peter franzen chair agenda - north norfolk clinical ... pc agenda pack... · in room 1 at the...
TRANSCRIPT

A meeting of the Joint Commissioning Committee for Primary Care will take place in public on Wednesday 28th September 2016, from 2.30-4.30pm
in Room 1 at the Jubilee Centre, Norwich Road, Aylsham, NR11 6JG
Peter Franzen CHAIR
AGENDA
Item Time SUBJECT Lead Format
1 2:30 Welcome and introductions Chair Verbal
2 2:35 Apologies for absence Chair Verbal
Fiona Theodom 3 2:40 Declarations of Interest ALL Verbal
The Chair and members of this meeting are reminded that if they have any pecuniary interest, direct or indirect, in any contract, proposed contract or other matter which is the subject of consideration at this meeting, they must, as soon as practicable after the commencement of the meeting disclose that fact. Other than in relation to Category B Primary Care Interests*, the holders of which may take part in the consideration and discussion of the matter but not any vote arising, conflicted personnel will otherwise be precluded from participation in the agenda item of any kind.
* Standards of Business Conduct Policy refers
4 2:45 Minutes of the last meeting and matters arising ALL Paper 5 2:50 Action Log ALL Paper 6 2:55 Notification of Any Other Business ALL Verbal 7 3:00 Primary Care Strategy S Ross-
Benham Verbal
8 3:05 Primary Care Development Group minutes S Ross-Benham
Paper
9 3:15 PMS-GMS Funding Proposal S Ross-Benham
Paper
10 3:25 Industrial Action – GP Undated Resignations Dr L Hunter
Paper
11 3:30 Performance Report – NHS England A Patman
Paper
12 3:40 Finance Report – NHS England T Lewis Paper 13 3:50 Estates Report – NHS England T Lewis Paper 14 4:00 Any Other Business Chair Verbal 15 4:10 Date and time of next meeting
Wednesday 26th October 2016, 2.30-4.30pm, Jubilee Family Centre, Norwich Road, Aylsham, NR11 6JG
JCC PC Agenda Pack 28.09.16 - Public Page 1 of 44

Register of Interests, August 2016
Name Interest Declared John Archibald Chief Executive, Victory Housing Trust; Trustee and Chairman, Voluntary Norfolk; Dr Penny Ayling Partner, Reepham and Aylsham Medical Practice; Husband is Consultant in Anaesthesia and Intensive Care, NNUH; Tony Belham General Manager, Birchwood Medical Practice, North
Walsham; Stephen Burke Chair, Foundations Independent Living Trust; Chair, Norfolk Family Mediation Service; Chair, North Norfolk Labour Party; Director, United for All Ages; Director, Good Care Guide; Non-Executive Director, Victory Housing Trust; Trustee, North Norfolk Community Transport; Trustee, Age UK Norfolk; Dr Elizabeth Christie Partner, Ludham and Stalham Green Surgeries;
Practice receives NHS funding in respect of research activities;
Dr Deborah Clark Partner, Holt Medical Practice;
Part-ownership, Kelling Pharmacy; Practice contracts with the CCG to provide minor surgery
services; Dr Carsten Dernedde Partner, Hoveton and Wroxham Medical Centre;
Practice receives NHS funding in respect of research activities;
Dr Anoop Dhesi Partner, Staithe Surgery, Stalham; Member, Norfolk and Waveney LMC; Commissioner Representative Governor, Norfolk and
Norwich University Hospitals NHS Foundation Trust ; Occasional Out of Hours Advanced Triage for EEAST /
Swifts; Dr James Gair Managing Partner, Birchwood Medical Practice, North
Walsham; Part-Owner, North Walsham Pharmacy Ltd;
Clive Gardner Non-Executive Director, Julian Support; Non-Executive Director, Havebury Housing Partnership; Holdings in quoted funds which may hold more than 5% of the shares in a company; unaware of any shareholdings in the field of health and social care which exceed 5% of the shares in a company;
JCC PC Agenda Pack 28.09.16 - Public Page 2 of 44

Dr Mark Gaskin Partner, Blofield Surgery Wife is a Speech and Language Therapist with NHS East Coast Community Healthcare Dr Angela Hallatt Partner, Mundelsey Medical Centre;
Brother is involved with contracting for NHS services; Dr Linda Hunter Acts as ‘Macmillan GP’ for the Macmillan Cancer Charity; Dr Manhar Joshi Partner, Fakenham Medical Practice;
Director, FMP (Norfolk) Ltd trading as Fakenham Pharmacy;
Dr Jane Keidan Inspector, Care Quality Commission; Expert Adviser, SHOT – UK independent haemo-vigilance
scheme; Adviser, PREVENTT – national trial of pre-operative IV
iron; Dr Peter Lawson Partner, Market Surgery, Aylsham;
Practice receives NHS funding in respect of research activities;
Dr Gordon McAnsh Partner, Wells Health Centre;
Director, Field House Pharma Ltd;
Dr Adam Maggio Trustee, Servants Church Charity; Director, Mundesley Medical Services Ltd; Dr Mike Noble Partner, Acle Medical Partnership; Honorary Senior Lecturer, University of East Anglia (UEA); Practice is in receipt of NIHR/HTA Research Grant linked
to the ARRISA-UU (University of Utrecht) Study; Dr Ian Smith Partner, Sheringham Medical Practice; Performs GP Triage for EEAST;
Practice receives funding in respect of research activities (PCRN);
Peter Franzen Non-executive Director of Anglia Farmers Affinity; Trustee and Vice Patron of Norfolk Community
Foundation Deputy Chairman; Non-Executive Director (NED); Senior
Independent Director – James Paget Hospital
NOTE: All practices in North Norfolk have federated with GPs throughout the rest of the county and with the Waveney area in Suffolk to establish Iceni Healthcare Ltd
All other members of the Council and Governing Body returned ‘nil’ Declarations
The Register is published onto the website and is available for inspection from the Head of Corporate Affairs; Interests will be further declared in NHS North Norfolk CCG’s Annual Report
and Accounts for the financial year ending 31st March 2017
JCC PC Agenda Pack 28.09.16 - Public Page 3 of 44

Practice Name
Member Representative
Acle Medical Partnership
Dr Mike Noble
Aldborough Surgery
Dr Mark Fleming
The Market Surgery, Aylsham
Dr Peter Lawson
Birchwood Surgery
Dr James Gair
Blofield Surgery
Dr Mark Gaskin
Brundall Medical Centre
Dr Anna Stenberg
Coltishall Medical Practice
Dr Tim Mansfield
Cromer Group Practice
Dr Simon May
Drayton & St Faiths
Dr Alan Lee
Fakenham Medical Practice
Dr Manhar Joshi
Holt Medical Practice
Dr Deborah Clark
Hoveton & Wroxham
Dr Carsten Dernedde
Ludham Surgery
Dr Elizabeth Christie
Mundesley Medical Centre
Dr Angela Hallatt and Dr Adam Maggio
Paston Surgery
Dr Anna Malpas-Sands
The Surgery, Reepham
Dr Penelope Ayling
Sheringham Medical Practice
Dr Ian Smith
The Staithe Surgery
Dr Anoop Dhesi
Wells Health Centre
Dr Gordon McAnsh
JCC PC Agenda Pack 28.09.16 - Public Page 4 of 44

Unconfirmed Minutes of a meeting of the Joint Commissioning Committee for Primary Care held in public
on Wednesday 24th August 2016 at The Jubilee Family Centre, Aylsham
Present John Archibald (JA) (Chair) Lay Member, NNCCG Tracey Lewis (TL) Interim Assistant Head of Finance (Direct Commissioning) -
NHS England - Midlands & East (East) Sally Ross-Benham (SRB) Head of Primary Care Commissioning, NNCCG Jackie Schneider (JS) Head of Clinical Commissioning/Nurse Member of the
Governing Body, NNCCG Fiona Theodom (FT) Contract Manager NHS England - Midlands & East (East) Mark Taylor (MT) Chief Officer, NNCCG Steven Kent (SK) Finance Manager, NHSE Helen Stratton (HS) Chief Finance Officer, NNCCG Tony Belham (TB) Business Manager, Executive Team Member, NNCCG Peter Franzen (PF) Lay Member, NNCCG Clive Gardner (CG) Lay Member, NNCCG
34.16 Apologies for absence Apologies were noted from, Joanna Yellon, Andrea Patman, Alex Stewart, Penny Ayling.
John Archibald (JA) introduced Peter Franzen (PF), new Lay Member for NNCCG, to the meeting who will Chair the Joint Commissioning Committee for Primary Care in future.
35.16 Declarations of Interest
No declarations of interest were made concerning any of the items for consideration on the agenda.
36.16 Minutes of the last meeting and matters arising
The minutes of the last meeting were approved as a true record, with the following amendment:
30.06 To add “NHSE is not a statutory consultee”.
37.16 Action Log
The following updates were noted in the Outstanding Issues Log:
3.3 Ongoing to be brought to the next meeting
6.4 Information requirements for committee: Raised at Primary Care Development meeting with regards national information. Jackie Schneider (JS) stated that GY& W are not in the position to share data as the Matrix has not been developed. Mark Taylor (MT) stated that part of STP feedback is that information is needed on Primary Care Access.
JCC PC Agenda Pack 28.09.16 - Public Page 5 of 44

