perceived goal ownership, regulatory goal cognition…iacmao/goal ownership.pdf · perceived goal...
TRANSCRIPT
Perceived Goal Ownership, Regulatory GoalCognition, and Health Behavior Change
Morris A, Okun, PhD; Paul Karoly, PhD
Objective: To investigate thelinks among perceived goal own-ership, regulatory goal cognition,and health behavior change. Meth-ods: A sample of 390 college stu-dents completed measures of (a)perceived goal ownership for agoal related to a health behaviorthat they, their dating partner, orboth were seeking to change, (b) 9aspects of regulatory goal cogni-tion, and (c) health behaviorchange. Results: As compared to
participants with self-set andjoint-set goals, participants withpartner-set goals reported lessadaptive regulatory goal cogni-tion and were less likely to reportpositive changes in health behav-ior. Conclusion: Efforts to changedating partner's health behaviorsshould be framed as joint-setgoals.
Key words: goals, health be-haviors, self-regulation
Am J Health Behav. 2007;31(l):98-109
Physicians, social scientists, and pub-lic health professionals increasinglyhave recognized the role played by
personal decisions in the display of health-risk behaviors. They have placed greateremphasis on the impact of motivation,responsibility, and feelings of empower-ment on the health and well-being of bothindividuals and communities.'"^ A num-ber of conceptual models have emergedthat characterize human thought andaction as inherently purposeful. Thesemodels seek to delineate the connectionsbetween symptoms of illness or healththreats, on the one hand, and persistentself-protective actions, on the other.
Several purpose-centered models fea-ture goal processes (eg, goal selection,goal setting, goal cognition) and self-regu-latory capacities as central, generativeconstructs. For example, the common-sense model (CSM) of health self-regula-
Morris A. Okun, Professor; Paul Karoly, Pro-fessor, Department of Psychology, Arizona StateUniversity, Tempe, AZ.
Address correspondence to Dr Okun, Depart-ment of Psychology, Arizona State University,Tempe, AZ 85287-1104. [email protected]
tion^ assumes that when people confronthealth threats they seek to understand ormake sense of them along a small set ofrepresentational dimensions (includingperceptions of causes, consequences, andthe possibility of control). Goals are thenframed in a manner that is consistentwith their common-sense understand-ings. Similarly, the social cognitive model'emphasizes the importance of 3 genericself-regulatory subfunctions: paying at-tention to (self-monitoring) one's healthbehavior and its environmental triggers,enlisting self- and social support (incen-tives) for one's health promotion efforts,and, once again, adopting specific goals toguide one's efforts over time. Models for-mulated within a social cognitive frame-work share the assumption that the envi-ronment, the person, and the person'sinstrumental actions contribute jointlyor reciprocally to healtb outcomes.^ Con-sequently these models view causationas a systems construct, rather than onethat derives from any single source (orsubsystem) operating unilaterally.^
Ironically, until reeently, the prefix selfin tbe term self-regulation has obscuredthe social aspects of goal pursuit. Sys-tems perspectives on self-regulation have
98
Okun & Karoly
made salient that the process of achiev-ing important personal goals, whetherthe setting is the nuclear family, theclassroom, an intimate dyad, or a team ofcoworkers, is necessarily transactionalin nature.^•''^ That goals should not beexamined in isolation is justified, webelieve, by a number of psychological pre-cepts. Examples include the widely sharedassumption that the maintenance andgrowth of any social organization dependsupon the exchange of information (ie,communication) among its members,"the view that social relationships arefundamental to human cognition,'^ andthe idea that even covert self-regulatoryprocesses (eg, self-evaluation) occur inrelation to private evaluative audi-ences. ' • •' Moreover, empirical evidencehas accumulated that shows how manypersonal goals explicitly involve the par-ticipation of significant others.
If self-/social regulation exists in thecontext of communication and the recip-rocal exchange of resources and informa-tion, then researchers must investigatethe factors that both facilitate and hindercommunicative flow. Within the broadpurview of social cognitive theory, thesocial contextual model of everyday prob-lem solving (SCM)' '*' ' provides a usefulanalytic platform from which to considerthe motivational role of social relation-ships. The SCM proposes that there areindividual differences in relational ap-praisals. In other words, when individu-als select, think about, and pursue theirgoals (or life tasks), there are differencesin how they strategically appraise thelink between their goals and the largersocial unit. For example, individuals maysee themselves as the sole owner of agoal, perceive that a goal is primarily self-created but as impacting significant oth-ers, or view goals as originating from asocial unit (eg, a family goal). The differ-ent types of goal construal (the solitary, theindirectly shared, and the directly shared)are said to give rise to different goal pursuitand problem-solving strategies, namely,individualism, supportiveness, and collabo-ration. Meegan and Berg ' bave shown thatcollege students tend to construe many oftheir life tasks or goals as involving otherpeople and that directly shared appraisalstend to occur most often in the socialdomain.
Interestingly, the SCM does not con-sider the possibility tbat a person may be
pursuing a goal that is imposed by signifi-cant others, a goal that is neither one'sown nor shared. Framed in terms of theconcept of life tasks, the college studentsin Meegan and Berg's^^ study rarely nomi-nated health goals. Physical health goalsoften are perceived as both difficult andsocially prescribed (by parents, doctors,teachers, public health experts, the me-dia, and sometimes by peers). Therefore,we sought to evaluate the implications ofself-ascribed goal ownership, not only alongthe relational dimensions of individual-ism and mutuality, but also along thedimension of external imposition.
Research from diverse sources sug-gests that when individuals see them-selves as externally constrained (coerced,forced, cajoled, or othervnse manipulated),they often display psychological "reac-tance" or resistance to what they per-ceive as threats to their freedom ofchoice.^^^'' Even when adults recognizethat external pressure to behave in cer-tain ways is in their best interests, theytend to not only resist health-relatedmessages, but to act in ways that directlyoppose tbe influencer's intentions—the"boomerang effect" (see Ringold^^ for areview).
To be effective, goals must not only beclearly framed from a content perspectivebut also thought about in a manner thatarticulates with definable regulatoryskills. Ford" bas proposed a control sys-tems view of self-directedness that in-cludes several specific functional units.These units include a directive, or com-mand function that specifies and appraisesthe nature of the consequences (goals)toward which the system is aimed; anenergizing or arousal function that pro-vides the affective charge; and a set offunctions that belp modulate or controlthe actor's goal-directed movements un-der various environmental conditions (eg,low support). An expanding literature^'°attests to the predictive potency of regula-tory goal process cognition in accountingfor success in health goal attainment.We, therefore, anticipated that regula-tory cognition and goal ownership wouldboth be associated with health behaviorchange.
