personality disorder integrated care pathway · “an integrated care pathway (or icp) is a...
TRANSCRIPT

Personality Disorder
Integrated Care Pathway
(PD–ICP)
November 2015

Acknowledgements
This document was produced by a partnership of NHS Highland staff, volunteers, service users
and staff from other public and third sector organisations.
The NHS Highland Personality Disorder Service will coordinate future reviews and updates of
this document.
NHS Highland would like to thank everyone involved in the creation of this document.
November 2015
Proposed review Date January 2017

Contents1 Introduction
1.1 Language and terminology ............................................................................................1
1.2 What is an ICP? ............................................................................................................1
1.3 What is Personality Disorder and why is an ICP necessary? .........................................1
1.4 How to use this ICP .......................................................................................................2
References...........................................................................................................................3
2 General Principles in Treating Personality Disorder
2.1 Introduction ...................................................................................................................5
2.2 Recovery .......................................................................................................................5
2.3 General Treatment Strategies .......................................................................................6
2.3.1 Collaboration ......................................................................................................6
2.3.1.1 Collaborative relationship ...................................................................6
2.3.1.2 Collaboration within and across teams ...............................................7
2.3.1.3 Social Network Involvement ...............................................................7
2.3.1.4 Mental Health Act and Compulsory Treatment ...................................7
2.3.1.5 Patient involvement ...........................................................................7
2.3.2 Consistency .......................................................................................................8
2.3.2.1 Treatment Frame ...............................................................................8
2.3.2.2 Splitting ...............................................................................................9
2.3.2.3 Endings and transitions ...................................................................10
2.3.3 Motivation .........................................................................................................10
2.3.4 Validation ........................................................................................................11
2.3.4.1 Case example ..................................................................................12
2.3.5 Self-management .............................................................................................13
2.4 Stages of Change Model (Trans-theoretical Model of Intentional Change) . .................13
2.5 Phases of Treatment .................................................................................................14
2.5.1 Phase 1 ............................................................................................................16
2.5.1.1 Case example ...................................................................................16
2.5.2 Phase 2 and 3 ..................................................................................................16
2.5.2.1 Case example ...................................................................................17
2.5.3 Timing and sequencing ....................................................................................17
2.6 Matched Care ...............................................................................................................17
References.........................................................................................................................20
3 Assessment, diagnosis and formulation
3.1 Assessment ..................................................................................................................21

3.1.1 Introduction .....................................................................................................21
3.1.2 Symptoms .......................................................................................................21
3.1.3 Personality Traits .............................................................................................21
3.1.4 Areas of assessment.........................................................................................23
3.2 Diagnosis .....................................................................................................................25
3.2.1 ICD-10 ..............................................................................................................26
3.2.2 F60 Personality Disorder ICD-10 (DCR-10) Criteria ........................................26
3.2.2.1 General Criteria for Personality Disorder ......................................................26
3.2.3 F60.0 Paranoid Personality Disorder ...............................................................26
3.2.4 F60.1 Schizoid Personality Disorder ................................................................27
3.2.5 F60.2 Dissocial Personality Disorder ...............................................................27
3.2.6 F60.30 Emotionally Unstable Personality Disorder, Impulsive Type . ..............27
3.2.7 F60.31 Emotionally Unstable Personality Disorder, Borderline Type ...............28
3.2.8 F60.4 Histrionic Personality Disorder ...............................................................28
3.2.9 F60.5 Anankastic Personality Disorder ............................................................28
3.2.10 F60.6 Anxious (Avoidant) Personality Disorder .............................................29
3.2.11 F60.7 Dependent Personality Disorder ...........................................................29
3.2.12 F60.9 Personality Disorder, unspecified .........................................................29
3.2.13 F61.0 Mixed Personality Disorders .................................................................29
3.2.14 DSM-IV ..........................................................................................................29
3.2.15 DSM-IV specific criteria for Borderline Personality Disorder ...........................29
3.3 Formulation ..................................................................................................................30
References.........................................................................................................................32
4 Self-management
4.1 Introduction .................................................................................................................35
4.2 What is self-management? ..........................................................................................35
4.3 Why is self-management important? ............................................................................36
4.4 Self-knowledge and self-reflection ...............................................................................37
4.5 Whose responsibility is self-management? ..................................................................37
4.6 What resources are available to support self-management? ........................................38
4.7 What have Highland patients found useful in supporting self-management? ...............39
References.........................................................................................................................41
5 Crisis Management
5.1 Introduction .................................................................................................................43
5.2 Crisis Planning ............................................................................................................44
5.3 Patient’s crisis (self-management) plan .......................................................................44
5.4 Clinical crisis care plan ................................................................................................44
5.5 Indicators of a Crisis ....................................................................................................44
5.6 Assessment and management of crises ......................................................................45
5.7 Risk assessment and management in crisis ................................................................46
5.8 Community management of crisis 47
5.9 Hospital management of crisis .....................................................................................47
5.10 After resolution of the crisis .......................................................................................47
References.........................................................................................................................48
6 Psychosocial Interventions
6.1 Introduction .................................................................................................................49
6.2 General psychosocial interventions .............................................................................50
6.3 Specific psychosocial interventions .............................................................................50
6.4 Interventions with a primary focus on Phase 1 .............................................................51
6.4.1 Dialectical Behaviour Therapy (DBT) ...............................................................53
6.4.2 Systems Training for Emotional Predictability and Problem Solving
(STEPPS) .....................................................................................................54
6.4.3 Cognitive Behaviour Therapy for Personality Disorder (CBTpd) . . ..................55
6.4.4 STAIRWAYS (follow-on group from STEPPS)...................................................56
6.5 Interventions with a primary focus on Phase 2 .............................................................57
6.5.1 Dialectical Behaviour Therapy—Prolonged Exposure (DBT-PE) . . .................58
6.5.2 Eye movement desensitisation and reprocessing (EMDR) ..............................59
6.5.3 Trauma Focused Cognitive Behavioural Therapy (tfCBT) ................................60
6.6 Interventions with a primary focus on Phase 3 .............................................................61
6.6.1 Occupational Therapy (OT) .............................................................................62
6.6.2 CAS Day Service for People with Personality Disorder ...................................63
6.6.3 Vocational Support Service ..............................................................................64
References.........................................................................................................................65
7 Medication
7.1 Introduction .................................................................................................................67
7.2 Medication for physical disorders .................................................................................67
7.3 Medication for co-occuring mental illness ....................................................................67
7.4 Medication for personality disorder ..............................................................................68
7.4.1 Managing polypharmacy .................................................................................69
7.5 Prescribing Principles ..................................................................................................70
7.5.1 Prior to starting treatment ................................................................................70
7.5.2 Having started treatment: ................................................................................71
References.........................................................................................................................72

8 Education and Awareness
8.1 Introduction ....................................................................................................................73
8.2 Education and awareness-raising resources ..................................................................73
8.3 Personality Disorder Integrated Care Pathway ...............................................................74
8.4 Scottish Personality Disorder Network (SPDN) ...............................................................74
9 Consultation
9 Consultation .....................................................................................................................75
10 Community Care
10.1 Introduction ................................................................................................................77
10.2 Primary Care .............................................................................................................77
10.2.1 When to refer to mental health services ........................................................77
10.2.2 General Principles .........................................................................................78
10.3 Community Mental Health Teams ..............................................................................79
10.3.1 Role of the CMHT in the treatment of Personality Disorder ...........................80
10.3.1.1 Assessment, Diagnosis and Formulation .......................................80
§1 Phase of treatment ....................................................................81
§2 Symptoms ...................................................................................81
§3 Personality Traits .......................................................................81
§4 Needs Assessment ....................................................................83
§5 Risk Assessment .......................................................................84
§6 Environmental Context ...............................................................84
10.3.1.2 Treatment and Management ..........................................................84
§1 What constitutes treatment of personality disorder
within a CMHT? .........................................................................84
§2 Care planning ............................................................................85
§3 Co-occurring disorders ...............................................................85
§4 Crisis planning ...........................................................................85
§5 Phase of treatment ....................................................................86
§6 Care Programme Approach ........................................................89
10.3.1.3 Risk management ...........................................................................89
10.3.1.4 Supervision ....................................................................................90
10.3.1.5 Social Network Involvement ............................................................90
References ......................................................................................................................92
11 Personality Disorder Service
11.1 Services offered by the PDS ......................................................................................93
11.1.1 Specialist Assessment and Treatment Recommendations ..............................93

11.1.2 Dialectical Behaviour Therapy (DBT) .............................................................93
11.1.3 Coping and Succeeding (CAS) Day Service ..................................................94
11.1.4 Consultation ..................................................................................................94
11.1.5 Education and awareness .............................................................................95
11.2 Services not currently offered by the PDS .................................................................95
11.3 How to access these services ...................................................................................95
References ......................................................................................................................96
12 Inpatient Care
12.1 An overview of the evidence ......................................................................................99
12.2 When to consider admission ......................................................................................99
12.3 During admission .....................................................................................................100
12.4 Discharge and transitions ........................................................................................100
12.5 Mental Health Act ....................................................................................................101
12.6 Structured Admissions Programme .........................................................................103
12.6.1 Specific characteristics of the Structured Admissions Programme..................105
References ......................................................................................................................106
Appendix Contents..............................................................................................................107


1. Introduction
This Personality Disorder Integrated Care Pathway Document (PD-ICP) has been developed by
a working group composed of a wide range of NHS Highland staff from different professional
backgrounds, representatives from other public sector and third sector organizations, volunteers
and service users. Every effort was made to consult widely at each stage of development to
ensure that the main aims of producing a clinically useful and well-used document were met.
This document updates and incorporates the NHS Highland Borderline Personality Disorder ICP
(BPD-ICP) which was originally completed in 2009. Whereas the 2009 BPD-ICP related only to
borderline personality disorder, this PD-ICP pertains to personality disorder more broadly.
1.1 Language and terminology
The sensitive nature of language and terminology remained apparent throughout the develop-
ment process. Agreement on terminology was sometimes difficult. For example, some people
preferred the term ‘patient’, some preferred ‘service user’ and some preferred ‘individual’. For
the sake of clarity, the decision was made to use the term ‘patient’ throughout the document and
to use the broad term ‘clinician’ to refer to health workers and social care workers employed by
NHS Highland. It was also decided to use the term ‘social network member’ rather than ‘carer’,
‘family member’ or ‘friend’. The term ‘carer’ in particular was felt, particularly by service user
members of the working group, to carry connotations of patients as passive recipients of care
rather than active participants in their own recovery. Aside from this one instance, no inference
should be drawn from the use of these particular terms as the choices were made by the
working group on a practical rather than a theoretical basis.
1.2 What is an ICP?
“An Integrated Care Pathway (or ICP) is a person-centred and evidence-based framework. It
tells multidisciplinary and multi-agency care providers, people using services, and their carers
what should be expected at any point along the journey of care. ICPs allow services to compare
planned care with what was actually delivered. This information can be used to develop services
and improve the patient journey.” (NHS QIS Standards for Integrated Care Pathways for Mental
Health Services, NHS Scotland, 2007)
In addition to these aims, this ICP aims to provide a single point where information, referral
forms and other useful resources can be easily found. In addition, it allows for NHS Highland’s
philosophy of care in relation to personality disorder to be made explicit.
1.3 What is Personality Disorder and why is an ICP necessary?
“Personality disorder refers to a complex mental disorder, not explainable by another adult
mental disorder, which represents a enduring and pervasive disturbance in the characterological
constitution and behavioural tendencies of an individual, usually involving several areas of
personality, and is nearly always associated with considerable personal and social disruption
and distress.” (World Health Organisation, 1993)
Personality disorder is common, affecting upwards of ten per cent of the general population. The
condition is typically associated with significant impairment of functioning and high levels of
1

distress for the sufferer and other people. People with personality disorder frequently have
contact with many different services and agencies, including primary care, general health,
mental health, housing, social work, criminal justice and third sector services. Not uncommonly,
these services find it challenging to effectively work with this group of people. This ICP aims to
provide guidance to promote best practice within NHS Highland and is based on best available
evidence. Although there is a significant risk of iatrogenic harm if this patient group is managed
inappropriately, many components of the disorder are eminently treatable and meaningful
sustained recovery is common.
1.4 How to use this ICP
This ICP has been divided into sections, each dealing with a particular aspect of the care and
treatment of personality disorder. The sections have been designed to stand alone and there will
inevitably be some overlap of content. Although the ICP itself is primarily a good practice
statement providing clinical guidance, another key aim has been to make easily available in one
place a repository of useful information, referral forms, educational materials and other
resources. The additional material can be located in the appendices, which will be updated as
required. The guidance in the body of the ICP itself will be reviewed on a yearly basis. The
Personality Disorder Service will take the lead in the updating and reviewing process. Although
the document can be printed, it is primarily intended to be used electronically and there are
internal and external click-able links throughout.
2
References
NHS Scotland. (2007). NHS QIS Standards for Integrated Care Pathways for Mental Health
Services.
World Health Organisation. (1993). International Classification of Disease, Tenth Edition, (ICD-
10).
3

4

2. General Principles in Treating PersonalityDisorder
2.1 Introduction
Personality disorder is an inherently complex condition which presents with difficulties in the
cognitive, affective, behavioural and interpersonal domains. Differing degrees of severity, along
with varying interpersonal and social contexts means that no two people with the disorder
present in the same way. Accordingly, it is widely recognised that a range of treatment and
management interventions are necessary to serve this patient group.
This section outlines some of the concepts which have influenced the development,
organisation and delivery of services for people with personality disorder in NHS Highland.
These include:
• Recovery
• General treatment strategies
• Stages of change model
• Phase-based treatment
• Matched care
2.2 Recovery
Treatment of personality disorder should follow recovery principles. Recovery is a framework for
thinking about mental health which is perhaps particularly applicable to personality disorder. A
full discussion of the recovery approach is beyond the scope of this document but the following
summary of important recovery principles, drawn from the Scottish Recovery Network website,
captures the key factors.
Any treatment for personality disorder should:
• Focus on what people can do, and on their unique attributes and characteristics rather
than focus on the things they cannot.
• Take a strengths based approach to the work and emphasise the role of hope and
optimism.
• Recognise recovery is a unique and individual experience and that people’s experiences
are influenced by their circumstances, background and life events. Opportunities and
circumstances also influence outcomes.
• Promote inclusion, equality and involvement.
• Recognise people are experts in their own experience and that empowerment is central to
wellness and recovery.
• Work towards goals which are important for the patient and which should be developed
collaboratively.
5

2.3 General Treatment Strategies
These strategies should inform the care and treatment of people with personality disorder in all
settings, not only to specific psychological interventions. Current evidence suggests that these
general therapeutic strategies are responsible for more of the benefit of any treatment for
personality disorder than any specific technique.
Although there is some overlap, the general treatment strategies can usefully be divided
between five headings:
• Collaboration
• Consistency
• Motivation
• Validation
• Self-management
2.3.1 Collaboration
2.3.1.1 Collaborative relationship
Building and maintaining a collaborative relationship (also referred to as the therapeutic alliance
or therapeutic relationship) is fundamental to the treatment of personality disorder. In contrast to
some mental state disorders such as major affective disorders and psychotic disorders, there is
little which can be delivered ‘to’ or ‘for’ the patient in terms of effective treatment. Rather,
personality disorder is a condition in which effective treatment can only be carried out ‘with’ the
person.
While outdated views of personality disorder as essentially untreatable have been overturned,
available evidence suggests that personality disorder is only a treatable condition within the
context of a collaborative relationship. In other words, if the patient does not wish to engage
collaboratively with treatment, then the disorder is untreatable. Shared understanding of this
principle is crucial for meaningful work to happen.
An important component of a collaborative relationship is a shared understanding of the roles
and responsibilities of both patient and professional. At the most basic level, the clinician is
responsible for delivering a reasonable standard of care and, unless there are very clear
reasons to assume otherwise (e.g. severe co-occurring major mental illness), each patient is
assumed to be a competent adult, responsible for their own choices and the consequences of
those choices. Encouraging each patient to take responsibility and engage collaboratively with
treatment is necessary to enable valuable positive risk taking to occur. Such an approach can
also assist clinicians to avoid assuming responsibility for patients and thereby making clinical
decisions that are unhelpful in the longer term, such as providing extended hospital admissions.
A collaborative relationship can help instil a sense of optimism and hope, and provide a basis for
a collaborative search for understanding. Furthermore, such a relationship encourages the
collaborative setting of realistic treatment targets and effective acquisition of skills and
knowledge. In addition, it enables modelling of effective interpersonal functioning and helps
maintain motivation in patients and professionals.
Ruptures within the relationship between patient and professional are to be expected. When
this occurs, the focus should be on early identification of markers of rupture, exploration of the
6
reasons for the rupture, and exploration and validation of the patient’s thoughts and feelings
about the rupture. Rapid repair to the relationship is the aim. This may require finding solutions
to prevent the rupture recurring.
2.3.1.2 Collaboration within and across teams
Collaboration is not only important between patients and professionals but also between
different professionals, teams and agencies. Good communication and joined-up working helps
ensure consistency. A shared care model will often be valuable in working with this patient
group, in which different clinicians and services work together to implement different parts of a
treatment plan.
2.3.1.3 Social network involvement
Members of the patient’s social network should be involved in the treatment plan where
appropriate. Education about the condition, along with a shared understanding of the
formulation and the treatment plan (and their role within it) can improve collaboration and
outcomes.
2.3.1.4 Mental Health Act and Compulsory Treatment
Compulsory treatment should be avoided except in exceptional circumstances and voluntary
treatment should resume as soon as possible. The potential harm of removing responsibility
from the patient and associated loss of collaborative working should be carefully considered.
Any benefit of detention is likely to occur at the safety and containment phases of treatment
only. Self-regulation and control are unlikely to occur while the patient’s responsibility for
themselves is removed and thus meaningful stabilisation is unlikely. Furthermore, there is no
good evidence for the effectiveness of compulsory treatment and some specialist psychological
interventions (e.g. Dialectical Behaviour Therapy or DBT) specifically state that patients should
engage with the treatment voluntarily. Similar cautions apply to patients who have been
instructed to attend a treatment program by the courts or other agencies.
2.3.1.5 Patient involvement
Patient involvement and collaboration is important not only within the treatment of individual
patients but also for the development and delivery of services for people with personality
disorder.
Patient involvement in services can be conceptualised as a continuum with increasing levels ofinput:
• Information: Patients are given information about services. Examples include provision
of leaflets and open days.
• Consultation: Information, views and feedback about services are sought from patients.
Examples include feedback forms for specific interventions and focus groups.
• Participation: Patients influence the development of the service. Examples include the
Personality Disorder Service Steering Group, which includes NHS staff, patients and
other stakeholders.
• Inclusion: Patients are involved in the delivery of the service. Examples include the
Volunteer Post in the CAS Day Service and co-delivery of education sessions.
7

• Partnership: Patients are involved in sharing decisions and responsibility. Examples
include patients sitting on interview panels for staff and volunteer appointments to the
Personality Disorder Service.
2.3.2 Consistency
Consistency can be taken to mean adherence to the treatment frame. Consistency within care
and treatment is particularly important as many patients will have limited previous experience of
consistent relationships. Often personality disorder pathology can make consistency difficult and
there will frequently be attempts to change the treatment frame by the patient or clinician.
Supportive limit setting is a vital component of therapy but can occasionally be met by negative
responses from the patient which should also be highlighted and addressed immediately.
Similarly, strong emotional responses on the part of the clinician must be managed in order to
maintain consistency. These reactions can be useful in helping the clinician understand the
reactions of other people to the patient. However, a clinician’s emotional responses to the
patient should only be explicitly revealed to the patient after significant reflection on whether the
revelation is likely to be therapeutic or not. Often, it is more useful to support the patient to
reflect on their own behaviour and the behaviour of other people in the context of the thoughts
and emotions which might lie behind the behaviours.
It may be necessary for the clinician to seek supervision to accept, examine, understand and
contain especially strong emotional responses. Regular supervision and consultation, and
working to a clear formulation can help maintain consistency of approach for an individual
therapist. Good communication and collaborative inter-professional working can help maintain
consistency across teams.
2.3.2.1 Treatment frame
Appropriate treatment frame management for anyone treating people with personality disorder
is a key therapeutic skill. Treatment frame refers to the agreed structure and “ground rules”
which are sometimes called the “limits” or “boundaries” of any therapeutic intervention. These
include limits of:
• Time: Including the timing (time and day) of sessions, the length of sessions, the length
of the contract and frequency of sessions, and arrangements for cancellations, missed
sessions etc.
• Place: Including the location and setting of sessions. Sessions should be private and
without interruption.
• Administration: Including explicit management structure, confidentiality and its limits,
communication with other professionals, and supervision arrangements.
• Task of therapy: Including treatment targets informed by the phase-based model and
specific short and long term goals which have been collaboratively agreed upon.
• Roles: Including the roles, responsibilities and interpersonal boundaries of therapist and
patient and agreement on how treatment goals will be attained.
Key aspects of the frame such as those outlined above should be made explicit and agreed at
the start of treatment. Some aspects may remain implicit but may need to be made explicit
when necessary—for example, in a situation where a patient offers the therapist a gift.
Once treatment has begun, it is the therapist’s responsibility to maintain a secure treatment
8

frame. A secure frame is one which is firm but not rigid, and which marries clarity, consistency
and reliability with sensitivity of response to the patient’s needs. An insecure frame lacks
consistency, reliability and predictability and often leads to a deterioration of the patient’s
condition.
At times there may be pressure to modify a limit or boundary within treatment. It is important to
recognise when such a modification would help maintain the treatment frame and when the
modification would threaten the frame. Any threat to the frame should be openly discussed
within treatment with a view to repair. This includes acknowledgement of errors of frame
management on the therapist’s part or unavoidable interruptions to the frame. In these
situations, the aim should be re-establishment of a secure treatment frame at the earliest
opportunity.
However, on rare occasions, such severe pressure will be put on the treatment frame by some
patients that it may be necessary to terminate the treatment contract. This should be considered
when it is likely to represent a less harmful option compared with continuing treatment within an
insecure frame. It is important to remain aware that resisting pressure to inappropriately modify
the frame will not make the patient worse, whereas giving in to pressure to inappropriately
modify the frame will not be helpful to the patient.
2.3.2.2 Splitting
In situations where several professionals have contact with a patient, the treatment frame
should be clearly shared and agreed by all involved. This helps reduce the risk of “splitting”.
Patients with personality disorder frequently experience the world in a polarised way which is
sometimes described as experiencing the world “in black and white”. This can mean that one
team member is experienced as “all good”, while another is experienced as “all bad”. This can
affect the behaviour of the practitioners involved. For example, the team member experienced
as “all good” may be more likely to want to offer the patient an overly nurturing care plan at the
expense of the patient taking responsibility for their own safety and recovery, whereas the team
member experienced as “all bad” may begin to think that the patient is not being helped by the
team and should be discharged. Dynamics such as this can contribute to team conflict,
especially if there are pre-existing professional or personal differences, can lead to the creation
of insecure treatment frames which are harmful for patients, and can leave professionals feeling
unsupported and uncontained. This process is sometimes known as “splitting”.
Splitting can also occur between different teams involved with a patient’s care, leading to a
potentially destabilising inconsistency of approach. This form of splitting is especially likely if
conflicting theoretical and attitudinal positions are held by different teams, particularly in
situations where communication between teams is sub-optimal and the ability to consider
alternative perspectives is reduced.
Therefore, good communication between everyone involved, regular self-observation and
reflection, and a consistent treatment frame are necessary not only for the benefit of the patient,
but also for the benefit of the professionals and services involved. In particularly complex cases,
consideration should be given to use of the Care Programme Approach which helps ensure
regular meetings, good communication and the provision of a clear written care plan
(incorporating the treatment frame) for all involved, thus optimising consistency. Appropriate
supervision also has an important role to play in helping professionals recognise and manage
splitting processes.
9

