peri 765 ~ 13 introduction to periodontal surgery 2013 6 slides per page
TRANSCRIPT
8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 1/15
11/21/20
SPECIAL TOPICS IN
PERIODONTAL THERAPY
PERI 765
LECTURE # 13
2013
Loma Linda UniversitySchool of Dentistry
Department of Periodontics
Introduction to PeriodontalSurgery
By ADRIAN MOBILIA D.D.S.
Periodontal Therapy
Data collection, Periodontal Diagnosis and Treatment Plan
Motivation and OHC
Modification of overhanging restorations, S&RP, polishing , fluoride topical
Interim evaluation
Re-evaluation
Diagnosis and treatment of acute infections
Supplemental Therapy
Re S&RP
Medication
Surgery
MAINTENANCE
Scheduling for Perio Surgery
Following initial therapy and re-evaluation
(for plaque related periodontal destruction)
Scheduling for Perio Surgery
• After temporary splinting of mobile teeth
Scheduling for Perio Surgery
• After temporary splinting of mobile
teeth

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 2/15
11/21/20
Scheduling for Perio Surgery
Prior to Ortho, Restorative,
Prosthodontics
Patient Preparation for Surgery
• Oral Hygiene Assessment
• Psychological
• Pre-surgical records
Radiographs
Charting
Etc.
• Pre-medication
• Nutritional and diet preparation
• Pre-operative medical assessment
Post-operative Care
• Inform patient verbally
• Also have written instructions
Objectives of the Periodontal Surgery
1.Access and visibility of the calculus
Increase SRP effectivenessLess tissue trauma
2. Pocket Depth Reduction
Improve long term stabilityEnhance maintenance by the patient and therapist
Objectives of the Periodontal Surgery
3. Modification of Osseous Defects
Establish physiologic architecture for the bone and soft tissues through
regeneration or resection
4. Repair or Regenerate the Periodontium
5. Provide Acceptable Soft Tissue ContoursEnhance plaque control and maintenanceImprove esthetics
Pocket Depth Deposit RemovalCaffesse et al
Probing Depths Roots Cleaned
1-3 mm 83%
4-6 mm 43%
>6 mm 32%

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 3/15
11/21/20
Molars vs. non-molarsNordland, et al.
Limited accessibility at molar furcation
defects reduces the efficacy of non-surgical
therapy (S/RP).
Drug induced overgrowth Drug induced overgrowth
Potential Disadvantages:
• Increased bone loss resulting from trauma,dehydration, prolonged surgical exposure
• Generally 0.5-1.0mm of crestal bone loss
after surgery• Up to 2.5mm loss in thin bony places if
poor flap adaptation
• Heat-induced osseous necrosis whenremoving bone:
≥ 47° C ≥ 1 min.
Surgical treatments
Resective
1.Gingivectomy / Gingivoplasty2.Distal Wedge3.Modified Widman4.Osseous5.Crown Lengthening with bone removal6.Tooth Hemisection7.Root Amputation
8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 4/15
11/21/20
Reconstructive
1.Flap Debridement2.Pedicle Soft tissue Grafts3.Free soft tissue Grafts4.Hard tissue grafts5.Guide tissue regeneration
Surgical treatments
POCKET MANAGEMENT
RESECTIVE
Gingivectomy
Osseous
NEW ATTACHMENTRepair
Regeneration
MUCOGINGIVALGingival width
Root Coverage
PRE -PROSTHETICCrown lengthening
Ridge Augmentation
CLASSIFICATION BASED ON GOALS
Principles of Periodontal Surgery
1.Know you patient’s health history
2.Develop a treatment plan related to therestorative treatment plan
3.Know the anatomy of the surgical site
4.Profound anesthesia
5.Aseptic technique
6.Atraumatic tissue management (smooth
incisions, careful flap reflection, carefulflap manipulation)
Principles of Periodontal Surgery
7. Hemostasis
8. Atraumatic suturing techniques(smallest needles for the area, sutures inkeratinized tissue, take adequate bites oftissue)
9. Obliterate dead space between flap andbone
10. Promote an stable wound healing
Surgical Anatomy Surgical Anatomy

