pep manual
TRANSCRIPT

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 1/48
Last Updated: June 30, 2009
Postexposure Prophylaxisfor
Occupational Bloodborne Exposures
A MANUAL FOR HEALTH CARE PROVIDERS
Kathy Hall, PA-C
Christopher Behrens, MD
David H. Spach, MD
and
The Northwest AIDS Education and Training Center

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 2/48
Dear Health Care Workers:
Any health care worker who experiences a bloodborne pathogen exposureshould receive a timely and accurate evaluation, as well as appropriatemanagement and follow-up. Although many institutions have a Postexposure
Prophylaxis (PEP) protocol, most lack a user-friendly, single-source documentthat addresses the multiple complex issues associated with an exposure.
The Northwest AIDS Education and Training Center (NW AETC) has developeda postexposure evaluation, treatment, and follow-up manual titled PostexposureProphylaxis for Occupational Bloodborne Exposures: A Manual for Health CareProviders. The recommendations in this manual are based on the 2005 U.S.Public Health Service Guidelines for the Management of Occupational Exposuresto HIV and Recommendations for Postexposure Prophylaxis.
We hope this manual will serve as a useful resource for you as you develop or
update your Postexposure Prophylaxis program.
Sincerely,
Kathy Hall, PA-CRiverStone Health and Northwest AIDS Education and Training CenterHIV Specialist, American Academy of HIV Medicine
Christopher Behrens, MDMedical Director, International Training and Education Center on HIV (I-TECH)Clinical Assistant Professor of Medicine, Division of Infectious DiseasesUniversity of Washington School of Medicine
David H. Spach, MDClinical Director, Northwest AIDS Education and Training CenterProfessor of Medicine, Division of Infectious DiseasesUniversity of Washington School of Medicine

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 3/48
TABLE OF CONTENTS
INTRODUCTION
INSTRUCTIONS FOR HEALTH CARE WORKERS …………………….….. 1
EVALUATION AND RECOMMENDATIONS BY EXPOSURE TEAM …….. 2
72 HOUR FOLLOW-UP VISIT ..………………………….…..…………..…… 7
TWO WEEK FOLLOW-UP VISIT ………………………………….….….…… 8
SIX WEEK FOLLOW-UP VISIT ……….……..………………………..…….… 9
12 WEEK FOLLOW-UP VISIT ………..………………………………..…..…. 10
24 WEEK FOLLOW-UP VISIT ………..………………………………………. 11
48 WEEK FOLLOW-UP VISIT (IF INDICATED) ….…….………………………. 11
REFERENCES ……..…………………………….…….….…………………… 12
TABLES
TABLE 1: CLASSIFICATION OF EXPOSURES VERSUS NON-EXPOSURES TO HIV ………………………………….……………………..….. 13
TABLE 2: CLASSIFICATION OF EXPOSURES VERSUS NON-EXPOSURES TO HBV AND HCV .….……...………………………..…..….…….. 14
TABLE 3: HIV PEP FOR PERCUTANEOUS INJURIES: SOURCE WITH
KNOWN HIV INFECTION …………………….…….....……..……... 15
TABLE 4: HIV PEP FOR PERCUTANEOUS INJURIES: SOURCE WITH UNKNOWN HIV STATUS, UNKNOWN SOURCE, OR HIV-NEGATIVE … 16
TABLE 5: HIV PEP FOR MUCOUS MEMBRANE AND NON-INTACT SKIN EXPOSURES ……………………………………..…..……….….. 17
TABLE 6: PREFERRED BASIC REGIMENS ….…………………………….…. 18
TABLE 7: ALTERNATIVE BASIC REGIMENS ...……………………………….. 19
TABLE 8: PREFERRED AND ALTERNATIVE EXPANDED REGIMENS ..…….….. 20
TABLE 9: AUTHORS’ RECOMMENDED BASIC AND EXPANDED REGIMENS ..... 21
TABLE 10: PRIMARY SIDE EFFECTS AND TOXICITIES ASSOCIATED WITH ANTIRETROVIRAL AGENTS ………………………………..….…. 22
TABLE 11: RECOMMENDED PEP FOR EXPOSURE TO HBV .…………....….… 26

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 4/48
FORMS
FORM 1: SUPERVISOR’S FOLLOW-UP REPORT OF INCIDENT …...………… 27
FORM 2: EXPOSURE CONTROL TEAM ASSESSMENT AND REPORT OF POSSIBLE BLOODBORNE PATHOGEN EXPOSURE .……..…..……. 29
FORM 3: INFORMED REFUSAL OF MEDICAL EVALUATION FOLLOWING EXPOSURE TO BLOODBORNE PATHOGEN(S) ....……….…..…….. 32
FORM 4: EMPLOYEE REFUSAL TO RECEIVE HEPATITIS B VACCINATION ....... 33
FORM 5: LACK OF DOCUMENTATION OF HEPATITIS B VACCINATION AND REFUSAL OF EVALUATION FOR IMMUNITY ..…….…..…….... 34
FORM 6: CONSENT FOR HIV TEST ….……….……….…………………….. 35
FORM 7: INCIDENT REPORT ...……….……….…………….……….…….. 36
FORM 8: SHARPS INJURY LOG ………….…………….……………….….. 37
FORM 9: SEVENTY-TWO HOUR FOLLOW-UP VISIT ..………….…...………. 38
FORM 10: HEALTH CARE WORKER WRITTEN OPINION …….…..…....…….... 39
FORM 11: TWO WEEK FOLLOW-UP VISIT: RECOMMENDATIONS FOR HCW …. 41
FORM 12: SIX WEEK FOLLOW-UP VISIT: RECOMMENDATIONS FOR HCW …… 42
FORM 13: TWELVE WEEK FOLLOW-UP VISIT: RECOMMENDATIONS FOR HCW 43
FORM 14: TWENTY-FOUR WEEK FOLLOW-UP VISIT: RECOMMENDATIONS
FOR HCW ………………………………………………………... 44
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 5/48
1
INSTRUCTIONS FOR HEALTH CARE WORKERS
1. In the Event of An ExposureIn the event of a possible exposure to a bloodborne pathogen, the health care
worker (HCW) should act promptly to carry out the steps listed below.
2. Decontaminate the Area of the Exposure • Needle stick
o Remove gloves immediately, if presento Wash area with soap and water
o Avoid squeezing or milking the woundo Do not use caustic agents, such as bleach
• Blood splash on skino Wash area with soap and water
• Blood/body fluid splash to mucous membranes
o Wash/irrigate area copiously with water or sterile saline
3. Contact Designated Person or Exposure Control Team All health care facilities should have an established system that assigns adesignated person or team to respond to a HCW who experiences anoccupational exposure to a bloodborne pathogen. The HCW should contactthis designated person (or exposure team) immediately after decontaminatingthe area of exposure. Henceforth in this document, we will refer to the personor team that responds to the exposure as the “Exposure Control Team”.
4. Source Patient
If possible, the HCW should attempt to keep the source patient in the clinicuntil the Exposure Control Team can evaluate the situation.
5. Contact your Supervisor The HCW should contact his or her supervisor. The supervisor shouldcomplete Form 1: Supervisor’s Follow-up Report of Incident (or a formsimilar to this).
6. Evaluation of Exposure and Follow-upThe evaluation of the exposure and the follow-up for the HCW will beperformed and arranged for by the Exposure Control Team.
The National Clinicians’ Post Exposure Prophylaxis Hotl ine (PEPline) at
1-888-448-4911 offers free advice on the management of occupationalexposures to HIV, hepatitis B and hepatitis C. Clinical consultation is available24 hours/day, 7 days/week.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 6/48
2
EVALUATION AND RECOMMENDATIONS BY EXPOSURECONTROL TEAM
1. Decontaminate• Check to make sure the HCW has decontaminated the area where the
exposure occurred. If the HCW has not already done this, decontaminateas instructed below:
o Decontamination of needlestick injuryRemove gloves immediately, if presentWash area with soap and water
Avoid squeezing or milking the woundDo not use caustic agents, such as bleach
o Decontamination of blood splash to skinWash area with soap and water
o Decontamination of blood/body fluid splash to mucous membranes
Wash/irrigate area copiously with water or sterile saline.
2. Determine the Risk of the Exposure • To determine whether or not the incident represents an actual exposure
for HIV use Table 1: Classification of Exposures Versus Non-Exposures to HIV. For hepatitis B virus (HBV) and hepatitis C virus(HCV) use Table 2: Classification of Exposures Versus Non-Exposures to HBV and HCV. You may find it helpful to begin tocomplete Form 2: Exposure Control Team Assessment of Possib leBloodborne Pathogen Exposure, as this form will help you obtain theinformation necessary for the exposure evaluation and subsequent steps.
• If the source for the exposure is unknown, such as a needlestick injury
involving a needle in a sharps container, expert consultation isrecommended.
• If the incident does not represent an exposure, skip to step 11, as nofurther action is required apart from completion of certain forms.
• If the incident does represent an exposure, proceed with medicalevaluation as outlined in the following steps. If the HCW refuses medicalevaluation they should complete and sign Form 3: Informed Refusal ofMedical Evaluation Following Exposure to Bloodborne Pathogen(s).
3. Counsel for HIV Exposure Risk and Postexposure Prophylaxis
• If the HCW may have been exposed to HIV, counsel the HCW about therisk of acquiring HIV from the exposure and the pros and cons of takingHIV Postexposure Prophylaxis (PEP) antiretroviral medications. UseTable 3: HIV PEP for Percutaneous Injuries: Source with Known HIVInfection to assist in exposure risk stratification for a Percutaneous InjuryInvolving Source with Known HIV Infection, and use Table 4: HIV PEP forPercutaneous Injuries: Source with Unknown HIV Status, UnknownSource, or HIV-Negative for Percutaneous Injury Involving Source with

