physicians are my coworkers, not my clients
TRANSCRIPT
MARCH 1995, VOL 61, NO 3 0 I’ I N I 0 N
Physicians are my coworkers, not my clients
business promotion videotape that described ways in which clients could either be attract-
ed to or turned away from a busi- ness was shown to hospital staff members during a recent staff inservice program. After the pro- gram, one staff member made a comment that made me think about how nurses and other hospi- tal staff members treat physicians. Essentially, the comment was that we (ie, nurses, other hospital staff members) should treat physicians as prospective clients, thereby ensuring future business with these physicians. I do not agree.
CURRENT TREND There is a current trend in the
medical community to treat physicians as clients and pursue them the way one would a prospective customer. To accom- plish this, hospital administrators have provided physicians with whatever they request, whenever they request it. Hospital staff members are encouraged to treat physicians as clients who might take their business elsewhere if they are not completely satisfied.
Not only does this attitude lead to increased medical costs (ie, we get whatever the physician wants, no matter what the cost), but it also leads to hospital staff members’ dissatisfaction with their work environments. Hospi- tal staff members are dissatisfied because they know physicians are more valued, and they are required to take whatever the physician hands out.
This is an absurd way to treat physicians. In today’s health care system, only the patient can be considered a client or consumer. Hospital staff members, nurses, and physicians are team members working together to provide the product (ie, total patient care) to the health care consumer.
Nurses are no longer physician “hand ma i de ns .“
They are health care providers in their
own right.
CHANGING RESPONSlBlllTlES The medical community has
made progress in changing the old adage that the physician is “cap- tain of the ship.” Physicians are no longer the sole providers of health care. Nurses also are providers of health care, and they are held equally accountable for the care they give. Gone are the days when nurses did anything a physician ordered. Today, nurses follow physicians’ orders, but they are responsible for question-
MARILYN C. VOLIN, RN, BSN, CNOR, is a clinical nurse level 111, amhula- tory surgery, St Luke’s Hospitul, Kunsas City, Mo.
ing those orders if they are incon- gruent with what the nurse knows to be prudent patient care. Hospi- tals also have their own areas of responsibility. Nurses, physicians, and hospitals all may be involved in litigation, either separately or collectively.
cian-built hospitals” existed only because physicians brought their patients to those hospitals. Hospi- tals are no longer built by physi- cians; they are built by communi- ties. Physicians no longer “train” nurses. Nurses have their own body of knowledge that is taught by nurse educators and peers alike. Nurses are no longer physician “handmaidens.” They are health care providers in their own right.
A partnership exists among hospitals, nurses, and physicians. Hospitals cannot exist without nurses and physicians, and nurses and physicians know that hospi- tals provide them the largest areas in which to practice. Nurses and physicians need each other to pro- vide total quality patient care. This partnership is a symbiotic relationship.
There was a time when “physi-
TEAMWORK
pital staff members, physicians, and nurses as a medical team, what they fail to realize is that many physicians have never joined the team as “team players.” Too often, physicians feel they are the most important part of the team. The very definition of a team implies that there is no one
While communities view hos-
584 AORN JOURNAL
MARCH 1995, VOL 61, NO 3
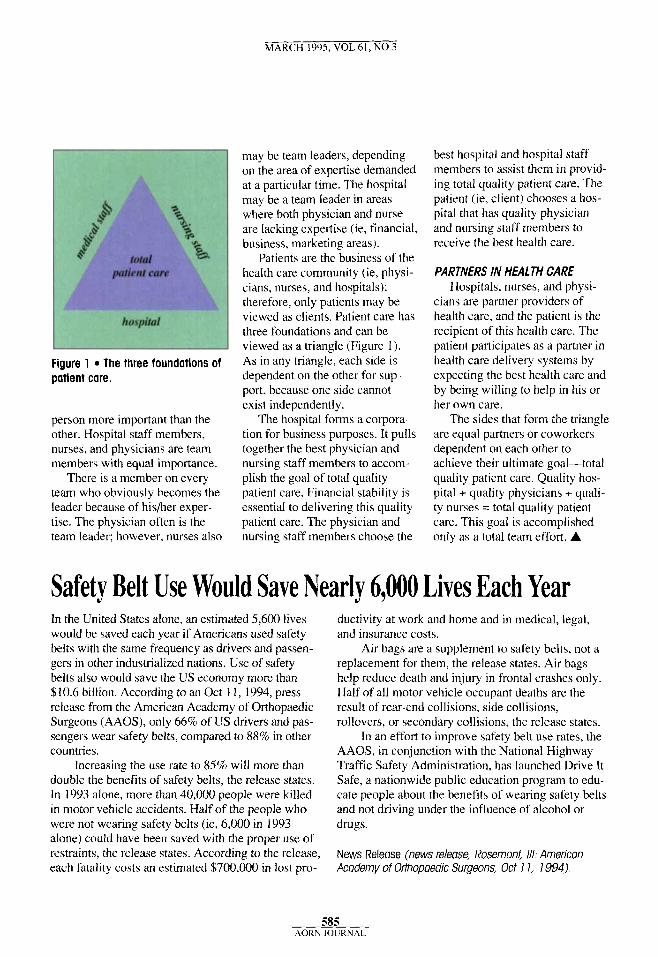
Figure 1 The three foundations of patient care.