2.3.2.3 Endings and transitions
Clinicians should recognise that withdrawal or ending of treatments, and transition from one
service to another, may evoke strong emotional responses in some patients. Such changes
should be highlighted and discussed as far ahead in time as possible and a crisis self-
management plan should be in place. Changes should be managed in a structured way which
is made explicit within the treatment frame. Collaboration between services and patients is
crucial at times of transition from one service to another to ensure as little inconsistency as
possible. When a patient is referred for assessment or treatment to another service,
consideration should be given as to whether support arrangements would be appropriate in the
interim.
2.3.3 Motivation
Up to 75% of people with personality disorder will be treatment-resisting, in other words they will
neither seek, nor wish to undertake treatment. Of the 25% who do seek treatment, levels of
motivation to change will vary from patient to patient and over time. Treatment is invariably
challenging and frequently requires intense sustained effort. For this reason, it is important to
build and maintain motivation for change. In fact, this is frequently the major focus of treatment
for people at the pre-contemplation, contemplation and preparation stages of change.
Strategies for increasing motivation include:
• Using discontent with the current situation to build motivation
• Instilling hope and an optimistic stance. This can involve education about the
disorder, effective treatments, and the relatively positive prognosis.
• Creating other alternatives. This often involves time spent teaching problem and
solution analysis.
• Identifying incentives for making changes and incentives for not making changes. This
often involves pros and cons of changing versus not changing.
• Managing ambivalence. This involves exploring the tension between fear of change
versus desire for change, highlighting and amplifying the discrepancy between current
and desired experience, encouraging consideration of the benefits of change, and
attending to the fear of change and associated concerns.
• Encouraging patience and persistence including highlighting that longstanding patterns
of experience and behaviour take a long time to change.
• Identifying internal and external obstacles to motivation and change.
In aiming to build and maintain motivation, professionals should avoid taking responsibility for
the patient or engaging in confrontational and coercive interventions. This is often difficult
because professionals frequently feel a sense of responsibility when progress is slow.
Occasionally, clinicians may find themselves pressuring the patient or giving advice. While this
may not be unwelcome for the patient, it undermines the necessary position of the patient
accepting responsibility for change. The only option open to the patient when professionals
adopt these overly-directive behaviours is to behave in a dependent manner.
Maintaining clinician motivation during what can often be slow, challenging work is also
important. A collaborative relationship with the patient, recognition that progress can sometimes
be slow but that significant recovery is possible, setting realistic treatment goals, maintaining
self-observation and reflection, and regular supervision all contribute to the maintenance of
10

therapist motivation.
2.3.4 Validation
Validation is a key strategy in the treatment of personality disorder and can be defined as
acknowledgement of the legitimacy of a person’s behaviour and experience. Invalidation is a
related concept, considered to be of significant importance in the development and maintenance
of personality disorder. Invalidation occurs when a person’s behaviour and internal experiences
are discounted or not regarded as legitimate. Invalidation occurs on a continuum, ranging from
having one’s opinion dismissed as “stupid” to severe neglect and physical or sexual abuse.
Invalidation, in transaction with an emotionally sensitive temperament, may play a particular role
in the development of borderline personality disorder.
The establishment of a validating treatment process strengthens the working relationship,
provides new and validating experiences to help counter previous invalidating experiences,
promotes self-validation and encourages the development of a more adaptive sense of self.
Validation can and should occur in almost every interaction with patients. However, it is
important to recognise that validation does not necessarily imply approval.
Validation involves active listening and observation, accurate reflection of the patient’s emotions,
thoughts and behaviours, and direct validation (the explicit acknowledgement of a thought,
emotion or behaviour as valid and legitimate for that person, both understandable in the current
context and in the context of previous experiences).
It is useful to help a patient distinguish between their experience, the reasons given for the
experience, the conclusions drawn from the experience, and the action based upon the
experience. While beliefs and emotions should be accepted and acknowledged, their origin and
implications should be questioned and explored.
It is important to recognise that unhelpful behaviours, for example self-harm or substancemisuse, may be the only way the person has had to cope with their experiences and that there isalways some validity to any behaviour in its own context.
Relentless self-invalidation is often present in people with personality disorder and usually
serves to maintain the disorder. Therefore, negative self-judgements should be identified and
highlighted and areas of competence should be recognised and acknowledged. This promotes
self-observation and reflection and can help to reduce self-invalidation over time.
Therapists should make every effort to avoid invalidating the patient. However, mistakes are
inevitable and therapists should openly acknowledge any errors they have made as soon as
possible. Minimising problems, prematurely focusing on the positive, providing inappropriate
reassurance, interpreting normal experiences as pathological and interpreting all problems as
stemming from personality disorder are frequently experienced as particularly invalidating by
patients. If a rupture does occur in the therapeutic relationship, it is important to identify this
quickly, to explore possible reasons, and to explore and validate the patient’s reaction to the
rupture.
11

2.3.4.1 Case example
Bill felt let down and angry when his friend did not telephone as promised. He decided
that his friend no longer liked him and that the only way that he could reduce his intense
anger was to cut himself, a behaviour which he had been trying to reduce.
In this situation, it was valid that Bill felt rejected and angry in light of his assumption that
his friend had rejected him (even though that assumption may have been incorrect). In
the past, people failing to telephone as arranged had signalled the rupture of friendships.
Bill’s judgement that only self-harm could reduce the intensity of his anger was also valid
(also probably incorrect), given that this had been the only strategy that had worked to
reduce his anger in the past. The act of self-harm was valid as the only solution Bill could
see to change an intolerable emotional state.
The therapist, after actively listening to Bill explain the situation, reflected her un-
derstanding of the situation and Bill’s associated emotions, thoughts and behaviours
back to him and checked out that she had understood correctly without missing any
important information. She then directly validated Bill’s experience while helping him
explore and question the antecedents and consequences:
Therapist: So, Bill, if I have understood you correctly, your friend didn’t phone you as
agreed, and you took this to mean that he no longer liked you. You felt let down and
angry and cut yourself to reduce your anger to a tolerable level. You then thought you
were a failure and felt ashamed. Is that about right? [accurate reflection following active
listening]
Bill: Yes, that’s about right.
Therapist: I can see why you felt angry and let down, anyone would if they thought their
friend had snubbed them and didn’t like them any more [direct validation]. . . but how did
you know for sure that your friend had deliberately let you down [exploring antecedent]?
Bill: Well, he didn’t phone, what else could it mean?
Therapist: What other alternative explanations might there be? [exploring antecedent]
Bill: I don’t know. . . well, I suppose he may have run out of credit or lost his phone.
Therapist: Possibly—I suppose we don’t know for sure until we have more information,
but I remember you said that a lot of people have let you down in the past, so I can see
why you made that judgement [direct validation; distinguishing judgement from fact]. I
can also see why you cut yourself—your anger was intolerable and you needed to do
whatever it took to feel differently, cutting yourself was the only thing you knew had
worked in the past [direct validation].
Bill: Yes, I had no other option.
Therapist: I recognise that’s how it seemed for you at the time, and I get that something
had to be done [direct validation] but you’ve identified before that cutting yourself causes
you to feel very ashamed and you’re left with a scar. Do you think it may have been
worth trying out any of the emotion regulation skills you have learned over the past few
weeks first? [exploring alternatives]
12
2.3.5 Self-management
Promoting and supporting self-management represents the overall aim of the treatment of
personality disorder. Self-management is such a broad topic that it has been given its own
section in this ICP. Please see the Self-management Section for further details.
2.4 Stages of Change Model (Trans-theoretical Model of Intentional
Change)
The Stages of Change Model or Trans-theoretical Model of Intentional Change (TTM)
(Prochaska, 2010) has been applied to many different patient groups with various health
conditions, and describes how people modify unhelpful behaviours, or increase or acquire
helpful behaviours.
Essentially the TTM is conceptualised as comprising 5 stages (see Figure 2.1) which are
progressed through sequentially (or sometimes as a cycle). Occasionally, there may
be a return from a particular stage to an earlier stage but population studies show that in
personality disorder sustained recovery is more likely than relapse. A relapse can be defined as
return from the Action or Maintenance stage to an earlier stage. This may occur due to
significant ongoing stressors or because subsequent and necessary phases of treatment have
not been undertaken at an approapriate time. For example, if trauma work is not made available
to an individual with post-traumatic features in a reasonable time after stabilisation, a recurrence
of previous unhelpful behaviours often occurs. This is usually as an ineffective attempt to deal
with overwhelming post traumatic symptoms.
• Pre-contemplation (Not ready)
People at this stage are not intending to take action in the next six months and are often
unaware of the unhelpful nature of their behaviour. Sometimes people at this stage may
have tried to change a number of times with limited success and may feel demoralised
and discouraged from trying again.
• Contemplation (Getting ready)
People are starting to recognise that their behaviour is unhelpful and begin to look more
closely at the pros and cons of their continued actions. They are usually increasingly
aware of the possible benefits of changing but remain significantly influenced by the
benefits of the current behaviour and apprehensive about change. This balance between
the pros and cons of changing can lead to people remaining at this stage for long periods
of time.
• Preparation (Ready)
People are intending to take action in the next month or so and may begin to make
small steps towards behaviour change.
• Action
People have made specific overt modifications in reducing unhelpful behaviour and/or
acquiring or increasing helpful behaviour.
• Maintenance People have maintained action for some time and are working to prevent
a return to previous behavioural patterns. In this stage, change strategies are not
employed as often as in the Action stage and people are typically increasingly confident
13

that they can maintain change.
The TTM can be applied to each phase of treatment within the overall treatment pathway. For
example, an individual may be in the maintenance phase with regard to stabilisation (phase 1)
but in the contemplation or preparation stage with regard to trauma work (phase 2). In such a
case, the TTM could help identify that the focus of the treatment should be on maintaining
stabilisation and increasing motivation for trauma work.
Motivational interventions to increase intention to change can be especially useful in the pre-
contemplation, contemplation and preparation stages by assisting patients to reach the stage
where meaningful behavioural change can occur. Examples of motivational interventions are
described under Motivation in the General Treatment Strategies section.
Figure 2.1: Stages of change model
2.5 Phases of Treatment
The overall goal in the treatment of personality disorder is to improve adaptation to the
environment rather than effect personality change. However, given the complexity of personality
disorder, at times it can be difficult to develop a specific treatment plan in the service of this
goal, and a structured approach can be of real value. There is expert consensus that phase-
based models are important in informing the sequence of interventions in the care and
treatment of complex mental disorders such as personality disorder.
The particular model used in this document adapts the work of Livesley (2003) and, like most
other phase-based models, comprises 3 main phases. However, Phase 1 (stabilisation) is
broken down into a further 3 sub-phases. This finer-grained model is more clinically useful. For
example, it can help explain why lengthy hospital admission usually fails to produce
stabilisation: while hospital admission has value in the safety phase and to some degree the
14
containment phase, it seldom has a positive effect (and often exerts a negative effect) on
promoting self-regulation and control. This is related to the removal of responsibility for self-
management from the patient.
Any treatment for personality disorder should be based upon an individual formulation with
clarity about the goals and purpose of the intervention for the person at that time. Each phase
should be worked through sequentially. The phases of treatment comprise:
1. Stabilisation (or MAKING STABLE). The focus is on the present:
a) Safety: Interventions to ensure the safety of the patient and others.
b) Containment: Interventions based primarily on general treatment strategies suchas validation and stabilising the environment in order to contain behavioural andaffective instability. May be supplemented with medication if appropriate in theshort term.
c) Regulation and control: Behavioural, cognitive and occasionally pharmacologi-cal interventions to reduce symptoms and improve self-regulation of affects andimpulses
2. Exploration and change (or MAKING SENSE). The focus is on the past:
Interventions to change the cognitive, affective, interpersonal and situational factors
contributing to the patient’s difficulties. This phase may include specific trauma work but
may be a more general exploration of long standing patterns of thinking and behaviour.
3. Integration and synthesis (or MAKING CONNECTIONS). The focus is on the
future: Interventions designed to promote a more integrated sense of self along with
more integrated and adaptive interpersonal systems
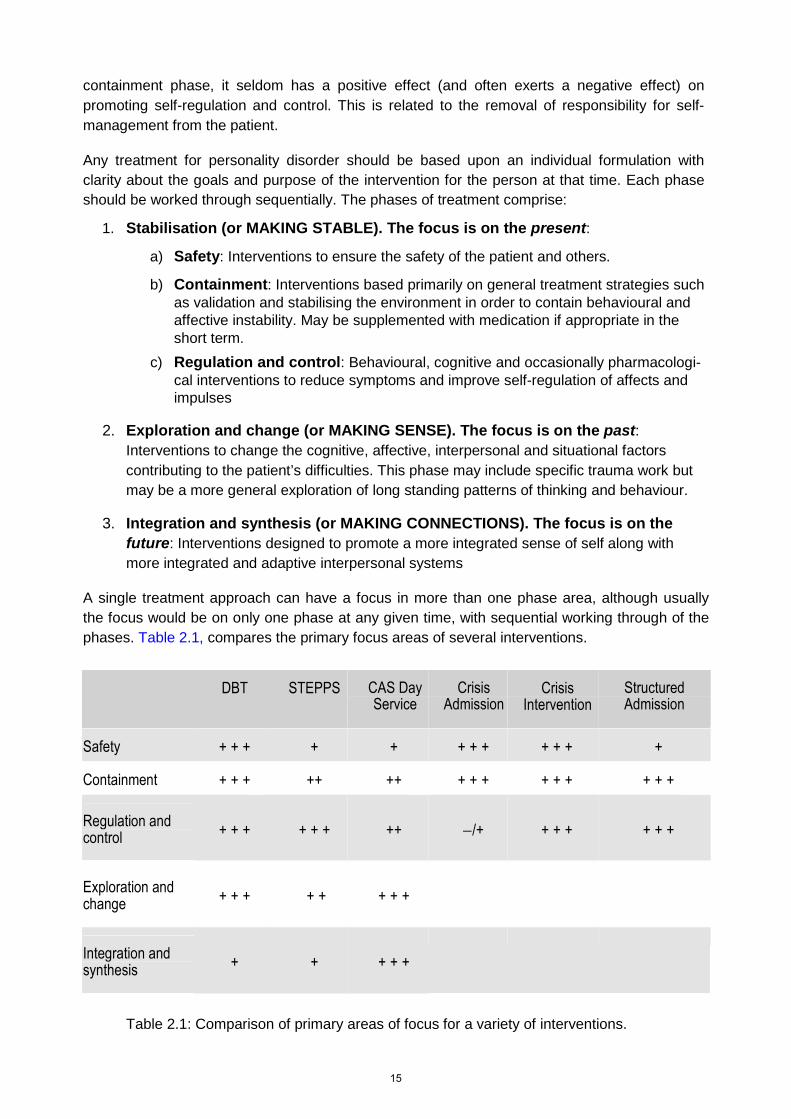
A single treatment approach can have a focus in more than one phase area, although usually
the focus would be on only one phase at any given time, with sequential working through of the
phases. Table 2.1, compares the primary focus areas of several interventions.
DBT STEPPS CAS DayService
CrisisAdmission
CrisisIntervention
StructuredAdmission
Safety + + + + + + + + + + + +
Containment + + + ++ ++ + + + + + + + + +
Regulation andcontrol + + + + + + ++ −/+ + + + + + +
Exploration andchange + + + + + + + +
Integration andsynthesis + + + + +
Table 2.1: Comparison of primary areas of focus for a variety of interventions.
15

2.5.1 Phase 1
People with personality disorder often present to services with emotional and behavioural
dysregulation, requiring stabilisation interventions. These can be effectively provided across
many settings and may range from supporting the problem-solving of a distressing interpersonal
situation, to treatment of an Axis 1 or physical comorbidity, to a specialist psychological therapy
targeting parasuicidal behaviour. Stabilisation may require support from several different
services or agencies. An overall formulation with clarity about the phase of treatment and
including explicit short and longer term goals is valuable in optimising consistency and may
mean the difference between repeated management of symptoms and treatment of the
underlying disorder.
2.5.1.1 Case example
Jane, a 25 year old lady with severe borderline personality disorder, presented with
multiple difficulties including poorly managed diabetes mellitus, alcohol dependence,
housing difficulties, marked emotional dysregulation, self-harming behaviours and
multiple suicide attempts. Stabilisation involved input from her psychiatrist who made the
diagnosis and stopped the antidepressant tablet which appeared to be contributing to
increased emotional dysregulation, her GP who helped her stabilise her diabetes, the
Addictions Service which helped her stabilise her alcohol dependence, the Housing
Officer who helped her to find appropriate accommodation, the DBT therapist who
provided specific psychological therapy with a beneficial effect on parasuicidal
behaviours, and her CPN who monitored her overall mental health, helped maintain
motivation and consistency, and co-ordinated the overall treatment plan under the Care
Program Approach.
2.5.2 Phases 2 and 3
Historically, less attention has been paid to the second and third phase within mainstream
mental health services, which remain more involved with stabilisation than any other phase of
treatment. However, it is often the case that patients are unlikely to progress in their recovery
once stabilisation occurs if the later phases are not addressed in some manner. Failing to
address Phases 2 and 3 can result in relapse and a return to previous unhelpful behaviours,
repeated presentations and a sense of frustration and helplessness in patients and
professionals.
For the most part, each of the three phases should be worked through in order, but it is
important to note that the phases of treatment may overlap slightly and that some interventions
will allow for work in more than one phase of treatment. For example, although standard DBT is
primarily focused on stabilisation, the emphasis can shift to exploration and change (and even
integration and synthesis) once stabilisation occurs. While some patients will require the input of
services during all phases of treatment, many will not. For example, someone who has been
supported to stabilise by services may then be able to meet the goals of Phase 2 and 3
themselves, or with minimal support.
Attaining stabilisation enables some patients to reflect on longstanding patterns of behaviour and
16

thinking and the skills they have acquired during Phase 1 allow them to make effective changes
to these patterns (exploration/change). They may not require specific input from services to
complete this Phase 2 work. These changes, as time goes on, may allow for involvement in new
opportunities, such as new employment, recreational activities and friendships, leading to a
more integrated sense of self within a new, healthier interpersonal context. Others may not
require support with Phase 2, but may benefit from Phase 3 input. Occasionally, people may
present without requiring specific stabilisation work, but would benefit from work targeted at
Phase 2 or Phase 3. The chances of meaningful recovery are increased when the tasks of all
the phases are addressed.
2.5.2.1 Case example
Bob was helped to stabilise by the input of his CPN and the STEPPS program. He did
not require any specific trauma work and, from his new position of emotional and
behavioural stability, he felt confident in being discharged from services. He was then
able to work through Phase 2 himself, exploring and making changes to long-standing
patterns of thinking and behaviour using the skills of self-observation and reflection which
he had learned in Phase 1 of treatment. He started some new recreational activities
locally and eventually he decided to re-enter the work-place. He obtained a part-time job
which, together with the recreational activities he was involved with, helped him achieve
many of the objectives of Phase 3 work including the development of new roles,
responsibilities, activities and relationships, all of which contributed to a more integrated
sense of self and a firmer sense of his place within his community.
2.5.3 Timing and sequencing
There is general agreement that patients should receive the right input at the right time and that
the different phases of treatment should be as joined-up as possible, although input for each
phase may be provided by different services. For example, the available evidence appears to
indicate that after a period of 2 months of stability, specific trauma work can usefully be started.
Experience suggests that waiting for longer does not provide any particular clinical benefit and a
hard-won window of opportunity may be lost. It is therefore of particular importance to strive for
a joined-up approach to working through the phases of treatment in a patient-centred way.
It is important to note that psychological interventions are not inert and have the potential to
cause harm. For example, undertaking emotionally intense trauma work in an individual who has
not been supported to appropriately stabilise first and has not learnt skills of self-regulation and
control has the potential to cause harm. The patient is likely to become emotionally dysregulated
and use unhelpful and potentially dangerous behaviours in an attempt to re-regulate. Use of the
phase-based model can reduce the potential for a psychological intervention to cause harm.
Movement through phases of treatment is not always one way. Occasionally, people will have a
recurrence of emotional and behavioural dysregulation after a period of stability. In cases like
this, the focus of treatment should return to the stabilisation phase. Almost invariably, the time
required to re-stabilise is shorter than the time taken for the initial stabilization work and usually
requires a focus on increasing motivation to use pre-existing skills or a brief revision of skills
rather than a fresh re-learning of skills.
2.6 Matched Care
17

The concept of matched (or stepped) care is based on the understanding that for most health
conditions, there will be a larger number of people with less severe forms of the disorder, with
numbers of those affected by the disorder becoming progressively smaller as severity increases.
Treatment is organised in tiers to best match intensity of service with complexity and severity of
need. This has benefits for patients and services but does require appropriate assessment and
signposting of patients to the most appropriate intervention for them at that time. For example,
STEPPS is the most appropriate stabilisation intervention for moderate severity borderline
personality difficulties but DBT is more appropriate for treating patients with more severe forms
of the disorder, given its more intensive approach.
The concept of matched care is sometimes represented as a pyramid, as in Figure 2.2.
Figure 2.2: Tiers of service provision for people with personality disorder.
In NHS Highland, services fall within the first 3 tiers of this model. Primary care, social care, third
sector and specialist outreach from the PDS (primarily in terms of education/awareness
interventions) comprise the first tier. Tier 2 includes inpatient and community mental health
services (including STEPPS), and PDS outreach interventions to these services. These outreach
interventions include education/awareness, and consultation/liaison interventions. The PDS
represents the third tier of service in NHS Highland incorporating DBT and the CAS Day Service.
Table 2.2 shows some examples of interventions for each phase of treatment available withinthe different tiers of service provision. This table is illustrative only and is by no meansexhaustive.
18

Table 2.2 Examples of available interventions by phase of treatment within each tier of serviceprovision.
Phase1(stabilisation)
Phase 2(exploration andchange)
Phase 3(integration andsynthesis)
Tier 1 (Primary care,social care, thirdsector)
Primary care:treatment of co-morbid physicalillness
Housing: assistancewith appropriateaccommodation
All agencies: modelnon- specific worksupporting self-reflection andidentification andchange of unhelpfulpatterns of behaviour
Employmentservices:Employability Officersupport
Tier 2 (Mainstreammental health)
Addictions services:treatment ofsubstancedependence
CMHT: STEPPS,treatment of co-occurring mentalillness
CMHT: STEPPS
Psychologydepartment: traumawork
CMHT: Occupationaltherapy support toengage inmainstreamcommunity activities,
Vocational SupportTeam
Tier 3 (Localspecialist services)
PDS: DBT PDS: DBT, DBT-PE PDS: CAS DayService
19
References
Bateman, A., & Krawitz, R. (2013). Borderline Personality Disorder—An evidence-based
guide for mental health professionals. Oxford.
Davidson, K. (2008). Cognitive Therapy for Personality Disorders. Routledge.
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder.
Guilford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Prochaska, J. O., & Norcross, J. C. (2010). Systems of psychotherapy: a trans-theoretical
analysis. Brooks & Cole.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley.
SRN. (2014). Scottish Recovery Network. http://www.scottishrecovery.net
20

3. Assessment, diagnosis and formulation
3.1 Assessment
3.1.1 Introduction
Personality disorder and personality-related conditions are by their very nature complex. Their
inherent complexity means that these conditions often require relatively more time to assess
than many other disorders. Three to four sessions to assess and formulate is not untypical.
Accurate diagnosis, formulation and treatment planning maximises the chance of recovery from
these chronic conditions, which are associated with so much distress, poor functioning and
resource uptake.
Personality disorder should no longer be viewed as a diagnosis of exclusion. In other words, it
should be considered as a diagnostic possibility from an early point in the assessment process,
rather than only receiving consideration later in the process when other diagnoses have been
excluded. Early consideration of the diagnosis helps to avoid situations where patients receive
inappropriate, unnecessary and sometimes harmful treatments.
While undoubtedly essential, diagnosis should constitute only one part of a broader formulation
of an individual’s situation, their condition and their needs. In general terms, it is more important
to identify the presence of personality disorder and to assess its severity than to subtype into
specific personality categories. Personality disorder presents with certain symptoms which are
predicated upon the interaction of an individuals personality traits and their environment. It is
important to assess both symptoms and traits.
3.1.2 Symptoms
Symptoms occur as a result of maladaptation of the personality to the environment. It is helpful
to think in terms of four broad headings:
• cognitive-perceptual (for example, excessive suspiciousness)
• affective (for example, emotional instability and anger difficulties)
• interpersonal
relationship with self/sense of self
interpersonal relationships
relationship with society
• behavioural/impulse control (including self-harm and suicidal behaviour)
3.1.3 Personality Traits
A personality trait (or variable) is a complex structure which represents the basic building block
of personality. In a given individual, genetic and environmental factors transact to form a
complex biopsychological system which produces observable trait-based behaviour.
Essentially, a personality trait represents a disposition to behave in a particular way. The term is
also sometimes used to refer to individual features of specific personality disorder, especially
when the full diagnostic criteria are not met. For example, someone meeting four of the five
criteria needed for a diagnosis of borderline personality disorder may be referred to as having
“borderline traits”.
21