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 7/48
3
Unknown HIV Status, Unknown Source, or HIV-Negative Source. UseTable 5: HIV PEP for Mucous Membrane and Non-Intact SkinExposures for Mucous Membrane and Non-Intact Skin Exposures.
• Consider contacting a local/regional PEP expert or the PEPline forassistance with counseling and risk stratification. The National Clinicians’
Post-Exposure Prophylaxis Hotline (PEPline) offers free advice to HealthCare Workers on the management of exposures to HIV, HBV, and HCV,24 hours/day, 7 days/week. The PEPline phone number is 888-448-4911.
4. Start HIV Ant iretroviral PEP
• If indicated and the HCW consents, start HIV PEP as soon as possible(ideally within 1-2 hours). The sooner PEP is started, the more effective itis thought to be. The time interval beyond which there is no benefitremains unknown. Antiretroviral PEP can be considered after 24-36 hoursafter the exposure, but expert consultation is recommended in thissituation.
•
If the source patient has known HIV infection, try to obtain pertinentinformation about their stage of HIV disease: most recent viral load,antiretroviral therapy history, and results from resistance testing (ifpreviously performed). Obtaining source patient information may help inestimating the exposure risk and in designing an HIV PEP regimen, butgathering this information should not delay timely administration of PEP.
• Based on the information you have obtained and the risk stratification,prescribe either a Basic (2-drug) or Expanded (3-drug) regimen. The2005 U.S. Public Health Service Guidelines for the Management ofOccupational Exposures to HIV and Recommendations for PostexposureProphylaxis provides recommendations for Preferred Basic Regimens
(Table 6: Preferred Basic Regimens), Alternative Basic Regimens(Table 7: Alternative Basic Regimens ), and Preferred and AlternativeExpanded Regimens (Table 8: Preferred and Alternative ExpandedRegimens). Nevirapine is contraindicated for use in PEP due to itspotential life-threatening toxicity in this setting.
• Given that new advances and data regarding antiretroviral therapy haveoccurred since the release of the 2005 U.S. Public Health ServiceGuidelines, we have included our 2009 authors’ recommendations forPreferred Basic Regimen and Preferred Expanded Regimens (Table 9:
Au thors ’ Recommended Basic and Expanded Regimens).
• We do not recommend using efavirenz as a preferred postexposure agent
for two reasons: (1) central nervous system adverse effects frequentlyoccur during the initial weeks after starting this medication, a problem thatcould be particularly problematic HCWs, and (2) efavirenz may beineffective if the source patient’s strain of HIV is resistant to non-nucleoside reverse transcriptase inhibitors (NNRTIs).
• We do not recommend initial use of abacavir because of the risk ofhypersensitivity reaction in the HCW (obtaining HLA-B5701 testing for theHCW would delay use of abacavir).
• We do not recommend the use of maraviroc since the source patient may

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 8/48
4
have X4-tropic HIV, or a mixture of HIV strains that include X4 HIV; a rapid HIV tropism assay is not commercially available. In the rare circumstancewhen the source patient very recently had an HIV tropism assayperformed, use of maraviroc could be considered if the source patient hadpure R5 HIV; expert consultation is advised in this circumstance.
•
When a source patient has known antiretroviral-resistant HIV, expertconsultation should be obtained to review any known resistanceinformation on the source patient and to determine the optimal PEPregimen.
• If the HCW is breastfeeding or pregnant, expert consultation isrecommended. In addition, review any medications or supplements theHCW may be taking, and investigate potential drug-drug interactions.
• Provide a minimum of 3-day supply of PEP medications. The totalduration of antiretroviral PEP is 28 days.
• Discuss the dosing and common side effects of the medicationsprescribed (Table 10: Primary Side Effects and Toxic ities) and provide
the HCW with contact numbers in the event they have significant sideeffects. If side effects develop, provide appropriate prescription(s), suchas anti-emetics and/or anti-diarrheals. If the side effects are severe,assess whether the medications need to be changed.
5. Determine HBV Immune Status and Administer HBV PEP if Needed • If the HCW may have been exposed to hepatitis B, determine whether the
HCW has been immunized against HBV, and if so, whether the HCW isknown to have responded to this vaccination (e.g. has documentedprotective hepatitis antibody titer). Details for HBV PEP are provided inTable 11: Recommended PEP for Exposure to HBV.
•
If hepatitis B vaccination is indicated but the HCW declines immunization,they should complete and sign Form 4: Employee Refusal to AcceptHepatitis B Vaccination.
• If the HCW claims to have had hepatitis B vaccination series and does notwish to accept HBV antibody testing or hepatitis B vaccine at the time ofexposure, they should complete and sign Form 5: Lack ofDocumentation of Hepatitis B Vaccine. The HCW may request thisvaccine at any time in the future.
6. Counsel after Exposure to Hepatitis C Virus• In the event the HCW was exposed to hepatitis C, there is no proven
effective PEP for HCV and thus PEP for hepatitis C is not recommended.Perform baseline testing for anti-HCV and ALT activity.
• The recommended baseline and follow-up testing consists of:o Testing for anti-HCV and ALT activityo Testing (at 4-6 months) for anti-HCV and ALT activity
o Some experts recommend HCV RNA testing at 4-6 weeks to makean earlier diagnosis of HCV infection, mainly because treatment ofpersons with very recently acquired HCV has been shown to havevery high cure rates

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 9/48
5
o Confirm all anti-HCV results reported positive by enzymeimmunoassay with supplemental anti-HCV testing (recombinantimmunoblot and/or HCV viral load)
7. Obtain Baseline Laboratory Studies for the HCW • Draw relevant baseline labs on the HCW. These generally include
baseline serologic testing for HIV, HCV, and hepatitis B (HIV Ab, HCV Ab,HBsAb), plus a baseline ALT level. In addition, if PEP is being consideredand the HCW is a female of child-bearing age, a stat pregnancy testshould be performed.
• If HIV PEP is initiated, a baseline complete blood count (CBC), BUN,Creatinine, and ALT should also be drawn.
• If written consent for HIV testing is required in the state where theexposure occurred, complete Form 6: Consent for HIV Test prior todrawing blood for the HIV antibody test on the HCW.
•
Drawing blood for laboratory studies on the HCW should not delay timelyadministration of PEP. If PEP is indicated, administer the first dose ofPEP and then obtain blood for laboratory studies.
8. Test Source Patient • Attempt to obtain permission to perform testing on the source patient for
HIV Ab, HCV Ab, and HBsAg. If these tests have previously beenperformed on the source patient, clinical judgment should be used todetermine whether the studies need repeating. The source patient shouldnot be charged for these tests.
• In certain circumstances where immediate information is needed on the
source patient, such as the situation where the exposed HCW is pregnant,use of the rapid HIV test (if available) may be appropriate for testing asource patient with unknown HIV status. Expert consultation is advised inthis situation.
• If the source patient refuses to give permission to have blood drawn, youshould contact your local health department for assistance in the matter.Laws and regulations regarding this scenario vary from state to state.
9. Counseling HCW About Preventing HIV Transmission • During the follow-up period, especially the first 6-12 weeks, the following
precautions are recommended for the HCW to prevent transmission of
HIV:o Do not donate blood, tissue, semen, or organs.o Do not become pregnant.o Do not engage in sexual intercourse during this time period. If the
HCW chooses to have sexual intercourse, they should use acondom consistently and correctly to reduce the risk of HIVtransmission.
o Women should not breast-feed infants during the follow-up period.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 10/48
6
10. Arrang ing Follow-up for the HCW
• Schedule a follow-up appointment that takes place within 72 hours.
• Provide the HCW with a copy of “ Exposure to B lood—What HealthcareWorkers Need to Know” .
•
Provide a contact number for the HCW in the event he or she has furtherquestions, or if problems develop with the PEP regimen.
• Offer psychological counseling referral for the HCW if indicated.
• Provide return precautions: instruct the HCW to return immediately forevaluation (e.g., Emergency Department or Urgent Care) if he or shedevelops significant adverse effects from the PEP regimen.
11. Complete Remaining Paperwork (forms not already completed)• Form 1: Supervisor’s Follow-Up Report of Incident (the HCW’s
supervisor should have completed)• Form 2: Exposure Contro l Team Assessment & Report of Possible
Bloodborne Pathogen Exposure (jointly completed by HCW andExposure Control Team)• Form 7: Incident Report Form 8: Sharps Injury Log

