perspectives on the past, present and future of cfast ... tokyo... · agreed to share data from 24...
TRANSCRIPT

Perspectives on the past, present and future of CFAST therapeutic area data standards development
Jon Neville, Critical Path Institute
CJUG-PhUSE Single Day Event 14 April 2017
1

Overview
• Background- what is Critical Path Institute (C-Path) and how did we get involved in CDISC therapeutic area standards?
• CFAST progress to date
• Understanding what drives change (with examples)
• Lessons learned/ future considerations
2

Disclaimers
The ideas shared in this presentation represent my perspective as a therapeutic area standards developer I cannot speak for CDISC, FDA, or PMDA
3

Cri$cal Path Ins$tute Created
Memorandum of Understanding created between the FDA and C-‐Path in 2005
Independent 501(c)3 founded in 2004 “… to foster development of new evalua$on tools to inform medical product development”
4

C-‐Path: A Public-‐Private Partnership
q Act as a trusted, neutral third party q Convene scien5fic consor5a of industry, academia, and
government for pre-‐compe55ve sharing of data/exper5se
• The best science • The broadest experience • Ac5ve consensus building • Shared risk and costs
q Enable itera5ve EMA/FDA/PMDA par5cipa5on in developing new methods to assess the safety and efficacy of medical products
• Official regulatory recogni5on through “qualifica5on” of Novel Methodologies / Drug Development Tools and development and use of data standards
5

Cri5cal Path Ins5tute Consor5a Twelve global consortia collaborating with 1,300+ scientists and 61 companies
Coalition Against Major Diseases Focusing on diseases of the brain
Coalition For Accelerating Standards and Therapies Data standards
Critical Path for Parkinson’s Consortium Enabling clinical trials in Parkinson’s Disease
Critical Path to TB Drug Regimens Accelerating the development of TB drug regimens and diagnostics
The Duchenne Regulatory Science Consortium Duchenne Muscular Dystrophy
International Neonatal Consortium Neonatal clinical trials
Polycystic Kidney Disease Outcomes Consortium
Multiple Sclerosis Outcomes Assessment Consortium
Patient-Reported Outcome Consortium Assessing treatment benefit
Electronic Patient-Reported Outcome Consortium Electronic capture of treatment benefit
Predictive Safety Testing Consortium Drug safety
Pediatric Trials Consortium Developing effective therapies for children
Biomarkers Clinical outcome assessment instruments
Clinical trial simulation tools Data standards In vitro tools

7
CAMD: The Value of Data Sharing, Standards, and Integration
q Nine member companies agreed to share data from 24 Alzheimer’s Disease trials
q The data were not in a common format q The data were remapped to CDISC
standards and pooled
q A new clinical trial simulation tool was created
and has been the first model endorsed by the FDA and EMA
q Researchers utilizing the model and the
database to advance research
Star5ng Point
Result
24 studies, >6500 pa5ents

CFAST, a joint ini$a$ve of Cri$cal Path Ins$tute (C-‐Path) and CDISC, was launched to accelerate clinical research and medical product development by facilita$ng the establishment and maintenance of data standards, tools and methods for conduc$ng research in therapeu$c areas important to public health. CFAST TA project collaborators include the U.S. Food and Drug Administra$on (FDA), TransCelerate BioPharma, Inc. (TCB) and the Na$onal Cancer Ins$tute Enterprise Vocabulary Services (NCI-‐EVS), with par$cipa$on and input from many other organiza$ons.
8
Coali5on For Accelera5ng Standards & Therapies (CFAST)

© CDISC 2016
CFAST Accomplishments - Snapshot • The CFAST Program is now in Year 5 • Published 29 Standards to date • Developed and piloted new processes, tools and
checklists • Developed what a TAUG should contain over time
§ Examples, metadata tables and implementation advice
• Utilized SHARE functionality as it became available
• Partnered with many different organizations § FDA, PMDA, C-Path Consortia, TransCelerate, NCI-
EVS, MS Society, One Mind, Gates, WWARN, CHDI, others..
9

