bmjopen.bmj.combmjopen.bmj.com/content/bmjopen/6/5/e010439.draft-revisions.pdf · for peer review...
TRANSCRIPT

For peer review only
Upper gastrointestinal bleeding increases risk of dialysis and all-cause mortality in patients with chronic kidney
disease
Journal: BMJ Open
Manuscript ID bmjopen-2015-010439
Article Type: Research
Date Submitted by the Author: 03-Nov-2015
Complete List of Authors: Liang, Chih-Chia; China Medical University Hospital, Division of Nephrology Chou, Che-Yi; China Medical University Hospital, Division of Nephrology Chang, Chiz-Tzung; China Medical University Hosptial, Division of
Nephrology Wang, I-Kuan; China Medical University Hospital, Division of Nephrology Huang, Chiu-Ching; China Medical University Hospital, Department of Internal Medicine
<b>Primary Subject Heading</b>:
Gastroenterology and hepatology
Secondary Subject Heading: Renal medicine
Keywords: chronic kidney disease, Dialysis < NEPHROLOGY, mortality
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 29 M
ay 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010439 on 5 May 2016. D
ownloaded from

For peer review only
Upper gastrointestinal bleeding increases risk of dialysis and
all-cause mortality in patients with chronic kidney disease
Chih-Chia Liang MD1,2,3,4
, Che-Yi Chou PhD1,2,4
, Chiz-Tzung Chang PhD1,2, I-Kuan
Wang MD1,2, Chiu-Ching Huang MD
1,2,3
1Kidney Institute and Division of Nephrology, Department of Internal Medicine, China
Medical University Hospital, Taichung 404, Taiwan
2College of Medicine, China Medical University, Taichung 404, Taiwan
3Graduate Program of Translational Medicine, China Medical University, Taichung
404, Taiwan
4Chih-Chia Liang and Che-Yi Chou equally contribute to this work
Correspondence: Chiu-Ching Huang MD
Address of corresponding author: Kidney Institute and Division of Nephrology,
Department of Internal Medicine, China Medical University Hospital, No. 2, Yu-der
Road, North District, Taichung 40447, Taiwan
Tel: +886-4-22052121-3483, Fax: +886-4-22058883, E-mail: [email protected]
Running title: UGI bleeding and risk of chronic dialysis
Word count: Abstract: 244; Text: 2131
Page 1 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Abstract
Objective
Lower renal function is associated with higher risk of upper gastrointestinal bleeding
(UGIB) in patients with chronic kidney disease not on dialysis (CKD-ND). It is
unclear if UGIB increases risk for chronic dialysis. The aim of the study was to
investigate risk of chronic dialysis in CKD-ND patients with UGIB using
competing-risks analysis.
Setting
Primary care for CKD patients between 2003 and 2009 were enrolled and
prospectively followed until Sep 2012 in one hospital
Primary and secondary outcome measures
Chronic dialysis (dialysis more than 3 months) started and all-cause mortality. The
risk of chronic dialysis was analyzed using competing-risks regression with
time-varying covariates.
Results
We analyzed 3163 CKD-ND patients with a mean age of 65 ± 14 years in 2.8
(interquartile range, 1.3-4.3) years. Of 3163 patients, 387 (12.4%) patients developed
UGIB, 989 (31.6%) patients started chronic dialysis, and 197 (6.3%) patients died.
UGIB increased all-cause mortality [aHR: 1.21, 95% confidence interval (CI): 1.05-
Page 2 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
1.38, p = 0.01]. UGIB was independently associated with a higher risk of chronic
dialysis (p < 0.01), with sub-distribution hazard ratio (aSHR) of 1.51 [95% CI, 1.24 –
1.83, p < 0.01] with adjustments for risk factors of chronic dialysis including basal
renal function, age, hemoglobin, serum albumin, and diabetes.
Conclusions
In patients with CKD stage 3-5 and not receiving dialysis, UGIB is associated with
increased risk of chronic dialysis and all-cause mortality after adjustments for
confounders.
Keywords
chronic kidney disease, upper gastrointestinal bleeding, chronic dialysis
Strengths and limitations of this study
� Upper gastrointestinal bleeding not only increases all-cause mortality but also
increases the risk of chronic dialysis in patients with chronic kidney disease.
� This association is showed in a cohort of CKD patients with adjustments for
confounders.
� The generalizability of this finding may be limited by one hospital and single
ethnic group.
Page 3 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Introduction
Upper gastrointestinal bleeding (UGIB) is a common gastrointestinal disorder in
patients with chronic kidney disease and not receiving dialysis (CKD-ND) 1 2. In
CKD-ND patients, the risk of UGIB was negatively associated with their renal
function at baseline 1. UGIB not only increased the risk of hospitalization but also
increased in-hospital mortality in CKD patients with and without dialysis 3. The
increased all-cause mortality associated with UGIB is usually explained by the
worsen comorbid conditions caused by UGIB.
Dialysis may be needed in patients with CKD-ND when UGIB leads to decreased
intravascular volume and the subsequent pre-renal acute kidney injury 4. Furthermore,
UGIB episodes may be the last straw for progression of CKD and may lead to chronic
dialysis if CKD-ND patients do not recover from acute kidney injury. However, the
long-term effect of UGIB on the risk of chronic dialysis in patients with CKD-ND is
not clear. The aim of the study was to investigate the risk of chronic dialysis after
UGIB in patients with CKD-ND. We utilized competing-risks analysis with
adjustments for all known confounders because both UGIB and CKD increase overall
mortality, and the risk of chronic dialysis may be overestimated if patients’ death was
not taken into consideration in the analysis 5 6.
Materials and Methods
Page 4 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Internal review board approval (DMR 99-IRB-301) was obtained for the review of
medical records, and the need for informed consent was waived. All patients in the
outpatient-based CKD program of China Medical University Hospital from June 2003
to December 2009 were analyzed. The CKD program included patients with CKD
stage 3-5 and not receiving dialysis diagnosed by nephrologists. No exclusion criteria
were applied. All patients were followed to the date of the date of initiation of chronic
dialysis including hemodialysis and peritoneal dialysis, loss to follow-up; death; or
until September 2012. There were two patients received kidney transplant and these
two patients were excluded in the analysis. As we aimed to investigate risk of chronic
dialysis, patients who received dialysis less than 3 months and patients who
discontinued dialysis because of a recovery of renal function were excluded. UGIB
was defined as melena, hematemesis, rectorrhagia, or the presence of red blood in
gastric lavage fluid, together with observation of a bleeding lesion or a lesion likely to
have bled on endoscopy of the upper digestive tract.7 Patients who had UGIB before
the date of enrollment of CKD program was defined as a history of UGIB. CAD was
defined as a positive exercise test, angiographic findings of at least one stenosis of
more than 50%, or positive findings on scintigraphy.8 Diabetes mellitus was defined
as use of insulin, use of a hypoglycemic agent, or a fasting plasma glucose level of
126 mg/dl or more.9 Hypertension was defined as taking antihypertensives without
Page 5 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
regard to the actual measurement of blood pressure, or having a systolic blood
pressure reading greater than 140 mm Hg or a diastolic blood pressure reading greater
than 90 mm Hg.10
A study nurse reviewed all the medical records and consulted a physician over
uncertainties. The study nurse and physician were blinded to the aim of the study, and
other physicians performed the analysis. Each patient’s body mass index (BMI), blood
urea nitrogen (BUN), and creatinine were measured at enrollment. Serum calcium,
phosphorus, and albumin were measured within 3 months. Estimated glomerular
filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology
Collaboration formula.11 The formula for white or other race was used because the
patients were all Chinese. The time-varying analysis used an average of three eGFR
measurements. Medications associated with a higher risk of UGIB, including
non-steroidal anti-inflammatory drugs (NSAIDs), aspirin, clopidogrel and warfarin,
were recorded based on the review of medical records.
Statistical analysis
Data were reported as mean ± standard deviation, median (interquartile range), or
frequency (percentage). All continuous variables were tested using skewedness and
kurtosis test for their normality. Data were analyzed using Student’s t test for
parametric variables, Kolmogorov-Smirnov test for non-parametric variables, or
Page 6 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
chi-square test for categorical variables. Possible confounders for all-cause mortality
were analyzed using multivariable Cox proportional hazard regression with
time-varying variables (eGFR and UGIB). Possible confounders of chronic dialysis
were analyzed using univariable competing-risks regression followed by multivariable
competing-risks regression with time-varying covariates. The competing-risks
regression was used because the Cox regression may over-estimate the risk of UGIB
when the competing events (mortality) were not analyzed.12 A sub-distribution hazard
ratio (SHR) and 95% confidence interval (CI) of confounders were calculated. In
multivariable analysis, the SHRs were reported as adjusted SHR (aSHR). The primary
outcome was defined as chronic dialysis and the competing event was patient’s death.
All analyses were performed using Stata version 13 SE (StataCorp, TX, USA) and a p
< 0.05 was considered statistically significant.
Results
Patient characteristics
We identified 3163 patients with CKD stage 3–5 and not on dialysis in the CKD
program (Table 1) in a median of 1.9 (interquartile range: 1.2–3.3) years. The mean
age was 65±14 years old and 1714 (54.2%) patients were male gender. Diabetes and
chronic glomerulonephritis were the main primary kidney disease. Of 3163 patients,
Page 7 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
226 (7.2%) patients had a history of UGIB and 380 (12.2%) patients had a history of
cardiovascular disease. The average BMI was 24.2±4.1 kg/m2, hemoglobin 10.6±2.4
g/dl, BUN 48±31 mg/dl, creatinine 3.8±2.9 mg/dl, calcium 9.1±0.7 mg/dl, phosphate
4.6±1.4 mg/dl, and serum albumin 3.4±0.6 mg/dl. In this study population, 61 (2.0%)
patients took NSAIDs, 351 (11.2%) patients took aspirin, 84 (2.9%) patients took
clopidogrel, and 64 (2.1%) patients took warfarin.
Outcomes and characteristics of patients with UGIB
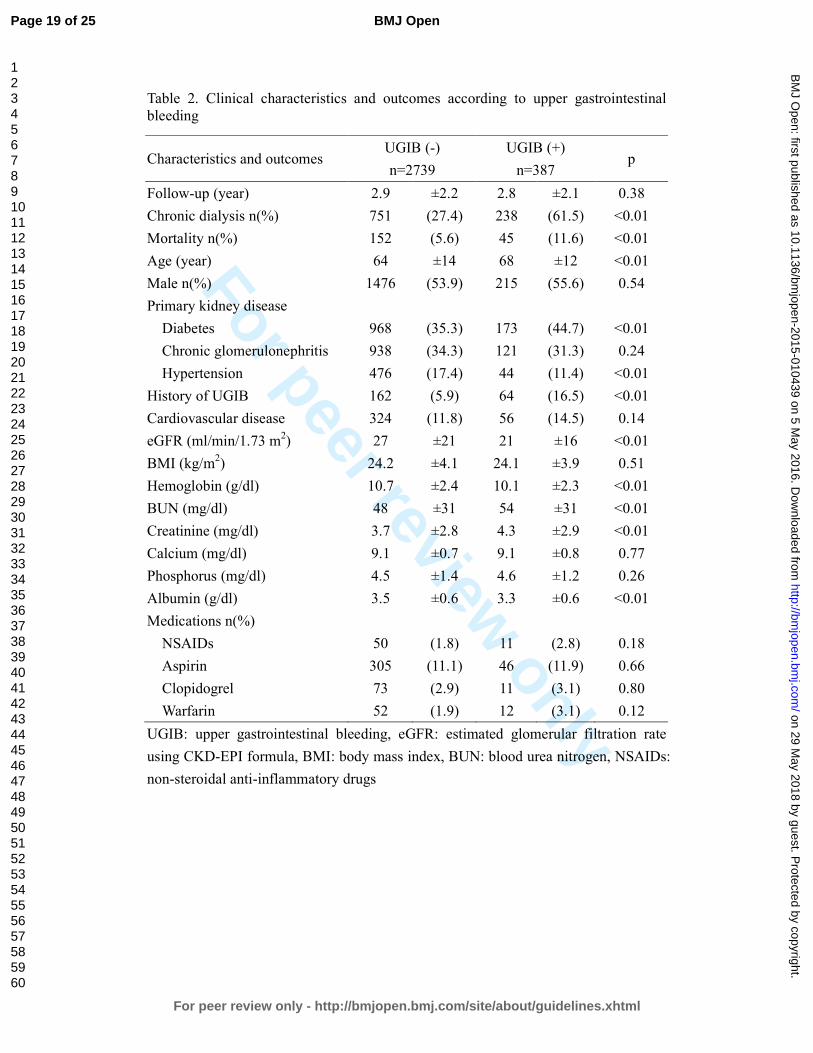
The times of follow-up were similar in patients with and without UGIB (2.9±2.2 vs.