Summary of Hypotheses and ResearchQuestionsIn sum, the present study tested 4
hypotheses and explored 2 research ques-
Am J Health Behav.™ 2007;31(1):98-109 99
Goal Ownership
tions. First, we predicted that when regu-latory goal cognition was ignored, per-ceived goal ownership would be signifi-cantly related to self-report of health be-havior change. More specifically, we pre-dicted that the percentage of self-reportedhealth behavior change that was positivewould be higher for participants with self-ascribed as opposed to partner-ascribedgoals. Our first research question was"Do participants with joint-set goals differfrom participants who perceive their goalsto be self-set or partner set with respect toself-report of heedth behavior change?"
Our second prediction was that goalownership would exert significant effectson regulatory goal cognition processes.We expected that participants who per-ceive their goals as self-set would exhibitmore adaptive regulatory goal cognition,as indexed by scales that assess the di-rective, regulatory, control and arousalfunctions, than would participants whocharacterized their goals as partner set.Our second research question was "Doparticipants with joint-set goals differ fromparticipants who perceive tbeir goals tobe self-set or partner set v ath respect toregulatory goal cognition processes?"
Our third prediction was that the regu-latory goal cognition process variableswould account for a significant amount ofthe variation in self-report of health be-havior change. As compared to partici-pants who did not report positive healthbehavior change, participants who re-ported positive health behavior changewere expected to show a more adaptivepattern of regulatory goal cognition.
Our final prediction was that the regu-latory goal cognition process variableswould mediate the effect of goal owner-ship on self-reported health behaviorchange.
METHODSampleStarting with the fourth week of the
2004 spring and fall semesters, partici-pants recruited for our study were stu-dents enrolled in an introduction to psy-chology course offered at a large south-western state university. To fulfill acourse requirement, students visited awebsite to learn about the menu of stud-ies that were available. The presentstudy was described as examining howindividuals in heterosexual dating rela-tionships attempt to positively influence
their dating partner's health behavior.Students were informed that to be eligiblefor this study they had to be single, datinga person of the opposite sex, involved withtheir dating partner for at least 3 monthsor longer, and in contact with their datingpartner during the past 30 days.
ProcedureStudents who signed up to participate
in the study were administered a surveyanonymously in groups ranging from 2 to20 people. The questionnaire includedthe eligibility criteria, demographics,items that elicited a health behavior,beliefs regarding why their dating part-ner wanted them to cbange this healthbehavior, translation of this health be-havior into a goal, single-item measuresof perceived goal ownership and healthbehavior change, validity checks for thesesingle-item measures, and a goal cogni-tion battery. Two students were excludedfrom the study because they did not meetall of the eligibility criteria. Among the403 students included in the study, 73%were women. Fifty-five percent of theparticipants were white, non-Hispanic,9% were Hispanic, 7% were Asian, 4%were African American, 2% were Ameri-can Indians, and the remaining 23% oftbe participants were of other ethnicitiesor were of mixed heritage. Forty-six per-cent of the participants in our study wereyounger than 19 years old, 42% were 19-20 years old, and the remaining 12% werebetween the ages of 21 and 39 years old.The majority of the participants reportedthat they had been dating their partnerfor longer than 1 year (52%) and that theyhad daily contact with their partners(65%). Only 5% of tbe participants re-ported tbat they were currently datingsomeone else as well as their datingpartner.
MeasuresHealth behaviors. Following the elici-
tation procedure used by Lewis and Rook, ^participants were instructed to recall atime during the past 3 months when theirdating partner tried to influence them todo something for their health. They wereasked to list the health-related behaviortbat their dating partner wanted them tochange during the past 3 months. Par-ticipants were told to raise their hand iftbey could not think of a single health-related behavior that their dating partner
100
Okun 8& Karoly
had tried to get them to change during thepast 3 months. No students raised theirhand.
Placing the health behavior in ameaningful context. To provide a mean-ingful context for this health behavior,participants were asked 2 questions. Firstthey were asked, "Why do you helieve thatyour dating partner wants you to changethis health-related behavior?" Second,they were asked, "How can this health-related behavior be restated as a goal?"For the latter question, participants wereprovided with a brief definition of a goaland an example of a translation of a health-related behavior into a health goal. Thewritten goal statements were coded intoone of 13 categories, including an "other"category. When participants listed morethan one health goal, the top-listed goalwas coded. Based upon 40 protocols codedby 2 independent raters, the Kappa forcorrespondence of the classification ofthe target health behavior was .88, whichis considered to be excellent intercoderreliability.^'' To insure that participantskept the same health behavior in mind asthey completed the survey, the remain-ing questions that pertained to healthwere all framed using the phrase "thishealth behavior" or "this goal."
Perceived goal ownership. Perceivedgoal oviTiership was assessed with thefollowing question: "Which phrase bestdescribes how you feel about ownership ofthis goal?" The response options were "itis my goal" (called self-set goal), "it is mypartner's goal" (called partner-set goal),and "it is our goal" (called joint-set goal),
As a validity check on this measure,we examined the relation between re-sponses to this item and to another itemin which participants were asked, "Whichphrase best describes your partner's in-volvement with the goal?" The responseoptions were "apathetic (my partnerdoesn't get involved enough)," "support-ive (my partner provides support)," "col-laborative (my partner and I work to-gether as a team)," and "bossy (my partneracts as if he or she is in charge of me").We expected that the percentage of par-ticipants who indicated that their datingpartner was either supportive or collabo-rative would be higher in the joint-setgoal group than in the partner-set goalgroup. There was a significant (P<.001)association between perceived goal own-ership and perceived involvement of dat-
ing partner, x (6) = 67.77. Among partici-pants with partner-set goals, 52% per-ceived that their partner was supportiveor collaborative. In contrast, among par-ticipants with joint-set and self-set goals,88% perceived that their partner wassupportive or collaborative.
Regulatory goal cognition. Dimen-sions of regulatory goal cognition weremeasured using scales from the Goal andProcesses Inventory - Health (GP1-H) «Maes et aP^ carried out an exploratoryfactor analysis with principal componentsextraction and varimax rotation of 69items from the Goals and Processes In-ventory - Health. Forty-eight items loadedon the 9 factors that were extracted witheigenvalues greater than 1.00. Thesefactors were labeled as follows: goal effi-cacy (6 items), self-efficacy (6 items), con-flict (7 items), commitment (6 items),positive emotions (4 items), negativeemotions (4 items), communication (5items), support (4 items), and pressure (6items). Maes et al ^ reported coefficientalphas for the 9 scales ranging from .69(efficacy) to .84 (support).
