performance improvement: how do we improve? deb syverson, rn, bsn, emt trauma program manager...
TRANSCRIPT

Performance Improvement: How Do We Improve?
Deb Syverson, RN, BSN, EMTTrauma Program Manager Sanford Health – Fargo, ND

Performance Improvement: How Do We Improve?

State and Regional Trauma Performance Improvement

Covering the Basics
Establish statute/regulations that provide confidentiality and discovery protection for all activities of Region and Statewide PI:• Trauma Registry Data• Performance Improvement process
NDCC Chap 23-01.2-01 A trauma PI program to monitor the performance of the trauma system. The proceedings and records of the program are not subject to subpoena or discovery, or introduction into evidence in any civil action arising out of any matter that is the subject of consideration by the program.
• Basic fundamentals in starting Regional and State Performance Improvement
• Developing PI Process/Guidelines• Indicators/Outcomes from ND
Performance Improvement
OBJECTIVES
• Trauma Registries are a MUST— All trauma designated and non-designated
facilities should be participating.— Determine statewide inclusion criteria for trauma
patient population you want in the registry— Create a trauma data dictionary for all users
GOOD DATA IN = GOOD DATA OUT Very important that all users are interpreting the
fields correctly Must provide yearly trainings and modules for new
users.
COVERING THE BASICS
• Trauma Registry Cont….— Oversight of Trauma Registry Data
Typically your lead agency State Epidemiologist Data Analyst
Checking for validity, generating reports, monitoring timely submissions
Registry Training
COVERING THE BASICS

• ND – 4 Regional Trauma PI Committees— Led by Level II Trauma Center Physician Chair,
State Medical Director, and State TPM— Multidisciplinary
Trauma Coordinators, Physicians, Advanced Practice Providers, and EMS from all level trauma centers in the region.
— Meetings held quarterly Video/teleconferencing
REGIONAL PI: HOW DO WE (ND) DO IT?

• Development of PI Guidelines/Plan— Mission: Continuously improve trauma care
outcomes and monitor trauma patient care and system issues and provide education.
— Objectives: Trauma Coordinators, Physicians, Advanced Practice Providers, and
EMS from all level trauma centers in the region - Improve patient outcomes
Identify performance improvement projects Identify education opportunities Maintain confidentiality Feedback to providers, facilities, EMS, and the State Trauma
Committee NON PUNITIVE!!!!!!
REGIONAL PI: HOW DO WE (ND) DO IT?

• Process – what do we look at?— All deaths from the Level IV and V trauma centers— Patients with an ISS > 15 that were transferred with:
Trauma Code not activated when patient met criteria GCS <8 and no definitive airway Transfer times > 2 hours Trauma team leader response times > 20 minutes Pneumo/Hemothorax identified and chest tube not
placed Pediatric patients less than 16 years of age that had CT
scans (Implemented in 2011)
REGIONAL PI