Update action log to have as standing item and to discuss with other CCG’s to aim consistency.
30.05 K Harding (KH) or representative to present slides at a future meeting. FT to chase.
15.4 Action closed but to be reinstated on log for Sally Ross Benham (SRB) to attend a meeting with the relevant Councils
38.16 Notification of Any Other Business
38.01 CG wished to raise the possibility of having an informal session on what NHSE envisage co-commissioning will look like now and in the future.
Action: session to be confirmed either before or after meeting for an hour with Fiona Theodom (FT) to lead.
39.16 Primary Care Strategy
39.1 This would be a standing item on the agenda.
39.2 A Council of Members workshop is scheduled in September to enable a discussion of the practicalities and reality of GP’s changing to meet the strategy over the next five years along with the STP vision.
39.3 FT to complete an information sheet for the CoM workshop in September on funding stream rules.
39.4 It is unclear what monies are involved which makes it difficult to plan.
39.5 Helen Stratton (HS) stated that £2.4 billion has been stated by NHSE, however there are conflicting information on the finances, is this new money and how to access this. More clarity is required, presently the only money available is from PMS but this is not badged to be used as MPC.
39.6 SRB would continue to create a strategy without any confirmed financial details, as this would be an evolving document
39.7 SN had produced a brief strategy.
39.8 The Committee wished to see the strategy before going to the Governing Body in October.
40.16 Primary Care Development Group Minutes
40.1 Meeting not held in July, however a question raised was about the change of contract from Serco to Capita.
JCC PC Agenda Pack 28.09.16 - Public Page 6 of 44
40.2 Tracey Lewis (TL) reported that there had been a national savings drive to cut 40% in efficiencies, part of this exercise was to review Exeter and the new formula for Carr-hill. Exeter system is expected to be redundant and replaced by a simpler system. All data currently held by Exeter will have to be addressed and integrated into the new system, this is not envisaged to be in place before April 2018.
41.16 NHSE Performance Report
41.1 FT presented the Primary Care Commissioning Report for July 2016, and stated that there were no significant changes since last month’s report.
41.2 HS asked if the new structure reflected dedicated budgets for TUPE.
41.3 FT replied that NHSE recognised that there may be changes in the next six months when the CCG’s take on fully delegated commissioning and this is currently being worked on.
41.4 JA stated that considering the changes ahead what resources from NHSE for Primary Care are to be given to the CCG’s.
41.5 FT replied that there were no resources per se, but working on how to provide resources to the CCG and also support other services such as Pharmacy, Dental and Optometry.
41.6 MT stated that the CCG needed to be clear about the sequence of meetings for the move to delegated commissioning to be communicated to, and at the latest the December Governing Body.
41.7 HS stated that there needs to be local decisions on how to deliver local outcomes.
41.8 JA asked about conflict of interest around transfer of resources between NHSE and the CCG.
41.9 FT replied that ongoing discussions will be held with NHSE and the CCG if the need arises.
42.16 NHSE Finance Report
42.1 TL presented the summary report for month 4 - July 2016, which provides an overview of the expenditure to date versus budgets for all practices in North Norfolk CCG.
42.2 TL highlighted the following:
i. Future reporting will contain more detailed information.
ii. Budgets to the Practices may look different on a month to month basis due toincreased accuracy of coding.
42.3 Discussion by the members took place on Practice budgets and the variances, with the assurance that these will be scrutinised by the CCG’s Chief Finance Officer.
JCC PC Agenda Pack 28.09.16 - Public Page 7 of 44

43.16 NHSE Estates Report
43.1 The committee noted the Estates Report prepared by KH.
44.16 Any other business
None
45.16 Questions from members of the public
None present
46.16 Date of and time of next meeting
Wednesday 28th September 2016, 2.30-4.30pm at the Jubilee Family Centre, Aylsham.
JCC PC Agenda Pack 28.09.16 - Public Page 8 of 44

Joint Commissioning Committee for Primary Care
Actions Log – 24th August 2016
Public Meeting
Will miss target date Action necessary to meet target
Set to meet target date Complete and closed
Meeting Date Item Ref. Action By whom By when Action Status 22.05.16 3.3 ToR: Clarification required on the working of para 13 relating to
voting rights of committee members. 27.07.16: FT to share wording prior to next meeting 24.08.16 ongoing to be brought to next meeting
JY
FT
22.06.16
24.08.16
G
22.05.16 6.4 Explore and develop information requirements for the committee 24.08.16- to have as a standing item on the agenda
SRB/JS SRB
28.09.16 28.09.16
G
27.07.16 30.5 SRB to seek clarification from KH for premises funding streams 24.08.16 KH or representative to present slides at future meeting
SRB/KH KT
24.08.16 G
22.06.16 15.4 Invite North Norfolk District Council and Broadland District Council to attend a future meeting to discuss developments, planning, S106/CIL. 24.08.16 re opened as need to extend invitation
SRB asap G
Closed Actions
Meeting Date Item Ref. Action By whom By when Action Status 22.06.16 16.2 (ii) AP to find out type of information recorded in relation to patient
engagement with primary care performance. AP 27.07.16 B
JCC PC Agenda Pack 28.09.16 - Public Page 9 of 44

Unconfirmed Minutes of the Primary Care Development Group Tuesday 9th August 2016
Rees Coghlan Room at the Aylsham Care Trust
Present:
Dr James Gair (Chair) (JG), Executive Team Member/GP – Birchwood Surgery Linda Marquis (LM), Practice Manager – Mundesley Surgery Tracy Neave (TN), Practice Manager - Cromer Surgery Tee Randall (TR), Practice Manager – Acle Surgery Sally Ross-Benham (SRB), Head of Primary Care Commissioning – NNCCG Fiona Hinton (FH), Practice Manager – Market Surgery Dr Anoop Dhesi (AD), Chair - NNCCG/GP – Stalham Surgery (from 10.20am)
In attendance:
Fiona Craig (FC) – Commissioning Manager – NNCCG for item 12/16 Jan Turton (JT) – Clinical Project Manager – NNCCG for item 13/16
Apologies:
Dr Penny Ayling, Paul Juson, Rebecca Champion, Jon Fox, Tony Belham
09/16 Minutes of the previous meeting
These were confirmed as an accurate record of the meeting and will be taken to the next Joint Commissioning Committee for Primary Care on 24th August.
10/16 Action Log
The action log was reviewed and updated (see attached).
11/16 Feedback from Joint Commissioning Committee for Primary Care (JCC PC)
11.1 SRB provided feedback from the meeting on 27th July. Currently the meetings are focussed on governance and fact finding from NHSE. Particular points of discussion at the joint committee were:
- Primary Care Strategy – updating on current situation of NNCCGs strategy; questions around where the strategy fits into the STP and the difficulties that this presents.
- Transfer from Serco to Capita - The PCDG group were very keen to know if the money saved from the transfer of the contract to Capita will be ploughed back into
JCC PC Agenda Pack 28.09.16 - Public Page 10 of 44

general practice. The group also wanted to feedback to NHSE that they did not feel that the service had improved following the transfer to Capita, many practices are still awaiting patient notes and have experienced other issues such as the ordering of equipment which is unreliable and sporadic. The group were also interested to know whether NHSE were sticking to their improvement plan and asked for clarity around the funding streams that are available. SRB agreed to raise these questions with NHSE and keep the PCDG informed.
- Patient Allocation Scheme is out to tender - Vulnerable practices - Practice finances – pots of money held centrally for items such as rent, waste
which will be allocated to CCGs - Primary Care Finance Workshop involving all Norfolk CCGs finance leads is
being held prior to the joint committee meeting on 24th August - Liaising with Broadland District Council (BDC) and North Norfolk District
Council (NNDC) to discuss growth in the North Norfolk area. BDC are attending the September meeting; SRB has tried to engage with the Head of Planning at NNDC but to date there has been no response.
4/16 Practice Visits Log
4.1 The log was circulated to the group to give an oversight of the current required actions following the practice visits. Particular points for discussion were:
- TICCS – TICCS liaison has received feedback issues. It was commented that the service provided by TICCS was no better than that given by the previous provider.
- Issues around nurse practitioners reading/receiving/ordering blood/xray results and having to pay £50 for nurse practitioners to undertake training for this.
5/16 Primary Care Strategy
SRB updated that an outline will be presented to the Executive Group on 16th August after which it will be circulated to the PCDG. There will be a workshop at September’s Council of Members meeting. A stakeholder event is planned for providers, GPs, the LMC and community engagement panel giving them the opportunity to participate and feed into the strategy. SRB anticipates finishing the draft by the end of October with sign off at the Governing Body.
6/16 Performance Measures
The group discussed ways in which NNCCG could measure the effectiveness of primary care services. It was recognised that it is not feasible for practices to have too many audits and that there is already a lot of data available through other means (primary care website, QOF, CQC data packs) which could be tapped into.
JCC PC Agenda Pack 28.09.16 - Public Page 11 of 44

There was a discussion about patient access to general practice. There is a Healthwatch report available which focussed on working with practices to explore ways to improve how they work with their patients and patient accessibility.
There was further discussion about the need to vocalise and demonstrate the pressure on general practice which has increased significantly particularly in the number of patient appointments. It is not possible for practices to continuing absorbing this pressure.
7/16 NN4 Update
SRB updated that there will be a meeting on 10th August with CCG, NCHC & NCC colleagues to develop the care plan templates. A key post for workload allocation has been identified working with practices and district nursing staff using existing hub resources.
8/16 Estate Bids
Feedback from NHS England is due at the end of August. NNCCG bid totalled £2.3m. If funding is approved NNCCG will work with an estates expert to develop plans.
9/16 Electronic Prescribing Service (EPS)
EPS is being rolled out across practices in North Norfolk. Leaflets are in hand.
10/16 QIPP Ideas
QIPP ideas had been submitted from the following practice: Aldborough, Drayton, Ludham and Stalham Green, Blofield and Mundesley. The group considered whether the submissions met the appropriate criteria in order to be progressed further.
Aldborough – For GP practices to be more involved in diagnosis/treatment of patients with dementia
Outcome of discussion: This idea was not approved as the group felt that the current shared care by hospitals/GPs worked well,
Drayton – Point of care testing to determine need for antibiotics in respiratory conditions
Outcome of discussion: Further information required on results of pilots currently underway. E Layward to producing costings of service.
Ludham and Stalham Green – Employed health trainers
JCC PC Agenda Pack 28.09.16 - Public Page 12 of 44