Some traits which are of particular importance in personality disorder are listed below with brief
descriptions of associated behaviours. Traits can be usefully organised into four main higher
order trait domains: (emotionally) dysregulated, detached, dissocial, and compulsive. There may
be overlap between some traits and it is worth noting that some of the names used for particular
traits may have different meanings when used in other contexts. The traits below are drawn from
the Personality Assessment Schedule (Tyrer, 2000). Other sources may label particular traits
differently.
It is important to remember that no personality trait is inherently negative. Many traits can be
described by more than one term, some with negative connotations and some with positive
connotations. For example: impulsive versus spontaneous; stubborn versus determined; aloof
versus self-contained and so on. Problems arise when a person’s personality traits are
maladapted to their environment. With more extreme expressions of particular traits,
maladaption is likely in a greater number of environments leading to greater severity of
personality disturbance.
Dysregulated (Internalising) Domain
Pessimism — holds a pessimistic outlook on life.
Worthlessness — feelings of inferiority
Lability — mood instability
Anxiousness — anxiety-proneness
Shyness — shyness and lack of self-confidence
Sensitivity — personal sensitivity and tendency to self-reference
Vulnerability — experiences excessive emotional distress when faced with adversity
Childishness — excessive self-centeredness
Resourcelessness — tendency to give up when faced with adversity
Dependence — excessive reliance on others for advice and reassurance
Submissiveness — limited ability to express own views or stand up for
oneself
Hypochondriasis — over-concern about illness and health
Detached (Schizoid/inhibited) Domain
Suspiciousness — excessive mistrust of others
Introspection — prone to rumination and fantasy
Aloofness — detachment and lack of interest in other people
Eccentricity — oddness in behaviour and attitudes; unwilling or unable to
conform
Dissocial (Externalising) Domain
Optimism — unrealistically optimistic, over-confident, excessively self-important
Irritability — excessively irritable
Impulsiveness — excessive impulsiveness
Aggression — excessive levels of (physical) aggression
Callousness — indifferent to the feelings of others
Irresponsibility — indifferent to the consequences of one’s behaviour
22

Compulsive (Anankastic) Domain
Conscientiousness — overly fussy, perfectionistic
Rigidity — inflexibility and difficulty adjusting to new situations
3.1.4 Areas of Assessment
Assessment for specific interventions may vary in emphasis but will generally cover the areas in
the general assessment below. While it is recognised that a comprehensive assessment
including all the components listed below may not be possible in every case, a detailed general
assessment of personality disorder will typically include information gathered from four main
sources: psychiatric history and mental state examination; collateral information; formal
structured assessment tools; and clinician observations.
• Detailed psychiatric history and mental state examination including:
Important developmental and interpersonal factors such as:
o Family and parental relationships including attachment patterns
o Reactions to key developmental events and transitions
o Losses, separations, relocations and responses to such events
o Preliminary assessment of history trauma and neglect. Full exploration at
assessment stage can be dysregulating and counterproductive if the patient
does not have adequate self-regulatory skills. However, the patient should be
made aware that traumatic events can be returned to in due course. An
instrument such as the Trauma History Screen (Carlson, 2005) may be
useful in gaining a trauma history.
o Peer and romantic relationships
o Important memories
Co-occurring disorders:
o Axis 1
• Post-traumatic conditions
Reliving experiences Constriction/avoidance Hyperarousal
• Substance use
• Other mental illness
o Physical health conditions
Risk assessment: consider using a structured tool such as STORM
Personal strengths and attributes
Motivation to change
Symptoms: current difficulties or disturbance in the following domains:
o Cognitive/perceptual
o Affective
23

o Interpersonal
• Relationship with self/sense of self• Interpersonal relationships• Relationship with society
o Behavioural/impulse control
Traits: traits underlie the symptoms and can be grouped into 4 domains:
o Dysregulated (internalizing)
o Dissocial (externalizing)
o Detached (schizoid)
o Compulsive (anankastic)
• Collateral information:
Healthcare records
Informant information from (as appropriate):
o Familyo Friends and acquaintanceso Professionals
• Clinician observations:
Of interactions with others
Within clinical encounters
• Formal structured assessment tools to be used where appropriate include :
CORE-Outcome Measure (CORE-OM): self-reported general measure of well-being,
problems, risk and functioning. This comes in CORE-34 (34 item) and CORE-10 (10
item) forms. (CORE, 1998)
Global Assessment of Functioning (GAF): clinician-completed global assessment of
functioning on 0-100 scale. This represents axis 5 of DSM-IV (DSM-IV, 1994).
Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): clinician
completed semi-structured interview for borderline personality disorder based on the 9
DSM-IV criteria (Zanarini, 2003).
Borderline Estimate of Severity over Time (BEST): self-reported measure of bor-
derline personality disorder used in STEPPS. This measure is reasonably sensitive to
change as it includes items relating to adoption of more adaptive behaviours. (Pfohl and
Blum, 1997).
WHOQOL-BREF: self-report quality of life measure (WHO, 2004).
Filter Questionnaire: self-report tool for presence of unhelpful core beliefs typically
associated with borderline personality disorder (from STEPPS, Blum et al., 2008).
Personality Belief Questionnaire (PBQ): self-report tool for presence of unhelpful core
beliefs associated with a broad range of personality disturbance (Beck, 2001)
Process of Recovery Questionnaire (PRQ): Self-report measure of recovery (Neil et
al., 2007)
Standardised Assessment of Personality Abbreviated Scale (SAPAS): short self-
report screening tool for presence of personality disorder (Moran, 2003).
Trauma History Screen (THS): self-report instrument assessing nature and severity of
historical traumatic events. (Carlson, 2005).
Personality Assessment Schedule (PAS): clinician-completed semi-structured
interview of personality pathology from a trait perspective. (Tyrer, 1988).
Clinical Global Impression (CGI): locally adapted clinician-completed tool with self-
24

report counterpart measuring clinical baseline and global change.
Some of these tools can be found in the Appendix. No tool used alone is adequate to
diagnose personality disorder and the information gathered should be placed in the
context of an overall assessment. Many of these tools can be repeated during and after
treatment to measure progress and outcomes.
3.2 Diagnosis
The current major diagnostic systems are the International Classification of Diseases, Tenth
Edition or ICD-10 (World Health Organisation, 1993), and the Diagnostic and Statistical Manual-
5 or DSM-5 (American Psychiatric Association, 2014). Both have a set of general criteria for
diagnosis of personality disorder and sets of criteria for a number of specific personality
disorders. There are slight differences in the categorisation of the two diagnostic systems but
they are currently broadly similar. ICD-11 (due in 2017) is likely to fundamentally change the
diagnostic process, switching to a simpler dimensional system, with greater scientific validity and
clinical utility. However, until this happens, it is recommended that the current ICD-10 diagnoses
are used. The exception is that DSM criteria should be used for the diagnosis of borderline
personality disorder. This is because there the evidence base relating to treatments for
Borderline Personality Disorder is based upon DSM-IV criteria rather than the ICD-10 equivalent
diagnosis, Emotionally Unstable Personality Disorder.
In clinical practice, co-occurrence of several different specific personality disorders in the same
individual is common. For example, only one in ten patients meeting criteria for borderline
personality disorder only meet criteria for that specific personality disorder. In cases where the
full criteria for more than one specific personality disorder are met, the diagnosis of F60.9
Personality disorder, unspecified should be made, with the prominent components specified.
For example: F60.9 Personality disorder, unspecified (moderate, with borderline,
dependent and anankastic components). It is useful, whatever the diagnosis, to indicate the
severity as mild, moderate or severe. ICD-11 is likely to use “mild” to describe personality
disorder with disturbance in only one higher trait domain, “moderate” for those with disturbance
in two or more higher trait domains, and “severe” is likely to be defined as those with disturbance
in two or more higher trait domains along with significant risk to themselves or others.
The diagnosis F61.0. Mixed Personality Disorder should be reserved for situations where the
general criteria for personality disorder are met, but the full criteria are not met for any specific
personality disorder category, although features from more than one specific category are
present.
This phenomenon of co-occurrence underlines some of the shortcomings of the current
classification systems. The DSM system has attempted to address the issue of co-occurrence of
specific personality disorders by describing 3 clusters of personality disorders which are said to
co-occur most frequently. While having some clinical usefulness, there is no robust empirical
basis to these clusters:
• Cluster A Odd/eccentric: schizoid, paranoid and schizotypal personality disorders
• Cluster B Dramatic: borderline (emotionally unstable), narcissistic, histrionic and
antisocial personality disorders
• Cluster C Anxious/avoidant: obsessive-compulsive (anakastic), avoidant (anxious) and
dependent personality disorders
It is worth noting that for patients under the age of eighteen, clinicians are cautioned against
making a diagnosis of personality disorder. However, undoubtedly patients under the age of
eighteen do present with personality-related conditions. In such situations terms such as
25

“emergent personality disorder” or “evolving personality disorder” are sometimes used. If the
clinician is unclear whether personality disorder is present or not, a presentation can still be
referred to as a “personality-related condition”, or particular traits can be described. The primary
aim in being clear about the role of personality versus major mental illness in such situations is
to avoid inappropriate, unnecessary and sometimes harmful treatments and to enable
appropriate early intervention.
3.2.1 ICD-10
3.2.2 F60 Personality Disorder ICD-10 (DCR-10) Criteria
3.2.2.1 General Criteria for Personality Disorder
G1. There is evidence that the individual’s characteristic and enduring patterns of inner
experience and behaviour as a whole deviate markedly from the culturally expected and
accepted range. Such deviations must be manifest in more than one of the following
areas:
1) cognition (i.e. ways of perceiving and interpreting things, people and events, forming
attitudes and images of self and others)
2) affectivity (range, intensity and appropriateness of emotional arousal and response)
3) control over impulses and gratification of needs
4) manner of relating to others and of handling interpersonal situations
G2. The deviation must manifest itself pervasively as behaviour that is inflexible, maladaptive, or
otherwise dysfunctional across a broad range of personal and social situations
G3. There is personal distress, or adverse impact on the social environment, or both
G4. There must be evidence that the deviation is stable and of long duration, having its onset in
late childhood or adolescence
G5. The deviation cannot be explained as a manifestation or consequence of other adult
mental disorders
G6. Organic brain disease, injury, or dysfunction must be excluded as the possible cause of
the deviation.
3.2.3 F60.0 Paranoid Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be present:
1) Excessive sensitivity to setbacks and rebuffs;
2) Tendency to bear grudges persistently, e.g. refusal to forgive insults, injuries, or
slights;
3) Suspiciousness and a pervasive tendency to distort experience by misconstruing the
neutral or friendly actions of others as hostile or contemptuous;
4) A combative and tenacious sense of personal rights out of keeping with the actual
situation;
5) Recurrent suspicions, without justification, regarding sexual fidelity of spouse or
sexual partner;
6) Persistent self-referential attitude, associated particularly with excessive self impor-
26

tance;
7) Preoccupation with unsubstantiated ‘conspiratorial’ explanations of events either
immediate to the patient or in the world at large.
3.2.4 F60.1 Schizoid Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be present:
1) Few, if any, activities provide pleasure;
2) Display of emotional coldness, detachment or flattened affectivity;
3) Limited capacity to express either warm, tender feelings, or anger towards others;
4) An appearance of indifference to either praise or criticism;
5) Little interest in having sexual experiences with another person;
6) Consistent choice of solitary activities;
7) Excessive preoccupation with fantasy and introspection;
8) No desire for, or possession of, any close friends or confiding relationships (or only
one);
9) Marked insensitivity to prevailing social norms and conventions, disregard for such
norms and conventions is unintentional
3.2.5 F60.2 Dissocial Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least three of the following must be present:
1) Callous unconcern for the feelings of others;
2) Gross and persistent attitude of irresponsibility and disregard for social norms, rules
and obligations
3) Incapacity to maintain enduring relationships, though with no difficulty in establishing
them;
4) Very low tolerance to frustration and a low threshold for discharge of aggression,
including violence;
5) Incapacity to experience guilt, or to profit from adverse experience, particularly
punishment;
6) Marked proneness to blame others, or to offer plausible rationalizations for the
behaviour that has brought the individual into conflict with society.
3.2.6 F60.30 Emotionally Unstable Personality Disorder, Impulsive Type
A. The general criteria for personality disorder (F60) must be met.
B. At least three of the following must be present, one if which must be (2):
1) Marked tendency to act unexpectedly and without consideration of theconsequences
2) Marked tendency to quarrelsome behaviour and to conflicts with others, especially
when impulsive acts are thwarted or criticized;
27

3) Liability to outbursts of anger or violence, with inability to control the resulting
behavioural explosions;
4) Difficulty in maintaining any course of action that offers no immediate reward;
5) Unstable and capricious mood.
3.2.7 F60.31 Emotionally Unstable Personality Disorder, Borderline Type
A. The general criteria for personality disorder (F60) must be met.
B. At least three of the symptoms mentioned in criteria B for F60.30 must be present, with at
least two of the following in addition:
1) Disturbances in an uncertainty about self-image, aims and internal preferences
(including sexual);
2) Liability to become involved in intense and unstable relationships, often leading to
emotional crisis;
3) Excessive efforts to avoid abandonment;
4) Recurrent threats or acts of self-harm;
5) Chronic feelings of emptiness.
3.2.8 F60.4 Histrionic Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be present:
1) Self-dramatization, theatricality or exaggerated expression of emotions
2) Suggestibility (the individual is easily influenced by others or by circumstances);
3) Shallow and labile affectivity;
4) Continual seeking for excitement and activities in which the individual is the centre of
attention;
5) Inappropriate seductiveness in appearance or behaviour;
6) Over-concern with physical attractiveness.
3.2.9 F60.5 Anankastic Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be met:
1) Feelings of excessive doubt and caution
2) Preoccupation with details, rules, lists, order, organisation, or schedule;
3) Perfectionism that interferes with task completion
4) Excessive conscientiousness and scrupulousness;
5) Undue preoccupation with productivity to the exclusion of pleasure and interpersonal
relationships;
6) Excessive pedantry and adherence to social conventions;
7) Rigidity and stubbornness;
28

8) Unreasonable insistence by the individual that others submit to exactly his or her
way of doing things, or unreasonable reluctance to allow others to do things.
3.2.10 F60.6 Anxious (Avoidant) Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be present:
1) Persistent and pervasive feelings of tension and apprehension;
2) Belief that one is socially inept, personally unappealing or inferior to others;
3) Excessive pre-occupation with being criticised or rejected in social situations;
4) Unwillingness to become involved with people unless certain of being liked;
5) Restrictions in lifestyle because of need for physical security;
6) Avoidance of social or occupational activities that involve significant interpersonal
contact, because of fear of criticism, disapproval or rejection.
3.2.11 F60.7 Dependent Personality Disorder
A. The general criteria for personality disorder (F60) must be met.
B. At least four of the following must be present:
1) Encouraging or allowing others to make the most of one’s important life decisions;
2) Subordination of one’s own needs to those of others on whom one is dependent,
and undue compliance with their wishes;
3) Unwillingness to make even reasonable demands on the people one depends on;
4) Feeling uncomfortable or helpless when alone, because of exaggerated fears of
inability to care for oneself;
5) Preoccupation with fears of being left to care for oneself;
6) Limited capacity to take everyday decisions without an excessive amount of advice
and reassurance from others.
3.2.12 F60.9 Personality Disorder, unspecified
3.2.13 F61.0 Mixed Personality Disorders
With features of several of the disorders in F60.x but without a predominant set of
symptoms that would allow a more specific diagnosis.
3.2.14 DSM-IV
For borderline personality disorder, DSM-IV criteria should be used in preference to the ICD-10
criteria for emotionally unstable personality disorder for the reasons outlined above.
3.2.15 DSM-IV specific criteria for Borderline Personality Disorder
A pervasive pattern of instability of interpersonal relationships, self-image, and affects, and
marked impulsivity beginning by early adulthood and present in a variety of contexts, as
indicated by five (or more) of the following:
1) Frantic efforts to avoid real or imagined abandonment (do not include suicidal or self-
29

mutilating behaviour covered in Criterion 5);
2) A pattern of unstable and intense interpersonal relationships characterized by alternating
between extremes of idealization and devaluation;
3) Identity disturbance: markedly and persistently unstable self-image or sense of self;
4) Impulsivity in at least two areas that are potentially self-damaging (e.g., spending, sex,
substance abuse, reckless driving, binge eating), (do not include suicidal or self-mutilating
behaviour covered in Criterion 5);;
5) Recurrent suicidal behaviour, gestures, or threats, or self-mutilating behaviour;
6) Affective instability due to a marked reactivity of mood (e.g., intense episodic dysphoria,
irritability, or anxiety usually lasting a few hours and only rarely more than a few days);
7) Chronic feelings of emptiness;
8) Inappropriate, intense anger or difficulty controlling anger (e.g., frequent displays of
temper, constant anger, recurrent physical fights);
9) Transient, stress-related paranoid ideation or severe dissociative symptoms;
3.3 Formulation
The main purpose of assessment is to allow the collaborative development of a formulation of
the different biological, psychological and social factors into a description of the patient’s life and
personality which helps explain current problems and symptoms and identifies which problems,
themes and goals will be the focus of treatment.
The style and emphasis of formulation will vary according to the specific purpose or intervention
but relevant information for the formulation includes:
• Diagnostic formulation, with ICD-10 “F-codes” where applicable. This should include the
primary diagnosis and any co-occurring diagnoses.
• Clinical formulation including:
Symptoms:
o Cognitive/perceptual
o Affective
o Interpersonal
• Relationship with self/sense of self• Interpersonal relationships• Relationship with society
o Behavioural/impulse control
Important personality traits
Personal strengths
Over- and under-developed behaviours
Relevant core beliefs
Relevant developmental events such as childhood trauma
• Treatment plan:
Interventions and approaches by phase of recovery (including self-management
approaches)
30

Short term and long term goals
Risk management plans; crisis plans
A useful method of formulation involves developing an understanding of the following five areas:
• Problems: shared view of the main difficulties with the patient wishes help
• Predisposing factors: factors from earlier life which increase vulnerability in adult life
• Precipitating factors: factors currently or recently present in the patients life which canor have contributed to triggering the problems
• Perpetuating factors: factors which contribute to maintaining the problems
• Protective factors: factors which contribute to resilience and the ability to cope withadversity.
It can be useful to think of predisposing, precipitating, perpetuating and protective factors in
terms of biological, psychological and social components.
While predisposing factors are usually historical and not amenable to change, change may be
effected by reducing exposure to (or challenging) precipitating or perpetuating factors. There is
also likely to be value in strengthening protective factors.
The draft formulation should be shared with the patient in verbal, written or diagrammatic form
as appropriate. The patient should be asked for their views on the formulation and changes
made appropriately. The aim is to develop a shared understanding of the difficulties and a
commitment to the treatment plan — a formulation which the patient does not recognise or agree
with, will not function as a basis for effective treatment. The formulation should be dynamic and
should be updated in light of any new information or significant changes to the situation.
An example of a formulation and a blank formulation template can be found in the Appendix.
31

References
American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental
Disorders, Text Revision (DSM-IV-TR) (4th ed.). Washington, DC: Author.
American Psychiatric Association. (2014). Diagnostic and Statistical Manual of Mental
Disorders (5th ed.). Washington, DC: Author. 5
Appleby, L., et al. (2000). An educational intervention for front-line health professionals in the
assessment and management of suicidal patients (The STORM Project). Psychological
Medicine, 30(4), 805–812. 4
Bateman, A., & Krawitz, R. (2013). Borderline Personality Disorder—An evidence-based guide
for mental health professionals. Oxford.
Blum, N., et al. (2008). Systems training for emotional predictability and problem solving
(STEPPS) for outpatients with borderline personality disorder: A randomized controlled
trial and 1-year follow-up. American Journal of Psychiatry, 165, 468–478.
Busner, J., & Targum, S. (2007). The Clinical Global Impressions Scale: Applying a Research
Tool in Clinical Practice. Psychiatry (Edgmont), 4(7), 28–37.
Beck, A., & Butler A. et al. (2001). Dysfunctional beliefs discriminate personality disorders.
Behavioral Research and Therapy, 39, 1213-1225.
Carlson, E., et al. (2011). Development and Validation of a Brief Self-Report Measure of
Trauma Exposure: The Trauma History Screen. Psychological Assessment, 23(2), 463–
477
Core System Group. (1998). CORE Group System (Information Management) Handbook.
Leeds: Core System Group.
Davidson, K. (2008). Cognitive Therapy for Personality Disorders. Routledge.
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder.
Guilford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
Moran, P., et al. (2003). Standardised assessment of personality - abbreviated scale (sapas):
preliminary validation of a brief screen for personality disorder. British Journal of
Psychiatry, 183, 228–232.
Murphy, M., & McVey, D. (Eds.). (2010). Treating Personality Disorder. Routledge.
Neil, S., et al. (2009). The questionnaire about the process of recovery (QPR) : a measurement
tool developed in collaboration with service users. Psychosis, 1(2), 145–155.
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Pfohl, B., et al. (2009). Reliability and validity of the Borderline Evaluation of Severity Over
Time (BEST): A self-rated scale to measure severity and change in persons with
borderline personality disorder. Journal of Personality Disorders, 23, 281–293.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley.
Skevington, S., et al. (2004). The World Health Organization’s WHOQOL-BREF quality of life
32

assessment: psychometric properties and results of the international field trial. A report
from the WHOQOL group. Quality of Life Research, 13(2), 299–310.
Tyrer, P. ed. (2000). Personality Assessment Schedule. In Personality Disorders: Diagnosis,
Management and Course (pp. 133–159). Butterworth Heinemann. 2
World Health Organisation. (1993). International Classification of Disease, Tenth Edition, (ICD-
10).
Zanarini, M., et al. (2003). Zanarini Rating Scale for Borderline Personality Disorder (ZAN-
BPD): a continuous measure of DSM-IV borderline psychopathology. Journal of
Personality Disorders, 17(3), 2
33

34

4. Self-management
4.1 Introduction
Personality disorder is a common condition affecting upwards of one in ten of the general
population, with a significant proportion of this number coming into contact with mental health
services. The condition can have long-lasting and far-reaching effects on people’s lives but there
is a great deal that can be done to support people to manage their own difficulties.
Promoting self-management is perhaps the key in the treatment of personality disorder. This
section aims to provide some useful ideas about how practitioners can work more collaboratively
with people who experience personality disorder and what can be helpful in promoting and
supporting self-management.
In recent years, there has been an increasing recognition of the importance of self-management
in many health conditions, especially chronic conditions. The Scottish Government’s Strategy for
Self Management, called “Gaun Yersel” was developed in partnership with the Long Term
Conditions Alliance Scotland (LTCAS) and published in 2008. Although the Gaun Yersel
document is not specific to personality disorder (or even mental health), it is fair to say that self-
management is as important in personality disorder as in almost any other condition. In the
treatment of personality disorder, every intervention should have as its ultimate aim to increase
the ability of the patient to self-manage.
4.2 What is self-management?
“Self management is a person-centred approach in which the individual is empowered and has
ownership over the management of their life and conditions. The role of health and social care
professionals, services and treatment is to support the person’s journey towards living well in the
presence or absence of symptoms.” (Gaun Yersel, 2008)
Self-management is sometimes confused with self-care. Although the two concepts are related,
self-care can usefully be thought about as the typical tasks of living each person completes on
an everyday basis. The ability to carry out these tasks of daily living is often compromised for a
person living with a long term condition. In contrast, self-management describes the process a
person develops to manage their health conditions. The components of effective self-
management for someone with a long-term condition will vary from person to person but will
often include:
• Development of knowledge and understanding of the condition and its management.
• Actively sharing in decision-making with health professionals, significant social network
members and other supporters.
• Monitoring signs and symptoms of the condition.
• Managing the impact of the condition on physical, emotional, occupational and social
functioning.
• Addressing risk factors for the condition.
• Promoting health by focusing on prevention and early intervention.
• Adopting a self-management care plan (for example a Wellness Recovery Action Plan or
similar) agreed and negotiated in partnership with health professionals, significant social
network members and other supporters.
35

