persistent idiopathic facial pain associated with
TRANSCRIPT

Case ReportPersistent Idiopathic Facial Pain Associated with SomatoformDisorder in an 11-Year-Old Boy
Yoshihiko Sakurai ,1 Asami Fujii,2,3 and Fumie Kato2,4
1Department of Pediatrics, Matsubara Tokushukai Hospital, 7-13-26 Amami-higashi, Matsubara, Osaka 580-0032, Japan2Department of Psychosomatic Medicine, Matsubara Tokushukai Hospital, 7-13-26 Amami-higashi,Matsubara, Osaka 580-0032, Japan
3Palliative Care Center, Nara Medical University Hospital, Kashihara, Nara 634-8522, Japan4Department of Psychosomatic and General Internal Medicine, Kansai Medical University, 2-5-1 Shinmachi, Hirakata, Osaka, Japan
Correspondence should be addressed to Yoshihiko Sakurai; [email protected]
Received 16 November 2018; Accepted 28 January 2019; Published 7 February 2019
Academic Editor: Liliana Dell'Osso
Copyright © 2019 Yoshihiko Sakurai et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Persistent idiopathic facial pain (PIFP) is a poorly understood chronic disorder that rarely occurs in children. An 11-year-old boyinitially presented with right cheek pain and a streptococcal infection 6 weeks previously. Facial cellulitis was suspected, which wasresolved by antibiotic treatment. The right cheek pain recurred within 4 weeks of this initial visit. Because the antibiotic treatmentdid not relieve the pain, the patient visited our outpatient clinic. Physical examination revealed facial tenderness in an area thatcorresponded with the region supplied by the second branch of the trigeminal nerve (maxillary nerve), suggesting trigeminalneuralgia (TN). However, brain magnetic resonance imaging revealed no vascular compression. Furthermore, the continuousnagging and dull nature of the pain experienced by the patient differed from the sudden and severe nature of pain associatedwith TN. Subsequently, PIFP was diagnosed. The patient was unable to attend school because of prolonged lassitude, nausea,headache, and anorexia. Psychological counseling revealed psychological stress related to his out-of-school life. Upon learningstress management through psychotherapy, his general malaise gradually improved, and he was able to attend school with morefacial expressions. This case indicates the psychogenic aspect of PIFP as well as the value of psychological counseling.
1. Introduction
Chronic pain is often seen during childhood. Thirty percentof children, including adolescents, have chronic pain thatpersists for more than 3 months [1]. Furthermore, more than50% of children between the ages of 9 and 13 years experiencechronic pain at least once [2]. Headaches, abdominal pain,and musculoskeletal pain are the major types of chronic painexperienced during childhood. However, individuals rarelycomplain of facial pain during childhood [3].
Although it is often ascribed to an injury or a headache,facial pain may also be the result of a neurological disor-der. Disorders involving both the central nervous system,including the thalamus and somatosensory area of the cere-bral cortex, and the peripheral nervous system, includingthe trigeminal nerve and its branches, may cause facial
pain. Trigeminal neuralgia (TN) is a representative disordercharacterized by unilateral facial pain due to a functionaldisorder of the trigeminal nerve. In TN, patients experiencecharacteristic brief, sudden, stabbing, electric-shock-like, andsevere episodes of pain [4]. When chronic facial pain lacksthe characteristics of other neurological disorders, includingTN, a diagnosis of persistent idiopathic facial pain (PIFP)—previously known as atypical facial pain — is made.
We report a case involving an 11-year-old boy with PIFPin whom psychological counseling was effective.
2. Case Presentation
An 11-year-old boy visited our outpatient clinic with com-plaints of persistent right cheek pain. His family historyrevealed that his father had severe hearing impairment.
HindawiCase Reports in PsychiatryVolume 2019, Article ID 4627850, 4 pageshttps://doi.org/10.1155/2019/4627850

2 Case Reports in Psychiatry
Figure 1: Head imaging study. Head computed tomography showedmucousmembrane swelling and fluid collection in bothmaximal sinuses(left). Brain magnetic resonance image. Vascular compression of the trigeminal nerve was not observed (right).
