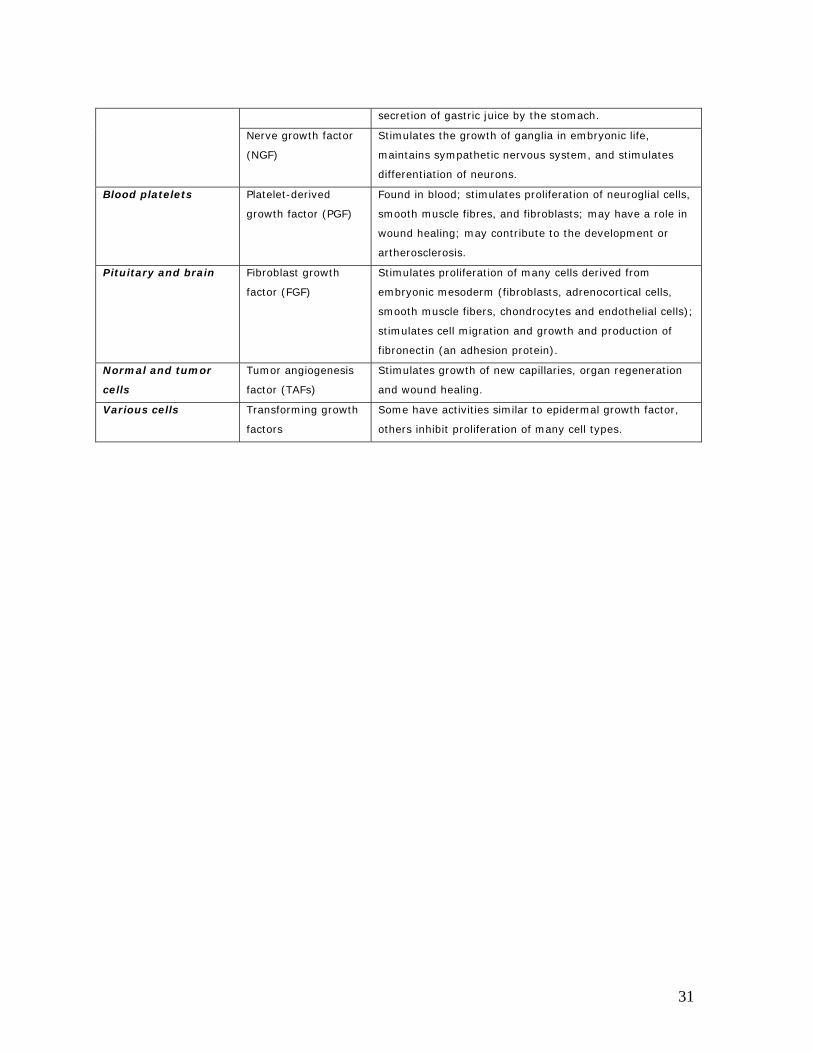
secretion of gastric juice by the stomach.
Nerve growth factor
(NGF)
Stimulates the growth of ganglia in embryonic life,
maintains sympathetic nervous system, and stimulates
differentiation of neurons.
Blood platelets Platelet-derived
growth factor (PGF)
Found in blood; stimulates proliferation of neuroglial cells,
smooth muscle fibres, and fibroblasts; may have a role in
wound healing; may contribute to the development or
artherosclerosis.
Pituitary and brain Fibroblast growth
factor (FGF)
Stimulates proliferation of many cells derived from
embryonic mesoderm (fibroblasts, adrenocortical cells,
smooth muscle fibers, chondrocytes and endothelial cells);
stimulates cell migration and growth and production of
fibronectin (an adhesion protein).
Normal and tumor
cells
Tumor angiogenesis
factor (TAFs)
Stimulates growth of new capillaries, organ regeneration
and wound healing.
Various cells Transforming growth
factors
Some have activities similar to epidermal growth factor,
others inhibit proliferation of many cell types.
31