In the present study, participants wereinstructed to keep their health goal inmind when responding to the items onthis questionnaire. Participants ratedeach item on a 5-point scale with anchorsof completely disagree (0) and completelyagree (4). Sample items include "It isclear to me how I can achieve thisgoal"(efficacy); "I feel totally confident thatI can achieve this goal" (self-efficacy);"This goal stands in the way of otherthings that are important to me" (con-flict); "Whatever happens, I will not giveup this goal" (commitment); "I feel happywhen pursuing this goal" (positive emo-tions); "It is stressful to pursue this goal"(negative emotions); "I talk to other peopleabout this goal" (communication); "Mypartner totally supports this goal" (sup-port); and "My partner forces me to workon this goal" (pressure). After performingitem analyses, we dropped one efficacyitem and one self-efficacy item. Scoreson the scales were computed by summingthe responses to the appropriate itemsand then dividing by the number of items.
Self-reported health behavior change.Participants were asked a question de-veloped by Lewis and Rook. ^ "What tjrpe ofimpact has your dating partner's attemptsto influence you had on this health be-havior?" The response options were (a)
Am J Health Behav.™ 2007;31(l):98-109 101
Goal Ownership
Table 1Frequency Distributions
Type of Health Behavior,for
GoalOwnerships and Self-Report of
Health Behavior Change(n=403)
Type of Health Behavior' PercentagesExercisingEating WellSmokingDrinking AlcoholRelaxingSleepingChanging WeightVisiting a PhysicianTaking DrugsDriving SafelyOtber
Goal OwnershipJoint setSelf-setPartner set
Self-report of Health Behavior ChangePositive changeNo changeNegative change
Note.a Health behaviors nominated by 6 or
1816141312964323
444214
7126
3
fewerrespondents were placed in the "other"category.
"my health behavior has changed towardwhat my dating partner wanted me to do,"(b) "my health behavior has not changedat all," or (c) "my health behavior haschanged toward the opposite of what mydating partner wanted me." As a validitycheck on this measure, we examined therelation between responses to this itemand to 2 items developed by Tucker.^^Participants were asked the extent towhich they (a) engaged in the healthbehavior and (b) ignored their dating part-ner or did nothing when their datingpartner attempted to get them to changethe health behavior they had nominated.The response options for both questionswere never (0), rarely (1), sometimes (2),and often (3). Relative to participants whoreported that they did not change theirhealth behavior, we expected that partici-pants who reported that they made apositive change in their health behavior
to have higher scores on the "engaging"item and to have lower scores on the"ignoring" item. As anticipated, self-re-port of health behavior change (0= nochange, 1 = positive change) was posi-tively correlated with scores on the "en-gaging" item, r , , (389) = .34, P<.001,O O .o ' point biscrmal ^ , ' . , ' '
and inversely correlated with scores onthe "ignoring" item, r ., , (387) = -.37,
o o I point bisermal * ' '
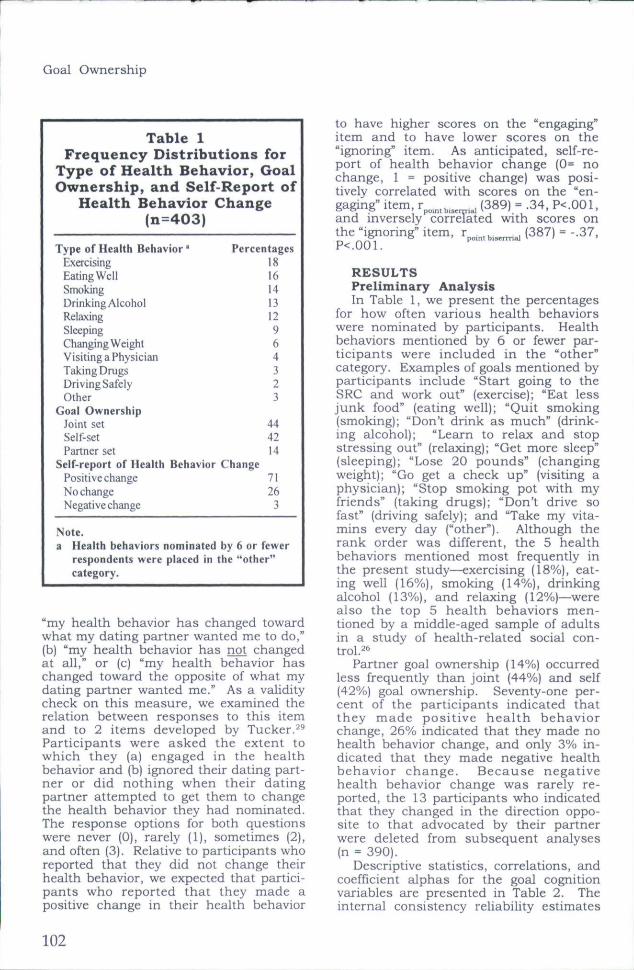
RESULTSPreliminary AnalysisIn Table 1, we present the percentages
for how often various health behaviorswere nominated by participants. Healthbehaviors mentioned by 6 or fewer par-ticipants were included in the "other"category. Examples of goals mentioned byparticipants include "Start going to theSRC and work out" (exercise); "Eat lessjunk food" (eating well); "Quit smoking(smoking); "Don't drink as much" (drink-ing alcohol); "Learn to relax and stopstressing out" (relaxing); "Get more sleep"(sleeping); "Lose 20 pounds" (changingweight); "Go get a check up" (visiting aphysician); "Stop smoking pot with myfriends" (taking drugs}; "Don't drive sofast" (driving safely); and "Take my vita-mins every day ("other"). Although therank order was different, the 5 healthbehaviors mentioned most frequently inthe present study—exercising (18%), eat-ing well (16%), smoking (14%), drinkingalcohol (13%), and relaxing (12%)—werealso the top 5 health behaviors men-tioned by a middle-aged sample of adultsin a study of health-related social con-
Partner goal ownership (14%) occurredless frequently than joint (44%) and self(42%) goal ownership. Seventy-one per-cent of the participants indicated thatthey made positive health behaviorchange, 26% indicated that they made nohealth behavior change, and only 3% in-dicated that they made negative healthbehavior change. Because negativehealth behavior change was rarely re-ported, the 13 participants who indicatedthat they changed in the direction oppo-site to that advocated by their partnerwere deleted from subsequent analyses(n = 390).