Outcome of discussion: Although the group recognised the benefit of the health trainers they did not feel this idea would save the CCG money. There was discussion about producing a signposting sheet to raise awareness of providers such as Broadly Active and Active Norfolk. F Craig agreed to produce some information for this.
Blofield – Facility to arrange ‘urgent’ blood transfusion to treat symptomatic anaemia without an emergency admission.
Outcome of discussion: SRB will explore this idea further with A Touray.
Mundesley – CCG supporting no FP10 prescribing skin emollients
Outcome of discussion: The group suggested a Home Remedies QIPP – a rolling programme of messages, posters and leaflets for patients about a variety of topics such as:
- Important items to keep in your medicine cabinet - When to call 999 - Signposting to different services
11/16 GMS/PMS Monies
SRB reported that there will be approximately £200k. The group discussed ways in which the money could be equally distributed between practices. The discussion focussed on using the money to support a primary care enhanced diabetes service and possibly funding a liaison service to support practice nurses. SRB to meet with J Turton and T Shayes to explore this option further.
12/16 Frequent Flyers and Links to Housing
F Craig provided the following update:
1. Focussing on targeting a different population of people and working with Marketand Birchwood Surgeries in order to create closer links with housing. Alsoworking with NNDC and Broadland District Council. Surgeries will be able toprovide a list of complex patients who might benefit from housing support oradaptations.
2. Targetted work on carers: trying to establish better links with carers. Workingwith Mat Phillips at Stalham Staithe surgery to find hidden carers and ensuringthey have the correct level of support. Currently finding a cohort of carers andlinking in support.
3. Frequent flyers: 10B list when patients are discharged from hospital - this list isbeing reviewed to facilitate community discharges.
13/16 Pre-Diabetes Prevention Programme
JCC PC Agenda Pack 28.09.16 - Public Page 13 of 44

J Turton circulated information regarding the programme.
14/16 Any Other Business
i. J Turton – Respiratory QIPP hoping to elaborate on the work undertaking lastyear for COPD, rather than mentoring nursing, in the first instance, with practiceswith high rates of respiratory patients, nurses will go into practices to reviewpatients then take a clinic with a respiratory nurse.
15/16 Date of Next Meeting
Tuesday 6th September from 2pm-4pm in the Nigel Grimsey Room, Aylsham Care Trust.
JCC PC Agenda Pack 28.09.16 - Public Page 14 of 44

SUBJECT Reinvestment of PMS funding
PRESENTED BY Sally Ross-Benham
SUBMITTED TO Joint Commissioning Committee for Primary Care (JCC PC) – 28th September 2016
PURPOSE OF PAPER The JCC PC is asked to:
receive and note the following report agree the proposal
IMPACT ON PATIENTS This will improve the health outcomes for patients of North Norfolk with respiratory conditions and pre-diabetes symptoms. It will reduce the need for more invasive, costly interventions at a later date for the patient.
OUTCOME OF EQUALITY IMPACT ASSESSMENT
To the CCG’s accountability and responsibilities
EXECUTIVE SUMMARY:
In North Norfolk CCG the switch of practices with a PMS contract to a GMS contract has released £220.5k of primary care budget in 2016/17 for the CCG to reinvest in a way that is equitable across practices and addresses local pressures, in agreement with NHS England.
There are two areas that NNCCG are proposing to reinvest the money in for 2016/17;
1. A locally commissioned service from primary care for an enhanced community respiratory
service. Cost £150,000
2. A locally commissioned service from primary care for pre‐diabetes pathway. Cost £70,000
Enhanced Community Respiratory Service
One of the highest costs incurred by NNCCG relates to respiratory diseases and their complications when patients with these LTCs attend one of the three acute hospitals in Norfolk. The Commissioning for Value Information for the CCG suggests there are financial and quality savings resulting from variation particularly in asthma, COPD and pneumonia care. Building on the work done to date with practices in reviewing the pathway and care of patients with respiratory conditions the CCG would like to introduce a primary care locally commissioned service for an enahnced community respiratory service enabling primary care to improve practice and to reduce unwarranted variation as well as improving clinical effectiveness and patient
Agenda item: 9
JCC PC Agenda Pack 28.09.16 - Public Page 15 of 44

experience; this will include clear guidance on patient identification and patient management: identifying those patients with COPD who will benefit from further interventions that are targeted according to their exacerbation levels, and reduce the number of emergency admissions. The introduction of a new locally commissioned service in this area will be supported by the
introduction of a GPwsI clinic led by respiratory specialists from primary care.
Pre‐Diabetes (PreDM) Locally Enhanced Service.
People with PreDM have a 12 times increased risk of developing type 2 diabetes (Santaguida et al 2005). Diabetes is a chronic and progressive disease that impacts upon almost every aspect of life. Life expectancy can be reduced by up to 15 years, with individuals largely dying due to macrovascular complications including cardiovascular disease and amputations2. Half of those who are diagnosed with Type 2 diabetes present with advanced complications. In the absence of intervention, the majority of PreDM patients are likely to develop Type 2 diabetes within five to ten years (Nathan et al 2007)1.
Various studies have shown that intervention can significantly reduce the risk of developing diabetes. The identification and management of PreDM therefore provides a substantial opportunity for preventing the future burden of Type 2 diabetes. Evidence suggests personalised lifestyle and educational interventions can delay or even reverse the disease process in patients with PreDM. As CVD accounts for much of the morbidity and mortality associated with Type 2 diabetes, even small reductions in cardiovascular risk would be clinically significant. The Wanless Report (2004)2 noted there is scope for significant cost‐ savings through the prevention of diabetes, earlier diagnosis and better management.
NHS Health Checks are expected to pick up many new cases of both Type 2 diabetes and PreDM over the next five years. Yet there is currently no national pathway or established guidance on the management of patients with PreDM, hence the need for a local pathway and guidelines. North Norfolk CCG has successfully bid to provide the NHS Diabetes Prevention Programme (see details below) and is introducing a locally commissioned serviced that aims to incentive practices to establish registers of patients with PreDM, give them lifestyle advice and interventions if necessary (for example, statins or antihypertensive medication) and recall them annually.
KEY RISKS: The volume of patients may be higher than expected which could lead to the service costing more than anticipated.
IMPACT ASSESSMENT
RESOURCE REQUIRED (if appropriate): £220k
REPORT DISCUSSED WITH:
REFERENCE DOCUMENT(S): PMS-GMS Monies 2016-17 word document.
JCC PC Agenda Pack 28.09.16 - Public Page 16 of 44

PMS reinvestment 2016/17 North Norfolk CCG
North Norfolk Clinical Commissioning Group
PMS Reinvestment 2016/17
1.0 Introduction
In North Norfolk CCG the switch of practices with a PMS contract to a GMS contract has
released £220.5k of primary care budget in 2016/17 for the CCG to reinvest in a way that is
equitable across practices and addresses local pressures, in agreement with NHS England.
There are two areas that NNCCG are reinvesting the money in for 2016/17;
1. A locally commissioned service from primary care for an enhanced community
respiratory service.
Cost £150,000
2. A locally commissioned service from primary care for pre‐diabetes pathway.
Cost £70,000
2.0 Enhanced Community Respiratory Service
One of the highest costs incurred by NNCCG relates to respiratory diseases and their
complications when patients with these LTCs attend one of the three acute hospitals in
Norfolk. The Commissioning for Value Information for the CCG suggests there are financial
and quality savings resulting from variation particularly in asthma, COPD and pneumonia
care.
Building on the work done to date with practices in reviewing the pathway and care of
patients with respiratory conditions the CCG would like to introduce a primary care locally
commissioned service for an enhanced community respiratory service enabling primary care
to improve practice and to reduce unwarranted variation as well as improving clinical
effectiveness and patient experience; this will include clear guidance on patient
identification and patient management: identifying those patients with respiratory
conditions who will benefit from further interventions that are targeted according to their
exacerbation levels, and reduce the number of emergency admissions.
The introduction of a new locally commissioned service in this area will be supported by the
introduction of a GPwsI clinic led by respiratory specialists from primary care.
JCC PC Agenda Pack 28.09.16 - Public Page 17 of 44

