physician involvement in setting priorities for health regions
TRANSCRIPT

Healthcare Management Forum Gestion des soins de santé 21
Introduction ntegrating physicians into healthcare organizations has beenidentified as a significant challenge.1 This is even moreimportant (and challenging) in integrated delivery systems.2
Although success in healthcare integration requires physiciansin leadership, the mechanisms to accomplish this areproblematic. Physicians who assume full time managerial rolesin organizations can feel alienated from their colleagues: “If Idon’t see patients, other physicians won’t respect me.”3 Althoughrecognizing the importance of physicians in management,organizations may consider it a waste of training and ability totake physicians away from what they were trained to do - takingcare of patients.4 However, their knowledge and expertise aboutpatient care makes physician input into organizational
processes crucial. The challenge is to draw on the expertise that physicianshave related to patient care, and include it appropriately in organizationaldecision-making processes.
We propose that program budgeting and marginal analysis (PBMA), a widelyused approach to aid healthcare decision makers in priority setting, can serveas a useful mechanism to link physicians into organizational decision-making. Traditionally, PBMA has been viewed as a fairly technical tool to aidin the re-allocation of resources to improve gains in health or other importantconsiderations such as access.5 Taking a broader view of PBMA, that sets theprocess within the organizational context in which the priority setting activityis conducted, allows a broader set of organizational goals to be identified.6
This paper draws on the Alberta experience with PBMA to highlight theinvolvement of physicians in organizational decision-making processes. Inthe next section, the integrated structure of health regions in Alberta is described.An outline of the PBMA process is presented, as well as a framework that
ORIGINAL ARTICLE
Physician Involvement in Setting Prioritiesfor Health Regions by Alexandra Harrison and Craig Mitton
Alexandra Harrison isthe Director ofPostgraduate MedicalEducation and a memberof the Department ofCommunity HealthSciences at the Universityof Calgary. She teachescourses on theHealthcare System andLeadership in Healthcare.
Her research interests are in Medical Education aswell as the design, function, and performance ofhealthcare organizations
Craig Mitton is aResearch Scientist in theCentre for HealthcareInnovation andImprovement in the B.C.Research Institute forChildren’s and Women’sHealth and AssistantProfessor in the Dept. of Healthcare andEpidemiology at the
University of British Columbia. He is also an ESRCAdvanced Institute of Management InternationalFellow (UK) and holds a New Investigator Award fromthe Canadian Priority Setting Research Network. Hisresearch interests are in the areas of priority settingand resource allocation in health organizations.
I
AbstractAlthough many authors have emphasized the importance of including physicians in organizational activities, especially inintegrated delivery systems, much of the literature has focused on physicianinvolvement in governance or as managers. In this paper, program budgetingand marginal analysis (PBMA) is suggested as a mechanism to link physiciansinto organizational decision-making processes. This research included a widerange of examples that demonstrate the versatility of PBMA, and many ways toinvolve physicians.
1843 FORUM.qxd 12/16/04 8:09 AM Page 21

22 Healthcare Management Forum Gestion des soins de santé
positions the priority setting process
within an organizational context. Brief
summaries of the Alberta PBMA case
studies, which describe the involvement
of physicians, are followed by a
discussion of issues related to physician
engagement in priority setting. Since
health regions in Alberta exhibit many
features of integrated healthcare delivery
systems, the experience gained through
this work has implications for enhancing
integration, particularly physician-
system integration, in other contexts.
Health regions as integrated systemsSeventeen health regions were
established in the province of Alberta in
1994, to replace more than 200 individual
hospital and health-related boards in
order to “promote coordination and
integration of health services”.7 More
recently, further re-structuring has
resulted in nine geographic health
regions. In many respects, the health
regions in Alberta reflect the definition
articulated by Shortell and colleagues for
an organized delivery system.8 The
regions are composed of a network of
organizations that provide a coordinated
continuum of services to a geographically
defined population, and are held
clinically and fiscally accountable for the
clinical outcomes and health status of
the population served by each region.
The health regions in Alberta also
encompass many aspects of integration
identified by Gilles et al.9 Clinical
integration is evident with both
horizontal integration, such as the
consolidation of hospital services, and
vertical integration, since each region
has been required to merge the
previously independent organizations
responsible for public health, acute care,
home care, and continuing care under a
single board with a single administrative
structure. There is also functional
integration evident with a number of
shared services across each region, such
as Human Resources.