His medical history showed that he had allergic rhinitisand chronic sinusitis that had been treated until 3 monthspreviously by an otolaryngologist.
The patient initially visited our outpatient clinic withcomplaints of high fever, sore throat, and comorbid rightcheek pain and mild swelling 6 weeks previously. A checkupat a dental clinic performed on the day before this initial visitrevealed no abnormal findings. He showed clinical symptomsof streptococcal pharyngitis. A rapid antigen test for group Astreptococcal infection showed positive results. The patientwas diagnosed with streptococcal infection. Facial cellulitiswas also suspected and treatment with amoxicillin helpedimprove symptoms. However, facial pain recurred within 4weeks of the initial visit. The patient had mild tendernessand swelling of the right cheek. Head computed tomographyrevealed mild mucous membrane swelling and effusion inboth sinuses (Figure 1 left). Because recurrence of cellulitiswith sinusitis was suspected, cefditoren pivoxil treatment wasinitiated. However, because the pain persisted, he visited ourdepartment.
Physical examination revealed no abnormal findingsexcept right cheek tenderness in the area that correspondedwith the region supplied by the second branch of thetrigeminal nerve (the maximally nerve). Although markedtenderness was evident, no point with hyperalgesia, wherea light touch elicited severe pain, was observed. No facialparalysis or oral disorders were observed. Blood examinationrevealed no abnormal findings. Recurrence of sinusitis wassuspected. Based on the physical examination and laboratorytests, the patient was clinically diagnosed with TN. Subse-quently, oral clarithromycin administration was initiated forsinusitis that might have caused or exacerbated TN.However,administration of clarithromycin for 1 week was not effectivefor his facial pain. Brain magnetic resonance imaging (MRI)revealed no neurovascular compression (Figure 1 right),which ruled out idiopathic, classical TN. During this time,we interviewed the patient on the nature of the right cheekpain. The patient described the pain as persistent, nagging,and dull in nature, which was completely different fromthe characteristics of pain associated with TN. Furthermore,
trigger maneuvers failed to evoke pain. These evaluationsexcluded TN, and, thus, PIFP was diagnosed in week 2. Lowdose of oral anticonvulsant carbamazepine (50 mg, twice aday) was initiated but was ceased due to general fatigue afterthe first administration.
Although the patient had been previously cheerful andgreeted us when entering the examination room, he becamegradually emotionless with headache and nausea in week5. In addition, feeding difficulties and numbness in thearms occurred. An orthostatic tolerance test revealed nopositive findings for orthostatic dysregulation. It becamedifficult for the patient to attend school in week 6. Becausevarious somatic symptoms developed in addition to PIFP,psychological factors were suspected to be pertinent in theetiology of PIFP. During a detailed medical interview withthe patient and his mother, several problems were revealed:the patient loved swimming but his swimming record hadplateaued after fixing his swimming form even though hepracticed vigorously at a top-class swimming club team.Moreover, because of a recent finger injury, he could notpractice as intensely as he wanted; therefore, his competitiveability as a swimmer deteriorated. Furthermore, in earlyadolescence, the patient had difficulties in communicationand his relationship with his father was strained due tothe father’s hearing impairment. Because these suggestedthat the circumstances surrounding him might have led tosomatoform disorders, psychological counseling was orderedin week 6.
As the patient faced, understood, and tolerated hispsychological stress through counseling and psychotherapytwice a week, he gradually became expressive, worked up hisappetite, and could attend school inweek 10. Although sinusi-tis recurred at week 29, no facial pain developed. The patientreceived psychological counseling twice or thrice a monthby this time. After 8 months, the frequency of counselingwas reduced to once in 2 months. During this period, thepatient's voice changed and became deeper at puberty. Afterconfirming that facial pain as well as general malaise did notoccur, even when the patient experienced distressing events,such as terminal examinations, counseling was ceased after 1
Case Reports in Psychiatry 3
TrigeminalLocation of pain
MRI findings
Nature of pain
Diagnosis
Other nerves Non-anatomic
SOL, AVM, MS
Secondary TN
Neurovascularcompression
Brief, electricshock-like
Classical TN
Normal
Idiopathic TN
Continuous Continuous
burning
Concomitant symptomsHerpeticeruption
Painfultrigeminal neuropathy
History Chicken pox Trauma
PIFP
(abr.)