Completed Standards – through September, 2016
Pre-CFAST
CFAST
Therapeutic Area Publication
Alzheimer’s Disease v1 Sep, 2011Tuberculosis v1 Jun, 2012
Pain Aug, 2012Virology v1 Dec, 2012Parkinson’s Dec, 2012
Polycystic Kidney Disease Feb, 2013Asthma Nov, 2013
Alzheimer’s Disease v2 Dec, 2013Multiple Sclerosis May, 2014
Diabetes Sep, 2014CV Endpoints Oct ,2014
Influenza Nov,2014QT Studies Dec, 2014
Chronic Hepatitis C Virus May, 2015Schizophrenia Jun, 2015Dyslipidemia Jun, 2015Virology v2 Sep, 2015
Traumatic Brain Injury Dec, 2015Diabetes ADaM Supplement Dec, 2015
COPD Jan, 2016Tuberculosis v2 Feb, 2016Breast Cancer May, 2016
Kidney Transplant Oct, 2016 Rheumatoid Arthritis Nov, 2016
Major Depressive Disorder Dec, 2016 Diabetic Kidney Disease Dec, 2016
Pain v1.1 Dec, 2016 Ebola Dec, 2016
Malaria Jan, 2017

© CDISC 2016
CFAST TA Standards Pipeline
11
Pre-CFAST 2012-2015 2015 2016 2017
Alzheimer’s v1 Asthma v1 Traumatic Brain Injury v1 One Mind
Kidney Transplant FDA-CFAST Yr3
Oncology – Lung FDA
Pain Univ of Rochester
Alzheimer’s v2 C-Path CAMD Consortium
Oncology - Breast Oncology – Colorectal FDA
CDAD FDA
Parkinson’s v1 Multiple Sclerosis MS Society
COPD Malaria Gates / WWARN
Polycystic Kidney Disease v1 PKD Foundation
Diabetes v1 Virology v2 FDA
Post Traumatic Stress Cohen Veterans Bioscience
TB v1 Gates Cardiology Endpoints v1 FDA
TB v2 (pediatrics) C-Path CPTR Consortium
Duchenne Muscular Dystrophy FDA – CFAST Yr3/C-Path D-RSC Consortium
Virology v1 Influenza FDA Rheum. Arthritis Ebola
Hepatitis-C FDA Cardiology Imaging Diabetic Kidney Disease
,
Schizophrenia FDA Oncology – Prostate FDA
HIV - FDA
Dyslipidemia Major Depression FDA CFAST Yr3
Huntington’s CHDI
http://www.cdisc.org/system/files/all/CFAST_ProjectPipeline.pdf

© CDISC 2016
TA Standards by Area Oncology
Infectious Diseases
Mental & Behavioral Disorders
Cardiovascular Neurological Chronic Respiratory Diseases
Autoimmune Diseases
Endocrinology Other
Breast Cancer v1 Tuberculosis v1 Tuberculosis v2, Gates
Schizophrenia FDA Dyslipidemia v1 Alzheimer’s v1,
v2
Asthma v1 Rheumatoid Arthritis v1
Polycystic Disease v1 University of Rochester
Pain v1 University of Rochester
Prostate Cancer v1 FDA
Influenza v1 Major Depressive Disorder v1 FDA
CV Endpoints v1 FDA
Traumatic Brain Injury v1 One Mind
COPD v1 Diabetes v1 Solid Organ (Kidney Transplant) v1 FDA
Colorectal Cancer v1 FDA
Hepatitis C, v1 FDA
Post Traumatic Stress Disorder v1 Cohen Veterans Bioscience
CV Imaging v1 Parkinson’s Disease v1
Diabetic Kidney Disease v1
Lung Cancer v1 FDA
Virology v1, v2 FDA
Bi-Polar v1 QT Studies v1
Multiple Sclerosis v1 MS Society
Malaria v1 Gates / WWARN
General Anxiety Disorder v1
Duchenne Muscular Dystrophy v1
Ebola v1 Huntington’s Disease v1
Vaccines v1
Parkinson’s v2
HIV v1 NIAID & FDA
CDAD FDA
4 9 8 4 5 2 1 3 2
12
Bold - ongoing Planned

© CDISC 2016
FDA Data Standards Catalogue v4.4 http://www.fda.gov/ForIndustry/DataStandards/StudyDataStandards/default.htm
Requirement of Study Data Standards – Data Exchange Standards
13
Studies that start after These dates.

© CDISC 2016
• Required e-Study Data for NDA’s using CDISC Oct 1st, 2016
• CDISC TA Standards may be used in NDA applications
14
(Slide courtesy of Hiroshi Sakaguchi, PMDA)
© CDISC 2016
Why so many changes? • Foundational standards (e.g., SDTM) were
created from relatively limited use cases
• Therapeutic areas take a closer look at more specific uses cases, which require specific strategies
• The next couple examples highlight where developers encountered a need for change in order to accommodate these use cases
15

