phantom-s study - resuvalresuval.free.fr/eg avc/2013/01_phantom-s_lyon_1.pdf · phantom-s study...
TRANSCRIPT

PHANTOM-S study Prehospital acute neurologic
therapy and optimization of
medical care in stroke
Matthias Wendt on behalf of the
PHANTOM-S study group

Recent guidelines
1. Intravenous rtPA (0.9 mg/kg, maximum dose 90 mg) is recommended
for selected patients who may be treated within 3 hours of onset of
ischemic stroke (Class I; Level of Evidence A).
2. In patients eligible for intravenous rtPA, benefit of therapy is time
dependent, and treatment should be initiated as quickly as possible
(Class I; Level of Evidence A).
3. Intravenous rtPA (0.9 mg/kg, maximum dose 90 mg) is recommended
for administration to eligible patients who can be treated in the time
period of 3 to 4.5 hours after stroke onset (Class I; Level of Evidence B).

tPA effects are time dependent
NNT
14
NNT
4.5
NNT
9
11%
Lees K et al, Lancet 2010 Wahlgren N et al, Lancet 2008
SITS-MOST-Registry: Proportion of patients according to OTT

Starting situation
Thrombolysis rate in Germany: ~ 5-10%
Thrombolysis rate in 14 Berlin Stroke Units: 12% (2010)
98min
44min
pre-hospital
54 min
in-hospital
Ad
mis
sio
n
Ala
rm
Bo
lus
times in 50 consecutive tPA treatments in Charité 2010
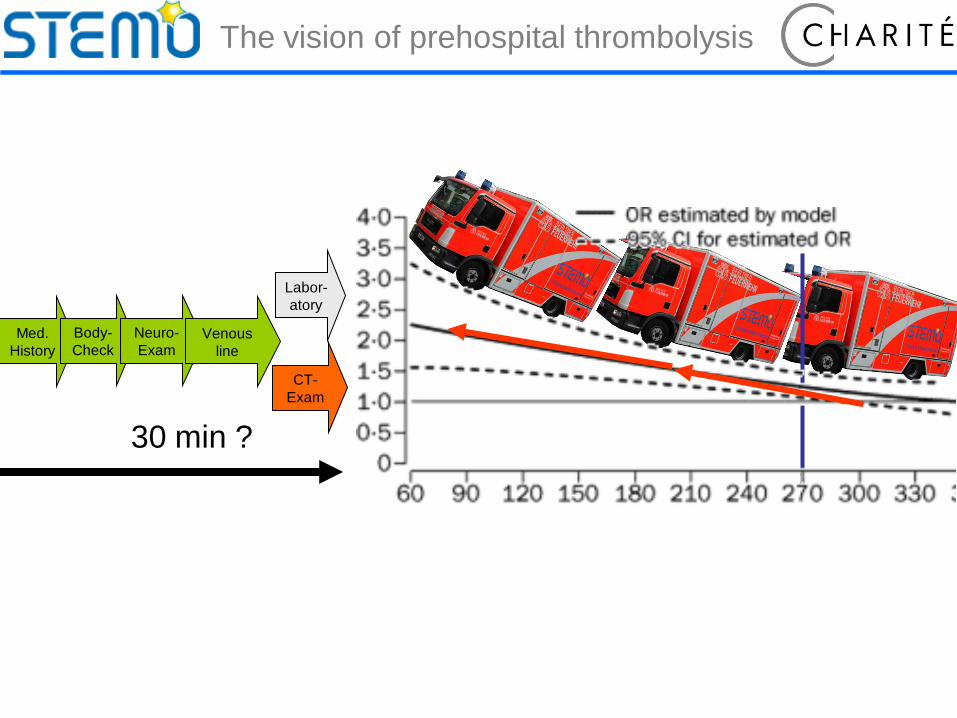
Labor-
atory
Med.
History
Body-
Check
Neuro-
Exam Venous
line
CT-
Exam
30 min ?
The vision of prehospital thrombolysis

STEMO-concept
Preconditions for tPA STEMO components
Discrimination to other
diseases
Neurologist as an
emergency physician
Exclusion of
hemorrhage/tumor
Compact CT with
teleradiology
Exclusion of coagulation
disorders
Point of care laboratory
Imaging of vessel
occlusion
CT-angiography

External view

Inside view

Deployment via stroke identification algorithm
Dispatch Center
Accuracy for stroke and TIA: 59%
Frequency of neurological diseases: 79%
Krebes S et al. Stroke 2012
Deployment process