• Process Cont….• State Trauma Registry used to pull cases• Cases reviewed by the State Medical Director
and State TPM• Facilities present cases at the regional meeting• Recommendations and/or education is
provided at the meeting along with written letter to the individual facilities or EMS agencies
• Regional Chair provides regional updates/issues to the State Trauma Committee
REGIONAL PI
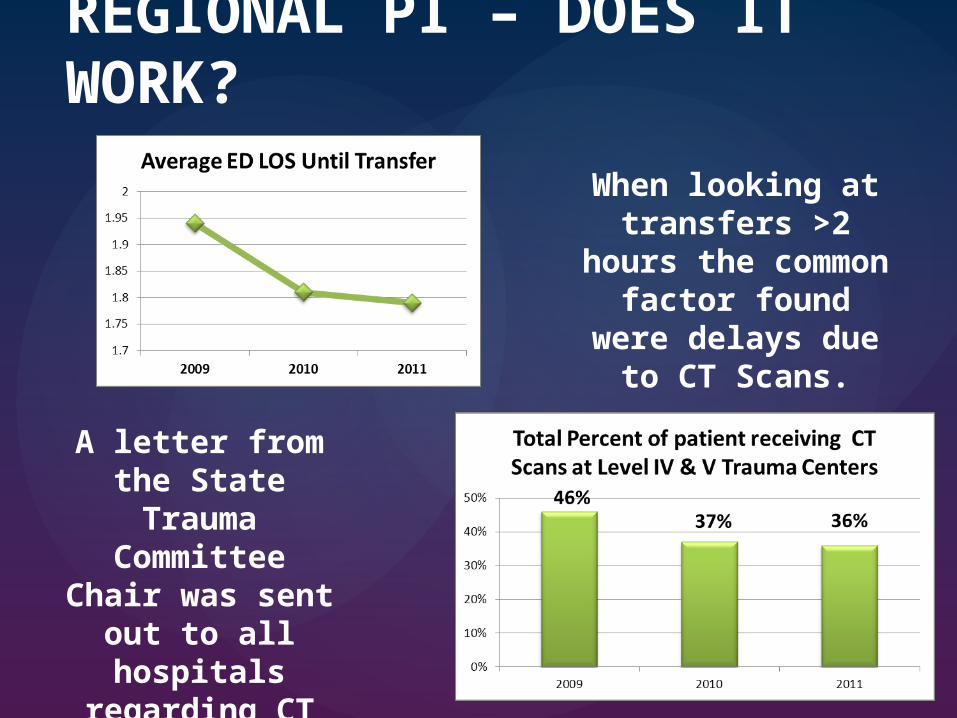
REGIONAL PI – DOES IT WORK?
When looking at transfers >2 hours the common factor found were delays due to CT