2.8±2.1 years, p = 0.38, Table 2). The rate of chronic dialysis in patients with UGIB
was higher than that of patients without UGIB (61.5% vs. 27.4%, p < 0.01). Patients
with UGIB were associated with a higher overall mortality rate, compared to patients
without UGIB (11.6% vs. 5.6%, p < 0.01). Therefore, a competing-risks analysis was
necessary to determine the risk of chronic dialysis in patients with and without UGIB.
In patients’ characteristics, patients with UGIB (68±12 years) were older than patients
without UGIB (64±14 years, p < 0.01) were. The percentage (55.6%) of diabetes as
the primary kidney disease was higher in patients with UGIB had diabetes (35.3% in
patients without UGIB, p < 0.01). Hypertension was the primary kidney disease in
11.4% of the patients with UGIB and 17.4% of the patients without UGIB (p < 0.01).
Page 8 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
The proportion of patients with cardiovascular disease in patients with UGIB was not
different from that of patients without UGIB. The patients with UGIB had a lower
eGFR (p < 0.01), a lower hemoglobin (p < 0.01), a higher BUN (p < 0.01), a higher
creatinine (p < 0.01), and a lower serum albumin (p < 0.01) than the patients without
UGIB did. There were no differences in serum calcium and phosphate levels in the
patients with and the patients without UGIB. The proportion of patients who took
NSAIDs, aspirin, clopidogrel, and warfarin were not different between the patients
with UGIB and the patients without UGIB.
UGIB increases all-cause mortality
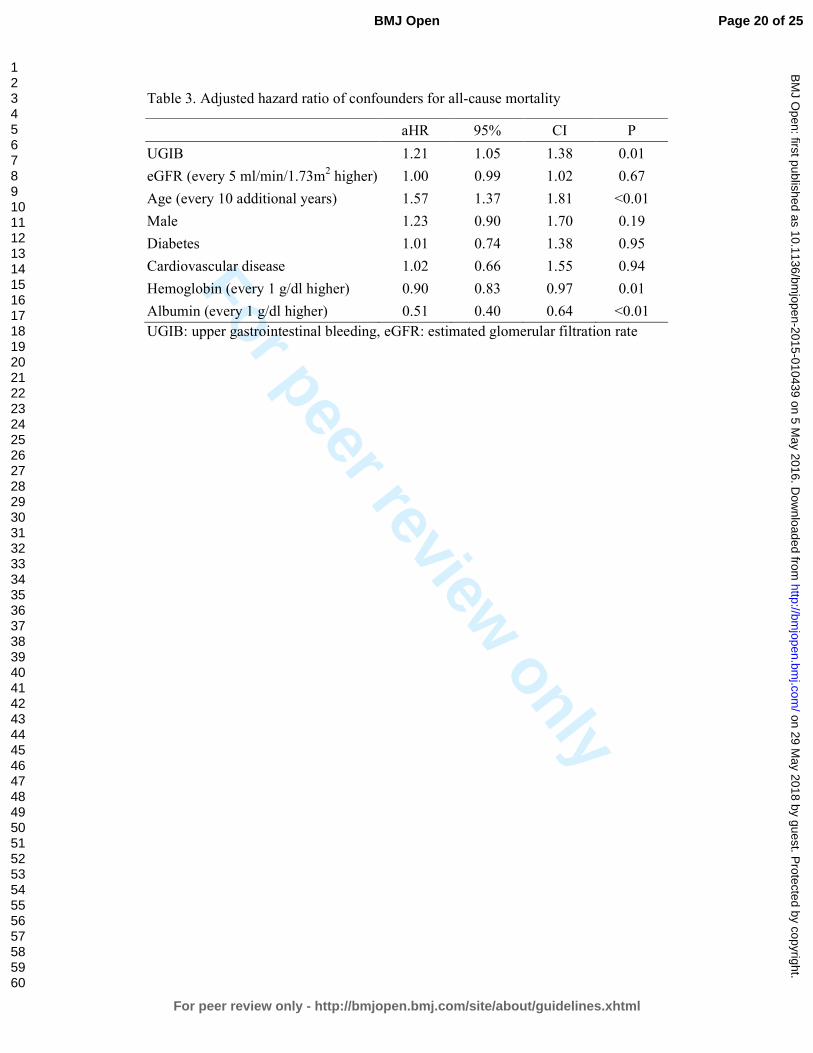
In the Cox regression with adjustments for confounders of all-cause mortality (Table
3), UGIB was independently associated with higher all-cause mortality with an
adjusted hazard ratio (aHR) of 1.21 (95% CI: 1.05-1.38, p = 0.01). Age (p < 0.01),
hemoglobin (p = 0.01), and albumin (p < 0.01) were associated with all-cause
mortality. The aHR were 1.57 (95% CI: 1.37-1.81) for every 10 additional years, 0.90
(95% CI: 0.83-0.97) for every 1 g/dl higher in hemoglobin, and 0.51 (95% CI:
0.40-0.64) for every 1 g/dl higher in serum albumin. Patients’ eGFR, gender, diabetes,
and comorbid cardiovascular disease were not associated with all-cause mortality.
Page 9 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
UGIB increased risk of chronic dialysis
The SHRs of the competing-risks analysis were showed in Table 4 in both univariable
and multivariable analyses. UGIB largely increased risk for chronic dialysis in
univariable analysis with a SHR of 2.51 (95% CI: 2.17-2.90, p < 0.01). Higher eGFR
(SHR: 0.74, 95% CI: 0.71–0.76, p < 0.01), male gender (SHR: 0.78, 95% CI: 0.69–
0.89, p < 0.01), higher hemoglobin (SHR: 0.78, 95% CI: 0.76–0.81, p < 0.01), and
higher serum albumin (SHR: 0.53, 95% CI: 0.48–0.59, p < 0.01) were associated
lower risk for chronic dialysis. In contrast, a history of UGIB (SHR: 1.36, 95% CI:
1.08–1.71, p = 0.01), diabetes as the primary kidney disease (SHR: 1.66, 95% CI:
1.46–1.89, p < 0.01), and higher BUN (SHR: 1.19, 95% CI: 1.17–1.22 for every 10
mg/dl higher, p < 0.01) were associated with higher risk of chronic dialysis. The
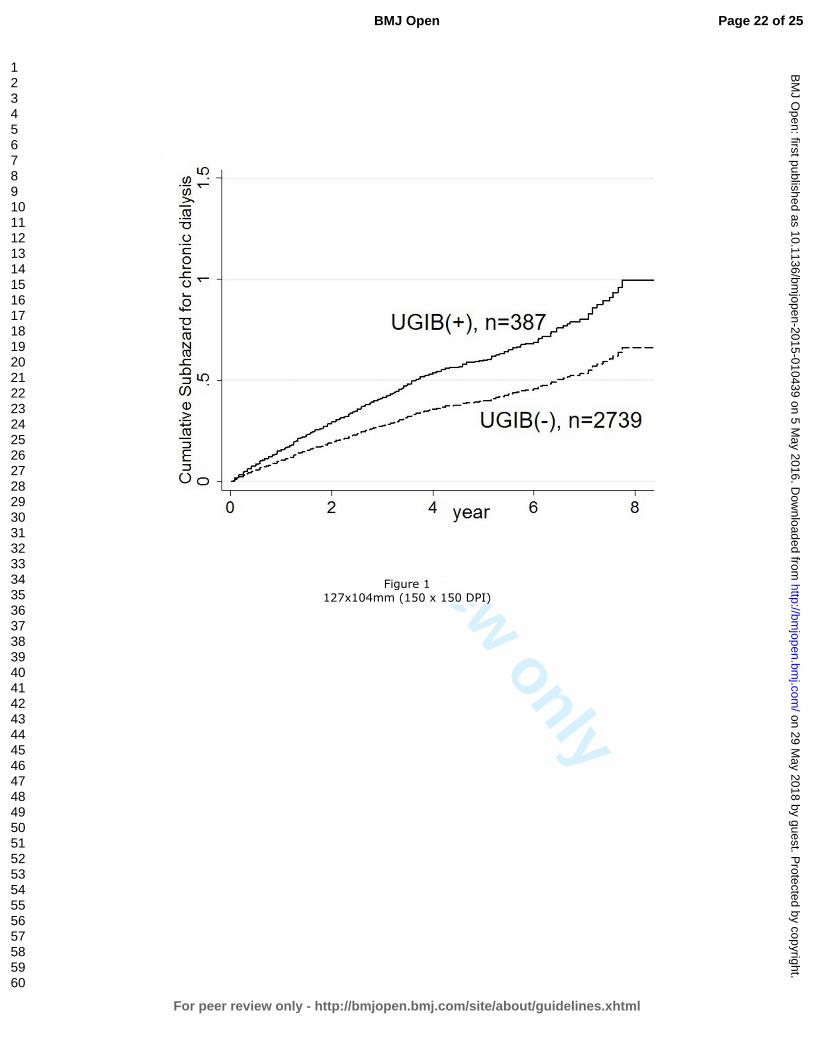
cumulative sub-hazard of chronic dialysis in patients with UGIB and patients without
UGIB was shown in Figure 1. Patients with UGIB were associated with a higher
hazard for chronic dialysis than patients without UGIB did (aSHR: 1.51, 95% CI:
1.24-1.83, p < 0.01). The confounders of chronic dialysis included patients’ eGFR
(aSHR: 0.81, 95% CI: 0.77–0.85, p < 0.01) and patients’ age (aSHR: 0.92, 95% CI:
0.86–0.98 for every 10 additional year, p < 0.01). Patients with diabetes as the
primary kidney disease were also associated with higher risk for chronic dialysis
(aSHR: 1.29, 95% CI: 1.10–1.51, p < 0.01). Hemoglobin (aSHR: 0.94, 95% CI: 0.90–
Page 10 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
0.98, p < 0.01) and serum albumin (aSHR: 0.75, 95%CI: 0.66–0.86, p < 0.01) were
associated with lower risk of chronic dialysis.
Discussion
In this cohort study of CKD stage 3-5 ND patients, UGIB was associated with higher
risk of chronic dialysis using competing-risks analysis with adjustments for
confounders. The competing-risks analysis was critical to this study because UGIB
remarkably increased all-cause mortality (Table 3). Patients’ renal function was one of
the most important confounders for chronic dialysis. The risk of chronic dialysis was
reduced by 20% for every five ml/min/1.73m2 higher of eGFR (Table 4) and the
SHRs of eGFR were similar in univariable and multivariable analysis. In summary of
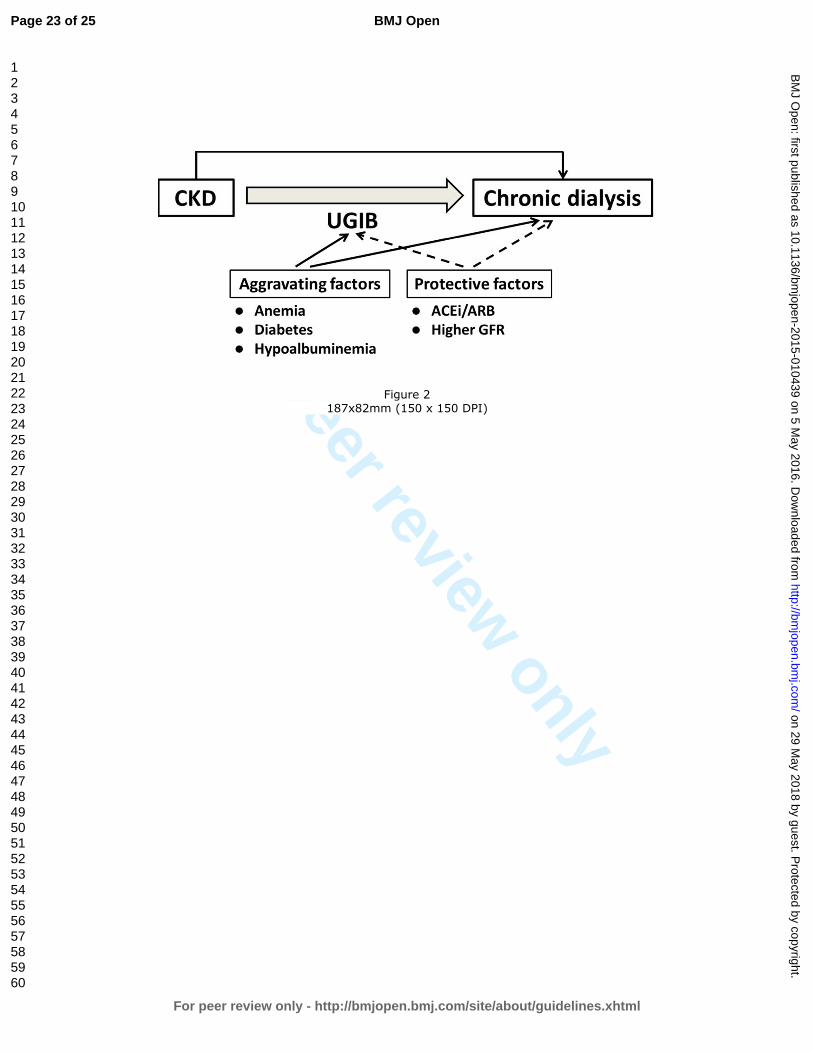
our previous studies 1 13 14
and this study (Figure 2), patients with CKD-ND were
more at risk for developing UGIB and UGIB may further accelerate the progression
of CKD to chronic dialysis. The common aggravating factors of CKD and UGIB are
anemia, diabetes, and hypoalbuminemia. On the other hand, higher GFR and uses of
angiotensionogen converting enzyme inhibitor (ACEi) or angiotensin II receptor
blocker (ARB) may protect from UGIB in this scenario. Some beneficial effects of
ACEi and ARB may come from their association with decreased risk of UGIB
independent of patients’ renal function 14.