Objectives and Hypothesis
Primary: Reduction of time from alarm to treatment
at least 20 minutes
Secondary outcomes:
tPA treatment rate
Safety (stroke and non-stroke): 7d mortality and hemorrhages
Process quality
Relevance of effects on local stroke population
3-month pilot study 2011 (Weber et al., Neurology, 2013):
• 23 prehospital tPA treatments
• Time from alarm-to-treatment: 62 min
• No safety concerns

Study design
• Prospective controlled study: 1 special ambulance, multiple hospitals
• Inclusion criteria:
Acute stroke suspected by dispatchers
Expected arrival at scene within
16 min (with 75% probability)
Age ≥ 18 y

Methods
Random allocation of STEMO- and control weeks
C S C S
S C S C
S C S C
Patient delivery to closest adequately equipped hospital
Ethics and data protection (approved by Berlin authorities)
• Informed consent on STEMO (tPA was given also in
Patients who were unable to give their informed consent)
• De-identified data collection from external hospitals
• 3-month FU only from tPA patients
C S C S
C S C S
S C S C
C S C S

Inclusion from 01.05.2011 to 31.01.2013:
10.5 months in both groups
STEMO-weeks
No transport
to hospital
N=117 (6%)
Control weeks
Incomplete
hospital data
N=106 (5%)
No transport
to hospital
N=132 (8%)
Incomplete
hospital data
N=100 (6%)
No transport
to hospital
N=276 (8%)
Incomplete
hospital data
N=186 (5%)
Evaluable
patients
N=1804
Evaluable
patients
N=1409
Evaluable
patients
N=2968
N=3668
in 322 days
STEMO
not deployed
N=1641
STEMO
deployed
N=2027
N=3430
in 320 days
Documentation from 28 hospitals
Included patients
N=7098
Cared in
STEMO
N=1457

Results 1: Total deployments
STEMO
deployed
STEMO
weeks
Control
weeks
N=1804 p N=3213 p N=2965
Age (years) 74 0.39 74 0.33 74
Male gender 44% 0.45 44% 0.50 45%
Diagnosis groups
Non-neurological 31%
0.35
31%
0.19
29%
Neurological / non-stroke 21% 22% 22%
Strokes and TIA 48% 47% 49%
tPA in Stroke-Mimics 0.3% 0.43 0.2% 0.97 0.2%
In-hospital death 3.4% 0.32 3.6% 0.43 4.0%

Results 2: Stroke patients
STEMO
deployed
STEMO
weeks
Control
weeks
N=866 p N=1516 p N=1457
Age (years) 76 0.56 76 0.89 76
Male gender 45% 0.87 45% 0.90 46%
Subtypes
TIA 21%
0.94
22%
0.87
22%
Ischemic stroke (AIS) 71% 71% 71%
Hemorrhagic stroke 5% 5% 5%
Others 3% 2% 2%
Transport to hospital
with Stroke Unit 95% <0.01 93% <0.01 87%
iv.-tPA rate (from AIS) 33% <0.01 29% <0.01 21%
In-hospital death 3.8% 0.41 4.4% 0.90 4.5%

Results 3: tPA treatments
STEMO
deployed
STEMO
weeks
Control
weeks
N=201 p N=312 p N=218
Age (years) 77 0.25 76 0.40 75
Male gender 46% 0.59 50% 0.85 49%
Severity (NIHSS;
median [IQR]) 8 [5-17] 0.02 8 [5-15] 0.09 7 [4-13]
Alarm-to-needle-time
(mean) 52min <0.01 62min <0.01 77min
Complications
Intracranial hemorrh. 3.5% 0.25 4.8% 0.58 6.0%
In-hosp. death within 7 d 4.5% 0.83 4.5% 0.82 4.1%
in STEMO
48 min
in STEMO N = 184

Zeit von Alarmierung bis Lysebeginn
48
35
42
42
53
0 20 40 60 80 100 120
Lysen imSTEMO
Standard-Versorgung
Ausgangslage
Minuten
STEMO Rettungsdienst Klinik
95 min
76 min
48 min
Acceleration of treatment
Alarm to treatment time
Starting situation
(2010)
Regular care
STEMO care
Minutes
Ambulance (prehospital)
Hospital