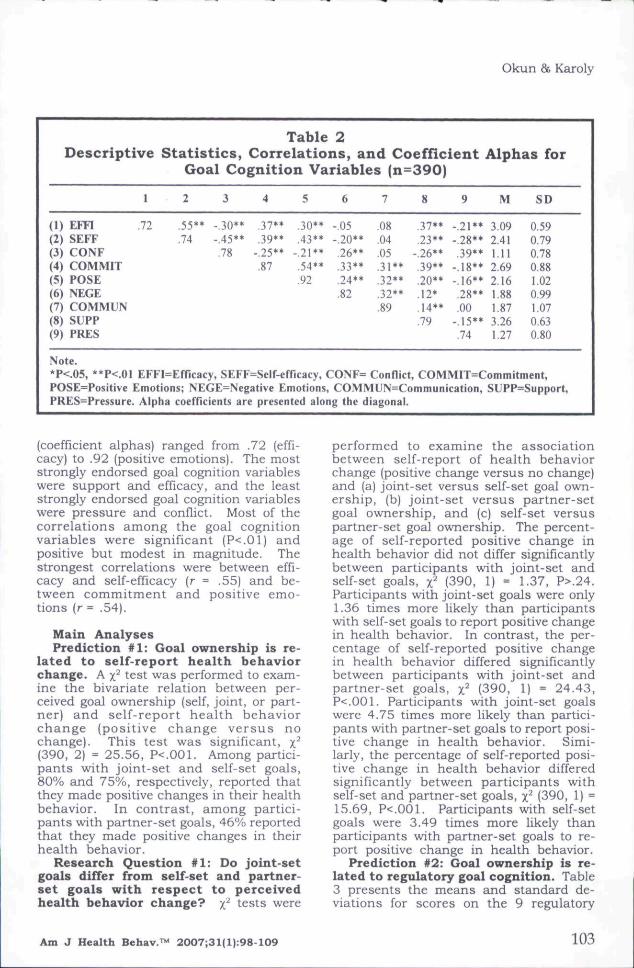
Descriptive statistics, correlations, andcoefficient alphas for the goal cognitionvariables are presented in Table 2. Theinternal consistency reliability estimates
102
Okun & Karoly
Table 2Descriptive Statistics, Correlations, and Coefficient Alphas for
Goal Cognition Variables {n=390)
(1)(2)(3)(4)(5)(6)(7)(8)(9)
1
Em .72SEFFCONFCOMMITPOSENEGECOMMUNSUPPPRES
2
.55**
.74
3
-.30**-.45**.78
4
.37**
.39**-.25**.87
5
.30**
.43**-.21**.54**.92
6
-.05-.20**,26**.33**,24**.82
7
.08
.04
.05
.31**
.32**
.32**
.89
8
.37**,23**
-.26**,39**.20**.12*.14**.79
9
-.21**-,28**.39**
-18**-.16**,28**.00
-,15**,74
M
3,092,411.112.692,161.881.873.261.27
SD
0.590,790,780,881,020.991.070.630.80
Note.*P<.05. **P<.01 EFFI=Efficacy. SEFF=Self-efricacy, CONF= Conflict, COMMIT=Commitment,POSE=Positive Emotions; NEGE=Negative Emotions, COMMUN=Communication, SUFP=Support,PRES=Pressure. Alpha coefficients are presented along the diagonal.
(coefficient alphas) ranged from .72 (effi-cacy) to .92 (positive emotions). The moststrongly endorsed goal cognition variableswere suppor t and efficacy, and the leaststrongly endorsed goal cognition variableswere p ressure and conflict. Most of thecorrelations among the goal cognitionvariables were significant (P<.01) andpositive but modest in magnitude. Thestrongest correlations were between effi-cacy and self-efficacy (r = .55) and be-tween commitment and positive emo-tions (r = .54).
Main AnalysesPrediction #1: Goal ownership is re-
lated to self-report health behaviorchange. A x test was performed to exam-ine the bivariate relation between per-ceived goal ownership (self, joint, or part-ner) and self-report health behaviorchange (positive change versus nochange). This test was significant, x(390, 2) = 25.56, P<.001. Among partici-pants with joint-set and self-set goals,80% and 75%, respectively, reported thatthey made positive changes in their healthbehavior. In contrast, among partici-pants with partner-set goals, 46% reportedthat they made positive changes in theirhealth behavior.
Research Question #1: Do joint-setgoals differ from self-set and partner-set goals with respect to perceivedhealth hehavior change? x tests were
performed to examine the associationbetween self-report of health behaviorchange (positive change versus no change)and (a) joint-set versus self-set goal own-ership, (b) joint-set versus partner-setgoal ownership, and (c) self-set versuspartner-set goal ovmership. The percent-age of self-reported positive change inhealth behavior did not differ significantlybetween participants with joint-set andself-set goals, x"* (390, 1) = 1.37, P>.24.Participants with joint-set goals were only1.36 times more likely than participantswith self-set goals to report positive changein health behavior. In contrast, the per-centage of self-reported positive changein health behavior differed significantlybetween participants with joint-set andpartner-set goals, x (390, 1) = 24.43,P<.001. Participants with joint-set goalswere 4.75 times more likely than partici-pants with partner-set goals to report posi-tive change in health behavior. Simi-larly, the percentage of self-reported posi-tive change in health behavior differedsignificantly between participants withself-set and partner-set goals, x^ (390, 1) =15.69, P<.001. Participants with self-setgoals were 3.49 times more likely thanparticipants with partner-set goals to re-port positive change in health behavior.