Scans.
A letter from the State Trauma
Committee Chair was sent out to all
hospitals regarding CT scans delaying
transfers.

REGIONAL PI – DOES IT WORK?
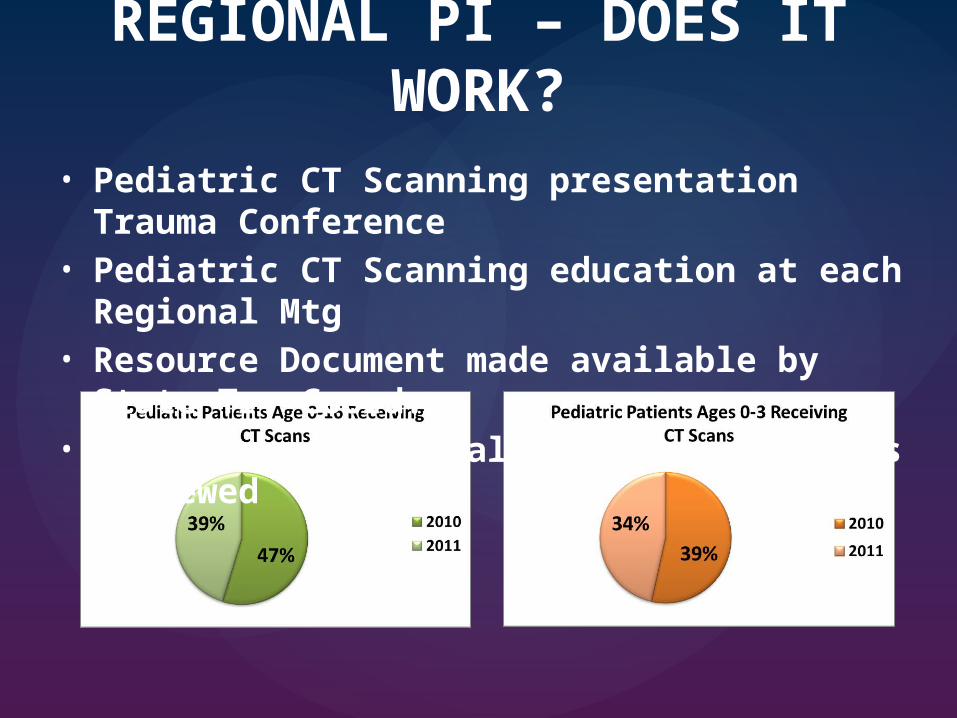
REGIONAL PI – DOES IT WORK?• Pediatric CT Scanning presentation Trauma Conference• Pediatric CT Scanning education at each Regional Mtg • Resource Document made available by State Tr. Coord.• Added as a “regional PI filter” – cases reviewed
Ben
chm
arki
ng!
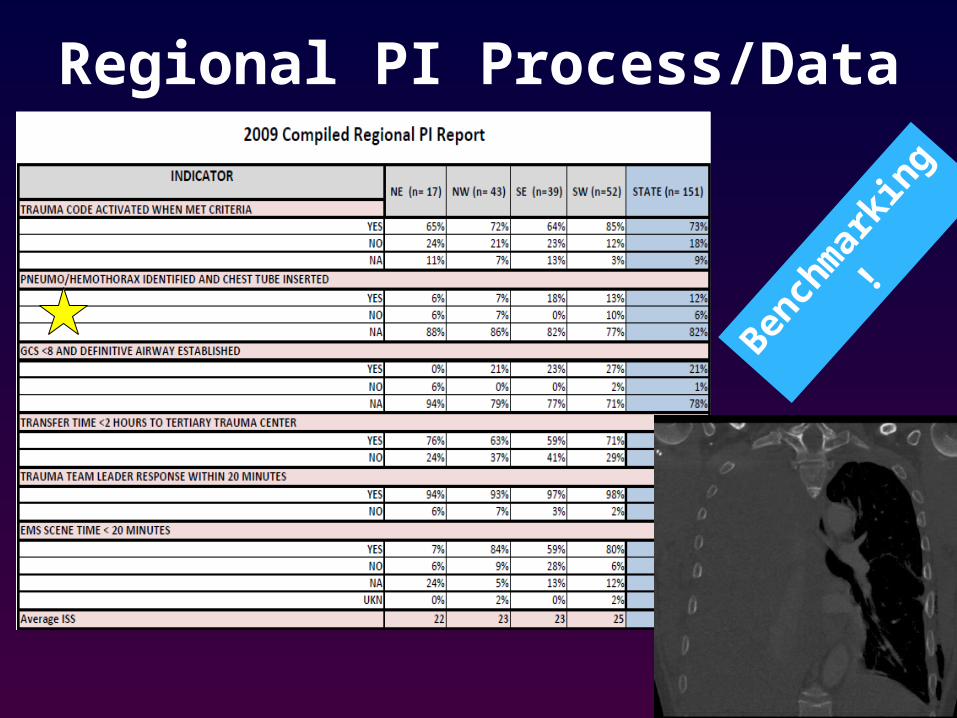
Regional PI Process/Data

