pharmacodynamics and pharmacokinetics of polyethylene glycol-hirudin in patients with chronic renal...
TRANSCRIPT
Kidney International, Vol. 58 (2000), pp. 2478–2484
Pharmacodynamics and pharmacokinetics of polyethyleneglycol-hirudin in patients with chronic renal failure
KATRIN ANNETT POSCHEL, ELKE BUCHA, HANS-U. ESSLINGER, PETER NORTERSHEUSER,UTE JANSA, SABINE SCHINDLER, GOTZ NOWAK, and GUNTER STEIN
Department of Internal Medicine IV, Research Unit “Pharmacological Haemostaseology,” Friedrich Schiller University of Jena,Jena, and Knoll AG, Department of Clinical Pharmacology, Ludwigshafen, Germany
Conclusion. Hence, PEG-Hi is considered safe in patientsPharmacodynamics and pharmacokinetics of polyethylene glycol-with CRF, but dosing and/or dose intervals should be adjustedhirudin in patients with chronic renal failure.according to the severity of renal impairment. Ecarin clottingBackground. Hirudin selectively inhibits thrombin without co-time is well suited for safe and reliable monitoring of PEG-Hi.factors and is eliminated via the kidneys. Recombinant hirudin
(r-hi) has a terminal elimination half-life (t1/2) of about 50 to 100minutes. Coupling of polyethylene glycol (PEG) to r-hi, givingPEG-hirudin (PEG-Hi), prolongs its t1/2 while enhancing effi- Unfractionated and low molecular weight heparins arecacy. We looked at the pharmacodynamic and pharmacokinetic the most common anticoagulants in use today and arebehavior of PEG-Hi in patients with impaired renal function. given to treat a wide range of indications. Patients with
Methods. Anticoagulant activity and the pharmacokineticend-stage renal failure on maintenance hemodialysis inparameters of a single intravenous bolus injection of 0.05 mg/kgparticular are exposed to substance-specific side effects,body weight PEG-Hi were studied in 38 subjects. They weresuch as lipid metabolism disorders, increased bleedingassigned to five groups: group IA, creatinine clearance (CCr) $
80 mL/min, 8 healthy volunteers; group IB, CCr $ 80 mL/min, tendency, osteoporosis, alopecia, and, increasingly, hep-8 patients with normal renal function); group II, CCr 79 to 50 arin-induced thrombocytopenia and heparin-inducedmL/min, 7 patients with mild chronic renal failure (CRF); group thrombosis [1–7]. Although there are several alternativeIII, CCr 49 to 20 mL/min, 10 patients with moderate CRF; and antithrombotic agents, their long-term use is not recom-group IV, CCr # 19 mL/min, 5 patients with severe CRF. Plasma
mended for a variety of reasons.and urine samples were collected from patients for up to 120Hirudin, a naturally occurring anticoagulant polypep-hours after dosing and from healthy volunteers for up to 24
tide obtained from the peripharyngeal glands of the med-hours.Results. PEG-Hi was well tolerated in all groups. No serious ical leech, Hirudo medicinalis, is a potent and highly
adverse events were noted. Cmax values were similar in all groups; selective thrombin inhibitor. Unlike heparin, it does notarea under the curve (AUC) increased in patients from 2.9 6 require the presence of antithrombin III (AT III) or1.0 mg · h/mL (IB) to 21.3 6 5.0 mg h/mL (IV). According to other endogenous cofactors. Furthermore, hirudins in-the severity of renal function, t1/2 was prolonged from 2 hours
hibit free and clot-bound thrombin, whereas heparins(IB) to 38.4 hours (IV), while total body clearance (CTB), renalinhibit only free thrombin. The recombinant equivalentclearance (CRenal), and recovery of PEG-Hi in the urine (FEo-t)of hirudin has proved to be an effective anticoagulantdecreased as follows: CTB from 23.3 6 6.6 (IB) to 2.9 6 0.6
mL/min (IV), CRenal from 7.8 6 5.0 (IB) to 0.8 6 0.5 mL/min and antithrombotic agent, allowing a new approach to(IV), and FEo-t from 40.2 6 18.9% (IB) to 12.6 6 13.0% (IV). the prevention and treatment of thromboembolic dis-Total plasma clearance of PEG-Hi was well correlated with eases in both the arterial and venous systems [8–11].CCr. Anti-IIa activity of PEG-Hi showed a closer linear relation- With a terminal elimination half-life of about 50 to 100ship to ecarin clotting time than to activated partial thrombo-
minutes (abstract; Esslinger et al, Thromb Haemost 65:plastin time.1291, 1991) [12, 13], hirudins are rapidly eliminated fromthe circulation via the kidneys. When using recombinanthirudin (r-hi) in patients with renal insufficiency, a changeKey words: pharmacokinetic parameters; PEG-hirudin; activated par-in the pharmacokinetics of the substance is to be ex-tial thromboplastin time; impaired renal function; anti-IIa activity,
ecarin clotting time, kidney failure. pected [14]. Since the establishment of ecarin clottingtime as a reliable bedside monitoring tool, r-hi has beenReceived for publication May 6, 1999given as an anticoagulant in single dosing [15–17] andand in revised form June 6, 2000
Accepted for publication June 9, 2000 regular hemodialysis treatment [18, 19].To achieve a prolongation of the elimination half-life, 2000 by the International Society of Nephrology
2478
Poschel et al: PEG-H in patients with CRF 2479
Table 1. Characteristics of the study participants
Serum CreatinineAge years creatinine clearance UPE
Group N M/F Diagnosis median (range) lmol/L mL/min mg/day
IA 8 7/1 HV 30 (22–60) 81.9611.4 144.7622.0 125618IB 8 7/1 GN 5, IN 2, PKD 1 40 (26–65) 96.1627.7 111.0632.0 72561084II 7 5/2 GN 4, IN 2 HN 1 49 (41–68) 167.1623.4 58.369.6 56761084III 10 6/4 GN 2, IN 6, DN 2 56 (37–66) 269.26126.1 35.7610.9 145262488IV 5 4/1 GN 1, IN 4 56 (45–73) 742.26238.8 10.862.5 12576371
Abbreviations are: HV, healthy volunteers; GN, glomerulonephritis; IN, interstitial nephritis/analgesic nephropathy; DN, diabetic nephropathy; HN, hypertensivenephropathy; PKD, polycystic kidney disease; UPE, urinary protein excretion; M, males; F, females. Data are median (range) or mean 6 SD.