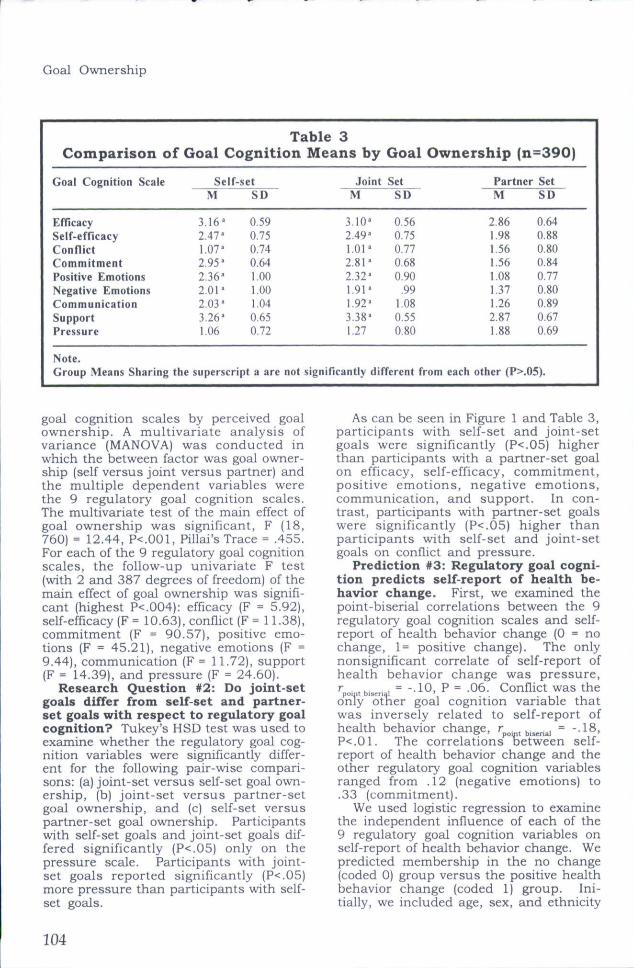
Prediction #2: Goal ownership is re-lated to regulatory goal cognition. Table3 presents the means and standard de-viations for scores on the 9 regulatory
Am J Health Behav.™ 2007;31(l):98-109 103
Goal Ownership
Comparison of
Goal Cognition Scale
EfficacySelf-efficacyConflictCommitmentPositive EmotionsNegative EmotionsCommunicationSupportPressure
Note.
Table 3Goal Cognition
Self-setM
3.16'2.47'1.07*2.95-2,36'2.01'2.03'3.26'1.06
SD
0,590.750.740.641,001,001.040,650,72
Group Means Sharing the superscript a are not
Means by
JointM
3.10'2,49'1.01'2.81'2.32'1.91'1,92'3.38'1,27
Goal Ownership (
SetSD
0.560,750.770.680.90
,991.080,550.80
significantly different from each
n=390)
Partner SetM
2.861.981.561.561.081.371.262.871.88
SD
0.640.880.800.840.770.800.890.670.69
other (P>.05).
goal cognition scales by perceived goalownership . A mult ivariate analysis ofvariance (MANOVA) was conducted inwhich the between factor was goal owner-ship (self versus joint versus partner) andthe multiple dependent variables werethe 9 regulatory goal cognition scales.The multivariate test of the main effect ofgoal ownership was significant, F (18,760) = 12.44, P<.001, Pillai's Trace = .455.For each of the 9 regulatory goal cognitionscales, the follow-up univariate F test(with 2 and 387 degrees of freedom) of themain effect of goal ownership was signifi-cant (highest P<.004): efficacy (F = 5.92),self-efficacy (F = 10.63), conflict (F = 11.38),commitment (F = 90.57), positive emo-tions (F = 45.21), negative emotions (F =9.44), communication (F = 11.72), support(F = 14.39), and pressure (F = 24.60).
Research Question #2: Do joint-setgoals differ from self-set and partner-set goals with respect to regulatory goalcognition? Tukey's HSD test was used toexamine whether the regulatory goal cog-nition variables were significantly differ-ent for the following pair-udse compari-sons: (a) joint-set versus self-set goal own-ership, (b) joint-set versus partner-setgoal ownership, and (c) self-set versuspartner-set goal ownership. Participantswith self-set goals and joint-set goals dif-fered significantly (P<.05) only on thepressure scale. Participants vidth joint-set goals reported significantly (P< .05)more pressure than participants with self-set goals.
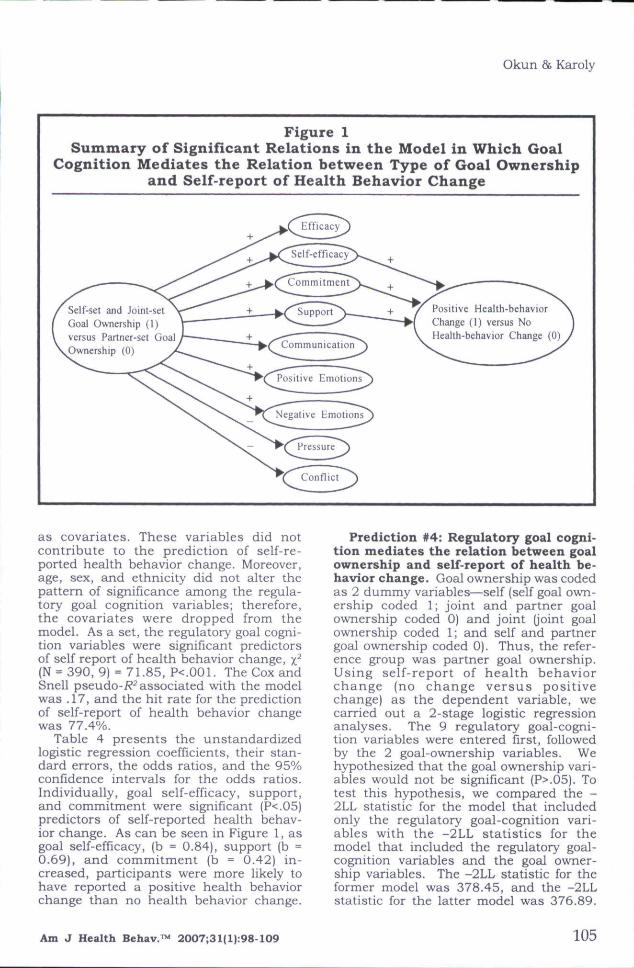
As can be seen in Figure 1 and Table 3,participants with self-set and joint-setgoals were significantly (P<.05) higherthan participants with a partner-set goalon efficacy, self-efficacy, commitment,positive emotions, negative emotions,communication, and support. In con-trast, participants with partner-set goalswere significantly (P<.05) higher thanparticipants with self-set and joint-setgoals on conflict and pressure.
Prediction #3: Regulatory goal cogni-tion predicts self-report of health he-havior change. First, we examined thepoint-biserial correlations between the 9regulatory goal cognition scales and self-report of health behavior change (0 = nochange, 1= positive change). The onlynonsignificant correlate of self-report ofhealth behavior change was pressure,po, tb.s n I = --10, P = .06. Conflict was the
only other goal cognition variable thatwas inversely related to self-report ofhealth behavior change, r^,^,^,,,,^^ = --18,P<.01. The correlations between self-report of health behavior change and theother regulatory goal cognition variablesranged from .12 (negative emotions) to.33 (commitment).