Some aspects of physician integrationare also apparent. For example, there is asingle medical staff organization (whichincludes about 1,500 physicians in theCalgary Health Region) and a commonphysician credentialing process for allhospitals in each region. The most obviousdeficiency in physician integration is thefinancial perspective. Most physicians inAlberta are paid on a fee-for-service basisfrom a provincial budget that is separatefrom health region budgets. Anothermeasure of physician integration toconsider is that of administrative involve-ment. Although a few physicians receivean honorarium for time committed tomajor administrative responsibilities(such as a Medical Director or ClinicalDepartment Head), more widespreadphysician involvement in administrativeprocesses is sought in the health regions.It has been suggested that greateradministrative involvement by physiciansincreases physician-system integrationand that greater physician-systemintegration is positively related to clinicalintegration and selected measures offinancial performance.9
Despite many macro level organizationalchanges in the health regions in Alberta,most budgets still reflect historicalspending patterns rather than anintegrated approach to deciding onpriorities that will benefit the healthregion or the population as a whole. It isdifficult to ‘maximize the health of thepopulation’ through historical allocationprocesses. Over the last few years, thePBMA framework has been applied in anumber of health regions in Alberta atvarious organizational levels to providedecision makers with a more informed,explicit approach to priority setting.10, 11
Internationally, PBMA has been used invarious countries including Britain,Australia, and New Zealand.
The PBMA process The stages of a PBMA process areoutlined in Table 1.
The following section explains the stepsin more detail.12
The first step is to determine the aim andscope of the priority setting activitywhich could be limited to a specific
PBMA Stages
1) Determine the aim and scope of the priority setting exercise
2) Compile a program budget (i.e. map of current activity and expenditure)
3) Form a stakeholder advisory panel
4) Determine locally relevant decision-making criteria and consultation requirede.g. Decision Makers, Board of Directors, Public etc.
5) Advisory panel identifies options for:a. areas for service growthb. areas for resource release by producing same level of output (or outcomes) with
fewer resources (i.e. increased efficiency)c. areas for resource release through scaling back or stopping some services
6) Advisory panel recommends:a. funding growth areas with new resourcesb. decisions to move resources from (5b) into (5a)c. trade-off decisions to move resources from (5c) to (5a) if relative value in (5c)
is deemed greater than that in (5a)
7) Use evidence from a variety of sources, including validity checks with additional stakeholders to make final decisions to inform the budget planning process
Source: Mitton and Donaldson 2004.
Table 1: Stages in a PBMA priority setting process
1843 FORUM.qxd 12/16/04 8:09 AM Page 22

Healthcare Management Forum Gestion des soins de santé 23
service or as broad as an entire sector ofcare. The next step is to develop aprogram budget for the chosen scope.This is a map of the current activity andexpenditure in the health organization orprogram (or set of programs) underconsideration, and provides a startingpoint for determining resource re-allocation and service re-design options.Following this, an advisory panel can bestruck. The panel should include arepresentative group of stakeholders thatis small enough to make the decision-making process manageable. In addition,data analysts and financial personnelshould be available to provide supportfor the decision-making process.
Before examining options for change, thepanel must identify the criteria they willuse to evaluate the activities that theywill be reviewing. Examples of criteriainclude: health gain, access, innovation,sustainability, staff retention/recruitment,and system integration, to name just afew. The criteria can be identified invarious ways, which may include a reviewof relevant business plans and otherinternal documents or input from otherstakeholders, such as the Board ofDirectors of the health organization orthe public. The criteria must be specifiedbefore the review begins and, if possible,be weighted to reflect their relativeimportance.
Once the advisory panel is set and thecriteria have been identified, a list ofservice growth options should bedeveloped and prioritized. Currentexpenditures then need to be examinedto identify opportunities for improvingoperational efficiency, and to identifyoptions for service reduction. Eachoption for growth and reduction shouldbe explicitly rated against the pre-definedcriteria, using available supportingevidence. Based on a broad set ofdecision-making inputs (e.g., evidencefrom the literature, local expert opinion,etc), decisions can be made to shiftresources from areas of operationalefficiency and/or service reductions toareas of proposed service growth.