thus enhancing the anticoagulant efficacy of hirudin, a (Jena, Germany). Written informed consent was ob-tained from each participant prior to enrollment.specially designed hirudin-mutein was covalently bound
to two polyethylene glycol (PEG)-5000 residues. TheTrial drug and drug administrationresulting compound, PEG-hirudin (PEG-Hi), exhibits
similar inhibitory activity and selectivity toward throm- Polyethylene glycol-hirudin is a chemically definedbin as its nonconjugated equivalent both in vitro and in conjugate of a recombinant hirudin mutein (rm-hirudin)vivo [abstract; Iorio et al, Ann Hematol 66(Suppl I):A18, and two molecules of PEG-5000 with a mean molecular1993]. Furthermore, with the exception of polymethyl- mass of 17 kD. The drug substance, a product of geneticmethacrylate membranes, PEG-Hi does not flow through engineering, was supplied by Knoll AG (Ludwigshafen,any of the high- and low-flux membranes. Moreover, pro- Germany) in lyophilisate form. Its specific antithrombinlongation of the elimination half-life of PEG-Hi entails activity is about 12,600 antithrombin units per milligrama dose reduction and, consequently, lower costs. PEG-Hi of protein. Lyophilized PEG-Hi was reconstituted withis well tolerated by healthy volunteers, and no immuno- 0.5 mL of sterile water for injection and was dilutedallergic reactions have been observed as described by with physiological saline to a concentration of 1 mg/mL.Esslinger et al [20]. Since PEG-Hi is eliminated exclu- Thereafter, the solution was administered intravenouslysively by renal excretion, impaired renal function might as a single bolus injection of 0.05 mg/kg body weight.have a significant impact on its pharmacokinetics. The
Blood and urine samplingpurpose of this study, therefore, was to determine thesingle-dose pharmacokinetics of intravenous PEG-Hi in Blood samples for the evaluation of anti-IIa activitypatients with varying degrees of chronic renal failure (CRF) and clotting parameters were collected in tubes con-in comparison to healthy volunteers. taining 1:10 vol/vol 3.8% sodium citrate from HVs and
patients before dosing and at 5, 10, 20, and 30 minutesand 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 14, 16, and 24 hours after
METHODSdosing. Additional blood samples were collected from
Subjects patients at 36, 48, 60, 72, 84, 96, 108, and 120 hoursafter dosing. After separation of the citrated blood, theEight volunteers between the ages of 22 and 60 andsamples were immediately centrifuged at 1500 3 g for30 patients between the ages of 26 and 73 with varying15 minutes at 48C. The resulting plasma was divided intodegrees of CRF were enrolled in the study. The subjectsaliquots and then shock frozen and stored at 2758C untilwere assigned to the following groups: group IA, creati-analyzed. Urine was collected from all subjects immedi-nine clearance (CCr) $ 80 mL/min, healthy volunteers;ately before dosing and during the following intervals:group IB, CCr $ 80 mL/min, patients with normal renal0 to 4, 4 to 8, 8 to 12, and 12 to 24 hours after dosing.function; group II, CCr 79 to 50 mL/min, patients withUrine collection for patients was extended to 24 to 48,mild CRF; group III, CCr 49 to 20 mL/min, patients with48 to 72, 72 to 96, and 96 to 120 hours after dosing. Themoderate CRF; and group IV, CCr # 19 mL/min, patientstotal volume voided during each collection interval waswith severe CRF.recorded, and 10 mL aliquots were shock frozen andThe patients’ characteristics are shown in Table 1.stored at 2758C until assayed.The final grouping of renal function and the subsequent
analyses of the pharmacokinetic data were based on CCrAnti-IIa activity and pharmacokinetic evaluationvalues, as determined on the basis of 24-hour urine col-
lection during the in-house study period after PEG-Hi Pharmacokinetic evaluation based on PEG-Hi anti-IIa activity was performed using compartment model-dosing. The study was approved by the Ethics Committee
of the Faculty of Medicine at the University of Jena independent procedures. Anti-IIa activity in plasma and

Poschel et al: PEG-H in patients with CRF2480
urine was measured using chromogenic substrate S-2238 up to six-weeks postdose. The “Total IgE” kit (Immuno-tech, Marseille, France) was used to determine total IgE(Chromogenix, Moelndal, Sweden) according to the
method originally described by Spannagl et al [21]. Peak class antibodies.plasma anti-IIa activity (Cmax) and time to Cmax (tmax) were
Statistical analysisrecorded as observed. The slowest hybrid rate constant(lz) and, hence, terminal half-life (t1/2 5 0.693/lz) were Statistical analysis was performed with descriptive
methods. Dependency of AUC0-t, t1/2, total body clearancecalculated from the slope of the terminal portion of logplasma anti-IIa activity versus time course. No descrip- (CTB) and renal clearance (CRenal) on creatinine clearance
(CCr) as well as the relationship between PEG-Hi plasmative statistics were provided if more than two thirds ofthe measurements at the respective sampling times were levels and coagulation parameters was analyzed by linear
regression.below the limit of quantitation (LOQ 5 100 ng/mL).