ED Intubated / GCS2
Data Report for Regions

Data Report for RegionsBenchmarki
ng!

Data Report for Regions

Regional PI ProcessRequesting Information
• Data is pulled from state trauma registry• Indicators “falling out”• State Trauma Coordinator contacts hospital for “abstract”• State Trauma Coordinator informs “Level IIs” if the patient
was transferred to higher level of care – to obtain follow information
• Data collated, form distributed (confidential)• Cases presented at regional meetings

Regional PI Process

Regional PI Process
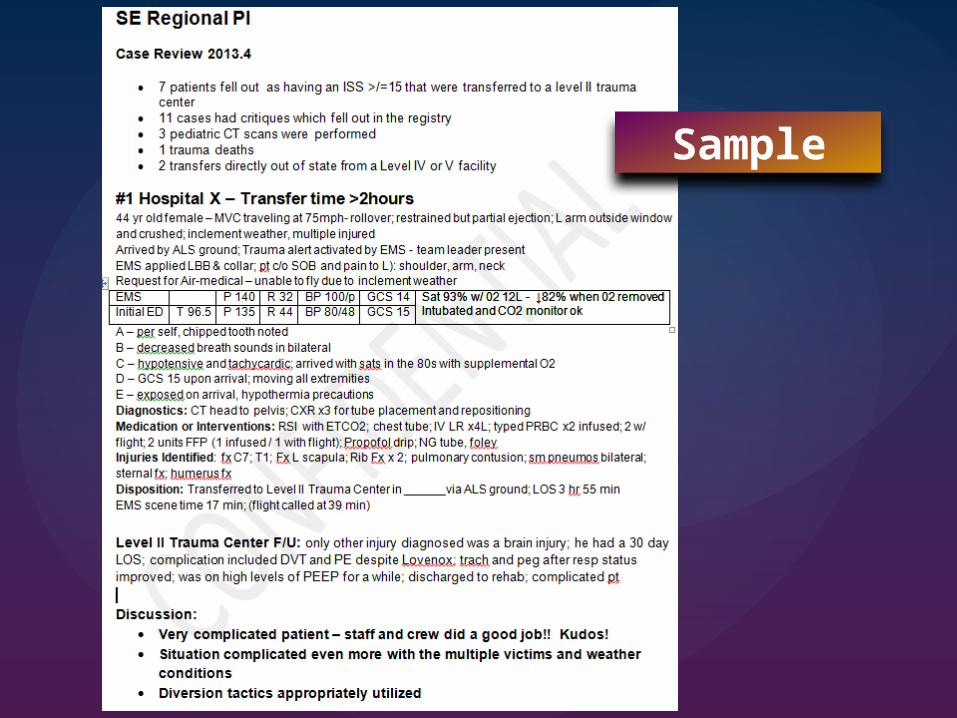
Sample

2009 vs. 2013
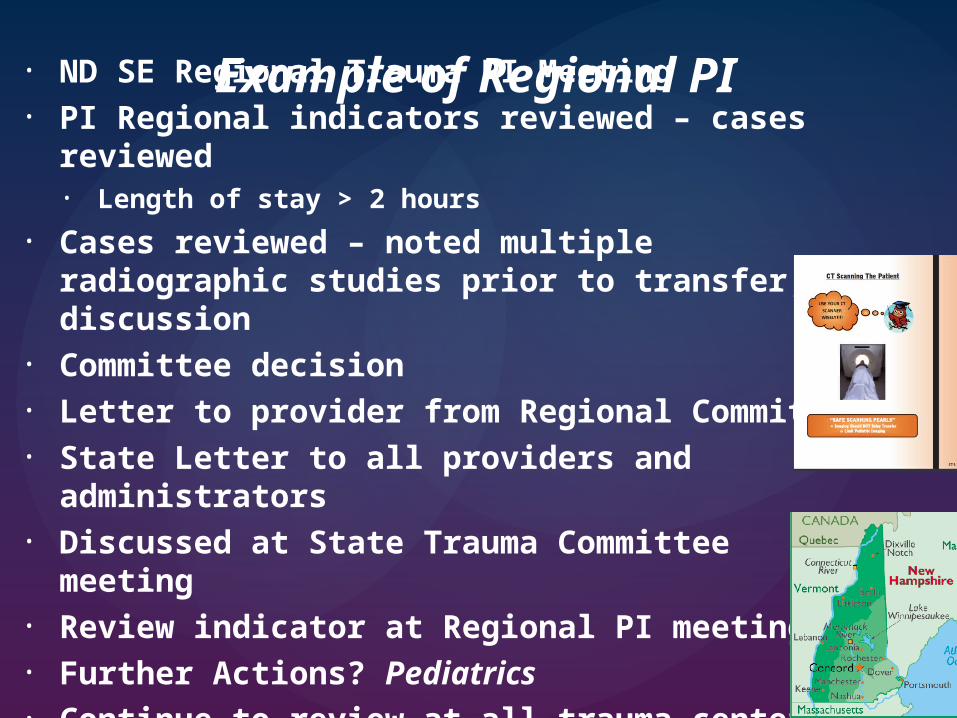
• ND SE Regional Trauma PI Meeting• PI Regional indicators reviewed – cases reviewed
• Length of stay > 2 hours
• Cases reviewed – noted multiple radiographic studies prior to transfer, discussion
• Committee decision• Letter to provider from Regional Committee• State Letter to all providers and administrators• Discussed at State Trauma Committee meeting• Review indicator at Regional PI meetings • Further Actions? Pediatrics• Continue to review at all trauma centers!
Example of Regional PI

Com
pile
d N
D R
eg
ion
al In
foS
am
ple
pag
e 1
on
ly

Minnesota – South Dakota
PERFORMANCE IMPROVEMENT

SD
Reg
ion
al P
I
• State Trauma Committee— Multidisciplinary— Meetings held every other month by video/teleconference
• State PI Guidelines — Mission / Objectives / Process
• Registry Submissions• Indicators:
— Transfers out of State---- “Transfer out of Level II trauma centers”
— Deaths – at level II Trauma Centers---- “predicted to Survive and Died <85 y/o”
STATE PI – HOW DO WE DO IT?