Page 11 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
In other confounders of chronic dialysis, diabetes was consistently associated with the
risk of chronic dialysis in both univariable and multivariable analyses. This may not
be surprised because diabetes is a well-known confounder of dialysis. However, male
patients, a history of UGIB, and BUN were not associated with chronic dialysis in
multivariable analysis, which may imply that UGIB was a more robust confounder of
chronic dialysis in this study. Although NSAIDs were well-known risk factors for
UGIB and chronic dialysis 15, we did not find a significant association of NSAIDs and
chronic dialysis. A limited number of patients who took these medications in this
study may explain this result.
Nausea/vomiting were uremic symptoms 16 and were indications of dialysis.
Nausea/vomiting were also common symptoms in patients with UGIB 17. Although
some CKD patients initiated dialysis because of UGIB-related nausea/vomiting rather
than uremic symptoms, the percentages of patients with nausea/vomiting at the
initiation of dialysis were similar in this study (data not shown). In addition, we
excluded these patients who underwent dialysis less than 3 months and discontinued
dialysis because of a recovery of renal function. UGIB-related nausea/vomiting did
not explain the association of UGIB and chronic dialysis in this study.
Page 12 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
The limitations of this study were its observational study design and the inclusion of
all patients in single medical center in Taiwan. This may limit the generalizability of
our finding to other ethnic groups. More studies of various ethnic groups and multiple
institutions are required to confirm our results. In spite of the limitations, this is the
first study indicating the association between UGIB and chronic dialysis independent
of all confounding factors that were considered. This association suggests UGIB not
only leads to acute renal failure due to intravascular volume depletion, but also
long-term consequence of irreversible kidney injury in this population.
Conclusions
Upper gastrointestinal bleeding is associated with higher risk of chronic dialysis in
patients with chronic kidney disease stage 3-5 and not receiving dialysis independent
of confounders of chronic dialysis such as diabetes and hypoalbuminemia. More
studies will be warranted to investigate if the reduction in UGIB risk may slow the
progression of CKD and delay the need of dialysis in patients with CND-ND.
Acknowledgments
This study was supported in part by Taiwan Ministry of Health and Welfare Clinical
Trial and Research Center of Excellence (DOH102-TD- B-111-004) and China
Page 13 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Medical University Hospital (DMR-101-019). The funders had no role in study design,
data collection and analysis, decision to publish, or preparation of the manuscript.
Contribution of Authors
Study concept, design, and acquisition of data: CC Liang; analysis, interpretation of
data, and drafting of the manuscript: CY Chou; critical revision of the manuscript for
important intellectual content: CT Chang, IK Wang; study supervision: CC Huang
Conflict of interest statement
The results presented in this paper have not been published previously in whole or
part. The authors have no conflicts of interest regarding the design or publication of
this study.
Data sharing statement
None
Page 14 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
References
1. Liang CC, Wang SM, Kuo HL, et al. Upper gastrointestinal bleeding in patients with
CKD. Clinical journal of the American Society of Nephrology : CJASN
2014;9(8):1354-9.
2. Yang JY, Lee TC, Montez-Rath ME, et al. Trends in acute nonvariceal upper
gastrointestinal bleeding in dialysis patients. Journal of the American Society of
Nephrology : JASN 2012;23(3):495-506.
3. Sood P, Kumar G, Nanchal R, et al. Chronic kidney disease and end-stage renal
disease predict higher risk of mortality in patients with primary upper
gastrointestinal bleeding. Am J Nephrol 2012;35(3):216-24.
4. Moreau R, Lebrec D. Acute renal failure in patients with cirrhosis: perspectives in
the age of MELD. Hepatology 2003;37(2):233-43.
5. Evans DW, Ryckelynck JP, Fabre E, et al. Peritonitis-free survival in peritoneal
dialysis: an update taking competing risks into account. Nephrology, dialysis,
transplantation : official publication of the European Dialysis and Transplant
Association - European Renal Association 2010;25(7):2315-22.
6. Bechade C, Guittet L, Evans D, et al. Early failure in patients starting peritoneal
dialysis: a competing risks approach. Nephrology, dialysis, transplantation : official
publication of the European Dialysis and Transplant Association - European Renal
Association 2014;29(11):2127-35.
7. Bernard B, Cadranel JF, Valla D, et al. Prognostic significance of bacterial infection
in bleeding cirrhotic patients: a prospective study. Gastroenterology
1995;108(6):1828-34.
8. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of
macrovascular events in patients with type 2 diabetes in the PROactive Study
(PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised
controlled trial. Lancet 2005;366(9493):1279-89.
9. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes
mellitus and impaired glucose tolerance. Archives of internal medicine
2005;165(8):863-7.
10. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for
hypertension: population study. BMJ (Clinical research ed) 2000;320(7233):479-82.
11. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular
filtration rate. Annals of internal medicine 2009;150(9):604-12.
12. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a
competing risk. J Am Stat Assoc 1999;94(446):496-509.
13. Liang CC, Muo CH, Wang IK, et al. Peptic ulcer disease risk in chronic kidney
disease: ten-year incidence, ulcer location, and ulcerogenic effect of medications.
Page 15 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
PloS one 2014;9(2):e87952.
14. Chou CY, Wang SM, Chang PH, et al. Angiotensin II receptor blocker prevents
upper gastrointestinal bleeding in hypertensive patients with chronic kidney disease
not on dialysis. Int J Clin Pract 2015.
15. Plantinga L, Grubbs V, Sarkar U, et al. Nonsteroidal anti-inflammatory drug use
among persons with chronic kidney disease in the United States. Ann Fam Med
2011;9(5):423-30.
16. Murtagh FE, Addington-Hall JM, Edmonds PM, et al. Symptoms in advanced renal
disease: a cross-sectional survey of symptom prevalence in stage 5 chronic kidney
disease managed without dialysis. Journal of palliative medicine
2007;10(6):1266-76.
17. Roderick PJ, Wilkes HC, Meade TW. The gastrointestinal toxicity of aspirin: an
overview of randomised controlled trials. British journal of clinical pharmacology
1993;35(3):219-26.
Page 16 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Legends
Figure 1. Cumulative sub-hazard for chronic dialysis in patients with and without
upper gastrointestinal bleeding (UGIB) using competing-risks regression with
adjustments for age, gender, diabetes, a history of UGIB, hemoglobin, blood urea
nitrogen (BUN), and albumin. (the primary outcome was chronic dialysis and the
competing events were patients’ death).
Figure 2. Upper gastrointestinal bleeding (UGIB) may accelerate the progression of
chronic kidney disease (CKD) and further increase the risk of chronic dialysis. In this
interactive scheme of UGIB and CKD, aggravating factors include anemia, diabetes,
and hypoalbuminemia, and protective factors contain a higher glomerular filtration
rate (GFR) and uses of angiotensionogen converting enzyme inhibitor (ACEi)/
angiotensin II receptor blocker (ARV).