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 11/48
7
72 HOUR FOLLOW-UP VISIT
Instructions for the Managing Clinician
1. Address HCW Questions or Concerns At this visit address any questions or concerns the exposed HCW may haveabout the exposure or PEP recommendations to date. Form 9: 72 HourFollow-up Visit provides a template that can be used to record details of thisand subsequent follow-up visits. Offer psychological counseling referral ifindicated.
2. Incorporate New InformationEvaluate and incorporate any new information that may have becomeavailable about the source patient since the initial evaluation. Decide whetheror not any of the PEP recommendations made at the initial evaluation should
be changed in light of this new information. Consider consulting the PEPlinefor advice (888-448-4911).
3. Review Baseline LabsReview the labs drawn on the HCW at the Initial Visit. Investigate anyabnormalities with further studies as indicated. If any baseline laboratorystudies are abnormal and PEP was prescribed, re-evaluate theappropriateness of the HCW’s specific PEP regimen. If baseline labs were notdrawn at the initial evaluation, draw them at this 72 hour visit.
4. Complete Form 10: Health Care Worker Written OpinionComplete this form at this visit if follow-up not planned. Otherwise have theform completed at the two week follow-up visit. Provide a copy to the HCW.
5. Educate the HCW about Primary (Acute) HIV Manifestations Advise the HCW regarding signs and symptoms of primary (acute) HIVinfection, which typically develop within 1 to 6 weeks of exposure and mayinclude fever, rash, sore throat, lymphadenopathy, headache, or flu-likesymptoms. If these symptoms should occur, advise HCW to seek promptevaluation for possible primary HIV infection.
6. Complete Outstanding FormsComplete any forms that were not completed at the Initial Evaluation.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 12/48
8
TWO WEEK FOLLOW-UP VISIT(FOR HCWS WHO INITIATED ANTIRETROVIRAL PEP)
1. Address HCW Questions or Concerns
Address any questions or concerns the exposed HCW may have about theexposure or PEP recommendations to date. Use Form 11: Two WeekFollow-up Visit : Recommendations for HCW to record details of this andsubsequent steps. Offer psychological counseling referral if indicated.
2. Incorporate New InformationEvaluate any new information that may have become available about thesource patient since the initial evaluation. Decide whether or not any of thePEP recommendations made at the initial evaluation should be changed inlight of this new information. Consider consulting the PEPline for advice(888-448-4911).
3. Review Al l HCW Lab StudiesReview all of the lab studies drawn on the HCW to date. Investigate anyabnormalities with further studies as indicated. If any laboratory studies areabnormal, re-evaluate the appropriateness of the specific PEP regimen.
4. Draw Chemistry Panel and CBCDraw chemistry panel and CBC to screen for toxicities from the antiretroviralmedications.
5. Complete Form 11: Two Week Follow-up Visit: Recommendations for HCW Complete this form and provide a copy to the HCW.
6. Complete Form 10: Health Care Worker Writ ten Opinion If not already done, complete this form and provide a copy to the HCW.
7. Discuss Primary (Acute) HIV ManifestationsRemind the HCW about signs and symptoms of primary HIV infection, whichtypically develop within 1 to 6 weeks of exposure: fever, rash, sore throat,lymphadenopathy, headache, or flu-like symptoms. If these symptoms shouldoccur advise HCW to seek evaluation immediately for possible primary HIVinfection.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 13/48
9
SIX WEEK FOLLOW-UP VISIT
1. Address HCW Questions or Concerns Address any questions or concerns the exposed HCW may have about the
exposure. Offer psychological counseling referral if indicated.
2. Review All HCW Lab StudiesReview any of the lab studies that have not already been reviewed with theHCW and inform the HCW about subsequent lab draws.
3. Evaluate for Acute (Primary) HIVIf the exposure involved HIV, review whether the HCW has experienced (or iscurrently experiencing) any symptoms that would suggest acute (primary) HIVinfection. The constellation of symptoms that would suggest acute HIVinfection includes fever, rash, sore throat, lymphadenopathy, headache, or flu-
like symptoms. Patients who have symptomatic acute HIV typically presentwithin 28 days of the initial infection. If you suspect acute HIV infection, thenorder an HIV RNA test along with HIV antibody testing.
4. Evaluate for Acute Viral Hepatit is If the exposure involved HCV (or HBV in a HCW not immune to HBV), reviewwhether the HCW has experienced (or is currently experiencing) anysymptoms that would suggest acute hepatitis (nausea, abdominal pain,fatigue, flu-like symptoms, jaundice, or dark urine). Patients with acute HCVinfection are usually asymptomatic, but those with symptomatic acute diseasetypically present 6-8 weeks after infection (range 5-12 weeks). If you suspect
acute HCV infection, order an HCV RNA test along with HCV antibody testing.
5. Complete Form 12: Six Week Follow-up Visit: Recommendations for HCW Complete this form and provide a copy to the HCW.
6. Draw Laboratory Studies for HIV and HCV as IndicatedOrder an HIV test if the HCW exposure involved HIV. Similarly, if theexposure involved HCV, then HCV antibody testing should be performed.Routine use of HIV RNA testing, without suspected acute HIV, is NOTrecommended. Considering most adults with acute HCV do not have obviousclinical symptoms (and treatment of adults with acute HCV results in very highcure rates), some experts recommend obtaining an HCV RNA test at this visit.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 14/48
10
12 WEEK FOLLOW-UP VISIT
1. Address HCW Questions or Concerns Address any questions or concerns the exposed HCW may have about the
exposure. Offer psychological counseling referral if indicated.
2. Review All HCW Lab StudiesReview any of the lab studies that have not already been reviewed with theHCW and inform the HCW about subsequent lab draws.
3. Evaluate for Acute (Primary) HIV If the exposure involved HIV, review whether the HCW has experienced (or iscurrently experiencing) any symptoms that would suggest acute (primary) HIVinfection. The constellation of symptoms that would suggest acute HIVinfection includes fever, rash, sore throat, lymphadenopathy, headache, or flu-
like symptoms. Patients who have symptomatic acute HIV typically presentwithin 28 days of the initial infection. If you suspect acute HIV infection, thenorder an HIV RNA test along with HIV antibody testing.
4. Evaluate for Acute Viral Hepatit is If the exposure involved HCV (or HBV in a HCW not immune to HBV), reviewwhether the HCW has experienced (or is currently experiencing) anysymptoms that would suggest acute hepatitis (nausea, abdominal pain,fatigue, flu-like symptoms, jaundice, or dark urine). Patients with acute HCVinfection are usually asymptomatic, but those with symptomatic acute diseasetypically present 6-8 weeks after infection (range 5-12 weeks). If you suspect
acute HCV infection, then order an HCV RNA assay along with HCV antibodytesting.
5. Complete Form 13: Twelve Week Follow-up Visit : Recommendations forHCW Complete this form and provide a copy to the HCW.
6. Draw Laboratory Studies for HIV and HCV as IndicatedIf the HCW exposure involved HIV, then order an HIV antibody test. Similarly,if the exposure involved HCV, then order an HCV antibody test. Any HCWwho has a positive HCV antibody test should undergo supplemental testingwith an HCV RNA test. Routine use of HIV RNA testing, without suspectedacute HIV, is NOT recommended. Considering most adults with acute HCV
do not have obvious clinical symptoms (and treatment of adults with acuteHCV results in very high cure rates), some experts recommend obtaining anHCV RNA test at this visit.
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 15/48
11
24 WEEK FOLLOW-UP VISIT
1. Address HCW Questions or Concerns Address any questions or concerns the exposed HCW may have about the
exposure. Offer psychological counseling referral if indicated.
2. Review All HCW Lab StudiesReview any of the lab studies that have not already been reviewed with theHCW and inform the HCW about subsequent lab draws.
3. Complete Form 14: Twenty-four Week Follow-up Visit : Recommendationsfor HCW Complete this form and provide a copy to the HCW.
4. Draw Laboratory Studies for HIV and HCV as IndicatedIf the HCW exposure involved HIV, then order an HIV antibody test. Similarly,if the exposure involved HCV, then HCV antibody testing should be
performed. Any HCW who has a positive HCV antibody test should undergosupplemental testing with an HCV RNA test.
48 WEEK FOLLOW-UP (IF INDICATED)
1. Address HCW Questions or Concerns Address any questions or concerns the exposed HCW may have about theexposure. Offer psychological counseling referral if indicated.
2. Review All HCW Lab StudiesReview any of the lab studies that have not already been reviewed with theHCW and inform the HCW about subsequent lab draws.
3. Draw Laboratory Studies for HIV and HCV Ant ibody Tests as IndicatedIf the original exposure involved both HIV and HCV (or the HCW has amedical condition that would impair their ability to mount an antibodyresponse to viral pathogens), then order antibody testing for HIV and HCV. Ifthe exposure involved only HIV, then antibody testing after 24 weeks is notrequired. Similarly, if the exposure involved HCV only, then HCV antibodytesting is not required after 24 weeks.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 16/48
12
SELECTED REFERENCES
Cardo DM, Culver DH, Ciesielski CA, et al. A case-control study of HIV seroconversion
in health care workers after percutaneous exposure. Centers for Disease Control andPrevention Needlestick Surveillance Group. N Engl J Med. 1997;337:1485-90.http://content.nejm.org/cgi/content/abstract/337/21/1485
Henderson DK. Managing occupational risks for hepatitis C transmission in the healthcare setting. Clin Microbiol Rev. 2003;16:546-68.http://cmr.asm.org/cgi/content/full/16/3/546?view=long&pmid=12857782
Henderson DK, Fahey BJ, Willy M, et al. Risk for occupational transmission of humanimmunodeficiency virus type 1 (HIV-1) associated with clinical exposures. Aprospective evaluation. Ann Intern Med. 1990;113:740-6.
http://www.annals.org/cgi/content/abstract/113/10/740
Gerberding JL. Clinical practice. Occupational exposure to HIV in health care settings.N Engl J Med. 2003;348:826-33.http://content.nejm.org/cgi/content/extract/348/9/826
Ippolito G, Puro V, Petrosillo N, et al. Simultaneous infection with HIV and hepatitis Cvirus following occupational conjunctival blood exposure. JAMA. 1998;280:28.http://jama.ama-assn.org/cgi/content/full/280/1/28
Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the use of
antiretroviral agents in HIV-1-infected adults and adolescents. Department of Healthand Human Services. November 3, 2008;1-139.http://aidsinfo.nih.gov/Guidelines/GuidelineDetail.aspx?MenuItem=Guidelines&Search=Off&GuidelineID=7&ClassID=1
Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public HealthService. Updated U.S. Public Health Service guidelines for the management ofoccupational exposures to HIV and recommendations for postexposure prophylaxis.MMWR Recomm Rep. 2005;54(RR-9):1-17.http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5409a1.htm
Sulkowski MS, Ray SC, Thomas DL. Needlestick transmission of hepatitis C. JAMA.2002;287:2406-13.http://jama.ama-assn.org/cgi/content/full/287/18/2406
Wang SA, Panlilio AL, Doi PA, et al. Experience of healthcare workers takingpostexposure prophylaxis after occupational HIV exposure: findings of the HIVPostexposure Prophylaxis Registry. Infect Control Hosp Epidemiol. 2000;21:780-5.http://www.journals.uchicago.edu/doi/abs/10.1086/501736