PMS reinvestment 2016/17 North Norfolk CCG
It will address the current wide variation in patient reviews, care and therapy across NNCCG by:
Introduction of a bespoke “standardised” electronic COPD Templatefor EMIS and SystmOne
Continue the delivery of education and up‐skilling of local respiratorypractice nurses/clinicians, by intensively targeted upskilling of thecurrent respiratory practitioners in GP practices ‐ to enable them tobetter manage patients in line with NICE COPD Guideline 2010
Raise awareness of the effectiveness of pulmonary rehabilitation
Earlier and accurate diagnosis of COPD: support implementation ofopportunistic COPD case finding in primary care through electronicdecision support tools e.g. OPC Tools; the roll out of the second datadownload by OPC will compare previous data from 2015 download.
Give clear guidance on patient management and support servicesavailable in the community including links with the integrated carecoordinator.
Cost savings will be realised from: A reduction in emergency admissions (primarily COPD exacerbations)
by using targeted patient identification. Reduction in COPD related pneumonia admissions: to be achieved by
continued education and advice around appropriate reduction in the prescribing of high dose ICS drugs, to thereby improve quality for patients who are currently inappropriately prescribed high dose ICS. These drugs have serious side effect /quality implications for patients (including increased risk of pneumonia), and cost impact on the CCG.
Objectives
Objective Number Objective Description Outcome Benefit
1. Support the delivery of treatment in Primary Care for patients with COPD: through the reintroduction of GPwsI clinics led by respiratory specialists from either primary care.
Reduction in COPD respiratory related unplanned admissions in 2016‐17
This will encourage earlier and more accurate diagnosis of COPD, with
JCC PC Agenda Pack 28.09.16 - Public Page 18 of 44
PMS reinvestment 2016/17 North Norfolk CCG
appropriate ongoing treatment.
Closer monitoring of those COPD patients who are at greatest risk
The opportunity to explore ways in which we can ensure NNUH discharge EA patients to primary care.
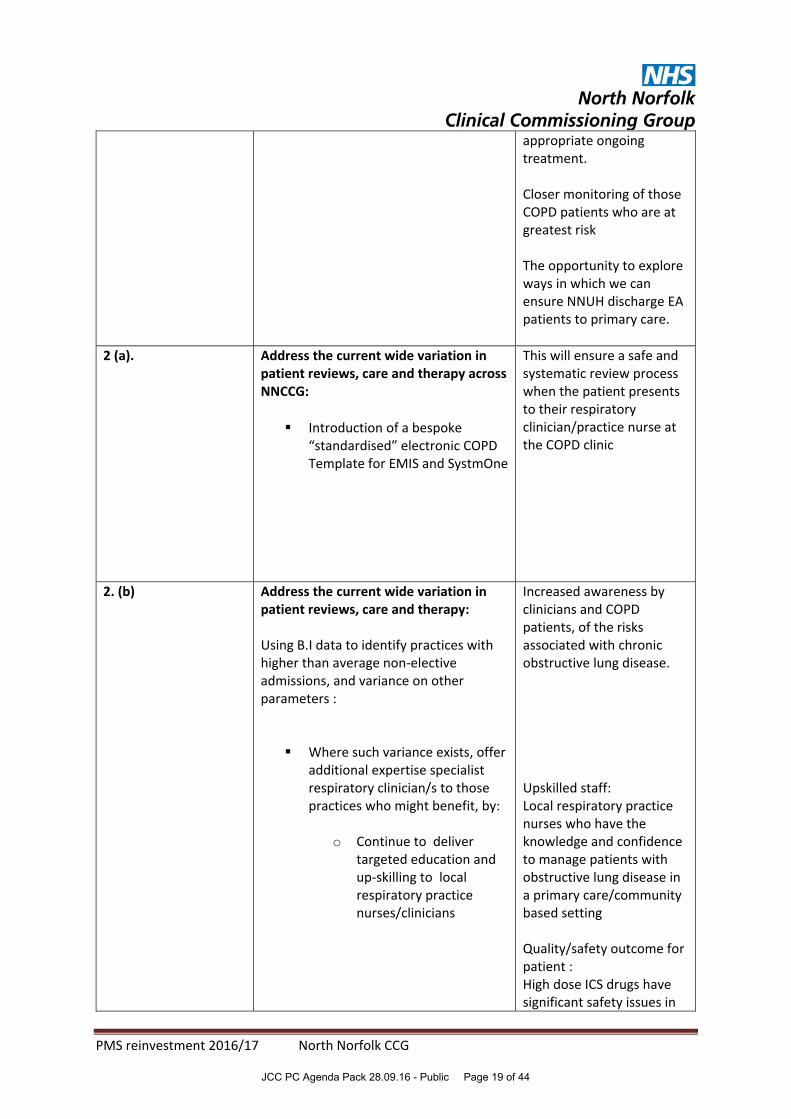
2 (a). Address the current wide variation in patient reviews, care and therapy across NNCCG:
Introduction of a bespoke“standardised” electronic COPDTemplate for EMIS and SystmOne
This will ensure a safe and systematic review process when the patient presents to their respiratory clinician/practice nurse at the COPD clinic
2. (b) Address the current wide variation in patient reviews, care and therapy:
Using B.I data to identify practices with higher than average non‐elective admissions, and variance on other parameters :
Where such variance exists, offeradditional expertise specialistrespiratory clinician/s to thosepractices who might benefit, by:
o Continue to delivertargeted education andup‐skilling to localrespiratory practicenurses/clinicians
Increased awareness by clinicians and COPD patients, of the risks associated with chronic obstructive lung disease.
Upskilled staff: Local respiratory practice nurses who have the knowledge and confidence to manage patients with obstructive lung disease in a primary care/community based setting
Quality/safety outcome for patient : High dose ICS drugs have significant safety issues in
JCC PC Agenda Pack 28.09.16 - Public Page 19 of 44

PMS reinvestment 2016/17 North Norfolk CCG
terms of side effects including cataracts, osteoporosis, diabetes and pneumonia
Reduced CCG prescribing costs.
Optimisation of therapy for those patients at risk of exacerbations, by:
Referral topulmonaryrehabilitationprogrammes
A self‐managementplan put in place,leading toimprovedawareness ofpatients in self‐care, leading tofewer crises orexacerbations
3. Make cost savings by: *Using targeted patient identification onexacerbation risk using OPC reports in the practices
*Specific BI data on admissions,categorised by Practice *Target the usage of high dose ICS (asindicated by OPC reports in Practices); to be achieved by continued education and advice around appropriate reduction in the prescribing of high dose ICS drugs, to thereby improve quality for patients who are currently inappropriately prescribed high dose ICS.
A reduction in emergency admissions,
Reductions in ICS prescribing (of specifically identified patients), leading to cost savings and reduced incidence of pneumonia; These drugs have serious side effect /quality implications for patients, and cost impact on the CCG
4. Raise awareness across all practices in NNCCG, of the effectiveness of pulmonary rehabilitation
A study in 2010 evaluating the effect of pulmonary rehabilitation delivered post COPD exacerbation
JCC PC Agenda Pack 28.09.16 - Public Page 20 of 44

PMS reinvestment 2016/17 North Norfolk CCG
NICE has stated that all those with COPD who are suitable for pulmonary rehabilitation should receive it
http://www.csp.org.uk/professional‐union/practice/evidence‐base/physiotherapy‐works/COPD
showed a reduction in re‐admissions of 26 per cent with cost effectiveness demonstrated
Glenfield hospital in
Leicester, UK has been
offering a pulmonary
rehabilitation programme
to patients with chronic
heart failure (CHF) as well
as to those with COPD.
Both sets of patients show
a marked improvement.
NB: This evidence is helpful
for the potential development
of a separate QIPP “Rehab”
Project
5. Earlier and accurate diagnosis of COPD:
Implementation of opportunisticCOPD case finding in primarycare through electronic decisionsupport tools e.g. OPC Tools; theroll out of the second datadownload by OPC will compareprevious data from 2015download
Identification of new/existing patients with COPD who are at risk of 2 or more exacerbations in the next twelve months. This second data download will also identify those patients not at serious risk of exacerbations, who are suitable for step down from high dose ICS
Discussion of the COPD diagnosis with patients (and carers) will help them better manage their condition (e.g. though signposting to advice on stop smoking and benefits of exercise/pulmonary rehab
Targeting case finding on those at high risk of having undiagnosed COPD will result in earlier diagnosis
JCC PC Agenda Pack 28.09.16 - Public Page 21 of 44

PMS reinvestment 2016/17 North Norfolk CCG
and evidence based chronic disease management
3.0 Pre Diabetes (PreDM) Pathway
Why do we need diabetes prevention?
People with PreDM have a 12 times increased risk of developing type 2 diabetes (Santaguida et al 2005). Diabetes is a chronic and progressive disease that impacts upon almost every aspect of life. Life expectancy can be reduced by up to 15 years, with individuals largely dying due to macrovascular complications including cardiovascular disease and amputations2. Half of those who are diagnosed with Type 2 diabetes present with advanced complications. In the absence of intervention, the majority of PreDM patients are likely to develop Type 2 diabetes within five to ten years (Nathan et al 2007)1.
Various studies have shown that intervention can significantly reduce the risk of developing diabetes. The identification and management of PreDM therefore provides a substantial opportunity for preventing the future burden of Type 2 diabetes. Evidence suggests personalised lifestyle and educational interventions can delay or even reverse the disease process in patients with PreDM. As CVD accounts for much of the morbidity and mortality associated with Type 2 diabetes, even small reductions in cardiovascular risk would be clinically significant. The Wanless Report (2004)2 noted there is scope for significant cost‐ savings through the prevention of diabetes, earlier diagnosis and better management.
NHS Health Checks are expected to pick up many new cases of both Type 2 diabetes and PreDM over the next five years. Yet there is currently no national pathway or established guidance on the management of patients with PreDM, hence the need for a local pathway and guidelines. North Norfolk CCG has successfully bid to provide the NHS Diabetes Prevention Programme (see details below) and is introducing a locally commissioned serviced that aims to incentive practices to establish registers of patients with PreDM, give them lifestyle advice and interventions if necessary (for example, statins or antihypertensive medication) and recall them annually.
The NHS Diabetes Prevention Programme (‘NDPP’) was announced in the NHS Five Year Forward View, published in October 2014, which set out the ambition to become the first country to implement at scale a national evidence‐based diabetes prevention programme modelled on proven UK and international models, and linked where appropriate to the new NHS Health Check. The NDPP is a joint initiative between NHS England, Public Health England and Diabetes UK which aims to deliver at a large scale services for people already identified with non‐diabetic hyperglycaemia, and who are therefore at high risk of developing Type 2 diabetes. High risk individuals will be offered a behavioural intervention to enable them to reduce their risk of developing Type 2 diabetes through weight loss, improved diet and increased levels of physical activity.
JCC PC Agenda Pack 28.09.16 - Public Page 22 of 44

PMS reinvestment 2016/17 North Norfolk CCG
It was locally agreed in Sept 2015 that NNCCG would act as the “Lead Organisation” on
behalf of five other partners;
Norfolk County Council (Public Health)
Norwich CCG
South Norfolk CCG
Norwich Medical School, University of East Anglia
Norfolk & Norwich University Hospitals NHS Trust
Having become a successful provider for programme NNCCG will deliver the NHS DPP, as
defined in the national specification. This service specification provides the minimum service
and quality requirements they must adhere to; this is supplemented by the local “spec”
which we have developed for central Norfolk.
Key aspects of NDPP ‐ Motivating people to enrol on programmes will be a shared
responsibility between local NHS and public health services and NHS DPP providers. Local
health economies will be required to identify eligible at risk individuals, as providers will not
be able to undertake this function. The remainder of the referral pathway will need to be
developed locally, and our demonstrator sites indicate that this requires input from providers.
Providers will only be in a position to contact people referred to them where consent has
been secured for the referral. The provider will be expected to make contact to discuss
enrolment on to the programme and will be held responsible for encouraging attendance and
participation. NHSE/PHE have constructed a payment mechanism that incentivises providers
to retain people on programmes.
When a participant completes or stops attending the programme, a discharge summary will
be provided to the referring practitioner. Referral pathways from this point will be down to
local determination.
There is no funding for GP practices to take on additional clinical work through this scheme
and we would like to further improve preventative care for those patients identified at risk of
diabetes by introducing a locally commissioned service for practices.
Under the locally commissioned service the practice will set up a register is to include patients with:
A history of gestational diabetes,
Impaired fasting glycaemia (>6 to < 7mmol/l) Impaired glucose tolerance (7.8‐11.0mmol/l)
HbA1c IFCC 42 to 47 mmol/mol
Exclude patients already diagnosed with diabetes.
JCC PC Agenda Pack 28.09.16 - Public Page 23 of 44