Page 17 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Table 1. Clinical characteristics of all patients at enrollment
Characteristics n=3163
Age (year) 65±14
Male gender n (%) 1714(54.2)
Primary kidney disease
Diabetes 1141 (36.5)
Chronic glomerulonephritis 1059 (33.9)
Hypertension 520 (16.6)
History of UGIB 226 (7.2)
Cardiovascular disease 380 (12.2)
eGFR (ml/min/1.73 m2) 19.2 (9.5-34.7)
BMI (kg/m2) 24.2±4.1
Hemoglobin (g/dl) 10.6±2.4
BUN (mg/dl) 48±31
Creatinine (mg/dl) 3.8±2.9
Calcium (mg/dl) 9.1±0.7
Phosphorus (mg/dl) 4.6±1.4
Albumin (g/dl) 3.4±0.6
Medications n(%)
NSAIDs 61 (2.0)
Aspirin 351 (11.2)
Clopidogrel 84 (2.9)
Warfarin 64 (2.1)
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate
using CKD-EPI formula, BMI: body mass index, BUN: blood urea nitrogen, NSAIDs:
non-steroidal anti-inflammatory drugs,
Page 18 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Table 2. Clinical characteristics and outcomes according to upper gastrointestinal
bleeding
Characteristics and outcomes UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.9 ±2.2 2.8 ±2.1 0.38
Chronic dialysis n(%) 751 (27.4) 238 (61.5) <0.01
Mortality n(%) 152 (5.6) 45 (11.6) <0.01
Age (year) 64 ±14 68 ±12 <0.01
Male n(%) 1476 (53.9) 215 (55.6) 0.54
Primary kidney disease
Diabetes 968 (35.3) 173 (44.7) <0.01
Chronic glomerulonephritis 938 (34.3) 121 (31.3) 0.24
Hypertension 476 (17.4) 44 (11.4) <0.01
History of UGIB 162 (5.9) 64 (16.5) <0.01
Cardiovascular disease 324 (11.8) 56 (14.5) 0.14
eGFR (ml/min/1.73 m2) 27 ±21 21 ±16 <0.01
BMI (kg/m2) 24.2 ±4.1 24.1 ±3.9 0.51
Hemoglobin (g/dl) 10.7 ±2.4 10.1 ±2.3 <0.01
BUN (mg/dl) 48 ±31 54 ±31 <0.01
Creatinine (mg/dl) 3.7 ±2.8 4.3 ±2.9 <0.01
Calcium (mg/dl) 9.1 ±0.7 9.1 ±0.8 0.77
Phosphorus (mg/dl) 4.5 ±1.4 4.6 ±1.2 0.26
Albumin (g/dl) 3.5 ±0.6 3.3 ±0.6 <0.01
Medications n(%)
NSAIDs 50 (1.8) 11 (2.8) 0.18
Aspirin 305 (11.1) 46 (11.9) 0.66
Clopidogrel 73 (2.9) 11 (3.1) 0.80
Warfarin 52 (1.9) 12 (3.1) 0.12
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate
using CKD-EPI formula, BMI: body mass index, BUN: blood urea nitrogen, NSAIDs:
non-steroidal anti-inflammatory drugs
Page 19 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Table 3. Adjusted hazard ratio of confounders for all-cause mortality
aHR 95% CI P
UGIB 1.21 1.05 1.38 0.01
eGFR (every 5 ml/min/1.73m2 higher) 1.00 0.99 1.02 0.67
Age (every 10 additional years) 1.57 1.37 1.81 <0.01
Male 1.23 0.90 1.70 0.19
Diabetes 1.01 0.74 1.38 0.95
Cardiovascular disease 1.02 0.66 1.55 0.94
Hemoglobin (every 1 g/dl higher) 0.90 0.83 0.97 0.01
Albumin (every 1 g/dl higher) 0.51 0.40 0.64 <0.01
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate
Page 20 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Table 4. Subdistribution hazard ratio (SHR) of risk factors for chronic dialysis in
univariable and multivariable competing-risks regression with time-varying covariates
Risk factors Univariable Multivariable
SHR 95% CI aSHR 95% CI
UGIB 2.51 (2.17-2.90)* 1.51 (1.24-1.83)*
eGFR (every 5 ml/min/1.73m2 higher) 0.74 (0.71–0.76)* 0.81 (0.77–0.85)*
Age (every 10 additional years) 0.95 (0.91–1.21) 0.92 (0.86–0.98)*
Male 0.78 (0.69–0.89)* 1.09 (0.92–1.28)
History of UGIB 1.36 (1.08–1.71)* 0.93 (0.71–1.22)
Diabetes 1.66 (1.46–1.89)* 1.29 (1.10–1.51)*
Hemoglobin (every 1 g/dl higher) 0.78 (0.76–0.81)* 0.94 (0.90–0.98)*
BUN (every 10 mg/dl higher) 1.19 (1.17–1.22)* 1.02 (0.99–1.06)
Albumin (every 1 g/dl higher) 0.53 (0.48–0.59)* 0.75 (0.66–0.86)*
NSAIDs 0.83 (0.49–1.38) 0.73 (0.38–1.40)
Aspirin 1.03 (0.84–1.26) 1.15 (0.91–1.45)
Clopidogrel 1.33 (0.94-1.88) 1.15 (0.76-1.73)
Warfarin 1.09 (0.69–1.74) 1.13 (0.63–2.04)
SHR: subdistribution hazard ratio, CI: confidence interval, aSHR: adjusted
subdistribution hazard ratio, UGIB: upper gastrointestinal bleeding, eGFR: estimated
glomerular filtration rate, BMI: body mass index, BUN: blood urea nitrogen, NSAIDs:
non-steroidal anti-inflammatory drugs
* p < 0.05
Page 21 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Figure 1
127x104mm (150 x 150 DPI)
Page 22 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Figure 2
187x82mm (150 x 150 DPI)
Page 23 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
1
STROBE Statement Checklist of items that should be included in reports of observational studies
Section/Topic Item
No Recommendation
Reported
on Page No
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 3
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4
Objectives 3 State specific objectives, including any prespecified hypotheses 4
Methods
Study design 4 Present key elements of study design early in the paper 6
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection
6
Participants 6
(a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of
follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the
rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable 7
Data sources/measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of
assessment methods if there is more than one group 7
Bias 9 Describe any efforts to address potential sources of bias 13
Study size 10 Explain how the study size was arrived at NA
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why NA
Statistical methods 12
(a) Describe all statistical methods, including those used to control for confounding 8
(b) Describe any methods used to examine subgroups and interactions 8
(c) Explain how missing data were addressed 8
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
7
(e) Describe any sensitivity analyses NA
Page 24 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from
For peer review only
2
Section/Topic Item
No Recommendation
Reported
on Page No
Results
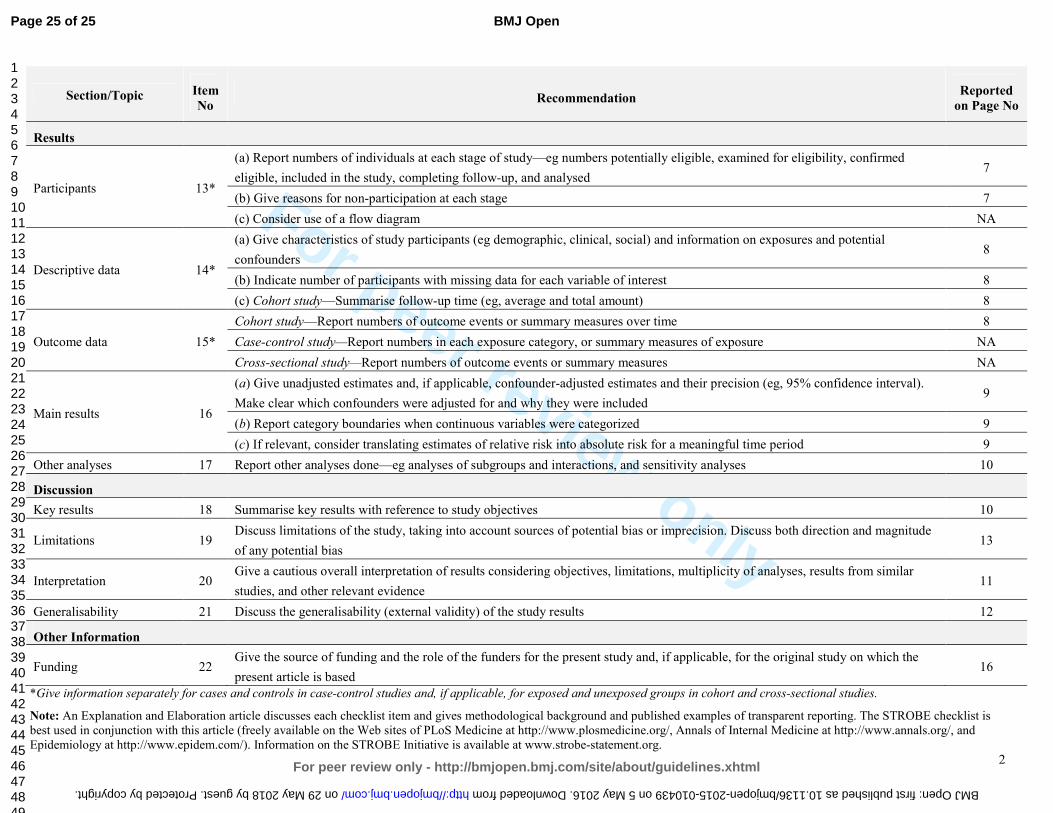
Participants 13*
(a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed
eligible, included in the study, completing follow-up, and analysed 7
(b) Give reasons for non-participation at each stage 7
(c) Consider use of a flow diagram NA
Descriptive data 14*
(a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders 8
(b) Indicate number of participants with missing data for each variable of interest 8
(c) Cohort study—Summarise follow-up time (eg, average and total amount) 8
Outcome data 15*
Cohort study—Report numbers of outcome events or summary measures over time 8
Case-control study—Report numbers in each exposure category, or summary measures of exposure NA
Cross-sectional study—Report numbers of outcome events or summary measures NA
Main results 16
(a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval).
Make clear which confounders were adjusted for and why they were included 9
(b) Report category boundaries when continuous variables were categorized 9
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period 9
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 10
Discussion
Key results 18 Summarise key results with reference to study objectives 10
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude
of any potential bias 13
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar
studies, and other relevant evidence 11
Generalisability 21 Discuss the generalisability (external validity) of the study results 12
Other Information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the
present article is based 16
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is
best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and
Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 25 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from

For peer review only
Upper gastrointestinal bleeding increases risk of dialysis and all-cause mortality in patients with chronic kidney
disease
Journal: BMJ Open
Manuscript ID bmjopen-2015-010439.R1
Article Type: Research
Date Submitted by the Author: 28-Jan-2016
Complete List of Authors: Liang, Chih-Chia; China Medical University Hospital, Division of Nephrology Chou, Che-Yi; China Medical University Hospital, Division of Nephrology Chang, Chiz-Tzung; China Medical University Hosptial, Division of
Nephrology Wang, I-Kuan; China Medical University Hospital, Division of Nephrology Huang, Chiu-Ching; China Medical University Hospital, Department of Internal Medicine
<b>Primary Subject Heading</b>:
Gastroenterology and hepatology
Secondary Subject Heading: Renal medicine
Keywords: chronic kidney disease, Dialysis < NEPHROLOGY, mortality, upper gastrointestinal bleeding
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 29 M
ay 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010439 on 5 May 2016. D
ownloaded from

For peer review only
Upper gastrointestinal bleeding increases risk of dialysis and
all-cause mortality in patients with chronic kidney disease
Chih-Chia Liang MD1,2,3,4, Che-Yi Chou PhD1,2,4, Chiz-Tzung Chang PhD1,2, I-Kuan
Wang MD1,2, Chiu-Ching Huang MD1,2,3
1Kidney Institute and Division of Nephrology, Department of Internal Medicine, China
Medical University Hospital, Taichung 404, Taiwan
2College of Medicine, China Medical University, Taichung 404, Taiwan
3Graduate Program of Translational Medicine, China Medical University, Taichung
404, Taiwan
4Chih-Chia Liang and Che-Yi Chou equally contribute to this work
Correspondence: Chiu-Ching Huang MD
Address of corresponding author: Kidney Institute and Division of Nephrology,
Department of Internal Medicine, China Medical University Hospital, No. 2, Yu-der
Road, North District, Taichung 40447, Taiwan
Tel: +886-4-22052121-3483, Fax: +886-4-22058883, E-mail: [email protected]
Running title: upper gastrointestinal bleeding and risk of chronic dialysis
Word count: Abstract: 258; Text: 2131
Page 1 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Abstract
Objective
Impaired renal function is associated with higher risk of upper gastrointestinal
bleeding (UGIB) in patients with chronic kidney disease and not on dialysis
(CKD-ND). It is unclear if UGIB increases risk for chronic dialysis. The aim of the
study was to investigate risk of chronic dialysis in CKD-ND patients with UGIB.
Setting
All CKD-ND stages 3-5 patients of a CKD program in one hospital between 2003 and
2009 were enrolled and prospectively followed until Sep 2012
Primary and secondary outcome measures
Chronic dialysis (dialysis more than 3 months) started and all-cause mortality. The
risk of chronic dialysis was analyzed using Cox proportional hazard regression with
adjustments for age, gender, and renal function, followed by competing-risks analysis.
Results
We analyzed 3126 CKD-ND patients with a mean age of 65 ± 14 years in 2.8 years.
Of 3126 patients, 387 (12.4%) patients developed UGIB, 989 (31.6%) patients started
chronic dialysis, and 197 (6.3%) patients died. UGIB increased all-cause mortality
[adjusted Hazard Ratio (aHR): 1.47, 95% confidence interval (CI): 1.04- 2.07, p <
0.01] and the risk of chronic dialysis (aHR; 1.30, 95% CI; 1.12-1.51, p < 0.01). The
Page 2 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
sub-distribution hazard ratio (SHR) of UGIB for chronic dialysis (competing event:
all-cause mortality) was 1.37 (95% CI, 1.15-1.64, p < 0.01) in competing-risks
analysis with adjustments for age, renal function, gender, diabetes, hemoglobin,
albumin, and urine protein/creatinine ratio.
Conclusions
UGIB is associated with increased risk of chronic dialysis and all-cause mortality in
patients with CKD-ND stages 3-5. This association is independent age, gender, basal
renal function, hemoglobin, albumin, and urine protein levels.
Keywords
chronic kidney disease, chronic dialysis, mortality, gastrointestinal bleeding,
Strengths and limitations of this study
� Upper gastrointestinal bleeding not only increases all-cause mortality but also
increases the risk of chronic dialysis in patients with chronic kidney disease.
� This association is showed in a cohort of CKD patients with adjustments for
confounders.
� The generalizability of this finding may be limited by one hospital and single
ethnic group.
Page 3 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Introduction
Upper gastrointestinal bleeding (UGIB) is a common gastrointestinal disorder in
patients with chronic kidney disease and not receiving dialysis (CKD-ND) [1,2]. In
CKD-ND patients, the risk of UGIB is negatively associated with their renal function
at baseline [1]. UGIB not only increases the risk of hospitalization but also increases
in-hospital mortality in CKD-ND patients and CKD 5 patients on dialysis [3]. The
increased all-cause mortality associated with UGIB is usually explained by the
worsen comorbid conditions caused by the UGIB[3-5].
Dialysis may be needed in patients with CKD-ND when UGIB leads to decreased
intravascular volume and the subsequent pre-renal acute kidney injury [6].
Furthermore, UGIB episodes may be the last straw for progression of CKD and may
lead to chronic dialysis if CKD-ND patients do not recover from acute kidney injury.
However, the long-term effect of UGIB on the risk of chronic dialysis in patients with
CKD-ND is not clear. The aim of the study was to investigate the risk of chronic
dialysis after UGIB in patients with CKD-ND.