Coagulation assays and bleeding timeRESULTS
Dadet reagent (Baxter, Columbia, MD, USA) was usedTolerabilityto determine the activated partial thromboplastin time
(aPTT). Monitoring of PEG-Hi concentrations consisted Polyethylene glycol-hirudin was very well tolerated with-out any serious adverse events. There were no signs ofof measuring the ecarin clotting time in the citrated whole
blood and plasma using a standardized reagent manufac- bleeding in the gastrointestinal tract or urogenital sys-tem. The platelet count as well as red and white bloodtured by Pentapharm (Basel, Switzerland). The ecarin
clotting time is a specific test for the determination of counts (RBC, WBC) were not affected by PEG-Hi. In 18subjects, IgE class prestudy antibody levels were abovehirudin in blood, plasma, or other body fluids. The starting
reagent, made of Echis carinatus snake venom, is ecarin. 120 ng/mL, with maximum levels of up to about 1600ng/mL. However, no allergic reactions were observedEcarin splits the prothrombin molecule at the arginine
320 peptide bond. This limited proteolysis produces a after injecting PEG-Hi, and IgE levels measured afterthe study and at six weeks’ follow-up were similar to thethrombin intermediate called meizothrombin. Hirudin
is able to inhibit meizothrombin with the same extent as baseline values. As a rule, there were no measurable IgGand IgM antibody titers against PEG-Hi. Existing titersthrombin. Meizothrombin also converts fibrinogen into
fibrin, but with considerably lower activity than throm- between 22 and 24 in eight subjects remained unchangedfor up to six weeks after PEG-Hi treatment. Clinical chem-bin. Fibrin conversion follows reaction kinetics of the first
order. Therefore, the calibration curve for hirudin is linear istry [total serum protein, triglycerides, alanine aminotrans-ferase (ALAT), gamma-guanidinium thiocyanate (g-GT),over a wide concentration range (50 to 5000 ng/mL) [22].
The quantitative estimation of fibrinogen was determined and alkaline phosphatase (APH)] values did not signifi-cantly change for up to 120 hours after the administrationas the protein concentration by the biuret method. Tem-
plate bleeding time was measured at a standardized hori- of PEG-H. Bilirubin increased within the normal range,whereas aspartate aminotransferase (ASAT) and choles-zontal cut on the volar aspect of the forearm made with