• Trauma Registry Date Submissions by All Hospitals
— Reports provided to the STC on facilities that were not submitting data to the registry
— Data submission essential criteria for trauma designation
STATE PI – Does it work?
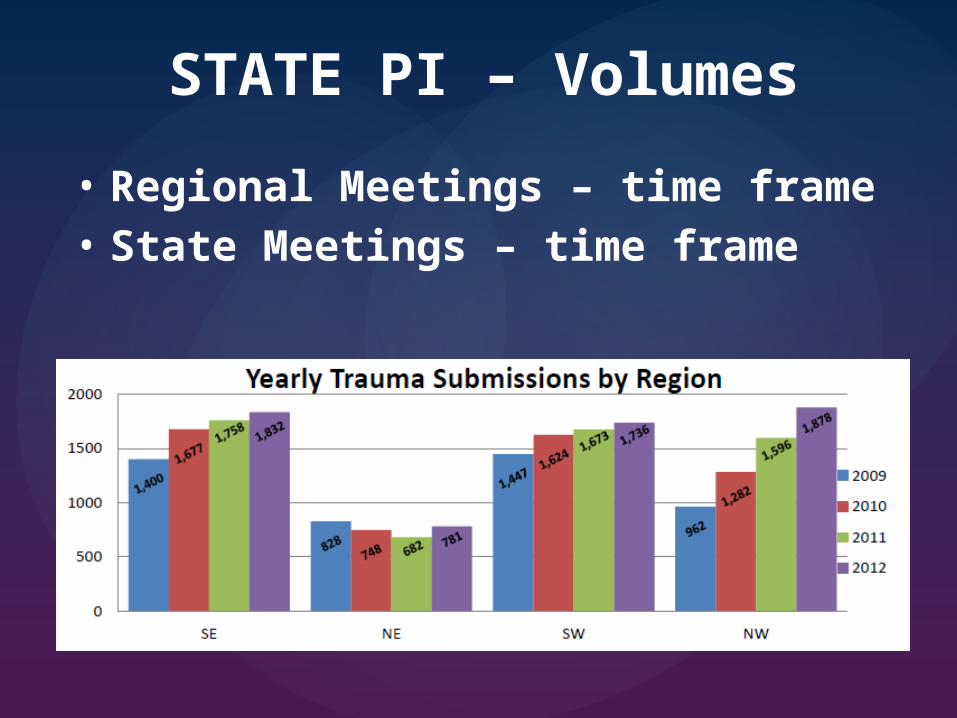
• Regional Meetings – time frame• State Meetings – time frame
STATE PI – Volumes