PMS reinvestment 2016/17 North Norfolk CCG
Practices will build a register of pre‐diabetes patients and ensure it is updated as appropriate.
The patients on the PreDM register will be invited for an annual review which will include:
Blood tests – HBA1C, Cholesterol, HDL, Us&Es
History taking
Measurements
BMI
Blood Pressure
Smoking status and advice
Alcohol assessment
CVD Risk
Option of referral to the Norfolk diabetes Prevention Programme
Advice
Education and treatment as appropriate
4.0 Conclusion
It is hard to be specific about exactly how many patients this will prevent needing secondary
care or proceeding on to a diabetic diagnosis but it is absolutely necessary to resource primary
care to deliver more preventative solutions if we are to improve health outcomes for patients
and make the whole healthcare system work more effectively.
JCC PC Agenda Pack 28.09.16 - Public Page 24 of 44

SUBJECT GPC Focus on industrial action and undated resignations
PRESENTED BY Dr Linda Hunter
SUBMITTED TO Joint Commissioning Committee for Primary Care (JCC PC)
PURPOSE OF PAPER The JCC PC is asked to:
receive and note the following
IMPACT ON PATIENTS
OUTCOME OF EQUALITY IMPACT ASSESSMENT
To the CCG’s accountability and responsibilities
EXECUTIVE SUMMARY:
KEY RISKS:
IMPACT ASSESSMENT
RESOURCE REQUIRED (if appropriate):
REPORT DISCUSSED WITH:
REFERENCE DOCUMENT(S):
Agenda item: 10
JCC PC Agenda Pack 28.09.16 - Public Page 25 of 44

Focus on industrial action and undated resignations
August 2016
JCC PC Agenda Pack 28.09.16 - Public Page 26 of 44

Executive Summary
Clearly, any proposals for action must balance the intended impact with the effect on patient care, ensuring that patient safety remains paramount.
Mass submission of undated resignations (page 5 onwards)
As part of co-ordinated action, GPs would submit to the BMA their letters of resignation
from their practice contract/salaried contract
The conditions under which the BMA could submit these letters would be specified in
advance
GP partners would need to take account of any contractual obligations they are subject to
when submitting an undated resignation letter, for example their partnership agreement
No breach of contract involved and no need to inform the commissioner at the time of
submitting the undated resignation
If not all partners in a practice wanted to submit undated resignation, partnership would
need to be mindful of viability of practice with remaining partners
Partnership would be liable for costs of any practice redundancies and other associated
costs, for example premises
Salaried GPs participating would be resigning from their contract with their practice
GPs resigning from their contracts would not be guaranteed an alternative contract in
future
GPs resigning from their contract would need to consider alternative employment options
in order to continue receiving an income
Industrial action that could lead to a breach of contract (page 8 onwards)
GP partners do not have the same (limited) immunities from the consequences of taking
industrial action as employees do
If a practice refuses to do something which is a contractual obligation, they could be served
with a breach notice or have their contract terminated irrespective as to whether it is done
as part of a campaign of industrial action
Forms of industrial action which would breach contractual or other legal obligations could
include:
o The complete or partial withdrawal of essential services
o The complete or partial withdrawal of other contracted services (without lawful
termination of the contract on the required notice)
o Non-compliance with various statutory and regulatory requirements such as:
Not undertaking appraisals (which would breach performer’s list
obligations)
Not undertaking revalidation (which would breach GMC rules)
Please note that this summary must be read in conjunction with the full guidance in order to ensure you are fully and accurately informed of the complexities of this subject.
JCC PC Agenda Pack 28.09.16 - Public Page 27 of 44

Failure to cooperate with the CQC (which would breach statutory
requirements and which could result in a termination of practice
registration and an inability of provide primary medical services)
Locum salaried GPs are not a party to the contract between the practice and the
commissioner and so are not directly affected by it
A ‘trade dispute’ between a salaried/locum GP and their practice would need to be proven
for salaried/locum GPs to take protected industrial action
Industrial action that would not breach the contract (page 11 onwards)
The withdrawal of services that are over and above their contractual obligations would
not constitute a breach of contract but could nonetheless be a form of industrial action
Such options may include:
o Increased use of external referral as a means of discharging the obligation to
provide essential services
o Withdrawal of non-contractual services that GPs voluntarily provide
o Withdrawal from additional services, such as the provision of contraceptive
services
o Withdrawal from enhanced services, such as the provision of minor surgery,
extended hours
o Withdrawal from the quality and outcomes framework
o Temporary suspension of new patient registration
JCC PC Agenda Pack 28.09.16 - Public Page 28 of 44

Introduction
The purpose of this guidance is to provide GPs with a broad overview of the main areas to note should they be in a situation where they are considering, or being asked for their willingness to, submit undated resignations and/or take industrial action.
The broad categories of action that GPs could consider taking include:
i. The mass submission of undated resignations
ii. Industrial action - involving the breaches of contracts by GP contractors
iii. Industrial action of a type that doesn’t breach contracts
iv. Action that is neither industrial action nor a breach of contract
It is important to note that there must be a trade dispute in place in order for any industrial action to be taken.
JCC PC Agenda Pack 28.09.16 - Public Page 29 of 44

Mass submission of undated resignations
How does the process of undated resignations work?
Submitting an undated resignation does not breach a GP contractor’s contract, but is clearly a significant step to take.
The concept of an undated resignation is that as part of action co-ordinated by the BMA, the GP practice, in accordance with its own governance procedures (which may in a partnership be by way of majority vote) determines to provide to the BMA with a letter of resignation, addressed to their commissioning body, for the BMA to date and send in prescribed circumstances. Where the GP practice consists of a single GP contractor this decision is likely to be easier to take than in larger practices.
An individual GP contractor who has been unable to persuade the GP practice to submit an undated resignation may wish to provide the BMA with a personal undated resignation from his/her practice. As discussed below GP contractors will need to be mindful of any contractual obligations under their partnership agreement, such as notice periods, in preparation for the eventuality of the BMA sending the as yet undated resignation to the practice.
The GP practice/contractor would need to provide the BMA with a written mandate providing the BMA with the authority to date and send the letter in prescribed circumstances. The mandate would need to specify:
A minimum number of resignations for the BMA to hold before it has the power to submit
the same on behalf of the GP practice/contractor
The conditions in which the BMA is authorised to submit the resignation.
At the time of any prospective action, careful consideration would need to be given to the authorisation that the BMA would be provided with. Matters that would need to be considered would include whether the authorisation were to be subject to a time limit and whether, and in what circumstances, the GP practice/contractor would be able to revoke the authorisation that it has provided to the BMA.
There would be no need for the GP practice or individual GP contractor to notify the commissioner or the GP Practice that it has given such a notice to the BMA to send.
Once the resignations have been submitted by the BMA on behalf of the GP practice or the contractor, then the GP practice/contractor would have formally resigned from their partnership and/or from their contract. The remaining partners would be under no obligation to offer a new partnership opportunity to the resigning GP in the future. Similarly the commissioner would be able to accept that resignation and would be under no obligation to offer the GP practice another contract. Likewise the commissioner would be able to offer the GP practice a less advantageous contract in the future.
The service of a notice of resignation on a commissioner will take effect in accordance with the contractual provisions. Six months’ notice is the standard provision in the GMS contract or three months when the GP contractor is a sole practitioner, and the GP practice would be required to work out the contractual notice period in the normal way. The service of a notice on a GP practice by a resigning GP contractor will take effect in accordance with the governance arrangements of the practice concerned.
JCC PC Agenda Pack 28.09.16 - Public Page 30 of 44