Materials and Methods
Patient enrollment
Internal review board approval (DMR 99-IRB-301) was obtained for the review of
medical records, and the need for informed consent was waived. All patients in the
Page 4 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
outpatient-based CKD program of China Medical University Hospital (CMUH) from
June 2003 to December 2009 were included. The CKD program included patients
with CKD-ND stages 3-5 diagnosed by nephrologists and no exclusion criteria were
applied. The CKD program supported by National Health Insurance Taiwan include
clinical endocrinologists, nephrologists, CKD nurses, dietitians, and social workers.
The purpose of the CKD program is to monitor the progression of CKD patients;
laboratory measurements and CKD education are performed at least four times a year.
All patients were followed to the date of the date of initiation of chronic dialysis
including hemodialysis and peritoneal dialysis, loss to follow-up; death; or until
September 2012. There were two patients received kidney transplant and these two
patients were excluded in the analysis because the timing of kidney transplantation
was not related to uremic symptoms. As we aimed to investigate risk of chronic
dialysis, patients who received dialysis less than 3 months and patients who
discontinued dialysis because of a recovery of renal function were excluded.
Definition of predictors
UGIB was defined as melena, hematemesis, or the presence of red blood in gastric
lavage fluid, together with observation of a bleeding lesion or a lesion likely to have
bled on endoscopy of the upper digestive tract[1]. Coronary artery disease (CAD) was
defined as a positive exercise test, angiographic findings of at least one stenosis of
Page 5 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
more than 50%, or positive findings on scintigraphy.[7] Diabetes mellitus was defined
as use of insulin, use of oral anti-diabetic medication, or a fasting plasma glucose
level of 126 mg/dl or more.[8] Hypertension was defined as taking antihypertensives
without regard to the actual measurement of blood pressure, or having a systolic blood
pressure reading greater than 140 mm Hg or a diastolic blood pressure reading greater
than 90 mm Hg.[9] Patients’ primary kidney disease including diabetes, chronic
glomerular nephritis (CGN), and hypertension was diagnosed by the primary care
physician and was recorded at enrollment.
Measurements of parameters
Each patient’s body mass index (BMI), blood urea nitrogen (BUN), and creatinine
were measured at enrollment. Serum calcium, phosphorus, albumin, urine
albumin/creatinine ratio (ACR), and urine protein/creatinine ratio (PCR) were
measured in 3 months after enrollment. Estimated glomerular filtration rate (eGFR)
was calculated using the MDRD Collaboration formula.[10] The formula for white or
other race was used because the patients were all Chinese. The time-varying analysis
used an average of three eGFR measurements. Medications associated with a higher
risk of UGIB, including steroids, non-steroidal anti-inflammatory drugs (NSAIDs),
aspirin, clopidogrel and warfarin, were recorded based on the review of medical
records.
Page 6 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Outcomes measurements
The CKD nurses recorded the outcomes (dialysis for more than 3 months or mortality)
and date of the outcomes in the computerized case-management system. The CKD
nurses also checked patients’ status in the computerized medical record system in
CMUH and contacted the patients who did not returned to the outpatient every 6
months. The percentage of patients who were lost to follow-up was 6% in the CKD
program. The outcomes were validated by a study nurse through a review of medical
records and the study nurse was blinded to the aim of the study, and other physicians
performed the analysis.
Statistical analysis
Data were reported as mean ± standard deviation, median (interquartile range), or
frequency (percentage) as appropriate. All continuous variables were tested using
skewedness and kurtosis test for their normality. Data were analyzed using Student’s t
test for parametric variables, Kolmogorov-Smirnov test for non-parametric variables,
or chi-square test for categorical variables. Factors with a p-value < 0.05 in
univariable Cox proportional hazard regression and risk factors of chronic dialysis in
the literature were considered as possible confounders. Possible confounders for
all-cause mortality and chronic dialysis were analyzed using multivariable Cox
Page 7 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
proportional hazard regression. An adjusted hazard ratio (aHR) and 95% confidence
interval (CI) of aHR in multivariable Cox regression with adjustments for age, gender,
and eGFR was calculated. We utilized competing-risks analysis [11] with adjustments
for confounders identified in Cox regression because the risk of chronic dialysis may
be overestimated if patients’ death was not taken into consideration [12,13]. An
adjusted sub-distribution HR (aSHR) and 95% CI of aSHR was calculated in
competing-risks analysis with adjustments for age, gender, eGFR, and confounders
for chronic dialysis. The primary outcome was defined as chronic dialysis and the
competing event was patient’s death in the competing-risks analysis. All analyses
were performed using Stata version 13 SE (StataCorp, TX, USA) and a p-value < 0.05
was considered statistically significant.
Results
Patient characteristics
We identified 3126 patients with CKD-ND stages 3–5 including 1691 males and 1435
female, aged 65±14 years (Table 1). Diabetes and chronic glomerulonephritis (CGN)
were the major forms of primary kidney disease. The basal eGFR of the patients was
21 (11-37) ml/min/1.73m2 and the urine PCR was 1.4 (0.5-3.6) g/g at enrollment.
Page 8 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Outcomes and characteristics of patients with UGIB
The times of follow-up were similar in the patients with UGIB and the patients
without (p = 0.38). The proportion of the patients with UGIB who start chronic
dialysis was higher than that of the patients without UGIB (61.5% vs. 27.4%, p < 0.01,
chi-square test). Patients with UGIB were associated with a higher all-cause mortality
than patients without UGIB (11.6% vs. 5.6%, p < 0.01). Patients with UGIB were
older than patients without UGIB (p < 0.01) were. The proportion of diabetes as the
primary kidney disease and the proportion of hypertension as the primary kidney
disease were higher in patients with UGIB. The proportion of patients with CAD was
not different among the patients with UGIB and the patients without UGIB. The
patients with UGIB had a lower eGFR, a lower hemoglobin, a higher BUN, a higher
creatinine, and a lower serum albumin than the patients without UGIB did. There
were no differences in serum calcium and phosphate levels in the patients with UGIB
and the patients without. The proportion of patients who took steroid, patients who
took NSAIDs, patients who took aspirin, patients who took clopidogrel, and patients
who took warfarin were not different among the patients with UGIB and those
without.
UGIB increases all-cause mortality
Page 9 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
UGIB was independently associated with higher all-cause mortality (Table 2) with an
aHR of 1.47 (95% CI: 1.04-2.07, p < 0.01). Serum albumin was independently
associated with all-cause mortality (p < 0.01) and the aHR was 0.52 (95% CI:
0.42-0.66) per 1 g/dl. Diabetes, CAD, hemoglobin, and PCR was not associated with
all-cause mortality. Use of steroid, NSAIDs, clopidogrel, and warfarin was not
associated all-cause mortality.
UGIB increased risk of chronic dialysis
UGIB was associated with an increased risk for chronic dialysis with an aHR of 1.30
(95% CI: 1.12-1.51, p < 0.01) in multivariable Cox regression with adjustments for
age, gender and eGFR. Diabetes was independently associated with increased risk of
chronic dialysis with an HR of 1.50 (95% CI: 1.31-1.72). Hemoglobin and serum
albumin were associated with lower risk of chronic dialysis. PCR was associated with
increased risk of chronic dialysis with an HR of 1.03 (95% CI: 1.02-1.05) per 1g/g.
Steroids, NSAIDs, clopidogrel, and warfarin were not associated with the risk of
chronic dialysis. The aSHR of UGIB for chronic dialysis was 1.37 (95% CI: 1.15-1.64,
p < 0.01) in competing-risks analysis with adjustments for age, gender, eGFR,
diabetes, hemoglobin, albumin, and PCR. The cumulative incidence of chronic
dialysis in patients with UGIB and those without is showed in Figure 1.
Page 10 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Discussion
In this cohort study of patients with CKD-ND stages 3-5, UGIB was associated with
higher risk of chronic dialysis using Cox proportional hazard regression adjustments
for age, sex, eGFR. The association of UGIB and increased risk of chronic dialysis was
further validated using competing-risks analysis with adjustments for age, gender,
eGFR, diabetes, hemoglobin, albumin, PCR and all-cause mortality was considered as
a competing endpoint. The competing-risks analysis was critical to this study because
UGIB was associated with increased all-cause mortality. UGIB can be a complication
of uremia because of the uremic coagulopathy. In this study, UGIB patients started
chronic dialysis after a median of 1.2 (interquartile range: 0.7-1.3) years. Uremic
coagulopathy associated UGIB may not be one of the uremic symptoms that required
dialysis in these patients. In summary of our previous studies [1,14,15] and this study
(Figure 2), patients with CKD-ND were more at risk for developing UGIB and UGIB
may further accelerate the progression of CKD to chronic dialysis. The common
aggravating factors of CKD and UGIB are anemia, diabetes, and hypoalbuminemia.
On the other hand, higher GFR and uses of angiotensionogen converting enzyme
inhibitor (ACEi) or angiotensin II receptor blocker (ARB) may protect from UGIB in
this scenario. Some beneficial effects of ACEi and ARB may come from their
association with decreased risk of UGIB [15].
Page 11 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Most of CKD patients died from CAD during the course of CKD progression and
only some of the CKD patients started chronic dialysis [16-18]. In our study, the
proportion of patients who started chronic dialysis was higher than that of patients
who died. This was not only observed in our previous studies [1,19] but also in other
cohort of CKD patients in Taiwan [20]. The high prevalence of chronic dialysis in
Taiwan may be explained by an ethnic difference [21] or the effectiveness of
multidisciplinary care for CKD in Taiwan [20].
Diabetes was associated with the risk of chronic dialysis because diabetes is a
well-known confounder of dialysis. NSAIDs were also well-known risk factors for
UGIB and chronic dialysis [22], but we did not find a significant association of
NSAIDs and chronic dialysis. Aspirin, clopidogrel, warfarin were not associated with
the risk of chronic dialysis in patients with CAD either. Steroids treatment was
relatively common in patients with CKD [23] and 3% of patients took steroids in this
study. Steroids treatment was not associated with the risk of chronic dialysis in this
study. A limited number of patients who took these medications in this study may
explain this result. In addition, nausea/vomiting can be uremic symptoms [24] and are
indications of dialysis. Nausea/vomiting are common in patients with UGIB [25].
Page 12 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Although some CKD patients initiated dialysis because of UGIB-related
nausea/vomiting rather than uremic symptoms, the percentages of patients with
nausea/vomiting at the initiation of dialysis were similar among patients with UGIB
and those without. In addition, we excluded patients who underwent dialysis less than
3 months and discontinued dialysis because of a recovery of renal function.
UGIB-related nausea/vomiting did not explain the association of UGIB and chronic
dialysis in this study.
The limitations of this study were its observational study design and the inclusion of
all patients in single hospital in Taiwan. This may limit the generalizability of our
finding to other ethnic groups. More studies of various ethnic groups and multiple
institutions are required to confirm our results. Patients of a CKD program were
analyzed in this study and therefore patient selection bias cannot be avoided. We also
recorded proton-pump inhibitor treatment for UGIB but did not find any beneficial
effect of proton-pump inhibitor in decreasing risk of chronic dialysis and all-cause
mortality. In spite of the limitations, this the first study that showed an association of
UGIB and chronic dialysis, independent of all confounders of chronic dialysis. This
suggests that UGIB not only leads to acute kidney injury but also results in long-term
consequence of irreversible kidney injury in this population.
Page 13 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Conclusions
Upper gastrointestinal bleeding is associated with increased risk of chronic dialysis in
patients with chronic kidney disease stages 3-5 and not receiving dialysis. This
association is independent of age, gender, basal renal function, diabetes, hemoglobin,
albumin, and urine protein levels. More studies will be warranted to investigate if
prevention of UGIB may slow the progression of CKD and delay the need of dialysis
in patients with CND-ND.
Acknowledgments
This study was supported in part by Taiwan Ministry of Health and Welfare Clinical
Trial and Research Center of Excellence (MOHW104-TDU-B-212-113002) and
China Medical University Hospital (DMR-101-019 & DMR-102-015). The funders
had no role in study design, data collection and analysis, decision to publish, or
preparation of the manuscript.
