persistent diarrhea & chronic diarrhea
TRANSCRIPT

PERSISTENT DIARRHEACHRONIC DIARRHEA
Moderator Presented by Dr. Sumit Das Dr. Fahad Muhamed Shareef A TAss. Prof. PG in Pediatrics
Dept. of Pediatrics

• Diarrhea
– 3 times in 24 hours
– Consistency important over frequency
• Acute Diarrhea
• Persistent Diarrhea
• Chronic Diarrhea
TERMS & DEFINITIONS

PERSISTENT DIARRHEA
• Starts as acute, lasts at least 14 days with
the exclusion of chronic or recurrent
diarrheal conditions
– Celiac disease Tropical Sprue
– Biochemical Congenital
– Metabolic

?WHY
• 10% of total diarrhea
• 35% of diarrheal deaths
• For every 100 children, 7 suffers
• PD in Malnutrition – 20%
• 60% < 6 months
• 90% < 1 year

RISK FACTORS & CAUSES• Repeated enteric infections
• Malabsorption of CHO & fats
• Malnutrition
• Very young age
• Recent introduction of animal milk
• Irrational usage of antibiotics
• Lack of breast feeding/ bottle feeding
• Improper therapy of ADD
• Protein dietary intolerance

PATHOGENESIS“PSIMI”
Mucosal injury d/t invasive pathogens
Malabsorption of macro & mircronutrients
Prolongation of mucosal injury & delayed intestinal repair
mechanisms (ineff. villous repair)
Sequential infection with multiple pathogens
Increased absorption of foreign proteins
Malnutrition
PRESENTATION
• Several loose stools
• Dehydration absent
• If present, inc stool output
dec oral intake
• Features of PEM

Clinical Evaluation• History & Physical Examn.
• Should be excluded from Chronic
diarrhoea
• To R/o associated systemic infections
– CBC
– URE & C/S
– CXR
• Stool microscopy
• Stool pH & reducing substance

• Nutritional management is the cornerstone
– Dietary management
– Supplemental vitamins & minerals
• Two third cases – OPD
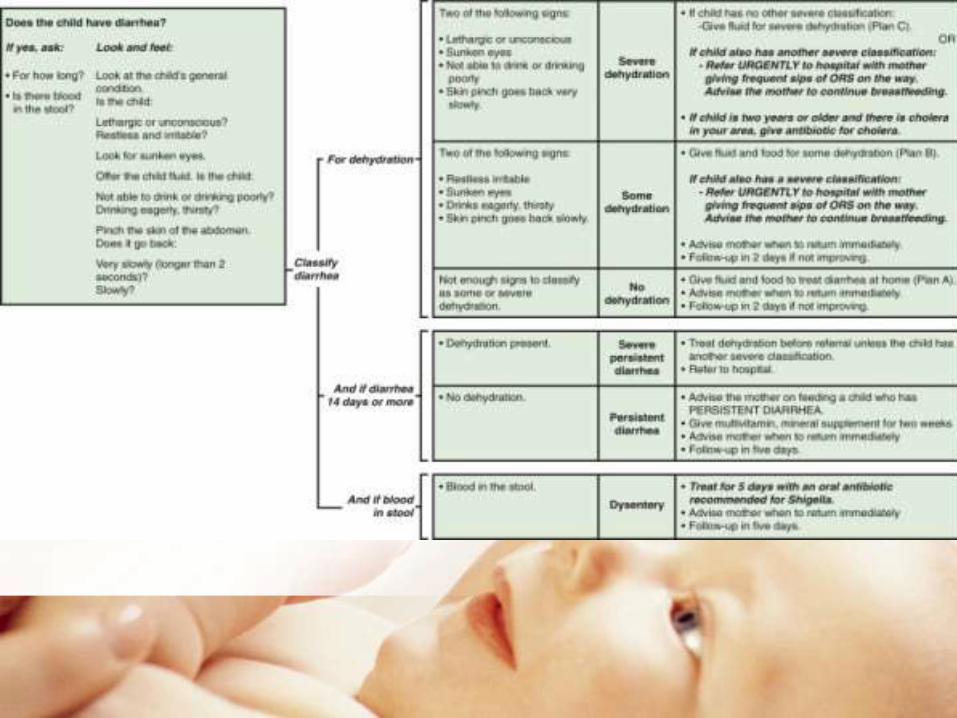
• Assess dehydration
• Hospitalization necessary or not
• Avoid unnecessary antibiotics
TREATMENT

