phuture 2014-15
DESCRIPTION
IPSF's Annual Educational and Scientific PublicationTRANSCRIPT

phuture
IPSF
Phu
ture
| Is
sue 1
9 | N
ovem
ber 2
015
Rational Use ofMedicines
Focusing on Antimicrobial
Resistance
InternationalPharmaceuticalStudents’Federation

From the Chairperson of Pharmacy Education
Phuture is the hallmark publication of pharmacy practice and pharmaceutical science from the students’ perspective. Ms. Dana Mohamad has worked diligently to bring quality articles for our member audience, partners, and those simply wanting to know what this federation has to offer.
I would like to take this opportunity to recognize members of the pharmacy education committee who were integral in making this publication a success.
Ms. Amber Liu, Canada/NetherlandsMs. Whitley Yi, United States of AmericaMs. Juliet Obi, NigeriaMs. Mariana Cunha, PortugalMs. Bernice Bonsu Adusah, GhanaMs. Sarah Romeili, Algeria
As a student run organization we are privy to the issues in our profession, and are pas-sionate about provoking positive changes in healthcare collectively and globally.
Thank you for your time, and please share what you have learned from the Interna-tional Pharmaceutical Students’ Federation.
Viva la Pharmacie!
Ms. Britany ManiChairperson of Pharmacy Education

Introduction
This year’s Phuture was designed to deliver an overall view of the progressing state of antimicrobial resistance as a great influence on both local and global public health.The Pharmacy Education Committee and I have worked to deliver articles from a wide range of regions, countries, degrees, and specialties to serve IPSF, whose mission is international pharmacy and health cooperation.
I hope this draws your attention to antimicrobial resistance and provides you with sound reading material. Thank you for reading this publication and thank you to our writers for providing articles which help this come to life. In addition, thank you to my fellow Pharmacy Education Coordinators -- Amber, Whitley, Brittany and the rest of our super team.
Viva la Pharmacie!
Dana MohamadEducational & Scientific Publications Coordinator

Since establishment in 1949, IPSF now represents over 313,000 pharmaceutical students and recent graduates in over 80 countries worldwide.
IPSF is the leading international advocacy organisation of pharmacy students promoting improved public health through provision of information, education, networking, and a range of publication and professional activities.
Design & Layout
Ms. Amy HowardIPSF Chairperson of Media and Publications
Ms. Sara DiTursiEditor-in-Chief
Ms. Sheena PatelMs. Katarina Zunic
Edited by

contentsQuestion & Answer 2Matthew Miller, PharmD, BCPS
Coming Together in the Fight Against Antimicrobial Resistance 6Laurens Oort, MSc.
Emergence of Antimicrobial-Resistant Bacteria in the Community 10T. Djerboua, MSc.
Genetic Immunization 14Dana Mohamad
Enterococcus species: A Matter of Concern 16Elsa Martins
Review of Antimicrobial Stewardship Certificate Programs in the United States 18Meghan Jeffres, PharmD
The Inclusion of Clinical Pharmacists to Effectively Combat Antimicrobial Resistance 20Sylvia Lee, Detron M. Brown MPH, Obinna Okafor, Enaefe Ziregbe
Running a Successful Campaign 23Medicine Awareness
AMR and Pharmacy Practice 25Michel Brilhante, MSc.
Antimicrobial Resistance in Croatia 27Katarina Žunić
An Inside Look and How to Reduce the Misuse of Antibiotics in Nigeria 28Mordi Chiedu Jr, Pharm and Ogunkoya David, Pharm
Focusing on Antimicrobial Resistance: U.K. Perspective 30Faith Matungamidze, MPharm and Mayur Kumar, MPharm
Antimicrobial Resistance in Colombia: A Challenge for Healthcare Professionals 32Margareth Charry
Focusing On Antimicrobial Resistance: A Ghanaian Perspective 34Bernice Bonsu Adusah
Focusing on Antimicrobial Resistance: An Algerian Perspective 36Khadidja Si Chaib, Pharm and Bouatta Rahima, Pharm
IPSF Phuture 20152
What are the capacity and trends for antibiotic use in your country and what are the most abused/misused medications?
There are numerous articles that evaluate antimicrobial prescribing habits here in the United States. A recent publication from Shapiro DL, et al evaluated a database from the National Center for Health Statistics (NCHS) to review the burden of antibiotic prescriptions from the ambulatory care setting as well types of agents being prescribed. According to the NCHS database, between the years 2007 and 2009 there were approximately 985 million annual visits (95% CI: 903-1066 million) and of those antibiotics were prescribed in 101 million visits annually (95% CI: 91-111 million). From this data set the authors determined that 61% (62 million visits annually) of antibiotic prescriptions were for broad spectrum therapies. The two most frequent offenders were fluoroquinolones (25 million per year) and macrolides (20 million per year). These therapies were commonly prescribed for acute respiratory tract infections (38%), more than half of which rarely require antibiotic therapy given the high likelihood of viral etiology. Another group, Hunkler RJ et al evaluated U.S. outpatient antibiotic prescribing for the year 2010 through the IMS Health Xponent database, which represents more than 70%
Clinical Pharmacy Specialist in Infectious Diseases at the University of Colorado Hospital
Question & Answer:The Scope of Antimicrobial Resistance in the United States and the
Efforts to Keep it Under Control
of U.S. prescriptions. During 2010, the authors identified some 258 million courses of antibiotics prescribed, which equated to 833 prescriptions per 1,000 persons. This group additionally identified that macrolides, mostly azithromycin, were the most frequently prescribed antibiotic. Regional variations existed with the largest concentrations of antibiotic prescribing present in the southeastern and midwestern states. However, in looking back from 2000 through 2010, the rate of outpatient antibiotic prescriptions has not increased drastically. The problem actually arises from the marked shift in antibiotic selection from narrow to broad spectrum therapies, which more than doubled from 2000 to 2010 (233 to 471 prescriptions per 1,000 persons). This same pattern holds true when reviewing antibiotic prescribing within hospitalized patients, with on average more than 50% of patients receiving an antibiotic during their encounter. Most of the prescribed therapies were for respiratory and genitourinary sources and most antibiotic therapies prescribed are considered broad spectrum. This is not to say that antibiotics are bad or that we want to stop people from using them, but we need to do a better job of utilizing them appropriately and for the correct duration.
Matthew Miller, PharmD, BCPS

Phut
ure
IPSF Phuture 2015 3
Clinical Pharmacy Specialist in Infectious Diseases at the University of Colorado Hospital from infection control, microbiology, phy-sician representation from other specialty areas, clinical and staff pharmacists, nursing, information technology and others frequently involved in the care of patients receiving antimicrobials. Goals of this group are to ensure the appropriate and timely selection of empiric antimicrobials, tailoring therapy to agents with the narrowest activity spectrum, minimizing unnecessary antimicrobial use, optimizing doses of available antimicrobials, individualizing treatment durations, and drug therapy monitoring for both efficacy and toxicity. Coordinated efforts from antimicro-bial stewardship programs (ASP) have shown reductions in CDAD, resistance, and improved patient outcomes. Some methods used by ASPs to impact antimicrobial use include: pre-authorization, prospective audit with feedback, clinical pathways, decision support, and rapid diagnostics. Here at the University of Colorado Hospital we utilize a multi-step method with pre-authorization of restricted antibiotics combined with prospective audit with feedback. In addition, we review positive cultures from the microbiology laboratory to facilitate de-escalation of therapy to the most appropriate and narrow spectrum agent(s) available. Our preauthorization strategy is a tiered approach with 3 levels of restriction. Level one is unrestricted, level two is approved through protocols outlined by the ASP by the clinical pharmacists, and level 3 is restricted to infectious diseases approval by way of pager that is rotated between infectious dis-eases trained pharmacists and physicians. In addition to these programs, there is much in the way of legislation to assist in developing stewardship initiatives, incentivize new drug development, and much more.
What measurements is your country taking to prevent/reduce antimicrobial resistance?
As previously eluded to above, antibiotic ther-apy is frequently not indicated with estimates from the Centers for Disease Control (CDC) in the range of 30-50% cases. Reasons for clas-sifying therapy as not indicated in descending order include; administration longer than rec-ommended (33%),non-infectious/non-bacte-rial syndromes (32%), treatment of coloniz-ing or contaminating microorganisms (16%), redundant antimicrobial coverage (10%), and spectrum of activity not indicated (4%). Costs of antibiotic misuse is evident with rise in antimicrobial resistance and Clostridium diffi-cile associated diarrhea (CDAD) in the United States, as outlined in the 2013 CDC Antibiotic Resistance Threat Report. Numerous publica-tions have drawn links between antibiotic exposure and the development of drug resist-ance and CDAD, with some classes showing greater risks. Additionally, both industrial and agricultural uses of antimicrobials have been tied to the development of antibiotic resistant bacteria that then can become part of normal flora. With limited new antibiotics in the drug pipeline, especially those with novel mecha-nisms, treating these infections caused by resistant organisms can prove quite difficult and a reliance of therapies with greater toxic-ity profiles becomes more prevalent. Antimi-crobial stewardship is a term tossed around increasingly, and will be one of the best meth-ods to combat this growing problem.
Antimicrobial stewardship refers to the coordinated efforts of an interdisciplinary group focused on improving antimicrobial use. This group typically consists of an infectious diseases physician and pharmacist acting as chair and co-chair, with representation

IPSF Phuture 20154
If no measurements had been taken what do you suggest could help reduce the abuse/misuse?
• Education of prescribers about the negative impact of inappropriate prescribing
• Develop algorithms and pathways to guide empiric antibiotic selection
How does your country train pharmacists to be experts in infectious diseases and antibiotic stewardship?
• Residency programs – 1st year general and 2nd year advanced specialty training
• Fellowship programs• Antimicrobial stewardship courses
offered through various organiza-tions (i.e. MAD-ID, SIDP)
• Informal training of current pharmacist staff by one or more pharmacists with advanced ID training
• Pharmacy school curriculum
What are the types of board certifications or training programs available after graduation?
• BCPS (Board Certified Pharmacotherapy Specialists)
• Added Qualifications – Infectious Diseases (AQ-ID)• Board certification by test
coming soon through BPS• ASP training programs with
certification through MAD-ID and SIDP to name a few
What are the requirements for completing such programs?
• BCPS – complete PGY-1 or have 3-years of practice experience• AQ-ID – BCPS + 2 years minimum
of ID experience after terminal training program with portfolio of projects, talks, etc. submitted for review
• ASP programs – anyone can take the course; some requirements of pro-ject related to ASP completed with portfolio for review prior to certifi-cate designation.
What are the roles/responsibilities of ID clinical pharmacists in your country?
• Traditional• Clinical rounding with ID services• Review of culture data• Review of antibiotic usage• Development of antimicrobial re-
lated initiatives, protocols, path-ways, order sets, etc. to promote the appropriate use of antimicro-bials
• Patient monitoring for efficacy/toxicity
• Dose optimization recommenda-tions
• Research • Infection prevention and epide-
miology• Education and precepting
• Non-traditional roles• Epidemiology and infection pre-
vention strategies• Assisting in legislation related to
ASPs and promoting new drug development
Phut
ure
IPSF Phuture 2015 5
What are the policies/strategies for implement-ing ASP?
• Tiered restriction policy• Short term – Reduce inappropri-
ate use of broad spectrum antibi-otics
• Long term – Halt/reverse resist-ance patterns and decrease CDAD
• Dose optimization• Short term – Improve patient
outcomes• Long term – Slow resistance
development
How is technology/innovation implemented to combat AMR?
• Rapid diagnostics • Rapid identification of bacteria,
CDAD, resistance mechanisms • Facilitate quicker de-escala-
tion of therapy and/or get patients on correct therapy for resistant infections quickly
• Biomarkers• Procalcitonin: optimize dura-
tion of therapy to shortest necessary for infection reso-lution to prevent over expo-sure which causes longer stays, greater risk of side effects, higher CDAD risk and increased resistance
• Infection surveillance programs that monitor culture data and antibiotic use and can quickly flag mismatches to prioritize interventions and improve effi-ciency of ASPs
• Clinical decision support