• Having access to and the ability to confidently use support services and mainstream
community resources.
4.3 Why is self-management important?
“The key to successful management of long term conditions lies in the hands of the person who
lives with the conditions. People need the right information and skills to develop healthy
responses to their conditions. Being told you have a condition for which there is no cure can
have a devastating effect on a person, their values and beliefs. Individual people respond in
individual ways and the impact of diagnosis will vary according to the effect of the symptoms on
the person’s life circumstances. This includes social, economic, psychological, cognitive and
cultural issues for that person, as well as the physical aspects of the condition. All of these
factors can have a profound impact on a person’s well-being and self-esteem. People cope as
best they can with the support they have but frequently they do not have the information or skills
to develop healthy responses to their condition, or make well informed decisions about their life,
let alone make plans for the future. To treat the medical condition in isolation from what is a
much more complex human picture is reductive. It ignores the fact that ultimately the key to the
successful management of long term conditions lies in the hands of the person who lives with
the condition and their desire and ability to care about themselves.” (Gaun Yersel, 2008)
People with long-term conditions make decisions, take actions and manage a broad range of
factors that affect their health on a day-to-day basis. Development of self-management skills is
likely to increase a person’s ability to proactively manage their own health, with benefits for
quality of life, sense of control, confidence levels, and specific health outcomes. Individual
clinicians, teams, services and organisations all have a role in supporting this process, as can
members of a patient’s social network. Conditions for effective self-management are most
favourable when patients, their social networks, professionals and organisations support the
approach.
Self-management can take many forms and what helps one person may not work for another.
However, time spent actively supporting, signposting or encouraging patients with personality
disorder to self-manage frequently results in the person feeling more empowered to make well-
informed decisions and more confident in their own recovery journey. This in turn increases the
likelihood of longer term health benefits. Support for self-management may take the form of
helping the patient access appropriate information, finding out what resources are available in
local communities, and developing specific skills of self-management.
Clinicians, social network members, voluntary sector workers and others have an important role
in promoting and supporting self management but the most important factor in any self-
management plan is recognition that the individual is an active agent and central to the self-
management agenda.
Promoting self-management is a key strategy in the treatment of personality disorder and
underpins most treatment approaches. A collaborative therapeutic relationship depends on the
patient engaging in self-management and the clinician supporting that process. In addition,
effective self-management can provide validation for the patient and increase motivation for the
recovery process.
36
4.4 Self-knowledge and self-reflection
Knowledge of oneself and one’s condition is crucial for effective self-management. Self-
knowledge can be usefully divided into two components – general knowledge about the disorder
which is attained through educational interventions, and specific self-knowledge which is
attained through self-observation and self-reflection.
Education about personality disorder should be an early component of any treatment process
and can be effectively delivered in a number of different formats. Education and awareness-
raising about personality disorder among clinicians is equally important.
Increasing capacity for self-reflection and understanding of the mental states of oneself and
others is a major goal in the treatment of personality disorder. These skills are basic to self-
regulation of emotion and impulse control, and are pre-requisite to changing unhelpful thoughts
and emotions. In addition, they are necessary for effective interpersonal functioning and
fundamental to the development of an integrated sense of self.
Self-reflection brings most benefit when used as a consistent strategy throughout the treatment
process and not as something that is undertaken intermittently. It is useful to highlight wherever
possible the importance of reflecting upon one’s thoughts, emotions and actions, and the value
of trying to understand the behaviours of other people in terms of their possible mental states. A
questioning style which encourages self-reflection around thoughts, emotions and behaviours is
more useful than simply providing patients with “the answers”. Supporting self-reflection may be
carried out informally or in a more structured manner such as behavioural/functional analysis
People with personality disorder can confuse their own judgements or appraisals of a situation
with the facts of the matter even more frequently than other people. Generation of alternative
perspectives and examination of a problem from different angles can enhance understanding of
difficulties in terms of internal states.
While patient self-reflection should be a primary treatment target, self-reflection in clinicans is
equally important. Strong emotions can be experienced when working with this patient group,
and understanding the origin of these emotional states can prevent inappropriate emotion-driven
behaviour on the part of the clinician. Supervision of clinicians working with this patient group is
important and should assist in self-reflection. Depending on the intensity of intervention that the
clinician is providing, supervision may occur within usual clinical supervision arrangements or
specific supervision may be required as a necessary component of a particular psychological
therapy.
4.5 Whose responsibility is self-management?
“Self management is an individual’s responsibility and supporting this process, ensuring effective
care and support is in place is everyone’s responsibility. To suggest that people should look after
themselves may seem like stating the obvious. However, many people either do not have the
necessary information and skills to make well informed decisions about their life or they choose
not to. Whatever the reason, successful management of life with a long term condition also
requires a degree of self awareness. People need to be realistic about their condition and any
limitations it may place on them, as well as how their life choices impact upon it. They also need
to be aware of the positive steps they can take to manage their condition and expand their life
choices. This is why partnership with the individual is central to the self management agenda.
37

Where people can access timely and appropriate information and support they will be more able
to make well informed decisions about their life. Part of this is therefore about enabling
everyone, individuals and organisations, to develop an understanding of recovery as a possibility
for us all. That may mean recovery at different levels with regards to the challenges faced.
Recovery needs to be adopted as a concept relating to self respect, spirit, self esteem and
sense of self. While people are generally unlikely to recover from the condition itself, effective
management of symptoms balanced with increased autonomy and independence can help
recover optimum wellbeing. Quality of life is critical with a key factor being the ability to live well
in the presence or absence of the difficulties long term conditions present.” (Gaun Yersel, 2008)
While self-management is clearly the patient’s responsibility, it is the responsibility of services to
support the process as far as possible. Self-management support can be described as the
assistance caregivers or health professionals give people with long term conditions in order to
encourage daily decisions that improve health-related behaviours and clinical outcomes. Key
factors in the process are a collaborative working partnership and a repertoire of methods and
resources which can contribute to effective, informed decision-making.
Self-management does not mean that people should be expected to manage alone without an
appropriate level of support. The intensity of support required will vary on the severity and stage
of the person’s difficulties. Some people may require minimal support at times but more
intensive support at other times.
Successful self-management relies on people having access to the right information, education,
support and services at the time when they need it. Self-management supporters have an active
role in ensuring individuals are:
• informed about their condition. This might include things like access to good quality
leaflets, books, websites and other resources, psycho-education groups and peer support,
including groups run by others with similar conditions.
• prepared for everyday challenges. This might include emotion regulation skills training,
goal setting, problem solving or recovery planning.
• supported when they need it. This might include support to make positive changes and
identification of areas where support is required including housing, financial, vocational,
educational, dietary, addiction and general health
4.6 What resources are available to support self-management?
The approach clinicians adopt can strongly influence (positively or negatively) a patient’s ability
to self-manage their health. The Appendix includes useful tools, skills and resources to help
patients improve confidence, knowledge and specific skills within different areas of self-
management support. Many resources and services will relate to more than one of these key
areas:
• Information should be trustworthy, accurate, relevant, culturally appropriate and clear to
understand. Useful resources can be found in the Appendix to this section.
• Skills enhancement. Many specific psychosocial interventions promote self-
management through goal-setting, problem-solving and emotion regulation including
DBT, STEPPS, and the CAS Day Service for people with Personality Disorder. Skills
38

training can also be delivered on an individual basis, using materials according to the
patient’s individual skills deficits rather than as part of a standardised treatment package.
In addition, there are other ways of delivering skills training, for example self-help
materials which patients can work through alone or with support. Self-help books,
websites and apps are all widely available. Some examples can be found in the
Appendix.
• Self-monitoring. This is an essential part of self-reflection and gaining self-knowledge.
This can be assisted by recording thoughts, emotions and behaviours by diaries or other
written records. Alternatively, self-monitoring apps are becoming increasingly available.
Examples can be found in the Appendix.
• Healthy lifestyle choices. The general health benefits of healthy lifestyle choices are
clear but the impact such choices can have on mental health should not be should not
underestimated. Regular exercise, a healthy diet, observing recommended limits on
alcohol, treating physical illnesses, engaging in a meaningful structured daily routine and
balancing work with rest and leisure activities can all have significant benefits on mental
health. Information about local resources can be found in the Appendix.
• Support networks. Appropriate support from health services and other agencies should
be provided when required. Too much support can be as harmful as too little in helping a
person to self-manage. Social support is also important, people should be encouraged to
build and strengthen their own support networks among neighbours, friends, family and
interest groups.
Sometimes support groups and helplines can be helpful. Examples can be found in the
Appendix
4.7 What have Highland patients found useful in supporting self-management?
When patients in the the Coping and Succeeding Day Service (CAS) for people with personality
disorder were asked the question: “What and who keeps you well?”, they answered that feeling
more connected to friends, family and community resources was fundamental to keeping well.
Peer support was also thought to be an important factor, with being around others who
understood the condition and did not judge seeming especially beneficial. Group members did
not place great importance on access to support from healthcare professionals, which may be
due to the group members being at Phase 3 of their recovery journey (largely stabilised, with a
focus on integration with the community and moving towards a life without services). However,
there was recognition that at certain points in their lives professional support may have been
more important in helping them to stay well, particularly when they were emotionally and
behaviourally dysregulated and requiring interventions from Phase 1 of the treatment model.
During Phase 1 of treatment, the group identified the importance of easy access to reliable
information which would enable them to better understand their condition, emotions and
behaviours.
The group at CAS identified that when working with healthcare professionals to support self-
management, the most important factors to promote effective working included:
• Validation and recognition of the patient’s own experience and knowledge of their
condition
39

• A supporting, collaborative relationship with the professional rather than a directive,
controlling relationship, with the patient taking the lead in their own care planning
• Effective communication between the patient and those involved in their care and
treatment
• A non-judgemental, understanding approach
• Specific approaches of value included:
• Support with goal setting
• Identifying trigger situations and further developing self-management skills which
are effective for those situations
• Problem solving, trouble-shooting and planning ahead
• Provision of clear, accurate information about the condition
• Support to find out about local activities
40

References
Lawn S and Battersby M (2009) Skills for person-centred care: Health professionals supporting
chronic condition prevention and self-management in D'cruz, et al. (Eds.) Knowledge-in-
practice in the caring professions: Multi-disciplinary perspectives. Ashgate.
LTCAS (2008) Gaun yerself: the Scottish self-management strategy for long-term conditions.
The Scottish Government
Von Korff M et al (1997) Collaborative management of chronic illness. Annals of Internal
Medicine.15;127(12):1097-102.
41

42

5. Crisis Management
5.1 Introduction
For the purposes of this section a “crisis” can be usefully defined as a brief acute, non-illness
impairment of functioning characterised by behavioural disorganisation and increased emotional
dysregulation with escalating dysphoria. The specific clinical features of a crisis will vary
according to the precipitating situation and the personality structure of the individual.
While a crisis is not a clinical disorder, one can contribute to the other. An emergency is more
than a crisis and requires a different type of response. Crises may be triggered by stress related
to a range of internal or external factors. Frequently interpersonal or social system factors are
important contributors. The duration of crisis episodes can vary significantly, but it would be
untypical for an acute crisis episode to last beyond 72 hours. However, crises may occur in a
connected series.
Many evolving crises will not require specific input from mental health services, especially if the
patient has prepared a crisis self-management plan. A distinction can usefully be drawn between
a crisis self-management plan and a clinical crisis care plan. A crisis self-management plan is
developed by the patient, often with the support of a clinician, and essentially provides a
description of a crisis and its early indicators, options and resources which have proved useful in
previous crises, things which have previously proved unhelpful when in crisis and which should
be avoided, and an outline plan of action for the next evolving crisis. This can be especially
useful as problem solving and cognitive flexibility is typically impaired with escalating emotional
arousal. In contrast, a clinical crisis care plan is developed by the treating team with the
collaboration of the patient to provide a plan outlining how the team aims to respond to the
patient’s next crisis.
When intervention by services is indicated, the aim is to enable the patient to return to their
usual level of functioning as soon as possible. Clinicians should avoid trying to achieve too much
during crisis episodes and keep goals and interventions as simple as possible. Only once the
acute crisis has resolved should longer term goals be addressed. In terms of the ‘phase-based
approach’ to the treatment of people with personality disorder, crisis management represents
Phase 1 (stabilisation) work, with the initial emphasis on safety and containment, although work
to promote self regulation is likely to follow shortly after.
Risk assessment is important in crisis episodes, especially of risk of suicide, although other risks
should also be considered. During risk assessment, it is important to draw the distinction
between chronic (longstanding) and acute (newly increased) risk. Many people with personality
disorder have chronic thoughts that life is not worth living or frank suicidal thoughts. Two
principal factors which can contribute to an acute increase in risk of suicide are increased intent
and increased impulsivity.
5.2 Crisis planning
Crisis planning is an important part of the care and treatment of people with personality disorder.
Both patients and clinicians have important roles to play in the process.
The patient’s crisis self-management plan and the clinical crisis care plan should both be seen
as dynamic documents to be reviewed and amended as the patient’s self-knowledge and skills
develop. In addition, review and update of both plans should occur at the earliest opportunity
43
after a crisis. Useful telephone support, advice and helplines can be found in the Appendix.
5.3 Patient’s crisis (self-management) plan
In assisting a patient to develop their own crisis self-management plan, clinicians support self-
management by highlighting the strengths and responsibilities of the patient. The format of a
patient’s crisis plan can vary, but will generally include individualised information on crisis
indicators, what has helped in the past, what has been unhelpful, useful contacts and specific
plans for self-management of future crises. Examples of template crisis self-management plans
are available in the appendix for this section.
Patient’s crisis self-management plans should be developed as early as possible in the
treatment process, ideally from the point of assessment and diagnosis. It is important that the
plan should be developed at a time when the patient is not in acute crisis and can draw upon
their baseline capacity for planning and problem solving. The clinician should support the patient
to take responsibility for developing their own plan and avoid providing “the answers” as far as
possible. The process itself should be a validating one, promoting the patient’s role of primary
responsibility in their own recovery and highlighting their ability to at least attempt to resolve
what may seem to be overwhelming problems.
In keeping with the principle of self-management, the finished document remains the property of
the patient for them to refer to when necessary. Clearly, for the plan to be useful in the process
of self-management, it should be kept in a readily accessible place, ideally carried by the patient
at all times. It is of particular importance for the patient to be able to locate the document as
easily as possible, as the ability to find the document when a crisis is evolving is likely to be
much reduced.
While it is important that it is recognised that the patient retains ownership of the document, it is
recommended that the patient shares it with those involved in their care. Clinicians can then
make the important information in the crisis plan accessible to other treating clinicians, for
example by keeping a copy in the patient’s medical notes, attaching a copy to clinic letters so
that it can be placed in SCI store or scanned into the patient record in Primary Care,
encouraging GPs to consider using the ‘Special Notes’ system for NHS24 contacts or similar.
5.4 Clinical crisis care plan
A clinical crisis care plan is developed by the treating team with the collaboration of the patient to
provide a plan on how the team aims to respond to the patient’s next crisis. Such a crisis care
plan may form part of standard care planning but for patients with more severe presentations,
the Care Programme Approach documentation may prove useful. The patient’s crisis self-
management plan is likely to complement a crisis care plan and consideration should be given to
keeping a copy of the crisis self-management plan with the crisis care plan or CPA.
5.5 Indicators of a Crisis
A crisis can be identified by acute changes in a range of domains. It is important to assess for
the presence of co-occuring mental state disorders such as psychosis or affective disorder which
may sometimes present with similar features.
Affective changes may include:
• Increased emotional lability
• Panic and anxiety
44
• Escalating dysphoria
• Low mood
• Anger
Behavioural changes may include:
• Parasuicidal behaviour (includes suicidal gestures and attempts, and non-suicidal self-
injury)
• Increased impulsivity
Cognitive / perceptual changes may include:
• Dissociation or transient psychotic features
• Reduced cognitive processing ability including reduced ability to cope and utilise
resources, to think logically and to problem solve.
• Reduced ability to retain awareness of the internal processes of oneself and others
Presence of these features can lead to worsening of difficulties regarding self, others and
society. Interpersonal stress is frequently a precipitating or perpetuating factor for crisis
episodes.
5.6 Assessment and management of crises
In times of crisis, patients with personality disorder are ideally assessed and managed by those
who know the patient and their background, although this may not always be possible. As far as
possible, aim to conduct the assessment in a quiet area with as few interruptions as possible
Each clinician will have their own approach to assessing a patient in crisis but assessment
should be undertaken with some overarching principles. The principles of validation and
collaboration are especially important.
Clinicians should adopt a calm, non-judgemental and non-confrontational approach. It is
important that clinicians should actively listen to the story and reflect the patient’s perception of
events back to them. It is important to validate the patient’s experience and avoid minimising,
inappropriately reassuring, or jumping to premature problem solving. Interpretations or
hypotheses about the reasons why a crisis occurred are likely to be of limited value at this stage
and the focus should remain on containment as far as possible.
Patients often report that it feels more containing in a crisis to have the validating experience of
feeling understood in the “here-and-now” in the context of recent (proximal) situational factors ,
rather than to understand the historical (distal) factors which may have led to the crisis. Distal
factors are more usefully explored in depth after resolution of the acute crisis. In practice
lengthy exploration during an acute crisis is unlikely to be helpful and may even contribute to
further destabilisation. Where the patient is new or unknown to the assessor then background
information on their psychiatric history and social context should be obtained if possible through
medical notes or CPA records .This can help maintain focus on the ‘here and now’ or proximal
factors during the crisis assessment. A picture of the current situation should be developed with
a view to promoting a return to previous level of functioning as soon as possible by supporting a
self-management and problem solving approach
It is helpful to use validating language to clearly acknowledge the distress of the patient.
Challenging the perspective of the patient on their own thoughts and feelings is likely to be
perceived as invalidating and this can put the therapeutic relationship at risk. An exception to
45

this is if a pattern of invalidating negative self-judgement is noted. In such a case, self-
invalidation should be gently challenged by highlighting the difference between facts and
judgments.
The clinician, after actively listening and then reflecting their understanding of the situation back
to the patient, can explore solutions together with the patient in a collaborative manner using
formal problem solving or solution analysis. The assessor should:
• Draw on the patient’s own resources and skills
• Reflect on solutions and promote an alternative perspective to the patient
• Highlight the patient’s responsibility in their own recovery
• If appropriate, involve the patient’s social network
In general, when the patient has a crisis self-management plan and/or crisis care plan, theseshould be utilised in the crisis management process.
• Crisis management should initially focus on safety and containment strategies. Work to
promote self-regulation should be introduced as soon as possible.
• Crisis management should comprise simple short-term interventions focusing on the
“here-and-now” rather than the past or the future, and aim for the minimum input
necessary to enable the patient to return to their previous level of functioning.
• Medication may have a role in some situations but in general the principle is “as little as
possible for a short a time as possible”. Prescribers should be aware of the risk of
overdose in those presenting in crisis and in particular the potentially disinhibiting effects
of benzodiazepines, see Medication Section.
5.7 Risk assessment and management in crisis
It is recommended that a detailed risk assessment be undertaken in patients presenting in
crisis. This should be carried out in an empathic and non-judgmental manner, taking account of
risks to the patient but also identifying risks to others, including children and vulnerable adults.
Patients’ crisis self-management plans, CPA plans and clinical crisis care plans should be used
where available to assist with the risk management process.
Risk assessment should include history, mental state and situation as well as systematic
assessment of static and dynamic risk factors. Structured tools such as STORM (Skills Training
On Risk Management) may be helpful, see Appendix. STORM documentation can be found in
the STORM folder on the NHS Highland intranet O drive.
Clinically indicated positive risk taking following a risk-benefit analysis is an important com-
ponent of the care and treatment of patients with personality disorder. While safety must always
remain a primary consideration in such an analysis, it must be recognised that complete
elimination of risk is impossible. Risk management decisions should as far as possible be made
by the multidisciplinary team in collaboration with the patient. It is important to recognise that,
while the clinical team is responsible for providing a reasonable standard of care, the patient
retains responsibility for their behaviour and the consequences of that behaviour. A patient with
personality disorder should always be assumed to be a competent adult, able to make and
responsible for their own choices, unless there are compelling reasons to think otherwise, for
example severe mental state disorder. In good multidisciplinary working, clinical responsibility
for risk management decisions belongs to the whole multidisciplinary team rather than any
single clinician.
46

5.8 Community management of crisis
Most crises will not require the input of services and can be resolved by the resources available
to the person in their social network. Self-help guides and information may be of value in
supporting this process. When involvement of mental health services is indicated by reason of
risk, severity or frequency of crises, relevant community services include:
• Community Mental Health Teams
• Braeside Crisis and Intensive Treatment Service, for Inverness sector patients who
present significant risk to themselves or others and who would otherwise be considered
for admission to hospital.
5.9 Hospital management of crisis
Acute in-patient management should be considered with the guidelines on in-patient manage-
ment in the ICP in mind. Admission to hospital should usually not be considered when other
options are appropriate.
5.10 After resolution of the crisis
At the earliest opportunity, the assessor should arrange that all clinicians involved in the
patient’s care are informed of the details of the crisis and the current treatment plan. In
addition, the patient’s crisis self-management plan and the clinical care plan should be updated
at the earliest possible opportunity.
Crises are likely to recur unless a patient’s situation changes or their ability to cope with their
situation changes. A crisis can therefore become a useful opportunity to open the discussion
about longer term care and treatment options for personality disorder.
47
References
Bateman, A., & Fonagy, P. (2006). Mentalization-based treatment for borderline personality
disorder. Oxford University Press.
Bridgett, C., & Polak, P. (2003a). Social systems intervention and crisis resolution. part 1:
Assessment. Advances in Psychiatric Treatment, 9, 424–431.
Bridgett, C., & Polak, P. (2003b). Social systems intervention and crisis resolution. part 2:
Intervention. Advances in Psychiatric Treatment, 9, 432–438.
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder.
Guilford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley
48
6. Psychosocial Interventions
6.1 Introduction
In the past, personality disorder has often been deemed untreatable and patients have been
excluded from services on that basis. However, over the past 20 years, several treatments have
demonstrated benefit in the treatment of personality disorder. The greater part of the work has
focused on borderline personality disorder, probably because of the often dramatic
presentations, high demand on services, and elevated suicide rates of people with the condition.
However, some studies have looked at other specific personality disorders with some success.
For example, there is some evidence that that Cognitive Behavioural Therapy (CBT) may be of
value in the treatment of avoidant personality disorder.
All treatments which have been demonstrated to be beneficial for personality disorder are forms
of psychosocial intervention. Despite a significant body of work, there has been no robust
experimental demonstration that any other form of treatment (including medication) is of
significant benefit in the treatment of the condition.
A psychosocial intervention can be defined as any intervention that emphasizes psychological or
social factors rather than biological factors. Psychosocial interventions can be taken to include
specific psychological therapies, such as Dialectical Behaviour Therapy (DBT), and more
general interventions, such as crisis planning, problem-solving training and psychoeducation.
All psychosocial interventions for personality disorder should be concordant with, and informed
by, the concepts described in the General Principles Section of this document, namely:
• Recovery
• General treatment strategies of:
Collaboration
Consistency
Motivation
Validation
Self-knowledge and self-reflection
• Stages of change model
• Phase-based treatment
Phase 1: Stabilisation (Making Stable): this phase, with a primary focus on
the present, deals with safety, containment and promotion of self-regulation and
control.
Phase 2: Exploration and Change (Making Sense): this phase, with a
primary focus on the past, can commence once stabilisation occurs, even
temporarily. The aim is to identify and make changes to the factors which underlie
the unhelpful behaviours. This phase can involve dealing with the effects of trauma
and dissociation; treating self and interpersonal problems; and treating maladaptive
traits.
Phase 3: Integration and Synthesis (Making Connections): this phase, with a
49

primary focus on the future, is not so much about changing existing psychological
and interpersonal structures and processes as putting new ones in place. The aim
is to promote a more integrated sense of self and a healthier interpersonal
environment — this may include new leisure activities, occupational/educational
activities, new roles and relationships.
• Matched care
The psychotherapies for personality disorder which have evidence of effectiveness are largely
derivatives of either psychodynamic approaches, or cognitive-behavioural approaches, although
some have features of both. Within NHS Highland, the specific psychosocial interventions
available are primarily cognitive-behavioural in orientation. For example, STEPPS and DBT, the
two main Phase 1 treatments for borderline personality disorder available in
NHS Highland, are cognitive-behavioural treatments.
6.2 General psychosocial interventionsThis represents a very broad category of interventions which are of value across different
conditions and will not be specific to the treatment of personality disorder. It is beyond the scope
of this document to attempt to make a list of general psychosocial interventions, but examples
include crisis planning, problem-solving training, emotion regulation training and psycho-
education of various kinds. The category of general psychosocial interventions also includes
recovery and relapse-prevention planning (for example, the Wellness Recovery Action Plan or
(WRAP). As stated previously, it is important that any interventions used are coherent with, and
informed by, the concepts described in the General Principles Section of this document and fit
within an overall psychologically-informed formulation and treatment plan.
Crisis planning is of particular importance in personality disorder and should be considered early
in any treatment process. When people with personality disorder experience intense emotions,
their ability to think clearly is reduced, often even more than for other people. Hence a crisis plan
can be invaluable, with options and contacts for dealing with a crisis situation readily available.
Although a crisis plan may be produced in collaboration with a clinician, it necessarily remains
the patient’s document. However, clearly it is likely to be useful for the patient to share copies
with relevant people. Examples of crisis self-management plan templates can be found in the
Appendix.
6.3 Specific psychosocial interventions
Specific psychosocial interventions are interventions which have been specifically developed for
the treatment of personality disorder. These interventions should be delivered in a phase-
appropriate manner as part of an overall treatment package. It is important to recognise that no
one intervention on its own represents a comprehensive treatment for personality disorder.
Review of the treatments for personality disorder with evidence of effectiveness reveals that the
different approaches have some features in common. The principal factors are listed in the
Borderline Personality Disorder NICE Guideline and include:
• having an explicit and integrated theoretical approach used by treatment team and
therapist and shared with the patient
• provision for appropriate therapist supervision
• clear structuring of care
50