When to hospitalize?
• Age < 4 mon & not breast fed
• Dehydration
• Severe malnutrition
– W/L < 70%
– W/A < 60%
– Pedal edema
• Systemic infection

Dietary Management
< 6 months
• Encourage exclusive breast feeding
• Reestablish breast feeding
• Replace animal milks with curds or lactose
free formula
• Cooked rice may be mixed if necessary

>6 months
• Continue Breast feeding
• Mixed diet
• Initiate DIET A
• DIET B
• DIET C

Milk cereal mixtures v/s
milk free diet• Highly palatable
• Provide good quality protein
• Some micronutrients
• Faster weight gain
• No significant increase in stool output
• No increasing risk of dehydration

Principles
• Total elimination of milk not necessary
• Limit intake to 2g/kg/day lactose (50-60
ml)
• Start feeding asap
• 6-7 feeds per day
• Start with 110kcal/kg and inc to 150kcal/kg
over 2 weeks
• If enteral intake diff, start NG feed

DIET A reduced lactose diet (65-70%)Ingredients Measures Wt/Vol
Milk 1/3 katori 50ml
Sugar 1.5 tsp 7g
Oil 1 tsp 4.5g
Puffed rice powder 2 tsp 6.0g
Water 2/3 katori 100ml
Calories/100g 85 kcal
Proteins/100g 2.0g
How to prepare

DIET Blactose free with reduced starch(15-20%)
Ingredients Measures Wt/Vol
Egg white 3 tsp Half egg white
Puffed rice powder 3 tsp 9.0g
Glucose 1.5 tsp 7g
Oil 1.5 tsp 7g
Water 3/4 katori 120ml
Calories/100g 90 kcal
Proteins/100g 2.4g
How to prepare

DIET CMonosaccharide based
Ingredients Measures Wt/Vol
Egg white 3 tsp Half egg white
Or Chicken puree 5 tsp 15 g
Glucose 1.5 tsp 7 g
Oil 1.5 tsp 7 g
Water 1 katori 150ml
Calories/100g 67 kcal
Proteins/100g 3 g
How to prepare

Supplementation
• 2 x RDA of multivitamins and minerals for
2-4 weeks
• At least Vit A (single dose) & Zinc 10-
20mg (2 weeks)
• In severe malnutrition,
– 50% Mg sulfate 0.2ml/kg/dose twice a day for
3 days
– Potassium 5-6meq/kg/day

Monitoring response
• Dec in no. of diarrheal stools
– <= 2 liquid stools/day for 2 consec. Days
• Adeq. Food intake
• Weight gain
Most children lose wt in the initial 1-2 days
and then show a steady gain

When to change diet• Marked increase in stool freq (10/day)
• Return of signs of dehydration
• Failure to establish wt gain by day 7
after discharge little milk after 10 days
No signs of lactose intolerance
Milk qty increased and normal diet ovr a
week

PARENTERAL NUTRITION
• PD with oral intolerance after 10 days
• Severe forms of IBD+ resistant colitis
• Severe NEC
COMPLICATIONS
PARTIAL PARENTERAL NUTRITION
• Isolyte P - 250ml 25%D – 150ml
• A.A – 100ml NaHCO3 – 20ml
• KCl – 5ml MVI – 2ml
• 50-60 ml/kg/d

Antimicrobial Therapy
• Gross blood in stools
• Asso systemic infection
• Severe malnutrition
• Screen for UTI and treat
• Group B Salmonella isolated in stool


PREVENTION
• Improving nutritional status
• Prevention and rational treatment of acute
diarrhea
• Promote exclusive breast feeding
• Ensure safe complemetary feeding
practices
• Zinc supplementaton
• Avoid irrational & unnecessary use of
antibiotics
• Continued feeding during diarrhea

CHRONIC DIARRHEA
• Diarrhea for >= 14 days with exclusion of
persistent diarrhea.
• Infections
• Malabsorption
• Metabolic
• Miscellaneous

INFECTIONS• Tuberculosis
• Eosinophilic gastroenteritis
• IBD
• NEC
• Henoch Scholein
MALABSORPTION
• Pancreatic diseases
• Liver diseases
• Intestinal diseases

INTESTNAL MALABSORPTION
• CELIAC DISEASE (TVA)
• GIARDIASIS
• BACTERIAL OVERGROWTH
• MALNUTRITION PVA
• TROPICAL SPRUE
• ABETALIPOPROTEINEMIA
• LYMPHANGIECTASIA
• ENZYME DEF.