The PBMA approach makes the prioritysetting process transparent, enablesexplicit comparison of options based onset criteria, and provides a forum throughwhich various pieces of information canbe considered by the relevant decisionmakers. The approach can be assophisticated or as basic as required bythe decision that needs to be made andthe time constraints.
An organizational approach to PBMAPrevious examples in the literature havetended to examine the PBMA process inisolation. That is, the focus has been ondefining a program, developing aprogram budget, striking a marginalanalysis expert panel, developingincremental wish lists and resourcerelease options, and then makingrecommendations for potential servicere-design. Following completion of theseven initial PBMA case studies inAlberta (described in the next section), itbecame clear that there was a broaderset of influences that were contributingto the success or failure of a given PBMAexercise. As a result, a conceptualframework was developed that positionsthe PBMA process more explicitly withinan organizational context, as per Figure 1.6
The ‘PBMA process’ box represents thestandard PBMA steps outlined above,with a number of the key lessons learnedfrom the various case studies in Albertalisted underneath. The model alsoidentifies a number of ‘inputs’ thatshould be in place for the PBMA processto be conducted, and some of the manyimportant outputs that might arise fromthis type of activity. One of these, asobserved by decision makers who havebeen involved in PBMA, is stakeholderengagement. Process barriers andfacilitators are also included in themodel. The factors for success includedin the model are not meant to beexhaustive; they capture observationsbased on the case studies conducted todate. The respective weight of any onefactor is not specified since this is adescriptive model.
The Case Studies Description
A total of seven PBMA case studies wereconducted in Alberta in three healthregions: the Calgary Health Region, theChinook Health Region and theHeadwaters Health Authority. The casestudies, summarized in Table 2, include awide range of examples of the
Figure 1: Conceptual framework for the PBMA process
OutputsInputs PBMAProcess
- program with manager- expert panel- health economist- research associate- knowledge of PBMA- relative org. stability
PBMA Process Issues to Consider- one-on-one meetings- program budget (for support)- data not used as a crutch- group chooses own criteria- critical review of literature- representative panel (not too big)
- self-rated usefulness by participants- further use of PBMA recommended- improved knowledge of service area- evaluation of historical services- engagement of various stakeholders- options for re-design proposed- re-allocation of resources- improved patient outcomes
Barriers- lack of trust between stakeholders- physicians not on board- misalignment of incentives- no (real or perceived) authority to change- lack of allocation experience- vertical budget silos- politics trumps evidence - specific program ‘too small’
Barriers - no genuine buy-in- too many other demands- politics prevents evaluation- discontinuity of personnel
1843 FORUM.qxd 12/16/04 8:09 AM Page 23
24 Healthcare Management Forum Gestion des soins de santé
application of PBMA. These case studies
are briefly described in the following
section to provide some context for the
findings related to physician involvement
in decision-making. Each of these
exercises followed the PBMA steps
outlined previously in the paper.
Calgary Health Region
The Calgary Health Region is primarily an
urban region, providing primary and
secondary care for citizens in the Calgary
area (about 900,000 people), tertiary care
for surrounding regions in Southern
Alberta, and certain quaternary services
for the entire province. The Region has
an annual budget of approximately
$1.5B. Three case studies were
conducted with programs in the Calgary
Health Region: Infant Head Cranial
Remodeling, Pediatric and Neonatal
Transport, and Musculoskeletal (MSK).
