phcl 436 lecture two. objectives the role of cognition in influencing adjustment to chronic...
TRANSCRIPT

Chronic disease and medication adherence
PHCL 436 Lecture two
Objectives The role of cognition in influencing
adjustment to chronic conditions What is medication adherence, prevalence,
reasons, measurements
Facing an illness What people thinks/do when adjusting to
chronic disease? What are the behaviours associated with
managing chronic disease?
Chronic disease and medication adherence

Managing chronic disease ◦ @ social level◦ @ individual level
Pharmacists◦ What affects patients reaction to disease◦ Pharmacists can help patients cope better
Chronic disease and medication adherence
Why chronic diseases???
Chronic disease and medication adherence

Behaviour of taking medication
Adherence
( Patients may pretend taking their medication) Hippocrates
(Unpredictable responses to therapy due to low compliance) David Sackett , 1972
( It is the extent to which the patient's behaviour matches agreed recommendations from the prescriber with emphasis the patients' freedom to decide whether to adhere to the prescriber's recommendations, and that failure to do so should not be a reason to blame the patient)*
What is adherence?
*National Institute for Health and Clinical Excellence (NICE) guideline

1ry non-compliance ◦ patient fails to dispense the medication
2ry non-compliance◦ don’t take the medication as directed
Or Intentional
◦ patient decides not to follow the treatment recommended
Unintentional◦ the patient wants to follow the treatment
recommendations but has practicality problemsI
Type of adherence

9
Studies showed that 33-50 % of patients in developed countries are non-adherent to their medication*
A quantitative review research from 1948 to 1998 found that the average percentage of non adherence is 24.8%
Prevalence of non-adherence
10
HIV, arthritis, and gastroenterology disease
pulmonary diseases, diabetes, and sleep disorders
Prevalence of non-adherence
11
40-50% of patients do not persist with their initial treatment for chronic disease more than 12 months
This proportion is higher in developing countries due to other reasons◦ difficulties in accessing healthcare facilities,
availability of medication, deficiency of education
Prevalence of non-adherence
12
USA, it been estimated to cost $100 billion each year, including ◦ 10% of hospital admissions and 23% of
admissions to nursing homes, that is exclusive of indirect costs such as doctor's frustrations not accomplishing treatment outcomes
Canada, the cost of poor adherence has been estimated to be $7 to $9 billion per year because of avoidable negative outcomes not being prevented
Consequences
13
More than 200 variables have been identified to postulate the affect adherence ◦ positively i.e. variables that increase adherence◦ negatively i.e. variables that decrease adherence
Reasons for non-adherence

14
Demographic data have been poorly correlated to patient adherence◦ patient age, gender, social status, features of the
disease, in addition to referral process* negative effect
◦ Increasing psychiatric symptoms◦ numbers of medications◦ frequencies of medications◦ complexity of the regimen◦ Duration◦ cost
Reasons for non-adherence
15
Very few variables were found to have positive strong correlation with adherence◦ increasing the degree of disability◦ administering parental medications
Reasons for non-adherence
16
Patients own beliefs and understanding about medicine and medication
Patient's unresolved concerns about disease Effect of everyday life constraints Effect of poor communication with health
care provider Effect of community and health care provider
attitude Effect of receiving conflicting information
when health care provider do not adhere to diagnostic and therapeutic standard
Reasons for non-adherence

Reasons for non-adherence
18
Variation in outcome and adherence relationship*
There are more factors affects accomplishing therapy outcomes by improving adherence◦ nature of the disease studies, regimen
complexity, tool to be used◦ Improving medication adherence and outcome
relationship should be initiated by using the appropriate technique
Reasons for non-adherence

19
• Direct observation• Medication
concentration in body fluids
Direct
• Self reports• Administration records Indirect
Measures of Adherence

20
Direct methods of assessing patient's behaviour of medication taking
◦ Directly observing the patient taking the medication, such as in tuberculosis direct observation therapy strategy (DOT)
◦ Direct measurement of metabolites, drug markers, or drug concentration in the patient's body fluids
Measures of Adherence

21
Indirectly measuring adherence either◦ by using process measures of medication taking
self reports, tablet counting, prescription filling dates
◦ using outcome measures therapeutic or preventive outcome measures
Measures of Adherence
22
Self report◦ Widely used, general or specific◦ Validation◦ ex: ASK 20, MARS, ACT◦ validation◦ Semi-structured interviews
Measures of Adherence
23
Pill count◦ Widely used◦ Medication Event Monitoring System (MEMS)◦ Cut-off 80% (HTN), 90% (HIV).
Measures of Adherence
24
Administration records ◦ Medication possession ratio (MPR), proportion of
days covered (PDC)◦ Cut-off?
Measures of Adherence
25
Drug Concentrations
◦ Increasing numbers of adherence studies are being conducted utilizes the advancement in the medication analysis technologies Pain medication Antipsychotic medication Addiction therapy
Measures of Adherence
26
There is no ideal tool to assess adherence. Many confounding factor affect each tool using multiple measure with high sensitivity
and the other with high specificity Depth understanding of each patient factors
is the only way to assess adherence and improving achievement of treatment outcomes
Measures of Adherence