We used logistic regression to examinethe independent influence of each of the9 regulatory goal cognition variables onself-report of health behavior change. Wepredicted membership in the no change(coded 0) group versus the positive healthbehavior change (coded 1) group. Ini-tially, we included age, sex, and ethnicity
104
Okun & Karoly
Figure 1Summary of Significant Relations in the Model in Which Goal
Cognition Mediates the Relation between Type of Goal Ownershipand Self-report of Health Behavior Change
Efficacy— - —-
Self-efficacy. — •
• ,
Commitment
Support Positive Health-behaviorChange (1) versus NoHealth-behavior Change (0)
Self-set and Joint-setGoal Ownership (!)versus Partner-set GoalOwnership (0)
Positive Emotions
Neeaiive Emotions
as covariates. These variables did notcontribute to the prediction of self-re-ported health behavior change. Moreover,age, sex, and ethnicity did not alter thepattern of significance among the regula-tory goal cognition variables; therefore,the covariates were dropped from themodel. As a set, the regulatory goal cogni-tion variables were significant predictorsof self report of health behavior change, x(N = 390, 9) = 71.85, P<.001. The Cox andSnell pseudo-i?^ associated with the modelwas .17, and the hit rate for the predictionof self-report of health behavior changewas 77.4%.
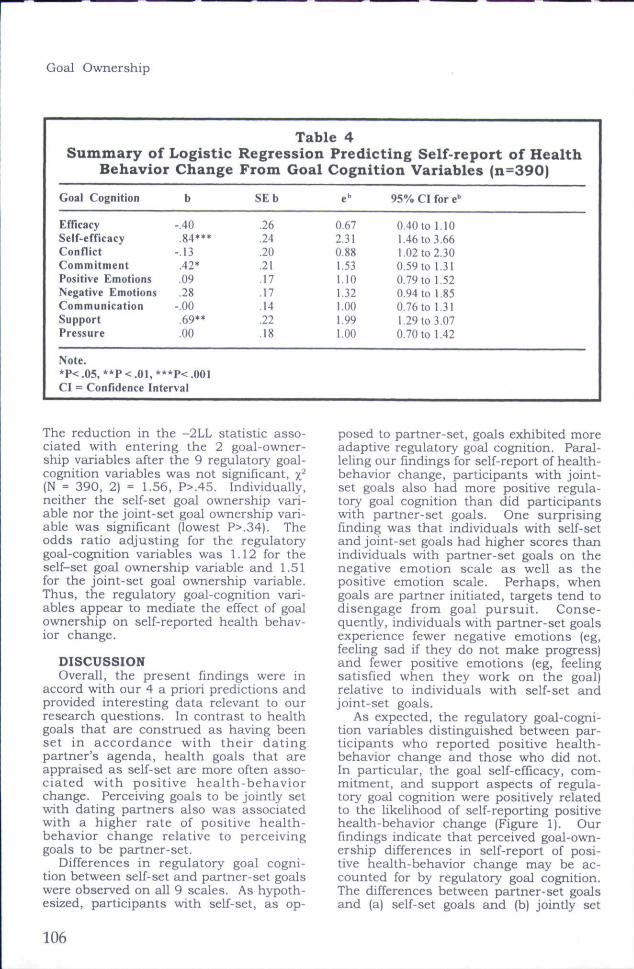
Table 4 presents the unstandardizedlogistic regression coefficients, their stan-dard errors, the odds ratios, and the 95%confidence intervals for the odds ratios.Individually, goal self-efficacy, support,and commitment were significant (P<.05)predictors of self-reported health behav-ior change. As can be seen in Figure 1, asgoal self-efficacy, (b = 0.84), support (b =0.69), and commitment {b = 0.42) in-creased, participants were more likely tohave reported a positive health behaviorchange than no health behavior change.
Prediction #4: Regulatory goal cogni-tion mediates the relation between goalownership and self-report of health be-havior change. Goal ownership was codedas 2 dummy variables—self (self goal own-ership coded 1; joint and partner goalownership coded 0) and joint (joint goalov^nership coded 1; and self and partnergoal ownership coded 0). Thus, the refer-ence group was partner goal ownership.Using self-report of health behaviorchange (no change versus positivechange) as the dependent variable, wecarried out a 2-stage logistic regressionanalyses. The 9 regulatory goal-cogni-tion variables were entered first, followedby the 2 goal-owner ship variables. Wehypothesized that the goal ownership vari-ables would not be significant (P>.05). Totest this hypothesis, we compared the -2LL statistic for the model that includedonly the regulatory goal-cognition vari-ables with the -2LL statistics for themodel that included the regulatory goal-cognition variables and the goal owner-ship variables. The -2LL statistic for theformer model was 378.45, and the -2LLstatistic for the latter model was 376.89.
Am J Health Behav.™ 2007;31(l|:98-109 105
Goal Ownership
Summary ofBehavior
Goal Cognition
EfficacySelf-efficacyConflictCommitmentPositive EmotionsNegative EmotionsCommunicationSupportPressure
Note.
LogisticChange
b
-.40.84***
-.13.42*,09,28
-.00.69**,00
*P< .05, **P < .01, ***p< .001CI = Confidence Interval
Table 4RegressionFrom Goal
SEb
,26.24,20,21,17.17,14,22,18
Predicting Self-report of HealthCognition Variables (n=390)
e"
0,672,310,881,531,101,321,001,991,00
95% CI for e
0.40 to 1.101.46 to 3,661.02 to 2,300.59 to 1,310,79 to 1,520.94 to 1,850,76 to 1,311,29 to 3.070,70 to 1.42
The reduction in the -2LL statistic asso-ciated with entering the 2 goal-owner-ship variables after the 9 regulatory goal-cognition variables was not significant, y^(N = 390, 2) = 1.56, P>.45. Individually,neither the self-set goal ownership vari-able nor the joint-set goal ownership vari-able was significant (lowest P>.34). Theodds ratio adjusting for the regulatorygoal-cognition variables was 1.12 for theself-set goal ownership variable and 1.51for the joint-set goal ownership variable.Thus, the regulatory goal-cognition vari-ables appear to mediate the effect of goalownership on self-reported health behav-ior change.
DISCUSSIONOverall, the present findings were in
accord with our 4 a priori predictions andprovided interesting data relevant to ourresearch questions. In contrast to healthgoals that are construed as having beenset in accordance with their datingpartner's agenda, health goals that areappraised as self-set are more often asso-ciated with positive health-behaviorchange. Perceiving goals to be jointly setwith dating partners also was associatedwith a higher rate of positive health-behavior ehange relative to perceivinggoals to be partner-set.