IPSF Phuture 20156
IPSF Treasurer 2013-15
Coming Together in the Fight AgainstAntimicrobial ResistanceAs with all effective therapies, the basis of antimicrobial therapy is that it specifically targets the pathogen and leaves the host cells unharmed. The discovery of the first antibiotic penicillin in 1928 by Alexander Fleming not only led to multiple Nobel prizes in this field of pharmaceutical research, but also started a new era of medicine. Nowadays we cannot imagine a time without antimicrobial drugs.
However, herein lies a problem. With so many antimicrobial drugs being used these days, animals are being given a wide range of antibiotics prophylactically and the pathogens have an increased opportunity to prove Darwin’s Theory of Evolution. “Superbugs” pop up in hospitals all over the world (e.g. MRSA) and numerous bacteria become resistant to antibiotics. Furthermore, the initial prescribing guidelines may not have accounted for the risks of antimicrobial resistance. It is only in recent years that there is a shift towards a stringent focus with regards to antimicrobial prescribing guidelines and antimicrobial stewardship. Patients not adhering to their prescribed regimens are also increasing the risk for resistance.
This short review will give an overview on what is being done to counteract this antimicrobial resistance in modern day pharmaceutical research, with a focus on antibacterial agents or antibiotics.
To find out where opportunities lie in order to outsmart pathogens, it is vital to figure out why resistance happened in the first place.
What is happening in the fight against resistance?
Interestingly, Brad Spellberg described in a short article in 2014 that the failure in the battle against bacterial pathogens is largely caused by the failure of the antibiotic market.1 Fewer new antibiotics are arriving on the market in the recent decade compared to previously. Over the past 30 years, there has been a 90% decline in new approvals of antibiotics alone.2 Three key points play a role here: 1) saturation of the antibiotic market have resulted in considerable barriers to discovering new antibiotics. With the “easily discovered” drugs already on the market, the scientific complexity to find novel targets is becoming more risky and time-consuming. 2) Due to the short use of antibiotics, research and development costs are very high in comparison to the profits made. 3) Extra regulations and an impractical trial design by the FDA has resulted in a difficulty of setting up the right clinical trials and a lot of discussions about the results, and are therefore less attractive to pharmaceutical companies.1
Back to the science that is being done. Over the last few years, research has shifted
Laurens Oort, MSc.

Phut
ure
IPSF Phuture 2015 7
away from the discovery of new generation antibiotics towards research focused on the reason behind the antibiotic resistance and how to effectively utilize current antibiotics. We have become dependent on antibiotics to eradicate infectious diseases of bacterial origin. Couple this dependency with the previously mentioned market barriers in research and development, it is no surprise that this shift in strategy has occurred.
SynergyOne very simple solution is utilizing a combination of available antimicrobial agents, focusing on different synthesis pathways within bacterial survival.3 As the effects of the individual antibiotics are generally well known, research only needs to elucidate the underlying mechanism of these drug-drug interactions. Some combinations might cancel each other out (i.e. antagonistic interactions), but others might show a synergistic interaction favourable to be used as antibacterial therapies. Unfortunately, investigating high numbers of drugs and their optimal combinations rapidly becomes prohibitive due to a combinatorial explosion of experiments required.3 Progress is being made in this field, however, with the use of predicting models to reduce the number of possible combinations and the effective use of large high throughput studies to generate a large data sets.4
This approach is convenient in the battle against antimicrobial resistance as it is a relatively rapid solution and increases treatment efficacy against the current resistant bacteria and therefore controls the resistance evolution.3 The downside of this approach is the transient factor, as it does not stop resistance or shed light on how resistance happened. Furthermore, it might increase the prevalence of multidrug resistant bacteria since when it does become resistant, it will
have resistance to more than one antibiotic, bringing us further behind against the com-plex problem.
NanomoleculesWith possible mechanisms of drug resist-ance like alteration of metabolic pathways or reduced accumulation of the drug by an altered pharmacokinetic balance, even the most effective antibiotic can be rendered use-less. Still, this does not need to be the end of these drugs. The resistance pathways can be reversed or bypassed relatively easily without the need of altering the drug. Nanoparticles can play a crucial role as carriers of antibiotics or can be applied as antibiotic agents them-selves.5 A wide range of building blocks like polymers, metals and lipids can ideally be made into nanoparticles.
Nanoparticles by themselves act along two major lethal pathways against bacteria, a) being the disruption of the membrane poten-tial, making holes in the membrane which causes the bacterium to lose crucial survival elements; and b) the production of reactive oxygen species – or free radicals – instigating DNA damage inside the bacteria.6
Metallic nanoparticles are being used already as antibacterial agents, even without fully understanding the mechanism of action. Metal-containing nanoparticles are hypoth-esized to make holes in the bacterial cell wall in Gram-negative bacteria by increasing the membrane permeability and inactivating the respiratory process chain. Once inside the bacterial membrane, the metal ion can then bind to sulfur or nitrogen in the thiol or amino groups in amino acids, thereby disrupting protein structures vital to cell survival.7,8 Nano-particles are especially effective against bio-films, which are colonies of bacteria or fungi that adhere to a surface and are protected by a layer of extracellular polymer matrix.9

IPSF Phuture 20158
The downside of using these particles is the potential toxicity for the carrier, i.e. cytotoxicity for human cells.
A novel aspect of using nanoparticles against antimicrobial resistant bacteria is to employ the particles in combination with other antibiotic agents. The binding effect of the nanoparticles to the biofilm can, at the same time, serve as a delivery mechanism for antibiotics that would otherwise be unable to pass through the biofilm via their original delivery method. It is notable that the formation of biofilms changes the physiology of the cells in such a way, that even elevated concentrations of antimicrobial agents typically capable of killing the individual parts are rendered ineffective against the biofilm as a whole, without the use of nanoparticles.10 Due to the relatively unspecific mode of action of nanoparticles, it is advantageous to use them in situations where resistance might occur. For this reason, efforts are being made to apply nanoparticles to surfaces of medical devices, fibers and textiles, rendering them antimicrobial.6
Manipulation of natural anti-infective methodsHumans are not completely at the mercy of bacteria when infected. Antimicrobial peptides (AMPs) are part of our first-line of defence. These short peptides express strong antimicrobial activity against a broad spectrum of bacteria. In addition to intracellular targets within the bacterial cell where they inhibit protein synthesis, cell wall synthesis or DNA replication among others, antimicrobial peptides simultaneously stimulate non-inflammatory host immune responses.11 Cationic AMPs show low risk of resistance development and are therefore a promising class of new antimicrobial agents against resistant pathogens. Research currently focuses on finding the fragment within known AMPs in order to modify the
AMP to enhance peptide stability without reducing the viability of the host cells.11
Alternatively, using viruses to infect and kill resistant bacteria has also become a promis-ing approach to replace antimicrobial drugs. Supposedly bacteriophages are able to infect bacteria and utilize the host machinery either for reproduction or integration in the bacterial DNA. Due to the shift to reproduction of the viral phage, the bacterial biological functions are subverted and the host undergoes lysis and dies while liberating a large number of new phages ready to infect the next bacterial cell.12 A more patient option, but very interest-ing from a research perspective, is the integra-tion of so-called “dominant sensitive genes” into the bacterial DNA.13 With some simple genetic engineering, certain resistant bacteria can be made sensitive again against antibi-otic agents. This may hold key advantages to revive the use of old generation antibiotics leading to the use of phage biotechnology synergistically with antibiotics.
Research into the pharmacokinetics and effi-cacy in humans is unfortunately lacking. Fur-thermore, concerns over the use of phages as therapeutic agents include the narrow host range, the potential resistance against the phages or neutralization by the spleen/liver.13
Conclusions and considerations for the futureThe three stated methods to battle antimicrobial resistance are only a few aspects within pharmaceutical research against resistance. It has become clear that the battle we thought we were about to win 50 years ago is not yet over. Bacteria have been evolving for millions of years and have the major advantage that they are fast growing single organisms. Regrettably, with a pharmaceutical industry not too keen on investing into antimicrobial agents with the current market barriers, the world has been sleeping while bacteria