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 17/48
13
TABLE 1: CLASSIFICATION OF EXPOSURES VERSUS NON-
EXPOSURES TO HIV
EXPOSURES
• Transfusion of blood or blood components
• Intravenous, intramuscular or subcutaneous injury with a needlecontaminated with a potentially infectious body fluid* whether or not the injuryresults in visible bleeding
• Any mucous membrane or break in the skin (e.g., non-healed wound ordermatologic condition that compromises the integrity of the skin) exposed toa potentially infectious body fluid
• Human bites:o Exposure to the individual doing the biting if the skin was broken resulting
in visible bleeding;
o Exposure to the bitten individual if the skin was broken and visiblybleeding AND the individual who was doing the biting was bleeding in themouth at the time of the bite
NON-EXPOSURES
• Intact skin or healed wound/skin lesion contaminated with potentiallyinfectious body fluid
• Intravenous, intramuscular or subcutaneous injury with a needlecontaminated with a fluid that is not potentially infectious
• Mucous membrane or break in the skin exposed to a fluid that is notpotentially infectious
*For exposures to HIV, a potentially infectious body fluid includes blood, amniotic fluid,
spinal fluid, pleural fluid, pus, semen, vaginal fluid, breast milk, or any fluid that is visiblybloody. Saliva, urine, and feces are not considered to be potentially infectious for HIV
unless visibly bloody.
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV andrecommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 18/48
14
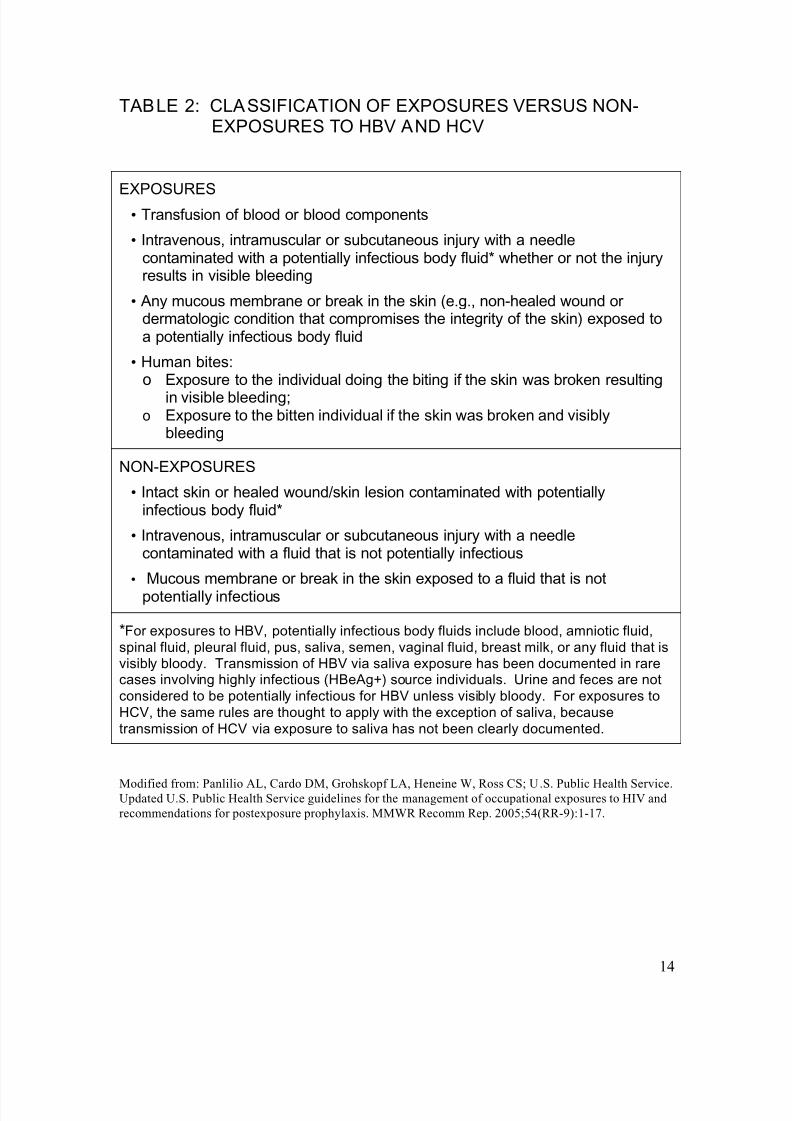
TABLE 2: CLASSIFICATION OF EXPOSURES VERSUS NON-
EXPOSURES TO HBV AND HCV
EXPOSURES
• Transfusion of blood or blood components
• Intravenous, intramuscular or subcutaneous injury with a needlecontaminated with a potentially infectious body fluid* whether or not the injuryresults in visible bleeding
• Any mucous membrane or break in the skin (e.g., non-healed wound ordermatologic condition that compromises the integrity of the skin) exposed toa potentially infectious body fluid
• Human bites:o Exposure to the individual doing the biting if the skin was broken resulting
in visible bleeding;o Exposure to the bitten individual if the skin was broken and visibly
bleeding
NON-EXPOSURES
• Intact skin or healed wound/skin lesion contaminated with potentiallyinfectious body fluid*
• Intravenous, intramuscular or subcutaneous injury with a needlecontaminated with a fluid that is not potentially infectious
• Mucous membrane or break in the skin exposed to a fluid that is notpotentially infectious
*For exposures to HBV, potentially infectious body fluids include blood, amniotic fluid,
spinal fluid, pleural fluid, pus, saliva, semen, vaginal fluid, breast milk, or any fluid that isvisibly bloody. Transmission of HBV via saliva exposure has been documented in rarecases involving highly infectious (HBeAg+) source individuals. Urine and feces are not
considered to be potentially infectious for HBV unless visibly bloody. For exposures to
HCV, the same rules are thought to apply with the exception of saliva, because
transmission of HCV via exposure to saliva has not been clearly documented.
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 19/48
15
TABLE 3: HIV PEP FOR PERCUTANEOUS INJURIES: SOURCEWITH KNOWN HIV INFECTION
Source with Known HIV Infection
Exposure Type
HIV-Infected Class 1* HIV-Infected Class 2^
Less Severe
– Solid needle
– Superficial injury
Recommend basic 2-drugPEP
Recommend expanded3-drug PEP
More Severe
– Large-bore, hollow needle
– Deep puncture
– Visible blood on device
– Needle used in patient'sartery or vein
Recommend expanded 3-drug PEP
Recommend expanded3-drug PEP
* HIV-positive, class 1 = asymptomatic HIV infection or known HIV RNA <1,500copies/mL.
^ HIV-positive, class 2 = symptomatic HIV infection, acquired immunodeficiencysyndrome, acute seroconversion, or known high viral load.
If drug resistance is a concern, obtain expert consultation. Initiation of PEPshould not be delayed pending expert consultation, and, because expertconsultation alone cannot substitute for face-to-face counseling, resourcesshould be available to provide immediate evaluation and follow-up care for allexposures.
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 20/48
16
TABLE 4: HIV PEP FOR PERCUTANEOUS INJURIES: SOURCEOF UNKNOWN HIV STATUS, UNKNOWN SOURCE,OR HIV-NEGATIVE
Infectious Status of Source
Exposure Type
Source of UnknownHIV Status*
Unknown Source^ HIV-Negative
Less Severe
– Solid needle
– Superficial injury
Generally no PEPwarranted; Considerbasic 2-drug PEP
1 for
source with HIV riskfactors
2
Generally no PEPwarranted; Considerbasic 2-drug PEP
1in
settings whereexposure to HIV-infected persons is
likely
No PEPwarranted
More Severe
– Large-bore, hollowneedle
– Deep puncture
– Visible blood ondevice
– Needle used inpatient's artery or vein
Generally no PEPwarranted; Considerbasic 2-drug PEP
1 for
source with HIV riskfactors
2
Generally no PEPwarranted; Considerbasic 2-drug PEP
1in
settings whereexposure to HIV-infected persons islikely
No PEPwarranted
* Source patient refuses testing or is unavailable.
^ Needle from sharps container.
1 The designation "consider PEP" indicates that PEP is optional and should be based on
an individualized decision between the exposed person and the treating clinicianregarding the risks versus benefits of PEP.
2 If PEP is initiated and the source is later determined to be HIV-negative, PEP shouldbe discontinued.
If drug resistance is a concern, obtain expert consultation. Initiation of PEP should not
be delayed pending expert consultation, and, because expert consultation alone cannotsubstitute for face-to-face counseling, resources should be available to provide
immediate evaluation and follow-up care for all exposures.
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 21/48
17
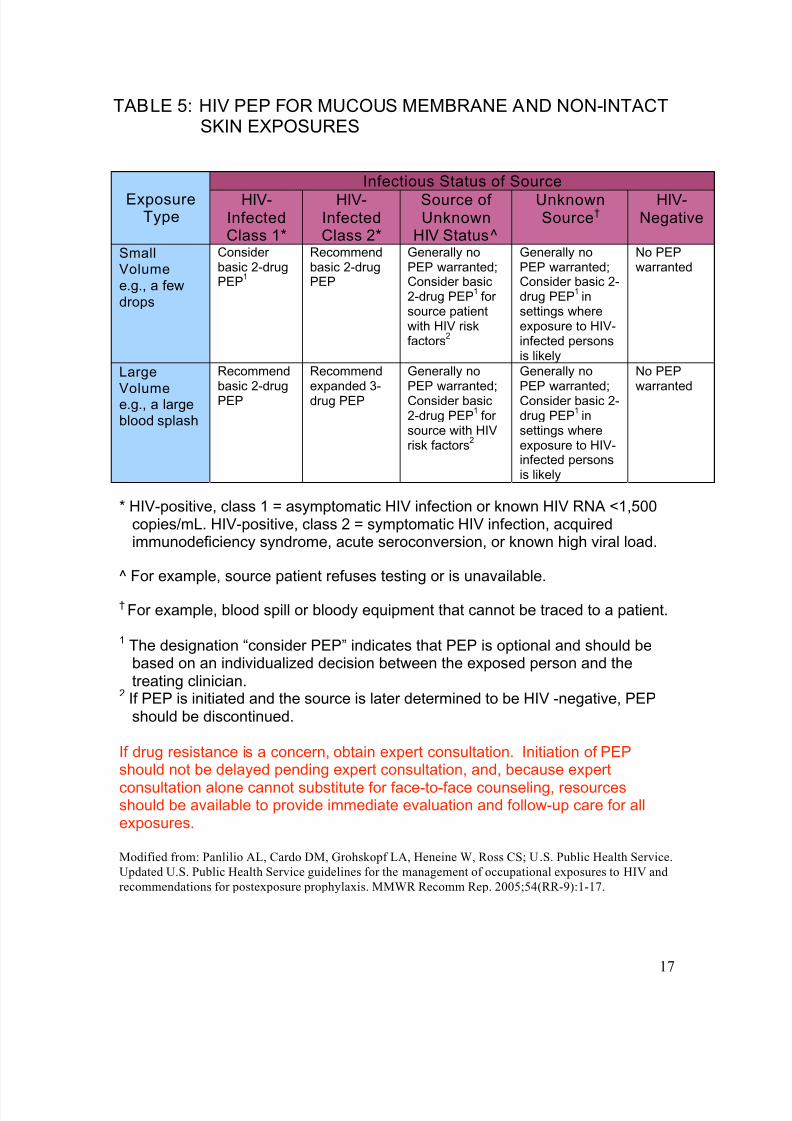
TABLE 5: HIV PEP FOR MUCOUS MEMBRANE AND NON-INTACTSKIN EXPOSURES
Infectious Status of Source
ExposureType
HIV-InfectedClass 1*
HIV-InfectedClass 2*
Source ofUnknown
HIV Status^
UnknownSource†
HIV-Negative
SmallVolume
e.g., a few
drops
Considerbasic 2-drugPEP
1
Recommendbasic 2-drugPEP
Generally noPEP warranted;
Consider basic2-drug PEP
1for
source patientwith HIV riskfactors
2
Generally noPEP warranted;Consider basic 2-drug PEP
1in
settings whereexposure to HIV-infected personsis likely
No PEPwarranted
Large
Volume e.g., a largeblood splash
Recommend
basic 2-drugPEP
Recommend
expanded 3-drug PEP
Generally no
PEP warranted;Consider basic2-drug PEP
1for
source with HIVrisk factors
2
Generally no
PEP warranted;Consider basic 2-drug PEP
1in
settings whereexposure to HIV-infected personsis likely
No PEP
warranted
* HIV-positive, class 1 = asymptomatic HIV infection or known HIV RNA <1,500copies/mL. HIV-positive, class 2 = symptomatic HIV infection, acquiredimmunodeficiency syndrome, acute seroconversion, or known high viral load.
^ For example, source patient refuses testing or is unavailable.
† For example, blood spill or bloody equipment that cannot be traced to a patient.
1 The designation “consider PEP” indicates that PEP is optional and should bebased on an individualized decision between the exposed person and thetreating clinician.
2 If PEP is initiated and the source is later determined to be HIV -negative, PEPshould be discontinued.
If drug resistance is a concern, obtain expert consultation. Initiation of PEPshould not be delayed pending expert consultation, and, because expert
consultation alone cannot substitute for face-to-face counseling, resourcesshould be available to provide immediate evaluation and follow-up care for allexposures.
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 22/48
18
TABLE 6: PREFERRED BASIC REGIMENS
ARV Components and Dosing
Zidovudine (AZT): 300mg bid or 200mg tid
plus
Lamivudine (3TC): 150mg bid or 300mg qd
Combivir (AZT/3TC): One tablet bid
Tenofovir (TDF): 300mg qd
plus
Emtricitabine (FTC): 200mg qd
Truvada (TDF/FTC): One tablet qd
Zidovudine (AZT): 300mg bid or 200mg tid
plus
Emtricitabine (FTC): 200mg qd
Tenofovir (TDF): 300mg qd
plus
Lamivudine (3TC): 150mg bid or 300mg qd
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 23/48
19
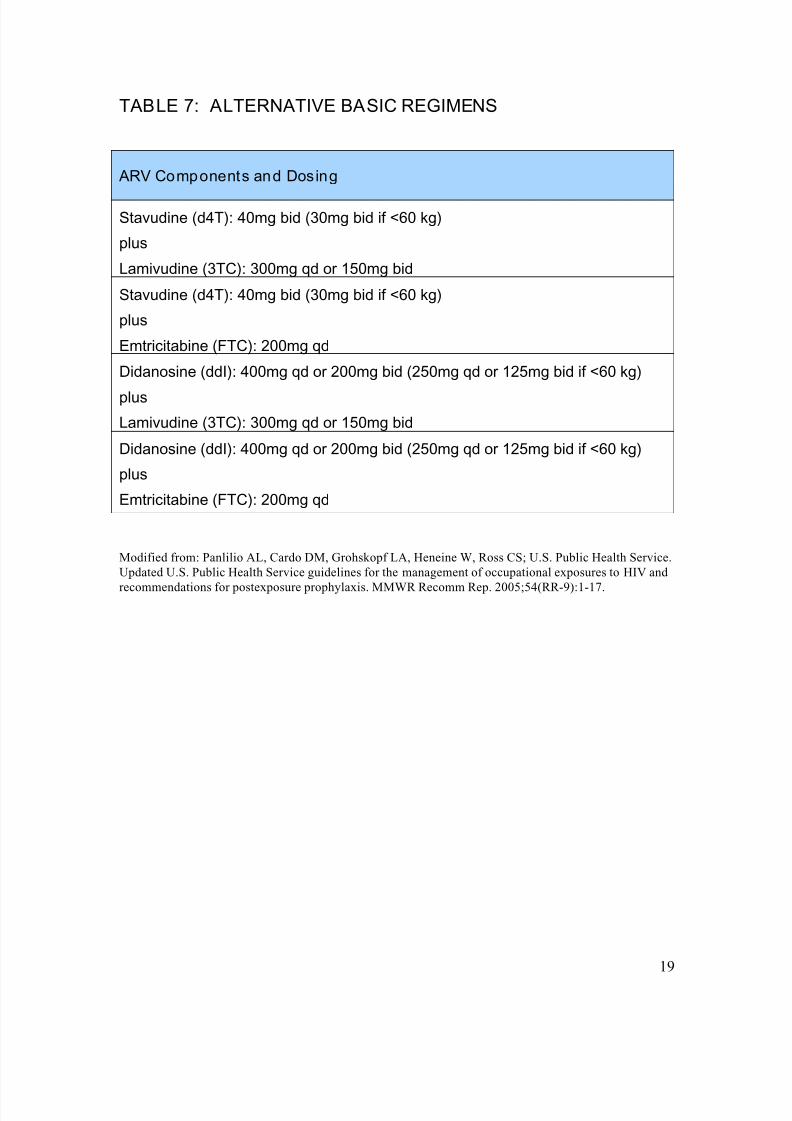
TABLE 7: ALTERNATIVE BASIC REGIMENS
ARV Components and Dosing
Stavudine (d4T): 40mg bid (30mg bid if <60 kg)
plus
Lamivudine (3TC): 300mg qd or 150mg bid
Stavudine (d4T): 40mg bid (30mg bid if <60 kg)
plus
Emtricitabine (FTC): 200mg qd
Didanosine (ddI): 400mg qd or 200mg bid (250mg qd or 125mg bid if <60 kg)
plus
Lamivudine (3TC): 300mg qd or 150mg bid
Didanosine (ddI): 400mg qd or 200mg bid (250mg qd or 125mg bid if <60 kg)
plus
Emtricitabine (FTC): 200mg qd
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 24/48
20
TABLE 8: PREFERRED AND ALTERNATIVE EXPANDEDREGIMENS
ARV Components and Dosing
Preferred Expanded Regimens:Basic Regimen plus the following
Lopinavir/Ritonavir (LPV/r): 200mg/50mg, 2 tabs bid
Al ternative Expanded Regimens:Basic Regimen plus one of the following
Atazanavir (ATV): 400mg qd, unless used in combination with tenofovir, in which
case ATV should be boosted with ritonavir, preferred dosing of atazanavir 300 mg+ ritonavir: 100 mg once daily
Atazanavir (ATV): 300mg qd
plus
Ritonavir (RTV): 100mg qd
Fosamprenavir (FPV): 1400mg bid
Fosamprenavir (FPV): 1400mg qd
plus
Ritonavir (RTV) : 200mg qd
Fosamprenavir (FPV) : 700mg bid
plus
Ritonavir (RTV): 100mg qd
Indinavir (IDV): 800mg bid
plus
Ritonavir (RTV): 100mg bid
Saquinavir (SQV) HGC or Tab: 1000mg bid
plus
Ritonavir (RTV): 100mg bid Nelfinavir (NFV): 1250mg bid
Efavirenz (EFV): 600mg qd
Modified from: Panlilio AL, Cardo DM, Grohskopf LA, Heneine W, Ross CS; U.S. Public Health Service.
Updated U.S. Public Health Service guidelines for the management of occupational exposures to HIV and
recommendations for postexposure prophylaxis. MMWR Recomm Rep. 2005;54(RR-9):1-17.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 25/48
21
TABLE 9: AUTHORS’ RECOMMENDED BASIC ANDEXPANDED REGIMENS
Preferred Basic Regimen
Tenofovir-Emtricitabine (Truvada): 300/200 mg; 1 tab qd
Preferred Expanded Regimen: Basic Regimen Plus One of the Following
Atazanavir (ATV): 300mg qd
plus
Ritonavir (RTV): 100mg qd
Darunavir (DRV): 600mg bid
plus
Ritonavir (RTV): 100mg bid
Fosamprenavir (FPV) : 700mg bid
plus
Ritonavir (RTV): 100mg qd
Lopinavir/Ritonavir (LPV/r): 200mg/50mg, 2 tabs bid