person more important than the other. Hospital staff members, nurses, and physicians are team members with equal importance.
There is a member on every team who obviously becomes the leader because of hisher exper- tise. The physician often is the team leader; however, nurses also
may be team leaders, depending on the area of expertise demanded at a particular time. The hospital may be a team leader in areas where both physician and nurse are lacking expertise (ie, financial, business, marketing areas).
Patients are the business of the health care community (ie, physi- cians, nurses, and hospitals); therefore, only patients may be viewed as clients. Patient care has three foundations and can be viewed as a triangle (Figure 1). As in any triangle, each side is dependent on the other for sup- port, because one side cannot exist independently.
The hospital forms a corpora- tion for business purposes. It pulls together the best physician and nursing staff members to accom- plish the goal of total quality patient care. Financial stability is essential to delivering this quality patient care. The physician and nursing staff members choose the
best hospital and hospital staff members to assist them in provid- ing total quality patient care. The patient (ie, client) chooses a hos- pital that has quality physician and nursing staff members to receive the best health care.
PARTNERS IN HEALTH CARE Hospitals, nurses, and physi-
cians are partner providers of health care, and the patient is the recipient of this health care. The patient participates as a partner in health care delivery systems by expecting the best health care and by being willing to help in his or her own care.
are equal partners or coworkers dependent on each other to achieve their ultimate goal-total quality patient care. Quality hos- pital + quality physicians + quali- ty nurses = total quality patient care. This goal is accomplished only as a total team effort. A
The sides that form the triangle
Safety Belt Use Would Save Nearly 6,000 Lives Each Year In the United States alone, an estimated 5,600 lives would be saved each year if Americans used safety belts with the same frequency as drivers and passen- gers in other industrialized nations. Use of safety belts also would save the US economy more than $10.6 billion. According to an Oct 11, 1994, press release from the American Academy of Orthopaedic Surgeons (AAOS), only 66% of US drivers and pas- sengers wear safety belts, compared to 88% in other countries.
double the benefits of safety belts, the release states. In 1993 alone, more than 40,000 people were killed in motor vehicle accidents. Half of the people who were not wearing safety belts (ie, 6,000 in 1993 alone) could have been saved with the proper use of restraints, the release states. According to the release, each fatality costs an estimated $700,000 in lost pro-
Increasing the use rate to 85% will more than
ductivity at work and home and in medical, legal, and insurance costs.
Air bags are a supplement to safety belts, not a replacement for them, the release states. Air bags help reduce death and injury in frontal crashes only. Half of all motor vehicle occupant deaths are the result of rear-end collisions, side collisions, rollovers, or secondary collisions, the release states.
In an effort to improve safety belt use rates, the AAOS, in conjunction with the National Highway Traffic Safety Administration, has launched Drive It Safe, a nationwide public education program to edu- cate people about the benefits of wearing safety belts and not driving under the influence of alcohol or drugs.
News Release (news release, Rosemont, 111: American Academy of Orthopaedic Surgeons, Oct 1 1, 1994).
585 AORN JOURNAL