Phut
ure
IPSF Phuture 2015 9
continue to evolve. In 2014, the WHO pub-lished a global report on antimicrobial resistance that for the first time, highlights the magnitude of this issue and the state of surveillance globally.14
It is possible that the battle may never be over. As demonstrated via previous strategies, the key to winning does not rest only with the development of new drugs. The solution may involve uniting the right elements of pharmaceutical research to develop intelligent combinatorial approaches for multiple simultaneous and complementary therapies, effective delivery methods or recycling nature’s own methods against resistant bacteria. Combination approaches should extend beyond biologically active molecules to include smart controlled delivery strategies.15
References
1. Spellberg, B. The future of antibiotics. Crit. Care18, 228 (2014).2. Shlaes, D. M., Sahm, D., Opiela, C. & Spellberg, B. The FDA reboot of antibiotic development. Antimicrob. Agents Chem-other.57, 4605–4607 (2013).3 Bollenbach, T. ScienceDirect Antimicro-bial interactions : mechanisms and implica-tions for drug discovery and resistance evolu-tion.4. Wood, K., Nishida, S., Sontag, E. D. & Cluzel, P. Mechanism-independent method for predicting response to multidrug combi-nations in bacteria. Proc. Natl. Acad. Sci.109, 12254–12259 (2012).5. Kandi, V. & Kandi, S. Antimicrobial prop-erties of nanomolecules : potential candidates as antibiotics in the era of multi-drug resist-ance. 1–5
6. Beyth, N., Houri-Haddad, Y., Domb, A., Khan, W. & Hazan, R. Alternative Antimicrobial Approach: Nano-Antimicrobial Materials. Evi-dence-Based Complement. Altern. Med.2015, 1–16 (2015). 7. Kumar, D. A., Palanichamy, V. & Roopan, S. M. Photocatalytic action of AgCl nanoparticles and its antibacterial activity. J. Photochem. Photobiol. B Biol.138, 302–306 (2014).8. Blecher, K., Nasir, A. & Friedman, A. The growing role of nanotechnology in combating infectious disease. Virulence2, 395–401 (2011).9. Neethirajan, S., Clond, M. A. & Vogt, A. Medical Biofilms - Nanotechnology Approaches. J. Biomed. Nanotechnol.10, 2806–2827 (2014).10. Jefferson, K. K. What drives bacteria to produce a biofilm? FEMS Microbiol. Lett.236, 163–173 (2004).11. Strempel, N., Strehmel, J. & Overhage, J. Potential Application of Antimicrobial Peptides in the Treatment of Bacterial Biofilm Infections. 67–84 (2015).12. Jassim, S. a a & Limoges, R. G. Natural solution to antibiotic resistance: Bacteriophages ‘The Living Drugs’. World J. Microbiol. Biotechnol.30, 2153–2170 (2014).13. Edgar, R., Friedman, N., Shahar, M. M. & Qimron, U. Reversing bacterial resistance to antibiotics by phage-mediated delivery of dominant sensitive genes. Appl. Environ. Microbiol.78, 744–751 (2012).14. WHO. ANTIMICROBIAL RESISTANCE Global Report on Surveillance 2014. World Heal. Organ. (2014).15. Brooks, B. D. & Brooks, A. E. Therapeutic strategies to combat antibiotic resistance. Adv. Drug Deliv. Rev.78, 14–27 (2014).
IPSF Phuture 201510
Assistant Microbiologist, Mouloud Maammeri University, Algeria
Emergence of Antimicrobial-Resistant Bacteria in the Community:Public Health in CrisisIntroductionWhereas bacterial resistance to antibiotics is breaking records in hospitals, the community has been relatively spared from multidrug resistant microorganisms. However, since the appearance of extended spectrum antimicrobials in community pharmacies such as third and fourth generation cephalosporins, fluoroquinolones and aminoglycosides, these substances are frequently misused and prescribed inappropriately, either as monotherapy or in conjunction with other antimicrobials. For many years now, all around the world, reports of severe community-acquired infections are increasing such as methicillin resistant-toxicogenic Staphylococcus aureus, Streptococcus pneumoniae with diminished susceptibility to penicillin, broad-spectrum beta-lactamase producing Enterobacteriaceae and extensively drug resistant Mycobacterium tuberculosis. This piece aims to shine light on the situation of antimicrobial resistance in the Algiers region, choosing urinary tract infections isolates as an example of study.
Patients and MethodsOur private clinical laboratory is situated east of the capital – Algiers is in an agricultural region of important urbanization and drains newcomers from different origins: nationally, from the Maghreb region (Western Sahara) but also from sub-Saharan region (Mali, Niger).
Our study spreads over a period of 27 months (January 2013 –March 2015). The samples were processed following standard bacteriological methods, antimicrobial susceptibility tests were performed in accordance with clinical, laboratory and standard institute recommendations.
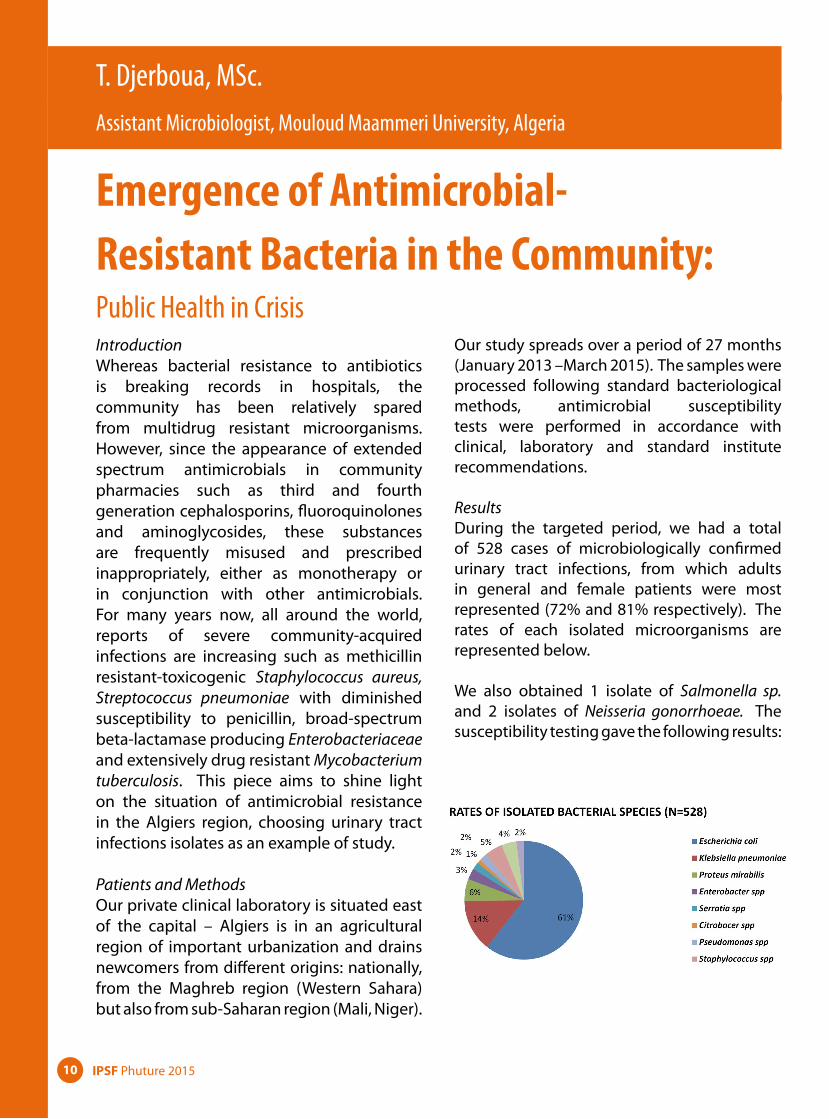
ResultsDuring the targeted period, we had a total of 528 cases of microbiologically confirmed urinary tract infections, from which adults in general and female patients were most represented (72% and 81% respectively). The rates of each isolated microorganisms are represented below.
We also obtained 1 isolate of Salmonella sp. and 2 isolates of Neisseria gonorrhoeae. The susceptibility testing gave the following results:
T. Djerboua, MSc.

Phut
ure
IPSF Phuture 2015 11
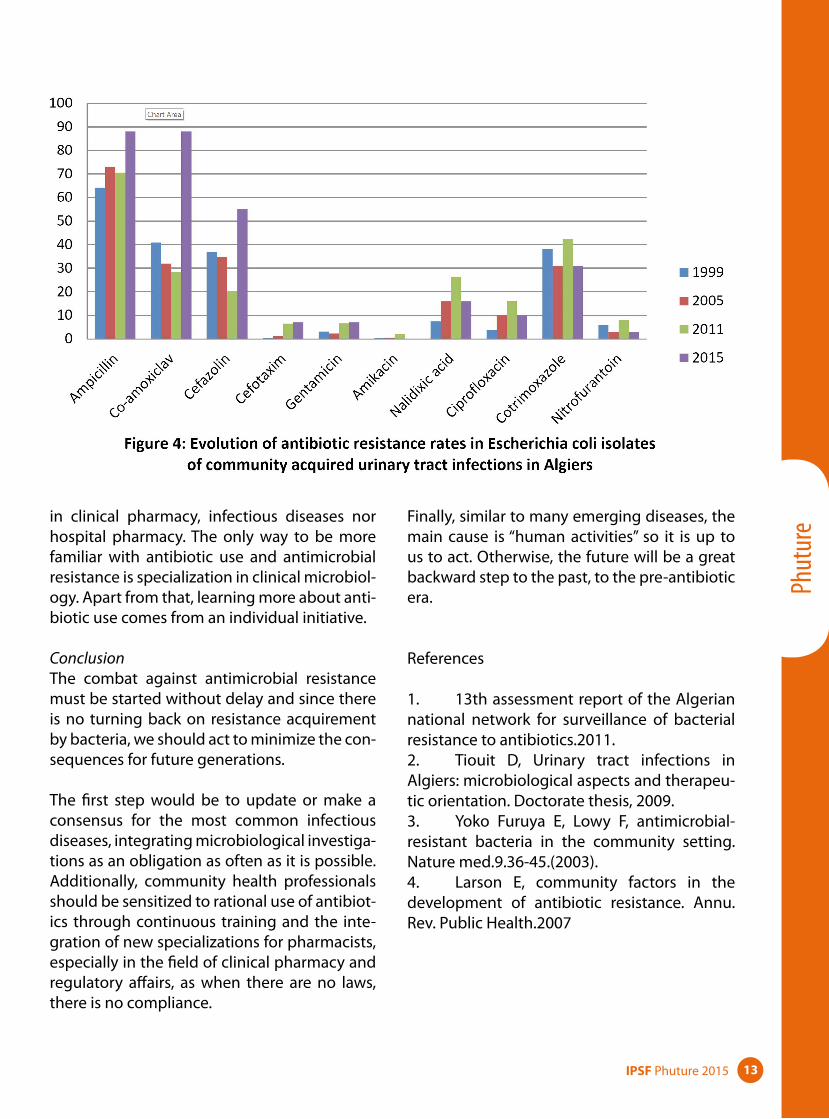
• Escherichia coli (Figure 1) • Among the 17 isolates that showed resistance to third generation cephalosporins
(Cefotaxime), 15 were ESBL producers, all in pediatric patients.
• Klebsiella pneumoniae (Figure 2) • Antimicrobial resistance in this germ is more important, 9% of isolates are multidrug
resistant, and up to 19% are resistant to third generation cephalosporins, the resist-ance to fluoroquinolones is also higher (22%).