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 26/48
22
TABLE 10: PRIMARY SIDE EFFECTS AND TOXICITIES ASSOCIATED WITH ANTIRETROVIRAL AGENTSUSED FOR HIV POSTEXPOSURE PROPHYLAXIS, BYCLASS AND AGENTS
Class and Agent Side Effect and Toxici ty
Nucleoside and Nucleotide Reverse Transcriptase Inhibito rs(NRTI and NtRTI)
Class warning: Al l NRTIs have the potential to cause lactic acidosis with hepatic steatos is
Abacavir (Ziagen; ABC)
Hypersensitivity reaction
Didanosine (Videx; ddl)
Pancreatitis; peripheral neuropathy;nausea
Emtricitabine (Emtriva; FTC)
Minimal toxicity; hyperpigmentation/skindiscoloration
Lamivudine (Epivir ; 3TC)
Minimal toxicity
Stavudine (Zerit; d4T)
Peripheral neuropathy; lipodystrophy;pancreatitis; hyperlipidemia; rapidlyprogressive ascending weakness (rare)
Tenofovir (Viread; TDF)
Asthenia, headache: diarrhea, nausea,vomiting, and flatulence; renalinsufficiency, Fanconi syndrome;potential for osteopenia (with long termuse)
Zidovudine (Retrovir ; ZDV; AZT)
Bone marrow suppression: macrocyticanemia; gastrointestinal intolerance:headache, insomnia, asthenia
Fixed-Drug Combination NRTIs
Combivir (Zidovudine + Lamivudine)
See zidovudine; see lamivudine
Epzicom (Abacavir + Lamivudine)
See abacavir; see lamivudine