a Surgicuttt device after inflating a sphygmomanometer terol displayed a falling tendency. In all patient groups,serum creatinine values declined after PEG-Hi dosing;cuff on the upper arm to 40 mm Hg [23].however, these differences were not statistically signifi-
Safety assessment cant. Concomitant treatment of underlying diseases wascontinued and consisted primarily of drugs against hyper-Routine clinical chemistry (including serum creatinine
and liver enzyme determinations) was performed, and tension, hyperuricemia, hyperlipidemia, hyperparathyroid-ism, hypocalcemia, and acidosis. None of the medicationshematological parameters were determined during a two-
week prestudy period, shortly before drug administration were considered to interfere with the study objectives.and after the study. The urinary protein pattern was
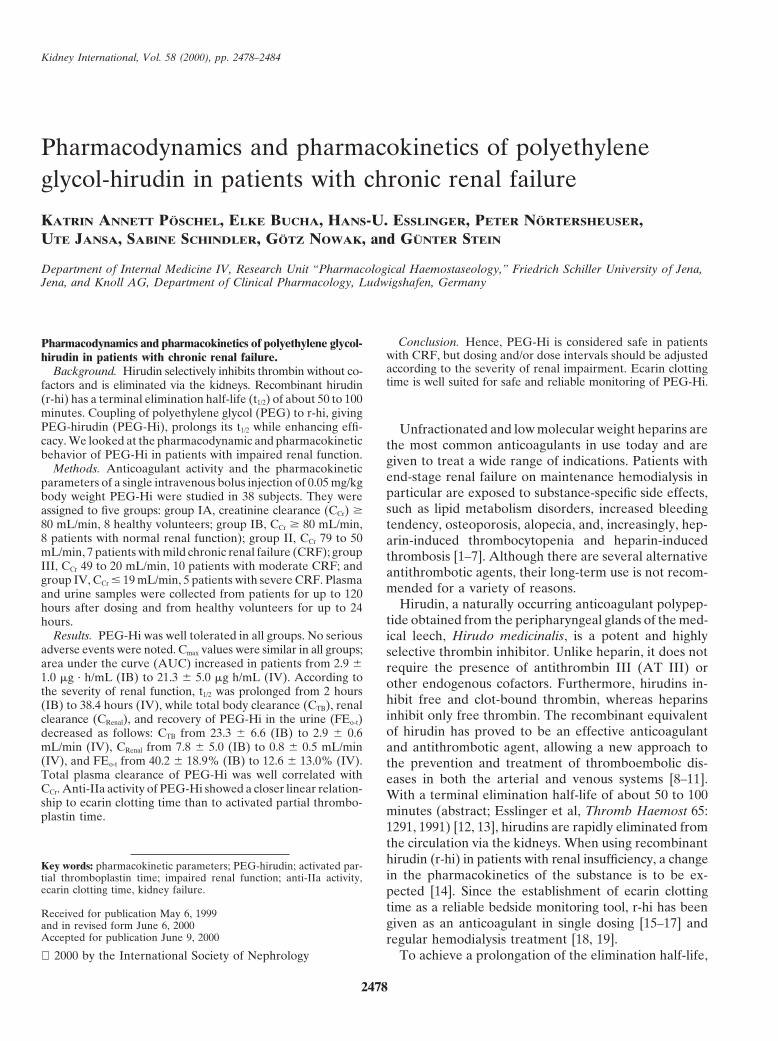
Pharmacodynamics and pharmacokinetic parametersdetermined by sodium dodecyl sulfate-polyacrylamidegel electrophoresis (SDS-PAGE) during the prestudy The mean plasma concentration time profiles and
pharmacokinetic parameters for each study group areperiod. Urine samples were checked repeatedly for he-maturia using reagent test strips (Combur9-Testt) as were shown in Figure 1 and Table 2, respectively. Cmax values
were similar in all groups. AUC increased distinctly inthe feces for occult blood with the hemo-Caret test. Echo-cardiograms, blood pressure, heart rate, and body tem- patients with moderate and severe renal failure. Total
body clearance from the plasma (CTB) and renal clear-perature were determined before dosing, and after thestudy. Specific anti–PEG-Hi antibody assays were per- ance (CRenal) values as well as recovery of PEG-Hi from
the urine decreased, whereas the elimination half-lifeformed using enzyme immunoassays with peroxidase-labeled goat immunoconjugates against human IgM and (t1/2) increased along with the severity of renal function
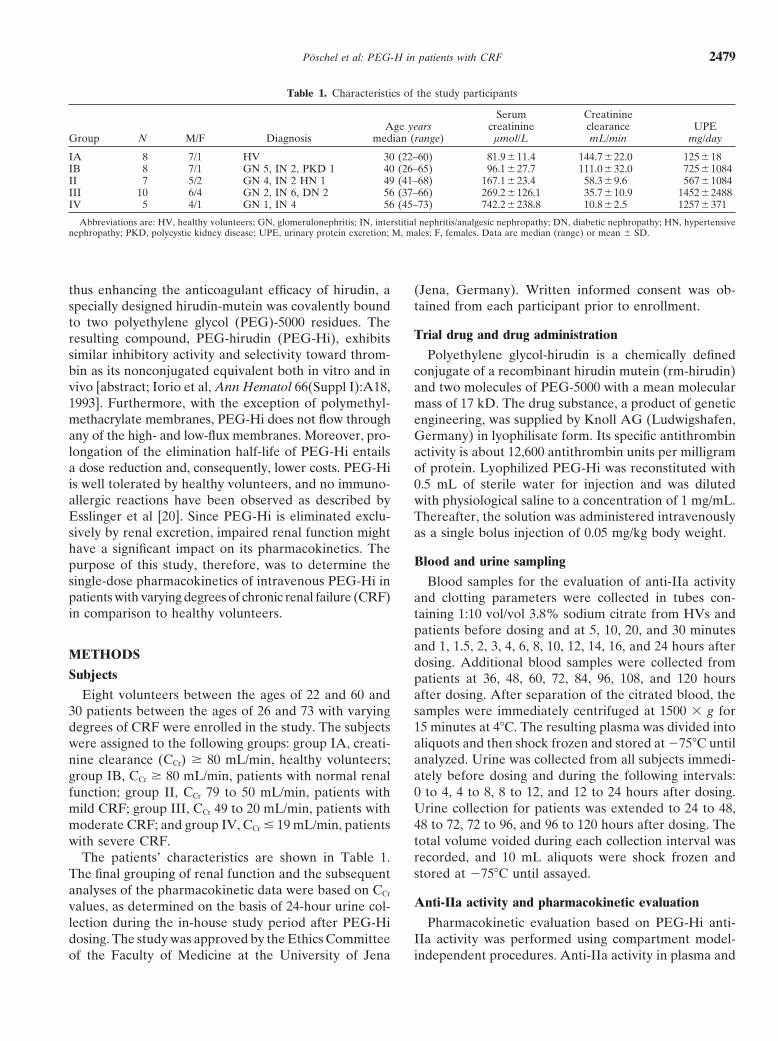
impairment. Total plasma clearance of PEG-Hi correlatedIgG (Nordic, Bochum, Germany), normal limits ,26, for
Poschel et al: PEG-H in patients with CRF 2481
Fig. 2. Linear regression and 95% CI of individual values of totalplasma clearance of PEG-Hi (CTB) versus creatinine (CCr). CTB 5 0.36 1Fig. 1. Mean plasma concentration time curve of polyethylene glycol- 0.2 3 CCr, r 2 5 0.86.hirudin (PEG-Hi) based on anti-IIa activity measured in subjects with
normal and impaired renal function. Symbols are: (s) groups IA and(n) IB, $80 mL/min; (e) group II, 79 to 50 mL/min; (h) group III,49 to 20 mL/min; (d) group IV, #19 mL/min).