• being relatively longer term (NICE guidelines suggest interventions of less than 3 months
should be not used to treat personality disorder unless the short intervention forms part of
a longer term treatment plan. This is in part because emotional dysregulation associated
with perceived abandonment is likely when a treatment ends and a shorter treatment is
unlikely to provide the opportunity to learn the skills needed to self-regulate effectively).
All specific psychosocial interventions should be delivered by professionals with the appropriate
training, experience and competencies. Given the challenges of working with people with
personality disorder, appropriate supervision is crucial. The intensity, frequency and form of the
supervision required is likely to vary from intervention to intervention. For example, the clinicians
delivering an extensively manualised treatment such as STEPPS may benefit from brief post-
group peer supervision between skills trainers, multidisciplinary discussion at CMHT meetings,
and discussion within usual clinical supervision. However, at times, certain challenging issues
may arise which may warrant additional supervision. Some more intensive interventions like
Dialectical Behaviour Therapy (DBT) have scheduled weekly supervision built into the treatment
model.
While psychosocial interventions should as far as possible be delivered according to the
protocols upon which evidence of benefit is based, it is recognised that rurality and remoteness
may sometimes make this impossible. In these situations, a flexible, pragmatic approach is
advised. For example, it may be reasonable to consider delivering the STEPPS materials to a
patient on an individual basis if attendance at a group is impossible. However, in such a case, it
should be made clear that the intervention which is being delivered is not STEPPS per se, and
consideration needs to be given to the treatment frame and related factors. The Personality
Disorder Service is available for consultation as required.
While it is acknowledged that some interventions may address more than one phase of
treatment, for the sake of clarity, the interventions commonly available in NHS Highland are
listed below under the phase of treatment which represents the usual primary focus. The
description for each intervention attempts to answer four questions:
• What is it?
• Who is it for?
• Who is it not for?
• How can it be accessed?
Each Intervention is on a separate page to simplify printing.
6.4 Interventions with a primary focus on Phase 1
Most of the evidence base for the treatment of personality disorder relates in particular to
borderline personality disorder. Perhaps understandably, given the dramatic, resource intensive
and risky presentations associated with marked emotional and behavioural dysregulation, almost
all the published literature for borderline personality disorder describes interventions with a focus
on Phase 1 (stabilisation).
While stabilisation is of paramount importance, it should usually be regarded as a means to
enable the subsequent phases of treatment to take place and not as an end in itself. Clinical
experience suggests that if subsequent phases of treatment are not undertaken when
necessary, relapse to previous unhelpful patterns of behaviour is likely, impeding the patient’s
51

recovery. As explained in more detail in the General Principles Section, subsequent phases of
treatment may not always require formal input from mental health services and may be worked
through by the person using their own personal and interpersonal resources. For example, a
person with emotional and behavioural dysregulation but without a significant trauma history
may attain sufficient behavioural and emotional stability from completion of the STEPPS
program to allow meaningful reflection on, and changes to, longstanding patterns of behaviour.
This might mean that the person recognises that lack of structure and meaningful use of time
had helped to maintain their difficulties in the past. They may decide to join new social groups
and enter employment (Phase 2). The improved interpersonal and social landscape which
results may contribute to an improved sense of self and connection to their family, friends and
wider society, reducing the likelihood of future relapse, distress and dysfunction (Phase 3).
52

6.4.1 Dialectical Behaviour Therapy (DBT)
What is it: DBT is a structured intensive CBT-based Phase 1, tier 3 treatment for people with
severe borderline personality disorder.
Treatment generally lasts for 6 months to 1 year. Each week the patient attends a 2 hour
skills training session in which 2 DBT therapists teach skills of mindfulness, emotion
regulation, distress tolerance and interpersonal effectiveness. It takes 26 weeks to
complete a cycle of the 4 skills modules. Patients often complete 2 cycles of skills
training.
In addition to the skills training, each patient attends for 1 hour of individual therapy each
week with the same therapist. This involves the patient recording daily emotions,
behaviours and thoughts on a diary card which is reviewed in session with a view to
enhancing and generalising skills.
DBT is not used as a stand-alone treatment but represents part of an overall care plan.
DBT is delivered by the Personality Disorder Service in Inverness, serving the whole of
NHS Highland.
Who is it for: Individuals with severe borderline personality disorder. DBT is primarily a
technology of behavioural and emotional stabilisation and has an evidence base in
reducing parasuicidal behaviour and psychiatric hospitalisation. Individuals are required to
be on the Care Program Approach for the duration of their involvement in DBT.
Who it is not for: Less severe forms of borderline personality disorder (consider STEPPS).
Personality disorders without a severe borderline component. Patients who pose risks
which are unmanageable in a community group setting.
How can it be accessed: In NHSH, the DBT program is a specialist service. Referrals are
taken from secondary and specialist mental health services. The PDS encourages contact
to discuss possible referrals.
53

6.4.2 Systems Training for Emotional Predictability and Problem Solving (STEPPS)
What is it: STEPPS is a highly manualised, tier 2, CBT-based skills training program with a
systems component for people with borderline personality disorder and traits. The
principle focus is on Phase 1 (stabilisation). STEPPS was originally developed as an
add-on to usual treatment rather than a stand alone treatment. Treatment lasts for 20
weeks. During that time the individual attends a weekly 2 hour skills training session in
which 2 STEPPS skills trainers teach skills addressing a broad range of difficulties
associated with borderline personality. Individuals are given specific homework each
week related to the topic of the session and they are also asked to record situations of
high emotional intensity. The first half of each session comprises a review of homework
and new skills are taught during the second half.
Significant others are involved as part of the reinforcement team and are given recom-
mendations on how to respond to the person with BPD in a situation of emotional
intensity. Participants should ideally also have an individual skills reinforcer with whom
they should meet weekly — this can be anyone with some knowledge of mental health
issues for example a GP, CPN, mental health social worker etc. The idea is that the
participant brings the homework to the reinforcer, explains that week’s topic and
discusses any problems, in much the same way that a child asks for help with school
homework from a parent. The individual skills reinforcer and the significant others make
up the reinforcement team. A session for members of the reinforcement team is usually
offered early in the 20 week program.
Who is it for: Individuals with moderate borderline personality disorder and or borderline
features. Severely behaviourally dysregulated individuals are more likely to benefit from
the more intensive DBT.
Who is it not for: People who do not fulfil criteria for borderline personality disorder or
experience borderline features. Patients who pose risks which are unmanageable in a
community group setting.
How can it be accessed: Each CMHT runs its own STEPPS group and referral of possible
candidates should the made to the CMHT.
54

6.4.3 Cognitive Behaviour Therapy for Personality Disorder (CBTpd)
What is it: CBTpd is a modified individual cognitive behaviour therapy for individuals with
personality disorder. It primarily focuses on Phase 1 (stabilisation) and 2 (making sense)
but there may be some work on Phase 3 (making connections) for some patients.
Treatment typically lasts for 30 sessions over a period of one year, which is a longer
course of treatment than in standard CBT. There is more of an emphasis on a
developmental perspective than in standard CBT and a written narrative formulation is
developed with the individual early in the therapy process. Early treatment targets include
behavioural stabilisation, especially of harmful behaviours. Later phases of treatment
attempt to reduce other overdeveloped behaviours and increase underdeveloped
behaviours. Cognitive work focuses on the level of core beliefs rather than at the level of
automatic thoughts as in standard CBT.
Who is it for: Individuals with personality disorder, although best evidence is for borderline
personality disorder. Individuals who are unable to benefit from a group based treatment,
for example people with hearing impairment, may also find CBTpd more suitable.
Who is it not for: People who do not fulfil criteria for personality disorder.
How can it be accessed: CBTpd availability within the PDS is currently limited but referrers
can contact the PDS or locality Clinical Psychologist/CBT therapist to discuss the
possibility of this intervention for particular patients
55

6.6.3 STAIRWAYS (follow-on group from STEPPS)
What it is: STAIRWAYS is a one-year long, twice monthly advanced group program developed
for clients with borderline personality traits and disorder who have completed the 20-week
STEPPS program. The reduction in frequency from the weekly STEPPS program is
designed to encourage group members to seek out non-therapy activities between
meetings. Each session lasts for 2 hours. New participants are able to join the group at
frequent intervals as opposed to STEPPS which runs as a 20 week closed group.
The program, which is cognitive-behavioural in orientation, reinforces and expands on the
skills learned in STEPPS with the aim of improved management of emotional intensity.
There is also an emphasis on the application of the new skills to specific goals and
challenges in the occupational, educational, recreational and interpersonal domains. The
primary focus of STAIRWAYS is on enhancing Phase 1 emotion regulation skills,
although there is increased focus on Phases 2 and 3 compared with STEPPS.
Who is it for: Individuals with moderate borderline personality disorder and traits (perhaps in
early remission) who have completed STEPPS and are relatively behaviourally stable.
Who is it not for: People who have not completed STEPPS. People who are significantly
behaviourally dysregulated.
How can it be accessed: STAIRWAYS is currently offered within the Inverness CMHT on a
limited basis only.
56

6.5 Interventions with a primary focus on Phase 2
People with personality disorder will often have a history of abuse. Around three quarters of
people with borderline personality disorder will have recallable abuse and about half of people
with BPD will meet criteria for post-traumatic stress disorder (PTSD). Some have suggested
that those people exposed to repeated, expected trauma which is perceived as inescapable,
can develop a condition known as complex PTSD. Although this disorder is not specifically
described in ICD-10 or DSM-5, it is frequently written about in mainstream journals. Its
diagnostic criteria are similar to borderline personality disorder and treatment approaches are
similar, although the evidence base is much smaller. The clinical utility of separating these
conditions is unclear.
Eye Movement Desensitisation and Reprocessing (EMDR) and Trauma-focused Cognitive
Behaviour Therapy (tfCBT) have been included in this section because of the high rates of
PTSD in the personality disorder patient group. However, strictly speaking, they are not
personality disorder-specific interventions, but were developed for people with PTSD (with or
without personality disorder).
Although Phase 2 treatment will often concern post-traumatic problems, sometimes the work
will deal with other difficulties in long-standing patterns of behaviour and thinking.
Integration or “joining-up” of the different phases of treatment in a timely manner is crucial. The
commencement of phase 2 treatment should occur when the patient is “stable enough”.
Although each decision should be made on a case by case basis, the criteria used to determine
readiness for trauma work within the DBT-PE protocol provides a reasonable guide:
• Not at imminent risk of suicide (by next month or by next session)
• No life-threatening behaviour for a period of 2 months or so
• Ability to control life-threatening behaviours in the presence of cues for those behaviours
• No serious therapy interfering behaviour
• Trauma work is the patients highest priority treatment target
• The patient wishes to engage in the work at this point
• Ability and willingness to experience intense emotions without escaping
Very often, progression through phases is not unidirectional and many people will require short
periods of restabilisation during later phases of treatment.
57

6.5.1 Dialectical Behaviour Therapy—Prolonged Exposure (DBT-PE)
What is it: DBT is a structured intensive CBT based Phase 1, tier 3 treatment for people with
severe borderline personality disorder.
Treatment generally lasts for 6 months to 1 year. Each week the patient attends a 2 hour
skills training session in which 2 DBT therapists teach skills of mindfulness, emotion
regulation, distress tolerance and interpersonal effectiveness. It takes 26 weeks to
complete a cycle of the 4 skills modules. Patients often complete 2 cycles of skills
training. In addition to the skills training, each patient attends for 1 hour of individual
therapy each week with the same therapist. This involves the patient recording daily
emotions, behaviours and thoughts on a diary card which is reviewed in session with a
view to enhancing and generalising skills.
DBT is not used as a stand-alone treatment but represents part of an overall care plan.
DBT is delivered by the Personality Disorder Service in Inverness, serving the whole of
NHS Highland.
Around half of patients with borderline personality disorder will also meet diagnostic
criteria for post-traumatic stress disorder. Once stabilisation has occurred with standard
DBT, it may be appropriate to consider using the DBT-Prolonged Exposure (DBT-PE)
protocol for Phase 2 of treatment (trauma work).
DBT-PE is an integration of DBT and standard Prolonged Exposure (a CBT approach with
an evidence base for treating PTSD). DBT-PE is delivered within the individual
component of DBT. The sessions will typically last 90 minutes to 2 hours, compared with
the 1 hour sessions of the standard DBT individual component.
The two main components of DBT-PE are imaginal exposure and in vivo exposure.
Imaginal exposure involves the patient voicing the narrative of relevant past traumatic
events and listening to recordings of the narrative between sessions until habituation to
the associated emotion occurs. In vivo exposure involves the construction of a hierarchy
of distressing situations which are avoided because of past trauma events and exposure
to the distressing situations. The aim is habituation to the associated emotions and
reduction in behavioural and cognitive avoidance.
DBT-PE is conceptualised as a treatment strategy within DBT and patients engage with
all usual components of DBT in DBT for the duration. If behavioural destabilisation occurs
during DBT-PE, the treatment focus will return to Phase 1 or standard DBT.
Who is it for: Individuals with severe borderline personality disorder and post-traumatic
symptoms. Individuals need to be on the Care Programme Approach for the duration of
their involvement in DBT.
Who it is not for: Patients not in DBT.
How can it be accessed: In NHSH, the DBT program is a specialist service. Referrals are
taken from secondary and specialist mental health services. The PDS encourages contact
to discuss possible referrals. Patients cannot be referred for DBT-PE itself (as opposed to
referring for DBT) as it represents a treatment strategy within DBT rather than a
standalone treatment in its own right. All patients who are referred for DBT will receive a
trauma assessment and DBT-PE will be offered if appropriate.
58

6.5.2 Eye Movement Desensitisation and Reprocessing (EMDR)
What is it: EMDR is a psychological treatment which has been demonstrated by several meta-
analyses to be effective in the treatment of post-traumatic stress disorder (PTSD). It is
recommended as a first line treatment for PTSD by NICE.
The treatment involves visualisation of traumatic events while experiencing auditory,
visual or tactile bilateral stimulation. It is not a treatment specifically for people with
personality disorder but was developed for people who experience PTSD. EMDR is listed
here given the substantial proportion of people with personality disorder who also meet
criteria for PTSD. EMDR represents a Phase 2 treatment.
Who is it for: Individuals with PTSD who are sufficiently stable.
Who it is not for: Individuals who are not sufficiently stable, especially those who use harmful
behaviours to regulate emotional distress.
How can it be accessed: Refer via Community Mental Health Team single point of referral.
Direct discussion with the person who provides EMDR in the sector might be helpful to
facilitate integration of Phase 1 with Phase 2 work.
59

6.5.3 Trauma Focused Cognitive Behavioural Therapy (tfCBT)
What is it: tfCBT is a form of CBT which has been demonstrated by several meta-analyses to
be effective in the treatment of post-traumatic stress disorder (PTSD). It is recommended
as a first line treatment for PTSD by NICE. tfCBT represents a Phase 2 treatment.
The treatment usually involves imaginal exposure to traumatic memories and real life
exposure to avoided situations, together with cognitive restructuring. These procedures
can involve narrating the story of the traumatic events within session and listening to
recordings of the story between sessions; actively exposing oneself to avoided and feared
situations; and challenging unhelpful thoughts which are helping maintain patterns of
avoidance. It is not a treatment specifically for people with personality disorder but is
listed here given the substantial proportion of people with personality disorder who also
meet criteria for PTSD.
Who is it for: Individuals with PTSD who are sufficiently stable.
Who it is not for: Individuals who are not sufficiently stable, especially those who use harmful
behaviours to regulate emotional distress.
How can it be accessed: Refer via Community Mental Health Team single point of referral.
Direct discussion with the person who provides tfCBT in the sector might be helpful to
facilitate integration of Phase 1 with Phase 2 work.
60

6.6 Interventions with a primary focus on Phase 3
For some people, Phase 1 work (perhaps with some Phase 2 work) will be sufficient to allow
Phase 3 to occur without the involvement of services. However, some patients will benefit from
a specific intervention to enable meaningful personal, interpersonal and social progress to
occur.
61

6.6.1 Occupational Therapy (OT)
What is it: Occupational Therapy is concerned with enabling individuals to live more productive
and enjoyable lives in vocation, employment, social interactions and leisure, through the
use of purposeful activities.
The occupational therapist usually works as part of a multi-disciplinary team and can
contribute to the overall care plan of individuals referred to the team. Each person is
assessed individually, goals are identified together and a programme of activities is
planned collaboratively. The individual is asked to identify outcomes which are
measurable to enable interventions to be evaluated, for example: “I want to be able to join
an evening class”, “I will be able to discuss my feelings with my partner”, “I want to be
able to do my own shopping and cooking” or, “I want to get an interesting job”. Activity
programmes are reviewed regularly and adapted as necessary.
Activity is at the core of occupational therapy practice. If the therapist cannot engage the
client in activity that has meaning and value for him, then there can be no meaningful
assessment and no treatment implementation. Engagement is achieved by involving the
client at all stages of the treatment process, by understanding what will motivate the
individual, and by establishing an expectation that clients attending occupational therapy
will be active in their own treatment processes. The activity must be purposeful and
achievable for the person and take place in settings relevant for that person. Activities can
take place on a 1:1 basis, in a group, or in both settings.
Summary of activity functions:• Activity is essential for the normal development of the individual. Without activity no
personal development can take place, and inability to perform activities competentlyleads to a maladaptive development.
• People use activity to explore the environment and to test their own position in it.
• We become embedded in our social and cultural context through activity.
• Activity helps to build a healthy personal and social identity.
• Activity is intrinsically satisfying.
• Activity is used to learn and practice skills that can be used for occupationalperformance.
• People are able to adapt to changing circumstances through activity.
• The individual can construct purpose and meaning in his life and gratify his needsthrough activity.
• Relationships with others can be made through shared activity.
Who is it for: OT is for anyone who wants to overcome physical, psychological or social
problems arising from illness or disability. The person needs to be motivated to identify
goals and to engage in activities.
Who is it not for: As OT requires active participation for it to be effective, it will not work if the
person is not ready to become involved in trying activities.
How can it be accessed: OTs work in hospitals and in the community. Within mental health
services, they are based in CMHTs (Community Mental Health Teams). A referral from a
GP, psychiatrist or other worker is required. Self-referrals can be made in some teams
and the person’s GP would be made aware.
62

6.6.2 CAS Day Service for People with Personality Disorder
What is it: The CAS (Coping and Succeeding) Day Service for people with personality disorder
is a community-based service which takes place each Friday from 09:30 to 15:30 at
Rowans, New Craigs Hospital. CAS Day Service represents a tier 3, Phase 3 (integration
or making connections) intervention. The usual length of treatment is 36 weeks.
CAS, a co-produced service, has been developed and is delivered by a partnership of the
Personality Disorder Service with service users and other stakeholders along Recovery
principles. The service is primarily directed at helping an individual make connections with
others and society and by doing so, enhance their self-identity, interpersonal and social
connections.
CAS has a primary focus on Phase 3 and, to a lesser extent, Phase 2 but it is not an
intervention with an emphasis on stabilisation. Other interventions (eg DBT or STEPPS)
are more appropriate for stabilisation of harmful behaviours. Furthermore, some
individuals, although behaviourally stable, may benefit from Phase 2-focused
interventions, for example specific trauma work, before making best use of CAS.
The CAS Day Service includes elements of structured group work, self-directed time and
social time. Broad themes covered in the core groups include promotion of physical health
and well-being; living skills; self-management; and vocational rehabilitation. These
themes are addressed by providing direct information and education; enabling direct
introduction to new activities/behaviours; and making and highlighting links between
people and services.
In the spirit of co-production, participants have a major role in planning and organising the
content of the core groups and the day to day running of the service. Participants develop
and work towards their own goals in the interpersonal, occupational, recreational and
educational domains.
Who is it for: Individuals with personality disorder or personality disorder in early remission
(not solely people with borderline personality disorder) who are motivated to make
changes and who do not carry current risk issues which would preclude safe placement in
a community setting.
Who is it not for: People who do not meet the general diagnostic criteria for personality
disorder.
People with current risk issues which preclude safe placement in a community setting —
for example, people who present a significant risk of violence to others or a significant risk
of harm to themselves.
People who are unwilling or unable to usefully work cognitively, affectively and be-
haviourally, for example people with active substance dependence, brain injury or low
weight anorexia nervosa.
How can it be accessed: CAS is part of the Personality Disorder Service, a specialist service
which accepts referrals from secondary and specialist mental health services. A self-
referral option is currently being piloted. New participants can join the group at frequent
intervals.
63
6.6.3 Vocational Support Service
What is it? The Vocational Support Service aims to work in partnership with individuals who
have experienced mental health challenges; supporting them on their vocational pathway.
The service will help individuals to identify vocational goals and support the steps towards
achieving them.
The Vocational Support Team will work individually with people to help explore opportu-
nities such as volunteering, further education, gaining or sustaining paid employment.
Support may also include identifying community activities, building self-confidence or
improving skills with computers and other technology in terms of preparing people for
vocational activities.
Who is it for? The Service is for those individuals, aged 18 or upwards, who have had difficulty
gaining or sustaining vocational activities due to mental ill health.
Who is it not for? This service is not for people who do not wish to move forward with
vocational goals.
How can it be accessed? The Vocational Support Team has two bases — one in Inverness
and the other in Thurso. For more information or to receive a referral form please contact:
Vocational Support Team (Inverness)
Rowans 1
New Craigs
Leachkin Road
Inverness IV3 8NP
Tel: 01463 253 635 Email: [email protected]
Vocational Support Team (Thurso)
The Bungalow
Dunbar Hospital
Thurso KW14 7XE
Tel: 01847 896 831 Email: [email protected]
64
References
Bateman, A., & Krawitz, R. (2013). Borderline Personality Disorder—An evidence-based guide
for mental health professionals. Oxford.
Blum, N., et al. (2008). Systems training for emotional predictability and problem solving
(STEPPS) for outpatients with borderline personality disorder: A randomized controlled
trial and 1-year follow-up. American Journal of Psychiatry, 165, 468–478.
Davidson, K. (2008). Cognitive Therapy for Personality Disorders. Routledge.
Harned, M., et al. (2014). A pilot randomized controlled trial of Dialectical Behavior Therapy with
and without the Dialectical Behavior Therapy Prolonged Exposure protocol for suicidal
and self-injuring women with borderline personality disorder and PTSD. Behaviour
Research and Therapy, 55, 7–17.
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder.
Guilford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
Murphy, M., & McVey, D. (Eds.). (2010). Treating Personality Disorder. Routledge.
NHS Education Scotland. (2011). The Matrix: A Guide to delivering evidence based
Psychological Therapy
http://www.nes.scot.nhs.uk/media/3325612/matrix_part_1.pdf
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley.
65

