perioperative glycemic control implementation · perioperative glycemic control implementation ......
TRANSCRIPT

Perioperative Glycemic Control Implementation
in a Community Hospital
Shaun Sullivan, MD & Janice Whitman,RN MSN CCRN Perioperative Medical Director & CNS Critical Care, APN
Skagit Valley Hospital
Bellingham Anesthesia Associates

Reality
“Public disclosure of the comparative performance of health care providers
is one mechanism for improving quality and controlling health care costs”
Marshall M et al. Dying to Know, Nuffield Trust Series No. 12
The Nuffield Trust and RAND 2000

Before SCOAP Elective Colorectal Resection, CHARS 2000-2003
17.7±38.2%

After SCOAP Elective Colorectal Resection CHARS 2006-2009
9.6±29.4%

Importance of Glucose Control
• Lower infection rates • Better cardiac performance • Better neurologic outcomes • Lower mortality • Reduced readmissions • Lower costs • Improved Patient Satisfaction
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Incidence of Inpatient Hyperglycemia
• Hyperglycemia occurred in 38% of hospitalized patients
– 26% hx of diabetes, 12% had no history of diabetes.
– 16% mortality rate with no previous hyperglycemia diagnosis.
– 3% mortality with diabetes history.
– 1.7% mortality with normoglycemia. – P<.01
• Longer hospital stays; higher admission rates to intensive care units. – Less chance to be discharged to home (required more
transitional or nursing home care).
– Causes: decompensation of DM 1 and 2, Glucocorticoids, vasopressors, stress from illness, injury, infection.
Moghissi, 2009; Umpierrez, 2002

Incidence of severe in-hospital morbidity between patients in whom intraoperative glycemic control was poor (4 consecutive glucose levels > 200 mg/dL) or tight. CV = cardiovascular morbidity; Inf: infectious morbidity; Neuro = neurologic morbidity; Resp = respiratory morbidity. *P<0.05 versus tight control.
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Why is Blood Glucose Control so Important in the Perioperative Setting?
Hyperglycemia vs No Hyperglycemia All Patients
16 14
12
10
8
6
4
2
0
30% of all hyperglycemic patients were not diabetic! All patients Bariatric Colectomy
All p<0.01
Normal
Gluc>18
0
SCOAP data courtesy of Sung (Steve) Kwon

Portland Diabetic Project Cardiac Surgical Wound Infection Data
Furnary©, 2006
0.6%
BG MG/DL

Post-Operative Glucose and Mortality for
Non-Cardiac Surgical Patients
Frisch, 2010; Adapted from Delllinger, 2011

Portland Diabetic Project Concluded:
• In patients who underwent open heart surgery, hyperglycemia increased the incidence of deep sternal wound infection.
• How much?
with BG of 175-225
with BG of 225-250
with BG >250

Univariate analysis comparing risk of adverse outcome between decreasing incremental mean glucose levels during the initial postoperative period. *P≤0.001 overall between mean glucose levels for each individual outcome. #P≤ 0.001 between glucose > 200 mg/dL and glucose 141 −170 mg/dL.. Anesthesiology 2010; 112: 860.
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Graph demonstrating the incidence of perioperative stroke or transient ischemic attack (stroke/TIA), myocardial infarction (MI), or death after CEA as a function of serum glucose level the morning of surgery. The incidence of stroke/TIA, MI, and death were increased (P < 0.05) in patients with preoperative serum glucose greater than 200 mg/dl and greater than 250 mg/dl. Asterisk, P< 0.05. McGirt MJ et al, Neurosurgery 2006
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Factors Associated with Surgical Costs
Reoperation In Hospital Mortality
Infections Length of
Stay
Presented at Washington State Hospital Association Safe Table on April 23, 2014

1 in 4 Surgery Patients Experiences Hyperglycemia Demographic > 65 years
1 in 4 will have Diabetes
2 in 4 are Prediabetic
Presented at Washington State Hospital Association Safe Table on April 23, 2014
Diabetes Care. 2011;33:1783–1788 Ann Surg 2013;257: 8–14

Pathophysiology of hyperglycemia
GLUCOSE
INCREASED GLUCOSE PRODUCTION
DECREASED INSULIN PRODUCTION
INSULIN RESISTANCE
RECEPTOR DEFECT

IMPLICATIONS OF HYPERGLYCEMIA
Decreased tissue perfusion Impaired metabolism
Impaired cardiac function
Decreased wound healing
Pro-thrombotic state
Pro-inflammatory state
Braitwaithe, et al. 2008; Adapted from Inzucchi, Magee, & O’Malley, 2010 Image retrieved from: http://pennstatehershey.adam.com/content.aspx?productId=42&pid=42&gid=000254

‘Stress’ Hyperglycemia— What Happens?
• Cytokines/inflammatory mediators contribute to: – Inability of immunoglobulin to bind with surface of invading bacteria so
decreased bactericidal capacity
– Impaired platelet function
– 54% increased blood stream infections
– 59% increase acute renal failure requiring dialysis and
– 50% increase in blood transfusions
• Relative hypoinsulinemia contributes to: – Decreased insulin sensitivity.
– Unrestrained free fatty acids and hepatic fatty acids.
– Increased ketone bodies and metabolic acidosis.
– Impaired myocardial contractility and larger infarct sizes.
– Glycosuria induced osmotic diuresis and extracellular K+ shift.
Berghe, 2001; Goldberg & Inzucchi, 2005

Presented at Washington State Hospital Association Safe Table, April 23, 2014

Ad
vers
e E
ven
ts (
%)
Increasing Glucose, Worse Outcomes
Postoperative Infection Composite Adverse Events 10.30% 6.50% 5.90%
0% <130 130-150 150-180 180-250
Postoperative Glucose
Presented at Washington State Hospital Association Safe Table on April 23, 2014
Ann Surg 2008;248: 585–591 Ann Surg 2013;257: 8–14

Washington State Hospital Survey March 2014
N = 44 Hospitals
Surgical, Infection
Prevention and Quality Leaders

Pre
op
erat
ive
Washington Hospitals Current Practice
·27% report a well established preop system
Who is screened for hyperglycemia before surgery?
·Screening predominantly DM 10% 20%
All patients
patients and morning of surgery ·Glucose targets
7% Patients with DM Patients with risk
factors for DM
reported were highly variable; from less than 125 to less than 250; one site reported target A1c <9.
63%
No guideline for screening
Unknown
Presented at Washington State Hospital Association Safe Table on April 23, 2014

Intr
aop
erat
ive
Washington Hospitals Current Practice
· 23% report well
established intra-
operative monitoring
Who is monitored intra-operatively?
All patients
8% 12% Patients with DM
·Half report monitoring
only for patients with
diabetes
·Glucose targets, when
established, were highly
variable
25% 3% 52%
Patients with risk factors for DM No guideline for screening Unknown
Presented at Washington State Hospital Association Safe Table on April 23, 2014

Post
op
erat
ive
Washington Hospitals Current Practice
·27% report a well
established postoperative system
·85% monitor patients
postoperatively;
Patients Monitored Post- Operatively
primarily those with
diabetes
·Glucose targets
somewhat variable
3% 12% 7% 78%
All patients Patients with DM Risk factors for DM No coordinated guideline
Presented at Washington State Hospital Association Safe Table on April 23, 2014

Dis
char
ge
Washington Hospitals Current Practice
·15% report a well established
postoperative system
· 82% provide glycemic
Patients Who Receive Hyperglycemia
Discharge Instructions
10% instructions at
discharge mostly DM
·73% report no
established glucose
target
18% 5%
67%
All patients
Patients with DM
Risk factors for DM
No coordinated guideline
Unknown
Presented at Washington State Hospital Association Safe Table on April 23, 2014

Best Practices
Preoperative Screening (prior to day of surgery)
• Check A1c in all patients with known diabetes < 90 days of surgery
• Patients with an A1c of > 8.5 may benefit from further evaluation prior to elective surgery
• Consider checking fasting glucose or A1c in all patients at risk for diabetes or pre-diabetes (i.e. BMI ≥ 30, ≥ 45 years old)

Best Practices Day of Surgery Monitoring
• Check fasting glucose on all patients with
known diabetes on arrival the day of surgery • Check fasting glucose in all patients at risk for diabetes or pre-diabetes (i.e. BMI ≥ 30, ≥ 45 years old)

Best Practices Day of Surgery Protocols
Glucose target: • On arrivaL <180mg/dL • Glucose ≥180mg/dL alone is not a reason to
cancel surgery; develop institutional protocol to manage this and any glucose >100
• If acidemia or hyperosmolar in the setting of hyperglycemia, do NOT proceed with surgery unless urgent/emergent

Best Practices
Intraoperative
Monitor glucose after induction and hourly in all patients with diabetes or initial DOS glucose >100mg/dL
Consider rechecking glucose post incision (stress or steroid induced hyperglycemia)
Glucose target: 100-180mg/dL Rx: Insulin infusion to keep glucose <180mg/dL; Do NOT use sliding scale subcutaneous insulin Develop a clear hypoglycemia protocol for this period

Best Practices
Postoperative – Post Anesthesia Care Unit Monitoring Glucose on arrival to PACU and hourly in:
All patients with a history of diabetes or BG >140mg/dL on DOS Consider for any patient at risk for perioperative stress or stress induced hyperglycemia Rx: Continue insulin infusion if begun intraoperatively Develop transition protocol from insulin infusion to basal- bolus SQ insulin if infusion will not be continued upon transfer to inpatient unit Develop a clear hypoglycemia protocol for this period

Best Practices
Discharge
Monitoring Ensure glucometer for home use Develop patient specific home monitoring recommendations
Glucose target (consistent with ADA outpatient recommendations) Premeal 70-130mg/dL; All other glucoses <180mg/dL
Intervention Ensure patient education Develop clear and patient friendly discharge instruction sheet Arrange follow up with primary care provider within 1 week of discharge Ensure summary of glucose control and goals are communicated to primary care provider and/or other follow-up provider

In H
osp
ital
Mo
rtal
ity
In H
osp
ital
Mo
rtal
ity
Diabetes or No Diabetes In Hospital Mortality
Atlanta Georgia, 2002
16% Washington State, 2013
1.7% 3%
0.6% 1%
2%
Presented at Washington State Hospital Association Safe Table on April 23, 2014
J Clin Endocrinol Metab. 2002;87:978-982. Ann Surg 2013;257: 8–14.
Targets Best Practices-Preoperative
Insufficient evidence to suggest delaying surgery for hyperglycemia alone. Consider optimizing preoperative glucose for patients with A1c >8.5 or frequent glucoses ≥ 180mg/dL.
Glucose <180mg/dL Presented at Washington State Hospital Association Safe Table on April 23, 2014

Targets Best Practices-Intraoperative
Glucose ≥ 180 mg/dL
Glucose 140-180 mg/dL
Glucose 100-180 mg/dL Presented at Washington State Hospital Association Safe Table on April 23, 2014

Targets Best Practices-Postoperative
Glucose ≥ 180 mg/dL
Glucose 140-180 mg/dL
Glucose 100-180 mg/dL Presented at Washington State Hospital Association Safe Table on April 23, 2014

What is a reasonable blood glucose target?
• 80-110 mg/dl in ICU patients.
Van den Berghe et al NEJM 2001.
• 100-180 mg/dl most perioperative patients
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Is strict control dangerous?
· Desai SP et al. 2012; “liberal vs strict control”:
Strict control = 90-120 mg/dl
Liberal control = 120-180 mg/dl
Liberal control not inferior for negative outcomes.
hypoglycemia (< 60 mg/dl) in strict control
group, but no difference in severe hypoglycemia (< 40 mg/dl) Presented at Washington State Hospital Association Safe Table, April 23, 2014

NICE-SUGAR trial 2009
• > 6000 pts
• ICU pts assigned to strict control (80-108mg/dl)
vs liberal control (< 180 mg/dl)
• Severe hypoglycemia (< 40 mg/dl):
6.8% Strict control group
0.5% Liberal group.
However other outcomes were no different. Presented at Washington State Hospital Association Safe Table, April 23, 2014

What is the best way to deliver
insulin?
· SQ vs IV—is your institution using SQ insulin in
the OR?
Presented at Washington State Hospital Association Safe Table, April 23, 2014
Why is glucose control so hard in the OR?
• Lack of knowledge about diabetes/glycemic control • Lack of education about basic treatment facts
-Do you flush your insulin tubing or just start insulin running? -Do you bolus with regular insulin prior to beginning a drip?
• Historical task prioritization in the OR (Glucose control as important as BP, Temp Control)
• POC glucose testing cumbersome, time consuming • Lag time between glucose measurement and Rx

(contd)
· Fear of overtreatment—e.g. hypoglycemia
· Perioperative Patients are more insulin resistant: – Stress hormone release (epi, norepi, cortisol, etc) – Delivery of exogenous catecholamines is common (ephedrine, epi, dopamine, etc) – Underlying conditions (e.g. infection) leading to surgery predispose to insulin resistance – Anesthetic agents may induce insulin resistance (e.g. sevoflurane, isoflurane induce insulin resistance in pigs)—and yet may have an overall positive effect by lowering stress hormone levels.
Presented at Washington State Hospital Association Safe Table, April 23, 2014

What do we know about glucose management in the OR?
• Do anesthesiologists follow established
protocols in testing and treating hyperglycemia in the OR?
• Are established protocols for glucose
management in the OR effective? • Kelly and Nair Studies
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Intra-operative Glucose Control Period
· Measure BG at induction and 1h into case.
· Anesthesia associated with hyperglycemia
even in non-diabetic subjects.
· Measure BG every 1h in Type 1 DM patients.
· Method of glycemic control intra-operatively.
· IV insulin (DM1, critically ill, neurosurgery,
TBI).
· Basal insulin with bolus correction doses.
· Some hospitals have placed glucometers on
every anesthesia cart. Wisse, 2012

Kelly Study
UWMC 2007 -retrospective chart review of pts
at with diabetes undergoing surgery to
determine blood glucose levels and compliance
of anesthesia providers to treat intraoperative
glucose. Both SQ and IV insulin regimens were in
use at the time.
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Kelly Study
•>250 charts reviewed •< 25% of anesthesia providers used insulin in OR
•Few patients hit target range of < 200 mg/dl
•In all patients treated (>200 cases reviewed), only 2 patients reached hypoglycemia
•Both patients had been treated with SQ insulin. •Why does this make sense?
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Nair Study #1
· Used a customized alert system in the
AIMS record keeper to nudge anesthesia
Providers to check a blood glucose level
within ½ hour of start of surgery, & hourly
thereafter (15 min grace period allowed)
· Compliance with glucose testing and compliance with a standard IV insulin Protocol were measured before and after institution of the alert system
Presented at Washington State Hospital Association Safe Table, April 23, 2014

· Compliance with glucose testing improved from 52.6% to 72.1% with the SAM alert system
· Compliance with glucose testing was much higher in cases where SAM was enabled (81%) than when the provider disabled the SAM alert (57.4%)
· However correct insulin dosing only improved from 13.5% to 24.4%--less than ¼ of patients received appropriate treatment.
· Target glucose levels did not improve significantly
Presented at Washington State Hospital Association Safe Table, April 23, 2014

Physiologic Insulin Secretion: Basal/Bolus Concept
Nutritional Insulin
Breakfast Lunch Supper
Insu
lin
(µU
/mL)
Glu
cose
(m
g/d
L)
Basal Glucose
150
100
50
0 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9
A.M. P.M.
Time of Day
Basal Insulin
50
25
0
Nutritional Glucose
Suppresses Glucose Production Between Meals & Overnight
The 50/50 Rule
Adapted from Maynard & Wesorick, Society of Hospital Medicine, 2008
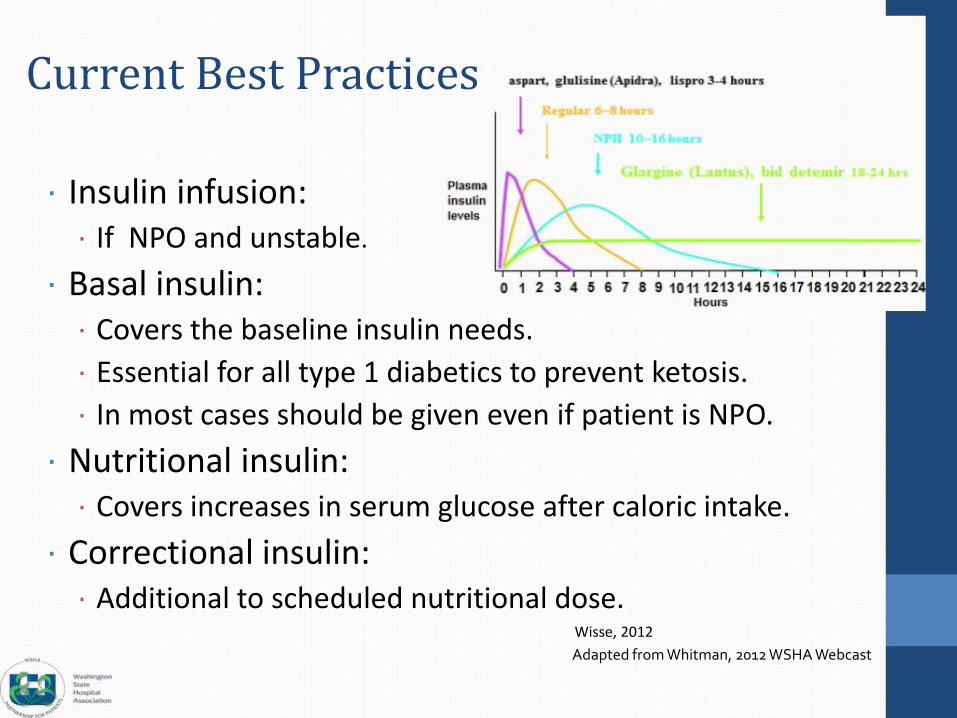
Current Best Practices
· Insulin infusion: · If NPO and unstable.
· Basal insulin: · Covers the baseline insulin needs.
· Essential for all type 1 diabetics to prevent ketosis.
· In most cases should be given even if patient is NPO.
· Nutritional insulin: · Covers increases in serum glucose after caloric intake.
· Correctional insulin: · Additional to scheduled nutritional dose.
Wisse, 2012
Adapted from Whitman, 2012 WSHA Webcast

STOP Oral Hypoglycemic Agents
STOP

Insu
lin In
sulin
Insu
lin
BG
(m
g/dL
) Why Not Sliding Scale?
Target range
Insulin Adapted from Whitman, 2012 WSHA Webcast

Pitfalls of Sliding Scale protocols
• Reactive rather than proactive.
• Problems: stacking, hypoglycemia and hyperglycemia more common.
• Nocturnal hypoglycemia and rebound hyperglycemia.
• Greater glucose variability.
Queale WS. Arch Int Med 1997;157:545; Umpierrez GE. Hosp. Med 2006;1:141
Hirsch IB. JAMA 2009; 301:213; Umpierrez GE. Am. J. Med 2007; 120:563

Pre-Operative Period · ALL patients with a blood
glucose of 180mg/dl and greater.
· Regardless of diabetes diagnosis or not.
· NOT to be used on OB patients, 23 hour admits or those admitted with DKA or HHS (hyperglycemic crises)
Review the protocol


SKAGIT REGIONAL HEALTH
Transition Algorithm SKAGIT VALLEY HOSPITAL
SKAGIT REGIONAL CLINICS INSULIN SUBCUTANEOUS PROTOCOL
· Transition any time of day. · Give basal insulin 2hrs
Attention Physician: All must be checked to initiate order
Blood Glucose (BG) Goals:
Pre-meal Goal - 90-150mg/dL or HgA1C
Goal Postprandial BG: Goal for BG @ 3 am or every 6 hours if NPO
HS Goal 90-180mg/dL or
Blood Glucose (BG) Monitoring Frequency: Before meals & at bed time 2 hours after meals 2-3AM
· If transitioning from IV insulin see Transition Protocols
Basal Insulin: Give units of Glargine (Lantus)
before stopping IV gtt Nutritional
Post-Breakfast
Give units of
Post-Lunch
Give units of
Post-Dinner
Give units of
Bedtime
Give units of
· TDD of SC basal insulin = IV units insulin used last
Glulisine (Apidra) Glulisine (Apidra) Glulisine (Apidra) Glulisine (Apidra)Insulin
Correction Algorithm for Hyperglycemia: To be administered IN ADDITION TO the scheduled insulin dose to correct pre-meal BG.
· Administer correctional insulin immediately post meal Low Medium High Individualized Algorithm · Give full dose if 50-100% of meal eaten · Give half dose if less than 50% of meal eaten · If BG check is every 6 hours for NPO patient, use the pre-meal Algorithm Insulin doses · Correction insulin type will be the same type as nutritional insulin
MANDATORY BG CHECK AT 3AM IF BEDTIME CORRECTIONAL INSULIN GIVEN. IF 3AM BG > 150mg/d USE BEDTIME BG DOSING
LOW DOSE ALGORITHM MEDIUM DOSE ALGORITHM 4 hrs x 5.
(For patients requiring less than 40 units insulin/day)
Premeal BG Additional Insulin
150-199 1 unit 200-249 2 units
(For patients requiring 40 to 80 units insulin/day)
Premeal BG Additional Insulin
1 unit150-199 200-249 3 units
· Also give nutritional insulin if timing with a
250-299 300-349
greater than 349
Bedtime / 3am BG
150-199 200-249
250-299
300-349
3 units 4 units
5 units
Additional Insulin
None
1 units
2 units
3 units
250-299 300-349
greater than 349
Bedtime / 3am BG
150-199
200-249
250-299
300-349
5 units 7 units
8 units
Additional Insulin
None
2 units
3 units
5 units
meal. 4 unitsgreater than 349
HIGH DOSE ALGORITHM
(For patients requiring more than 80 units insulin/day)
greater than 349 7 units
INDIVIDUALIZED ALGORITHM
(For patients requiring an individualized protocol)
Premeal BG
150-199
200-249
250-299
Additional Insulin
2 units
4 units
7 units
Premeal BG
150-199
200-249
250-299
Additional Insulin
300-349 10 units 300-349
greater than 350 12 units greater than 350
Bedtime / 3am BG Additional Insulin Bedtime / 3am BG Additional Insulin
150-199 None 150-199
200-249 2 units 200-249
250-299 5 units 250-299
300-349 7 units 300-349
greater than 349 10 units greater than 349
Hypoglycemia Protocol for blood glucose less than 70mg/dL
A. If pt can take PO, give 15 grams of fast-acting carbohydrate (120mL apple/orange juice, 240mL nonfat milk) B. If patient cannot take PO, give 25mL of D50 as IV push C. Check finger-stick glucose every 15-20 minutes until BG above 100mg/dL
Date: Time: Provider Signature:
SULINSUBCUTANEOUSPROTOCOL

Post-Operative Period
· Initiate for BG
>140mg/dL x2
or >180mg/dL x 1
· Goal range
110-180 mg/dL
· Standard infusions
are regular insulin
100units/100 mLs in
a dedicated line

Signs and Symptoms of Hypoglycemia
· Sweating
· Hunger
· Irritability
· Pallor
· Anxiety
· Dizziness
· Shakiness
· Headache
· Confusion
· Tachycardia
· Trembling
· Weakness
Hypoglycemia can occur without symptoms, so it is important to check blood glucose levels regularly.
Adapted from Whitman, 2012 WSHA Webcast

Treating Hypoglycemia: 3 Steps
Give 15g of glucose or Wait 15 mins Recheck BG – give another fast-acting another 15g if carbohydrate necessary
· 4oz (1/2 cup) fruit juice * Assess for cause · 8 oz (1 cup) milk
· 1 Tbsp honey
· IV Dextrose
Goal to restore BG above 100
Avoid overtreatment (excessive amount of glucose),
which may result in significant hyperglycemia over next 4-6 hrs.
Adapted from Whitman, 2012 WSHA Webcast

Presented at Washington State Hospital Association Safe Table, April 23, 2014

Summary · Hyperglycemia and diabetes are common
perioperatively, each independently associated with worse outcomes
· Treatment with insulin improves outcomes
· Preoperatively optimize if time allows
· Intraoperatively minimize hyperglycemia
· Postoperatively maintain euglycemia (100- 180mg/dL)
· At discharge, re-evaluate the best home regimen, provide targeted education
Presented at Washington State Hospital Association Safe Table, April 23, 2014