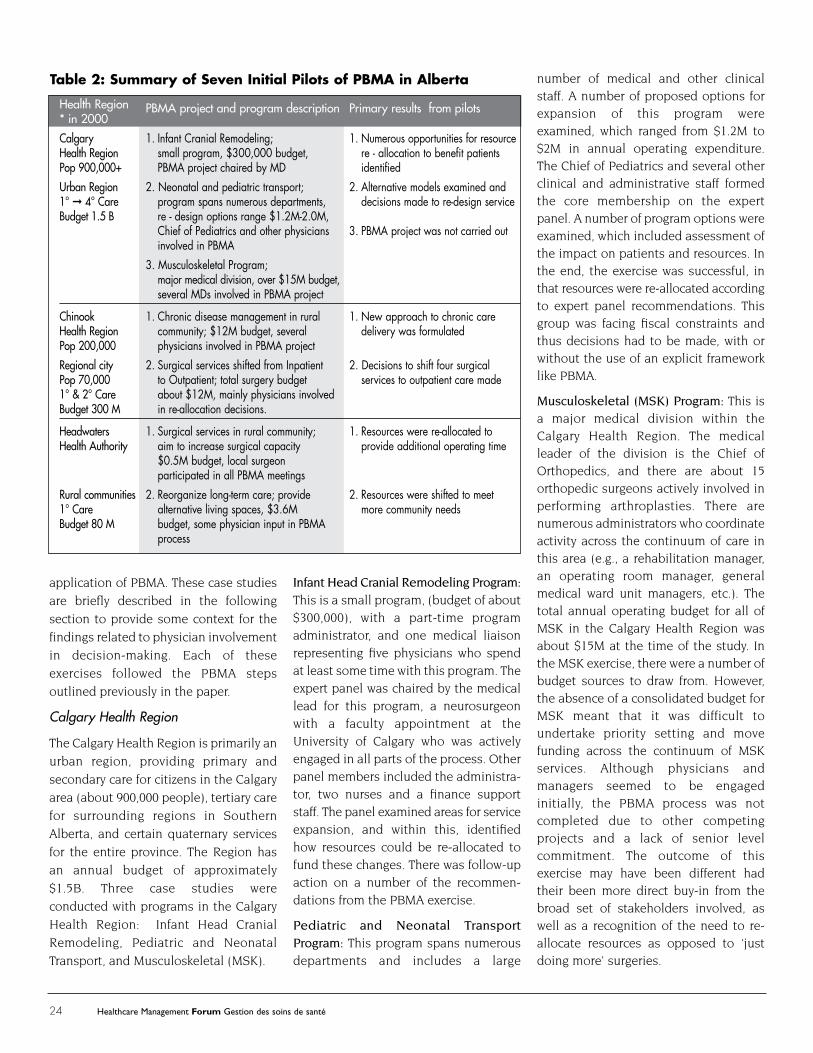
Infant Head Cranial Remodeling Program:This is a small program, (budget of about
$300,000), with a part-time program
administrator, and one medical liaison
representing five physicians who spend
at least some time with this program. The
expert panel was chaired by the medical
lead for this program, a neurosurgeon
with a faculty appointment at the
University of Calgary who was actively
engaged in all parts of the process. Other
panel members included the administra-
tor, two nurses and a finance support
staff. The panel examined areas for service
expansion, and within this, identified
how resources could be re-allocated to
fund these changes. There was follow-up
action on a number of the recommen-
dations from the PBMA exercise.
Pediatric and Neonatal TransportProgram: This program spans numerous
departments and includes a large
number of medical and other clinicalstaff. A number of proposed options forexpansion of this program wereexamined, which ranged from $1.2M to$2M in annual operating expenditure.The Chief of Pediatrics and several otherclinical and administrative staff formedthe core membership on the expertpanel. A number of program options wereexamined, which included assessment ofthe impact on patients and resources. Inthe end, the exercise was successful, inthat resources were re-allocated accordingto expert panel recommendations. Thisgroup was facing fiscal constraints andthus decisions had to be made, with orwithout the use of an explicit frameworklike PBMA.
Musculoskeletal (MSK) Program: This isa major medical division within theCalgary Health Region. The medicalleader of the division is the Chief ofOrthopedics, and there are about 15orthopedic surgeons actively involved inperforming arthroplasties. There arenumerous administrators who coordinateactivity across the continuum of care inthis area (e.g., a rehabilitation manager,an operating room manager, generalmedical ward unit managers, etc.). Thetotal annual operating budget for all ofMSK in the Calgary Health Region wasabout $15M at the time of the study. Inthe MSK exercise, there were a number ofbudget sources to draw from. However,the absence of a consolidated budget forMSK meant that it was difficult toundertake priority setting and movefunding across the continuum of MSKservices. Although physicians andmanagers seemed to be engagedinitially, the PBMA process was notcompleted due to other competingprojects and a lack of senior levelcommitment. The outcome of thisexercise may have been different hadtheir been more direct buy-in from thebroad set of stakeholders involved, aswell as a recognition of the need to re-allocate resources as opposed to ‘justdoing more’ surgeries.
