photo: trym i. bergsmo. best and worst cases sameline grimsgaard md mph phd national research center...
TRANSCRIPT

Photo: Trym I. Bergsmo

Best and worst cases
Sameline Grimsgaard
MD MPH PhD
National research center in complementary and alternative medicine;
NAFKAM
Norway

Norwegian weekly: Allers 1992
Lennart aged 59:– Thyroid cancer
diagnosed in 1989– Metastases April 1990
(liver and bone) – No radiation therapy– Healing x 6– Regression of tumor on
radiological follow-up August 1990

Considerations
Skepticism: – Cured this week and dead next week?– Incorrect diagnosis?
Curiosity:– What happened?

Norwegian weekly: Allers 2003
Lennart aged 70:– ”I am energetic and
healthy! … I had four tumors removed in 1994…medical examinations once yearly have been fine..”
Kari Victoria (healer): – ” The energy come from
some higher powers”
Is Lennart a ”best-case”?

What is a best and worst case?
A clinical course of serious disease that is very different from what was expected based upon medical examinations: – A “best case” could be full or long time recovery of
cancer or other disease with a poor prognosis, after CAM-treatment.
– A “worst case” could be when use of CAM has serious side effects or contributes to delayed conventional treatment with serious consequences for the disease.

Best and worst cases WHY?

Study objectives
1. Provide data for CAM-treatment• Help patients to choose treatment based on correct
information
2. Provide data for CAM-research• Seek out therapies, therapists and case
characteristics to be focused in further research

1-5-year relative survival of breast cancer stage IVFemales, Norway 1992-96
0
20
40
60
80
100
Diagnosis 1. year 2. year 3. year 4. year 5. year
% o
vere
lven
de
Source: Cancer Registry in Norway
Per
cent
sur
vivi
ng

Research strategies: Bench to bedside vs. CAM
CAM practice
Best cases seriesBest cases series Worst casesWorst cases
Product / compound
Animal testing
In vitro studies
Clinical trials
Established medical practice
Mechanistic research Clinical trials
Related projects
National Cancer Institute, USA:• Best-case program
• Quantitative data, only
Quantitative and qualitative data:• NAFKAMNAFKAM in collaboration with Scandinavian
researchers and patient organizations
• Collaborating with the NCI
• Both best and worst cases

Best and worst cases-HOW?

SPONTANEOUS COMMUNICATIONSSPONTANEOUS COMMUNICATIONS
SELECTION
QUANTITATIVE AND QUALITATIVE DATA
INDEPENDENT EXPERT PANEL
Independent researchersREGISTER
REPORT RESEARCH PROJECTS

Spontaneous communications
What do we need to know?1. Full name and date of birth
2. Diagnoses and year of diagnoses
3. CAM and conventional treatment history
4. Effects and side effects of the treatment
5. What do you consider most important for how your disease progressed?

Criteria for follow-up
1. Serious and / or life threatening disease
2. General agreement on diagnostic criteriaE.g. Cancers, multiple sclerosis, asthma
3. CAM treatment during the course of disease
Consider cases who have only conventional treatment during the course of disease?

Quantitative data
Sociodemographic data• Name, age, marital status, level of education…
Case history and documentation• Medical history
• Results of pathology reports and medical imaging reports (X-rays, CT-scans etc.)
• Treatment schedule for both CAM and conventional treatment
• Adverse reactions /side effects

Qualitative data
Taped interviews focusing the cases’ experience and reflection on: Disease and illness history
• Treatment course and life contexts
Choice of treatment (conventional and CAM)• Motivation, expectations and goals
Communication with therapists• Concordance and compliance
Outcomes related to treatment and life contextsEvaluation of treatment courses

Qualitative data
Process and context- oriented:
1. Phenomenological “data” The case (informant) describes
2. Hermeneutical “data” The case (informant) interprets
The case (informant) interprets in a dialog with the researcher