66

7. Medication
7.1 Introduction
No drugs are licensed for the treatment of personality disorder in the UK and evidence for
efficacy of drug treatment is scarce. Inappropriate use of medication can impede development of
personal responsibility for recovery, impair functioning and contribute to a sense of pessimism
when progress does not occur.
The only treatments with evidence of effectiveness in the treatment of personality disorder are
psychosocial interventions. When drug treatment is used, it should be as an adjunct to
psychosocial interventions. Medication should be avoided as the primary or sole treatment of
personality disorder.
When prescribing any medication, please consult the relevant generic guidance on monitoring
for adverse effects, maintaining a record of medication, prescribing off-license, and prescribing in
pregnancy and breastfeeding. In particular, be aware of guidance cautioning against the use of
Valproate in women of child-bearing age.
7.2 Medication for physical disorders
People with personality disorder are frequently prescribed medications for physical health
conditions. There is a complex interplay between physical health, mental health and the
medications used in the treatment of these conditions. Medications like some analgesics and
other sedating drugs can sometimes negatively impact on both mental health and general
functioning and it is recommended that regular holisitic review of the risk-benefit balance for the
patient occurs for all prescribed medications. This can be usefully carried out in liaison between
primary care, mental health services and other specialist services, for example pain
management services.
7.3 Medication for co-occurring mental illness
If there is co-occurring mental illness, this should be treated with medication as appropriate.
People with co-occurring personality disorder are often excluded from randomised controlled
trials for mental state disorders. This has an impact on the generalisibility of much of the
evidence base. In light of this, close monitoring of response and side effects is recommended as
people with personality disorder may experience atypical effects with psychotropic medication.
For example, increased emotional dysregulation, dysphoria and parasuicidal phenomena occur
not infrequently when SSRIs are prescribed to individuals with borderline personality disorder.
It is recommended that treatment for co-occurring mental illness takes into account personality
factors. If personality factors are not addressed as part of the overall treatment plan, progress
may be slower. Consideration should be given to prioritising treatment of personality factors
where appropriate, for example, when traits of rigidity and perfectionism predispose to recurrent
depressive episodes.
67

7.4 Medication for personality disorder
A single page summary and treatment algorithm can be found in the Appendix.
If prescribing is unavoidable, the specific prescribing principles detailed below should be
followed, ideally using a written prescribing agreement, a copy of which should be sent to the
patient, a copy to the GP, and a copy kept in the casenotes. This prescribing process is likely to
have more therapeutic benefit than the medication itself and is informed by the general principles
of management of personality disorder.
For understandable reasons, some people with personality disorder are keen for a “quick fix” to
their difficulties in the form of a medication. There can be resistance to any suggestion that
medication may not be helpful, especially when they may have experience of other people
experiencing benefit from psychotropic medication with other mental disorders. It is not hard to
understand why many people would prefer the relatively easy solution of taking a tablet versus a
lengthy and perhaps challenging psychosocial treatment. This position should be validated and if
a patient remains keen for a trial of medication, despite explanation of the lack of evidence,
effective alternatives and possible adverse effects, then the prescribing process below should be
used.
For some people, this prescribing process (which effectively functions as a series of behavioural
experiments) can be helpful in demonstrating that medication is of limited value in the treatment
of personality disorder. Patients may then be more likely to recognise the need to assume
greater responsibility in their own recovery and may begin to consider engaging more personally
demanding but potentially more effective psychosocial treatments.
Medication should be directed at specific symptoms or related symptom clusters rather than the
overall disorder. See Table 7.1 for guidance on choices of medication according to the higher
order domain to which the symptom belongs. This guidance is based upon the American
Psychiatric Association’s guideline for the treatment of patients with borderline personality
disorder (itself based upon earlier work by Soloff, 1998) and recommendations by Tyrer and
Bateman (2004). The guidance represents expert opinion and should be used in the context of
the extremely limited evidence base for benefit of drugs in the treatment of personality disorder.
A review of drug treatment in borderline personality disorder carried out by the Cochrane library
(Cochrane Library, 2010) describes mixed results from individual studies. It was unable to draw
firm conclusions in favour of benefit or harm and stated that “current findings of trials and this
review are not robust and can easily be changed by future research endeavours. In addition, the
studies may not adequately reflect several characteristics of clinical settings (among others,
patients’ characteristics and duration of interventions and observation periods).”
The NICE Guideline for the Treatment of Borderline Personality Disorder (NICE, 2009)
recommends that drug treatment should not be used “specifically for borderline personality
disorder or for the individual symptoms or behaviour associated with the disorder” and that
“antipsychotic drugs [should not be] used in the medium- or long-term treatment of borderline
personality disorder”. The NICE Guideline for the Treatment of Borderline Personality Disorder
suggests:
• considering “drug treatment in the overall treatment of comorbid conditions”
• cautiously considering “short-term use of sedative medication as part of the overall
treatment plan for people with borderline personality disorder in a crisis. . . [for] no longer
68

than one week”. When prescribing in these circumstances, the recommendation is to
choose a drug with a low side effect profile, low addictive properties, minimum potential
for misuse and relative safety in overdose, for example a sedating anti-histamine like
Hydroxyzine or Promethazine. Please note that sedative antihistamines are not licensed
for this purpose and informed consent should be obtained and documented (completion of
the Prescribing Agreement Form serves this purpose). Prescribe the lowest effective dose
and issue fewer tablets more frequently if there is a significant risk of overdose.
• reviewing “the treatment of those who do not have a diagnosed comorbid mental or
physical illness and who are currently being prescribed drugs…[aiming] to reduce and
stop unnecessary drug treatment”.
The NICE Guideline for the Treatment of Antisocial Personality Disorder (NICE, 2009)
recommend that “pharmacological interventions should not be routinely used for the treatment of
antisocial personality disorder or associated behaviours of aggression, anger and impulsivity”.
While evidence for the use of medications in personality disorder is scant overall, occasionally
patients do appear to gain individual benefit from specific drugs. In these cases the drug should
be kept under regular review at the lowest effective dose and stopped if benefit is not sustained.
Table 7.1 Guidance on choice of medication in personality disorder targeted by symptom cluster.
7.4.1 Managing polypharmacy
Polypharmacy is common in patients with personality disorder. Patients are frequently
prescribed a greater number of psychotropic medications in higher doses than many individuals
with severe mental illnesses like bipolar affective disorder and schizophrenia in which the
evidence base for use of medication is much stronger. This is often because of the distress in
which these patients present and an understandable desire on the part of the prescriber to “do
something”. Very often, short term medications become long term medications, with upward
creep of doses and new medications added. Sometimes there can be reluctance (from both
patient and prescriber) to stop medication despite any apparent benefit in case the medication is
Symptom Cluster First line drugchoices
Second line drugchoices
Third line drugchoices
Impulsive-behaviouraldyscontrol symptoms
Generic SSRI Olanzapine
Sodium Valproate
Carbamazepine
Low dose antipsychotic
Olanzapine
Sodium Valproate
Carbamazepine
Low dose antipsychoticAffective dysregulation Generic SSRI
or MirtazapineDifferent generic SSRIor Mirtazapine
Olanzapine
Sodium Valproate
Carbamazepine
Low dose antipsychoticCognitive-perceptual symptoms Low dose
antipsychoticDifferent low doseantipsychotic
No third linerecommendations
Interpersonal difficulties Drug treatment inappropriate for this symptom cluster
69

actually having some effect and its withdrawal leads to a deterioration. The end result is often a
patient on inappropriately high doses of unlicensed, often sedative, medication with significant
adverse effects in multiple domains. Impairments may involve the cognitive and motivational
domains crucial for most psychosocial treatments, and reduction in general functioning which
can negatively affect the person’s environment, interpersonal situation and mental state.
Regular review of medication is recommended for all patients. If polypharmacy is an issue, the
following approach to address the problem is recommended.
• Review each medication individually:
• How long the patient has been on the drug?
• Establish dose, frequency, compliance.
• Establish the patient’s view on the target or purpose of the drug - for example,
‘anxiety’.
• Ask the patient to self-rate the symptom or problem which the medication is being used
to treat — for example 8/10 anxiety.
• If the medication is effectively controlling the problem (for example, self-rated anxiety
1/10), continue prescription at the lowest effective dose. Keep under regular review
and stop if benefit is not sustained.
• If the medication is not effectively controlling the problem (for example, self-rated
anxiety 8/10), stop the drug. Some medications, such as benzodiazepines, may require
a relatively slow downward titration and appropriate guidelines should be followed, for
example those in the British National Formulary.
Aim to stop all ineffective medications as soon as is safely possible. A period of at least 3
months is advised before any further psychotropics are prescribed. Any further prescriptions
should be under the terms of the outlined prescribing agreement.
7.5 Prescribing Principles
7.5.1 Prior to starting treatment
• Agree target symptom with individual.
• Discuss treatment options, side-effects and usual time taken for drugs to exert any effect.
• Avoid drugs that are dangerous in overdose or can cause dependence. Prescribe limited
quantities of psychotropic medication during periods of high suicide risk.
• Discuss limits of efficacy and evidence base.
• Agree that the decision of which medication to take, and indeed the decision to take
medication at all, is the patient’s responsibility.
• Allow patient to make the choice of drug from the options given. Give a clear recom-
mendation if asked, but avoid persuading the patient.
• Agree how long the trial of medication will last. The trial period will typically be the same
length of time as for a licensed indication with similar symptoms. For example, an SSRI
prescribed off-license in borderline personality disorder for the symptom of dysphoria
should be given a trial of 4–6 weeks, which is the typical trial period for an SSRI in major
70
depressive disorder.
• Explain that if the patient stops taking the drug for any reason, no alternative drug will be
prescribed until the trial period has elapsed.
• Agree how symptom change will be objectively measured. There are no specific tools for
this purpose but improvement should be measurable in clearly operationalised terms. For
example, if an SSRI is prescribed in an attempt to modify self-cutting behaviour, a specific
target should be developed in collaboration with the patient before starting treatment. If
the target specified is: “a reduction in the number of episodes of self-cutting in a seven
day period”, then a baseline frequency is required against which to measure change. A
diary card or similar would clearly be useful here. Less objectively measurable symptoms
such as dysphoria can also be measured. This could be achieved by a simple ‘1 to 10’
self-rating of mood. Formal rating scales for depression are probably of little value for
measuring this symptom unless the patient is actually suffering with clinical depression as
opposed to dysphoria, because they measure the depressive syndrome rather than
individual symptoms. Tools such as the BEST and CORE can measure overall progress
but it is important to be mindful that any drug treatment should be targeted at a specific
symptom (or related symptom cluster) and not the entire disorder.
• Agree on a measure of improvement in the target symptom which will represent an
acceptable outcome for the patient. For example, a reduction in dysphoria from 8/10 to
4/10.
• The clinician and patient should then sign the prescribing agreement. This gives the
patient the opportunity to give their informed consent to treatment and gives the prescriber
written documentation to refer to at subsequent reviews. The prescribing agreement can
be found in the Appendix.
7.5.2 Having started treatment:
• Prescribe within safety limits; consider weekly scripts.
• Meet with the individual regularly to discuss response and side effects.
• After agreed trial period, stop the drug if patient experiences no improvement.
• If the patient decides for any reason to stop the medication before the agreed trial period
ends, no other drug should be prescribed until that period has elapsed. This should be
discussed with the patient before starting the drug and prior to signing the prescribing
agreement.
• At the end of the agreed period, review the self-recorded measure of the target symptom.
If the agreed goal is met, continue the medication and regularly review its effect on the
agreed treatment target. If the medication ceases to be effective it should be stopped.
• Change doses gradually as individuals with personality disorder frequently complain of
increased sensitivity to side effects and discontinuation effects.
• Regularly review prescribed medication and aim to stop any unnecessary or ineffective
treatments for either the personality disorder itself or any comorbidity.
• Aim to keep drug treatment at the lowest effective dose for the shortest duration.
71

References
American Psychiatric Association. (2001). Practice guideline for the treatment of patients with
borderline personality disorder. American Journal of Psychiatry, 1–52.
Cochrane Library (2010). Pharmacological interventions for borderline personality disorder.
http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005653.pu
b2/abstract 2
NICE. (2009). Antisocial Personality Disorder Treatment and Management. NICE Clinical
Guideline 77. 3
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78. 2
Soloff, P.(1998). Algorithms for pharmacological treatment of personality dimensions. Symptom
specific treatments for cognitive-perceptual, affective, and impulsive-behavioral
dysregulation. Bulletin of the Menninger Clinic, 62, 195–214.
Tyrer, P., & Bateman, A. (2004). Drug treatment of personality disorder. Advances in Psychiatric
Treatment, 10, 389–398.
72

8. Education and Awareness
8.1 Introduction
Education about personality disorder is of recognised benefit to those who suffer with these
conditions, members of their social networks, and the staff, agencies and services involved with
this patient group.
Personality disorder is common in the general population. People with personality disorder
frequently have contact with many different services and agencies including primary care,
general health, mental health, housing, social work, criminal justice and third sector services.
The difficulties with which people with personality disorder present may vary depending on the
agency or service involved. For example, an individual may present to the housing services as
someone with difficulty in maintaining a tenancy whereas the Emergency Department may view
the person’s primary problem as repeated overdoses. For social services, childcare and
parenting issues may be viewed as the principal problem, and so on.
The complexity associated with personality disorder means that patients with the condition
frequently pose significant challenges to the professionals working with them. Occasionally
professionals can find it hard to understand why individuals present as they do, and the
emotional responses of professionals to particular behaviours or patterns of behaviour can be
intense and sometimes unhelpful. Education with the aim of enhancing knowledge, attitudes
and skills can be of real value in helping professionals become more aware of the issues which
frequently accompany personality disorder. This includes factual knowledge about these
conditions, contributing factors, prognosis and treatment approaches. In turn, improved
knowledge and active self-reflection can contribute to more helpful attitudes and more
compassionate responses towards patients with these conditions.
This section deals only with education and awareness interventions for professionals. While no
less important, issues related to patient (and social network) education can be found in the
Psychosocial Interventions Section and Selfmanagement Section. In addition, psycho-
educational materials which may be of benefit to patients, social network members and
professionals can be found in the Appendix.
8.2 Education and awareness-raising resources
Until now, much of the education and awareness delivered by the Personality Disorder Service
has been on an ad-hoc basis. Educational sessions have been provided to many of the
disciplines, services and the agencies listed above, and in other settings. Sessions have usually
followed specific requests and been tailored according to particular needs. In some settings,
educational sessions have been co-delivered with service users. Service user involvement in
73

education and awareness-raising adds the patient’s unique experience of living with personality
disorder to the professional perspective.
The Personality Disorder Service educational programme is currently undergoing development,
including evaluation of the possibility of electronically available educational modules. Currently,
the main regular educational sessions occur four times per year. Each session covers a
different personality disorder-related subject and lasts for approximately 2 hours. The PDS
distributes dates and topics by email. Anyone with an interest in personality disorder is
welcome. As well as these regular sessions, the PDS service will consider any request for
education on subjects related to personality disorder.
8.3 Personality Disorder Integrated Care Pathway
This ICP itself aims to serve as a valuable educational tool. Each section summarises an
important topic in personality disorder and useful resources and links can be found throughout.
In addition, the publication of this document will be supported by an educational and awareness
raising program. The educational support aims to be broad in scope, including primary care,
general health, mental health, other public sector and third sector services.. This list is not
intended to be exclusive, and the PDS will endeavour to respond to requests for awareness-
raising of the PD-ICP document.
8.4 Scottish Personality Disorder Network (SPDN)
The NHS Highland PDS is actively involved with the SPDN. The SPDN was established by the
Scottish Government in 2006 to promote awareness of personality disorder and to provide a
forum to allow professionals, patients and members of their social networks to meet in order to
help progress work on personality disorder locally and nationally. The SPDN usually meets at
least three times a year in different locations around Scotland. This is to ensure that interested
individuals can access the Network. Conferences are open to service users, members of their
social networks and professionals.
74

9. ConsultationThe Personality Disorder Service (PDS) is currently developing its consultation function. The
PDS aims to provide a range of consultation modes including general recommendations on the
management and treatment of personality disorder, discussion of specific aspects of a clinical
case, focused supervision and consultation for professionals engaged in delivering general or
specific psychosocial treatments to individuals with personality disorder, full case consultation
and formal further opinions. The PDS welcomes requests for consultation.
Contact details
Personality Disorder Service
Psychotherapy Department
Greenfields House
New Craigs Hospital
Leachkin Road
Inverness
IV3 8NP
Telephone: 01463 253681
Personality Disorder Service Referral Form
75

76

10. Community Care
10.1 Introduction
Personality disorder is a common disorder affecting upwards of one in ten of the general popu-
lation. Of these people, around a quarter will be treatment-seeking, while about three quarters
while be treatment-resisting (will not seek treatment or will actively avoid treatment).
Most treatment of people with personality disorder occurs in the community. As with most
conditions, large numbers of people with milder forms of the disorder will be managed within
primary care, smaller numbers with more severe difficulties will be managed in secondary care
and a yet smaller number with the most severe difficulties will receive input from specialist
tertiary services. Even at the most severe end of the spectrum of difficulties, community
treatment is generally preferred to hospital treatment for the reasons outlined in the In-patient
Section.
General issues relating to care and treatment of personality disorder within Primary Care and
Community Mental Health Teams (CMHTs) are discussed in this section. Specific psychosocial
and pharmacological interventions are discussed in their respective sections.
10.2 Primary Care
People with personality disorder are heavy users of primary care services. Typically, around a
quarter of people in a general practice clinic fulfil the diagnostic criteria for personality disorder.
Although personality disorder may not be the given reason for attendance, the condition
appears to be associated with increased rates of other mental health and physical health
problems, substance use conditions, medically unexplained symptoms and frequent attendance
in primary care settings.
10.2.1 When to refer to mental health services
For patients already involved with mental health services, any existing care plan should be
followed except in exceptional circumstances. Care plans should be made easily available in
the casenotes or other patient information systems.
Patients who have no current involvement with mental health services and who are assessed as
needing the input of these services should be directed to the appropriate service according to
whether they represent an emergency or not.
Emergency referrals (those patients who require to be seen the same day for reasons of
significant risk) should generally be directed to the Mental Health Assessment Team (MHAT) at
New Craigs Hospital. MHAT can assess which treatment, including inpatient treatment is most
appropriate. GPs in the Inverness sector may also consider referring to Braeside Crisis and
Intensive Treatment Service. Braeside aims to provide an alternative to in-patient care for
patients with mental disorder who present a current significant risk to themselves or others.
Non-emergency referrals should be made to the sector Community Mental Health Team
(CMHT) via the single point of referral. Sometimes it can be difficult to establish if a
77

presentation is related to a mental state condition or a personality disorder (or both). In these
circumstances, referral to the CMHT for clarification of diagnosis is reasonable. Other
situations when referral to the CMHT might be considered include when the patient is unable
to be managed solely in primary care because of issues of severity, complexity, co-morbidity
or risk; or when the person’s personality appears to be acting as a vulnerability factor to
mental illness.
Just as it would be inappropriate for all people with depression to be referred to secondary
care mental health services, so it would also be inappropriate for all people with personality
disorder to be referred; matched care should be the aim. Regular communication and
discussion between primary care and community mental health services is likely to be of
benefit in maintaining the referral threshold at the most appropriate level.
Useful referral information includes:
• whether the general criteria for personality disorder are met, with some description of
severity
• an outline of the difficulties experienced by the patient in the four main domains:
cognitive-perceptual
affective
interpersonal
o relationship with self including sense of self
o interpersonal relationships
o relationship with society
behavioural/impulse control (including self-harm and suicidal behaviour)
• concurrent physical and mental health conditions
• appropriate risk assessment, perhaps using a structured tool such as STORM
10.2.2 General Principles
Whether a person has mental health services involvment or not, they are likely to continue to
require the input of primary care to some degree. Every contact should be informed by the
concepts and principles outlined in the General Principles Section:
• Collaboration
This applies equally to collaboration with the patient and collaboration with the wider
team. Ensure that everyone is clear about their roles and responsibilities, and the
treatment frame. The importance of personal responsibility and self-management should
be emphasised. The Care Program Approach (CPA) can be very valuable in helping
clarify roles and promote consistency. CPA meetings provide a valuable opportunity for
professionals and the patient to assess needs and risk and develop an appropriate care
plan collaboratively. While it is recommended that patients at the more severe end of the
personality disorder spectrum who have multi-disciplinary or multi-agency involvement
should be managed under the CPA, any clear written care plan shared between all
relevant professionals and the patient is likely to improve care delivery.
• Consistency
Limiting the number of General Practitioners a patient sees to one or two in order to allow
78
a good working relationship to develop can be of value in promoting collaboration and
consistency.
If a Care Program Approach (CPA) care plan or other written care plan is in existence,
then it is important that clinicians (including out of hours staff) are aware and able to
easily access the information. Inconsistency, for whatever reason, can lead to significant
anxiety and dysregulation. A shared plan can make it less difficult to appropriately
maintain limits in the face of pressure. Consider placing any care plan in “special notes”
or similar.
Often GPs, working within tight clinic schedules or in out-of-hours settings, come under
significant pressure from patients in distress to “do something”. This can sometimes
result in unhelpful reactive prescribing. It is important to remember that standing by a
decision not to prescribe, while validating the patient’s desire for the situation to change
and explaining the rationale of the care plan, is in fact often “doing something”
therapeutic. If medication is felt to be appropriate, it is recommended that a written
prescribing agreement is used. See Medication Section for further details.
• Motivation
Some suggested strategies for increasing motivation to change can be found in General
Principles Section.
• Validation
Validation involves active listening and observation, accurate reflection of the patient’s
emotions, thoughts and behaviours, and direct validation (the explicit acknowledgement
of a thought, emotion or behaviour as valid and legitimate for that person, both
understandable in the current context and in the context of previous experiences). It is
important to recognise that validation does not necessarily imply approval.
• Promotion of self-management
Supporting self-management across health conditions is a key part of the role of primary
care. Further information on how the concept relates to personality disorder can be found
in the Self-management Section.
Promoting self-knowledge and self-reflection are a component of self-management which
is particularly important in personality disorder. This process may involve provision of
general information about the condition but should also comprise more individual-specific
knowledge gained by a process of self-reflection. Wherever possible, consider
highlighting the importance of attempting to understand the mental state of oneself and
others and how thoughts and emotions influence behaviour. For the clinician, a “not
knowing” or gently curious style which encourages the patient to reflect on the thoughts,
emotions and behaviours of themselves and others is usually more useful than simply
providing patients with “the answers”.
10.3 Community Mental Health Teams
People with personality disorder make up a significant component of the clinical load of CMHTs.
This will include people with a primary problem of personality disorder and people with other
mental disorders whose treatment may be made more challenging by coexisting personality
disorder or whose personality functions as a contributing factor to other mental disorders. Most
people with personality disorder in mental health services receive their treatment from generalist
rather than specialist services and this is likely always to be the case. The value of a
79