0
2
4
6
8
10
12
14
16
18
-10
-30
-50
-70
-90
-110
-130
-150
-170
SITS-MOST
STEMO
Onset-to-treatment-time compared to regular care
SITS-MOST
11%
64%
% of
treatments
Real time benefit?
0
2
4
6
8
10
12
14
16
18
-10
-30
-50
-70
-90
-110
-130
-150
-170
SITS-MOST
STEMO
minutes
from onset

Limitations
Randomisation of weeks, not at patient level
Evaluation of one prehospital facility („monocentric“)
No 3-month outcome (will be provided as functional
outcome for patients with informed consent (only STEMO
patients)

Summary and conclusions
STEMO concept
can be integrated in a metropolitan EMS
safe (for all patient groups)
superior to regular care regarding
Quality of care
Proportion of patients receiving tPA
Time to treatment
Effects remain relevant after inclusion of cases who could not
be managed by STEMO
Further potentials (ICH, triage for interventional treatment)

is teamwork! Dispatch Center
Project partners (Berliner Feuerwehr, BRAHMS, CSB, MEYTEC)
Technology Foundation Berlin for funding
Berlin hospitals for their outstanding cooperation
Berlin and it‘s citizens for their openness
STEMO-team and neuroradiologist
Merci beaucoup pour
votre attention!

Disclosures
Co-funding by the
European Union
(European Regional Development Fund)
The STEMO project has been funded by the Technology Foundation
Berlin with co-funding by the European Union.
The Center for Stroke Research Berlin (CSB) is funded by the German
Federal Ministry for Education and Research (BMBF).

0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
1. quartile 2. quartile 3. quartile 4. quartile
minutes
Alarm to treatment times (mean times)
Our learning curve

Interview algorithms for acute stroke identification at the dispatch center.
Krebes S et al. Stroke 2012;43:776-781
Copyright © American Heart Association
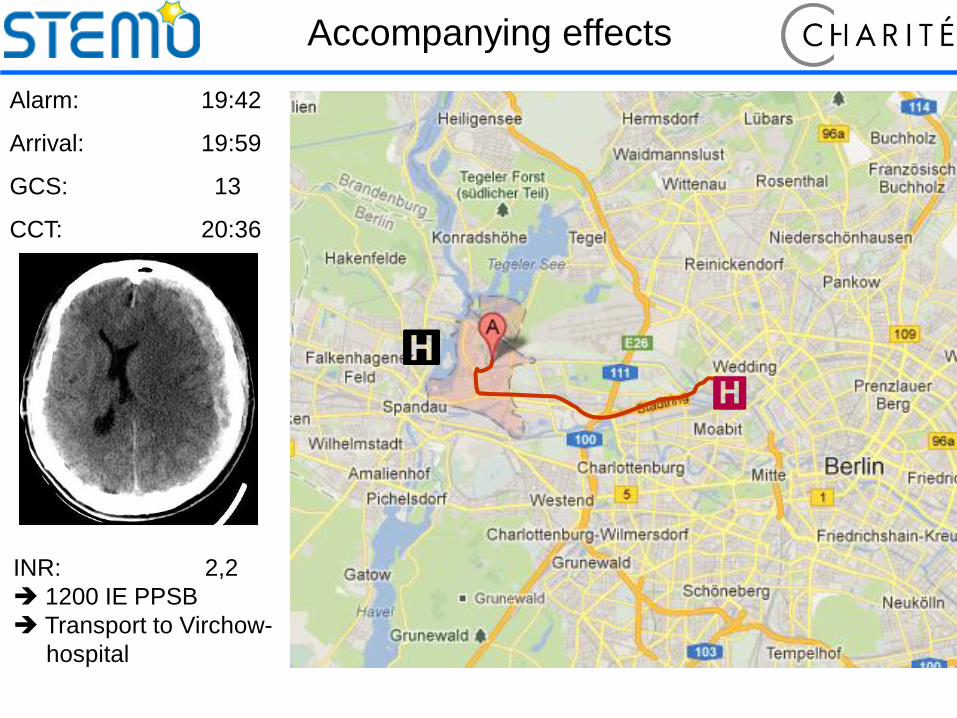
Alarm: 19:42
Arrival: 19:59
GCS: 13
CCT: 20:36
INR: 2,2
1200 IE PPSB
Transport to Virchow-
hospital
Accompanying effects

Arrival CVK: 21:00
GCS: 5
Left side mydriasis
INR: 1,52
OP: 21:40
Day 0 (OP)
Day 18
Day 36
Day 131
Status 4 months after incidence:
•No focal neurology
•Slightly slowed down
•Patient at home
Accompanying effects