dull, aching,or nagging
Purelyparoxysmal
With concomitantcontinuous pain
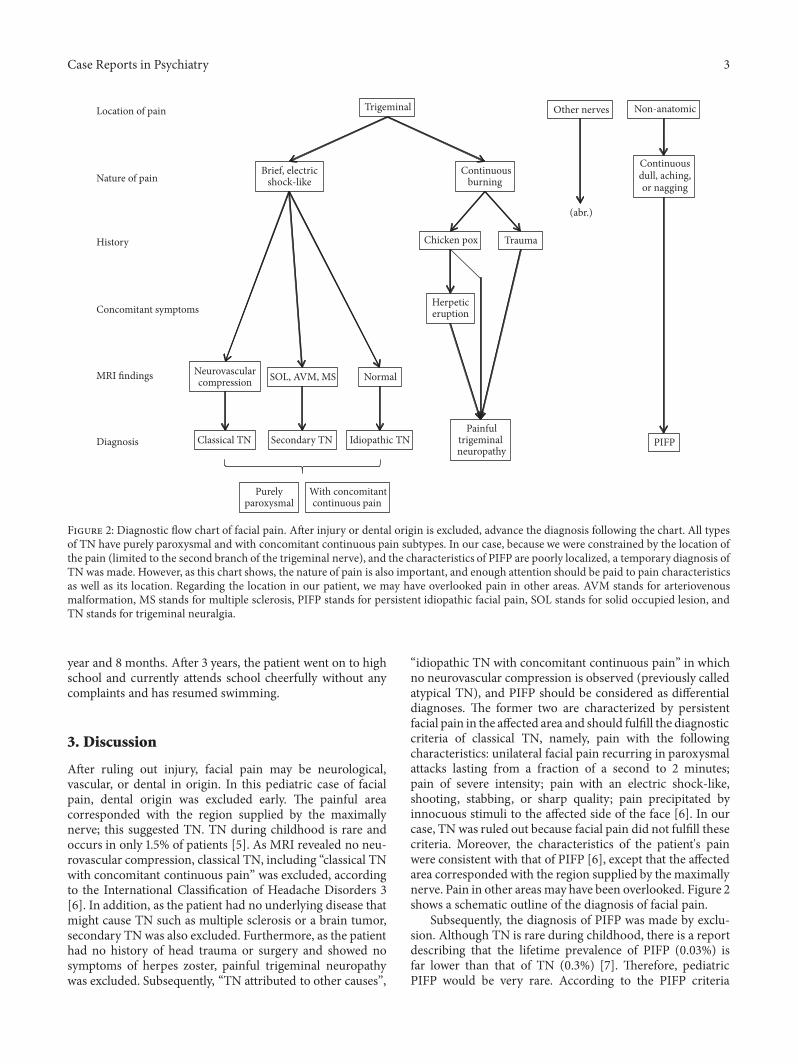
Figure 2: Diagnostic flow chart of facial pain. After injury or dental origin is excluded, advance the diagnosis following the chart. All typesof TN have purely paroxysmal and with concomitant continuous pain subtypes. In our case, because we were constrained by the location ofthe pain (limited to the second branch of the trigeminal nerve), and the characteristics of PIFP are poorly localized, a temporary diagnosis ofTN was made. However, as this chart shows, the nature of pain is also important, and enough attention should be paid to pain characteristicsas well as its location. Regarding the location in our patient, we may have overlooked pain in other areas. AVM stands for arteriovenousmalformation, MS stands for multiple sclerosis, PIFP stands for persistent idiopathic facial pain, SOL stands for solid occupied lesion, andTN stands for trigeminal neuralgia.
year and 8 months. After 3 years, the patient went on to highschool and currently attends school cheerfully without anycomplaints and has resumed swimming.