Table 2: Summary of Seven Initial Pilots of PBMA in Alberta
Health Region PBMA project and program description Primary results from pilots* in 2000
Calgary 1. Infant Cranial Remodeling; 1. Numerous opportunities for resourceHealth Region small program, $300,000 budget, re - allocation to benefit patientsPop 900,000+ PBMA project chaired by MD identifiedUrban Region 2. Neonatal and pediatric transport; 2. Alternative models examined and1° � 4° Care program spans numerous departments, decisions made to re-design serviceBudget 1.5 B re - design options range $1.2M-2.0M,
Chief of Pediatrics and other physicians 3. PBMA project was not carried outinvolved in PBMA
3. Musculoskeletal Program;major medical division, over $15M budget,several MDs involved in PBMA project
Chinook 1. Chronic disease management in rural 1. New approach to chronic care Health Region community; $12M budget, several delivery was formulatedPop 200,000 physicians involved in PBMA projectRegional city 2. Surgical services shifted from Inpatient 2. Decisions to shift four surgical Pop 70,000 to Outpatient; total surgery budget services to outpatient care made1° & 2° Care about $12M, mainly physicians involvedBudget 300 M in re-allocation decisions.
Headwaters 1. Surgical services in rural community; 1. Resources were re-allocated toHealth Authority aim to increase surgical capacity provide additional operating time
$0.5M budget, local surgeonparticipated in all PBMA meetings
Rural communities 2. Reorganize long-term care; provide 2. Resources were shifted to meet 1° Care alternative living spaces, $3.6M more community needsBudget 80 M budget, some physician input in PBMA
process
1843 FORUM.qxd 12/16/04 8:09 AM Page 24

Healthcare Management Forum Gestion des soins de santé 25
Chinook Health Region
The Chinook Health Region is located inthe southern end of the province, andincludes small and medium sizecommunities including the city ofLethbridge (population 70,000). Itprovides both primary and secondarycare for a population of about 200,000with a budget of about $300M. Two casestudies were conducted in the Region:one for managing chronic disease, theother for surgical services.
Chronic Disease: The first case study, inthe small town of Taber, related tochronic disease management. The PBMAproject was undertaken to find resourceswithin the $12M Taber budget to developa multidisciplinary chronic disease clinicwith a budget of about $200,000. Theexpert panel included representationfrom a range of clinical staff (e.g.,pharmacy, home care, nursing, socialwork) and two of the eight GPs practicingin the area. The interdisciplinary panelassessed the potential impact on bothpatient outcomes and resources todetermine the best use of the limitedresources for chronic disease manage-ment. Despite a lack of managerialexperience on the panel, and a relativelyslow process (12 months), a new approachto chronic care delivery was formulatedfor this rural community.
Surgical Services: The second Chinookcase study examined shifting four majorsurgical divisions from inpatient tooutpatient services. The total surgicalbudget was about $16M, which spannedmany individual departments andclinical staff. A core working group of twosenior administrators and two dataanalysts met individually with physiciansand other clinical staff in each affectedarea. Through this consultative process,a large number of surgeons were directlyinvolved in the final recommendations.The surgical services exercise, like thechronic diseases project was alsosuccessful in that resources were freedup in the surgical disciplines in the study
from the existing model of care tofinance the new model of care that wasproposed. This budget-neutral resultexemplifies the basic tenet of shifting orre-allocating existing resources to bettermeet program or organizational objectivessuch as health gain.
Headwaters Health Authority
At the time of the study, the HeadwatersHealth Authority (budget $80M) wascomprised mainly of rural communitiesand ran from Claresholm, approximately120 km south of Calgary, along the southand west outskirts of Calgary, andextended west to the mountain town ofBanff. There were two case studies in thisregion, one in the town of Canmore, theother in Claresholm. (As part of the re-structuring in 2002, Headwaters wasintegrated into the Calgary Health Region).
Canmore: A rural surgical department inthe town of Canmore, with a $0.5Mbudget, used the PBMA process toidentify opportunities for growth and forreleasing resources to fund the proposedincrease in surgical capacity. Thisexercise was conducted over a four-monthperiod. A general surgeon participatedon the expert panel, along with thesenior administrator for Canmore, thehospital nursing manager and theoperating room manager. The panel re-allocated resources within the surgicalservices budget to provide additionaloperating time. The panel anticipatedthat the PBMA exercise might drawattention to their budget challenges.Although the panel believed thatimproved patient benefit would resultfrom an even greater allotment ofoperating theatre time, the groupprovided their recommendations withinthe existing budget constraints.