Table 2. Pharmacokinetic parameters of PEG-hirudin
Group IA Group IB Group II Group III Group IVParameter N 5 8 N 5 8 N 5 7 N 5 10 N 5 5
CCr mL/min 144.7622.0 111.0632.0 58.369.6 35.7610.9 10.862.5Cmax ng/mL 9746119 10006169 11076288 11136103 931674tmax hours 0.08 (0.08–0.17) 0.13 (0.08–0.17) 0.08 (0.08–0.08) 0.08 (0.08–0.17) 0.17 (0.08–0.50)t1/2 hours 1.6 (1.3–2.1) 2.0 (1.1–4.6) 4.1 (3.0–10.0) 12.0 (4.1–32.2) 38.4 (26.0–87.2)AUC0-t lg · h/mL 1.8560.5 2.4860.8 4.5761.2 9.9564.9 13.5462.2AUC lg · h/mL 2.1560.5 2.8661.0 5.4261.2 12.9166.3 21.3165.0CTB mL/min 30.765.6 23.366.6 12.164.2 6.563.4 2.960.6CRenal mL/min 10.664.8 7.865.0 3.060.9 2.261.4 0.860.5Vc L 4.360.8 4.060.7 4.961.4 6.662.8 10.964.7MRT hours 2.360.4 3.361.6 6.862.8 23.4614.3 59.0627.5FE0-t % 42.6618.8 40.2618.9 30.1617.8 27.9610.9 12.6613.0
Values as mean 6 SD or median and range. Abbreviations are: CCr, creatinine clearance; t1/2, elimination half-life; AUC, area under the plasma concentration-timecurve from time zero to time infinity; CTB, total body clearance from the plasma; CRenal, renal clearance of PEG-hirudin; Vc, apparent volume of the control or plasmacompartment; MRT, mean residence time; FEo-t, fraction of PEG-hirudin dose recovered in urine up to the last concentration above the lower limit of quantification.
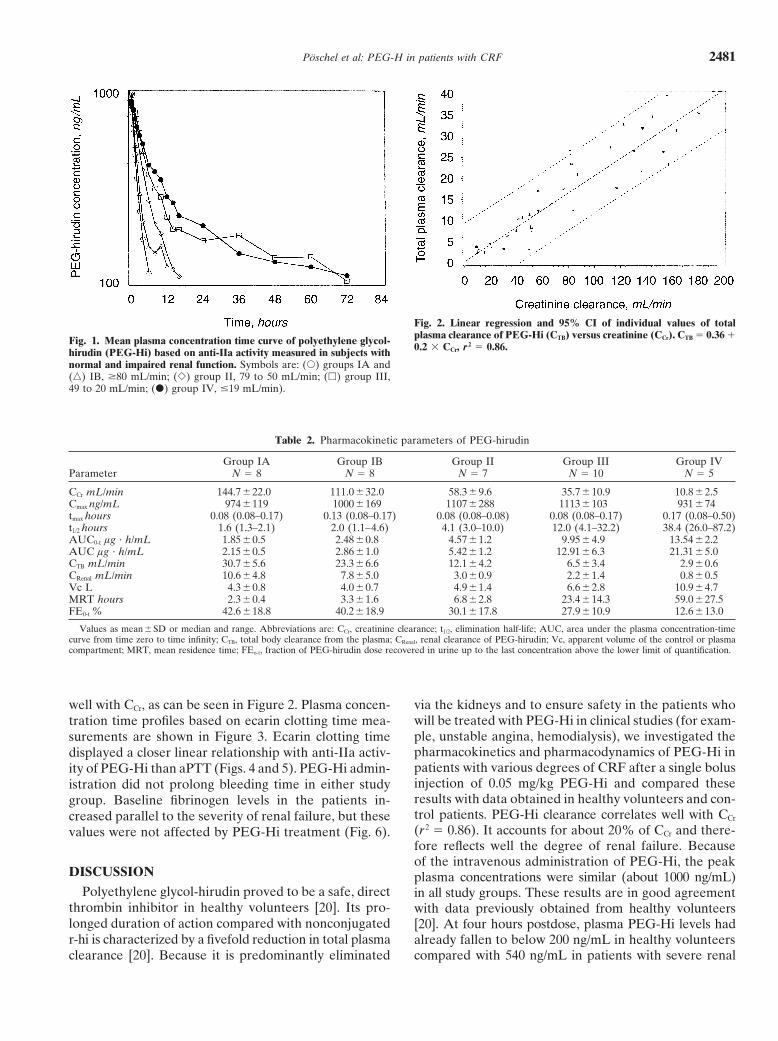
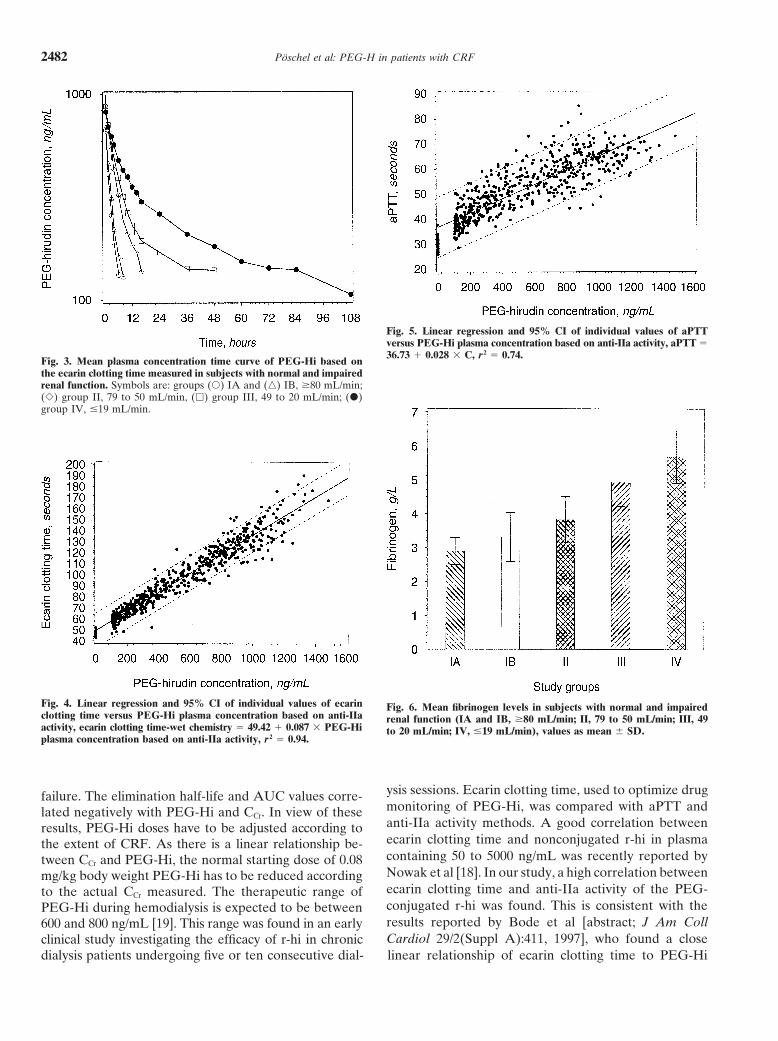
well with CCr, as can be seen in Figure 2. Plasma concen- via the kidneys and to ensure safety in the patients whowill be treated with PEG-Hi in clinical studies (for exam-tration time profiles based on ecarin clotting time mea-ple, unstable angina, hemodialysis), we investigated