Contribution of Authors
Study concept, design, and acquisition of data: CC Liang; analysis, interpretation of
data, and drafting of the manuscript: CY Chou; critical revision of the manuscript for
important intellectual content: CT Chang, IK Wang; study supervision: CC Huang
Page 14 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Conflict of interest statement
The results presented in this paper have not been published previously in whole or
part. The authors have no conflicts of interest regarding the design or publication of
this study.
Data sharing statement
No additional data available.
Page 15 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
References
1. Liang CC, Wang SM, Kuo HL, et al. Upper gastrointestinal bleeding in patients with
CKD. Clin J Am Soc Nephrol 2014;9(8):1354-9.
2. Yang JY, Lee TC, Montez-Rath ME, et al. Trends in acute nonvariceal upper
gastrointestinal bleeding in dialysis patients. J Am Soc Nephrol
2012;23(3):495-506.
3. Sood P, Kumar G, Nanchal R, et al. Chronic kidney disease and end-stage renal
disease predict higher risk of mortality in patients with primary upper
gastrointestinal bleeding. Am J Nephrol 2012;35(3):216-24.
4. Åhsberg K, Höglund P, Staël von Holstein C. Mortality from peptic ulcer bleeding:
the impact of comorbidity and the use of drugs that promote bleeding. Alimentary
pharmacology & therapeutics 2010;32(6):801-10.
5. Leontiadis GI, Molloy-Bland M, Moayyedi P, et al. Effect of comorbidity on
mortality in patients with peptic ulcer bleeding: systematic review and meta-analysis.
Am J Gastroenterol 2013;108(3):331-45; quiz 46.
6. Moreau R, Lebrec D. Acute renal failure in patients with cirrhosis: perspectives in
the age of MELD. Hepatology 2003;37(2):233-43.
7. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of
macrovascular events in patients with type 2 diabetes in the PROactive Study
(PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised
controlled trial. Lancet 2005;366(9493):1279-89.
8. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes
mellitus and impaired glucose tolerance. Arch Intern Med 2005;165(8):863-7.
9. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for
hypertension: population study. BMJ 2000;320(7233):479-82.
10. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate
glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Annals of internal medicine
1999;130(6):461-70.
11. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a
competing risk. J Am Stat Assoc 1999;94(446):496-509.
12. Evans DW, Ryckelynck JP, Fabre E, et al. Peritonitis-free survival in peritoneal
dialysis: an update taking competing risks into account. Nephrology, dialysis,
transplantation : official publication of the European Dialysis and Transplant
Association - European Renal Association 2010;25(7):2315-22.
13. Bechade C, Guittet L, Evans D, et al. Early failure in patients starting peritoneal
dialysis: a competing risks approach. Nephrology, dialysis, transplantation : official
publication of the European Dialysis and Transplant Association - European Renal
Page 16 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Association 2014;29(11):2127-35.
14. Liang CC, Muo CH, Wang IK, et al. Peptic ulcer disease risk in chronic kidney
disease: ten-year incidence, ulcer location, and ulcerogenic effect of medications.
PloS one 2014;9(2):e87952.
15. Chou CY, Wang SM, Chang PH, et al. Angiotensin II receptor blocker prevents
upper gastrointestinal bleeding in hypertensive patients with chronic kidney disease
not on dialysis. Int J Clin Pract 2015.
16. Winkelmayer WC, Levin R, Avorn J. Chronic kidney disease as a risk factor for
bleeding complications after coronary artery bypass surgery. Am J Kidney Dis
2003;41(1):84-9.
17. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death,
cardiovascular events, and hospitalization. N Engl J Med 2004;351(13):1296-305.
18. Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of
chronic kidney disease to kidney failure. JAMA 2011;305(15):1553-9.
19. Chen IR, Wang SM, Liang CC, et al. Association of walking with survival and RRT
among patients with CKD stages 3-5. Clin J Am Soc Nephrol 2014;9(7):1183-9.
20. Wang SM, Hsiao LC, Ting IW, et al. Multidisciplinary care in patients with chronic
kidney disease: A systematic review and meta-analysis. European journal of internal
medicine 2015;26(8):640-5.
21. Xu R, Zhang L, Zhang P, et al. Comparison of the prevalence of chronic kidney
disease among different ethnicities: Beijing CKD survey and American NHANES.
Nephrology, dialysis, transplantation : official publication of the European Dialysis
and Transplant Association - European Renal Association 2009;24(4):1220-6.
22. Plantinga L, Grubbs V, Sarkar U, et al. Nonsteroidal anti-inflammatory drug use
among persons with chronic kidney disease in the United States. Ann Fam Med
2011;9(5):423-30.
23. Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D,
PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the
study to evaluate early kidney disease. Kidney Int 2007;71(1):31-8.
24. Murtagh FE, Addington-Hall JM, Edmonds PM, et al. Symptoms in advanced renal
disease: a cross-sectional survey of symptom prevalence in stage 5 chronic kidney
disease managed without dialysis. J Palliat Med 2007;10(6):1266-76.
25. Roderick PJ, Wilkes HC, Meade TW. The gastrointestinal toxicity of aspirin: an
overview of randomised controlled trials. Br J Clin Pharmacol 1993;35(3):219-26.
Page 17 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Legends
Figure 1. Cumulative incidence of chronic dialysis in patients with and without upper
gastrointestinal bleeding (UGIB) using competing-risks regression with adjustments
for age, gender, renal function, diabetes, hemoglobin, albumin, and urine
protein/creatinine ratio. The primary event was chronic dialysis and the competing
event was all-cause mortality.
Figure 2. Upper gastrointestinal bleeding (UGIB) may accelerate the progression of
chronic kidney disease (CKD) and further increase the risk of chronic dialysis. In this
interactive scheme of UGIB and CKD, aggravating factors include anemia, diabetes,
and hypoalbuminemia, and protective factors contain a higher glomerular filtration
rate (GFR) and uses of angiotensionogen converting enzyme inhibitor (ACEi)/
angiotensin II receptor blocker (ARB).
Page 18 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
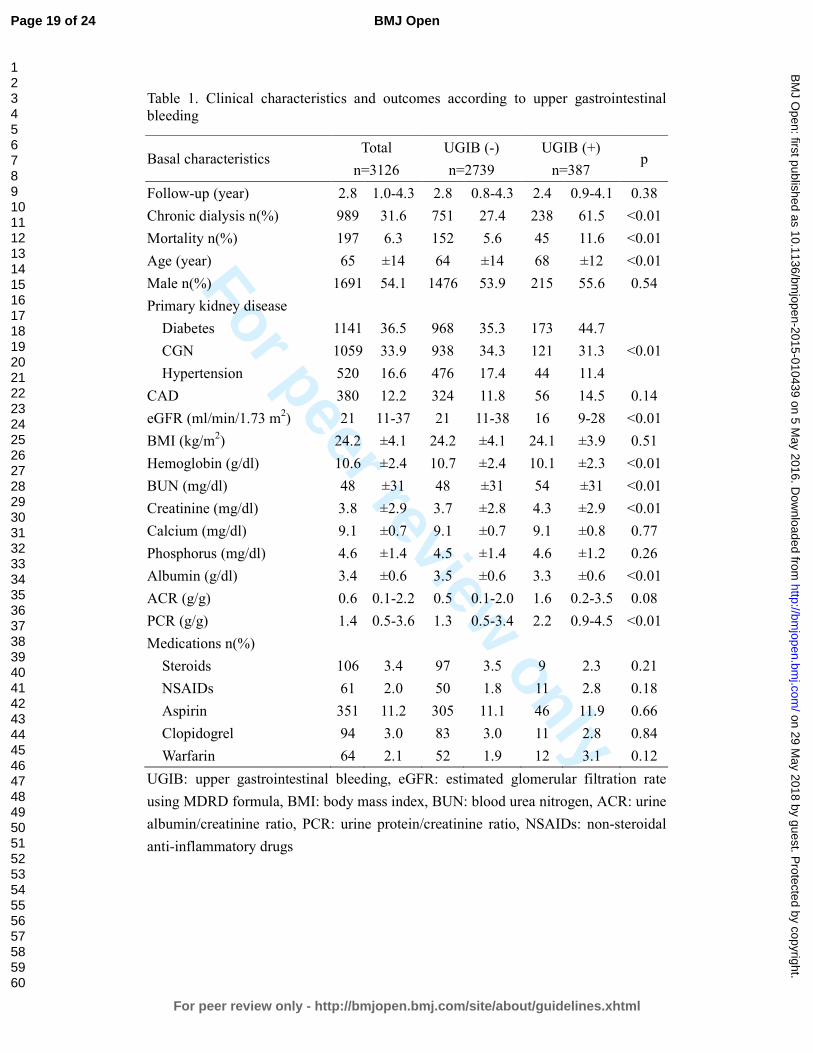
For peer review only
Table 1. Clinical characteristics and outcomes according to upper gastrointestinal bleeding
Basal characteristics Total
n=3126
UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.8 1.0-4.3 2.8 0.8-4.3 2.4 0.9-4.1 0.38
Chronic dialysis n(%) 989 31.6 751 27.4 238 61.5 <0.01
Mortality n(%) 197 6.3 152 5.6 45 11.6 <0.01
Age (year) 65 ±14 64 ±14 68 ±12 <0.01
Male n(%) 1691 54.1 1476 53.9 215 55.6 0.54
Primary kidney disease
Diabetes 1141 36.5 968 35.3 173 44.7
<0.01 CGN 1059 33.9 938 34.3 121 31.3
Hypertension 520 16.6 476 17.4 44 11.4
CAD 380 12.2 324 11.8 56 14.5 0.14
eGFR (ml/min/1.73 m2) 21 11-37 21 11-38 16 9-28 <0.01
BMI (kg/m2) 24.2 ±4.1 24.2 ±4.1 24.1 ±3.9 0.51
Hemoglobin (g/dl) 10.6 ±2.4 10.7 ±2.4 10.1 ±2.3 <0.01
BUN (mg/dl) 48 ±31 48 ±31 54 ±31 <0.01
Creatinine (mg/dl) 3.8 ±2.9 3.7 ±2.8 4.3 ±2.9 <0.01
Calcium (mg/dl) 9.1 ±0.7 9.1 ±0.7 9.1 ±0.8 0.77
Phosphorus (mg/dl) 4.6 ±1.4 4.5 ±1.4 4.6 ±1.2 0.26
Albumin (g/dl) 3.4 ±0.6 3.5 ±0.6 3.3 ±0.6 <0.01
ACR (g/g) 0.6 0.1-2.2 0.5 0.1-2.0 1.6 0.2-3.5 0.08
PCR (g/g) 1.4 0.5-3.6 1.3 0.5-3.4 2.2 0.9-4.5 <0.01
Medications n(%)