Claresholm: The Claresholm CommunityService Area used PBMA to re-design itsdelivery of long-term care. The annualoperating budget for long-term care inClaresholm was about $3.6M. TheClaresholm long-term care exercise had
direct physician involvement on theexpert panel, as well as a broadrepresentation of non-medical clinicalstaff. As a result of the project, severaltraditional long-term care beds wereclosed and a number of alternative livingspaces were identified. The exercise wassuccessful in that resources were shiftedaccording to panel recommendations tomeet more needs for those requiringlong-term care services.
Case Study SummaryIn summary, the PBMA approach wassuccessful in six of the seven examples.The range of outputs from theseexercises is reflected on the right handside of Figure 1. The case studies includeda wide spectrum of locations andservices. They included urban, regionaland rural centres, with a variety ofmedical and surgical services includingacute and chronic care, and patientpopulations ranging from Pediatrics tolong-term care. A key element in thesuccess of the projects was physicianinvolvement, which is examined in moredepth in the next section.
Physician Involvement with PBMAA number of key issues related tophysician involvement in decision-making were identified in the Albertacase studies mentioned above. First,through follow-up surveys with expertpanel members, the importance ofhaving both medical and managerialrepresentatives involved in the PBMAprocess was consistently recognized. Inparticular, there was a sense that withoutdirect physician involvement, it wasunlikely that recommendations would befollowed. Participants also indicated thatas a direct result of the PBMA exercises,there was improved communicationamong medical groups and with managers.In addition, all parties gained a betterunderstanding of the economic pressuresfaced in healthcare. A further benefit ofthis type of consensus decision-makingapproach was that in contrast to previous
1843 FORUM.qxd 12/16/04 8:09 AM Page 25

26 Healthcare Management Forum Gestion des soins de santé
historical allocation practices, thevarious stakeholders were broughttogether to explicitly address key issuesin a non-threatening manner.
Second, it was recognized that thestructure of the relationship betweenphysicians and health regions in Albertais problematic in terms of settingpriorities and allocating resources. InAlberta, as in other provinces, themajority of physicians operate as defacto private entrepreneurs, who use thefacilities of the health region yet are notresponsible for the fiscal management ofthe health region. In contrast, healthregions are responsible for providingservices within their given fundingenvelope. Since physicians are notdirectly accountable to the healthregions, this can compromise theregion’s ability to offer services that willmaximize health benefit for the resourcesavailable. An advantage of PBMA is thatit can be used even if the structuralrelationship between the health regionand medical staff is not aligned. ThePBMA process does not depend on onetype of physician reimbursementstructure, or even having a formalrelationship between the health regionand the physicians who work in theregion. If physicians are willing to investtime in the priority setting process,managers and physicians together, asexperts in their own fields, can tackle thedilemma of resource limitations in aproactive manner.
Third, in priority-setting processes likePBMA, it is helpful to keep in mind thatphysicians and managers have distinctbut complementary skills. If managersask physicians for their input, managersmust be willing to accept the advice evenif is not what they want to hear.Physicians and other clinicians are wellpositioned to assess the impact ofresource shifts on the patient populationbeing served. Physicians, on the otherhand, at some point in priority-settingactivity, need to take a broader view ofthe allocation of system resources. The
mandate of a health region is to meet thehealth needs of the population with theresources available, which does notnecessarily mean meeting all the needsof a particular program or one group ofphysicians.
Fourth, the ability of health regions toshift resources is limited by the majorimpact that physicians have on resourceutilization. This is potentially problematicfrom a priority setting perspectivebecause physicians are the main driversof utilization, and as such will influenceto a great degree the health regions’operational budget. Physicians havepower over utilization but limitedaccountability for overall resourceutilization. This restricts the ability of theadministrators in health regions to shiftresources, even if informed by anevidenced based process. However,PBMA provides a mechanism to overcomethis structural issue by incorporatingphysicians into the priority settingprocess and operationalizing integration(i.e. to make decisions about howresources might be reallocated forintegrated service provision). Theconceptualized framework (Figure 1)provides additional information aboutthe predisposing organizational factorsthat will contribute to success.
In summary, it was observed that thePBMA approach draws clinicians andmanagers together to work toward thecommon goals of improving healthbenefit and meeting health needs. It wasalso recognized that it is advantageousto have wide representation from front-line clinical staff, including physicians.Since most physicians are not employeesof the health region, if managers want toalter programs and services, physicianinvolvement and leadership is vital.PBMA can serve as a vehicle for directlyincorporating physician views into thedecision-making process, which wasrecognized by clinicians and managersalike as a necessary part of an informed,evidence-based approach to prioritysetting.
Discussion The Regional Health Authorities Act13 gives
health regions a mandate to meet the
health needs of those living in a defined
geographic region. To accomplish this,
health regions need to assess the needs
of the population, integrate services, and
allocate, or re-allocate, resources to
maximize the benefits to the population
it serves. A truly integrated service delivery
model will require health regions to have
mechanisms that allow re-allocation of
resources across programs and even
portfolios.
There is increasing recognition of the
need to involve physicians in organiza-
tional activities. National agencies
responsible for postgraduate medical
education in both Canada (the Royal
College of Physicians and Surgeons of
Canada) and the United States
(Accreditation Council for Graduate
Medical Education) have identified the
importance of providing training for
residents to enhance their participation
in the health systems in which they will
work.14,15 Other recent reports also
highlight the need to connect physicians
with their health systems. The Institute
of Medicine in the United States
suggests that “healthcare organizations
design and implement more effective
organizational support processes to
make change in the delivery of healthcare
possible”.16 A report on healthcare reform
in Alberta recommends “providing better
alignment between physicians and
regional health authorities”.17
Integrating physicians into organizational
activities in appropriate and meaningful
ways is a major challenge in healthcare
organizations. Physicians are frustrated
when they are not able to provide the
best care available for their patients due
to fiscal constraints, but they usually do
not have economic accountability for
organizational expenditures. Similarly,
managers are frustrated by their
responsibility for resource allocation
without control over the clinical
1843 FORUM.qxd 12/16/04 8:09 AM Page 26

Healthcare Management Forum Gestion des soins de santé 27
decisions that drive the use of resources.
The PBMA approach brings these two
solitudes (both necessary perspectives)
together to make decisions about the
best use of available resources.
PBMA offers a mechanism for physicians
to gain a better understanding of, as well
as contribute to, their healthcare
organizations in a manner that draws on
their clinical expertise. PBMA does not
require physicians to give up clinical
involvement. In fact, it is the physician’s
clinical perspective that is important to
bring to the priority setting process.
PBMA offers clinicians a window into the
broader mandate of the organization and
the need to prioritize organizational
resources. It encourages them to widen
their professional focus beyond concern
for the individual patient to consider the
structures and processes that are needed
to make patient care possible. This
‘systems’ view is a new perspective for
many physicians but necessary to ensure
the services provided optimize the health
of the populations served.
Increasingly, physicians are expected to
use the best available evidence in their
clinical practices. However evidence
alone is not enough to change clinical
practice.18 Discussion with local opinion
leaders is a crucial step in the application
of evidence. PBMA provides a structured
process for managerial and clinical
experts to review and discuss the
available evidence relevant to the making
decisions about organizational priorities.
Conclusion Although many authors have emphasized
the importance of including physicians in
organizational activities, especially in
integrated delivery systems,19 much of
the literature has focused on physician
involvement in governance20,21 or as
managers.3,4 In this paper, PBMA is
suggested as a mechanism to link
physicians into organizational decision-
making processes. This research included
a wide range of examples that demonstrate
the versatility of PBMA, and many waysto involve physicians. The steps in thePBMA process, as well as its broaderrelation to an organizational context aredescribed. A key lesson from these casestudies is the importance of participationby physicians in the priority settingprocesses. Without the involvement ofphysicians, it is unlikely that the realresource shifts that occurred would havetaken place. For physicians, PBMAprovides a sound vehicle for medicalinvolvement in decisions about wherehealthcare resources should be directed.Since these decisions will have a directimpact on clinical care, it is crucial tohave physicians involved in this process.
References1. Burns LR, Thorpe DP. Trends and models in physician-
hospital organization. Healthcare Management Review1993;18(4):7-20.
2. Johnson RL. Commentary on ‘The challenges of governingintegrated healthcare systems’. Healthcare ManagementReview 1995;20(4):82-87.