2013 Quarter 4
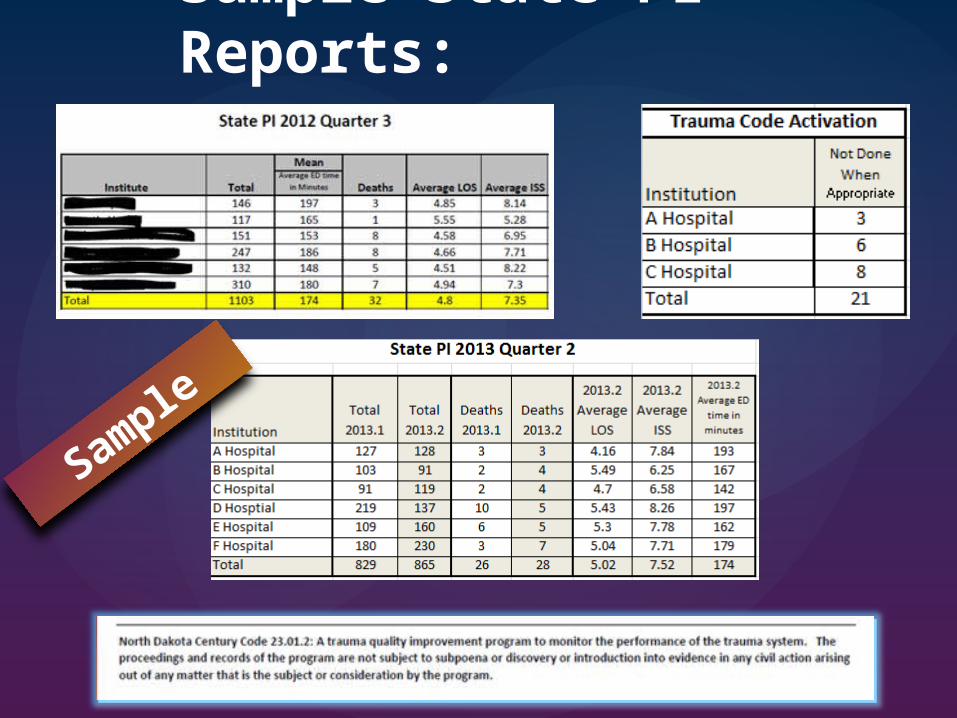
Sample State PI Reports:
Sample

Sample State PI Reports:
Sample

Overall Regional & State PI Impact
• Pleasantly Surprising• Tripled participation at the
regional meetings• Has improved communication
between sending and receiving facilities

• Provided great educational opportunities:— Annual Statewide Trauma Conference— Annual State Trauma Coordinators’ face to face
meetings— Improvement to individual hospital PI process
Overall PI Impact on Patient Care

Start With The BasicsStart Simple, Start Now!
Amy Eberle, RNTrauma CoordinatorSanford Health – Bismarck [email protected]
Ruth Hursman, RNState Trauma CoordinatorDivision of EMS & Trauma – Bismarck [email protected]
Great Resource People…..

Inclusive State Trauma System
An inclusive state trauma system should provide integrated, appropriate, and standardized medical care to trauma patients, wherever in the state the injury should happen.
Care
EducationPreventio
nBy Definition:

• All hospitals and providers expected to participate.• Trauma resources to be spread amongst all providers.• Hospitals to maintain a basic level of function.• Healthcare Providers need to maintain a standardized
level of trauma care.
What does Inclusive mean?
• All hospitals and providers expected to participate.— Legislature mandated participation in 2009
• Trauma resources to be spread amongst all providers.• Hospitals to maintain a basic level of function.
— State trauma committee site visits— Addition of State Trauma Medical Director 2012
• Healthcare Providers need to maintain a standardized level of trauma care.— All ED providers must pass Advanced Trauma Life Support©— Rural Trauma Team Development Course (made available)
Towards Inclusive….the ND Historical Journey……


North Dakota: An Inclusive State-Wide Trauma System
• All hospitals and providers expected to participate— 2011 - All hospitals designated!
Level I - 0Level II - 6Level III - 0Level IV - 9 Level V - 30

• Standardized Education Available — ATLS® mandatory for all practitioners (M.D., NP, PA who
cover the ED)— Rural Trauma Team Development Course®— Trauma Treatment Guidelines Manual
• Healthcare providers need to maintain a standardized level of trauma care.— PI process for Regional continues— State PI process was implemented!!— Evidence based care - State Trauma Treatment Guidelines
ND: An Inclusive State-Wide Trauma System
Important everyone plays fair in the sandbox!

• State Trauma Medical Director— 2011 Legislative session provided small appropriations for
a contracted position— Provides leadership/direction – keeps everyone on the
same page— “Rule Enforcer”— Provides Education/Outreach— Integrates with other services:
— Disaster, EMS, Injury Prevention, National Organizations
ND: An Inclusive State-Wide Trauma System

Moving Forward…..• Continue to maintain our State Trauma Registry• Continue to develop (revise) our PI process • Continue our Legislative Efforts
— Stabilize the State Trauma Medical Director position— Obtain adequate manpower at the Department of Health— Secure adequate funding for trauma system activities
Education/Outreach Trauma designation visits Trauma Registry support
• Continue to build leadership• Enhance Resources• Continue to educate the Public
ND: An Inclusive State-Wide Trauma System
What’s Next??

Performance Improvement: How Do We Improve?
• State & Regional PI• Inclusive State-Wide Trauma
System• Priorities for Optimal Trauma Care