Once a notice of resignation had been served the GP practice/contractor would not have any entitlement to change their mind, however they would be free to contact the commissioner/ GP practice to see if the commissioner/GP practice was agreeable to the notice of termination being withdrawn and/or a new relationship being agreed.
Does the GP contractor need to have regard to provisions within their partnership agreement?
Yes. Some partnership agreements contain a provision requiring that no more than one partner can resign within any given period of time. Depending upon the wording of the partnership agreement this may pose problems if two or more partners are planning to submit resignations at the same time. GP contractors in such circumstances would be well advised to take independent legal advice so as to avoid exposing themselves to legal liabilities from their partners for breaching the partnership agreements. It may be that the partners are agreeable to a Deed of Variation to allow for multiple resignations at the same time; however this will be a matter for discussion and possibly negotiation.
What is the position if some of the partners wish to submit undated resignations and other partners do not?
As described above the partners should have regard to the content of their partnership agreements. In principle the contract with the commissioner may survive a resignation of part of the partnership, although the resource implications on the remaining partners would need to be considered in terms of the practice viability.
What are the ramifications of undated resignations on salaried GPs?
A salaried GP who learns that the partners within their practice have submitted undated resignations may worry about the security of their job.
The salaried GP would also be aware that if the BMA were to send resignations en masse that there may be a large number of other salaried GPs facing redundancy at the same time as themselves and conclude that it is better to move practice in advance of resignations being activated.
Can a salaried GP submit an undated resignation?
Yes, however, salaried GPs are not a party to the contract between the practice and the commissioner and so are not directly affected by it. If the BMA were to serve undated resignations provided by salaried GPs then it would have to serve these on to the Practices themselves for them to have legal effect. Salaried GPs may take a different view to partners, based on their specific contractual agreement with their practice, mindful that any resignation to lend political leverage to changes to the practice’s national contract, would result in a loss of their employment and income (and not necessarily any changes to their specific contract).
Can a locum GP submit an undated resignation?
JCC PC Agenda Pack 28.09.16 - Public Page 31 of 44
Some locums may consider they have already “resigned” from their national contract, and others may have chosen locum work as a rejection of the pressures in the national contract; therefore an undated resignation from locum work (and ceasing to receive an income) may not practically gain significant support. Further many locums typically work short term contracts or provide ad hoc sessions, therefore it may be that there is no contract to resign from. If the locum is working within a contractual arrangement for an agency, chambers or a practice, the same issues apply as in respect of salaried GPs above.
Can PMS contract holders resign their contracts in the same way as GMS practices?
Yes, all PMS contract holders can resign their contract in accordance with the terms of that contract. They would be shutting down their NHS contract and will need to retire or find an alternative source of work and would need to fund any costs associated with this decision in the same way as a GMS contract holder would.
Where a GP practice submits an undated resignation and resigns the practice contract, what liabilities do they hold for staff e.g. redundancies?
They will be liable for the costs of any redundancies, and potentially other costs relating to the closure of a practice, including any costs relating to premises and any other contractual obligations that the GP practice owes to any third parties. GP practices considering such action need to have regard to the contracts they have entered into including the provisions of any lease of premises, contracts of employment and contracts with any third parties and their partnership agreements.
Where a GP practice submits undated resignations and resign their contract, could a salaried GP claim constructive dismissal?
It is difficult to see good grounds for a claim of constructive dismissal in these circumstances.
Income implications of undated resignations
It is important to note that resigning from a contract of work would effectively cease income for the GP concerned, unless alternative work was undertaken. Seeking undated resignations without alternative employment proposals may seem an unrealistic expectation. The financial implications of this, and any additional liabilities, is likely to be a limiting factor for many GPs taking up this option, or expressing a willingness to do so.
JCC PC Agenda Pack 28.09.16 - Public Page 32 of 44

Industrial action that could lead to a breach of contract
While it is legal and possible for GP practices/contractors to take industrial action the legal implications are very different than they are for employees. While employees have certain limited immunities at law from the consequences of taking industrial action1, GP practices/contractors have no such immunity. Therefore any breach of contract by a GP practice/contractor is actionable against the GP practice/contractor irrespective as to whether it is done as part of a campaign of industrial action.
If a GP practice/contractor refuses to do something that is a contractual obligation then they could be served with a breach notice by the commissioner, or have their contract terminated depending upon the nature of the contractual breach.
Forms of industrial action that would breach contractual or other legal obligations could include:
i. The complete or partial withdrawal of essential services
ii. The complete or partial withdrawal of other contracted services (without lawful
termination of the contract on the required notice)
iii. Non-compliance with various statutory and regulatory requirements such as:
Not undertaking appraisals (which would breach performer’s list obligations).
Not undertaking revalidation (which would breach GMC rules).
Failure to cooperate with the CQC (which would breach statutory requirements
and which could result in a termination of practice registration and an inability
of provide primary medical services)
GP practices/contractors will in particular need to be mindful of provisions in their contract that give contractual force to the requirement to comply with all legislation and have regard to any guidance produced by the Secretary of State as required by section 94 of the GMS Regulations which states as follows:
“94 Compliance with legislation and guidance
The contractor must—
(a) comply with all relevant legislation; and
(b) have regard to all relevant guidance issued by the Board, the Secretary of State or local authorities in respect of the exercise of their functions under the Act”.
All of the above forms of industrial action would constitute a breach of contract and could have professional as well as commercial consequences for the GP contractor.
1 (providing that the provisions of the Trade Union Labour Relations (Consolidation) Act 1992 (‘TULRCA’) and, once it is in force, the Trade Union Act 2016, are complied with)
JCC PC Agenda Pack 28.09.16 - Public Page 33 of 44

What are the implications of taking industrial action for a GP practice / contractor?
GP practices/contractors could be served with breach notices, or have their contact terminated by their commissioning body, in response to industrial action.
In 2012, over 100 breach notices were served in London in response to the single day’s industrial action from GPs.
The legal advice at that time was that there was no effective action that GPs, or the BMA, could take to legally resist the breach notices.
What are the implications of taking industrial action for salaried GPs?
Before industrial action can be lawfully commenced there must be a ‘trade dispute’ between an employee and their employer. The meaning of trade dispute is defined in section 218 of the Trade Union Labour Relations (Consolidation) Act 1992 (‘TULRCA’) as follows:
“218 Meaning of "trade dispute" in Part IV
(1) In this Part "trade dispute" means a dispute between employers and workers, or between workers and workers, which is connected with one or more of the following matters—
(a) terms and conditions of employment, or the physical conditions in which any workers are required to work;
(b) engagement or non-engagement, or termination or suspension of employment or the duties of employment, of one or more workers;
(c) allocation of work or the duties of employment as between workers or groups of workers;
(d) matters of discipline;
(e) the membership or non-membership of a trade union on the part of a worker;
(f) facilities for officials of trade unions; and
(g) machinery for negotiation or consultation, and other procedures, relating to any of the foregoing matters, including the recognition by employers or employers' associations of the right of a trade union to represent workers in any such negotiation or consultation or in the carrying out of such procedures.”
GP practices/contractors would be claiming to have a dispute with their employer (the commissioner) on the basis of 218(1)(a) – terms and conditions of employment.
Salaried GPs would be taking industrial action against their employer, which would be the GP practice for which they work. In 2012, salaried GPs were able to take industrial action as the dispute related to their pension, which was part of their terms and condition of employment.
If the BMA is unable to demonstrate a trade dispute between salaried GPs and their employers then it cannot call upon them to take industrial action and any industrial action they do take would
JCC PC Agenda Pack 28.09.16 - Public Page 34 of 44

lack the protections afforded by TULRCA allowing their employers to dismiss them for a repudiatory breach of contract.
What are the implications of taking industrial action for locum GPs?
The same principles apply as for salaried GPs above. However, locums are potentially in a weaker position as they are often not going to be regarded as ’employees’, and if they are not employees they will lack any protection from taking industrial action even if they were able to establish a trade dispute.
Will GP practices/contractors benefit from the same protections from unfair dismissal that TULCRA provides for employees?
No, GP practices/contractors have no protection from unfair dismissal as this protection only applies to employees.
Once the Trade Union Act 2016 comes into force what turnout at ballot is needed for industrial action to be lawful and what percentage must vote in favour of industrial action for it to proceed?
A minimum turnout of 50% of those eligible to vote will be required for the ballot to be valid. In terms of the vote in favour of IA a simple majority is sufficient, however when, as in this case, the strike is to affect important public services there is an additional criteria that 40% of all members entitled to vote must have supported the industrial action for it to be legal.
JCC PC Agenda Pack 28.09.16 - Public Page 35 of 44

Industrial action that would not breach the contract
There may be some work that GP practices/contractors undertake that goes over and above their contractual obligations and the withdrawal of such services would not constitute a breach of contract but could nonetheless be a form of industrial action applied in a coordinated fashion by GPs, via the BMA, to place pressure on government to address legitimate concerns. Such options may include:
(i) Increased use of external referral as a means of discharging the obligation to
provide essential services
(ii) Withdrawal of non-contractual services that GPs voluntarily provide
(iii) Withdrawal from additional services, such as the provision of contraceptive
services
(iv) Withdrawal from enhanced services, such as the provision of minor surgery,
extended hours
(v) Withdrawal from the quality and outcomes framework
(vi) Temporary suspension of new patient registration
What are essential services?
The GMS Regulations do not seek to define in specific terms the range of functions or activities comprise ‘essential services’. The key provision is Regulation 17, which describes the services which the contractor must provide in paragraphs (4), (5) and (6). These services may be summarised as follows:-
“Paragraph (4):
Throughout core hours and ‘delivered in the manner determined by the practice in discussion with the patient’, services required for the management of registered patients and temporary patients, who are or believe themselves to be:-
(a) ill, with conditions from which recovery is generally expected: (b) terminally ill (c) suffering from chronic disease
‘Management’ is defined in paragraph (5) and includes:
(a) offering consultations and, where appropriate, physical examination for the purposes of identifying the need, if any, for treatment or further investigation; and (b) the making available of such treatment or further investigation as is necessary and appropriate, including the referral of the patient for other services under the Act and liaison with other health care professionals involved in the patient’s treatment and care.
Paragraph (6):
The provision of appropriate ongoing treatment and care to all registered patients and temporary residents taking into account their specific needs including
(a) advice in connection with the patient’s health including health promotion advice; (b) the referral of patients for other services under the Act”.
JCC PC Agenda Pack 28.09.16 - Public Page 36 of 44

It can be seen therefore that while the scope of ‘essential services’ is very wide, and will include diagnostic services, the manner in which the services are to be provided is to be determined by the practice in discussion with the patient, which clearly therefore allows for the possibility of such essential services to be provided by way of external referral.
What does increased use of external referrals for essential services involve?
The mere fact that a service is an essential service does not mean that the GP practice has to necessarily undertake all the work involved. If it is available to the patient via external referral then the GP practice can deliver the essential service by way of making an external referral of the service to be provided by, for example, a local hospital.
Examples of services that can often be obtained via external referral are likely to include, among other things:
Phlebotomy
ECGs
Spirometry
Ambulatory BP monitoring
Glucose tolerance testing or any other in-house pathology services
Routine pregnancy testing (where there is no requirement to exclude ectopic
pregnancy).
There is no case law on whether the increased use of external referral could lawfully be used as a means of industrial action, however there would appear to be scope, albeit with some risk, that a programme of industrial action could be conducted on this basis.
Withdrawal of voluntarily provided services
Many GP practices provide community nursing services. Sometimes these are commissioned as an ‘enhanced service’, and when they are then the relevant contract would need to be terminated or varied before any withdrawal of those services if it were to not constitute a breach of the contract. In some cases the services are provided without any contractual obligation upon the GP Practice / contractor, which is to say that the provision of these services via community nursing based services falls outside the scope of ‘essential services’. Examples of work undertaken by such community nursing services GPs provide are:
(i) wound care (including dressings and suture removal for procedures performed outside the practice);
(ii) nursing care of leg ulcers and other chronic conditions (including Doppler assessment);
(iii) nursing care for incontinent and catheterised patients;
(iv) ear syringing;
JCC PC Agenda Pack 28.09.16 - Public Page 37 of 44

(v) provision of prescriptions for conditions which are being managed solely by community nurses.
Rather than providing such services via the provision of community based nursing services the GP practice can take steps to ensure the provision of essential services via other means, such as external referral.
Withdrawal from additional services, enhanced services, or the quality and outcomes framework
A GP practice wishing to withdraw from additional services, enhanced services, or the quality and outcomes framework will need to have regard to the contractual notice provisions to which these are subject and give appropriate notice of such termination.
The commissioning body may procure the additional or enhanced services from another provider and may decline to offer the GP practice with the opportunity to provide such services in the future.
A GP practice that ceases to provide additional services will lose a defined % of their global sum. A GP practice who stops providing enhanced services will lose the payments related to that.
A GP practice who withdraws from QOF will lose the associated payments. . If they later re-join QOF in the same financial year they will find that the work required to satisfy the scheme is still required.
Temporary Suspension of Patient List
Regulation 21 of the GMS Regulations details the circumstances in which a GP practice can refuse to admit a patient onto the patient list.
It states that:
“…[t]he contractor may only refuse an application … if the contractor has reasonable grounds for doing so which do not relate to the applicant's age, appearance, disability or medical condition, gender or gender reassignment, marriage or civil partnership, pregnancy or maternity, race, religion or belief, sexual orientation or social class”.
A question has therefore arisen as to whether it would be lawful for the GP practice to refuse access to the patient list on ground that their trade union had asked them to do so as part of a campaign of industrial action. The answer to this question will hinge upon whether or not such a direction by a union constitutes ‘reasonable grounds’ for doing this. If the answer is ‘yes’ then there would not be a breach of contract and the industrial action would be lawful. If the answer is ‘no’ then the refusal would be a breach of contract and the practice would be exposed to breaches notices and termination.
There are a range of legal opinions (but no case law) upon this matter and practices cannot be confident that refusing applications to the patient list on this basis would be lawful.
The BMA is firmly of the view that where the reason for refusing an application to join the patient list is inspired by genuine patient safety concerns then it will be lawful for the GP practice to do the same. The BMA has produced guidance on this. It may well be that some practices should be considering refusing access to their patient lists on patient safety grounds and if general practice continues to be underfunded then this is likely to be increasingly the case in the future, this reality
JCC PC Agenda Pack 28.09.16 - Public Page 38 of 44

would not however lend itself well to a campaign of industrial action in which the union would need to be able to co-ordinate a start and end to such action in a coordinated way. There may be financial implications for practices not registering new patients, with the list size reducing due to patients moving or dying, and will impact greater in areas of greater turnover.
Nursing Homes
There is often an expectation that GP practices will, free of charge, provide services to residential and nursing homes that are additional to what practices are funded and commissioned to do through essential services. Such extra services are said to include demands for repeat prescriptions over and above practices’ usual arrangements; requests to write in the home’s clinical records in addition to keeping the normal clinical notes in the practice held patient record; the expectation of GPs carrying out regular weekly visits to the home regardless of clinical needs and requests to complete authorisation forms for staff to administer over the counter remedies.
Another commonly recurring issue is the expectation by nursing homes and/or pharmacies that practices should prescribe at seven day intervals for patients having their drugs dispensed by means of daily dosage trays and that this is done primarily to assist pharmacists on whom this obligation is said to fall.
In the absence of any contractual obligation to provide these services then the GP practice could withdraw them as part of a campaign of industrial action.
Schedule 3 Part 1 of the GMS Regulations provides, at paragraph 5, for circumstances where the GP may be required to attend a patient outside the practice premises. Such attendance may be required where, in the contractor’s reasonable opinion, it would be inappropriate for the patient to attend at the practice premises. These obligations will need to continue to be discharged in order to avoid a breach of contract, however this does not mean that GPs need to attend nursing homes where there is no clinical need to do the so.
Permitted Applications
GP contractors could make an application to reduce the size of their practice area, or for a formal closure of their list, or to temporarily opt-out of the provision of additional services. Commissioners are required to consider such applications that are made and act fairly and rationally in dealing with these requests. Therefore whilst there is some scope for a series of mass applications to cause administrative difficulty for commissioners, it is also probable that they would consider their options for responding to this action so limiting its potential effectiveness.
JCC PC Agenda Pack 28.09.16 - Public Page 39 of 44

SUBJECT Finance Report
PRESENTED BY Tracey Lewis, Interim Head of Finance (Direct Commissioning) NHS England
SUBMITTED TO Joint Commissioning Committee for Primary Care (JCC PC)
PURPOSE OF PAPER The JCC PC is asked to:
receive and note the following report
IMPACT ON PATIENTS
OUTCOME OF EQUALITY IMPACT ASSESSMENT
To the CCG’s accountability and responsibilities
EXECUTIVE SUMMARY:
KEY RISKS:
IMPACT ASSESSMENT
RESOURCE REQUIRED (if appropriate):
REPORT DISCUSSED WITH:
REFERENCE DOCUMENT(S):
Agenda item: 12
JCC PC Agenda Pack 28.09.16 - Public Page 40 of 44