multidisciplinary team approach in treating personality disorder cannot be over-estimated and
increasing evidence is emerging which suggests that generalist multi-disciplinary care based
upon a shared psychologically-informed care plan can be as effective as specific psychological
treatments for personality disorder. In some instances it may be clinically indicated to limit the
number of professionals involved with a patient at any one time. In all cases, it is of real
importance that someone in the team functions as a caseholder, keyworker or point of contact,
and maintains an overview of the persons care and treatment, ideally for the duration of their
involvement with the team.
Over the past decade or so, documents such as the report “Personality Disorder in Scotland:
Demanding Patients or Deserving People” (Scottish Executive Mental Health Division and
Centre for Change and Innovation, 2004) have emphasised that no one should be excluded
from services solely on the basis of a diagnosis of personality disorder. While such exclusion did
unfortunately happen in the past, this practice is now regarded as absolutely unacceptable, not
least because of the ever-increasing evidence base of effective treatments for personality
disorder.
10.3.1 Role of the CMHT in the treatment of Personality Disorder
At a minimum, CMHTs should be able to provide assessment, diagnosis and formulation, offer a
variety of treatment strategies based upon the formulation, and signpost to other services as
appropriate.
10.3.1.1 Assessment, Diagnosis and Formulation
CMHTs should be able to provide an assessment, diagnosis and formulation function as
outlined in the Assessment, Diagnosis and Formulation Section of this ICP.
While most clinicians are well placed to describe and discuss personality traits and symptoms, a
formal diagnosis of personality disorder should usually only be made by a senior psychiatrist.
During the diagnosis process, is important that the patient receives balanced, honest feedback
in a form which they can understand. Personal strengths should be emphasised while
acknowledging difficulties and the importance of personal responsibility in the recovery process.
Explanation of treatment options and the relatively positive prognosis should be given. For
example, patients are often heartened to hear that studies suggest that around three quarters of
those meeting the diagnostic criteria for borderline personality disorder no longer do so after a
period of six years.
While many patients describe a sense of relief on receiving a diagnosis or formulation that
makes sense of their difficulties, many others find receiving a diagnosis of personality disorder
an upsetting experience. This is at least in part due to myths and misinformation perpetuated by
the media, and the associated stigma. Psychiatrists should consider giving verbal and written
information on personality disorder when discussing the diagnosis with the patient and asking
them to return with any questions once they have reflected on the information. It is also
reasonable to advise patients about the large amount of misleading information regarding
personality disorder on the internet, and recommend that they exercise caution in what they
read. Some useful information leaflets are available in the Appendix.
Occasionally, patients can have difficulty with the term “personality disorder”. If this is the case, it
may be helpful to explain that the term simply serves as short hand to describe sets of
80
symptoms and traits which typically occur together, and has the principle purpose of ensuring
delivery of the treatment that is best matched to the patient’s problems. Some patients with
borderline personality disorder find the reframing of their difficulties as “emotional intensity
disorder” (which is the terminology used in the STEPPS program) to be more acceptable. In any
case, the terminology is much less important than the clinician and patient agreeing on the
presenting features.
Assessment should aim to establish diagnosis and produce a formulation upon which an
individual’s treatment plan should be based. Particularly important components of the
assessment in guiding treatment planning include:
• phase of treatment
• symptoms
• personality traits
• needs assessment
• risk assessment
• environmental context
§1 Phase of treatment
Most commonly, patients will be referred to a CMHT needing input at phase 1 or 2. See the
General Principles Section for a more detailed description of phases of treatment.
§2 Symptoms
Symptoms occur as a result of maladaptation of the personality to the environment. It can be
helpful to think in terms of four broad headings:
• cognitive-perceptual (for example, excessive suspiciousness)
• affective (for example, emotional dysregulation and harmful anger)
• interpersonal
◦ relationship with self including sense of self
◦ interpersonal relationships
◦ relationship with society
• behavioural/impulse control (including self-harm and suicidal behaviour)
§3 Personality Traits
A personality trait or variable is a complex structure which represents a basic building block of
personality. In any given individual, genetic factors and environmental factors transact with each
other to form a complex biopsychological system which produces observable trait-based
behaviour. This biopsychological system can be described in terms of both biological processes
and psychological processes. Essentially, a personality trait represents a disposition to behave
in a particular way.
The term “trait” is also sometimes used to refer to individual features of specific personality
disorders, especially when the full diagnostic criteria are not met. For example, someone
meeting four of the five criteria needed for a diagnosis of borderline personality disorder may be
81

referred to as having “borderline traits”.
Some traits which are of particular importance in personality disorder are listed below with brief
descriptions of associated behaviours. Traits can be usefully organised into four main higher
order trait domains: dyregulated, detached, dissocial, and compulsive. There may be some
overlap between some traits and it is worth noting that some of the names used for particular
traits may have different meanings when used in other contexts. The traits below are drawn
from the Personality Assessment Schedule (Tyrer, 2000), and other sources may label
particular traits differently.
It is important to remember that no personality trait is inherently negative. Many traits can be
described by more than one term, some with negative connotations and some with positive
connotations. For example: impulsive versus spontaneous; stubborn versus determined; aloof
versus self-contained and so on. Problems arise when a person’s personality traits are
maladapted to their environment. With more extreme expressions of particular traits,
maladaption is likely in a greater number of environments leading to greater severity of
personality disturbance.
Dysregulated (Internalising) Domain
Pessimism — holds a pessimistic outlook on life.
Worthlessness — feelings of inferiority
Lability — mood instability
Anxiousness — anxiety-proneness
Shyness — shyness and lack of self-confidence
Sensitivity — personal sensitivity and tendency to self-reference
Vulnerability — experiences excessive emotional distress when faced with adversity
Childishness — excessive self-centeredness
Resourcelessness — tendency to give up when faced with adversity
Dependence — excessive reliance on others for advice and reassurance
Submissiveness — limited ability to express own views or stand up for
oneself
Hypochondriasis — over-concern about illness and health
Detached (Schizoid/inhibited) Domain
Suspiciousness — excessive mistrust of others
Introspection — prone to rumination and fantasy
Aloofness — detachment and lack of interest in other people
Eccentricity — oddness in behaviour and attitudes; unwilling or unable to
conform
Dissocial (Externalising) Domain
Optimism — unrealistically optimistic, over-confident, excessively self-important
82

Irritability — excessively irritable
Impulsiveness — excessive impulsiveness
Aggression — excessive levels of aggression
Callousness — indifferent to the feelings of others
Irresponsibility — indifferent to the consequences of one’s behaviour
Compulsive (Anankastic) Domain
Conscientiousness — overly fussy, perfectionistic
Rigidity — inflexibility and difficulty adjusting to new situations
§4 Needs Assessment
While it will certainly not be necessary to provide the CPA for every patient referred to the
CMHT, the Care Programme Approach Needs Assessment Checklist provides a comprehensive
systematic guide to needs assessment. Common areas of need for people with personality
disorder, from which specific treatment goals can be identified, include:
• medication including:
polypharmacy
compliance issues
• concurrent mental health conditions including:
mood and anxiety disorders
substance misuse disorders
• physical health including:
not accessing appropriate care for medical conditions
reduced self-care including suboptimal management of chronic medical conditions
• emotional support including:
crisis resolution
containment strategies
• accommodation including:
difficulty maintaining a tenancy
• social/interpersonal situation including:
lack of interpersonal contacts
lack of leisure time activities
• employment, education or other meaningful, structured use of time
• financial including
debt problems
benefits issues
83

financial management difficulties
• dependent children/ other dependents including
difficulties managing childcare tasks
§5 Risk Assessment
Each individual risk should be specified in the care plan with indicators of an increase in risk
identified. Current level of risk of each specific situation occurring should be estimated as far as
possible. A clear risk management plan should be in place for each identified risk, with roles and
responsibilities made explicit. Consideration should be given to the use of a recognised tool such
as STORM in assessing the particular risk of suicide. The overall aim is to minimise the risk of
harm to the patient and those around them, while always promoting the personal responsibility
so vital for recovery.
The CPA documentation provides a useful structure for risk assessment and risk management.
§6 Environmental Context
This includes the interpersonal and social context which should become apparent during
assessment.
10.3.1.2 Treatment and Management
Evidence is emerging that structured multidisciplinary treatment based upon a sound
formulation can be of equal benefit to specific psychotherapies in the treatment of personality
disorder. CMHTs are well placed to enable the continuity of care which is so important in
maintaining consistency in the treatment of personality disorder, and to oversee the treatment
plan over the longer term. As well as this more general approach, all CMHTs should be
regularly delivering STEPPS groups for patients with borderline personality disorder and similar
difficulties (see Psychosocial Section). CMHTs can usefully deliver focused preparatory work for
STEPPS groups in the period between referral to the team and the start of the next STEPPS
group, for example anxiety management strategies for people who experience anxiety in group
settings.
Aside from treatment directed towards personality disorder itself, community teams play a vital
role in wider treatment and management including treatment of comorbidity, management and
monitoring of medication and environmental management. Any treatment offered by the team
should be focused and time-limited (although perhaps of long duration). At any given time, both
the clinician and the patient should be absolutely clear about the nature and purpose of the
work they are undertaking. Open-ended, unstructured contact should be avoided as this may
encourage unhelpful dependence. If a patient is unwilling to engage in their treatment plan,
motivation work may be indicated. However, sometimes, despite motivational strategies, a
patient may still decide that they do not wish to engage in treatment at that time. In these cases,
it may be less harmful to discharge a patient rather than engage in unfocused, unstructured,
dependence-inducing contact.
§1 What constitutes treatment of personality disorder within a CMHT?
For an intervention to be considered a treatment for personality disorder, the primary goal must
84

be to improve the difficulties associated with the patient’s personality disorder. A distinction can
be drawn between treatments aimed at a patient “overcoming” their personality difficulties by
seeking to initiate change in the patient, and treatment or interventions which “take account” of
the personality difficulties in order to minimise the impact of the personality disorder on the
patient and those around them. Examples of the former include psychological treatments like
DBT and STEPPS and any skills reinforcement or skills generalisation carried out by the CMHT.
Examples of the latter include environmental management (interventions aiming to improve
adaptive fit between the person and their environment), interventions aimed at changing the
social or interpersonal environment (family interventions etc) and adaptations to standard
interventions for another condition (changing the treatment approach for major depressive
disorder in someone with a concurrent personality disorder).
§2 Care planning
The following points are important to consider in collaboratively developing a care plan:
• The jointly developed care plan should be based on the individual formulation and cover
personality disorder and any co-occurring disorders.
• The patient should be supported to develop a crisis self-management plan as early as
possible in the treatment episode.
• A crisis care plan identifying how a team aims to respond to a crisis should be made
explicit
• The phase of treatment should be clearly identified.
• Risk management plans should be explicit.
• Care Programme Approach may by useful in helping to manage complexity or severity. See
http://intranet.nhsh.scot.nhs.uk/org/dhs/mhandlearningdisabilities/cpa/Page/
Default.aspx.
• Quality assurance including appropriate supervision.
• Social network involvement where appropriate
§3 Co-occurring disorders
Personality disorder not only causes difficulties in its own right, but often functions as a
vulnerability factor for other mental health problems which can frequently be more challenging
to treat in the presence of personality disorder. Consequently, due attention should be paid to
any personality difficulties when there are co-occurring mental health problems. It is rarely
adequate to simply treat mental state disorders using standard approaches in such situations.
§4 Crisis planning
Crisis planning is of particular importance in personality disorder and should be a task
considered very early in any treatment process. When people with personality disorder
experience intense emotions, the ability to think clearly is reduced even more than it would be
for other people. Hence a crisis self-management plan, with options and contacts for dealing
with a crisis situation clearly listed, can be invaluable. Although a crisis may be produced in
collaboration with a clinician, it necessarily remains the patient’s document. However, clearly it
is likely to be beneficial for the patient to share copies with relevant people. Examples of
template crisis self-management plans can be found in the Appendix.
85

§5 Phase of treatment
Identification of the phase of treatment is a primary task. This section should be read in
conjunction with the General Principles Section.
1 Stabilisation (or MAKING STABLE). The focus here is on the present:
a Safety and
b Containment: The main aims of the first two parts of the stabilisation phase are
management of symptoms and crises. Interventions should be kept simple and
focused with the goal of returning the patient to the previous level of functioning as
soon as possible. It is important to avoid attempting to achieve too much during the
safety and containment phases
of treatment. See Crisis Management Section.
c Regulation and control: Once acute behavioural dysregulation has stabilised (even
temporarily), work can begin on the third part of the stabilisation phase. The main
aims are to promote self-management of impulsivity, self-harming behaviour and
emotions.
Useful strategies include behavioural analysis which can help the person to identify
the antecedents and reinforcing consequences of unhelpful behaviours. Distancing,
mindfulness, emotion regulation, distress tolerance and interpersonal effective skills
and strategies are likely to be of value in identifying solutions. These generic
approaches do not “belong” to any particular psychosocial intervention. However,
while it is entirely reasonable for these skills to be taught on an individual basis
outwith specific psychosocial approaches like STEPPS or DBT, it is important that
the clinician and patient are clear that what is being delivered in such a situation
does not constitute a DBT or STEPPS intervention.
A crisis self-management plan can prove very valuable in maintaining stabilisation
and preventing dysregulation by providing a clear set of helpful options when a
patient’s capacity to think clearly is reduced.
STEPPS and DBT are essentially stabilisation treatments which can be considered as
adjunctive to standard community psychiatric care (see Psychosocial Intervention Section). If
a patient in DBT or STEPPS treatment has contact with a CMHT clinician, reinforcement and
generalisation of skills represents a useful focus for therapeutic work. The responsibility
should rest with the patient to collaborate with the CMHT clinician in such a way that
reinforcement and generalisation occurs. This may include keeping the CMHT clinician up to
date on which skills are currently being taught and examples of how they are applying them
in their daily lives. While the concept of a reinforcer is built into STEPPS, this concept is not
a core concept of DBT. However, if a CMHT clinician has concerns that a patient in DBT is
not using their CMHT time to effectively reinforce and generalise skills, then it would be
reasonable to alert the DBT therapist, with the patient’s knowledge. Solutions could then be
found within DBT individual therapy.
DBT can be considered for patients with severe borderline personality disorder and recent,
potentially lethal parasuicidal behaviour or emergency hospitalisation who are also on the
Care Programme Approach.
86

STEPPS skills training groups run within each of the CMHTs and this intervention should be
considered for moderate borderline personality disorder or borderline traits (the terminology
used within the STEPPS program is “emotional intensity disorder”). Ideally, every participant
should have a reinforcement team. This is ideally composed of members of the social
network and a health professional (CPN, GP, support worker etc). The reinforcers need not
have in-depth knowledge of STEPPS but serve to help consolidation and generalisation of
skills. The health professional reinforcer can support the participant to complete the weekly
homework. Other ways of delivering reinforcement including by telephone or in small groups
have also proven effective. Borderline problems form a continuum of severity and while
benefit is likely to be greater if a patient has a full reinforcement team, service-based
evidence suggests that a health professional reinforcer is not an absolute requirement,
although it is certainly preferable.
2 Exploration and change (or MAKING SENSE). The focus here is on the past:
This phase can involve dealing with the effects of trauma and dissociation; treating self and
interpersonal problems; and treating maladaptive traits.
Post-traumatic stress disorder can be treated via specific psychosocial interventions such as
EMDR or trauma-focused CBT, (see Psychosocial Interventions Section).
However, for less severe presentations, psychoeducation and self-directed exposure may be
of value. Dissociation is likely to benefit from general improvement in emotion regulation but
the patient may also benefit from learning grounding strategies.
Intrapersonal (self) and interpersonal problems often relate to maladaptive schemas. These
can be addressed through formal psychological interventions or by within general clinical
contact by supporting self-reflection, identification of long-standing patterns of thinking and
behaviour, and introduction of more adaptive patterns. For example, it might be gently
brought to a patient’s attention that they have a pattern of negatively interpreting neutral
comments, becoming angry and breaking off relationships. Clearly, this kind of work can very
naturally take place within general clinical contact and does not need to be limited to specific
psychotherapy settings.
Behavioural strategies which may be useful include challenging behavioural avoidance, en-
vironmental management strategies (guided by needs assessment), behavioural rehearsal
and role play.
No personality trait is intrinsically maladaptive. Maladaptation occurs when the behaviours
through which the trait is expressed interact with the environment to prove unhelpful. Some
traits can be relatively plastic and amenable to some change but others are less so. In case
of less malleable traits, the task is to modulate the trait as far as possible but also to help
modify the social and environmental context so that adaptive fit is improved. In many
situations, it can be helpful to view traits as relatively stable characteristics which the patient
needs to learn to use constructively.
• Increase acceptance and tolerance of the trait
Many (but certainly not all) people with personality disorder can be intolerant of their own
basic traits in contrast to most non-personality disordered individuals who are usually
reasonably comfortable with their traits, even those which they would like to change.
Related negative self-judgements and self-invalidation can have markedly detrimental
effects in terms of self-view, emotional responses and unhelpful behaviours used to change
intolerable emotional states. Mindfulness-based approaches can be helpful in increasing
87
acceptance of traits.
Psycho-education may help reduce internal conflict and increase self-acceptance.
Explanation that traits are to a significant extent biologically determined can help people
assume ownership of their traits, whereas emphasising the role of environmental influence
on traits can help the patient understand that it is possible, within limits, to change the way
traits are expressed. Another useful strategy is to encourage patients to identify ways in
which their traits might be beneficial if the fit with the environment was more adaptive. A
good example is the trait of conscientiousness. . Clearly, moderate levels of
conscientiousness, attention to detail and orderliness would be regarded as desirable by
most people. The realisation that traits are only maladaptive when they are expressed in
unhelpful or inflexible ways can facilitate change by helping the person see that they do not
need to change a fundamental part of themselves but rather more specific aspects of
behaviour related to the trait.
• Reduce trait expression
For people at the extreme end of a trait distribution, the threshold for interpreting situations
as relevant to the trait is low. Cognitive and behavioural strategies can be of value here in
helping to restructure the way situations are perceived so that the tendency to see
situations as relevant to a given trait is reduced. For example, the core beliefs and
assumptions that are typical for people with high levels of anxiousness can be identified
and challenged cognitively and via behavioural experiment. This may modify a tendency to
over-estimate the risk associated with particular situations.
Increasing behavioural alternatives can also be a useful strategy. For example, someone
with high levels of submissiveness can modify trait expression by learning assertiveness
skills and putting new, more assertive behaviours into practice. Similarly, teaching effective
relaxation skills can provide incompatible behavioural alternatives to becoming anxious for
people with high anxiousness levels.
People with high levels of anxiousness and emotional lability traits could usefully attempt to
substitute the unhelpful, trait-amplifying behaviours of rumination and catastrophisation with
healthier, trait-reducing behaviours of problem solving, distraction and self-soothing.
•Promote more adaptive trait-based behaviour
The goal here is not to reduce trait expression but to replace the maladaptive behaviours
associated with the trait with more adaptive behaviours. For example someone with high
levels of stimulus-seeking may engage in risky sexual behaviour, become involved in
fights and misuse substances. More adaptive replacement behaviours could include, for
example, high-risk sports.
•Promote the selection and creation of environments compatible with the adaptive
expression of problematic traits
This strategy is about improving the goodness of fit between the person and the
environment by modifying the environment rather than the traits. For example, someone
with high levels of social avoidance may function poorly in a busy sales job, but may do
very well in a relatively solitary occupation such as a long distance lorry driver. Similarly, a
person with high levels of compulsivity may do very well in an administrative job which
requires methodical attention to detail but do less well in a less ordered work environment.
Similar considerations apply to accommodation, leisure time activities and the
interpersonal environment.
3 Integration and synthesis (or MAKING CONNECTIONS). The focus here is on the
88
future:
The key difference with this phase, with a primary focus on the future, is not so much
about changing existing psychological and interpersonal structures and processes as
putting new ones in place. The aim is to promote a more integrated sense of self and a
healthier interpersonal environment — this may include development of new leisure
activities, occupational or educational activities, together with new roles and
relationships. A wide range of activities can help with this process of developing more
stable and healthy representations of the self and others by promoting new roles,
relationships and responsibilities. The role of the CMHT more likely to be in supporting
this process rather than in providing the activities.
§6 Care Programme Approach Where there are issues of particular complexity or severity,
consideration should be given to using the Care Programme Approach or similar approach or
process which supports the aims listed below:
• Clarity about roles and responsibilities
• Improved communication and reduced “splitting”
• Regular needs assessment and planning
• Regular risk assessment and planning
• Allowing for the care team, rather than one individual clinician to support the patient to
take positive, clinically-indicated risks. This helps avoid scenarios where one clinician is
overly risk-averse to the detriment of the patient by ensuring that clinical decisions are
taken in a well-reasoned way by a multidisciplinary team.
• Enabling managed transition from one phase of treatment to another and ensuring that all
involved are aware of the current treatment phase
• Influencing the interpersonal environment (including the CMHT) to minimise the impact of
personality disorder. For example, mental health services can sometimes represent most
or all of a patient’s interpersonal contacts. In these cases, the balance between providing
support without fostering dependency becomes very important.
• Influencing nature and frequency of contact between patients and other services and
agencies with a view to gains in some of the areas described in the needs assessment.
This might include involving agencies such as housing in an attempt to help stabilise the
environment.
• Highlighting which interventions are helpful at which times and, conversely, which are
not.
10.3.1.3 Risk management
Many patients with personality disorder carry significant risk issues and a degree of anxiety
can be experienced by patients, relatives and professionals as a result. However, elimination
of risk is impossible and working in a way which tries to eliminate all risk is often harmful.
Clinically indicated positive risk taking with the aim of increasing personal responsibility and
development of skills is a key part of the treatment of personality disorder. Unless there is a
compelling reason to do otherwise (for example, co-occurring severe mental state disorder), it
is important at all times to treat a patient with personality disorder as a competent adult, with
89
capacity to make their own choices and responsible for their own behaviour. Although the
clinician is responsible for carrying out clinical practice at a reasonable standard of care, the
patient is ultimately responsible for their own behaviour. This understanding is necessary to
enable the collaboration between the team and the patient which is necessary for recovery.
At times, patients may pose a risk to other people. Staff should remain aware of what
constitutes unacceptable behaviour, taking appropriate action as per NHS Highland policy if
such behaviour occurs. If the unacceptable behaviour constitutes criminal behaviour such as
displays of aggression or the obstruction of health care workers in the legimate course of their
duties, consideration should be given to involving the police rather than treating law-breaking
as a health issue in the first instance. The importance of maintaining a safe treatment frame is
paramount. Clinical experience suggests that if external behavioural modifiers such as the
ability to access police and criminal justice services are inappropriately removed, then clinical,
behavioural and functional deterioration is likely. An individual is unlikely to be harmed by
appropriately maintaining a limit whereas they are unlikely to be helped by inappropriately
ignoring a limit.
Multidisciplinary care planning means that the team jointly accepts any risk associated with a
patient, rather than a single clinician. The Care Programme Approach can help formalise risk
assessment and management plans and identify roles and responsibilities clearly. At times it
may be helpful to document if a person has a chronically raised risk of completed suicide (for
example in situations where a history of parasuicidal behaviour is present), which treatments
have been offered and what has been helpful, unhelpful or harmful.
It is important to distinguish between chronic and acute risk of suicide. Acute risk increase oftenoccurs in the presence of increased impulsivity or intent.
Important factors to consider in reviewing an adverse event are:
• Was there a foreseeable risk? Appropriate assessment and documentation of risk is
crucial.
• Was there a reasonable response? Any decision should be well reasoned, come from a
caring, therapeutic position and have a documented cost-benefit analysis. This allows for
clinically indicated (but sometimes superficially counterintuitive) responses. For example,
not admitting someone with potentially lethal self-harming behaviour to hospital.
• Was there a reasonable standard of practice? Quality of practice should be assured
with regular supervision and communication with the rest of the team. Relevant guidance
should be followed and reasons documented if it is not. Documentation should be of a
reasonable standard.
10.3.1.4 Supervision
Appropriate supervision is important for clinicians providing treatment for individuals with
personality disorder. Peer supervision, discussion within multidisciplinary team meetings, time
within usual clinical supervision and specific supervision may all be valuable according to the
nature, severity and complexity of the situation. The Personality Disorder Service is available for
consultation as appropriate.
10.3.1.5 Social Network Involvement
The issue of carer involvement in the treatment of personality disorder is a contentious one.
90

There is even some controversy over the term carer itself inasmuch as it is deemed by some to
be an invalidating term which moves the focus from self-management. Bearing that in mind, the
term “social network” is used here.
It is recommended that consideration of individual circumstances is given in relation to social
network involvement. Some patients will be very keen to avoid such involvement for a variety of
reasons and this should always be respected. However, involvement of social supports can
sometimes be helpful in modifying the interpersonal environment. If the decision is made to
involve social supports, education about personality disorder and how it can present can be
helpful to all concerned.
91

References
Appleby, L., et al. (2000). An educational intervention for front-line health professionals in the
assessment and management of suicidal patients (The STORM Project). Psychological
Medicine, 30(4), 805–812. 2, 14
Bateman, A., & Krawitz, R. (2013). Borderline Personality Disorder—An evidence-based guide
for mental health professionals. Oxford.
Blum, N., et al. (2008). Systems training for emotional predictability and problem solving
(STEPPS) for outpatients with borderline personality disorder: A randomized controlled
trial and 1-year follow-up. American Journal of Psychiatry, 165, 468–478.
Davidson, K. (2008). Cognitive Therapy for Personality Disorders. Routledge.
Division, S. E. M. H., for Change, C., & Innovation. (2004). Personality Disorder in Scotland:
Demanding Patients or Deserving People?
Linehan, M. (1993). Cognitive-Behavioural Treatment of Borderline Personality Disorder.
Guilford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
Murphy, M., & McVey, D. (Eds.). (2010). Treating Personality Disorder. Routledge. National
Institute for Mental Health in England. (2003). Personality Disorder: No longer a diagnosis of
exclusion.
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley.
Tyrer, P. ed. (2000). Personality Assessment Schedule. In Personality Disorders: Diagnosis,
Management and Course (pp. 133–159). Butterworth Heinemann.
92