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 5/15
11/21/20
Surgical Anatomy
• External bevel
• Sulcular
• Internal bevel
• Scalloped
• Linear
• Vertical releasing
Types of Incisions
• External bevel
Types of Incisions
External bevel
Types of Incisions
• Sulcular
Types of Incisions Types of Incisions
• Internal bevel

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 6/15
11/21/20
• Internal bevel
Types of Incisions
• Scalloped
Types of Incisions
• Linear
Types of Incisions
Vertical releasing
Increases access and allowsdisplacement of the flap
Types of Incisions
Types of Incisions
• Vertical releasing
Dr. Adrian Mobilia
• Vertical releasing
Types of Incisions

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 7/15
11/21/20
Incorrect placement of a
Vertical incision
Center of the tooth
Center of the papillae
Over the bone defect
Cut back incision
Used in pediculate flaps that are laterallydisplaced
Types of Incisions
Cut back incision
Used in pediculate flaps that are laterallydisplaced
Types of Incisions
Dr. Stephen Silston
Dr. Stephen Silston Dr. Stephen Silston

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 8/15
11/21/20
Dr. Stephen Silston Dr. Stephen Silston
Dr. Stephen Silston Dr. Stephen Silston
Periosteal incision
Releases flap tension allowingdisplacing coronally the flap
Types of Incisions
Dr. Adrian Mobilia

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 9/15
11/21/20
Dr. Adrian Mobilia Adrian Mobilia DDS
Adrian Mobilia DDS Adrian Mobilia DDS
Adrian Mobilia DDS

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 10/15
11/21/20
Classification of Flaps
• Full thickness (epithelium, connective and periosteum)
• Partial (split) thickness (epithelium and connective)
• Undisplaced
• Displaced (Pediculate flaps)
• Apically displaced
• Coronally displaced
• Laterally displaced
Pediculate Flaps
Designed to be placed in a position different thanthe original
Most of the time have two vertical incisions
The base of the flap should be equal or larger thanthe coronal portion
To preserve a good irrigation the high/base ratioshould not exceed 2:1
Pediculate Flaps
The ratio flap height : flap base should not exceed 2:1
Periodontics Medicine, Surgery and Implants. Rose & Mealey
Pediculate Flaps
Periodontics Medicine, Surgery and Implants. Rose & Mealey
Classification of Flaps
• Full thickness • Full thickness
Classification of Flaps