Steroids 106 3.4 97 3.5 9 2.3 0.21
NSAIDs 61 2.0 50 1.8 11 2.8 0.18
Aspirin 351 11.2 305 11.1 46 11.9 0.66
Clopidogrel 94 3.0 83 3.0 11 2.8 0.84
Warfarin 64 2.1 52 1.9 12 3.1 0.12
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate
using MDRD formula, BMI: body mass index, BUN: blood urea nitrogen, ACR: urine
albumin/creatinine ratio, PCR: urine protein/creatinine ratio, NSAIDs: non-steroidal
anti-inflammatory drugs
Page 19 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
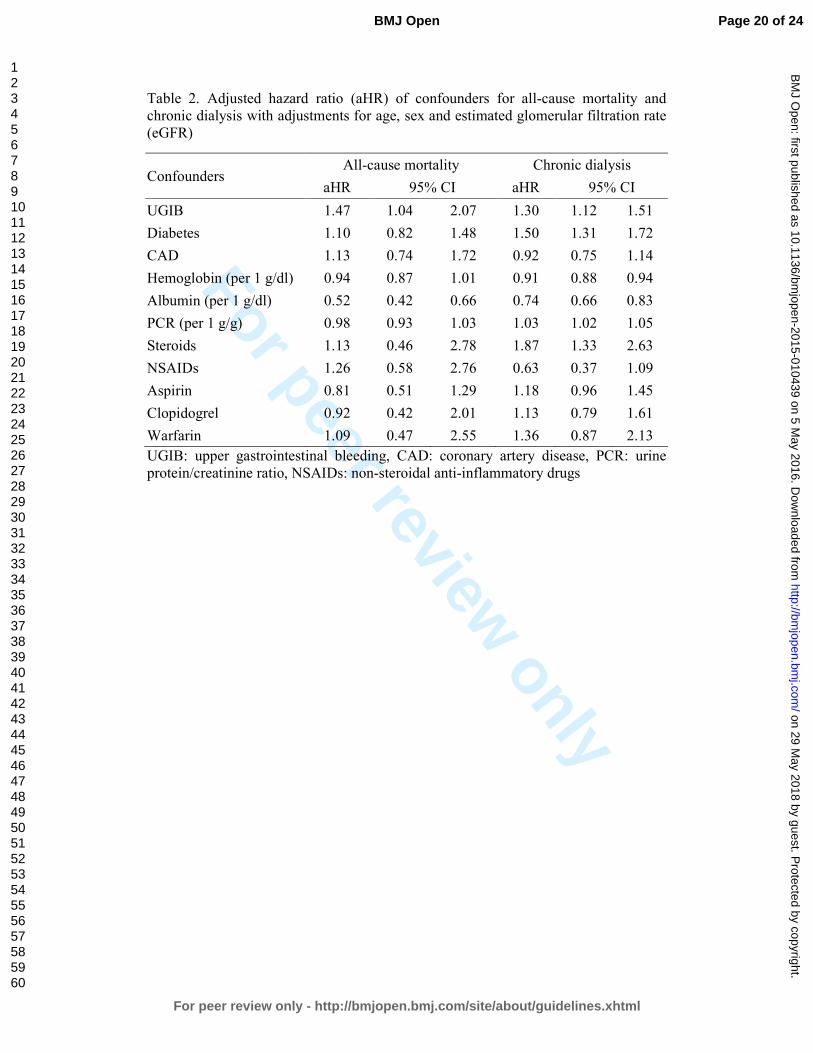
For peer review only
Table 2. Adjusted hazard ratio (aHR) of confounders for all-cause mortality and chronic dialysis with adjustments for age, sex and estimated glomerular filtration rate (eGFR)
Confounders All-cause mortality Chronic dialysis
aHR 95% CI aHR 95% CI
UGIB 1.47 1.04 2.07 1.30 1.12 1.51
Diabetes 1.10 0.82 1.48 1.50 1.31 1.72
CAD 1.13 0.74 1.72 0.92 0.75 1.14
Hemoglobin (per 1 g/dl) 0.94 0.87 1.01 0.91 0.88 0.94
Albumin (per 1 g/dl) 0.52 0.42 0.66 0.74 0.66 0.83
PCR (per 1 g/g) 0.98 0.93 1.03 1.03 1.02 1.05
Steroids 1.13 0.46 2.78 1.87 1.33 2.63
NSAIDs 1.26 0.58 2.76 0.63 0.37 1.09
Aspirin 0.81 0.51 1.29 1.18 0.96 1.45
Clopidogrel 0.92 0.42 2.01 1.13 0.79 1.61
Warfarin 1.09 0.47 2.55 1.36 0.87 2.13
UGIB: upper gastrointestinal bleeding, CAD: coronary artery disease, PCR: urine protein/creatinine ratio, NSAIDs: non-steroidal anti-inflammatory drugs
Page 20 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Figure 1
73x54mm (300 x 300 DPI)
Page 21 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Figure 2
187x82mm (150 x 150 DPI)
Page 22 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
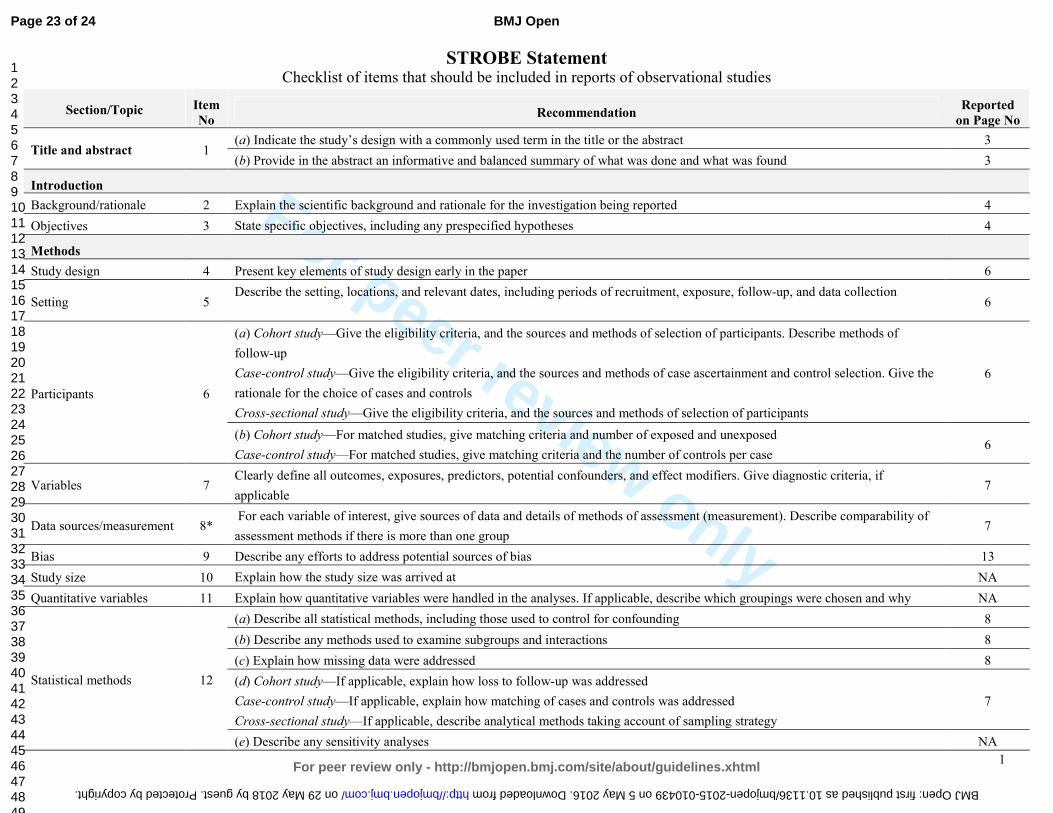
For peer review only
1
STROBE Statement Checklist of items that should be included in reports of observational studies
Section/Topic Item
No Recommendation
Reported
on Page No
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 3
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4
Objectives 3 State specific objectives, including any prespecified hypotheses 4
Methods
Study design 4 Present key elements of study design early in the paper 6
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection
6
Participants 6
(a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of
follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the
rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable 7
Data sources/measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of
assessment methods if there is more than one group 7
Bias 9 Describe any efforts to address potential sources of bias 13
Study size 10 Explain how the study size was arrived at NA
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why NA
Statistical methods 12
(a) Describe all statistical methods, including those used to control for confounding 8
(b) Describe any methods used to examine subgroups and interactions 8
(c) Explain how missing data were addressed 8
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
7
(e) Describe any sensitivity analyses NA
Page 23 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from
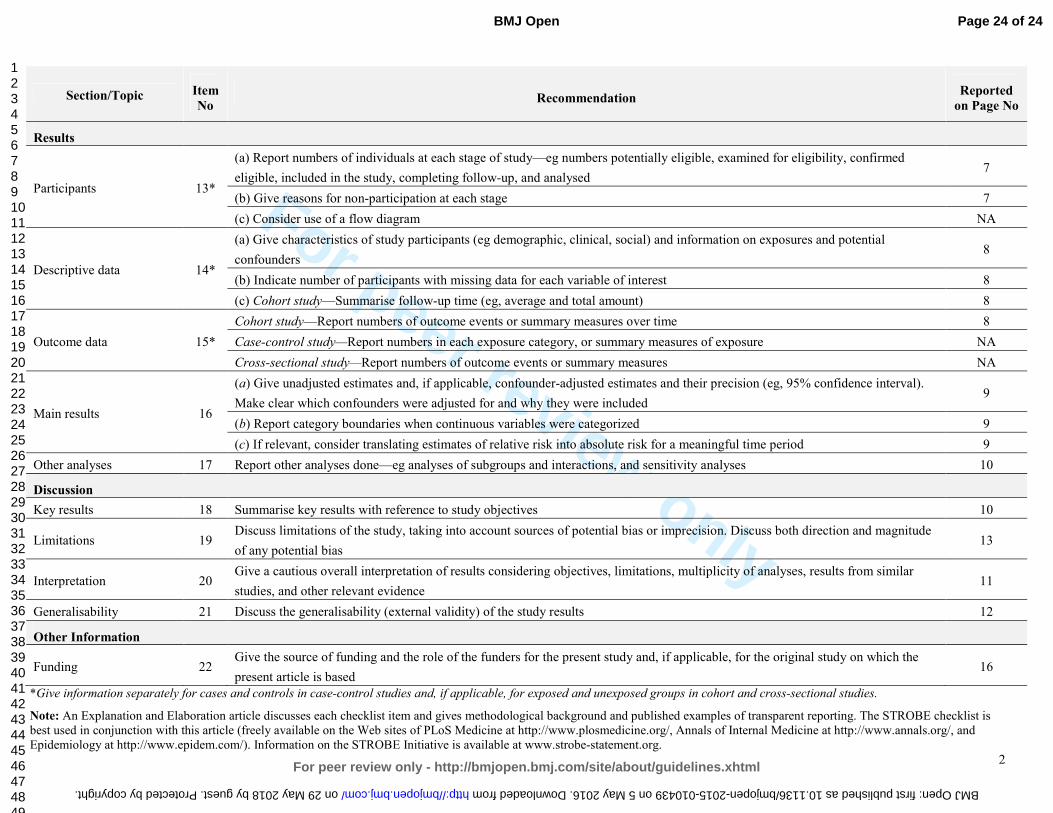
For peer review only
2
Section/Topic Item
No Recommendation
Reported
on Page No
Results
Participants 13*
(a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed
eligible, included in the study, completing follow-up, and analysed 7
(b) Give reasons for non-participation at each stage 7
(c) Consider use of a flow diagram NA
Descriptive data 14*
(a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders 8
(b) Indicate number of participants with missing data for each variable of interest 8
(c) Cohort study—Summarise follow-up time (eg, average and total amount) 8
Outcome data 15*
Cohort study—Report numbers of outcome events or summary measures over time 8
Case-control study—Report numbers in each exposure category, or summary measures of exposure NA
Cross-sectional study—Report numbers of outcome events or summary measures NA
Main results 16
(a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval).
Make clear which confounders were adjusted for and why they were included 9
(b) Report category boundaries when continuous variables were categorized 9
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period 9
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 10
Discussion
Key results 18 Summarise key results with reference to study objectives 10
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude
of any potential bias 13
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar
studies, and other relevant evidence 11
Generalisability 21 Discuss the generalisability (external validity) of the study results 12
Other Information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the
present article is based 16
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is
best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and
Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 24 of 24
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from
For peer review only
Upper gastrointestinal bleeding as a risk factor for dialysis and all-cause mortality: a cohort study of chronic kidney
disease patients in Taiwan
Journal: BMJ Open
Manuscript ID bmjopen-2015-010439.R2
Article Type: Research
Date Submitted by the Author: 28-Mar-2016
Complete List of Authors: Liang, Chih-Chia; China Medical University Hospital, Division of Nephrology Chou, Che-Yi; China Medical University Hospital, Division of Nephrology Chang, Chiz-Tzung; China Medical University Hosptial, Division of
Nephrology Wang, I-Kuan; China Medical University Hospital, Division of Nephrology Huang, Chiu-Ching; China Medical University Hospital, Department of Internal Medicine
<b>Primary Subject Heading</b>:
Renal medicine
Secondary Subject Heading: Renal medicine
Keywords: Chronic renal failure < NEPHROLOGY, Gastroduodenal disease < GASTROENTEROLOGY, Dialysis < NEPHROLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 29 M
ay 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010439 on 5 May 2016. D
ownloaded from
For peer review only
Upper gastrointestinal bleeding as a risk factor for dialysis and
all-cause mortality: a cohort study of chronic kidney disease patients
in Taiwan
Chih-Chia Liang MD1,2,3,4, Che-Yi Chou PhD1,2,4, Chiz-Tzung Chang PhD1,2, I-Kuan
Wang MD1,2, Chiu-Ching Huang MD1,2,3
1Kidney Institute and Division of Nephrology, Department of Internal Medicine, China
Medical University Hospital, Taichung 404, Taiwan
2College of Medicine, China Medical University, Taichung 404, Taiwan
3Graduate Program of Translational Medicine, China Medical University, Taichung
404, Taiwan
4Chih-Chia Liang and Che-Yi Chou equally contribute to this work
Correspondence: Chiu-Ching Huang MD
Address of corresponding author: Kidney Institute and Division of Nephrology,
Department of Internal Medicine, China Medical University Hospital, No. 2, Yu-der
Road, North District, Taichung 40447, Taiwan
Tel: +886-4-22052121-3483, Fax: +886-4-22058883, E-mail: [email protected]
Running title: upper gastrointestinal bleeding and risk of chronic dialysis
Word count: Abstract: 253; Text: 2131
Page 1 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Abstract
Objective
Impaired renal function is associated with higher risk of upper gastrointestinal
bleeding (UGIB) in patients with chronic kidney disease and not on dialysis
(CKD-ND). It is unclear if UGIB increases risk of chronic dialysis. The aim of the
study was to investigate risk of chronic dialysis in CKD-ND patients with UGIB.