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 27/48
23
Trizivir (Zidovudine + Lamivudine + Abacavir)
See zidovudine; see lamivudine; seeabacavir
Truvada (Tenofovir + Emtricitabine)
See tenofovir; see emtricitabine
Non-nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
Delavirdine (Rescriptor ; DLV) Rash; increased transaminase levels;headache
Efavirenz (Sustiva; EFV)
Rash; central nervous systemsymptoms; increased transaminaselevels; false-positive cannabinoid test;teratogenic in monkeys
Etravirine (Intelence; ETR) Rash; nausea
Nevirapine (Viramune; NVP)
Contraindicated for use in postexposureprophylaxis
Fixed-Drug Combination of NRTIs + NNRTI
Atripla (Tenofovir + Emtricitabine +Efavirenz)
See tenofovir; see emtricitabine; seeefavirenz
Protease Inhibito rs
Atazanavir (Reyataz; ATV) Indirect hyperbilirubinemia; prolonged
PR interval: use caution in patients withunderlying conduction defects or onconcomitant medications that can causePR prolongation; hyperglycemia; fatmaldistribution; nephrolithiasis
Darunavir (Prezista; DRV) Skin rash (darunavir has sulfa moiety);hepatotoxicity; diarrhea, nausea;headache; hyperlipidemia;transaminase elevation; hyperglycemia;fat maldistribution
Fosamprenavir (Lexiva; FPV) Skin rash; diarrhea, nausea, vomiting;headache; hyperlipidemia;transaminase elevation; hyperglycemia;fat maldistribution

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 28/48
24
Indinavir (Crixivan; IDV) Nephrolithiasis; GI intolerance, nausea;indirect hyperbilirubinemia;hyperlipidemia; fat maldistribution
Lopinavir/ritonavir (Kaletra; LPV/rTV) GI intolerance, nausea, vomiting,
diarrhea (higher incidence with once-daily than twice-daily dosing); asthenia;hyperlipidemia, elevated serumtransaminase; hyperglycemia; fatmaldistribution
Nelfinavir (Viracept; NFV) Diarrhea; hyperlipidemia;hyperglycemia; fat maldistribution;serum transaminase elevation
Ritonavir (Norvir ; RTV) GI intolerance, nausea, vomiting,diarrhea; paresthesias (circumoral and
extremities); hyperlipidemia; hepatitis;asthenia; taste perversions;hyperglycemia; fat maldistribution
Saquinavir (Invirase; SQV) GI intolerance, nausea, vomiting,diarrhea; headache; elevatedtransaminase enzymes; hyperlipidemia;hyperglycemia; fat maldistribution
Tipranavir ( Aptivus; TPV) Hepatotoxicity; skin rash (hassulfonamide moiety); rare intracranialhemorrhage; hyperlipidemia;
hyperglycemia; fat maldistribution
Fusion Inhibitors
Enfuvirtide (Fuzeon; T-20) Local injection site reactions; increasedbacterial pneumonia; hypersensitivityreaction
Integrase Inhibito rs
Raltegravir (Isentress; RAL) Nausea, diarrhea; headache; pyrexia;
CPK elevation

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 29/48
25
Source: This table is adapted from Panel on Antiretroviral Guidelines for Adults and Adolescents.
Guidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescents. Department of
Health and Human Services. November 3, 2008;1-139.
CCR5 Antagonists
Maraviroc (Selzentry; MVC)
Abdominal pain; cough; dizziness;musculoskeletal symptoms; pyrexia;rash; upper respiratory tract infections;
hepatotoxicity; orthostatic hypotension

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 30/48
26
TABLE 11: RECOMMENDED PEP FOR EXPOSURE TO HBV
Baseline testing of all exposed HCWs should be performed for ALL exposures.
HBV PEP should be initiated immediately (within 24 hours) according to the following table from CDC
MMWR 2001 Vol 50 No. RR-11, Table 3:
Anti body Response Status Vaccinationstatus ofexposed
HCW*
Source HBsAg
Positive
Source HBsAg
Negative
Source unknown or not
available for testing
Unvaccinated HBIG x 1 and initiateHBV vaccine series
Initiate HBV vaccineseries
Initiate HBV vaccineseries
If known high risk source,
treat as if HBsAg positive
Previously
VaccinatedKnownresponder 1
No treatment No treatment No treatment
Knownnonresponder 2
HBIG x 1 and initiaterevaccination or HBIGx 2
No treatment
Consider
revaccination
If known high risk source,treat as if HBsAg positive
Anti bodyResponseUnknown
Test exposed HCW
for anti-HBs**
1. If adequate,1 notreatment is
necessary
2. If inadequate,2
administer HBIG x
1 and vaccine
booster
No treatment Test exposed HCW for
anti-HBs**
1. If adequate,1 notreatment is
necessary
2. If inadequate,2
administer vaccine
booster and recheck
titer in 1-2 months
* Those previously infected with HBV are immune to re-infection and do not require PEP.
Hepatitis B immune globulin; dose is 0.06 mL/kg intramuscularly. When indicated, HBIG shouldbe administered as soon as possible (preferably within 24 hours). Its effectiveness >7 days afterexposure is unknown.
1 A responder has adequate levels of serum antibody to HBsAg (i.e., anti-HBs
10 mlU/mL).
2 A nonresponder has inadequate response to vaccination (i.e., anti-HBs < 10 mlU/mL).
The option of giving one dose of HBIG and reinitiating the vaccine series is preferred fornonresponders who have not completed a second 3-dose vaccine series. For persons whopreviously completed a second vaccine series but failed to respond, two doses of HBIG one monthapart are preferred.
** Antibody to HbsAg.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 31/48 27
FORM 1: SUPERVISOR’S FOLLOW-UP REPORT OF INCIDENT
Supervisor to Complete:
Name of Employee or Client:
Days lost from work? Yes No Number of days:Work restrictions: Yes No Specify:
Describe in detail what employee/client was doing when accident/injury occurred (to the
best of your knowledge):
Specify part of body affected and how affected:
Explain in detail how and why this accident/injury occurred:

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 32/48 28
List action(s) taken to prevent similar accidents/injuries from occurring:
A preventable accident/injury is one in which the employee/client failed to do everything
within reason to prevent it from occurring.
In your opinion was this a preventable or non-preventable accident by the
employee/client?
Please explain:
Signature of Supervisor who conducted the investigation Date
Af fected Employee to Complete:
I have read the above and received a copy of the “Incident Report” and this“Supervisor’s Follow-up Report of Incident” (if requested).
Additional Comments:
Signature of Affected Employee Date

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 33/48 29
FORM 2: EXPOSURE CONTROL TEAM ASSESSMENT &REPORT OF POSSIBLE BLOODBORNE PATHOGENEXPOSURE
To be completed jointly by the Exposure Contro l Team and the affected HCW
I. INCIDENT INFORMATION (this section to be completed by the affected HCW)
Name of Affected HCW: Date of Birth:
Date and time of incident: Location of incident:
What procedure was being performed?
At what site and how did the exposure occur?
If the exposure was related to a sharp device, what device was used?
Type: Brand:
For a needlestick exposure:
Was this a needle that had been used in a vein or artery?
What was the gauge of the needle?
What was the estimated depth of the injury?
Was fluid injected? ___________ If yes, estimate the volume:
For mucous membrane or non-intact skin exposure:
Estimate the volume of material that splashed you:
Describe the condition of your mucous membrane or skin at the site of exposure
(e.g., chapped, abraded, intact):
II. INCIDENT CLASSIFICATION (to be completed by Exposure Control Team)
Date & Time of Evaluation:
Name of Exposure Control Team Member managing the HCW:
Does the incident described above represent a definite or possible exposure toone or more blood or body fluid pathogens (refer to Table 1 for assistance withthis determination)? Yes No
If Yes, complete this form and proceed with evaluation of HCW for PEP for thepathogen(s). If this incident does NOT represent an exposure to blood or body fluid
pathogens, PEP is not warranted; however, complete section III below and update
hepatitis B and tetanus vaccination status as needed.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 34/48 30
III. HEALTH CARE WORKER INFORMATION (to be completed jointly by the
affected HCW and the Exposure Control Team)
Hepatitis B vaccination (circle one): Full series Partial series NoneStatus of Response to Hepatitis B Vaccine (date of test):
History of chronic Hepatitis B? (Date of Diagnosis)
History of chronic Hepatitis C? (Date of Diagnosis)
History of HIV infection? (Date of Diagnosis)
Allergies to Medications:
Last Td booster:
HCW medical history & current medical conditions:
HCW current medications/supplements:
Baseline HBVsAb, HBsAg, HCV Ab, HIV Ab labs drawn: Yes No
If starting Antiretroviral PEP Medications, CBC, BUN, Cr, ALT drawn: Yes No
IV: RELEVANT SOURCE PATIENT INFORMATION to be completed by the
Exposure Control Team). Note: Attempts to gather this information should not delaydecision-making on PEP. If information on the source patient is not immediately
available, proceed to the next section and administer PEP if indicated. Additional
information on the source patient can be considered at the 72 hour follow-up visit.
Source patient name: Chart number:
Diagnosis(es):
History of Hepatitis B? Hepatitis C? HIV?
Abnormal ALT/AST? History of transfusion before 1985?
High-risk sexual behavior? Injection drug user?