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 11/15
11/21/20
• Partial (split) thickness
Classification of Flaps
• Partial (split) thickness
Classification of Flaps
• Undisplaced
Classification of Flaps
• Displaced – apically
Classification of Flaps
• Displaced – apically
Classification of Flaps
• Displaced - coronally
Classification of Flaps
8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 12/15
11/21/20
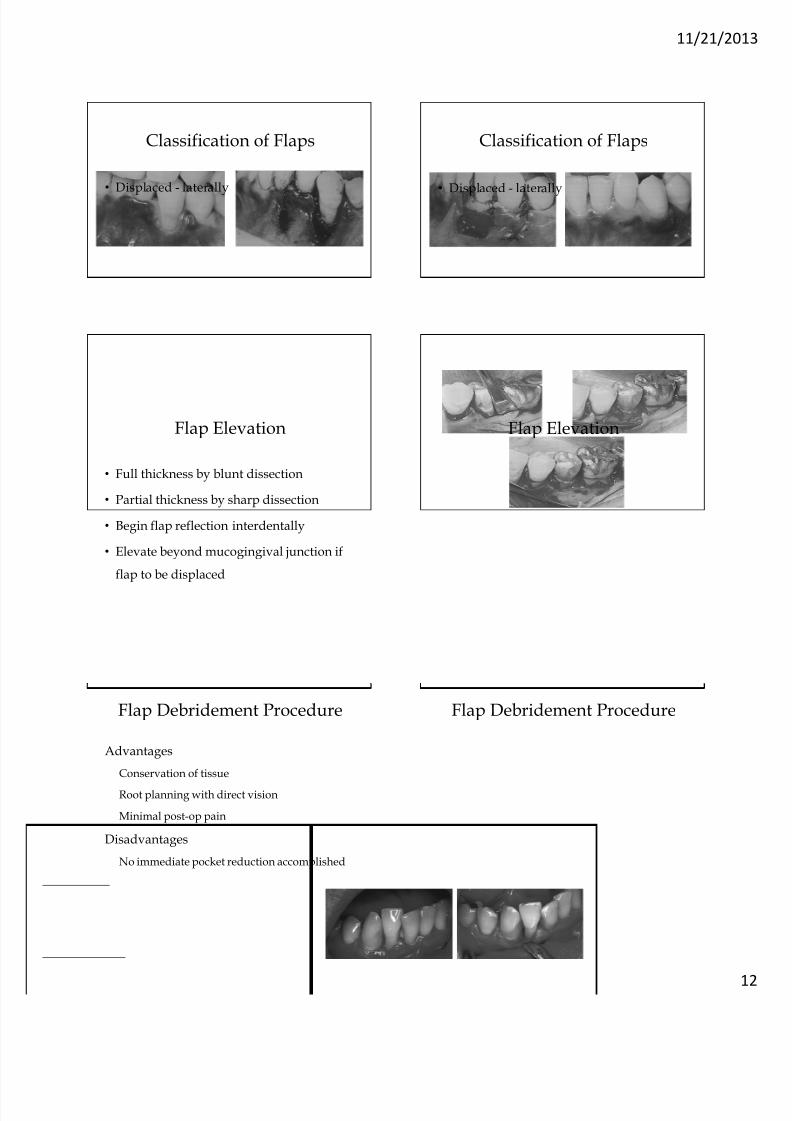
• Displaced - laterally
Classification of Flaps
• Displaced - laterally
Classification of Flaps
Flap Elevation
• Full thickness by blunt dissection
• Partial thickness by sharp dissection
• Begin flap reflection interdentally
• Elevate beyond mucogingival junction if
flap to be displaced
Flap Elevation
Flap Debridement Procedure
Advantages
Conservation of tissue
Root planning with direct vision
Minimal post-op pain
Disadvantages
No immediate pocket reduction accomplished
Flap Debridement Procedure
8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 13/15
11/21/20
Flap Debridement Procedure Flap Debridement Procedure
SutureObjective:
Flap adaptation and stabilization of the wound
• Flap must achieve its position passively
• Do not rely in sutures to pull beyond the passiveposition
• Any tension in the flap increases the chance ofcomplications
Purpose of Suturing
Approximation of flap (wound) edges, asmuch as possible, for Primary or SecondaryIntention closure.
Adaptation of soft tissues to teeth, rootstructure or implants.
Compression of flap to the underlyingconnective tissue or bone to minimize
hematoma formation, (dead space).
Ideal Suture
• Biologically inert
• Strong
• Dissolves/absorbs in body fluids after
serving its purpose• Loses strength at the same rate that the
tissues gain strength
• Easy to handle
• Easy to sterilize
• High knot security
Choice of Suture material
Depends upon:
• Properties of the suture material
• Absorption rate
• Handling characteristics
• Knotting properties
• Size of the suture material
• Type of needle to be used