EXAMPLE 1: VIROLOGY A NEW APPROACH TO MICROORGANISM NOMENCLATURE
16
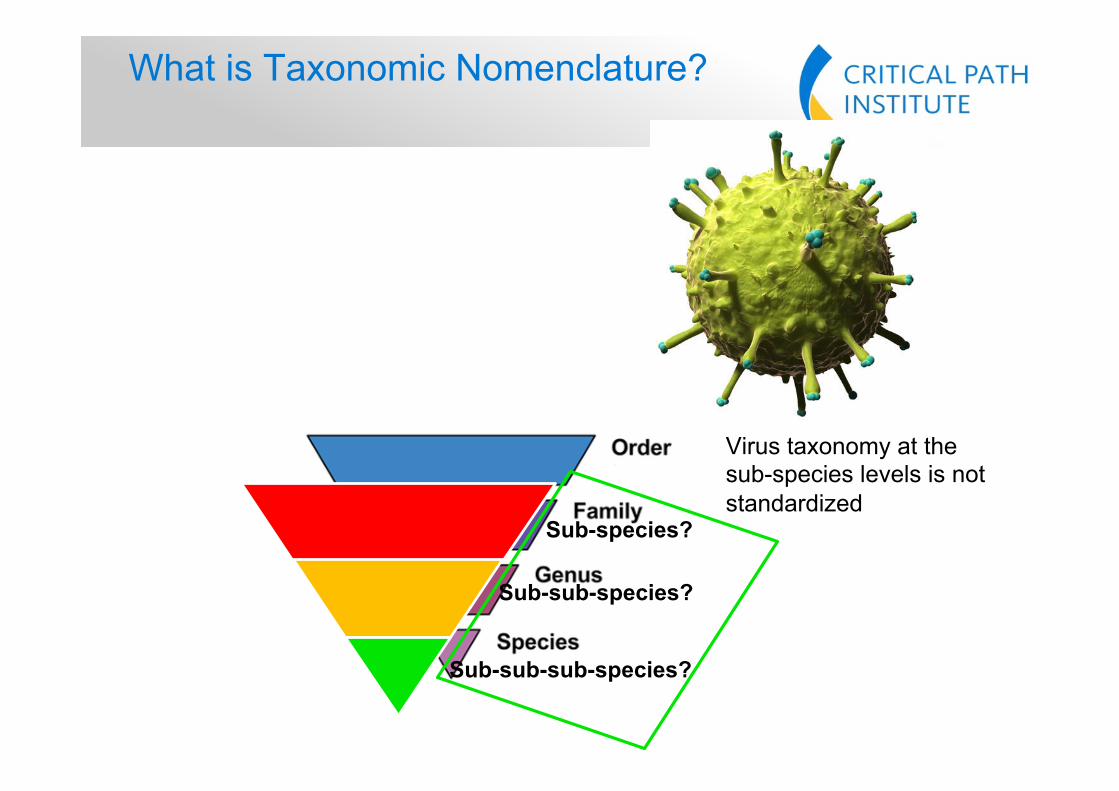
What is Taxonomic Nomenclature?
17
Sub-species?
Sub-sub-species?
Sub-sub-sub-species?
Virus taxonomy at the sub-species levels is not standardized

Virus Nomenclature- Virology v1.0
18
5. SPECIES and STRAIN were added to the domains to allow for the separation of genetic and genomic data from pathogens, such as viruses (that are the subject of this user guide) from genetic data on their human hosts (whose species and stain, if not human, would be submitted in the Demographics domain). 6. It was suggested that SUBSTRAIN and CLADE be added to the domains. However, because of ambiguous definitions and because the hierarchy used seems to differ, these potential additions were deferred until a future version.

© CDISC 2016
Virus Nomenclature Issue
19
HIV Influenza A Hep C Hep B HPV
SPECIES level Species Species Species Species Species Subspecies Level 1 Type Subtype Genotype Genotype Type
Subspecies Level 2 Group Strain Subtype Sub-‐genotype
Subspecies Level 3
Subtype (or Clade)
Recombina$on Type
Subspecies Level 4 Subclade
--NSPCES
--NSTRN?

© CDISC 2016
NHOID and Non-host Organism Identifiers (OI) Domain
20

© CDISC 2016
Advantages of NHOID/OI approach to Nomenclature • Agnostic with regard to pathogen nomenclature
terminology • Works for any non-host organism • It’s modular – take what you need:
§ NHOID provides a “snapshot” of bug identity § OI dataset provides parsed details of taxonomy when
needed without the need for countless new variables like –NSPCES and –NSTRN
21

EXAMPLE 2: TUBERCULOSIS A HARMONIZED APPROACH TO PHENOTYPIC DRUG SENSITIVITY TESTING (DST)
22

Phenotypic Drug Sensitivity Testing Results
SR SRR
ug/ml antibiotic

Microbiology Susceptibility Examples in SDTMIG 3.2: Why They Don’t Work
1. Sometimes the drug concentration is the result of the test and sometimes it is a pre-defined part of the test; the current model cannot support both structures.
2. Drug name is the test: a. Doesn’t tell you what the test is (i.e. MIC) b. Controlled terminology team will not control drug names
3. No where to represent information on the pathogen that is being tested. Must link back to the identification record in MB.