Differences in regulatory goal cogni-tion between self-set and partner-set goalswere observed on all 9 scales. As hypoth-esized, participants udth self-set, as op-
posed to partner-set, goals exhibited moreadaptive regulatory goal cognition. Paral-leling our findings for self-report of health-behavior change, participants with joint-set goals also had more positive regula-tory goal cognition than did participantswith partner-set goals. One surprisingfinding was that individuals vidth self-setand joint-set goals had higher scores thanindividuals with partner-set goals on thenegative emotion scale as well as thepositive emotion scale. Perhaps, whengoals are partner initiated, targets tend todisengage from goal pursuit. Conse-quently, individuals with partner-set goalsexperience fewer negative emotions (eg,feeling sad if they do not make progress)and fewer positive emotions (eg, feelingsatisfied when they work on the goal)relative to individuals with self-set andjoint-set goals.
As expected, the regulatory goal-cogni-tion variables distinguished between par-ticipants who reported positive health-behavior change and those who did not.In particular, the goal self-efficacy, com-mitment, and support aspects of regula-tory goal cognition were positively relatedto the likelihood of self-reporting positivehealth-behavior change (Figure 1). Ourfindings indicate that perceived goal-own-ership differences in self-report of posi-tive health-behavior change may be ac-counted for by regulatory goal cognition.The differences between partner-set goalsand (a) self-set goals and (b) jointly set
106
Okun 8s Karoly
goals in terms of the percentage of self-report of positive health-behavior changeappears to be due to the lower levels of goalself-efficacy, commitment, and supportthat are associated with perceiving goalounership to be partner set (Figure 1).One possibility is that attempts to imposehealth-related goals on dating partnersare associated with psychological reac-tance.-"' Psychological reactance, in turn,may be associated with less adaptive regu-latory goal cognition and the lack of posi-tive change in health behavior.
LimitationsWe view the present research as pre-
liminary for several reasons.First, the relations among goal owner-
ship, regulatory goal cognition, and healthbeliavior change may partially reflectmethod variance due to relying solely onself-report measures. Second, interpre-tive caution is always justified when dataare cross-sectional and retrospective. Howcautious readers need to be in interpret-ing the present findings also depends, inpart, upon their position with regard tothe currently active debate on the "illu-sory" nature of personal initiative.
Investigators such as Wegner '' ^ haveconducted many ingenious experimentssuggesting that people's subjective senseof having initiated an action on the basisof forethought, an intention, or a goal ispurely an illusion. He maintains that thebrain does this to help craft a coherent-appearing (but after-the-fact, "folk psy-chological") account of why we do what wedo.
What Wegner and his colleagues fail toacknowledge is the idea that self-regula-tion or volition is an unfolding, systems-centered process, rather than a tempo-rally isolated event. In other words, theprocess of self-regulation works in concertu/ith rather than in contrast to automatic-^ y 33-36 'pj.jg present authors have not at-tempted to localize volition in time, butrather have sought to show that subjec-tive beliefs (about the origin or ownershipof a goal) can have implications for healthbehavior change. Although ownershipattributions, like agency or causal sourceattributions, can be false, this is not al-ways the case. Whereas subjective be-liefs can prove to have no predictive valuefor health variables, they can, at times,equal or surpass objective indicators.^''
Third, our procedure for eliciting health
goals asked participants about a healthbehavior that their dating partner wantedthem to change. For our research pur-poses this procedure made sense becausewe wanted to ensure that there was ad-equate variability in goal ownership. Anelicitation procedure that simply askedparticipants for their health goals, how-ever, would undoubtedly have yielded moreself-set health goals and fewer goals thatwere joint set or partner set.
Fourth, we assessed goal ownershipwith one item, but we conceptualize thisvariable as encompassing a sense of re-sponsibility and long-term commitmentas well as a sense of authorship or per-sonal causation. Similarly, we assessedhealth behavior change with a singleitem, and some researchers have con-ceptualized this variable as multidimen-sional.^^ In future research, the mea-surement of these variables can be im-proved hy using multi-item scales.
Fifth, we chose to focus on one type ofpopulation (self-selected college students)and one type of relationship (dating). Thus,we do not know whether the relationsobserved in the present study among per-ceived goal ownership, goal cognition, andhealth behavior change generalize toother types of populations (middle-agedadults) or to other types of relationships(spousal). Although college students maynot construe health maintenance as oneof their most salient life tasks,^' in thepresent study, almost 80% of the collegestudents were above the midpoint on thescale that assessed commitment to thehealth goal that was nominated. Further-more, college students warrant study be-cause they are considered to be an at-riskpopulation with respect to many healthbehaviors including alcohol and substanceabuse, eating disorders, lack of exercise,poor nutrition, poor sleep habits, and un-safe sex practices.^^'^^ Although the psy-chological investment in dating relation-ships is lower than in spousal relation-ships, establishing an intimate relation-ship with a romantic partner is an impor-tant developmental task for individualsin emerging adulthood, a period of lifefrom the late teens through the twen-ties.""
CONCLUSIONSRecent self-regulation models have
incorporated the notion that social fac-tors play an important role in health be-
Am J Health Behav.™ 2007;31(I):98-X09 107
Goal Ownership
havior change.''' The present findings helpto clarify the transactional nature of self-regulatory processes by suggesting thatself-selected and mutually selected (joint)goals can have similar effects on impor-tant health outcomes. In contrast to par-ticipants with self-set and joint-set goals,participants with partner-set goals re-ported less positive regulatory goal cogni-tion and a lower percentage of positivehealth-behavior change. The present datasuggest that when family members,friends, and romantic partners seek tochange the health behaviors of peoplewho are important to them, they would bewise to foster self- and joint ownership ofhealth goals.
From a clinical (applied) perspective, itis often better to involve would-be goalchangers in a communal effort to bringabout change because, among the manyreasons that "2 heads are better thanone," the change process benefits from 2task monitors and from a mutual supportnetwork. Of course, potential costs ofmutual goal efforts include the possibilityof a motivational "crash" when one mem-ber of the dyad withdraws from the pursuitor when members of tbe would-be changeteam come into tactical conflict.
Future research should seek to un-pack the goal ownership construct anddevelop methods for its assessment invarious dyadic relationships and in largersocial units. Over the years, the notion ofgoal commitment has been the most widelyused concept to capture the idea of agenticstrength. Nevertheless, commitment orownership is clearly multidimensional,involving, at the very least, a sense ofpersonal responsibility, sacrifice (ie, whatone is willing to give up in order to achievea goal), and energy expenditure. Addi-tionally, the relations between the vari-ous dimensions of goal ownership andgoal cognition and health behavior changemay vary across relationship type. It wouldbe important, therefore, to study the rela-tions between the various components ofgoal ownership and goal cognition andhealth behavior change in the context ofmultiple dyadic relationships such asthose involving spouses, best friends, par-ent and child, physician and patient aswell as larger social units (eg, familiesand friends). •
REFERENCESl ,Bandura A. Self-Efficacy: The Exercise of
Control. New York: Freeman 1997,2,Gochman DS. (Ed). Handbook of Health Be-
havior Research. New York: Plenum 1997,3.Maes S, Karoly P. Self-regulation assessment
and intervention in physical health and ill-ness: A review. Applied Psychology: An Interna-tional Review. 2005;54:267-299.