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 35/48 31
If the source patient is HIV-infected, please provide the followi ng information if
known:
Stage of HIV disease:
History of antiretroviral therapy (if any):
Last CD4 count, with date:
Last HIV RNA (viral load), with date:
Antiretroviral resistance information (if known):
Any other information that may be relevant:
V. EXPOSURE CONTROL TEAM PEP RECOMMENDATIONS, BYPATHOGEN (To be completed by Exposure Control Team. See Tables 1-4 for
assistance.)HBV:
HCV:
HIV:
Td Booster indicated? Yes No
Does the HCW agree with these recommendations? Yes No
If not, describe plans of the HCW for PEP:
COMMENTS/NOTES/PEPLINE ADVICE:
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 36/48 32
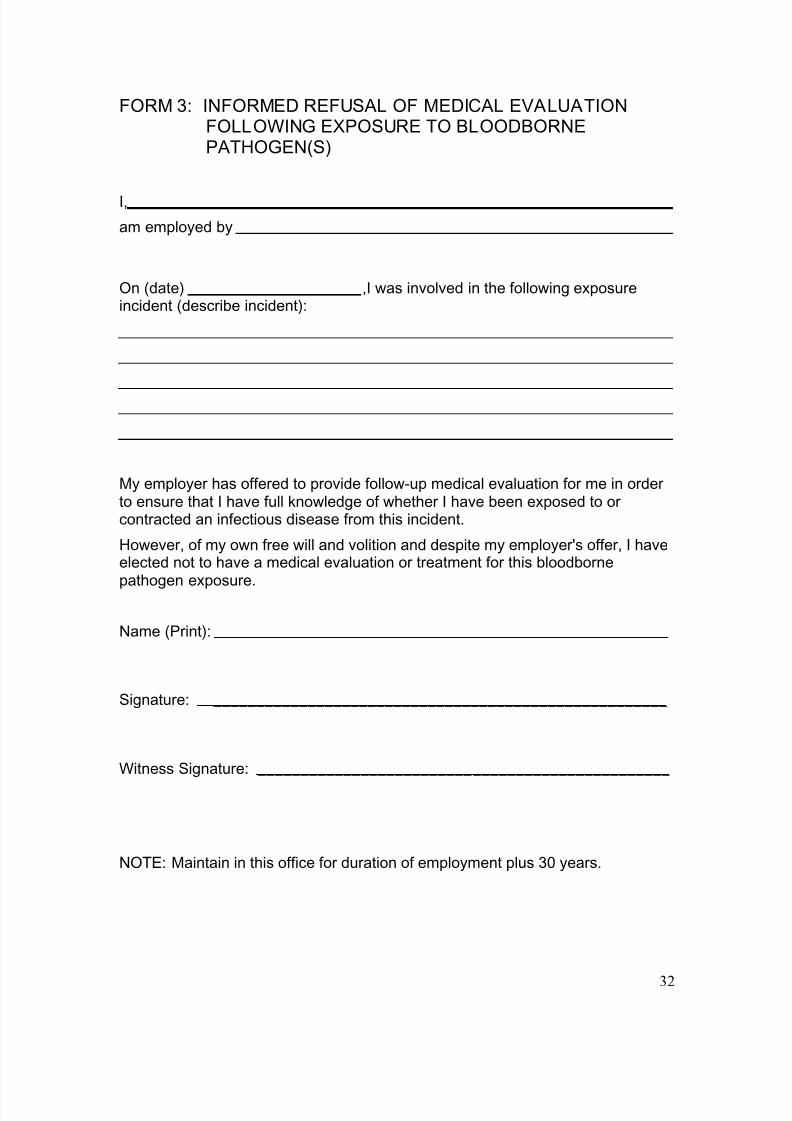
FORM 3: INFORMED REFUSAL OF MEDICAL EVALUATIONFOLLOWING EXPOSURE TO BLOODBORNEPATHOGEN(S)
I,
am employed by
On (date) ,I was involved in the following exposureincident (describe incident):
My employer has offered to provide follow-up medical evaluation for me in orderto ensure that I have full knowledge of whether I have been exposed to orcontracted an infectious disease from this incident.
However, of my own free will and volition and despite my employer's offer, I haveelected not to have a medical evaluation or treatment for this bloodbornepathogen exposure.
Name (Print):
Signature: _____________________________________________________
Witness Signature: ________________________________________________
NOTE: Maintain in this office for duration of employment plus 30 years.

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 37/48 33
FORM 4: EMPLOYEE REFUSAL TO RECEIVE HEPATITIS B
VACCINATION
STATEMENT
I understand that due to my occupational exposure to blood or other potentiallyinfectious materials, I may be at risk of acquiring hepatitis B virus (HBV) infection.I have been given the opportunity to be vaccinated with hepatitis B vaccine.
However, I decline hepatitis B vaccine at this time. I understand that by decliningthis vaccine, I may continue to be at risk of acquiring hepatitis B, a seriousdisease. If in the future I continue to have occupational exposure to blood orother potentially infectious materials and I want to be vaccinated with hepatitis Bvaccine, I can receive the vaccination series at no charge to me.
Name (Print): __________________________________
Signature: _____________________________________
Date: _________________________________________
Employer: _____________________________________
Witness: _______________________________________
8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 38/48 34
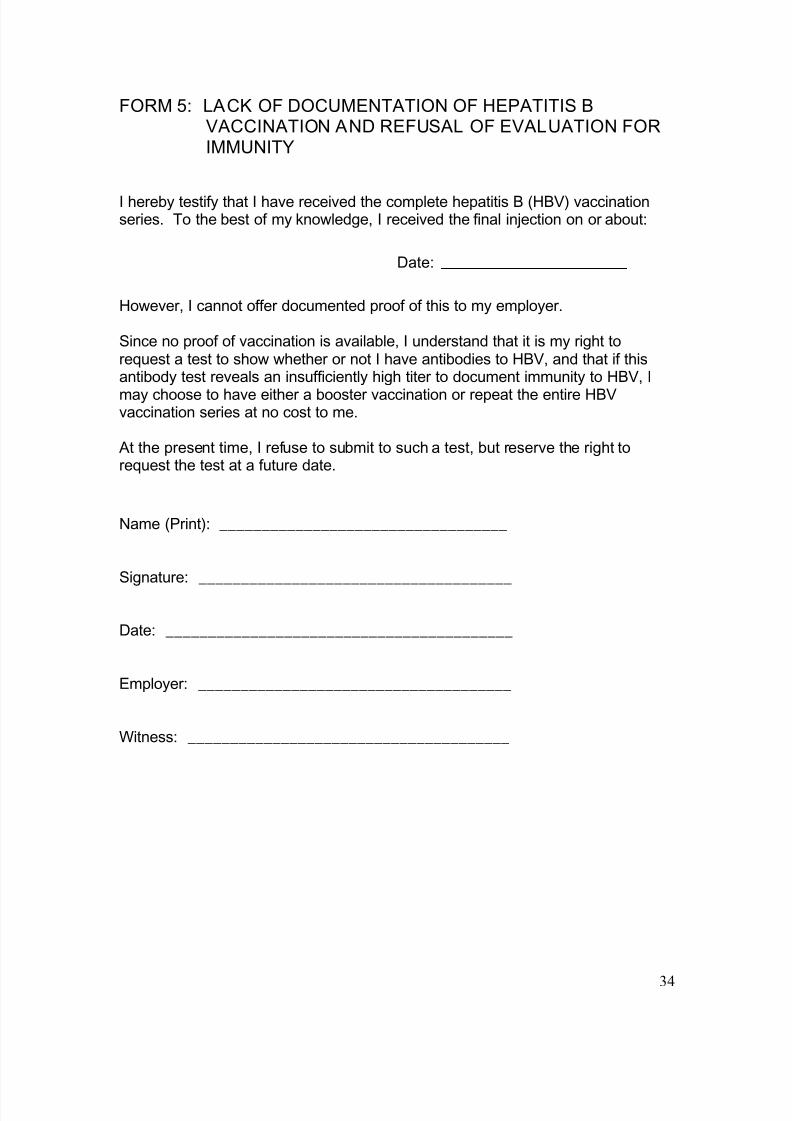
FORM 5: LACK OF DOCUMENTATION OF HEPATITIS B
VACCINATION AND REFUSAL OF EVALUATION FOR
IMMUNITY
I hereby testify that I have received the complete hepatitis B (HBV) vaccinationseries. To the best of my knowledge, I received the final injection on or about:
Date:
However, I cannot offer documented proof of this to my employer.
Since no proof of vaccination is available, I understand that it is my right torequest a test to show whether or not I have antibodies to HBV, and that if thisantibody test reveals an insufficiently high titer to document immunity to HBV, I
may choose to have either a booster vaccination or repeat the entire HBVvaccination series at no cost to me.
At the present time, I refuse to submit to such a test, but reserve the right torequest the test at a future date.
Name (Print): __________________________________
Signature: _____________________________________
Date: _________________________________________
Employer: _____________________________________
Witness: ______________________________________