© CDISC 2016
Row STUDYID DOMAIN USUBJID MBSEQ MBLNKID MBTESTCD MBTEST MBORRES
1 ABC MB ABC-01-01 1 LKN03 MTBINH M. Tuberculosis INH Resistant
NEGATIVE
Row STUDYID DOMAIN USUBJID MSSEQ MSLNKID MSTESTCD MSTEST MSCAT MSORRES
1 ABC MS ABC-01-01 1 LKN03 GROWTH Growth DST NEGATIVE
2 ABC MS ABC-01-01 2 LKN03 DSTDRUG Drug Susceptibility Test Name
DST Isoniazid
3 ABC MS ABC-01-01 3 LKN03 DSTCONC Drug Susceptibility Test Concentration
DST 0.1
Drug Sensitivity Testing – TB v1.0
But… • Phenotypic drug susceptibility data is challenging to model as four separate
rows across two domains. • Susceptibility records need to be linked back to the identification in order to
determine what organism is the subject of the test.

© CDISC 2016
Drug Sensitivity Testing – Virology v1.0
26
7. Representing viral resistance data in an SDTM-based domain model is a challenge. An initial attempt was made to model these data in the Microbiology domains, but this approach was abandoned because the current MB/MS domain structures are limited to resistance based on only one result. Virology data, on the other hand, includes multiple results, and a net assessment that summarizes these results. The use of the LB domain, which already includes examples of viral test data, was next considered but this approach was felt to create too high a burden for creating test codes which would have included the virus as part of the test name. After considering these alternatives, the team chose to create a Viral Resistance (VR) domain that includes the species and strain variables, eliminating the need to maintain pathogen-specific test names.

© CDISC 2016
1. Virology team felt that viral resistance data could not be adequately supported by the MS domain so the Viral Resistance (VR) domain was created.
2. Created: a. Descriptive test codes without the drug name b. New variables for: species and drug name 3. Now have a structure works great for MIC, IC50 etc.!
But… • Now we have a VR domain and an MS domain. Does it make sense to
create a new resistance domain for each non-host organism ....fungi, parasites, worms etc.?
• The virology group did not create a corresponding virus identification domain analogous to MB. Can MB be used for all pathogen identification?
• How do we harmonize efforts and make one set of domains work for all relevant data?
YES!
Drug Sensitivity Testing – Virology v1.0

© CDISC 2016
Proposal for one all-encompassing MS domain
NHOID
• From Virology v1.0 • Use MSTESTCD/TEST to represent the name of the test. • Variable to represent the name of the drug being used.
• From Virology v2.0 • Use the NHOID variable to represent the organism that is the subject of the
test. • From TB v2.0
• Add two new variables to accommodate test results when the drug concentration is a pre-specified part of the test.
MSAGENT Microbial
Susceptibility Microbial
Susceptibility Microbial
Susceptibility
MICROSUS
MICROSUS
MICROSUS

© CDISC 2016
Advantages of a Unified Approach for Microbiology Domains
• One domain for all DST, regardless of non-host organism
• Allows results to represented in one domain as they are reported
• Provides unambiguous home for individual concepts (Test, drug, concentration and units, organism)
29

© CDISC 2016
Summary of changes discussed • --NSPCES and –NSTRN deprecated
(Addition of NHOID to be formalized in SDTM v1.6)
• VR domain deprecated in favor of a unified MS domain (Additional required variables MSAGENT, MSCONC, MSCONCU to be formalized in SDTM v1.6)
30
© CDISC 2016
What are We Getting at? • All early-version standards guides are “stakes in the
ground.” • Standards are continuously evolving as we learn more
and examine more use-cases • Updates and changes may appear abrupt, but only occur
after much vetting, discussion and feedback from the community, including implementers
• The good news: The more TAs we develop, the more overlapping concepts emerge (=REUSABILITY!)
31
© CDISC 2016
General Observations & Lessons Learned
• Focus has been on: § the number of standards developed § meeting timelines § SDTM and Terminology
• CDISC user community slow to implement TA standards § Difficult to implement, need to refer to other standards, hard to keep
up with the number of standards produced, user unwillingness to adopt due to provisional status
§ Clear request from CDISC community and Regulatory Authorities to slow down
• Cross-team dependencies, not fully considered § Resulted in re-work, more time needed, adjusted timelines § Contributed to inconsistency between standards; Foundational
standards not keeping pace
• Impact on Staff workload (C-PATH & CDISC, NCI-EVS), not fully considered
32