IPSF Phuture 201512
DiscussionThe evolution and distribution of antimicrobial resistance in time, space and population is a dynamic process affected by many different factors, whether direct (abusive antibiotic con-sumption) or indirect (emergence and spread of resistance from hospitals to community, food industry)
Figure 3: Factors that contribute to the spread of antimicrobial resistance in the community
In Algeria, antimicrobial resistance is in a con-stant expansion. In this study, the increase is noted from year to year and from childhood to adulthood. We also noticed in our study that for some antibiotics, resistance is more predominant in a population. For example, third-generation cephalosporin resistance is mainly seen in children, probably due to the recent introduction of this class of antibiotics to community pharmacies. Fluoroquinolone resistance, on the other hand, is found only in adults in whom it is widely used. For example, many patients suspected of sexually transmit-ted diseases will benefit from an ambulatory prescription of fluoroquinolones without any microbiological investigation.
These two groups of antibiotics, extremely potent, and of vital importance in case of severe infections, experience an unprecedented use and the consequences are already showing up. It is very hard to appreciate the real impact since there are very few similar prospective studies. Data is often scarce, sparse, and some-times contradictory. While risk factors for anti-microbial resistance in community are being emphasized in many studies, pointing out the cause is much more difficult since numerous healthcare professionals are involved.
Algeria’s policy on combating antibacterial resistance is, at the moment, an individual or group initiative. In fact, there are no laws, plans or recommendations on how to face this public health problem. For now, the only organization dedicated to this is a network of microbiolo-gists, created in 2002, called the “Algerian net-work of surveillance of microbial resistance to antibiotics”. The actions, however, are very lim-ited due to many administrative and budget limitations.
In Algeria, pharmacists’ interventions on pre-scriptions is very limited as pharmacy studies are still very basic. There are no specialization
Phut
ure
IPSF Phuture 2015 13
in clinical pharmacy, infectious diseases nor hospital pharmacy. The only way to be more familiar with antibiotic use and antimicrobial resistance is specialization in clinical microbiol-ogy. Apart from that, learning more about anti-biotic use comes from an individual initiative.
ConclusionThe combat against antimicrobial resistance must be started without delay and since there is no turning back on resistance acquirement by bacteria, we should act to minimize the con-sequences for future generations.
The first step would be to update or make a consensus for the most common infectious diseases, integrating microbiological investiga-tions as an obligation as often as it is possible. Additionally, community health professionals should be sensitized to rational use of antibiot-ics through continuous training and the inte-gration of new specializations for pharmacists, especially in the field of clinical pharmacy and regulatory affairs, as when there are no laws, there is no compliance.
Finally, similar to many emerging diseases, the main cause is “human activities” so it is up to us to act. Otherwise, the future will be a great backward step to the past, to the pre-antibiotic era.
References
1. 13th assessment report of the Algerian national network for surveillance of bacterial resistance to antibiotics.2011.2. Tiouit D, Urinary tract infections in Algiers: microbiological aspects and therapeu-tic orientation. Doctorate thesis, 2009.3. Yoko Furuya E, Lowy F, antimicrobial-resistant bacteria in the community setting. Nature med.9.36-45.(2003).4. Larson E, community factors in the development of antibiotic resistance. Annu. Rev. Public Health.2007
IPSF Phuture 201514
Genetic Immunization:Fiction to Fact CRISPR Technology
Science fiction has been leading many inven-tions recently by sparking the imagination of scientists to reach for the impossible. But is it really possible to create modifications to human DNA and preventing a cell from being infected? Surprisingly the answer is yes, using the Clustered Regularly Interspaced Short Palin-dromic Repeat (CRISPR).
This technology was inspired by a natural defense system in bacteria against viruses. The CRISPR technology did not only give Emmanuelle Charpentier & Jennifer Doudna several international awards, but brought new promise to genetic engineering, gene editing and a way to avoid diseases that are no longer responsive to antibiotics or have no definite cure, such as HIV/AIDS.
An overview: • When a bacterium is invaded by a
virus, it is triggered to produce two arms of short RNA in a sequence matching that of the viral DNA, form-ing a complex with cas9 protein (nat-urally present): an enzyme that can cleave DNA.
• The matching sequence on the RNA (known as the guide RNA) finds its way to the viral DNA. The cas9 then finds its way to the viral DNA, hence disabling the virus.
• Scientists discovered that this method could be applied to any DNA, not only viral, by leading the cas9 enzyme to any DNA sequence through alteration of the guide RNA sequence to target an exact location of choice .
• Fortunately, this is applicable in living cells as well and will not cause cell fail-ure.
• The resulting complex will bind to the virus DNA once it enters the nucleus, locking onto a short sequence known as the PAM.
• Cas9 will unzip the DNA and match it to the target RNA. Hence, it enhances the chance of creating a mutation in the viral DNA and making it unrec-ognizable by the complex so that it will no longer be cut. Should the DNA fuse back without the formation of a mutation, the complex will attempt to cleave it time after time until a muta-tion has occurred.
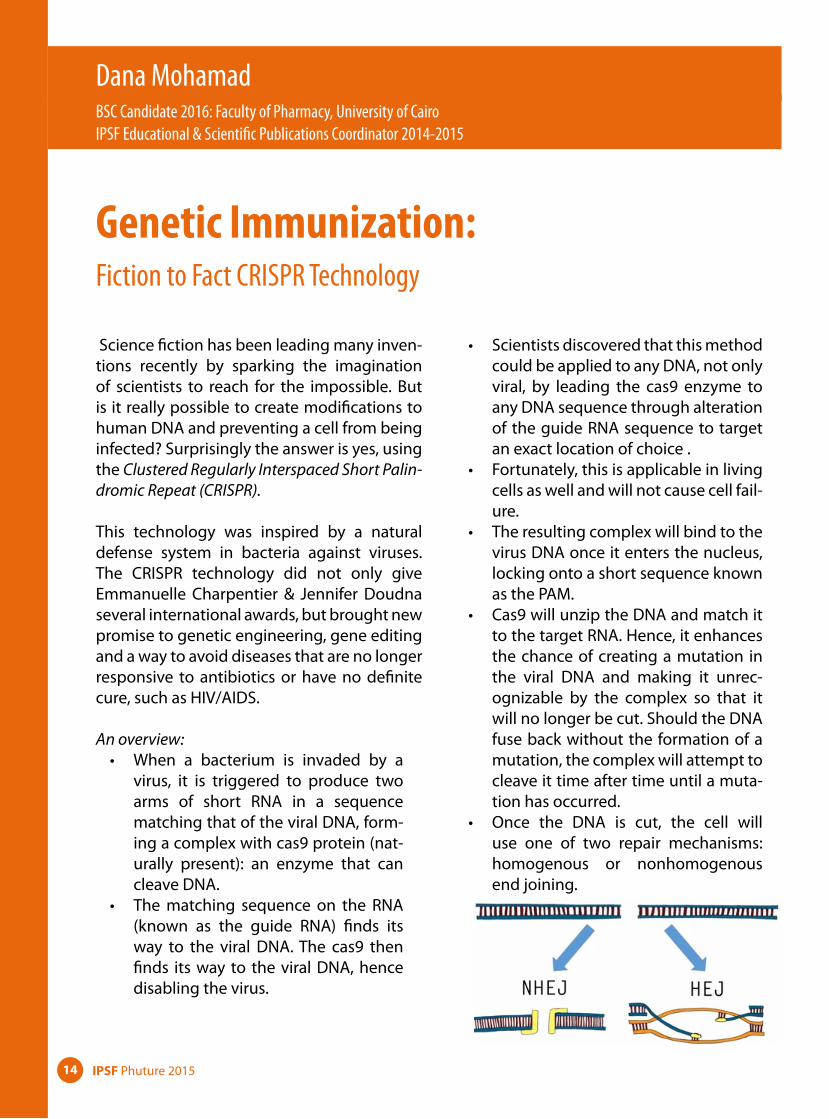
• Once the DNA is cut, the cell will use one of two repair mechanisms: homogenous or nonhomogenous end joining.
Dana Mohamad BSC Candidate 2016: Faculty of Pharmacy, University of Cairo IPSF Educational & Scientific Publications Coordinator 2014-2015
Phut
ure
IPSF Phuture 2015 15
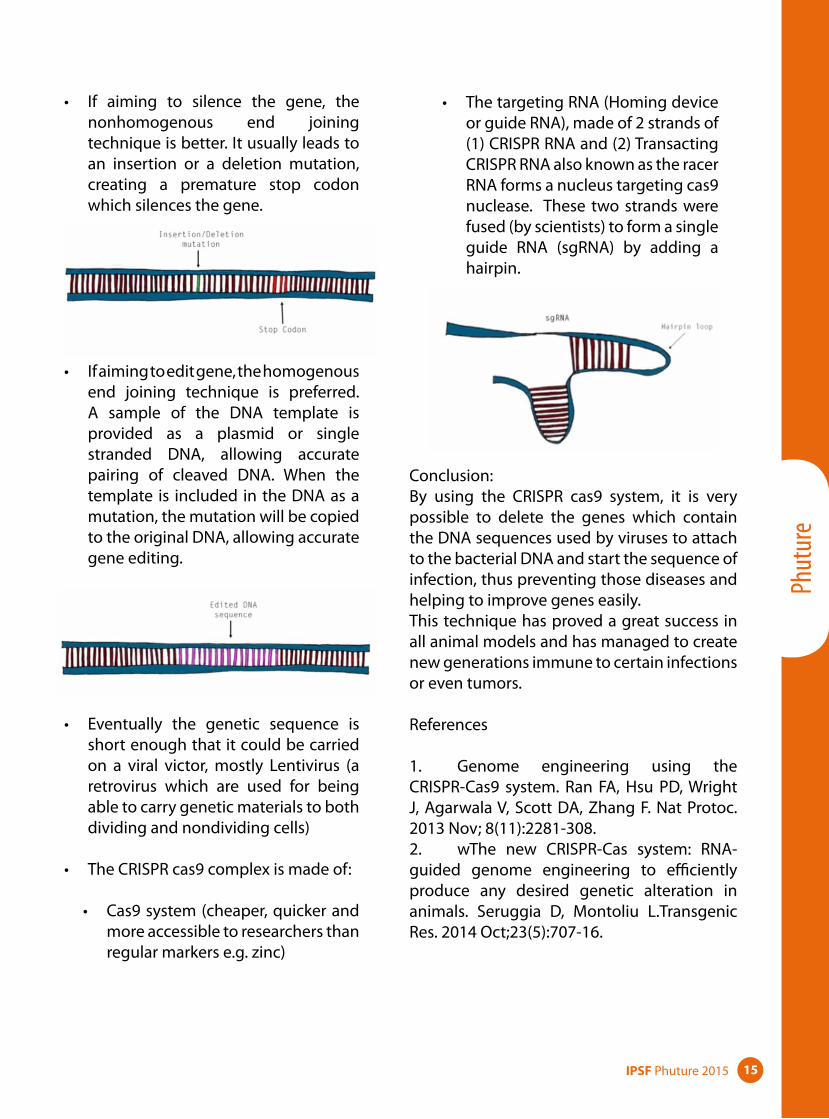
• If aiming to silence the gene, the nonhomogenous end joining technique is better. It usually leads to an insertion or a deletion mutation, creating a premature stop codon which silences the gene.
• If aiming to edit gene, the homogenous end joining technique is preferred. A sample of the DNA template is provided as a plasmid or single stranded DNA, allowing accurate pairing of cleaved DNA. When the template is included in the DNA as a mutation, the mutation will be copied to the original DNA, allowing accurate gene editing.
• Eventually the genetic sequence is short enough that it could be carried on a viral victor, mostly Lentivirus (a retrovirus which are used for being able to carry genetic materials to both dividing and nondividing cells)
• The CRISPR cas9 complex is made of:
• Cas9 system (cheaper, quicker and more accessible to researchers than regular markers e.g. zinc)
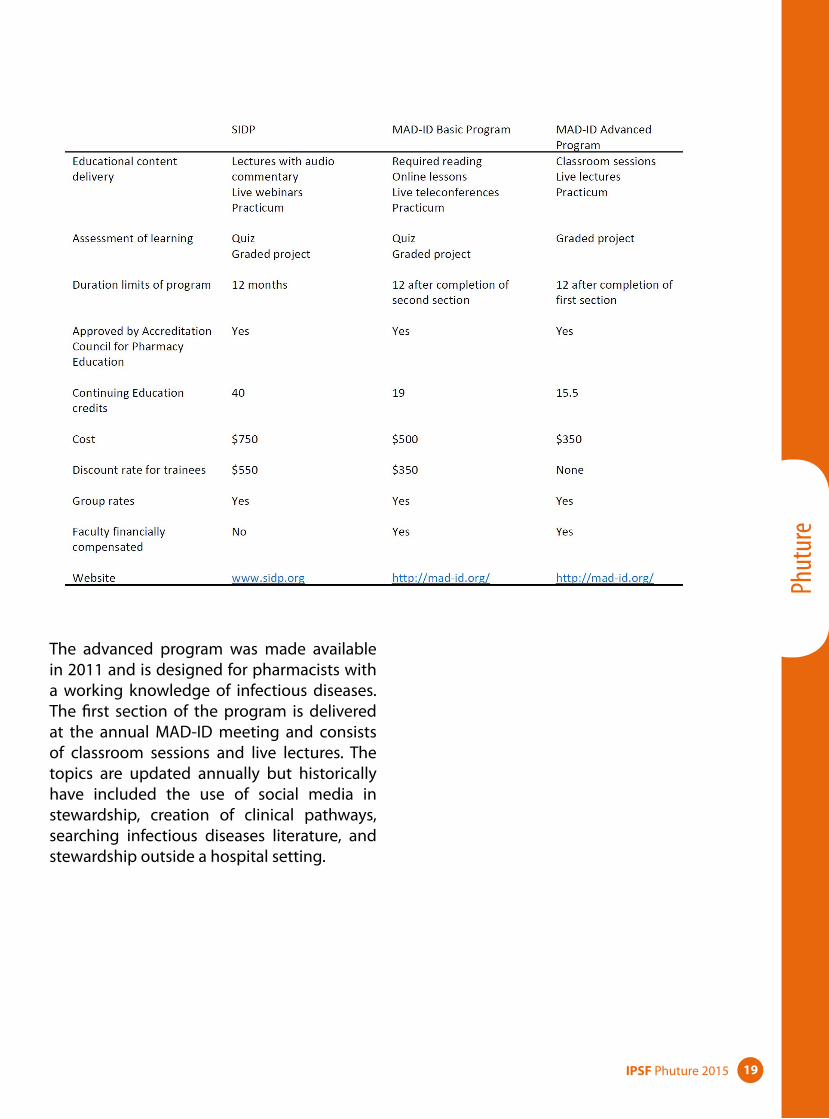
• The targeting RNA (Homing device or guide RNA), made of 2 strands of (1) CRISPR RNA and (2) Transacting CRISPR RNA also known as the racer RNA forms a nucleus targeting cas9 nuclease. These two strands were fused (by scientists) to form a single guide RNA (sgRNA) by adding a hairpin.
Conclusion:By using the CRISPR cas9 system, it is very possible to delete the genes which contain the DNA sequences used by viruses to attach to the bacterial DNA and start the sequence of infection, thus preventing those diseases and helping to improve genes easily.This technique has proved a great success in all animal models and has managed to create new generations immune to certain infections or even tumors.
References
1. Genome engineering using the CRISPR-Cas9 system. Ran FA, Hsu PD, Wright J, Agarwala V, Scott DA, Zhang F. Nat Protoc. 2013 Nov; 8(11):2281-308.2. wThe new CRISPR-Cas system: RNA-guided genome engineering to efficiently produce any desired genetic alteration in animals. Seruggia D, Montoliu L.Transgenic Res. 2014 Oct;23(5):707-16.