thesurements are shown in Figure 3. Ecarin clotting timepharmacokinetics and pharmacodynamics of PEG-Hi indisplayed a closer linear relationship with anti-IIa activ-patients with various degrees of CRF after a single bolusity of PEG-Hi than aPTT (Figs. 4 and 5). PEG-Hi admin-injection of 0.05 mg/kg PEG-Hi and compared theseistration did not prolong bleeding time in either studyresults with data obtained in healthy volunteers and con-group. Baseline fibrinogen levels in the patients in-trol patients. PEG-Hi clearance correlates well with CCrcreased parallel to the severity of renal failure, but these(r 2 5 0.86). It accounts for about 20% of CCr and there-values were not affected by PEG-Hi treatment (Fig. 6).fore reflects well the degree of renal failure. Becauseof the intravenous administration of PEG-Hi, the peak
DISCUSSION plasma concentrations were similar (about 1000 ng/mL)Polyethylene glycol-hirudin proved to be a safe, direct in all study groups. These results are in good agreement
thrombin inhibitor in healthy volunteers [20]. Its pro- with data previously obtained from healthy volunteerslonged duration of action compared with nonconjugated [20]. At four hours postdose, plasma PEG-Hi levels hadr-hi is characterized by a fivefold reduction in total plasma already fallen to below 200 ng/mL in healthy volunteers
compared with 540 ng/mL in patients with severe renalclearance [20]. Because it is predominantly eliminated
Poschel et al: PEG-H in patients with CRF2482
Fig. 5. Linear regression and 95% CI of individual values of aPTTversus PEG-Hi plasma concentration based on anti-IIa activity, aPTT 536.73 1 0.028 3 C, r 2 5 0.74.