3. Coddington DC, Moore KD, Fisher EA. Physician Leaders inIntegrated Delivery. Medical Group Management Journal1997;44(5):84-88,90.
4. LeTourneau B, Curry W. Physicians as executives: boon orboondoggle? Frontiers of Health Services Management1997;13:3-17.
5. Donaldson C, Farrar S. Needs assessment: developing aneconomic approach. Health Policy 1993;25:95-108.
6. Mitton C, Donaldson C. Setting priorities and allocatingresources in health regions: lessons from a projectevaluating program budgeting and marginal analysis(PBMA). Health Policy 2003;64:335-348.
7. Alberta Health. Regional Health Authorities User’s Guide.Edmonton: Alberta Health; 1994.
8. Shortell SM, Kellogg JL, Gilles RR, Anderson DA, Mitchell JB,Morgan KL. Creating organized delivery systems: thebarriers and facilitators. Hospital & Health ServicesAdministration 1993;38(4):447-466.
9. Gillies RR, Shortell SM, Anderson D, Mitchell J, Morgan K,Conceptualizing and measuring integration: findings fromthe health systems integration study. Hospital & HealthServices Administration 1993;38(4):467-489.
10. Donaldson C, Mitton C, Martin H, Hasselback P, Nelson D,Dean S, et al. Priority setting within regional fundingenvelopes: the use of program budgeting and marginalanalysis. Ottawa: Canadian Health Services ResearchFoundation; 2002.
11. Mitton C, Patten S, Waldner H, Donaldson C. Prioritysetting in health authorities: a novel approach to ahistorical activity. Social Science and Medicine 2003;57:1653-1663.
12. Mitton C, Donaldson C. The Priority Setting Toolkit: A Guideto the Use of Economics in Healthcare Decision Making.London: BMJ Books; 2004.
13. Province of Alberta. Regional Health Authorities Act.Edmonton: Queen’s Printer for Alberta;1994.
14. The Royal College of Physicians and Surgeons of Canada.Skills for the new millennium report of the societal needsworking group CanMEDS 2000 project. Ottawa: RCPSC;1996.
15. The Accreditation Council for Graduate Medical Education.GME Core Curriculum. Chicago:ACGME;2000.
16. Institute of Medicine. Crossing the quality chasm: a newhealth system for the 21st century. Washington, DC:NationalAcademy Press;2001.
17. Premier’s Advisory Council on Health. A framework forreform. Government of Alberta:December 2001.
18. Lockyer J, Mazmanian P, Harrison A, Knox A. The adoptionof innovation. In: Davis D, Fox R, editors. The physician aslearner: linking research to practice. Chicago, IL: AmericanMedical Association; 1994:33-45.
19. Burns LR, Walston SL, Alexander JA, Zukerman HS,Andersen RM, Torrens PR, et al. Just how integrated areintegrated delivery systems? Results from a national survey.Healthcare Management Review 2001;26(1):20-39.
20. Kocher C, Kumar K, Subramanian R. Physician-hospitalintegration strategies: impact on physicians involvement inhospital governance. Healthcare Management Review1998;23(3):38-47.
21. Alexander JA, Zuckerman HS, Pointer DD. The challenges ofgoverning integrated healthcare delivery systems. HealthcareManagement Review 1995;20(4):69-81.
St. Mary’s General Hospital Appoints Chief Operating Officer
St. Mary’s General Hospital (Kitchener) would like to announce theappointment of Marion Bramwell to Chief Operating Officer, in additionto her roles as Executive Vice President and Chief Nursing Executive.A tremendous asset to St. Mary’s, Ms. Bramwell will continue to overseecorporate strategic planning and implementation, the strengthening ofthe hospital’s academic linkages and partnerships for education andresearch, lead many of St. Mary’s strategic initiatives and oversee themajority of our clinical programs.
Ms.Bramwell is a Registered Nurse,holds a Bachelor of Arts Degree (Psychology) and a Masterof Health Science (Health Administration). She is a Certified Health Executive with the CanadianCollege of Health Service Executives (CCHSE) and is a Surveyor with the Canadian Councilon Health Services Accreditation (CCHSA). Most recently, Ms. Bramwell was appointed to theProvincial Health Human Resources Strategic Advisory Group and the Board of GovernorsConestoga College (Kitchener).
1843 FORUM.qxd 12/16/04 8:09 AM Page 27