What knowledge?
1. Similarities and uniqueness of: – Individuals who constitute best and worst cases
– Clinical pictures of best and worst cases
– CAM-therapies
– case-therapist cooperation
– CAM-therapists
2. Outcomes of combining conventional and CAM -treatment

Useful knowledge?
Cannot be used to:• Estimate incidence of best and worst cases
• Generalize findings to large groups of patients
Can be used to:• Generate hypotheses and new research projects
• Contribute validated information to patients, patient organizations and therapists

Ethical considerations
Cases must not be ”trapped in CAM”Disclosure of expert panel conclusions?
To cases if they ask for itTo therapists if cases allow for it
No legal actions regarding the law of quackeryApproved by:
– The regional board of research ethics– The Norwegian data inspectorate– The directorate of Health and Social affairs

When is a case a best or worst case?
Depends on the disease
Use available statistics
Use clinical experience
Always a matter of judgment
Where are we today?
Approx. 150 communications
More than 80 cases:– 40 are evaluated (initial selection)– 20 selected for follow-up with collection of
additional information• 18 potential best cases; 10/18 are cancer cases
• 2 potential worst cases; side effects of homeopathy

Where are we today?
International collaboration– National Cancer Institute; best case program
Scandinavian collaboration– Researchers:
• Karolinska Institutet, Sweden• Laila Launsø, Denmark
– Patient organizations• Cancer• Asthma and allergy• Multiple sclerosis
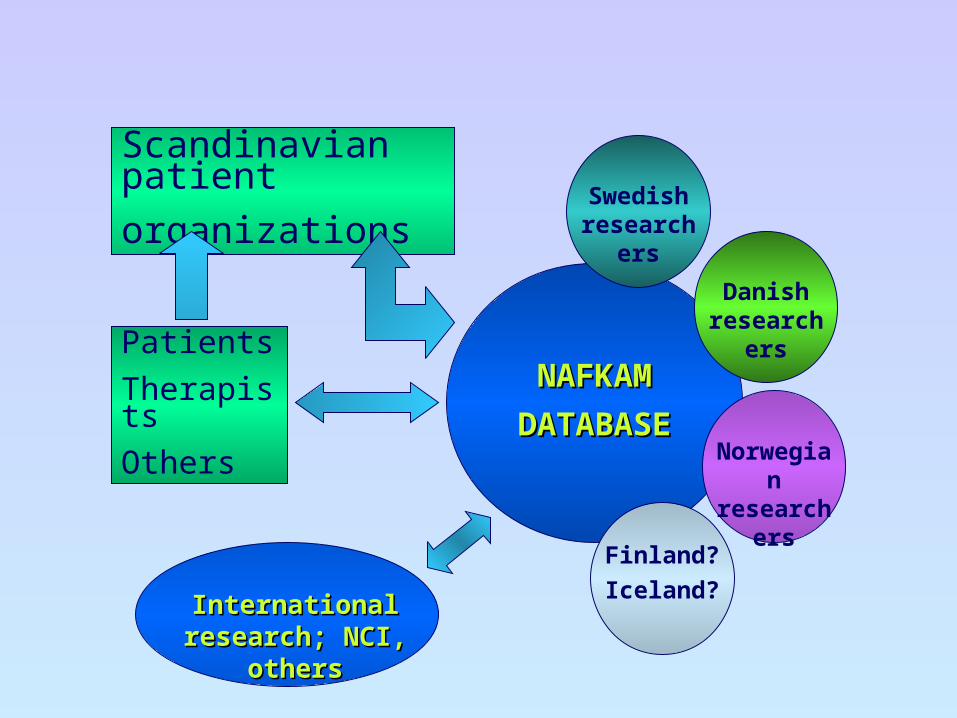
NAFKAMNAFKAM
DATABASEDATABASE
Swedish researchers
Danish researchers
International research; International research; NCI, othersNCI, others
Scandinavian patient
organizations
Patients
Therapists
Others
Finland?
Iceland?
Norwegian researchers

Best and worst cases
Pho
to:
Try
m I
. Ber
gsm
o