Fig. 3. Mean plasma concentration time curve of PEG-Hi based onthe ecarin clotting time measured in subjects with normal and impairedrenal function. Symbols are: groups (s) IA and (n) IB, $80 mL/min;(e) group II, 79 to 50 mL/min, (h) group III, 49 to 20 mL/min; (d)group IV, #19 mL/min.
Fig. 4. Linear regression and 95% CI of individual values of ecarin Fig. 6. Mean fibrinogen levels in subjects with normal and impairedclotting time versus PEG-Hi plasma concentration based on anti-IIa renal function (IA and IB, $80 mL/min; II, 79 to 50 mL/min; III, 49activity, ecarin clotting time-wet chemistry 5 49.42 1 0.087 3 PEG-Hi to 20 mL/min; IV, #19 mL/min), values as mean 6 SD.plasma concentration based on anti-IIa activity, r 2 5 0.94.
ysis sessions. Ecarin clotting time, used to optimize drugfailure. The elimination half-life and AUC values corre-monitoring of PEG-Hi, was compared with aPTT andlated negatively with PEG-Hi and CCr. In view of theseanti-IIa activity methods. A good correlation betweenresults, PEG-Hi doses have to be adjusted according toecarin clotting time and nonconjugated r-hi in plasmathe extent of CRF. As there is a linear relationship be-containing 50 to 5000 ng/mL was recently reported bytween CCr and PEG-Hi, the normal starting dose of 0.08Nowak et al [18]. In our study, a high correlation betweenmg/kg body weight PEG-Hi has to be reduced accordingecarin clotting time and anti-IIa activity of the PEG-to the actual CCr measured. The therapeutic range ofconjugated r-hi was found. This is consistent with thePEG-Hi during hemodialysis is expected to be betweenresults reported by Bode et al [abstract; J Am Coll600 and 800 ng/mL [19]. This range was found in an earlyCardiol 29/2(Suppl A):411, 1997], who found a closeclinical study investigating the efficacy of r-hi in chronic
dialysis patients undergoing five or ten consecutive dial- linear relationship of ecarin clotting time to PEG-Hi

Poschel et al: PEG-H in patients with CRF 2483
concentrations from 100 to 3000 ng/mL in unstable an- ACKNOWLEDGMENTSgina patients. We thank Mrs. A. Kossmehl and Mrs. B. Morgenroth for their
skilled technical assistance, and Mrs. E. Hembd for her assistance inOur results support evidence that anti-IIa activity andthe statistical evaluation.ecarin clotting time assays are optimal tools for monitoring
the anticoagulant effect of PEG-Hi, whereas aPTT seems Reprint requests to Prof. Dr. Gunter Stein, Universitat Jena, Klinikfur Innere Medizin IV, Erlanger Allee 101, D-07747 Jena, Germany.to be less reliable especially in the presence of higherE-mail: [email protected] concentrations. PEG-Hi did not prolong bleed-
ing time in either study group. This is in keeping withREFERENCESearlier study results in healthy volunteers [20]. Age and
gender or special renal disease of the patients, such as 1. Schrader J, Andersson LO, Armstrong VW, Kundt M, StibbeW, Scheler F: Lipolytic effects of heparin and low molecular weightdiabetic nephropathy, were not of primary interest inheparin and their importance in haemodialysis. Semin Thromb
this study, which focused on the influence of the degree Hemost 16:41–45, 19902. Teraoka J, Mastui N, Nagagawa S, Takeuchi J: The role ofof renal impairment on the pharmacokinetic and phar-
heparin in the changes of lipid pattern during a single hemodialysis.macodynamic parameters of PEG-Hi.Clin Nephrol 17:76–81, 1982
The nature of the renal disease did not influence the 3. Swartz RD: Hemorrhage during high-risk hemodialysis using con-trolled heparinization. Nephron 28:65–69, 1981pharmacokinetics of PEG-Hi. PEG-Hi was well tolerated
4. Ginsberg JS, Kowalchuk G, Hirsh J, Brill-Edwards P, Bur-in all patient groups. Clinical parameters such as echocar-rows R, Coates G, Webber C: Heparin effect on bone density.
diogram, pulse rate, and body temperature were not Thromb Haemost 64:286–289, 19905. Jacques LB: Heparins: Anionic polyelectrolyte drugs. Pharmacolaffected by the administration of PEG-Hi. No serious
Rev 31:99–166, 1979adverse events and no signs of bleeding in the gastro-6. King DJ, Kelton JG: Heparin-associated thrombocytopenia. Ann
intestinal tract or urogenital system were noted. No in- Intern Med 100:535–540, 19847. Warkentin TE, Kelton JG: Heparin-induced thrombocytopenia,fluence of clinical relevance on blood counts or clinical
in Annual Review of Medicine, Palo Alto, Annual Reviews Inc.,chemistry values was observed. There were also no dif-1989, pp 31–44
ferences in anti–PEG-Hi antibody levels (IgM, IgG) or 8. Finkle CD, Pierre AS, Leblond L, Deschenes I, Dimaio J, Wino-cour PD: BCH-2763, a novel potent parenteral thrombin inhibitor,IgE antibodies before dosing or six weeks thereafter. Inis an effective antithrombotic agent in rodent models of arterial andall patient groups, serum creatinine levels declined aftervenous thrombosis: Comparisons with heparin, r-hirudin, hirulog,
PEG-Hi administration; however, these decreases were inogatran and argatroban. Thromb Haemost 79:431–438, 19989. Ohyama T, Hori T, Moriike M, Asano T, Hayashi H, Iwadenot statistically significant. This observation has already
K, Hosoda S: Anti-thrombotic effects of CX-397, a recombinantbeen reported by Nowak et al using r-hi [18]. The im-hirudin analog, in a canine model of coronary artery thrombosis.