8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 14/15
11/21/20
Sutures are classified according tothe number of strands
Monofilament vs. MultifilamentStrands
Monofilament vs. MultifilamentStrands
Monofilament sutures:
• Single strand of material.
• Less resistance as they pass through
tissues:
•
Less infection.
Monofilament vs. MultifilamentStrands
Multifilament sutures:
• Several filaments, or strands, twisted orbraided together.
• Greater tensile strength, pliability andflexibility.
• May be coated to help them pass relativelysmoothly through tissues/ enhance handlingcharacteristics.
Monofilament vs. MultifilamentStrands
Absorbable vs.Non-Absorbable
Sutures are classified according to theirdegradation properties:
1- Absorbable
2- Non-Absorbable
Absorbable Sutures:
• Lose their tensile strength in less than 60
days.
• Natural absorbable sutures are destroyed by
proteases (proteolysis) while synthetic
absorbable sutures are hydrolyzed.
Absorbable vs.Non-Absorbable
8/12/2019 Peri 765 ~ 13 Introduction to Periodontal Surgery 2013 6 slides per page
http://slidepdf.com/reader/full/peri-765-13-introduction-to-periodontal-surgery-2013-6-slides-per-page 15/15
11/21/20
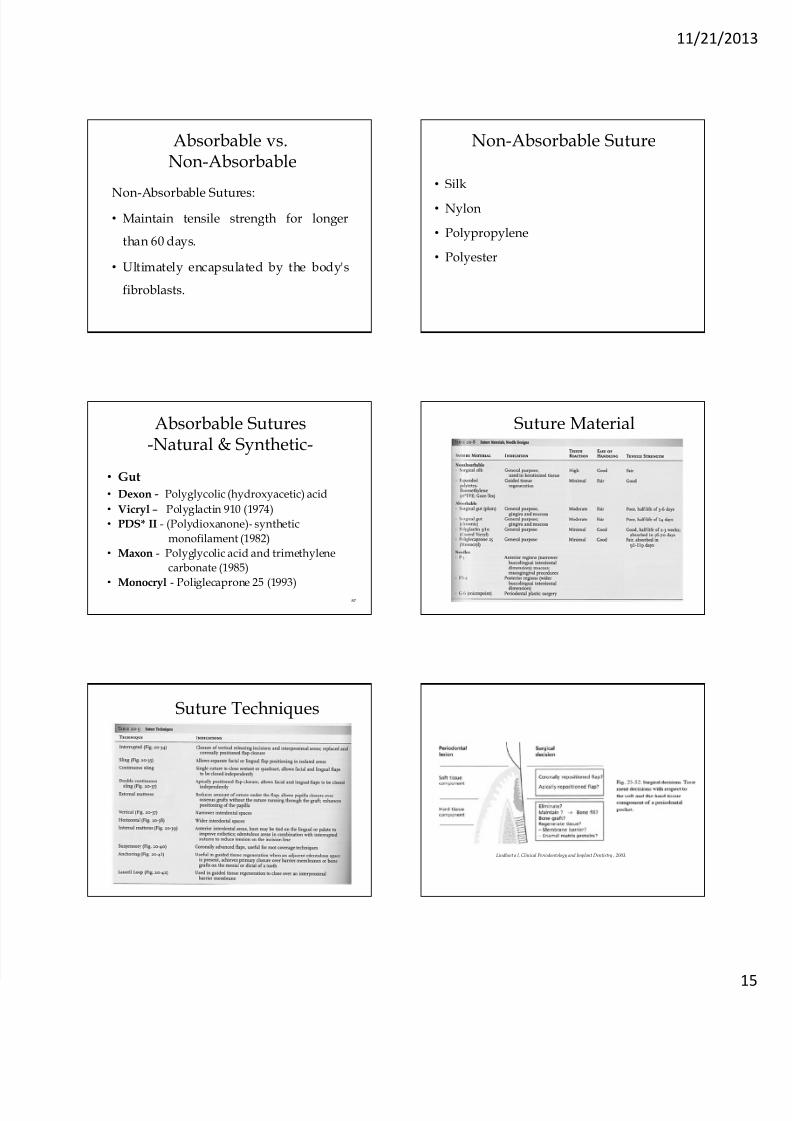
Non-Absorbable Sutures:
• Maintain tensile strength for longer
than 60 days.
• Ultimately encapsulated by the body's
fibroblasts.
Absorbable vs.Non-Absorbable
• Silk
• Nylon
• Polypropylene
• Polyester
Non-Absorbable Suture
Absorbable Sutures-Natural & Synthetic-
• Gut
• Dexon - Polyglycolic (hydroxyacetic) acid
• Vicryl – Polyglactin 910 (1974)
• PDS* II - (Polydioxanone)- synthetic
monofilament (1982)
• Maxon - Polyglycolic acid and trimethylene
carbonate (1985)
• Monocryl - Poliglecaprone 25 (1993)
87
Suture Material
Suture Techniques
Lindheet a l, Clinical Periodontology and Implant Dentistry , 2003.