What is chronic disease ?
“illnesses that are prolonged, do not resolve spontaneously, and arerarely cured completely”

Domains of adjusting to a diagnosis of chronic disease
interpersonal
cognitive
emotionalbehavioural
Physical components
Psychological adjustment to a diagnosis of chronic disease domians
Psychological adjustment to chronic disease themes:
It requires adjustment across different domains of life.
It happens over time. There are marked differences in the way
individuals adjust.
Stanton et al (2007)
Psychological adjustment to chronic disease
What people do to adjust?
Adaptive task Enhancement of self steam
Psychological adjustment to chronic disease

Social factors and adjusting to chronic disease
Social factors
Culture and ethnicity
Gender Nature of the disease
Interpersonal support
Social recourse
Social isolation

Inherent optimism
Outlook on life and adjustment to chronic disease
التفائل

Lazarus’s appraisal modelRole of perception and
thought in response to illness and people management of their chronic disease
Cognitive appraisal processes and adjustment to chronic disease

Lazarus’s appraisal model
Cognitive appraisal processes and adjustment to chronic disease
Coping process and adjustment to chronic disease
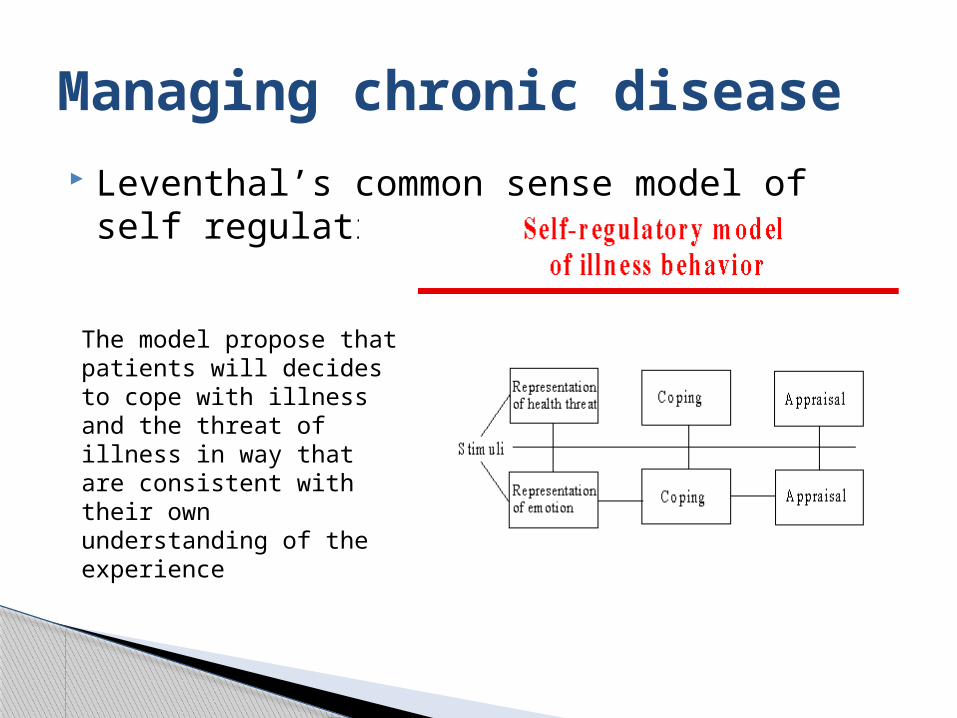
Leventhal’s common sense model of self regulation