IPSF Phuture 201516
University of Porto, Portugal
Enterococcus species:A Matter of Concern
Antimicrobial resistance (AMR) is a serious threat to public health, compromising our ability to prevent, treat and avoid clinical complications of a wide range of infections. Several entities, like the European Centre of Disease Prevention and Control (ECDC) or World Health Organization (WHO), are com-mitted in assessing and communicating this emerging problem, publishing surveillance data and promoting awareness strategies every year.
Among the bacteria more commonly associ-ated with nosocomial infections, there areEnterococcus species, particularly Enterococ-cus faecalis and Enterococcus faecium. These hospital-related enterococci are usually resist-ant to several antimicrobials including vanco-mycin, which results in very limited treatment options. 1-4
In the last decade, the European mean per-centage of vancomycin-resistant Enterococ-cus faecium (VRE) presented a decreasing trend. However, there are significant differ-ences between countries (0-42.7%), Portugal being one of those having higher incident rates (22.0% in 2013). 5
The mechanism of acquired vancomycin resistance in Enterococcus faecium is morefrequently associated with the vanA or vanB gene clusters, which are located in mobile genetic elements and thus can be transferred between isolates. VanA is the one more freq- uently identified in Portugal.6 This is of con-cern, since genus borders may be crossed and vanA transference may even occur in more pathogenic bacteria, like methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Staphylococcus aureus (VRSA). Although this is a very rare event, it has already been reported in some countries like U.S.A, Iran and Portugal.7-12 The nosoco-mial strains of enterococci, namely VRE, also belong to specific clonal lineages enriched with several features and appearing to be bet-ter adapted to the hospital setting. 2-4
Therefore, the dissemination of these VRE strains and/or their resistance genes to other pathogenic bacteria like MRSA, contribute to the emergence of VRSA and may cause seri-ous consequences for health care security, since vancomycin is an antibiotic of last resort used for treating MRSA infections.
Elsa Martins

Phut
ure
IPSF Phuture 2015 17
References
1. Gilmore MS, Lebreton F, van Schaik W. Genomic transition of enterococci from gut commensals to leading causes of multidrug-resistant hospital infection in the antibi-otic era. Current opinion in microbiology. 2013;16(1):10-6.2. Arias CA, Murray BE. The rise of the Enterococcus: beyond vancomycin resistance. Nature reviews Microbiology. 2012;10(4):266-78.3. Top J, Willems R, Bonten M. Emergence of CC17 Enterococcus faecium: from com-mensal to hospital-adapted pathogen. FEMS immunology and medical microbiology. 2008;52(3):297-308.4. Werner G, Coque TM, Franz CM, Grohm-ann E, Hegstad K, Jensen L, et al. Antibiotic resistant enterococci-tales of a drug resistance gene trafficker. International journal of medi-cal microbiology : IJMM. 2013;303(6-7):360-79.5. European Centre for Disease Preven-tion and Control. Antimicrobial resistance sur-veillance in Europe 2013. Annual Report of the European Antimicrobial Resistance Surveil-lance Network (EARS-Net). Stockholm: ECDC; 2014.6. Freitas AR, Novais C, Tedim AP, Francia MV, Baquero F, Peixe L, et al. Microevolution-ary Events Involving Narrow Host Plasmids Influences Local Fixation of Vancomycin-Resistance in Enterococcus Populations. PLoS ONE. 2013;8(3):e60589.7. Novais C, Freitas AR, Sousa JC, Baquero F, Coque TM, Peixe LV. Diversity of Tn1546 and its role in the dissemination of vancomycin-resistant enterococci in Portugal. Antimicrobial agents and chemotherapy. 2008;52(3):1001-8.
8. Willems RJL, Top J, van Santen M, Rob-inson DA, Coque TM, Baquero F, et al. Global Spread of Vancomycin-resistant Enterococcus faecium from Distinct Nosocomial Genetic Complex. Emerging Infectious Diseases. 2005;11(6):821-8.9. Centers for Disease Control and Prevention Vancomycin- resistant Staphylococcus aureus—New York, 2004. MMWR Morb Mortal Wkly Rep. 2004;53:322–3gene. N Engl J Med. 2003;348:1342–7.10. Chang S, Sievert DM, Hageman JC, Boul-ton ML, Tenover FC, Downes FP, et al. Infection with vancomycin-resistant Staphylococcus aureus containing the vanA resistance gene. N Engl J Med. 2003;348:1342–7.11. Tenover FC, Weigel LM, Appelbaum PC, McDougal LK, Chaitram J, McAllister S, et al.Vancomycin-resistant Staphylococcus aureus isolate from a patient in Pennsylvania. Antimicrob Agents Chemother. 2004;48:275–80.12. Dezfulian A, Aslani MM, Oskoui M, Farrokh P, Azimirad M, Dabiri H, et al. Identification and Characterization of a High Vancomycin-Resistant Staphylococcus aureus Harboring VanA Gene Cluster Isolated from Diabetic Foot Ulcer. Iranian Journal of Basic Medical Sciences. 2012;15(2):803-6. 13. Friães A, Resina C, Manuel V, Lito L, Ramirez M, Melo-Cristino J. Epidemiological survey of the first case of vancomycin-resistant Staphylococcus aureus infection in Europe. Epidemiology & Infection. 2015;143(04):745-8.

IPSF Phuture 201518
Assistant Professor, Department of Clinical Pharmacy University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences
Review of Antimicrobial StewardshipCertificate Programs in the United StatesThere are two antimicrobial stewardship cer-tificate programs in the United States. The first program was developed in-house by members of the Society of Infectious Diseases Pharmacists (SIDP). SIDP is an association of pharmacists and other healthcare profession-als that promote the judicial use of antimicro-bials through education, research, post-grad-uate education, and legislation. Content for the certificate program was first developed in 2009 and underwent a comprehensive update and peer review in 2014. The continu-ing education company ProCE now houses and distributes the certificate. SIDP members still create and maintain all the content which consists of three phases.
Phase 1 consists of 24 hours of pre-recorded lectures and serves as the self-learning com-ponent. Content includes modules on micro-biology, pharmacology, pharmacokinetics (PK) and pharmacodynamics (PD), disease states and treatments, stewardship interven-tions, measuring stewardship outcomes, and infection control. Phase 2 is a series of six live webinars. The webinar topics are an imple-mentation of a stewardship program, under-standing the hospital antibiogram, multidrug resistant organisms, rapid diagnostic tests, computer support systems, and stewardship program outcomes. Phase 3 is ten hours of practice skills that take place in the pharma-cist-owned clinic or institution where they
will implement a stewardship component, document the intervention, and report the intervention and findings to SIDP for review and approval.
The certificate program offered by Making a Difference In Infectious Diseases (MAD-ID) has two programs, basic and advanced. The basic program has three sections similar to the SIDP program. The first section is nine hours of online learning which includes read-ing three articles and four online lessons. The lessons are antimicrobial stewardship over-view, microbiology and antimicrobial PK/PD, mechanisms of antimicrobial resistance, and surveillance of resistance. The second section is another series of online lessons with an option to teleconference with faculty live. The topics of section two include epidemiology, advanced antimicrobial stewardship, public health, infection control, PK/PD at the bed-side, and de-escalation of antimicrobial regi-mens. The third and final section is a practical component where pharmacists select from a list of activities to be completed at their own clinic or institution.
Meghan Jeffres, PharmD
Phut
ure
IPSF Phuture 2015 19
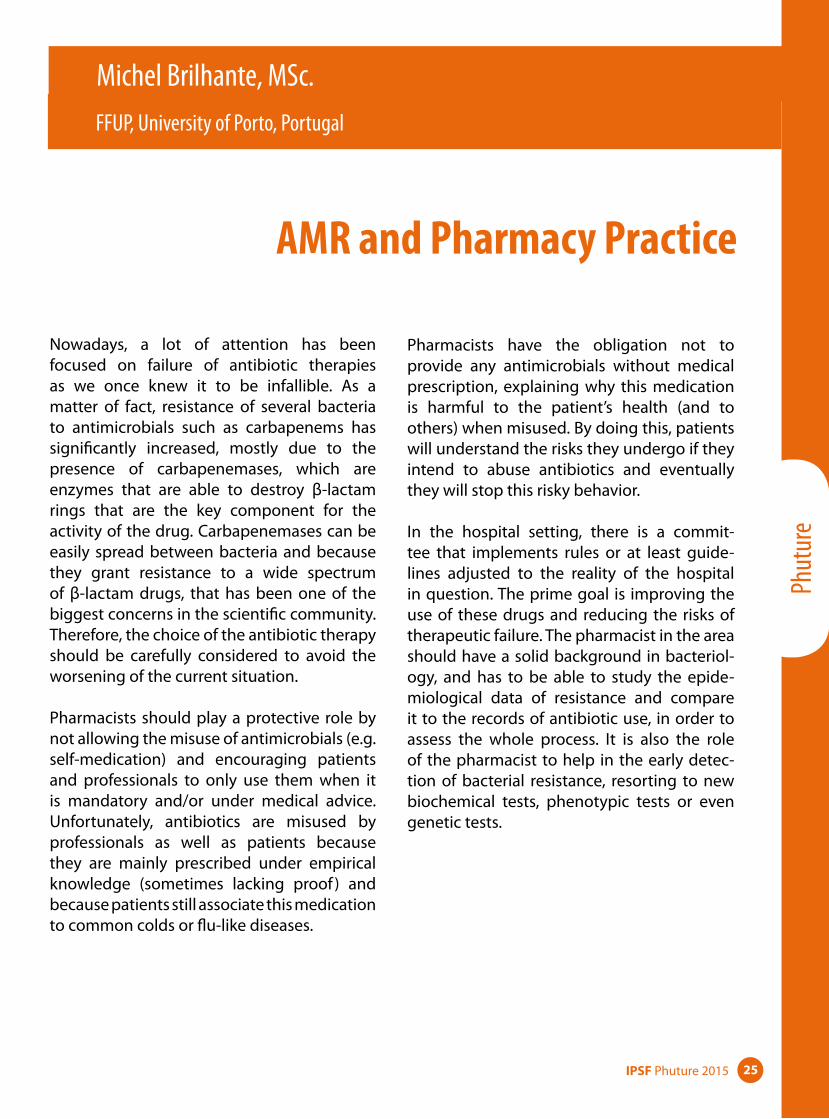
The advanced program was made available in 2011 and is designed for pharmacists with a working knowledge of infectious diseases. The first section of the program is delivered at the annual MAD-ID meeting and consists of classroom sessions and live lectures. The topics are updated annually but historically have included the use of social media in stewardship, creation of clinical pathways, searching infectious diseases literature, and stewardship outside a hospital setting.