4.Schwarzer R, Social-cognitive factors in chang-ing health-related behaviors. Current Direc-tions in Psychological Science. 200I;10:47-51.
5,Weinstein ND. Testing four competing theo-ries of health-protective behavior. HealthPsychoi. 1993:12:324-333.
6,Leventhal H, Brissette I, Leventhal E, Thecommon-sense model of self-regulation ofhealth and illness. In Cameron LD, LeventhalH, (Eds). The Self-Regulation of Health andIllness Behaviour, New York: Routledge2003:42-65.
7.Bandura A. The primacy of self-regulation inhealth promotion. Applied Psychology: AnInternational Review. 2005;54:245-254.
8.Vancouver JB, The depth of history and expla-nation as benefit and blame for psychologicalcontrol theories, J Appl Psychoi. 2005;90:38-52,
9.Karoly P. Mechanisms of self-regulation: asystems view, Annu Rev Psychoi. 1993;44:23-52.
10,Karoly P. A goal systems-self-regulatory per-spective on personality, psychopathology, andchange. Review of General Psychology.1999;3:264-291.
11,Ford DH. Humans as Self-Constructing Liv-ing Systems: A Developmental Perspective onBehavior and Personality, Hillsdale, N. J,:Erlbaum 1987.
12,Vygotsky L, Thought and Language, London:MIT 1986.
13,Hermans HJM, Voicing the self: from infor-mation process ing to dialogicalinterchange. Psychoi Bul. 1996;119:31-50.
14.Higgms ET. Self-discrepancy: A theory relat-mg self and affect. Psychoi Rev. 1987; 94:319-340,
15,Cantor N, Norem JK, Niedenthal PM, et al.Life tasks, self-concept ideals, and cognitivestrategies in a life transition. J Pers Soc Psychoi.1987:53:1178-1191.
16.Zirkel S, Cantor N. Personal construal of lifetasks : those who struggle withindependence. J Pers Soc Psychoi. 1990:58:172-185.
17,Leary MR. The sociometer, self-esteem, andthe regulation of interpersonal behavior. InBaumeister F, Vohs KD, (Eds). Handbook ofSelf-Regulation: Research, Theory, and Ap-plications, New York: Guilford 2004:373-391,
18,Vohs KD, Ciarocco NJ, Interpersonal func-tioning requires self-regulation. In BaumeisterF, Vohs KD, (Eds). Handbook of Self-Regula-tion: Research, Theory, and Applications,New York: Guilford 2004:392-407.
19,Wegner DM, Erber R. Social foundations ofmental control. In Wegner DM, Pennebaker
108
Okun & Karoly
JW, (Eds), Handbook of Mental Control.Englewood Cliffs, NJ,: Prentice-Hall 1993:36-56.
20.Berg CA, Meegan SP. Deviney FP. A social-contextual model of coping with everydayproblems across the lifespan. InternationalJournal of BehavioralDevelopment 1998;22:239-261,
21,Meegan SP, Berg CA, Whose Ufe task is itanyway? Social appraisal and life task pur-suit. J Pers. 2001:69:363-389,
22.Brehm JW. A Theory of Psychological Reac-tance. New York: Academic Press 1966.
23.Brehm JW. Responses to Loss of Freedom, ATheory of Psychological Reactance, Morristown,N,J,: General Learning Press 1972,
24.Wicklund RA. Freedom and Reactance,Potomac, Maryland: Erlbaum 1974,
25,Ringold DJ. Boomerang effects in response topublic heal th in tervent ions: someunintended consequences in the alcohol bev-erage market. Journal of Consumer Policy.2002:25:27-63.
26.Lewis MA, Rook KS. Social control in per-sonal relationships: Impact on health behav-iors and psychological distress. Health Psychoi.1999:18:63-71.
27,Orwin RG. Evaluating coding decisions. InCooper H, Hedges LV, (Eds). The Handbook ofResearch Synthesis, New York: Russell SageFoundation 1994:139-162.
28.Maes S, Pomaki G, Joekes K, et al. The Goalsand Processes Inventory (GAPI), Leiden: LeidenUniversity, Health Psychology Unit 2001.
29.Tucker JS. Health-related social control withinolder adults' relationships, J Geront B PsychoiSci Soc Sci. 2002:57B:387-395.
30.Lewis MA, Butterfield RM, Antecedents and
reactions to health related social control. PersSoc Psychoi Bull 2005:20:1-12,
31.Wegner DM, The Illusion of Conscious Will.Cambndge, MA,: MIT Press 2002,
32,Aarts H, Custers R, Wegner DM, On theinference of personal authorship: Enhancingexperienced agency by priming effect infor-mation. Conscious Cogn. 2005:14:439-458.
33.Dennett DC. Freedom Evolves. New York:Viking 2003,
34,Namias E, Agency, authorship, and illusion.Conscious Cogn. 2005:14:771-785.
35,van Duijn M, Bem S. On the alleged illusionof conscious will. Philosophical Psychology.2004:18:699-714.
36,Karoly P, Boekaerts M, Maes S, Toward con-sensus in the psychology of self-regulation:how far have we come? How far do we have yetto travel? Applied Psychology: An InternationalReview. 2005:54:300-311.
37,Singh-Manoux A, Marmot MG, Adler NE.Does subjective social status predict healthand change in health status better than objec-tive status? Psychosom Med. 2005:67:855-861.
38,Sands T, Archer J Jr,, Puleo S. Prevention ofhealth-risk behaviors in college students:Evaluating seven variables. Journal of CollegeStudent Development. 1998:39:331-342,
39,Leslie E, Own N, Salmon J, et al. Insuffi-ciently active Australian college students:Perceived personal, social, and environmen-tal influences, Prev Med. 1999:28:20-27.
40,Amett J J . Emerging adulthood: a theory ofdevelopment from the late teens through thetwenties. Am Psychoi 2000:55:469-480.
41,Gebhardt WA, Maes S. Integrating social-psy-chological frameworks for health behavior re-search. Am J Health Behau. 2001;25:528-536.
Am J Health Behav.™ 2007;31(lJ:98-109 109