Miscellaneous
• TODDLER’S DIARRHEA
• CHRONIC NON SPECIFIC DIARRHEA
• IRRITABLE BOWEL SYNDROME
• AUTOIMMUNE ENTEROPATHY
• MOTILITY DOSORDERS
• ENDOCRINE
• NEOPLASTIC DISORDERS
• MANCHAUSEN BY PROXY

Clinical evaluation• Onset
– At birth chloride diarrhea, microvillous inclusion dis.
– 6 mon autoimmune enteropathy
– Infant Hirschsprung’s dis
– Abrupt Infections
– Gradual Rest
• Weight loss : Malabsorption,neoplasm
• Dietary history
– Lactose intolerance, cow’s protein, soy protein, egg protein
– Overfeeding, chewing gum diarrhea, Non specific diarrhea
• Treatment history
– Antibiotics, prpnl, digitalis, cholestyramine, Munchausen
• Family history : IBD, IBS

STOOL CHARACTERISTICS
• Blood Dysentry
• Oil/ food particles Malabsorption, maldigestion
• White/ tan colour Celiac disease, absence of bile
• Loose & bulky Celiac disease
• Greasy & yellowish exocrine pancreatic insuff
• Liquid as water Cong. Chloride diarrhea


• Plain x-ray abdomen
• Ultrasonography
• Colonoscopy
• Capsule endoscopy

STEP 1 Intestinal microbiology
• Stool cultures
• Microscopy for parasites
• Viruses
• Stool electrolytes
• H2 breath test
Screening test for celiac disease (transglutaminase 2 autoantibodies)
Noninvasive tests for:
• Intestinal function
• Pancreatic function and sweat test
• Intestinal inflammation
Tests for food allergy
• Prick/patch tests
DIAGNOSTIC WORK UP

TEST NORMAL VALUES IMPLICATION
α1-Antitrypsin concentration <0.9 mg/g stoolIncreased intestinal permeability
and protein loss
Steatocrit <2.5% (>2 yr old) Fecal fat loss
Fecal reducing substances Absent Carbohydrate malabsorption
Elastase concentration >200 µg/g stool Exocrine pancreatic dysfunction
Chymotrypsin concentration>7.5 U/g
>375 U/24 hExocrine pancreatic dysfunction
Fecal occult blood AbsentFecal blood loss, distal intestinal
inflammation
Calprotectin concentration 100 µg/g stool Intestinal inflammation
Fecal leukocytes <5/microscopic field Colonic inflammation
Nitric oxide in rectal dyalisate <5 µM of NO2−/NO3
− Rectal inflammation
Dual sugar (cellobiose/mannitol)
absorption test
Urine excretion ratio:
0.010 ±0.018Increased intestinal permeability
NON INVASIVE TESTS

STEP 2 INTESTINAL MORPHOLOGY
• Standard jejunal/colonic histology
• Morphometry
• PAS staining
• Electron microscopy
STEP 3 SPECIAL INVESTIGATIONS
Intestinal immunohistochemistry
Anti-enterocyte antibodies
Serum chromogranin and catecholamines
Autoantibodies
75SeHCAT measurement
Brush border enzymatic activities
Motility and electrophysiological studies

TREATMENT• General supportive measures
– Replacement of fluids & electrolytes
• Nutritional rehabilitation
• Elimination diet
• Treat the cause

CELIAC DISEASE
• Immunologically mediated small intestinal
enteropathy
• Sensitivity to gluten
• Multiple associations
• Classic form :
– 6m- 24m
– Chronic diarrhea, anorexia,vomiting
– Abd pain & distension
– Poor weight gain & wieght loss

• Older children
– Diarrhea, nausea, vomiting
– Abd pain, bloating,
– Weight loss & constipation
• Extraintestinal symptoms• In Late presentation
• Short stature, IDA
• DH, delayed puberty
• Hepatitis, osteopenia
• Arthritis, Epilepsy

• DIAGNOSIS
• Serology
– Anti-gliadin IgA & IgG
– Anti-reticulin IgA
– Anti- endomysial Ig A - high
– Anti-TTG high
• Intestinal biopsy & HPE
– Villous atrophy wt crypt hyperplasia
– Abnormal surface epithelium
– Full clinical & histological remission
• TREATMENT
• Strict gluten free diet

PERSISTENT v/s CHRONIC
• Onset
• Age group
• Wt. loss
• Dehydration
• Recurrence
• Etiology