provement in renal function observed in our patients dur- Thromb Haemost 79:423–430, 199810. Eriksson BJ, Ekman S, Kalebo P, Zachrisson B, Bach D, Closeing PEG-Hi anticoagulation might be related to enhanced
P: Prevention of deep-vein thrombosis after total hip replacement:renal perfusion and inhibition of fibrin-bound thrombin Direct thrombin inhibition with recombinant hirudin, CGP 39393.[24]. In patients with acute and CRF, higher fibrinogen Lancet 347:635–639, 1996
11. Breddin HK: Neue Aspekte zu Hirudin. Medwelt 48:64–66, 1997levels reflecting hypercoagulable status should be taken12. Iyer L, Shavit J, Koza M, Calabria R, Moran S, Fareed J:into consideration. In our study, the direct thrombin inhib- Alteration of pharmacokinetics and pharmacodynamics of recom-
itor PEG-Hi had no influence on fibrinogen serum levels binant hirudin (rHV 2-Lys 47) after repeated intravenous adminis-tration in dogs. Thromb Res 69:59–70, 1993after single bolus administration. Finally, it should be
13. Markwardt F: The development of hirudin as an antithromboticpointed out that so far no specific antidote to PEG-Hi drug. Thromb Res 74:1–23, 1994is available. However, dialysis with polymethylmeth- 14. Nowak G, Bucha E, Goock T, Thieler H, Markwardt F: Pharma-
cology of r-hirudin in renal impairment. Thromb Res 66:707–715,acrylate-type dialyzers may be used to remove PEG-Hi1992from the system if bleeding or adverse effects occur (G. 15. Thieler H, Goock T, Nowak G: Ist Hirudin als Antikoagulanz
Nowak, personal communication). bei dialysepflichtigen Patienten geeignet? Nieren-Hockdruckkr20:354–453, 1991In summary, a single intravenous bolus injection of
16. Vanholder R, Camez A, Veys N, Soria J, Irshahi M, Soria C,0.05 mg/kg body weight PEG-Hi proved to be safe in Ringoir S: Recombinant hirudin: A specific thrombin inhibitingpatients with CRF. Impaired renal function results in anticoagulant for hemodialysis. Kidney Int 45:1754–1759, 1994
17. Vanholder R, Camez A, Veys N, Van Loo A, Dhondt AM,higher AUC values, prolonged elimination half-lives,Ringoir S: Pharmacokinetics of recombinant hirudin in hemodia-
and reduced CTB and ClRenal values. In view of its pharma- lyzed end-stage renal failure patients. Thromb Haemost 77:650–cokinetic properties, PEG-Hi dosing and/or dose inter- 655, 1997
18. Nowak G, Bucha E, Brauns I, Czerwinski R: Anticoagulationvals should be adjusted according to the severity of renalwith r-hirudin in regular haemodialysis with heparin-induced throm-
impairment. Because of the close correlation between bocytopenia (HIT II): The first long-term application of r-hirudinecarin clotting time and PEG-Hi plasma concentrations, in a haemodialysis patient. Wien Klin Wochenschr 109:354–358, 1997
19. Bucha E, Nowak G, Czerwinski R, Thieler H: R-hirudin asthis assay is considered to be well-suited for safe andanticoagulant in regular hemodialysis therapy: Finding of therapeu-
reliable monitoring of PEG-Hi treatment in patients with tic r-hirudin blood/plasma concentrations and respective dosages.Clin Appl Thromb Hemost 5:164–170, 1999renal impairment.

Poschel et al: PEG-H in patients with CRF2484
20. Esslinger HU, Haas S, Maurer R, Lassmann A, Dubbers K, 23. Mielke C: Template bleeding time: Technical evaluation and com-parison to other methods in normal adults, in Platelet FunctionMuller-Peltzer H: Pharmacodynamic and safety results of PEG-
hirudin in healthy volunteers. Thromb Haemost 77:911–919, 1997 Testing, Washington DC, DHEW Publications (NIH) 78-1087, 1976,p 1321. Spannagl M, Bichler J, Birg A, Lill H, Schramm W: Develop-
ment of a chromogenic substrate assay for the determination of 24. Weitz JI, Huboda M, Massel D, Maraganore H, Hirsh J: Clot-bound thrombin is protected from inhibition by heparin-antithrom-hirudin in plasma. Blood Coagul Fibrinolysis 2:121–127, 1991
22. Nowak G, Bucha E: Quantitative determination of hirudin in bin III but is susceptible to inactivation by antithrombin III-inde-pendent inhibitors. J Clin Invest 86:385–391, 1990blood and body fluids. Semin Thromb Hemost 22:197–202, 1996