Managing chronic disease
The model propose that patients will decides to cope with illness and the threat of illness in way that are consistent with their own understanding of the experience
Heuristics (mental rules) associated with illness and illness representation
◦ Intuitive time and space representation◦ Pattern of symptoms relating to previous
experience◦ Cultural beliefs and social experience◦ Active social comparisons
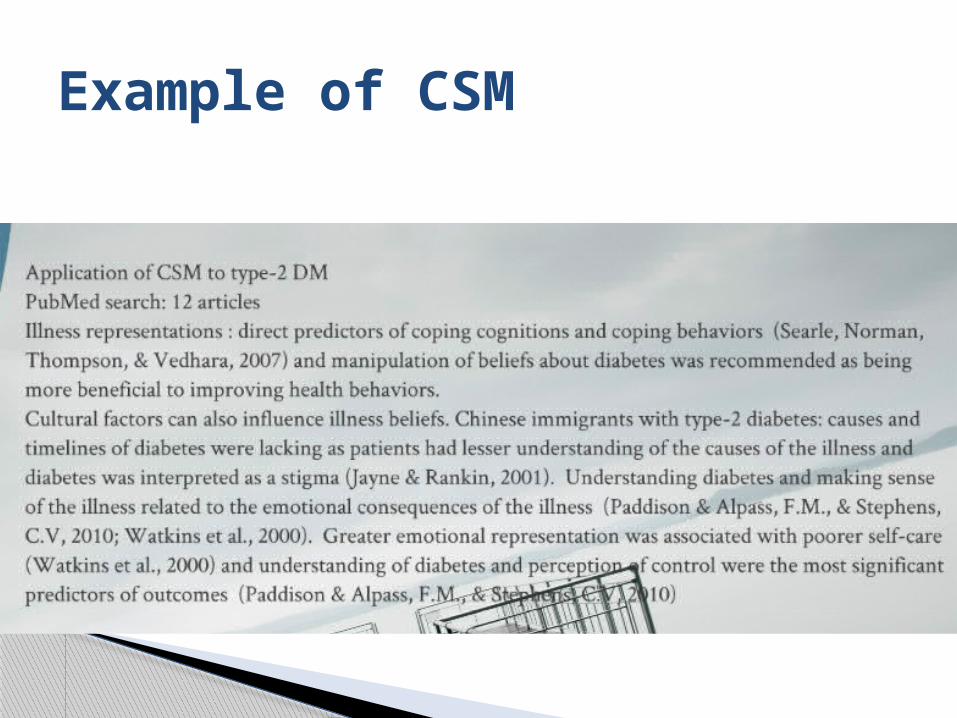
Example of CSM
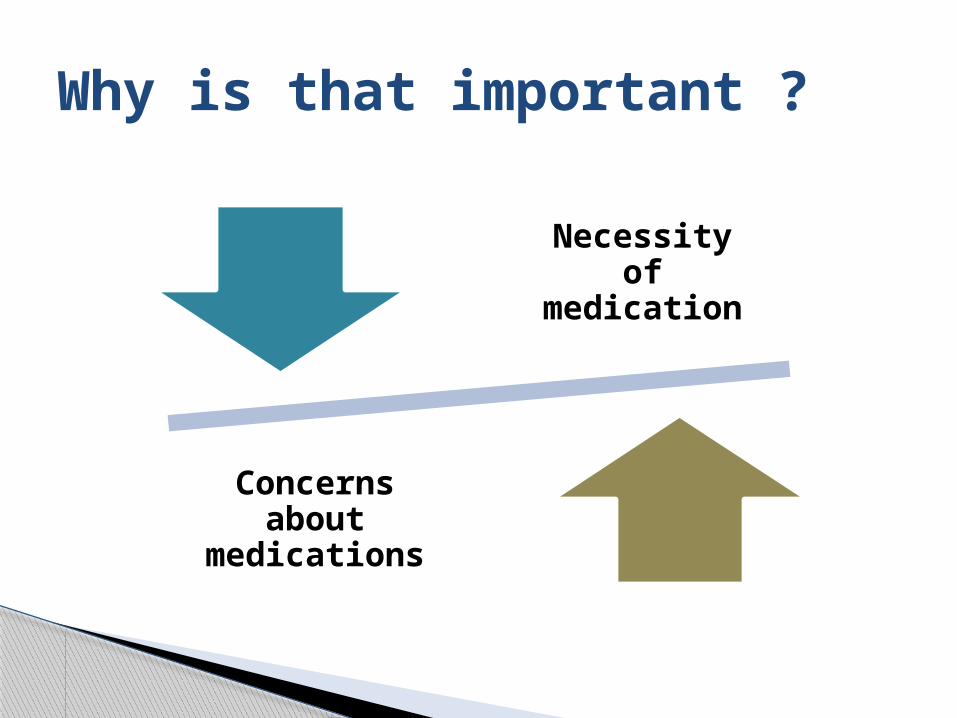
Why is that important ?
Necessity of medication
Concerns about
medications
pathways.nice.org.uk nice.org.uk
NICE guidelines

Haynrs et al 2008 Cochrane review
Intervention to improve adherence
How people think and behave when they have chronic disease
It is difficult to adjust and adjusting is a dynamic process!
Coping is affected by inner thoughts and their surroundings
Lazarus’s stress and coping theory Leventhal’s self regulation theory Overwhelming impact on medication taking
behavior
Conclusion

Next week quiz

Social and Cognitive Pharmacy. Donyai, Parastou. Chapter five.
Medicines adherence. Involving patients in decisions about prescribed medicines and supporting adherence. NICE guidelines 2009. http://guidance.nice.org.uk/CG76
Interventions for enhancing medication adherence (Review). http://www.cochrane.org/
References