North Norfolk CCG Joint Committee – Month 5 (August 2016) ‐ Financial Performance Reporting
This report gives an update of the financial performance against GP Primary Care budgets of
member practices up to Month 5 (August 2016). In 2016/17 joint commissioning arrangements are
limited to general practice services. This report provides an overview of the expenditure to date
versus budgets associated with North Norfolk CCG. Future period reporting will contain more
detailed information around year to date expenditure and year end forecasts in line with CCG
requirements. All detail is dependent upon the accuracy of the coding within the financial system
which is reviewed throughout the year.
A detailed report by expenditure type at practice level is produced on a monthly basis for discussion
at the next appropriate Joint Committee meeting in the annual meeting calendar. As a result of this
monthly review the CCG will note that budgets directly attributable to the practice within the CCG
may change month on month as coding becomes more accurate. It is this adjusted coding which will
inform any national submission for future delegated co‐commissioning budgets. As well as budgets
allocated directly to practices the CCG can expect to receive apportioned allocations for services not
directly paid to practices but which support GP contract delivery for example, clinical waste and
other discretionary payments.
North Norfolk
Year to Date Budget
Year To Date
Expenditure Variance
Full Year Budget
D82001 Holt Medical Practice GMS 2015 1,016,516 1,032,185 15,669 2,444,100
D82004 Cromer Group Practice GMS 2015 683,441 683,066 (375) 1,713,822
D82005 Sheringham Medical Practice GMS 2015 536,093 540,556 4,463 1,275,500
D82009 The Staithe Surgery GMS 2015 501,257 505,773 4,516 1,229,259
D82016 Market Surgery Aylsham GMS 523,684 535,557 11,873 1,287,768
D82025 Hoveton & Wroxham Medical Centre GMS 2015 656,584 647,544 (9,040) 1,541,498
D82028 Ludham & Stalham Green Surgery GMS 2015 401,096 402,038 942 974,540
D82029 Drayton & St Faiths Medical Practice GMS 2015 933,343 947,724 14,381 2,212,885
D82030 Hungate Street Surgery & Reepham Surgery
GMS 501,697 501,952 255 1,209,571
D82032 Brundall Medical Partnership GMS 473,094 476,057 2,963 1,166,305
D82038 Wells Health Centre GMS 2015 177,377 178,795 1,418 442,100
D82053 Mundesley Medical Centre GMS 2015 391,337 392,571 1,234 951,498
D82054 Fakenham Medical Practice GMS 2015 980,792 986,522 5,730 2,308,915
D82059 Birchwood Medical Practice GMS 2015 620,802 619,013 (1,789) 1,524,943
D82062 Coltishall Medical Practice GMS 540,865 512,492 (28,373) 1,195,279
D82066 Paston Surgery GMS 2015 414,952 419,083 4,131 1,010,877
D82080 Blofield Surgery GMS 414,743 420,245 5,502 1,114,529D82103 Horsford Medical Centre PMS (3) 0 3 0D82104 Acle Medical Partnership GMS 560,024 553,845 (6,179) 1,389,464
D82628 Aldborough Surgery GMS 2015 222,778 226,455 3,677 525,101
10,550,472 10,581,471 30,999 25,517,954
JCC PC Agenda Pack 28.09.16 - Public Page 41 of 44
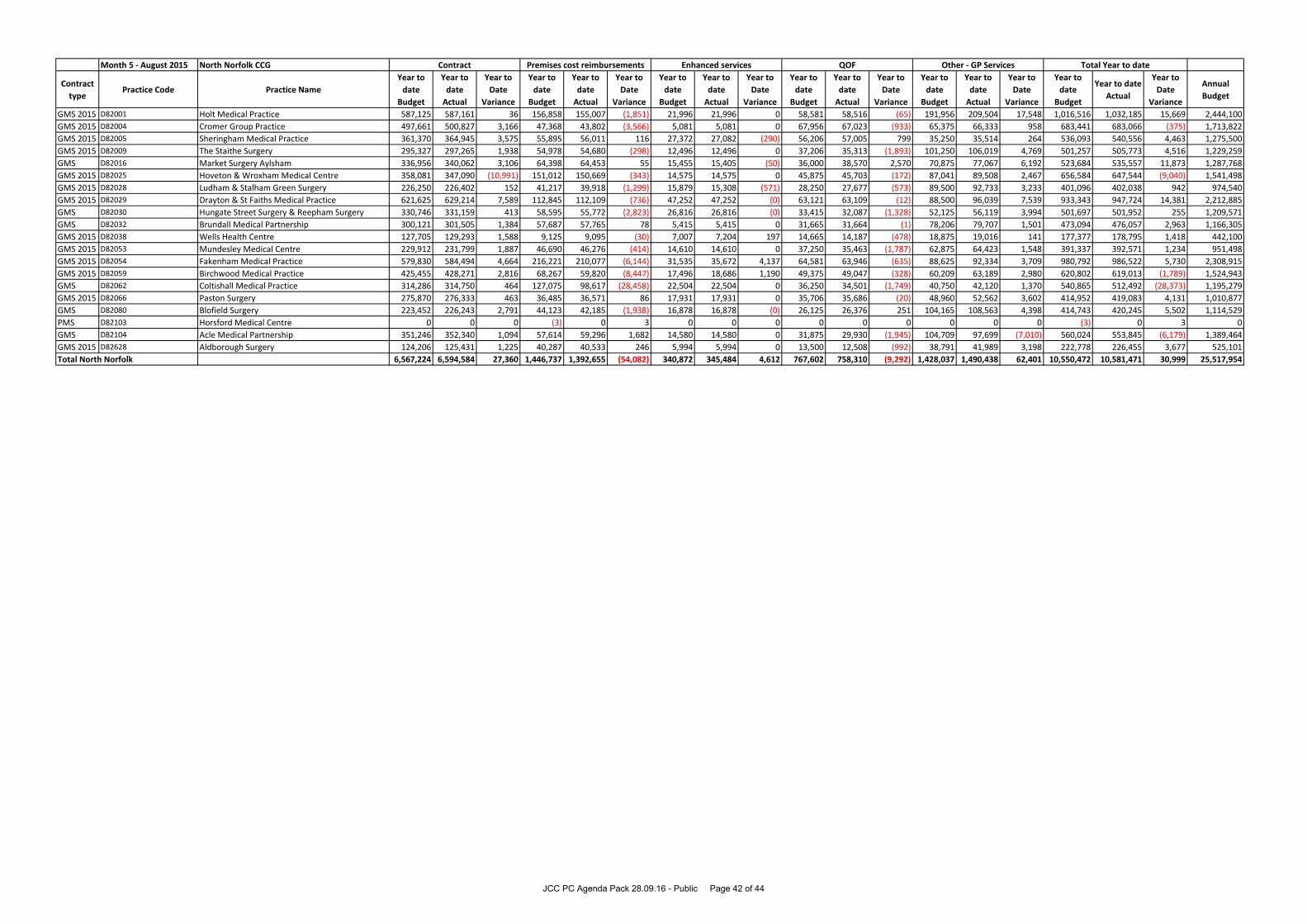
Month 5 - August 2015 North Norfolk CCG
Contract
typePractice Code Practice Name
Year to
date
Budget
Year to
date
Actual
Year to
Date
Variance
Year to
date
Budget
Year to
date
Actual
Year to
Date
Variance
Year to
date
Budget
Year to
date
Actual
Year to
Date
Variance
Year to
date
Budget
Year to
date
Actual
Year to
Date
Variance
Year to
date
Budget
Year to
date
Actual
Year to
Date
Variance
Year to
date
Budget
Year to date
Actual
Year to
Date
Variance
Annual
Budget
GMS 2015 D82001 Holt Medical Practice 587,125 587,161 36 156,858 155,007 (1,851) 21,996 21,996 0 58,581 58,516 (65) 191,956 209,504 17,548 1,016,516 1,032,185 15,669 2,444,100
GMS 2015 D82004 Cromer Group Practice 497,661 500,827 3,166 47,368 43,802 (3,566) 5,081 5,081 0 67,956 67,023 (933) 65,375 66,333 958 683,441 683,066 (375) 1,713,822
GMS 2015 D82005 Sheringham Medical Practice 361,370 364,945 3,575 55,895 56,011 116 27,372 27,082 (290) 56,206 57,005 799 35,250 35,514 264 536,093 540,556 4,463 1,275,500
GMS 2015 D82009 The Staithe Surgery 295,327 297,265 1,938 54,978 54,680 (298) 12,496 12,496 0 37,206 35,313 (1,893) 101,250 106,019 4,769 501,257 505,773 4,516 1,229,259
GMS D82016 Market Surgery Aylsham 336,956 340,062 3,106 64,398 64,453 55 15,455 15,405 (50) 36,000 38,570 2,570 70,875 77,067 6,192 523,684 535,557 11,873 1,287,768
GMS 2015 D82025 Hoveton & Wroxham Medical Centre 358,081 347,090 (10,991) 151,012 150,669 (343) 14,575 14,575 0 45,875 45,703 (172) 87,041 89,508 2,467 656,584 647,544 (9,040) 1,541,498
GMS 2015 D82028 Ludham & Stalham Green Surgery 226,250 226,402 152 41,217 39,918 (1,299) 15,879 15,308 (571) 28,250 27,677 (573) 89,500 92,733 3,233 401,096 402,038 942 974,540
GMS 2015 D82029 Drayton & St Faiths Medical Practice 621,625 629,214 7,589 112,845 112,109 (736) 47,252 47,252 (0) 63,121 63,109 (12) 88,500 96,039 7,539 933,343 947,724 14,381 2,212,885
GMS D82030 Hungate Street Surgery & Reepham Surgery 330,746 331,159 413 58,595 55,772 (2,823) 26,816 26,816 (0) 33,415 32,087 (1,328) 52,125 56,119 3,994 501,697 501,952 255 1,209,571
GMS D82032 Brundall Medical Partnership 300,121 301,505 1,384 57,687 57,765 78 5,415 5,415 0 31,665 31,664 (1) 78,206 79,707 1,501 473,094 476,057 2,963 1,166,305
GMS 2015 D82038 Wells Health Centre 127,705 129,293 1,588 9,125 9,095 (30) 7,007 7,204 197 14,665 14,187 (478) 18,875 19,016 141 177,377 178,795 1,418 442,100
GMS 2015 D82053 Mundesley Medical Centre 229,912 231,799 1,887 46,690 46,276 (414) 14,610 14,610 0 37,250 35,463 (1,787) 62,875 64,423 1,548 391,337 392,571 1,234 951,498
GMS 2015 D82054 Fakenham Medical Practice 579,830 584,494 4,664 216,221 210,077 (6,144) 31,535 35,672 4,137 64,581 63,946 (635) 88,625 92,334 3,709 980,792 986,522 5,730 2,308,915
GMS 2015 D82059 Birchwood Medical Practice 425,455 428,271 2,816 68,267 59,820 (8,447) 17,496 18,686 1,190 49,375 49,047 (328) 60,209 63,189 2,980 620,802 619,013 (1,789) 1,524,943
GMS D82062 Coltishall Medical Practice 314,286 314,750 464 127,075 98,617 (28,458) 22,504 22,504 0 36,250 34,501 (1,749) 40,750 42,120 1,370 540,865 512,492 (28,373) 1,195,279
GMS 2015 D82066 Paston Surgery 275,870 276,333 463 36,485 36,571 86 17,931 17,931 0 35,706 35,686 (20) 48,960 52,562 3,602 414,952 419,083 4,131 1,010,877
GMS D82080 Blofield Surgery 223,452 226,243 2,791 44,123 42,185 (1,938) 16,878 16,878 (0) 26,125 26,376 251 104,165 108,563 4,398 414,743 420,245 5,502 1,114,529
PMS D82103 Horsford Medical Centre 0 0 0 (3) 0 3 0 0 0 0 0 0 0 0 0 (3) 0 3 0
GMS D82104 Acle Medical Partnership 351,246 352,340 1,094 57,614 59,296 1,682 14,580 14,580 0 31,875 29,930 (1,945) 104,709 97,699 (7,010) 560,024 553,845 (6,179) 1,389,464
GMS 2015 D82628 Aldborough Surgery 124,206 125,431 1,225 40,287 40,533 246 5,994 5,994 0 13,500 12,508 (992) 38,791 41,989 3,198 222,778 226,455 3,677 525,101
Total North Norfolk 6,567,224 6,594,584 27,360 1,446,737 1,392,655 (54,082) 340,872 345,484 4,612 767,602 758,310 (9,292) 1,428,037 1,490,438 62,401 10,550,472 10,581,471 30,999 25,517,954
Total Year to dateContract Premises cost reimbursements Enhanced services QOF Other - GP Services
JCC PC Agenda Pack 28.09.16 - Public Page 42 of 44

SUBJECT Estates Report
PRESENTED BY Kerry Harding - Estates Adviser, NHS England
SUBMITTED TO Joint Commissioning Committee for Primary Care (JCC PC)
PURPOSE OF PAPER The JCC PC is asked to:
receive and note the following report
IMPACT ON PATIENTS
OUTCOME OF EQUALITY IMPACT ASSESSMENT
To the CCG’s accountability and responsibilities
EXECUTIVE SUMMARY:
KEY RISKS:
IMPACT ASSESSMENT
RESOURCE REQUIRED (if appropriate):
REPORT DISCUSSED WITH:
REFERENCE DOCUMENT(S):
Agenda item: 13
JCC PC Agenda Pack 28.09.16 - Public Page 43 of 44

NHS England and North Norfolk Clinical Commissioning Group
Primary Care Co‐Commissioning Joint Committee
September 2016
Part 1
1. Primary Care Infrastructure Fund (PCIF)
PCIF has been renamed ‘Estates and Technology Transformation Fund’ (ETTF). All CCG’s
have now submitted their estates and technology bids onto the portal, which is now
closed. Bids had to be in line with Strategic Estates Plans, supported in principle by the
CCG and prioritised. We received 10 bids from North Norfolk, 9 for improvements to
existing premises and 1 IT scheme. The final first stage review of bids is currently being
completed by the NHS England national team, on the basis on regional recommendations
already submitted. The outcome of the initial bid process is expected to be relayed to
applicants before the end of September.
Bids that are supported will be subject to due diligence before final approval is given for a
scheme/project.
2. Other Premises Developments
The only current project in North Norfolk is the Acle Medical Partnership Infection Control
works scheme, which is now complete
JCC PC Agenda Pack 28.09.16 - Public Page 44 of 44