IPSF Phuture 201520
Sylvia Lee, Detron M. Brown MPH, Obinna Okafor, Enaefe Ziregbe
The Inclusion of Clinical Pharmacist to Effectively Combat Antimicrobial ResistanceAccording to the World Health Organization (WHO), antimicrobial resistance (AMR) is the ability of a microorganism to render a drug ineffective that was previously used efficiently in treating an infection.1 Microbes include but are not limited to bacteria, fungi, and viruses. Many factors contribute to the spread of AMR, thus requiring coordinated action among healthcare workers.1 Even though AMR is not a novel issue, it remains a growing concern and challenge for professionals in the health-care realm. The number of first-line antimicro-bial medications available for effective treat-ment has dwindled, consequently leading to increased infection and mortality rates. Fear-ful of the national and global spread of AMR, the healthcare industry in the United States along with other countries and organizations are continually seeking out new and innova-tive collaborations and programs.
In January 2007, in an effort to expand and combat against AMR, the Infectious Disease Society of America (IDSA) and the Society for Healthcare Epidemiology of America (SHEA) developed new guidelines for the recom-mended personnel that should be included in the antimicrobial stewardship team.4 These guidelines suggested that both highly trained infectious disease physicians and pharmacists lead the infectious disease team.2 Upon publi-cation of these new guidelines, the Society of Infectious Disease Pharmacist (SIDP) and
the American College of Clinical Pharmacy (ACCP) produced guidelines outlining the steps for pharmacists to be trained in combat-ing infectious diseases and AMR.The roles of infectious disease clinical phar-macists have become increasingly perti-nent due to the increasing spread of AMR. Although there are several drug classes that if mismanaged can lead to AMR, antibiotics are of particular importance and are among the most misused drugs in the United States.2
Penicillin serves as one of the first recorded and commonly used antibiotics. After the mass production of penicillin for wounded soldiers during the end of World War II, the first recorded cases of antibiotic resistance occurred.2 Several debates have occurred concerning whether some bacteria devel-oped resistance to antibiotics or whether they have an innate resistance to antibiotics, but the major issue faced today is the explosion in the number of antibiotic resistance cases.2
According to the Center for Disease Control (CDC) at least two million people in the United States are infected with antibiotic resistant bacteria annually and as a result, 23,000 peo-ple die.2 Antibiotic misuse and abuse by clini-cians are a large contributing factor to AMR. Traditionally, clinicians may prescribe antimi-crobials without accurately diagnosing the infectious disease.4 This is typically because the symptoms can be life threatening and
Howard University, USA

Phut
ure
IPSF Phuture 2015 21
immediate treatment is needed, whereas properly diagnosing an infectious disease requires time consuming laboratory tests.5 Additionally, the use of antimicrobials in the United States are restricted but this is not the case in all countries.5
The aforementioned poor practices do not only contribute to AMR, but also include undesirable side effects and potential allergic reactions. A study conducted by the National Health Care and Safety Network of the CDC demonstrated that most nosocomial infec-tions are a result of bacteria that are resist-ant to multiple antibiotics.2 These infections include methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Entero-cocci (VRE), E.coli, and Enterobacter species.2
Preventative measures that can be imple-mented by healthcare providers to combat antibiotic resistance include obtaining cul-tures and prescribing antibiotics for the cor-rect dose, duration and reassessing prescrip-tions within 48 hours based on culture results and patient examination. Health care provid-ers should also document the dose, duration and indication for antibiotics prescribed while following good hand hygiene practices, and other infection control measures with every patient.2 It is important that proper preven-tative practices are employed because drug choices are limited due to antimicrobial drug resistance. AMR is a multi-tiered issue with a number of factors coming into play.
Antimicrobial resistance creates financial chal-lenges for all shareholders. Specifically, the cost associated with developing new drugs and regulations present obstacles in com-bating drug-resistant bacteria. In the United States, the “National action plan for combat-ing antibiotic-resistant bacteria” provides a roadmap to guide the nation in rising to this challenge.7
The vision of this plan is for the United States to work domestically and internationally to prevent, detect, and limit illness and death related to infections caused by antibiotic-resistant bacteria through implementing measures to mitigate the emergence and spread of antibiotic resistance and ensuring the continued availability of therapeutics for the treatment of bacterial infections.7 By 2020, this plan will ideally lead to a reduction in the incidence of serious threats, including but not limited to carbapenem-resistant Enterobacteriaceae (CRE), methicillin-resistant Staphylococcus aureus (MRSA), Clostridium difficile and human immunodeficiency virus (HIV).3 Along with improved antibiotic stewardship in various healthcare settings, the plan will include expanded surveillance and elimination of medically important antibiotics for growth promotion in animals.5
Despite the urgent need for new antibiotics, very few drugs exist in the drug development pipeline and commercial interests remain low. An intensified effort in research with regard to drug development will be required to facilitate clinical trials and attract investments. The plan will support research, provide regulatory guidance and encourage public/private partnerships. This will reduce the risks and obstacles faced by companies who are developing new antimicrobials and/or other medications..5
Prudent use of antibiotics in healthcare and agriculture is essential to slow the emergence of resistant microbes. Antibiotics are a very limited resource and preserving their useful-ness will require cooperation and engage-ment by healthcare providers, healthcare leaders, pharmaceutical companies, and patients. Prevention of resistance also requires rapid detection and control of infections and outbreaks across community and healthcare settings.

IPSF Phuture 201522
The United States has begun and continues to incorporate and evolve the roles of clinical pharmacists in infectious disease therapy. These pharmacists are able to serve in both administrative and clinical capacities. Administratively, they can oversee antibiotic restriction policies, surveillance of antibiotic use, and work on antimicrobial monographs. Clinically, they are able to help influence dosing, interpret laboratory results, and share their knowledge of microbiology. Clinical pharmacists have extensive training in medication therapy, and are required to do annual continuing education to further their knowledge and scope of practice. Including clinical pharmacists in the selection process of an appropriate drug regimen based on patient diagnostics and risk factors, benefit the patients and increase their chances of survival. Furthermore, programs ranging from residencies, to fellowships, to opportunities in earning additional degrees that expose pharmacists to infectious diseases and antibiotic stewardship programs, truly make pharmacists experts in mitigating the spread of AMR. There are no permanent solutions for AMR but a concerted effort among clinical pharmacists and other healthcare professionals, policy makers, and patients are required to effectively combat against antimicrobial resistance.
References
1. “Antimicrobial Resistance.” WHO. N.p., Apr. 2015. Web. 20 July 2015.2. Center for Disease Control and Preven-tion (2013). Antibiotic/Antimicrobial Resist-ance. Available from: http://www.cdc.gov/drugresistance/3. Davies, Julian, and Dorothy Davies. “Ori-gins and evolution of antibiotic resistance.” Microbiology and Molecular Biology Reviews 74.3 (2013): 417-433.4. Drew RH, White R, Macdougall C, Hermsen ED, Owens RC. Insights from the Society of Infectious Diseases Pharmacists on antimicrobial stewardship guidelines from the Infectious Diseases Society of America and the Society for Healthcare Epidemiology of America. Pharmacotherapy. 2009;29(5):593-607.5. Levy, Stuart B. “Factors impacting on the problem of antibiotic resistance.”Journal of Antimicrobial Chemotherapy 49.1 (2002): 25-30.6. Michael CA, Dominey-howes D, Lab-bate M. The Antimicrobial Resistance crisis: causes, consequences, and management. Front Public Health. 2014;2:145. Retrieved from https://www.whitehouse.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf7. 2015 National Action Plan for Combat-ing Antibiotic-Resistant Bacteria. Washing-ton, D.C.: The White House (US); 2015 Mar. 62p. Available from: https://www.whitehouse.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf

Phut
ure
IPSF Phuture 2015 23
Introduction As medication experts, pharmacists along with pharmacy students can have a meaningful positive impact on the understanding of the appropriate use of medicines. Increasing medication awareness should be one of the priorities for anyone involved in protecting public health. Educating each other about prescription and nonprescription products, drug abuse, alcohol, the risks of antimicrobial resistance, special vulnerable populations and possible interactions can make a powerful difference in improving patient’s health or even saving a life. The IPSF Medicine Awareness Campaign covers broad areas revolving around correct use of medicines. It is our responsibility to work towards responsible use of medicines and participating in a MAC would be a great innovative way to do just that. Having IPSF’s support, examples of projects around the world will provide you with ideas and opportunities for you to successfully run a campaign.
Goal To improve the proper use of medicines and the public knowledge of important medication related issues.
First Steps1. Focus on an issue about which you
want to educate more people• Antimicrobial Resistance• Prescription Drug Misuse/Abuse
2. Make a plan of what type of campaign you will have
3. Establish a way you will reach out to people
4. Gather other pharmacy students for help and ideas for the campaign
5. Build a timeline of when things will occur
6. Make sure you have enough materials for the campaign to be successful
7. Contact the Medicine Awareness Coordinator or Chairperson of Public Health for further Information
The CampaignMake sure you have gathered everything on the day of your event.
• The right team: • Pharmacy students• Pharmacists• Other healthcare professions• Professors
• The perfect timing:• Make sure the timing of the
campaign will allow for the most participation
• May take place throughout the whole year
Medicine Awareness Campaigns
Running a Successful Campaign:A How-To Guide

IPSF Phuture 201524
• Useful campaign materials • IPSF Medicine Awareness
Campaign Kits (contact: [email protected])
• Additional materials from related global or local awareness campaigns:
• World Health Organization - who.int
• Centers for Disease Control and Prevention - cdc.gov
• Food & Drug Administration - fda.gov
• Additional materials: • Videos • PowerPoint presentations • Poster and postcards • Surveys
• The right target population:• Patients• Fellow colleagues and professors
at university• People in the streets
• The right place for greater participation of your target population:• Your school• Public places• A local clinic• A local pharmacy
• The right promotion:• Social media• Word of mouth • Other internet outlets• School• Information desk • Promo material in pharmacies
• The right funding sources:• School• Pharmacy organizations• Health promotion organizations
Possible Timeline
4-6 months before• Start brainstorming ideas for cam-
paigns• Look for a solid team of students to
help you• Research resources that can help you
with materials and awareness• Start reaching out to entities where
you want the campaign to be• Decide on exact date, time and loca-
tion• Distribute tasks to each team member
2-3 months before• Team meetings and delegating
responsibilities• Start advertising for the event• Create a budget and start fundraising • Reach out to media outlets including
online, TV and radio
1 month before• Make sure you have a detailed techni-
cal plan for the day of the event• Expand advertising• If necessary, recruit additional team
members and volunteers for the day of the event
1 week before• Go over responsibilities with the team
in preparation for the event• Make sure all materials will be avail-
able for the event
After the Campaign• Write a report and send it to the IPSF
Medicine Awareness Coordinator • Evaluation of the campaign and its
successes• Don’t forget to thank everyone who
participated!
Phut
ure
IPSF Phuture 2015 25
FFUP, University of Porto, Portugal
AMR and Pharmacy Practice
Nowadays, a lot of attention has been focused on failure of antibiotic therapies as we once knew it to be infallible. As a matter of fact, resistance of several bacteria to antimicrobials such as carbapenems has significantly increased, mostly due to the presence of carbapenemases, which are enzymes that are able to destroy β-lactam rings that are the key component for the activity of the drug. Carbapenemases can be easily spread between bacteria and because they grant resistance to a wide spectrum of β-lactam drugs, that has been one of the biggest concerns in the scientific community. Therefore, the choice of the antibiotic therapy should be carefully considered to avoid the worsening of the current situation.
Pharmacists should play a protective role by not allowing the misuse of antimicrobials (e.g. self-medication) and encouraging patients and professionals to only use them when it is mandatory and/or under medical advice. Unfortunately, antibiotics are misused by professionals as well as patients because they are mainly prescribed under empirical knowledge (sometimes lacking proof ) and because patients still associate this medication to common colds or flu-like diseases.
Pharmacists have the obligation not to provide any antimicrobials without medical prescription, explaining why this medication is harmful to the patient’s health (and to others) when misused. By doing this, patients will understand the risks they undergo if they intend to abuse antibiotics and eventually they will stop this risky behavior.
In the hospital setting, there is a commit-tee that implements rules or at least guide-lines adjusted to the reality of the hospital in question. The prime goal is improving the use of these drugs and reducing the risks of therapeutic failure. The pharmacist in the area should have a solid background in bacteriol-ogy, and has to be able to study the epide-miological data of resistance and compare it to the records of antibiotic use, in order to assess the whole process. It is also the role of the pharmacist to help in the early detec-tion of bacterial resistance, resorting to new biochemical tests, phenotypic tests or even genetic tests.
Michel Brilhante, MSc.