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 39/48 35
FORM 6: CONSENT FOR HIV TEST
To be signed by HCW prior to baseline HIV antibody testing
I have been informed that my blood will be tested in order to detect whether ornot I have antibodies to the Human Immunodeficiency Virus (HIV), which is thecausative agent of Acquired Immune Deficiency Syndrome (AIDS). I understandthat the test is performed by withdrawing blood and then testing the blood forantibodies to HIV.
I have been informed that the test result may rarely be falsely positive (i.e.,suggest that a person is infected with HIV when in fact that person is not infected with HIV), or it may rarely be falsely negative (i.e., suggest that a personis not infected with HIV when in fact that person is infected with HIV). Iunderstand that HIV infection does not necessarily imply AIDS, the diagnosis ofwhich requires other clinical and laboratory evidence in conjunction with this
blood test.
I have been informed that if I have any questions regarding the nature of theblood test, the potential benefits & risks associated with testing, or alternatives tothe test, I may ask those questions before I decide to consent to the test.
I understand that the results of the test are confidential and will only be releasedto those health care practitioners directly responsible for my care and treatmentand to others as required by law. I further understand that no additional releaseof the results will be made without my written authorization.
By my signature below, I acknowledge that I have been given all the information Idesire concerning the blood test and release of its results, and that all of myquestions about the test have been answered. I hereby state my consent for theperformance of test on my blood to detect evidence of infection with the HumanImmunodeficiency Virus (HIV).
Name (Print): _________________________________________________
Signed: ______________________________________________________
If signed by other than the patient, indicate relationship: _________________
Date: ___________________

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 40/48 36
FORM 7: INCIDENT REPORT
Af fected Health Care Work er to compl ete, wi th Supervi sor Signatur e at bott om
Name:
Date of birth: Gender: Marital Status: No. Dependents:
Parent/Guardian (if applicable):
Location of incident (specific address):
Date and time of incident:(Day of week) (Date) (Time, a.m. or p.m.)
Did you return to work during the next scheduled shift? Yes No
If “No,” will wage loss exceed six work days? Yes No Not sure
Date of return, if returned to work
Description of incident:
Specify part of body affected and how affected:
Names of witness(es) to the incident:
Intervention/Attending Physician's name/address/phone number:
Outcome:
First reported to:Name, Position, Date
Signature of Employee Position Date
Signature of Supervisor Position Date
Check all that apply:Received Medical Treatment: Yes NoGiven Work Restrictions: Yes No Absence from work: Yes No
HUMAN RESOURCES USE ONLY
Workers’ Comp Claim Filed: Yes No N/A Signature: Date:

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 41/48 37
FORM 8: SHARPS INJURY LOG
To be completed by exposed employee, with addit ional signatures at bottom
Name: Date:
Job classification: Program:
Source patient:
Date and time of exposure:
Procedure being performed:
Instrument being used: Brand: Size:
Describe the incident:
Was a safety device used? Yes No
If “Yes,” was the safety feature activated? Yes No
Did the injury occur before or after activation of protective mechanism? Yes No
If a safety device were not used, could a safety device have prevented the injury?
Yes No
If “Yes,” how:
Could any of the following controls have prevented the injury? Describe how.
Engineering control
Administrative control
Work Practice control
Signatures: Date:
Exposed Employee: _____________________
Supervisor: ____________________________
Safety Director: _________________________

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 42/48 38
FORM 9: SEVENTY-TWO HOUR FOLLOW-UP VISIT
HCW Name: Date of Exposure:
Managing Clinician: Date:
I. Record PEP interventions that were made at initial visit (if any), HCWadherence to these recommendations, and any HCW concerns regarding
these recommendations:
II. Record any new information that may have become available about the
Source Patient or the exposure since the initial evaluation:
III. Record baseline laboratory studies performed on HCW at the initial visit:
IV. List changes, if any, to PEP recommendations made at initial visit, including
any interventions performed today (e.g., vaccinations, new medications, etc.):
1. HIV:2. HBV:3. HCV:
4. Other interventions or changes performed today:
V. List indicated vaccinations, blood tests, and follow-up visits (check box ifindicated): Hepatitis B vaccine #2 in 1 month on
Hepatitis B vaccine #3 in 6 months on
Hepatitis B immune globulin (HBIG)1 in 1 month on
Return visit in 2 weeks (if on antiretroviral therapy for HIV PEP) on
Repeat HIV antibody testing in
o 6 weeks on
o 3 months on
o 6 months on
Repeat Anti-HCV antibodies and ALT in 6 months on
If source patient is HCV+ with documented viral load, consider HCV Viral
Load at 6 week follow-up on
1 A 2
nd dose of HBIG one month later is indicated only in the very rare scenario of an exposure to a source
patient with known or suspected chronic HBV infection involving a HCW who is a known non-responder
to two HBV vaccination series (see Table 3 from CDC Guidelines: MMWR 2001 Vol 50 No. RR-11).

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 43/48 39
FORM 10: HEALTH CARE WORKER WRITTEN OPINION
NOTE: The Healthcare Worker’s Written Opinion must be completed and givento employee within 15 days after the completion of the evaluation.
Date: ____________________________
Employee Name: SSN:
Provider Signature:
NOTE: Information concerning the source individual’s HIV, HBV, or HCV statusmust be treated as confidential.
1. The employee has been informed of the results of the evaluation
On date: by whom:
2. The employee has been told about any medical conditions resulting fromexposure to blood or other infectious diseases which require further evaluation ortreatment (see Summary of Bloodborne Diseases on next page)
On date: by whom:
Original to employeeCC: EmployerCC: Employee Record/CHC Chart

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 44/48 40
SUMMARY OF BLOODBORNE DISEASES
Acquisition of bloodborne pathogens, most commonly via percutaneous injurywith a contaminated needle, is a major concern to health care workers. Morethan 20 diseases have been transmitted in the hospital setting by needle sticks
including HIV, hepatitis B, hepatitis C, syphilis, and malaria.
Prevention of transmission in the hospital setting of these agents requires strictadherence to universal blood and body fluid precautions, use of propertechniques for obtaining blood and disposing of needles and sharps, andimmunization of hospital personnel with significant exposure to blood or bodyfluids with hepatitis B vaccine.
DISEASES THAT CAN BE
TRANSMITTED BY BLOOD OR
OTHER POTENTIALLY INFECTIOUS
MATERIALS
OTHER POTENTIALLY INFECTIOUS
MATERIALS THAT MAY CONTAIN
BLOODBORNE PATHOGENS
Hepatitis B Virus (HBV)
Human Immunodeficiency Virus (HIV)Hepatitis C Virus (HCV)
Delta Hepatitis
SyphilisMalariaBabesiosis
Brucellosis
Leptospirosis ArboviraI InfectionsRelapsing Fever
Creutzfeldt-Jakob DiseaseHuman T-Lymphotrophic Virus Type 1Cytomegalovirus (CMV)
Semen
Vaginal secretionsCerebrospinal fluid
Synovial fluid
Pleural fluidPericardial fluidPeritoneal fluid
Amniotic fluid
Saliva in dental procedures Any body fluid visibly contaminated withblood
Any unfixed tissue or organ from a humanHIV- or HBV-containing cell, tissue, ororgan cultures; and culture medium
Blood, organs, or other tissues from HIV- orHBV-infected experimental animals
Source U S Department of Labor (1989)

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 45/48 41
FORM 11: TWO WEEK FOLLOW-UP VISIT:RECOMMENDATIONS FOR HCW
To be completed by the managing clin ician; copy to HCW after completed
HCW Name: Date of Birth:
Managing Clinician: Date/Time:
I. Record PEP interventions made to date, including the HIV PEP regimen thatwas prescribed, HCW adherence to these recommendations, and any HCW
concerns regarding these recommendations:
II. Record any new information that may have become available about thesource patient or the exposure since the last evaluation:
III. Record any laboratory studies performed on HCW since the exposure:
IV. List changes, if any, to HIV PEP recommendations made at prior visits, and
any other interventions performed or recommended today (e.g., vaccinations,
referrals, etc.):
V. Reminders to HCW regarding follow-up blood tests and vaccinations (check
box if indicated):
Hepatitis B vaccine #2 on
Hepatitis B vaccine #3 on
Hepatitis B immune globulin (HBIG)1 on
Repeat HIV antibody testing at
o 6 weeks ono 3 months on
o 6 months on
Repeat Anti-HCV antibodies and ALT on
1 A 2
nd dose of HBIG one month later is indicated only in the very rare scenario of an exposure to a source
patient with known or suspected chronic HBV infection involving a HCW who is a known non-responder
to two HBV vaccination series (see Table 3 from CDC Guidelines: MMWR 2001 Vol 50 No. RR-11).

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 46/48
42
FORM 12: SIX WEEK FOLLOW-UP VISIT:RECOMMENDATIONS FOR HCW
To be completed by the managing clin ician; copy to HCW after completed
HCW Name: Date of Birth:
Managing Clinician: Date/Time:
I. Record adherence with PEP regimen, total duration of PEP completed, and
any side effects that have persisted:
II. Record any immunizations or laboratory studies performed on HCW since the
exposure:
III. Perform HIV antibody test:
IV. Consider Performing HCV antibody test:
V. Reminders to HCW regarding follow-up blood tests and vaccinations (checkbox if indicated):
Hepatitis B vaccine #3 on Repeat HIV antibody testing at
o 3 months on and
o 6 months on
Repeat Anti-HCV antibodies and ALT on

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 47/48
43
FORM 13: TWELVE WEEK FOLLOW-UP VISIT:RECOMMENDATIONS FOR HCW
To be completed by the managing clin ician; copy to HCW after completed
HCW Name: Date of Birth:
Managing Clinician: Date/Time:
I. Record any immunizations or laboratory studies performed on HCW since the
exposure:
II. Perform HIV antibody test:
IV. Consider HCV antibody test and consider testing for HCV RNA if earlierdiagnosis of HCV is desired:
V. Reminders to HCW regarding follow-up blood tests and vaccinations (checkbox if indicated):
Hepatitis B vaccine #3 on
Repeat HIV antibody testing at
o 6 months on
Repeat Anti-HCV antibodies and ALT on

8/19/2019 PEP Manual
http://slidepdf.com/reader/full/pep-manual 48/48
FORM 14: TWENTY-FOUR WEEK FOLLOW-UP VISIT:RECOMMENDATIONS FOR HCW
To be completed by the managing clin ician; copy to HCW after completed
HCW Name: Date of Birth:
Managing Clinician: Date/Time:
I. Record any immunizations or laboratory studies performed on HCW since theexposure:
II. Perform HIV antibody test:
IV. Perform HCV antibody test:
V. If patient receiving hepatitis B vaccine series, give 3rd dose: