perinatal hiv transmission update joan m. duggan, m.d
TRANSCRIPT

PERINATAL HIV TRANSMISSIONUPDATE
JOAN M. DUGGAN, M.D.
MCT
• Objectives:– Identify the CDC antiretroviral treatment strategies
to prevent transmission of HIV from mother to child– Identify the CDC labor and delivery strategies to
prevent transmission of HIV from mother to child– July 8, 2008 CDC/ Public Health Service Task Force
Statement on MCT – http:// AIDSinfo.nih.gov
The Scope of the Problem
• HIV currently infects 33 million people worldwide (Dec 2008: UNAIDS) and millions have died from HIV and co-morbidities– 22 million people in sub-Sahara Africa
• Up to 60% are women
– 1.2 million in N. America + Europe• 370,000 are women

Percent of adults (15+) living with HIV who are female 1990–2007
2.4
Sub-Saharan Africa
GLOBAL
Caribbean
Asia
Latin America
Eastern Europe& Central Asia
0
10
20
30
40
50
60
70
1990 ‘91 ‘92 ‘93 ‘94 ‘95 ‘96 ‘97 ‘98 ‘99 2000 ‘01 ‘02 ‘03 ‘04 ‘05 ‘06 2007
Percentfemale(%)

The Scope of the Problem
• Women infected with HIV (UNAIDS 2008)– 15.4 million women worldwide – The vast majority of these women are of
childbearing age • age 15 – 49
– > 2.0 million children (<15YO) now living with AIDS/HIV primarily by MCT (UNAIDS 2008)

The Scope of the Problem
• A significant number of HIV infected women are pregnant – For example, in 1998, 21% of pregnant women under
age 20 in South Africa were HIV infected• In 2001, it was 15.4% for that age group, but over 30% for
pregnant women ages 25 – 29
– Approximately 370,000 infants and children are infected with HIV worldwide per year
• Now, <250 HIV infected babies born/year in US
– 1995 -- 16,000 HIV infected children born in US
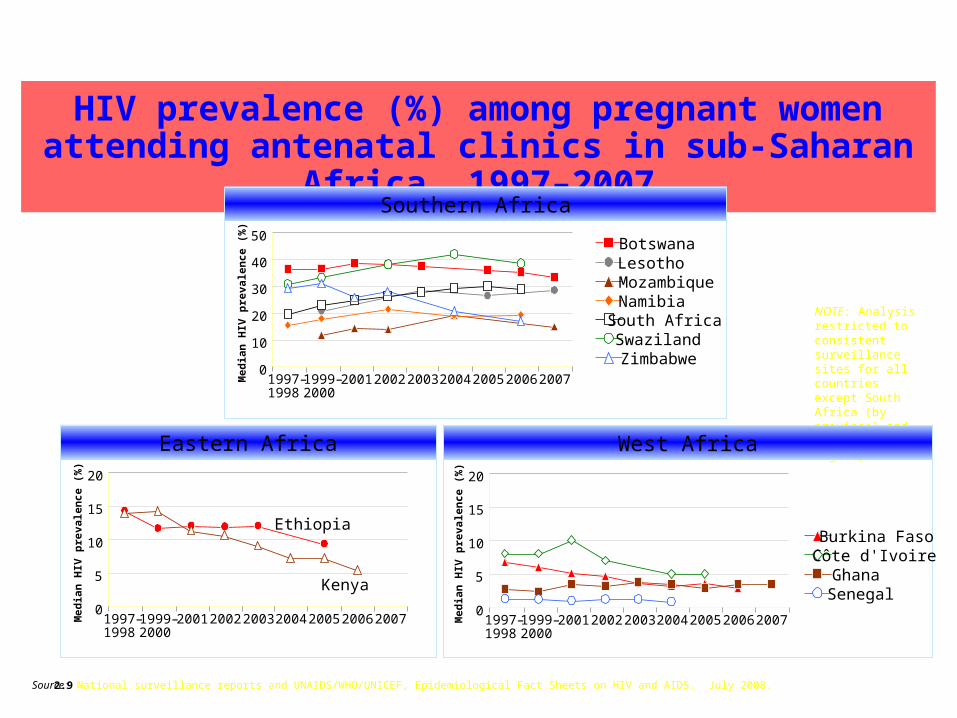
HIV prevalence (%) among pregnant women attending antenatal clinics in sub-Saharan Africa, 1997–2007
NOTE: Analysis restricted to consistent surveillance sites for all countries except South Africa (by province) and Swaziland (by region)
Southern Africa
0
10
20
30
40
Med
ian
HIV
pre
vale
nce
(%
) 50 BotswanaLesothoMozambiqueNamibiaSouth AfricaSwazilandZimbabwe
1997–1998
1999–2000
2001 2002 2003 2004 2005 2006 2007
West Africa
0
5
10
15
20
Med
ian
HIV
pre
vale
nce
(%
)
0
5
10
15
20
Med
ian
HIV
pre
vale
nce
(%
)
Eastern Africa
1997–1998
1999–2000
2001 2002 2003 2004 2005 2006 2007 1997–1998
1999–2000
2001 2002 2003 2004 2005 2006 2007
Ethiopia
Kenya
Burkina FasoCôte d'IvoireGhanaSenegal
2.9 Source: National surveillance reports and UNAIDS/WHO/UNICEF, Epidemiological Fact Sheets on HIV and AIDS. July 2008.
AIDS in Women
• Ohio Data through December 2006– 11,631 people living with HIV/AIDS in Ohio
• 3,066 are women (21%)
– Counties with highest number of HIV/AIDS cases in women in Ohio
• Cuyahoga (Cleveland) – 723 23%
• Franklin (Columbus) – 515 19%
• Hamilton (Cincinnati) – 361 19%
• Montgomery (Dayton) 209 22%
• Lucas (Toledo) – 218 29%
MCT of HIV
• Perinatal transmission of HIV is a growing problem – Until there is a cure, MCT will occur
• Undeveloped countries>>> developed countries
– Transmission rates in developed countries are generally <2% in women diagnosed with HIV and receiving HAART
• Transmission rates in undeveloped countries can range from 14% - 33% (up to 48% in one study)

MCT of HIV
• MCT HIV transmission occurs relatively frequently without treatment– There are no absolute parameters/thresholds for
transmission or protection • Multiple risk factors contribute to a graded response to
transmission (eg – viral load, maternal health)
– When does perinatal HIV transmission occur during the course of pregnancy?
• Important to understand in order to evaluate treatment strategies

Timing of HIV Transmission
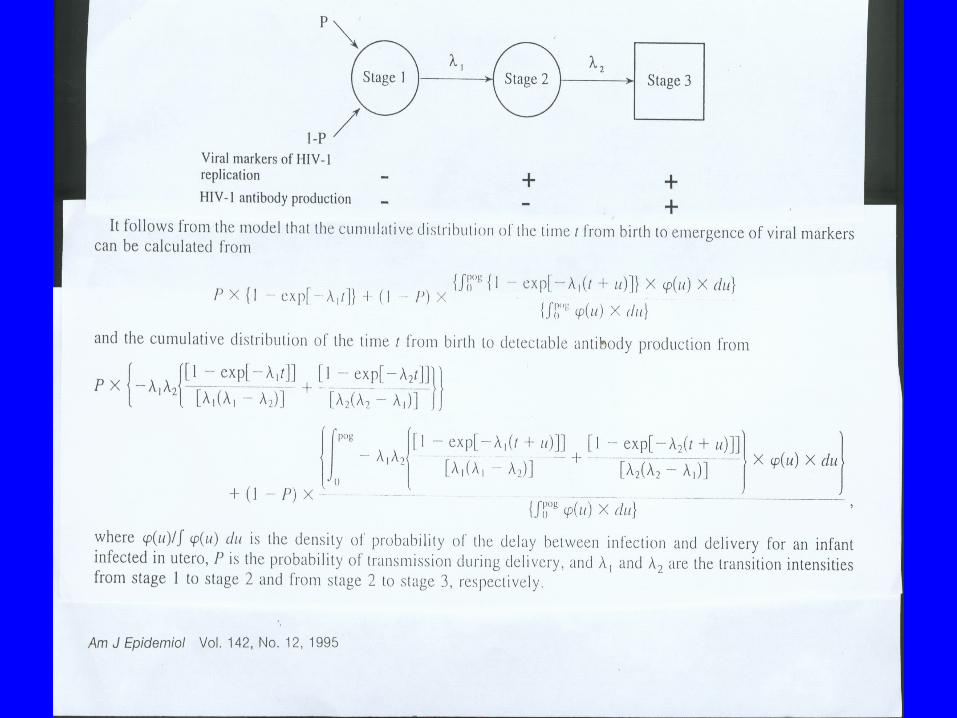
• French Collaborative Study (Am J Epidem 1995:142:1330-7) evaluated non-breast feeding MCT
– Analysis of 495 infants using the Markov model
– 35% (i.e. – one-third) of infections occur in utero• Of these infections, 92% occur in the last 2 months
• HIV can be detected in fetal tissues aborted at 8 weeks gestation
– 65% (i.e. - two-thirds) of cases of MCT occur intrapartum
• These are the usual quoted transmission rates
Timing of HIV Transmission
• Kourtis, et al JAMA 2001 285: 709 –712– Analysis of ten treatment trials (PACTG 076,
PETRA, SAINT, others) for non-breast feeding MCT challenged this view
– Graphic depicts this in the next slide• Around 30% intrapartum transmission
• Around 70% in utero transmission

CD4 counts and Viral loads
• Need to define two terms - CD4 count and HIV viral load - and understand their clinical use – CD4 count
• “T-helper cell” - Coordinating cell for immune system function
• initially the CD4 count falls after infection and then rebounds to levels slightly below those seen prior to infection
• a variety of factors (eg: host genotype, virus genotype, viral load 6 - 12 months after infection) determine long term outcome
• on average, the CD4 count falls by 10 cells/month: normal count>500 cells/mm
CD4 counts
• CD4 Count > 500 (28%) often asymptomatic• CD4 Count 200 - 500 increasing incidence of thrush,
shingles, pneumococcal pneumonia, etc.• CD4 Count <200 (14%) at risk for opportunistic
infections (PCP, candida esophagitis, toxoplasmosis, etc.). Begin PCP prophylaxis. AIDS
• CD4 Count <50 at risk for MAI, CMV. Begin MAC prophylaxis

HIV INFECTION
0100200300400500600700800900
1000
0 1M 2M 3M 6M 2Y 3Y 4Y 5Y 6Y 7Y 8Y 9Y 10Y
TIME
HIV Viral Load
• The amount of virus in blood (either proviral DNA or genomic RNA) can be measured using polymerase chain reaction (PCR) or other nucleic acid test
• Quantities of HIV in plasma can be detected down to 20 copies of virus per cc of blood • This is a reasonable representation of the
amount of virus in lymphoid tissue

HIV Viral Load
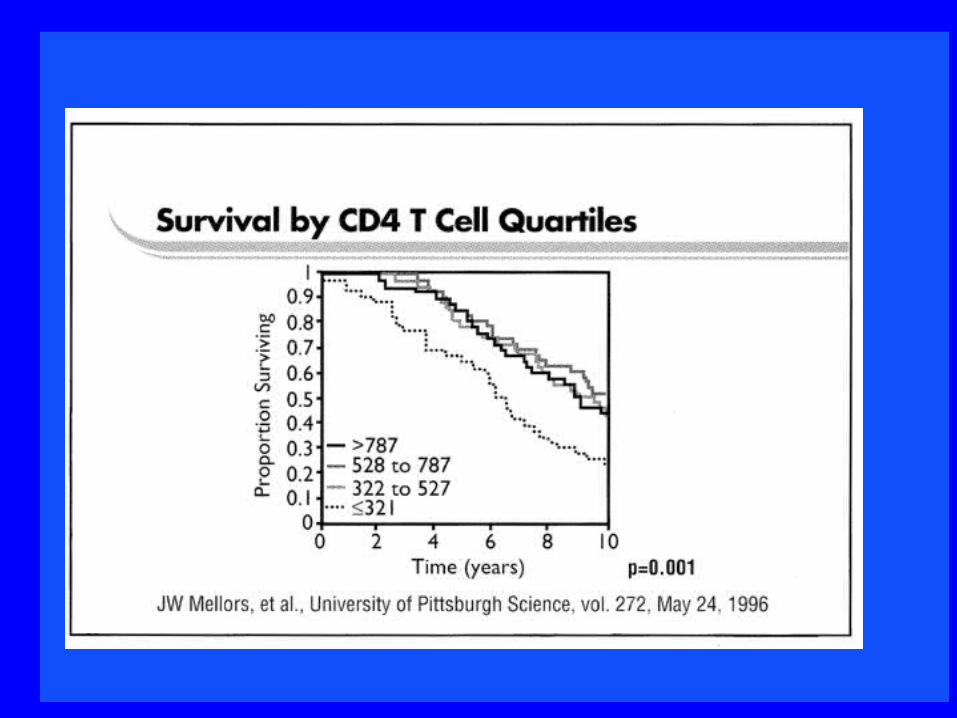
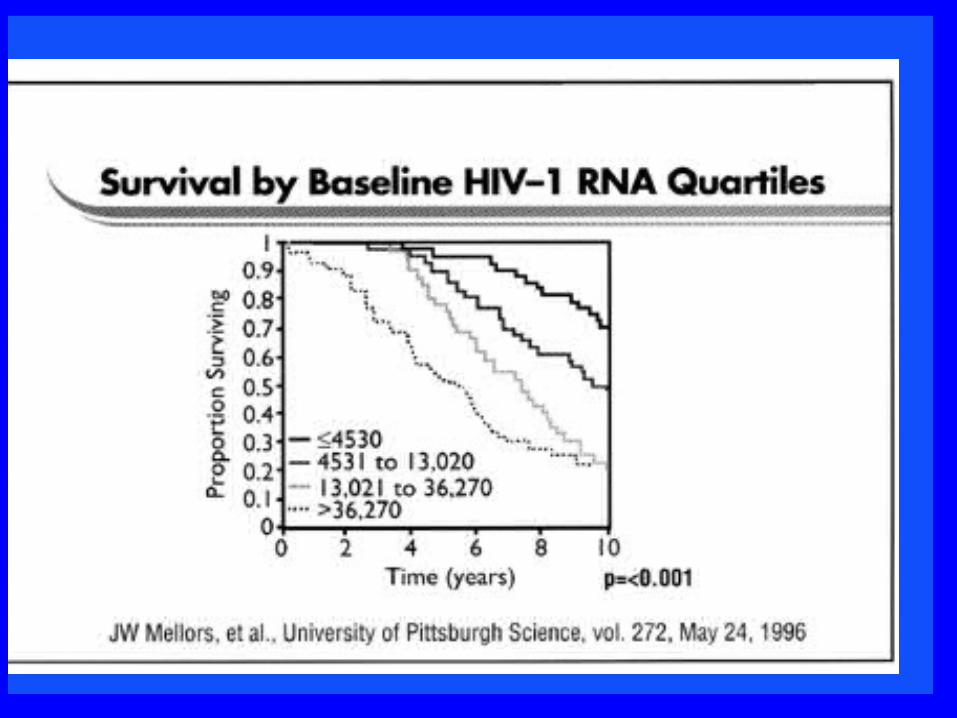
• 209 HIV + men enrolled in MACS study in Pittsburgh 4/84 - 3/85
• Extensive information available on patients - blood samples, CD4 counts, clinical progression
• Viral load is the best predictor of clinical outcome• Like a train heading towards a cliff - CD4 tells
you where the train is - viral load tells you how fast it is traveling
Strategies to Prevent MCT
• PACTG 076:– In 1994, a landmark study was released which
demonstrated for the first time a specific, effective therapy to decrease MCT
– This study revolutionized the care of HIV infected women and set the gold standard for all subsequent care
• Analysis of this study continues (eg. PACTG 219/076)
PACTG 076
• Connor, et al. Reduction of Maternal-Infant Transmission of HIV Type 1 with Zidovudine Treatment. NEJM Nov 3, 1994.– USPHS issued AZT guidelines August, 1994– Randomized, double-blind placebo controlled
study• 477 HIV + pregnant women (14 to 34 week gestation)
with CD4 >200 were enrolled• 409 women went to term (415 live births)
PACTG 076
• Women received AZT or placebo – Ante partum: 100mg po 5x/day– Intrapartum: 2mg/kg IV AZT over 1 hour, then
1mg/kg/hr until delivery– Postpartum: for the neonate 2mg/kg q6hrs po X 6
weeks beginning 8 - 12 hours after birth : no breastfeeding
• Infants were evaluated for HIV infection by peripheral blood mononuclear cell culture at weeks 12, 24, and 78
– ELISA and Western Blot were also performed at weeks 72 and 78
PACTG 076
• Results– No differences in demographics or pregnancy
outcomes between the placebo and AZT groups• Placebo group: 25.5% infected infants at 72 weeks age• AZT group: 8.3% infected infants at 72 weeks age• NEARLY 70% REDUCTION IN MCT• Since publication of this study, use of AZT during
pregnancy has been the standard of care– Intra-partum and post-partum aspects of PACTG 076
currently used as per the original study

How does AZT work in MCT?
• How did AZT cause the reduction in MCT?– Sperling RS, et al. NEJM Nov 28,1996.
– 1) a high maternal viral load is a risk factor for HIV MCT
– 2) AZT reduces the maternal viral load, but the reductions seen only partly explain the decreases in MCT
• Role of AZT resistance in MCT– Eastman PS, et al. JID March 1998.
– Conclusion: AZT resistance did not appear to be a significant factor in MCT/ AZT failure in this study
Beyond AZT – available agents • NRTIs
– AZT (retrovir/zidovudine) – Didanosine/Videx – Stavudine/Zerit – Lamivudine/Epivir – Abacavir/Ziagen– Tenofovir/Viread– Emtricitabine/Emtriva
• NNRTIs– Nevirapine/Viramune*– Delavirdine/Rescriptor– Efavirenz/Sustiva – Etravirine/Intelence
• PIs– Saquinavir (Invirase/Fortovase) – Ritonavir/Norvir– Indinavir/Crixivan– Nelfinavir/Viracept – Amprenavir/Agenerase – Lopinavir+ritonavir/Kaletra– Atazanavir/Reyataz– Tipranavir/Aptivus– Darunavir/Prezista– Fosamprenavir/Lexiva
Beyond AZT – available agents
• Entry inhihitors– Enfuvirtide/Fuzeon– Maraviroc/Selzentry
• Integrase inhibitor– Raltegravir/Isentress
Beyond AZT – Recommended agents
• NRTI– AZT– Lamivudine
• AZT and lamivudine are usually used together as combivir one pill bid
• NNRTI– Nevirapine if CD4 < 250
• Viramune 200mg po qday X 2 weeks, then 200mg po bid
• PI– Lopinavir/ritonavir (increased dose)
• Kaletra three tabs po bid
Beyond AZT
• Combinations of Antiretrovirals are used in pregnant women– HAART – highly active antiretroviral therapy
• In general, avoid 1) Zerit/Videx, 2) Sustiva 3) nevirapine with CD4 >250 4) oral amprenavir solution (dissolved in propylene glycol)
• In general, preferred agents are AZT, epivir, nevirapine with CD< 250, lopinavir/ritonavir
– Combivir (one bid) and Kaletra (three bid)

For the HIV+ Pregnant woman, the CDC suggests...
• AZT should be part of antiretroviral therapy during pregnancy when feasible– PACTG 076 should be followed for intra-partum and post-
partum management– HAART should be routinely used with preferred agents
• Goal of therapy is an undetectable viral load before labor and delivery• HAART should be given for MCT regardless of viral load or need for
treatment of the mother
For the HIV+ Pregnant woman, the CDC suggests...
• Recommendations are outlined in clinical scenarios – July 8, 2008 Public Health Service Task Force – http:// AIDSinfo.nih.gov– 6 Clinic scenarios for HAART use in pregnancy to
decrease MTCT
– 4 Clinical scenarios for mode of delivery to decrease MTCT
CDC Scenario #1
• HIV infected woman receiving HAART who becomes pregnancy– Continue HAART if successfully suppressing
viremia (<50 copies/cc)• Avoid EFV, D4T/ddI , other potential teratogens and
adjust antiretroviral therapy as needed• If stable on NVP, can continue• Consider adding AZT
– HIV resistance testing if viral load >1,000

CDC Scenario #2
• HIV infected pregnant woman who is antiretroviral naïve and has indications for HAART– AIDS, CD4<350, Hx of OI, HIVAN– HIV resistance testing– Initiate HAART regimen
• Use preferred agents including AZT if feasible
• Repeat HIV resistance testing if viral load suppression sub-optimal

CDC Scenario #3
• HIV infected pregnant woman who is antiretroviral naïve and does not require treatment for her own health– HIV resistance testing – Consider HAART after first trimester complete
• Use preferred agents including AZT if feasible
• Repeat HIV resistance testing if viral load suppression sub-optimal
CDC Scenario #3 (con’t)
• HAART to prevent MCT only– Can consider use of AZT alone if HIV VL <
1,000• Controversial and many doctors (including myself)
do not agree with this strategy
– Consider D/C of HAART after delivery

CDC Scenario #4
• HIV infected pregnant woman who is HAART experienced but not currently receiving antiretrovirals– Begin HAART based on resistance testing and
treatment history and information about potential medication teratogenicity
• Use preferred agents including AZT if feasible• Repeat HIV resistance testing if viral load
suppression sub-optimal
CDC Scenario #5
• HIV-infected woman who has received no HAART prior to labor – 1) Give IV AZT during labor and give AZT to the
infant postpartum as per PACTG 076
– 2) Give IV AZT and single dose nevirapine at onset of labor followed by single dose nevirapine to newborn at 48 - 72 hours
• Consider 3-7 days AZT/3TC starting intra-partum or post-partum to decrease nevirapine resistance
– Other “short course” options exist

CDC Scenario #6
• Infants born to mothers who have received no antiretroviral therapy during pregnancy or labor and delivery– Initiate post-partum AZT as soon as possible
(preferably within 6 - 12 hours of birth)• AZT may be used in combination with other
antiretrovirals particularly if the mother has known or suspected AZT resistant virus

CDC Recommendations
• The following are included in all the scenarios– Resistance testing at start of therapy and if
failure to suppress viral load– Continue oral regimen during labor and
delivery and add IV AZT as per PACTG 076
CDC Recommendations con’t
• No increased monitoring is recommended for viral load and CD4 counts
• Discussion of antiretroviral therapy should be noncoercive and the woman makes the final decision about medical therapy
• Refusal to accept medical care (AZT/other drugs) should not result in punitive action or denial of care– All pregnant women who have received antiretroviral
therapy during pregnancy should be reported to the Antiretroviral Pregnancy Registry
“Short Course” Therapy for MCT
• HIVNET 012 : – Single dose nevirapine to mother in labor and single dose
nevirapine a day to infant 2 -3 days later and breast feeding allowed: 47% reduction in MCT
• 65% of women in this study developed nevirapine resistance (CROI,2005)
• Use of nevirapine in subsequent pregnancies being studied
• Thailand– AZT 2x/day starting at 36 weeks and every three hours
orally during labor and no breast feeding: 50% reduction in MCT

“Short Course” Therapy for MCT
• Cote d’Ivoire– AZT 2x/day starting at 36 weeks and every three hours
orally during labor and breast feeding allowed: 37% reduction in MCT
• PETRA trial– AZT 300 mg given every three hours and lamivudine
150mg given every 12 hours during labor, and then AZT/lamivudine given for one week to mother and child (all meds given orally): 37% reduction in MCT to date
CDC Scenario #1 – Delivery
• HIV infected woman presenting > 36 weeks gestation, no HAART, no labs available before delivery– Start HAART or PACTG 076
– Consider C-section at 38 weeks to reduce MCT• If scheduled c-section, give AZT beginning 3 hours before
surgery (loading dose and 3 hours infusion)
• Prophylactic antibiotic therapy– Cefotetan, cefoxitin, cefazolin, amp-sulbactam, clinda/FQ, etc
• Post-partum PACTG 076

CDC Scenario #2 - Delivery
• HIV infected woman who is on HAART, but has a viral load >1,000 at 36 weeks– Continue HAART – Consider C-section at 38 weeks to reduce MCT
• If scheduled c-section, give AZT beginning 3 hours before surgery (loading dose and 3 hours infusion)
• Prophylactic antibiotic therapy prior to C-section
• Post-partum PACTG 076
CDC Scenario #3 - Delivery
• HIV infected woman who is on HAART, and has an undetectable viral load at 36 weeks– No information on elective C-section reducing
the <2% MCT when VL undetectable to an even further level
• Study in CID Feb 2005 challenges that view
• Vaginal delivery if feasible
CDC Scenario #4 - Delivery
• HIV infected woman scheduled for elective C-section who presents with early labor or rupture of membranes– Start IV AZT immediately
– Labor progressing rapidly, deliver vaginally • If minimal cervical dilation, can administer loading dose AZT
and proceed with C-section
• Can use pitocin to expedite delivery
• Avoid scalp electrodes, other invasive monitoring procedures
• Post-partum PACTG 076
HIV Testing in Pregnancy
• CDC is recommending “adoption of simplified HIV testing procedures….CDC will promote recommendations for routine HIV testing of all pregnant women, and, as a safety net, for the routine screening of any infant whose mother was not screened.”– MMWR April 18, 2003/vol 52/no. 15

Conclusions
• HIV MCT is largely preventable– PACTG 076 rates @25% without treatment
• Most centers treating HIV in pregnancy report <1%
– Need to get testing during pregnancy• If testing not done in pregnancy, test neonate/child ASAP• Consider testing in the second and third trimester in selected
areas and patients
– Need to institute appropriate therapy and plan for appropriate mode of delivery
– Antiretroviral agents recommended for use in pregnancy are relatively safe
Conclusions
• HIV MCT is largely preventable– Three antiretroviral agents recommended– C-section for VL> 1,000– No breast-feeding– Diagnosis of HIV during pregnancy
• Test older children
– Birth of an HIV infected infant is a sentinel event representing missed testing and treatment opportunities