IPSF Phuture 201526
For instance, Blue-Carba is a biochemical test that was developed by our laboratory in the Pharmacy Faculty of University of Porto and it is a cheaper, quicker and easier alternative to detect carbapenemases. Now, some laborato-ries in the hospital setting perform this test to detect carbapenemases in bacteria causing infections and as the result, the physician can choose the best therapeutic drug to treat the patient in shorter period of time, increasing the success rate of antibiotherapy.
To conclude, the future is never certain but we must act accordingly in order to induce the changes we want to see. Only by doing so we can evolve as better professionals. Bacterial resistance is a silent menace as many profes-sionals call it, so we need to be more sensitive and alert in this matter to achieve a better clinical outcome for all patients.
Phut
ure
IPSF Phuture 2015 27
and antimicrobial prophylaxis before surgery. Each year, November 18th is marked as Euro-pean Antibiotic Awareness Day and a symp-osium takes place on the subject. There is no way for a pharmacist in Croatia to become an expert in the field of infectious disease and antibiotic stewardship, however there are postgraduate studies of advanced classes in microbiology. Clinical pharmacists should check prescriptions and decide whether anti-biotics are the best way to treat the patient before administering them. If it is in their opin-ion that giving a different drug would have a better effect, they should discuss it with the doctor. However, clinical pharmacists in Croa-tia still don’t have the authority to do this and it is not a part of the patient’s regular treat-ment. For now, the only thing pharmacists can do in fighting AMR is to educate patients and advise them to be more responsible in their usage of these medications.
Resources
http://www.iskra.bfm.hr/http://www.pharma.unizg.hr/
Faculty of Pharmacy and Biochemistry, University of Zagreb, Croatia
Antimicrobial Resistance in Croatia
Since the late 20th century, antimicrobial resistance is one of the most important medi-cal issues in Croatia. Antibiotics are prescrip-tion drugs, but patients misuse them by shortening their therapy or using medica-tions that were prescribed to them in a previ-ous infection. Patients also have a tendency to pressure their doctor into prescribing them an antibiotic even though it is not indicated in their case. In 1996, the Croatian Academy of Medical Sciences decided to form an Anti-microbial Resistance Committee. This com-mittee was made to monitor AMR all over the country. Nowadays, ISKRA (Interdisciplinary Section for the Control of AMR) is coordinating every event, campaign, national statistics and education on AMR. The latest annual statistic was published in 2013. A total of 40 centers took part in antibiotic resistance surveillance, which allowed for collection of data for more than 90% of the population. A total of 92% of the total consumption of antibiotics has been outside hospitals.
In 2013 there was a decrease in the consump-tion of all classes of antibiotics, except for broad spectrum penicillins. It is especially positive that the use of broad spectrum antibi-otics like cephalosporins and penicillins with beta-lactamase inhibitors has been decreas-ing. ISKRA has also written the national guide-lines on treating throat ache, urinary infec-tions, prevention, control and treating MRSA,
Katarina Žunić
IPSF Phuture 201528
Ogunkoya David, Pharm, Obafemi Awolowo University, Ile-Ife, Nigeria
An Inside Look and How to Reduce the Misuse of Antibiotics in NigeriaNumerous medications including painkillers (tramadol, paracetamol), cough suppressants (those containing codeine) and antibiotics have been misused in recent times. Of these medications, antibiotics seem to have the highest toll of misuse. The misuse of antibi-otics is not surprising as there are imminent studies which show the increase in antibiotic resistance especially in developing countries of which Nigeria is one. To make it simpler, antibiotic misuse can be categorized into misuse by healthcare professionals espe-cially those with prescribing rights, misuse by unskilled practitioners as well as misuse by patients and the general public.
Although individual strategies have been put in place to help reduce to the barest minimum the misuse of antibiotics, it can’t be stressed enough that collaborative efforts among healthcare professionals, government and regulatory bodies and the general public would make an outstanding change in the misuse of antibiotics and consequently the rate of antibiotic resistance in Nigeria.
In hospital settings, there has been a reported clinical misuse of antibiotics. Even in indus-trialized countries, there is an excessive use of antibiotics, of which the management of diarrhea and viral respiratory infections is a typical example. In many instances, clinicians prescribe antibiotics for patients who have
malaria fever in addition to the artemisinin-combination therapy mostly as to help com-bat typhoid fever if that is the case. This even encourages patients to go to drug stores and purchase these antibiotics which are readily sold to them without prescriptions.
Several strategies were put in place to help reduce the clinical misuse of antibiotics such as the adoption of antibiotic monitoring systems and hospital formularies as well as creation of an essential drug list. Although the implementation of these strategies would tremendously help reduce the clinical misuse of antibiotics, some factors render the strate-gies ineffective in developing countries like Nigeria. They include limited/irregular drug supply, cost and the availability of some anti-biotics from unofficial sources.
On the other hand, misuse of antibiotics has also risen up largely due to the practices of unskilled practitioners who make these anti-biotics available with the snap of a finger. In the rural areas and communities, where the skilled or trained health professionals are scarce, the only available sources are the drug vendors, community health workers and medicine stores. Because of the limited level of training they have, they often prescribe antibiotics unnecessarily or even change a prescription when the antibiotic is not avail-able without asking the prescriber.
Mordi Chiedu Jr, Pharm, Coka Pharmacy, Benin, Nigeria

Phut
ure
IPSF Phuture 2015 29
The general public also plays a huge role in the rise of antimicrobial resistance. This is largely due to the fact that they are able to purchase antibiotics from unofficial sources. A typical example is the selling of medications including antibiotics by drug peddlers in bus parks, garages and market places. These drug peddlers usually deceive people and convince them to purchase the drugs even they know little or nothing about the indications, dosage and side effects.
To help combat this issue of antibiotic resist-ance, collaborative efforts are needed from every aspect of the society as no one can work in isolation to reach a common goal. Antibi-otic audits and national formularies should be adopted in clinical settings, health care pro-fessionals should continue to engage in medi-cal education and the general public should be continuously educated about the effects of misusing antibiotics. Healthcare professionals should be encouraged to take up more train-ing and specialize in infectious diseases either through board certifications or residency pro-grams. Regulatory bodies should work more earnestly to make sure antibiotics are avail-able only through official sources and moni-tor the supply of drug to hospitals.
Last but not the least, more healthcare profes-sionals should be encouraged to set up clinics and drug stores in rural areas to ease acces-sibility to proper health management by peo-ple in the rural settings. Education cannot be overstressed as it is the only key to awareness and proper understanding by the general public. Urging our healthcare professionals to continue to serve as advocates for rational use of antibiotics is essential.
Edited and Compiled by:Ms. Juliet Obi PANS, Nigeria
IPSF Phuture 201530
Faith Matungamidze, MPharm, Liverpool John Moores University, UK
Rational Use of Medicine:Focusing on Antimicrobial Resistance
U.K. Perspective
Today, antimicrobial resistance still is a propa-gating peril which threatens the well-being of the public nationally and globally. Antimi-crobial resistance (AMR) is a threat that has been evoked by misuse by general practi-tioners prescribing antibiotics for inessential indications like cold and coughs. Due to the misuse of antibiotics, bacteria have managed to obtain resistance against antibiotics, and creating more barriers to destroying the bac-teria. Antimicrobial resistance is an issue that can be resolved with the help of pharmacists. Pharmacists in their discipline have access to a broad spectrum of other health care disci-plines that are linked. Because pharmacists are experts in medicines and their appropri-ate uses, they have a key role in rationalizing the use of antibiotics. Community pharma-cists especially serve the greatest volume of patients. (Oredope,D.2014). Furthermore, community pharmacist’s expertise will be a great help as pharmacists can educate gen-eral practitioners on which medicines will be optimal for certain problems of patients.
Pharmacists with doctoral degrees in areas that revolve around immunology contribute to creating new medicines to combat certain diseases and carry out vital research in anti-microbial resistance, as it’s one of the main concerned areas today in preventing further propagation of resistant bacteria to modern antibiotics.
An antimicrobial resistant bacterium is a huge threat to those who are immunocom-promised. Due to the widespread resistance gained by the bacteria against antibiotics in hospitals, it has now proliferated vastly in the community (The American Society of Health-System Pharmacists, n.d.). Mutations and resistance to antibiotics make it harder to eradicate this problem and suppressing it is a first step towards eradicating AMR completely. Eradicating this type of bacteria is a challenge that can be solved by research into AMR. Research is the heart of solving this problem and academic pharmacists are those who can clarify and comprehend research since they are most competent compared to the tradi-tional pharmacist. Academic pharmacists with alliance of regulatory pharmacists can achieve a common goal of suppressing AMR. Collectively they can prevail in eradicating AMR with correct regulations and legislation on control of AMR in addition to academic research solving this problem.(World Health Organisation,2014). Additionally, surveillance technology has been created for rapid detec-tion of resistance of bacteria to antibiotics.
In the United Kingdom, antibiotic steward-ship and infectious disease training are done through a postgraduate program. Certifica-tion is awarded upon completion by prospec-tive universities that have been accredited by
Mayur Kumar, MPharm, Keele University, UK

Phut
ure
IPSF Phuture 2015 31
the General Pharmaceutical Council (GPHC). Pharmacists would secure a position in this role and through experience. Non-traditional roles allow pharmacists to use their sound pharmaceutical knowledge in public health avenues to collaborate efforts in order to minimize AMR. For instance infectious disease pharmacist work in hospitals assisting in anti-microbial stewardship programs. This involves the pharmacists working in different infec-tious disease departments for adult and pedi-atric patients in optimizing the use of antimi-crobial agents while reducing transmission of infections between patients. For instance the pharmacists can educate and support patients by encouraging them to finish their full course of antibiotics (Philip Howard, 2013). They can also provide education to hospital staff on the optimal use of antimicrobial agents.
The Antibiotic Guardian presents strategies to educate health care professionals and the public on the issue of antimicrobial resistance and how each professional can play their part. It is a campaign that calls on everyone in the UK and abroad, including students, the public and the medical community, to become an antibiotic guardian. (Public Health England, 2015). Each antibiotic guardian chooses one simple pledge about how they will make better use of antibiotics and help save these medicines from becoming obsolete.
As students we all have a role right now. We can educate our family and friends and also encourage and raise awareness of the Antibi-otic Guardian campaign.
References
1. Department of Health, United King-dom. UK Five Year Antimicrobial Resistance Strategy 2013 to 2018. 2013. p. 6, 28.2. Eyre M. Novel antibiotic class created. BBC News [Internet]. 2015 [cited 2 Dec 2015];. Available from: http://www.bbc.com/news/health-293068073. Howard P, Ashiru-Oredope D, Gilchrist M, et al. Time for pharmacy to unite in the fight against antimicrobial resistance. The Pharma-ceutical Journal, 2013 Nov 13; 291:537. 4. Public Health England. Antibiotic Guardian [Internet]. 2015 [cited 2 Dec 2015]. Available from: https://antibioticguardian.com/5. The American Society of Health-System Pharmacist, n.d. The Pharmacist’s Role in Pre-venting Antimicrobial Resistance. [Internet] Available from: https://www.ashpadvantage.com6. World Health Organization. Pharma-cists have decisive role in combating antibiotic resistance, says new WHO European survey. 13 Nov 2014.7. Ashiru-Oredope D. Community phar-macists must help conserve antibiotics [Inter-net]. Pharmaceutical Journal. 2014 [cited 3 Dec 2015]. Available from: http://www.phar-maceutical-journal.com/opinion/community-pharmacists-must-help-conserve-antibiot-ics/20066496.article?adfesuccess=1