3. Discussion
After ruling out injury, facial pain may be neurological,vascular, or dental in origin. In this pediatric case of facialpain, dental origin was excluded early. The painful areacorresponded with the region supplied by the maximallynerve; this suggested TN. TN during childhood is rare andoccurs in only 1.5% of patients [5]. As MRI revealed no neu-rovascular compression, classical TN, including “classical TNwith concomitant continuous pain” was excluded, accordingto the International Classification of Headache Disorders 3[6]. In addition, as the patient had no underlying disease thatmight cause TN such as multiple sclerosis or a brain tumor,secondary TNwas also excluded. Furthermore, as the patienthad no history of head trauma or surgery and showed nosymptoms of herpes zoster, painful trigeminal neuropathywas excluded. Subsequently, “TN attributed to other causes”,
“idiopathic TN with concomitant continuous pain” in whichno neurovascular compression is observed (previously calledatypical TN), and PIFP should be considered as differentialdiagnoses. The former two are characterized by persistentfacial pain in the affected area and should fulfill the diagnosticcriteria of classical TN, namely, pain with the followingcharacteristics: unilateral facial pain recurring in paroxysmalattacks lasting from a fraction of a second to 2 minutes;pain of severe intensity; pain with an electric shock-like,shooting, stabbing, or sharp quality; pain precipitated byinnocuous stimuli to the affected side of the face [6]. In ourcase, TN was ruled out because facial pain did not fulfill thesecriteria. Moreover, the characteristics of the patient's painwere consistent with that of PIFP [6], except that the affectedarea corresponded with the region supplied by the maximallynerve. Pain in other areas may have been overlooked. Figure 2shows a schematic outline of the diagnosis of facial pain.
Subsequently, the diagnosis of PIFP was made by exclu-sion. Although TN is rare during childhood, there is a reportdescribing that the lifetime prevalence of PIFP (0.03%) isfar lower than that of TN (0.3%) [7]. Therefore, pediatricPIFP would be very rare. According to the PIFP criteria

4 Case Reports in Psychiatry
[6], patients with PIFP present with high levels of psychi-atric comorbidity and psychosocial disability. Taking thesetogether, PIFP in the patient was suspected to be due tosomatization of psychological stress.
There is no specific treatment for PIFP. A multidisci-plinary biopsychosocial approach with the use of antidepres-sant and antiepileptic drugs and psychological counselinghelps relieve pain [8, 9]. In our case, the patient was obligedto stop carbamazepine because of general fatigue after thefirst administration. Considering that the patient was underpsychological stress, complaints after administration mightbe attributed to psychological refusal ofmedical intervention.
Psychological counseling revealed that the patient inhis early adolescence had little difficulty in school life buthad some problems in his out-of-school life. One was theconflict with his father, which is common in preadoles-cent boys. However, his father's hearing impairment ledto communication difficulties and might have complicatedthe situation. In addition, although swimming was givenconsiderable importance by the patient, the gap betweenreality and expectations as a competitive swimmer hadwidened. Psychological counseling also revealed that he likedreading books and had an excellent understanding of thiscausal relationship and insight of his situation. Due to theseadvantages, he understood his position and controlled hisown emotion. However, with too much consideration forothers, he behaved older than his age, which might haveexacerbated psychological stress.
Sand-play therapy and psychological counseling withlistening attitude gradually enabled the patient to expresshis emotion. Appetite loss was first improved. Headacheand nausea consecutively disappeared. Lastly, facial painwas gradually improved in accordance with the repetitivecounseling. These suggest that somatization due to psy-chological stress underlies the pathogenic mechanism ofPIFP in our case. PIFP might occur as somatization in thepatient with overadaptation tendency, triggered by out-of-school problems on the background of the vague sense ofunease characteristic to preadolescence. Expression of self-consciousness that the patient acquired through psychologi-cal therapeutic support might produce improvements.
The importance of the psychological perspectives ofchronic pain has been underscored [10]. When encounteringa pediatric patient suspected of having PIFP, one should notonly determine the cause of facial pain but also consider thepsychological problems that the patient might have.