© CDISC 2016
Map of Teams – Foundational Teams are mostly Volunteer
33

© CDISC 2016
General Observations & Lessons Learned • No planning for maintenance of standards
§ now focusing on an update effort, increased work
• Addition of documents and deliverables by FDA § FDA Recommendations documents
• May not get these in the future § TA Specifications § FDA request for a “change log” capturing the differences
between public review and publication § Extend Public Review from 30 to 60 days
34

© CDISC 2016
Map of CDISC Products
35

© CDISC 2016
CFAST Collaboration – Next Steps • Move to “collaborative integration” model for project
organization: § Animal Rule (collaboration between CDISC/C-Path) § Already collaborating in this integrative manner on HIV v1 § The product will be a complete co-developed HIV v1.
• See concept map • TA projects scoped to reach B2E goals
§ (Protocol), CDASH, SDTM, ADaM, Terminology, QRS
36
CDISC C-PATH

© CDISC 2016
Integrative Standards Development Model
37
CDISC – Prevention C-Path – Treatment TAUG - HIV v1

© CDISC 2016
Next Steps for Future Projects • Aligned timelines
§ When there is more than on grant awarding organization and be transparent about the community it takes to develop a CDISC standard
• Redefine “success” § Greater focus on quality and completeness vs. quantity § Adoption of TAUGs Regulatory Authorities
• by user community – difficult to measure (TAC, CAC, TLC, Members) § Strive for a better balance between the CFAST project pipeline and foundational
standards development • Evaluate “topic guides” inclusion in the pipeline discussions.
• Revise grant writing process & template language to include B2E approach
38

© CDISC 2016 39
Approving Body
Approving Body Modeling
Consultation Team
MCT
Approval by MCT to start
Internal Review
SRC & Copy-Editing
SRC & Publication Committee
TLC-GC or TAPSC – Technical Leadership Team – Governance Committee or TA Steering Committee MCT- SR - Modeling Consultation Team - Super Reviewers Modeling Forum
Consider Translation Requirements
Copy-Editing, GSP and formatting
check
60-day Public Review

© CDISC 2016
Revised Process
40

© CDISC 2016
CDISC Review Councils
41
Modeling Review Council (MRC) Standards Review Council (SRC)
Provide early input on technical approaches (Concept Maps, CDASH, SDTM, ADaM, Controlled Terminology, XML Tech)
Review packages of documents/standards after internal review and prior to public review to ensure harmonization with existing standards
Review packages of documents/standards prior to internal review to ensure harmonization with existing standards
Ensure that all public review comments have been appropriately addressed
Review modeling issues that have been escalated for resolution from internal CDISC teams

Other future considerations
• Many concepts addressed in TAs apply to multiple disease areas
• The data modeling approaches to these concepts should be easier to find
• A new type of cross-cutting topic area user guide has been proposed
• Address a given concept with examples from multiple use cases
• Published as a standalone mini-guide • TAUGs could point to these guides
42

Examples of Cross-cutting Topics
Topic Teams Involved Description Combination Therapies / Drug Regimens
SDTM, CDASH, ADaM, SHARE* Representation of regimens that combine multiple products or even medications with other treatment modalities (e.g., radiation, surgery). Representation of active ingredient doses for combination products.
Patient Diaries SDTM, CDASH, SHARE* Agree how to represent timing of diary data., The occasions when diary data are collected are not visits defined in the Trial Visits domain, and there is disagreement about how they time periods evaluated should be represented (e.g., as intervals around time points or as retrospective questions relative to dates) Issues related to transcription or extraction of diary data into CRFs.
Imaging SDTM, CDASH, ADaM, SHARE* Consolidation of examples? Explaining representation of methods?
Assessment Intervals SDTM, ADaM, SHARE*
Epidemiology-based Findings
SDTM, CDASH, ADaM, SHARE* Trial design for epidemiological studies? Applicability of informed consent, disposition.
43
Pilot case: currently in
development

Conclusion
• CFAST has accomplished significant work in 5 years, and is the single biggest driver of change to foundational standards
• Changes to foundational models only happen after careful consideration of multiple stakeholder needs and use cases (though we acknowledge change can be disruptive)
• The process continues to evolve as we apply lessons learned in support of a higher quality output and broader impact analyses
44

© CDISC 2014 45