IPSF Phuture 201532
Universidad del Atlántico, Colombia
Antimicrobial Resistance in Colombia: A Challenge for Healthcare Professionals
There is no question that antimicrobial resist-ance (AMR) is a global threat to public health. It is a natural biological phenomenon1 with transcendence beyond the individual who has taken the antimicrobial treatment. As a result, the World Health Organization (WHO) published at the end of 2014 a study that tries to quantify the AMR problem on a worldwide scale. At the 2015 World Health Assembly (WHA) the Global Action Plan (GAP) for anti-microbial resistance was established. Regard-ing GAP, the real concern is the misuse of anti-microbial around the world and the lack of new antimicrobials. Since 1987 no new type of antibiotic has been developed, but only partially modified molecules have interfered. AMR has no borders, no country can fight on its own. It urges us to determine the best way to decrease that impact. As future phar-macists, highly accessible to the community, we have the role in improving awareness and preventing misuse of antimicrobials.
In spite of the fact that prescription and con-sumption of antibiotics is different world-wide, it is well known that all antimicrobials are given in the consultations of primary care. In Colombia, there are much more factors to be considered, as was told by the president of Colombian Infectology Association, Mr. Carlos Álvarez, “We do not have a global policy on rational use of antimicrobials”, regarding
the antimicrobial management procedure in our country.
In Colombia, a real concern regarding the AMR problem began in the 1990s, through hos-pital bacterial pathologists. In fact, the most important and relevant data are from hospital settings, outside the community and primary care. In Colombia the community pharmacist is not seen as a true healthcare professional, simply a medicine dispenser. The contribu-tion that could be made in this area is really important and there are a lot of possibilities to improve rational use of medicines. Multiple, combined strategies may reduce the spread of AMR, in both hospital and community set-tings. Those strategies include properly edu-cating healthcare professionals, in continued training, and defining procedures and policies are the best to achieve that goal. As future pharmacists, we will be communicators, lead-ers and healthcare professionals with a spe-cific aim: improve people’s health. With a sim-ple advice given by a community pharmacist, it will be a big change, letting people know how important adherence is in any medical treatment. Also, knowing that pharmacists can support them if they have any doubts and follow the progress in their recovery in a col-laborative practice with physician.
The Ministry of Health in Colombia is currently working on how to reduce the spread of AMR
Margareth Charry

Phut
ure
IPSF Phuture 2015 33
and its impact on the healthcare system. In early 2007, Colombia decided to begin the organization of an integrated surveillance of AMR. At that time, there was no formal inte-grated system at the national level for surveil-lance of AMR. The Instituto Nacional de Salud (INS) was the only organization working with passive surveillance and ad hoc studies on serotypes and trends of antimicrobial suscep-tibility in pathogens of importance in human health such as Streptococcus pneumoniae, Haemophilus influenzae, Neisseria meningitidis, Neisseria gonorrhoeae, Salmonellaspp. and Shi-gella species.2
Also, for AMR in humans, four groups of researchers reported results in human hospitals and clinical cases (Pfaller et al., 1999; Arias et al., 2003; Leal et al., 2006; Miranda et al., 2006). The research of all these groups showed an increasing trend in the occurrence of antimicrobial resistance in several microorganisms that cause disease in human populations. For instance, the Bogota Bacterial Resistance Control Group’s (GREBO – Grupo para el Control de la Resistencia Bacteriana de Bogota) reported the frequencies and antimicrobial resistance patterns of E. coli and E. faecalis in intensive care units of hospitals of third level who participates in a surveillance network in Colombia (Alvarez et al., 2006; Cortes et al., 2013). Also, for AMR in humans, four groups of researchers reported results in human hospitals and clinical cases. The research of all these groups showed an increasing trend in the occurrence of antimi-crobial resistance in several microorganisms that cause disease in human populations.2
Nevertheless, in the case of food animals and food of animal origin, there were no surveil-lance reports. Although the Instituto Colom-biano Agropecuario (ICA) had information on AMR bacterial isolates from clinical cases in different animal species and regions of the country. The Instituto Nacional de Vigilancia de Medicamentos y Alimentos (INVIMA) had few analyses of AMR in some bacteria in food of animal origin.2 But, the rapid development of Colombia’s animal production industry has raised food safety issues including the emer-gence of antibiotic resistance. The Colombian Integrated Surveillance Program for Antimi-crobial Resistance (COIPARS) was established as a pilot project to monitor AMR on poultry farms, slaughterhouses and retail markets.
References
1. Guzman MA. Resistencia antimicrobi-ana: el gran reto para la infectologia contem-poránea. Biomédica. 2014 Apr; 34(1).
2. Donado-Godoy P, Castellanos R, León M, et al. The establishment of the Colombian Integrated program for antimicrobial resist-ance surveillance (COIPARS): a pilot project n poultry farms, slaughterhouses and retail market [Internet]; 2012 [cited 2015 July 20]. Available from: http://onlinelibrary.wiley.com/doi/10.1111/zph.12192/epdf

IPSF Phuture 201534
Intern Pharmacist, 37 Military Hospital, Ghana IPSF Pharmacy Education Committee Member
Rational Use Of Medicines: Focusing On Antimicrobial Resistance
A Ghanaian Perspective
Rational use of medicines require that patients receive medications appropriate to their clini-cal needs in doses that meet their individual requirements, for an adequate period of time and at the lowest cost to the patients and their community. Antimicrobial resistance is the resistance of microorganisms to antimi-crobial medicines (antibiotics, antivirals, anti-malarials) to which the microorganism was previously sensitive. Resistant strains develop and render the medications ineffective. Irra-tional medicine use includes inappropriate use of antimicrobials, inadequate dosage for bacterial infections, failure to prescribe in accordance with clinical guidelines and also inappropriate self-medication . These factors eventually lead to antimicrobial resistance. Its high proportions to common treatments have become a global phenomenon that poses a profound threat to human health, with negative effects on the patient outcomes and health expenditures.
In Ghana, pharmacists, prescribers, regulatory bodies and patients are all to be blamed for the current trend of the abuse and misuse of antimicrobials. On a typical day in a community pharmacy, one would find more than ten people coming in for various antimicrobials without prescriptions. Our country is faced with numerous common ailments of upper respiratory tract infections, sexually transmit-ted infections (STIs), skin infections, food-
borne diseases and malaria. The treatment regimen of these conditions are mainly anti-microbials and hence it is not surprising that we have a high level of use of these agents in Ghana.
The commonly abused and misused anti-microbials include metronidazole, amoxicil-lin, ciprofloxacin, clindamycin, doxycycline, chloramphenicol, azithromycin and a variety of antimalarial treatments available amongst many others. A typical case is that of a young man who walks into a community pharmacy asking for “metronidazole 500mg” scribbled on a piece of paper. When questioned by the pharmacist-in-charge on why he wants those tablets, he says a friend recommended them to treat his erectile dysfunction. The list of myths and inappropriate use is endless.
One of the biggest problems is the ease of accessing these medicines. There are numer-ous chemical shops which sell these medicines even though most of them are not licensed to sell majority of those agents. At bus stations and on buses, one would find drug peddlers marketing these antimicrobials. In some com-munity pharmacies, one may find unqualified personnel and even pharmacists, who would sell these medicines without prescriptions for monetary gains. Sometimes patients are also not advised by pharmacists on the need to finish their course of treatment.
Bernice Bonsu Adusah

Phut
ure
IPSF Phuture 2015 35
There is also the problem of unqualified pre-scribers and prescribers who are not involved in continued education to upgrade their knowledge and hence keep on prescribing inadequate doses of antimicrobials. Patients who obtain these agents with prescriptions, more often than not, do not finish the required course of treatment due to patients becom-ing asymptomatic after beginning treatment. Long durations of treatment and frequency of administration of these medicines also con-tribute to patient nonadherence.
One may ask if there are no laws guiding our practices or why nothing is being done to help curb this menace. Interestingly, a lot of policies are in place to help curb this problem. The problem however is with the implemen-tation and enforcement of these policies. The policies are not being adequately imple-mented because of the lack of personnel to help implement them. There are policy guide-lines such as the use of standard treatment guidelines and essential medicines list to aid prescribers and pharmacists in carrying out their duties.
Very often in community pharmacies, phar-macists are faced with the challenge of turn-ing down the request of clients who wish to buy these medicines without prescriptions. By law, pharmacists are required to provide medical aid in cases of simple ailments of common occurrences and hence are allowed to offer treatment in these cases. However, it would be appropriate that pharmacists gave out antimicrobials only when these agents are really needed especially in cases of STIs.
Pharmacists need to enforce the use of pre-scriptions when purchasing antimicrobials. Offering appropriate advice to clients who want to purchase antimicrobials over-the-counter would help people understand the need to be properly diagnosed before
purchasing antibiotics due to the sensitiv-ity profile of the various agents. Pharmacists have to stand tall in this fight to help prevent the development of resistance against these agents. Resistance may eventually be the least of our problems as the side effects of the anti-microbials can even be life-threatening.
In Ghana, pharmacists are broadly trained as custodians of medicines and hence do not become experts in infectious diseases and antibiotic stewardship. The bottom line to controlling this fast growing problem would be centered on a team effort of all healthcare providers, the establishment of continued education programs on the mechanism of actions and the appropriate use of these agents and lastly, the enforcement of the laid down policies by all stakeholders.
Viva la Pharmacie!

IPSF Phuture 201536
Bouatta Rahima, Pharm University of Algiers, Algeria
Rational Use of Medicines:Focusing on Antimicrobial Resistance
An Algerian Perspective
In my country Algeria, antibiotics are widely used in their different forms (e.g. tablets, oral suspensions). Everyone has access to antibi-otics, even without a prescription from some local pharmacies! The reason behind this situation is that there is no law that prohibits pharmacists from dispensing antibiotics with-out a prescription. As well, doctors sometimes overprescribe antibiotics, and sometimes pre-scribe them unnecessarily.
As a consequence, the rate of resistant bac-teria to antibiotics increased, and many of the available treatment options for common bacterial infections are becoming more and more ineffective. In some situations, infected patients cannot be treated adequately by any of the available antibiotics.
Last year, my graduation thesis was on the issue of gram negative bacilli resistance to beta-lactams. I did an internship in the unit of bacteriology at a public teaching hospital for a period of two months along with my col-league. We collected bacterial strains from dif-ferent departments of the hospital (pediatric, nephrology, neonatology etc.) and we studied all types of samples (e.g. urine, blood, cere-brospinal fluid). After identifying the isolated gram negative bacilli, we studied their sensi-tivity to antibiotics (mainly to beta-lactams) and then we determined the mechanism of resistance, when it exists, by performing com-plementary tests.
Khadidja Si Chaib, Pharm University of Algiers, Algeria
ResultsThe Gram-negative bacilli (BGN) represent the majority of isolates in the medical bacteriology laboratory with 58% of the isolated strains resistance profile to beta-lactams. The resistance to beta-lactams was split as follows:

Phut
ure
IPSF Phuture 2015 37
Multi-bacterial resistance to antibiotics is currently a true public health problem, and it results in mortality mainly in the hospital setting. The resistant bacteria occupy a sig-nificant place in human pathology. Conse-quently, it is imperative to study this resistance and to implement all necessary measures to fight and control the diffusion of resistance: by fighting the self-medication, increasing awareness campaigns on self-medication and the dangers of antibiotic resistance, limiting the prescription of antibiotics to bacterial infections, reserving broad spectrum antibiot-ics for hospital use and fighting against noso-comial infections especially in multi-resistant bacteria.
As part of the fight against the self-medication phenomenon, our association (Association Scientifique des Étudiants en Pharmacie d’Alger) ASEPA, organized a public awareness campaign themed “ The dangers in the misuse of antibiotics” where I was the coordinator of the campaign. This event aimed mainly to inform people about antibiotics, their side effects, the resistance to antibiotics and its consequences, as well as the dangers in the misuse of antibiotics. We provided advice to people regarding the proper use of antibiotics, by answering some questions. For example:
When should we take antibiotics? How do we take them? For how long do we take them? We noticed that people were misinformed regarding the use of antibiotics. Thus, we concluded that such campaigns should be increased in order to alert the largest number of people in the fight against resistance to antibiotics.

InternationalPharmaceuticalStudents’Federation
Andries Bickerweg 52517 JP The Hague the Netherlands
Tel +31 70 302 1992Fax +31 70 302 [email protected]
This work is licensed under the Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0