11. Personality Disorder Service
The NHS Highland Personality Disorder Service (PDS) is a specialist outpatient service for NHS
Highland. The PDS offers consultation, assessment and specific psychosocial interventions. It
does not currently offer a case management service.
11.1 Services offered by the PDS
The main services offered by the PDS are:
11.1.1 Specialist Assessment and Treatment Recommendations
In order to ensure that patients receive the most appropriate treatment recommendations, the
PDS uses a standardised assessment to produce a formulation and a phase-based treatment
plan. The assessment includes current symptoms, personality traits, detailed background
history (including trauma history) and mental state examination. The information is gathered
from various sources including patient history, case-records, informant histories from
professionals and social network members and formal structured assessment tools. The main
purpose of the standardised assessment is to allow the collaborative development of a
formulation of the relevant biological, psychological and social factors into a description of the
patient’s life and personality which helps contextualise current problems and symptoms and
identify which problems, themes and goals will be the focus of treatment. Usually, 5 to 6 hours
are spent face-to-face with the patient. In addition, time is spent reviewing notes, speaking with
informants, and constructing the formulation and treatment plan. The assessment, formulation
and treatment recommendations are then discussed with the patient. This process usually takes
around 8 weeks, at the end of which time a detailed assessment letter, formulation and
treatment recommendations are sent to the referrer, with copies to all members of the care
team and the patient. It is recommended that this documentation is kept at the front of the
psychiatric casenotes in the “Important Information” section. It is hoped that the formulation and
treatment plan generated by the assessment will usefully inform future clinical contacts and care
planning. Best available evidence suggests that standard psychiatric care organised by a
psychologically-informed formulation can deliver benefit roughly equivalent to specific
psychosocial interventions such as DBT.
11.1.2 Dialectical Behaviour Therapy (DBT)
This is a primarily Phase 1 (stabilisation) intervention for patients with severe borderline
personality disorder. DBT is an intensive psychosocial intervention largely based on cognitive-
behavioural principles. It comprises a weekly skills training group, concurrent weekly individual
psychotherapy and weekly peer supervision for all therapists. The treatment usually lasts six
months to one year.
For patients with co-occurring post traumatic stress disorder (PTSD), the DBT Prolonged
Exposure protocol (DBT-PE) may be of benefit. This Phase 2 trauma reprocessing intervention
is delivered within the individual component of DBT treatment and bears many similarities to the
standard prolonged exposure approach (PE) for PTSD uncomplicated with borderline personality
disorder. DBT-PE can only be delivered to patients as part of an overall DBT treatment and not
93
as a stand-alone intervention.
DBT is an intensive intervention for patients with severe and complex borderline personality
disorder. Therefore referrers should only consider DBT if STEPPS or other secondary care
approaches are inappropriate for reasons of complexity or severity. To ensure that a holisitic
approach is taken to each patient’s care and treatment needs, to allow for effective structuring of
the environment, and to optimise communication and collaboration between the patient and the
services involved, patients in DBT are required to be on the Care Program Approach.
DBT can be offered only when clinically indicated by reason of severity and cannot be offered
solely because of local lack of availability of other better matched, less intensive options.
11.1.3 Coping and Succeeding (CAS) Day Service
The CAS (Coping and Succeeding) Day Service for people with personality disorder is a
community-based service which takes place each Friday from 0930 to 1530 at Rowans, New
Craigs Hospital. The usual length of treatment is 36 weeks. CAS has been developed in
partnership with service users along Recovery principles and represents a co-produced service.
The service is primarily directed at helping a person enhance interpersonal and social
connections in order to help them build a life away from mental health services. This process
usually has benefits for self-image. CAS has a primary focus on Phase 3 (integration) and, to a
lesser extent, Phase 2 (exploration and change). It is not an intervention with an emphasis on
Phase 1 (stabilisation). Other interventions such as DBT or STEPPS are more appropriate for
stabilisation of harmful behaviours. Furthermore, patients with post-traumatic features are likely
to benefit from specific trauma work (Phase 2) before making best use of CAS.
The CAS Day Service includes elements of structured group work, self-directed time and social
time. Broad themes covered in the core groups include promotion of physical health and well-
being; living skills; self-management; and vocational rehabilitation. These themes are addressed
by providing direct information and education; enabling direct introduction to new
activities/behaviours; and making and highlighting links between people and services. In the
spirit of co-production, participants play the major role in planning and organising the content of
the group activities and the day to day running of the service. Participants develop and work
towards their own goals in the interpersonal, occupational, recreational and educational
domains. The overall aims include promotion of self-management and planning for a worthwhile
life without mental health services.
The service is not only for individuals with borderline personality disorder, but is for any patient
who meets the general criteria for personality disorder or whose personality disorder is in early
remission. Potential CAS members must be ready to make changes. CAS would not be suitable
for people who do not meet the general diagnostic criteria for personality disorder; people with
current risk issues which preclude safe placement in a community setting (for example, people
who present a significant risk of violence to others or a significant risk of harming themselves);
or people who are unwilling or unable to usefully work cognitively and behaviourally, for
example people with active substance dependence, brain injury, or low weight anorexia
nervosa. New participants can join the group at frequent intervals.
11.1.4 Consultation
The PDS is currently developing its consultation function. The aims include to provide a range
of consultation modes including recommendations on the general management and treatment
94

of personality disorder, discussion of specific aspects of a clinical case, specific supervision for
professionals engaged in delivering general or specific psycho-social treatments to patients with
personality disorder, full case consultation and formal further opinions. Requests for
consultation are welcomed. See below for contact details.
11.1.5 Education and awareness
Until now, much of the education and awareness delivered by the Personality Disorder Service
has been on an ad-hoc basis. Educational sessions have been provided to various audiences in
many settings. Sessions have usually followed specific requests and been tailored according to
particular needs. In some settings, educational sessions have been co-delivered with service
users. Service user involvement in education and awareness-raising adds the patient’s unique
experience of living with personality disorder to the clinician’s perspective.
The Personality Disorder Service educational programme is currently undergoing a process of
development, including evaluation of the possibility of electronically available educational
modules. Currently, the main regular educational sessions occur four times per year. Each
session covers a different personality disorder-related subject and lasts for approximately 2
hours. Dates and topics are distributed by email. Anyone with an interest in personality disorder
can contact the PDS to be placed on the distribution list.
As well as these regular sessions, the PDS service will consider any request for education on
subjects related to personality disorder. See below for contact details.
The PDS has hosted development of this PD-ICP document, which is hoped to serve as a
valuable educational resource. Each section summarises an important topic in personality
disorder and useful resources and links can be found throughout. The publication of this
document will be supported by an educational and awareness-raising program. The educational
support aims to be broad in scope, including New Craigs Hospital, Community Mental Health
Teams, Addictions Services, Primary Care, Accident and Emergency and Secondary Care
Community Services. This list is not intended to be exclusive, and the PDS will endeavour to
respond to all requests for awareness-raising of the PD-ICP document.
11.2 Services not currently offered by the PDS
Although requests for the following services are sometimes received, the PDS is currently
unable to provide:
• Case management
• A general diagnostic service. Secondary care teams are well placed to make the
diagnosis of personality disorder and the diagnosis should be made before referral to the
PDS, which should ordinarily be for one of the reasons below.
• “Stand alone” trauma work. In other words, although trauma work is available for
patients in DBT, it cannot be provided outwith the DBT setting.
11.3 How to access these services
Although the options available to treat personality disorder in NHS Highland have increased
considerably over recent years, it remains the case that no single intervention represents a
complete treatment for personality disorder.
95

Care and treatment of personality disorder in NHS Highland follows a matched care model and
most patients with personality disorder will not require referral to the PDS. Reasons to consider
referral to the PDS include:
• Complexity, including lack of response to treatments provided within other settings
• Severity, as indicated by, for example, potentially lethal parasuicidal behaviour or
emergency psychiatric hospital admission
• Lack of treatment progress after adequate trial of appropriate treatment, including
identified need for a structured intensive Phase 3 (integration or making connections)
intervention
Currently, the PDS only accepts referrals from secondary care mental health services.
Discussion of potential referrals with the PDS is encouraged, see below for contact details. The
standardised assessment supersedes the previous system used by the PDS where patients
were referred for specific interventions such as DBT or CAS Day Service and a single PDS
referral form (details of which can be found below) replaces the separate DBT and CAS forms.
The referral form has a clinician-completed component and a patient-completed supporting
statement. Referrals cannot be processed until both parts are received.
It is recommended that patients are informed that they are being referred for assessment rather
than for a specific treatment such as DBT, even if it seems likely that this will be offered.
Contact details
Personality Disorder Service
Psychotherapy Department
Greenfields House
New Craigs Hospital
Leachkin Road
Inverness
IV3 8NP
Telephone: 01463 253681
Personality Disorder Service Referral Form
96
References
Bateman, A., & Fonagy, P. (2009). Randomised controlled trial of out-patient mentalisation
based treatment versus structured clinical management for borderline personality
disorder. American Journal of Psychiatry, 166, 1355–1364.
McMain, S., et al. (2009). A randomised controlled trial of dialectical behaviour therapy versus
general psychiatric management for borderline personality disorder. American Journal
of Psychiatry, 166, 1365–1374.
97

98

12. Inpatient Care
12.1 An overview of the evidence
Best available evidence suggests that, on the whole, acute in-patient care is at best neutral and
at worst damaging to the long term recovery of people with personality disorder. However, there
will of course be occasions when inpatient care can be life-saving in the short term if used
judiciously.
Long term specialist residential placements also fail to show positive long term benefits. This
suggests that the problem is not due to a lack of specialist skills, knowledge or attitudes within
acute ward staff.
One study showed that a short stay in a specialist residential unit followed by long term
outpatient treatment had significantly better outcomes in a variety of indicators than long stay
specialist residential treatment.
Severity of personality disorder also appears to be a negative predictor of outcome for inpatient
treatment, but this does not seem to be the case for outpatient treatment.
There appears to a principle of “less is more” as regards inpatient treatment. The benefit of
“less” may be explained by the incremental accrual of skills by managing emotional crises in the
everyday interpersonal and social contexts in which they arise. This contrasts with a pattern of
avoiding such situations by admission to hospital, which inhibits in vivo skills development.
Admitting a dysregulated, emotionally sensitive individual to a highly emotionally-charged
environment, where staff may have different views on the appropriateness of the admission and
respond differently to the patient as a result, can have significant dysrregulating effects. Many
people with borderline personality disorder are likely to be particularly sensitive to real or
perceived disapproval from staff and/or other patients. This increased emotional sensitivity, and
sensitivity to rejection in particular, can lead to an emotional response of intolerable intensity.
Very often, the only strategies available to the patient to modify such unpleasant emotional
states are unhelpful, for example self-harm, use of drugs or alcohol etc. Use of such strategies in
the inpatient setting is often viewed negatively by staff, and any disapproval or even gentle
challenging of the behaviour may be experienced by the patient as a rejection, leading to a
further intolerable emotional response, which in turn may lead to more unhelpful behaviour in an
attempt to feel better, with further challenges by staff, and so on.
12.2 When to consider admission
For these reasons, careful consideration should be given to alternative services capable of
meeting the person’s needs. However, there may be occasions where in-patient admission is the
most appropriate course of action. A description of circumstances when admission should be
considered should be detailed in the care plan where possible. Care plans should be available in
the case notes. Copies of Care Programme Approach plans are also held in the Assessment
Suite at New Craigs Hospital.
Situations where consideration may be given to admission when all other options have been
explored and deemed less appropriate include:
• Management of an acute increase in suicide risk (as opposed to chronic suicide risk
which is unlikely to be improved, and may be increased by, admission) or other extremely
99

risky behaviour. Important factors to consider are an acute increase in suicidal intent or
impulsivity. Tools such as STORM can be useful in identifying an acute increase on
chronic baseline risk.
• Changes to medication which cannot be managed in the community. This may involve
rationalisation of polypharmacy more rapidly than could be done as an outpatient.
• Intensive assessment which cannot be carried out in the community. This may include
clarification of diagnosis. Personality disorder can occasionally present similarly to axis 1
disorders but treatment approaches are usually significantly different.
• Treatment of co-occurring severe mental state disorders.
The short and long term potential benefits of admission should be weighed against the short and
long term risks of harm and discussed with the patient. Consideration of admission to hospital
must be balanced against the evidence that admission to hospital (especially lengthy admission)
may be harmful for many patients with borderline personality disorder, in terms of extending the
duration of the disorder and acute symptomatic deterioration.
Any existing care plans, for example CPA care plans, should be considered in the decision-
making process.
12.3 During admission
If it is considered that admission to hospital is unavoidable:
• The phase of treatment should be identified and indicated to everyone involved. Hospital
admission is likely to be of benefit in safety and containment (Phase 1a and 1b) but is
likely to be detrimental to the development of self-regulation and control (Phase 1c). This
may help to explain why meaningful stabilisation is uncommon during extended hospital
admission.
• Admission should be kept as short as possible, with the timescale agreed and
documented at the point of admission. Most acute behavioural dysregulation recedes
within 24-72 hours. This provides a timeframe for discharge to community treatment and a
clear rationale should be documented for admissions which exceed this duration given
that it seems very likely that the risk of harm increases with the length of admission.
• Clear objectives and purpose for the admission should be agreed and documented at the
outset. At the time of admission the aims of admission should be agreed with the patient
and documented along with the reasons why other options where considered and
rejected.
• Roles and responsibilities of staff and patients should be clearly explained and agreed,
with contingencies of treatment frame explicitly explained. For example, it may be
explained to the patient that non-engagement with the agreed treatment plan may lead to
a review of the usefulness of continuing the admission. The treatment plan may include
components such as an expectation that the patient takes responsibility to problem solve
any factors contributing to an acute crisis, that they undertake not to self-harm while in
hospital, that an attempt is made to enhance and use self-regulatory skills.
• An admission may be viewed as an opportunity to review care plans, crisis plans and
goals, and successfully re-establish outpatient treatment.
• An admission may be an opportunity to refer for a phase-appropriate treatment.
100

• Avoid inappropriate use of medication, especially benzodiazepines and similar sedatives.
• During admission contact should be maintained with the person’s key worker in Commu-
nity Mental Health Services.
• Crisis admissions should aim to (in line with standard crisis resolution approaches):
• Stabilise the acute crisis rather than tackle the underlying disorder. The aim is a
return to pre-crisis functioning and rapid discharge.
• Re-establish care plan and crisis plan
• Address changeable stressors
• Reduce access to means of suicide
• Identify and mobilise current supports
The Crisis Admission Document may be helpful in supporting the patient and care team to keep
the admission focused and time-limited.
12.4 Discharge and transitions
Effective discharge planning should begin as soon as possible from the time of admission and
should involve the multi-agency and multi-disciplinary team, the patient and where appropriate a
significant social network member. The discharge process should be a seamless process,
ensuring that appropriate services are available for the patient. Discharge and/or transfer care
plans need to be well coordinated, based on the individual’s assessed needs, reviewed
regularly, and include ongoing risk assessment and management. This can only be done with
effective planning and communication.
Consider Care Programme Approach (CPA) for individuals with frequent readmissions, with
clarity in the care plan about benefit and/or harm associated with hospital admission and a clear
alternative community plan.
12.5 Mental Health Act
Although personality disorder is one of the three listed types of mental disorder in terms of the
Mental Health (Care and Treatment) (Scotland) Act 2003, there is expert consensus that
compulsory treatment should be used only in the most extreme circumstances and management
on a voluntary basis should be resumed as soon as possible.
Compulsory treatment essentially removes personal responsibility for self-management from the
patient. Assumption of responsibility by the patient for their own recovery is a fundamental
principle in the treatment of personality disorder. Therefore, for most people with personality
disorder, detention to hospital represents management rather than treatment.
The five criteria for making the three forms of detention under the MH(S)A are similar:
• Emergency Detention Certificate criteria state that the medical practitioner considers it
likely that:
• the patient has a mental disorder;
• and because of that mental disorder, the patient’s decision-making ability with
regard to treatment for that mental disorder is significantly impaired;
• The practitioner must also be satisfied that:
• it is necessary as a matter of urgency to detain the patient in hospital in order to
101

determine what medical treatment should be provided to the patient for the
suspected mental disorder;
• there would be significant risk to the health safety or welfare of the patient or to
the safety of another person if the patient was not detained in hospital;
• making arrangements with a view to granting a short-term detention certificate
would involve undesirable delay.
• Short-term Detention Certificate criteria state that the medical practitioner considers it
likely that:
• the patient has a mental disorder;
• because of the mental disorder, the patient’s ability to make decisions about the
provision of medical treatment is significantly impaired;
• it is necessary to detain the patient in hospital for the purpose of determining
what medical treatment should be given to the patient or giving medical
treatment to the patient;
• if the patient was not detained in hospital there would be significant risk to the
health, safety or welfare of the patient or to the safety of another person;
• the granting of the short-term detention certificate is necessary.
• Compulsory Treatment Order criteria which the tribunal must be satisfied are fulfilled:
• that the patient has a mental disorder;
• that because of the mental disorder the patient’s ability to make decisions about
the provision of medical treatment is significantly impaired;
• that medical treatment which would be likely to prevent the mental disorder
worsening or alleviate any of the symptoms or effects of the disorder is
available for the patient;
• that if the patient was not provided with such medical treatment there would be
a significant risk to the health, safety or welfare of the patient or to the safety of
another person;
• that the making of a Compulsory Treatment Order in respect of the patient is
necessary.
• Points to consider for each criterion include:
• EDC,STDC,CTO: The patient has a mental disorder.
• Personality disorder is one of the three broad categories of mental disorder in
terms of the MH(S)A. The other 2 categories are mental illness and learning
disability.
• EDC, STDC, CTO: Significantly impaired decision making ability(SIDMA):
• Best available evidence indicates that hospital treatment is, on the whole,
at best neutral and at worst harmful for people with personality disorder.
Therefore it may be difficult to argue that SIDMA is present on the basis
of a patient refusing hospital treatment alone.
• Best available evidence shows, on the whole, no significant benefit for
drug treatment. Therefore it may be difficult to argue that SIDMA is
102

present on the basis of a patient refusing drug treatment alone.
• EDC: It is necessary as a matter of urgency to detain the patient in hospital in order to
determine what medical treatment should be provided to the patient for the suspected
mental disorder:
• STDC: it is necessary to detain the patient in hospital for the purpose of determining
what medical treatment should be given to the patient or giving medical treatment to the
patient:
• CTO: that medical treatment which would be likely to prevent the mental disorder
worsening or alleviate any of the symptoms or effects of the disorder is available for the
patient:
The treatment provided for an individual should be phase-appropriate. Most patients who
are considered for detention will need treatments aimed at promoting safety (Phase 1a),
containment (Phase 1b) or self-regulation and control (Phase 1c). Hospital treatment
may be useful in promoting safety and containment but is likely to have a neutral or
negative effect on self-regulation and control. Therefore, although hospital treatment
may alleviate isolated symptoms, for example high intensity nursing care may physically
prevent suicidal behaviour, it is unlikely that hospital treatment will prevent the disorder
itself from worsening, and may be likely to contribute to a global deterioration. Clinical
experience suggests that these factors are even more relevant when patients are
detained than during informal admissions.
Several different models of psychological therapy have been shown to be effective in the
treatment of personality disorder.. All trials involved voluntary patients, and there is no
evidence base for the treatment of involuntary patients. Furthermore, many of the
treatment models expressly discourage use of compulsion for reasons of conflict with
the general and specific factors and theoretical principles upon which the treatments are
based.
• EDC, STDC, CTO: significant risk to the health, safety or welfare of the patient or to the
safety of another person if not detained in hospital/ provided with medical treatment:
• As outlined above, while high intensity nursing care may promote safety by
physically preventing suicidal behaviour and acutely lower the risk of suicide,
hospitalisation and detention may actually increase chronic suicide risk and worsen
prognosis.
• STDC, CTO: necessity:
• Consideration should be given to all other treatment options, especially those with an
evidence base and those coherent with the general principles of the treatment of
personality disorder. Often hospital treatment, especially under detention, amounts to
conservative management of the disorder rather than positive treatment. There should
be recognition that risk cannot be entirely eliminated whatever the course of treatment
or management. Furthermore, positive, collaborative risk-taking based upon a position
of compassion and firm clinical rationale often forms an indispensable component of
the treatment of personality disorder.
12.6 Structured Admissions Program
This program was developed for patients with personality disorder who had multiple crisis
103

admissions. It allows patients and the treating team to schedule 4 one-week admissions in
year 1, 3 one-week admissions in year two, 2 one-week admissions in year 3 and 1 one-
week admission in year 4, provided crisis admissions are avoided. Each admission will have
a specific goal or goals which will be worked towards using a CBT-type framework. These
admissions are not used for other purposes, for example medication changes etc. The
program is arranged by the user’s sector consultant psychiatrist. Continued contact with the
Community Mental Health Services must be maintained and the person must have a named
key-worker in the community.
Essentially the Structured Admissions Program is a team approach, with all the team
members and the individual aiming towards an increase in structure, stability, confidence
and independence.
The agenda for each admission will be discussed and agreed at a multidisciplinary meeting
of the patient together with relevant community and hospital based clinicians at least 4
weeks before the admission.
Clinicians should be cautious of adapting this intervention without fully considering the
behavioural contingencies and risk-benefit balance of any adaptation.
The Structured Admissions Program as originally conceived represents a Phase 1
intervention.
The evidence base for this intervention is comprised of non-experimental, descriptive
evaluation. There should be a clear clinical rationale for considering this intervention over
other Phase 1 interventions such as DBT or STEPPS with more robust evidence bases.
There is unlikely to be any added benefit in an individual engaging in both a psychological
therapy like DBT and the Structured Admissions Program. In fact, there may be theoretical
conflict. It is suggested that if a patient is on the Structured Admissions Program and is being
considered for referral for DBT or STEPPS, that the case should be discussed with the
appropriate service at the time of referral.
104

12.6.1 Specific features of the Structured Admissions Programme:
1. The individual wishing to have structured admissions should be made aware that they are
an alternative to crisis admissions.
2. The number of structured admissions per year will be identified at the start of each year and
will be linked to the care plan based upon individual need. The composition of the team
should remain consistent across admissions, as far as possible.
3. The maximum number of structured admissions per year is four. The program can also
commence with three structured admissions per year. The annual number of admissions
reduces by one each year. Once the individual progresses to a single admission in a year,
needs will be reassessed.
4. Though structured right from the start, these admissions do not happen automatically. Each
admission will be on the merit and benefits of the previous one - how this has helped the
individual cope with stress, how the coping strategies learnt have been made use of when in
crisis etc.
5. There will be no medical input during admission except for technicalities of admission and
discharge.
6. The focus is on de-stressing and learning ways to manage distress in the context in which it
arises, rather than medicalising the issue.
7. If there are difficult dates or anniversaries, admissions can be planned around theses dates.
Planning needs to be done before structuring the admissions.
8. Intense Nursing, Occupational Therapy and Physiotherapy input will be provided as
planned before each admission.
9. No other psychology/ psychotherapy session will be possible during the admission week, if
some one is already in psychological treatment, the individual is expected to rearrange
those sessions which occur during the period of admission. This should not prove
problematic as structured admission weeks are known to the individual from the start of the
year.
10. Structured admission is from Monday- Friday morning, no passes are usually allowed during
this period. Patients are encouraged to keep visitors to a minimum during the admission
period, as this can negatively impact upon the de-stressing process and contribute to
valuable loss of time which could otherwise be spent working with the team.
11. Structured admission is from Monday- Friday morning, no passes are usually allowed during
this period. Patients are encouraged to keep visitors to a minimum during the admission
period, as this can negatively impact upon the de-stressing process and contribute to
valuable loss of time which could otherwise be spent working with the team.
12. Individuals undertake not to engage in self harming behaviours, alcohol or drug use during
admission. Such behaviours could lead to early discharge.
13. The individual is expected to take responsibility for their own treatment.
105
References
Bateman, A., & Krawitz, R. (2013). Borderline Personality Disorder—An evidence-based guide
for mental health professionals. Oxford.
Livesley, J. (2003). Practical Management of Personality Disorder. Guilford.
NICE. (2009). Borderline Personality Disorder Treatment and Management. NICE Clinical
Guideline 78.
Samson, M., McCubbin, R., & Tyrer, P. (2006). Personality disorder and community mental
health teams. Wiley.
106