Consent
Written informed consent was taken from the patient andhis guardians for publication of this case report and theaccompanying images.
Conflicts of Interest
The authors declare that there are no conflicts of interestregarding the publication of this article.
Acknowledgments
This research received no specific grant from any fundingagency in the public, commercial, or not-for-profit sectors.
References
[1] S. King, C. T. Chambers, A. Huguet et al., “The epidemiology ofchronic pain in children and adolescents revisited: a systematicreview,” PAIN, vol. 152, no. 12, pp. 2729–2738, 2011.
[2] A. van Dijk, P. McGrath, W. Pickett et al., “Pain prevalence innine- to 13-year-old schoolchildren,” Pain Research & Manage-ment, vol. 11, no. 4, pp. 234–240, 2006.
[3] L. Kondev and A. Minster, “Headache and facial pain inchildren and adolescents,” Otolaryngologic Clinics of NorthAmerica, vol. 36, no. 6, pp. 1153–1170, 2003.
[4] R. Melzack, C. Terrence, G. Fromm, and R. Amsel, “Trigeminalneuralgia and atypical facial pain: Use of the McGill painquestionnaire for discrimination and diagnosis,” Pain, vol. 27,no. 3, pp. 297–302, 1986.
[5] A. Ekici, A. Yakuta, A. Incesulub et al., “Trigeminal neuralgia:a rare cause of facial pain in a child,” International Journal ofClinical Pediatrics, vol. 2, no. 2, pp. 74-75, 2013.
[6] Headache Classification Committee of The InternationalHeadache Society, “The international classification of headachedisorders, 3rd edition,” in Cephalalgia, vol. 38, no. 1, pp. 1–121,2018.
[7] D. Mueller, M. Obermann, M.-S. Yoon et al., “Prevalence oftrigeminal neuralgia and persistent idiopathic facial pain: Apopulation-based study,” Cephalalgia, vol. 31, no. 15, pp. 1542–1548, 2011.
[8] J. M. Zakrzewska, “Chronic/persistent idiopathic facial pain,”Neurosurgery Clinics of North America, vol. 27, no. 3, pp. 345–351, 2016.
[9] P. Cornelissen,M. van Kleef, N.Mekhail et al., “Evidence-basedinterventional pain medicine according to clinical diagnoses. 3.Persistent idiopathic facial pain,” Pain Practice, vol. 9, no. 6, pp.443–448, 2009.
[10] Y. Ishizaki, H. Yasujima, Y. Takenaka et al., “Japanese clinicalguidelines for chronic pain in children and adolescents,” Pedi-atrics International, vol. 54, no. 1, pp. 1–7, 2012.

Stem Cells International
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
MEDIATORSINFLAMMATION
of
EndocrinologyInternational Journal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Disease Markers
Hindawiwww.hindawi.com Volume 2018
BioMed Research International
OncologyJournal of
Hindawiwww.hindawi.com Volume 2013
Hindawiwww.hindawi.com Volume 2018
Oxidative Medicine and Cellular Longevity
Hindawiwww.hindawi.com Volume 2018
PPAR Research
Hindawi Publishing Corporation http://www.hindawi.com Volume 2013Hindawiwww.hindawi.com
The Scientific World Journal
Volume 2018
Immunology ResearchHindawiwww.hindawi.com Volume 2018
Journal of
ObesityJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Computational and Mathematical Methods in Medicine
Hindawiwww.hindawi.com Volume 2018
Behavioural Neurology
OphthalmologyJournal of
Hindawiwww.hindawi.com Volume 2018
Diabetes ResearchJournal of
Hindawiwww.hindawi.com Volume 2018
Hindawiwww.hindawi.com Volume 2018
Research and TreatmentAIDS
Hindawiwww.hindawi.com Volume 2018
Gastroenterology Research and Practice
Hindawiwww.hindawi.com Volume 2018
Parkinson’s Disease
Evidence-Based Complementary andAlternative Medicine
Volume 2018Hindawiwww.hindawi.com
Submit your manuscripts atwww.hindawi.com