Setting
All CKD-ND stages 3-5 patients of a CKD program in one hospital between 2003 and
2009 were enrolled and prospectively followed until Sep 2012.
Primary and secondary outcome measures
Chronic dialysis (dialysis more than 3 months) started and all-cause mortality. The
risk of chronic dialysis was analyzed using Cox proportional hazard regression with
adjustments for age, gender, and renal function, followed by competing-risks analysis.
Results
We analyzed 3126 CKD-ND patients with a mean age of 65 ± 14 years in 2.8 years.
Of 3126 patients, 387 (12.4%) patients developed UGIB, 989 (31.6%) patients started
chronic dialysis, and 197 (6.3%) patients died. UGIB increased all-cause mortality
[adjusted Hazard Ratio (aHR): 1.51, 95% confidence interval (CI): 1.07- 2.13] and the
risk of chronic dialysis (aHR; 1.29, 95% CI; 1.11 - 1.50). The sub-distribution hazard
Page 2 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
ratio (SHR) of UGIB for chronic dialysis (competing event: all-cause mortality) was
1.37 (95% CI, 1.15-1.64) in competing-risks analysis with adjustments for age, renal
function, gender, diabetes, hemoglobin, albumin, and urine protein/creatinine ratio.
Conclusions
UGIB is associated with increased risk of chronic dialysis and all-cause mortality in
patients with CKD-ND stages 3-5. This association is independent of age, gender,
basal renal function, hemoglobin, albumin, and urine protein levels.
Keywords
chronic kidney disease, chronic dialysis, mortality, gastrointestinal bleeding,
Strengths and limitations of this study
� Upper gastrointestinal bleeding not only increases all-cause mortality but also
increases the risk of chronic dialysis in patients with chronic kidney disease.
� This association is shown in a cohort of CKD patients with adjustments for
confounders.
� The generalizability of this finding may be limited by one hospital and a single
ethnic group.
Page 3 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Introduction
Upper gastrointestinal bleeding (UGIB) is a common gastrointestinal disorder in
patients with chronic kidney disease and not receiving dialysis (CKD-ND) 1 2. In
CKD-ND patients, the risk of UGIB is negatively associated with their renal function
at baseline 1. UGIB not only increases the risk of hospitalization but also increases
in-hospital mortality in CKD-ND patients and CKD 5 patients on dialysis 3. The
increased all-cause mortality associated with UGIB is usually explained by the
worsen comorbid conditions caused by the UGIB3-5.
Dialysis may be needed in patients with CKD-ND when UGIB leads to decreased
intravascular volume and the subsequent pre-renal acute kidney injury 6. Furthermore,
UGIB episodes may be the last straw for progression of CKD and may lead to chronic
dialysis if CKD-ND patients do not recover from acute kidney injury. However, the
long-term effect of UGIB on the risk of chronic dialysis in patients with CKD-ND is
not clear. The aim of the study was to investigate the risk of chronic dialysis after
UGIB in patients with CKD-ND.
Materials and Methods
Patient enrollment
All patients in the outpatient-based CKD program of China Medical University
Hospital (CMUH) from June 2003 to December 2009 were included. The CKD
Page 4 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
program included patients with CKD-ND stages 3-5 diagnosed by nephrologists and
no exclusion criteria were applied. The CKD program supported by National Health
Insurance Taiwan includes clinical endocrinologists, nephrologists, CKD nurses,
dietitians, and social workers. The purpose of the CKD program is to monitor the
progression of CKD patients. Laboratory measurements and CKD education are
performed at least four times a year. All patients were followed to the date of initiation
of chronic dialysis including hemodialysis and peritoneal dialysis, loss to follow-up,
death, or until September 2012. There were two patients who received kidney
transplant and these two patients were excluded in the analysis because the timing of
kidney transplantation was not related to uremic symptoms. As we aimed to
investigate risk of chronic dialysis, patients who received dialysis less than 3 months
and patients who discontinued dialysis because of a recovery of renal function were
excluded.
Definition and measurements
UGIB was defined as melena, hematemesis, or the presence of red blood in gastric
lavage fluid, together with observation of a bleeding lesion or a lesion likely to have
bled on endoscopy of the upper digestive tract1. Coronary artery disease (CAD) was
defined as a positive exercise test, angiographic findings of at least one stenosis of
more than 50%, or positive findings on scintigraphy.7 Diabetes mellitus was defined
Page 5 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
as use of insulin, use of oral anti-diabetic medication, or a fasting plasma glucose
level of 126 mg/dl or more.8 Hypertension was defined as taking antihypertensives
without regard to the actual measurement of blood pressure, or having a systolic blood
pressure reading greater than 140 mm Hg or a diastolic blood pressure reading greater
than 90 mm Hg.9 Patients’ primary kidney disease including diabetes, chronic
glomerular nephritis (CGN), and hypertension was diagnosed by the primary care
physician and was recorded at enrollment.
Each patient’s body mass index (BMI), blood urea nitrogen (BUN), and creatinine
were measured at enrollment. Serum calcium, phosphorus, albumin, urine
albumin/creatinine ratio (ACR), and urine protein/creatinine ratio (PCR) were
measured in 3 months after enrollment. Estimated glomerular filtration rate (eGFR)
was calculated using the MDRD Collaboration formula.10 The formula for white or
other race was used because the patients were all Chinese. The time-varying analysis
used an average of three eGFR measurements. Medications associated with a higher
risk of UGIB, including steroids, non-steroidal anti-inflammatory drugs (NSAIDs),
aspirin, clopidogrel and warfarin, were recorded based on the review of medical
records.
Outcomes measurements
The CKD nurses recorded the outcomes (dialysis for more than 3 months or mortality)
Page 6 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
and date of the outcomes in the computerized case-management system. The CKD
nurses also checked patients’ status in the computerized medical record system in
CMUH and contacted patients who did not return to the outpatient every 6 months.
The percentage of patients who were lost to follow-up was 6% in the CKD program.
The outcomes were validated by a study nurse through a review of medical records
and the study nurse was blinded to the aim of the study, and other physicians
performed the analysis.
Statistical analysis
Data were reported as mean ± standard deviation, median (interquartile range), or
frequency (percentage) as appropriate. All continuous variables were tested using
skewedness and kurtosis test for their normality. Data were analyzed using Student’s t
test for parametric variables, Kolmogorov-Smirnov test for non-parametric variables,
or chi-square test for categorical variables. Factors with a p-value < 0.05 in
univariable Cox proportional hazard regression and risk factors of chronic dialysis in
the literature were considered as possible confounders. Possible confounders for
all-cause mortality and chronic dialysis were analyzed using multivariable Cox
proportional hazard regression. An adjusted hazard ratio (aHR) and 95% confidence
intervals (CI) of aHR in multivariable Cox regression with adjustments for age,
Page 7 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
gender, and eGFR were calculated. We utilized competing-risks analysis 11 with
adjustments for confounders identified in Cox regression because the risk of chronic
dialysis may be overestimated if patients’ death was not taken into consideration 12 13.
An adjusted sub-distribution HR (aSHR) and 95% CI of aSHR were calculated in
competing-risks analysis with adjustments for age, gender, eGFR, and confounders
for chronic dialysis. The primary outcome was defined as chronic dialysis and the
competing event was patient’s death in the competing-risks analysis. All analyses
were performed using Stata version 13 SE (StataCorp, TX, USA) and a p-value < 0.05
was considered statistically significant.
Ethical considerations
Internal review board approval (DMR 99-IRB-301) was obtained for the review of
medical records, and the need for informed consent was waived.
Results
Patient characteristics
We identified 3126 patients with CKD-ND stages 3–5 including 1691 males and 1435
female, aged 65±14 years (Table 1). Diabetes and chronic glomerulonephritis (CGN)
were the major forms of primary kidney disease. The basal eGFR of the patients was
21 (11-37) ml/min/1.73m2 and the urine PCR was 1.4 (0.5 - 3.6) g/g at enrollment.
Patients with UGIB were older and more often had diabetes, a lower eGFR, a lower
Page 8 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
hemoglobin, a higher BUN, a higher creatinine, and a lower serum albumin. They,
however, had similar use of steroid, NSAIDs, aspirin, clopidogrel, and warfarin.
There were no differences in serum calcium and phosphate levels in the patients with
UGIB and the patients without.
Mortality and risk of chronic dialysis in patients with upper gastrointestinal
bleeding
The times of follow-up were similar in the patients with UGIB and the patients
without (p = 0.38, Table 2). The proportion of the patients with UGIB who start
chronic dialysis was higher than that of the patients without UGIB (61.5% vs. 27.4%,
p < 0.01). Patients with UGIB were associated with a higher all-cause mortality than
patients without UGIB (11.6% vs. 5.6%, p < 0.01).
UGIB increases all-cause mortality
UGIB was independently associated with higher all-cause mortality (Table 3) with an
aHR of 1.51 (95% CI: 1.07 - 2.13, p = 0.02). Patients’ age, eGFR, and serum albumin
were independently associated with all-cause mortality. The aHR was 1.05 for every
one additional year (95% CI: 1.04 – 1.07, p < 0.01), 0.99 for every ml/min/1.73m2 of
eGFR (95% CI: 0.0.98-1.00, p < 0.01), and 0.52 per g/dl of serum albumin (95% CI:
Page 9 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
0.42 – 0.65, p < 0.01). Diabetes, CAD, hemoglobin, and PCR were not associated
with all-cause mortality. Use of steroid, NSAIDs, clopidogrel, and warfarin were not
associated all-cause mortality, either.
UGIB increases risk of chronic dialysis
UGIB was associated with an increased risk of chronic dialysis with an aHR of 1.29
(95% CI: 1.11-1.50, p < 0.01). Diabetes was independently associated with increased
risk of chronic dialysis with an HR of 1.49 (95% CI: 1.30 - 1.72, p < 0.01).
Hemoglobin and serum albumin were associated with lower risk of chronic dialysis.
PCR was associated with increased risk of chronic dialysis with an HR of 1.29 (95%
CI: 1.11-1.50) per 1g/g. Steroids, NSAIDs, clopidogrel, and warfarin were not
associated with the risk of chronic dialysis. The aSHR of UGIB for chronic dialysis
was 1.37 (95% CI: 1.15-1.64, p < 0.01) in competing-risks analysis with adjustments
for age, gender, eGFR, diabetes, hemoglobin, albumin, and PCR. The cumulative
incidence of chronic dialysis in patients with UGIB and those without is shown in
Figure 1.
Discussion
In this cohort of patients with CKD-ND stages 3-5, UGIB was associated with higher
Page 10 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
risk of chronic dialysis. The association of UGIB and risk of chronic dialysis were
further validated using competing-risks analysis. The competing-risks analysis was
critical to this study because UGIB was associated with increased all-cause mortality.
UGIB can be a complication of uremia because of the uremic coagulopathy. In this
study, UGIB patients started chronic dialysis after a median of 1.2 (interquartile range:
0.7-1.3) years. Uremic coagulopathy associated UGIB therefore may not be one of the
uremic symptoms that required dialysis in these patients. In summary of our previous
studies 1 14 15 and this study (Figure 2), patients with CKD-ND were more at risk for
developing UGIB and UGIB may further accelerate the progression of CKD to
chronic dialysis. The common aggravating factors of CKD and UGIB are anemia16,
diabetes, and hypoalbuminemia1. In addition, higher GFR and uses of
angiotensinogen converting enzyme inhibitor (ACEi) or angiotensin II receptor
blocker (ARB) may protect UGIB in this scenario 15. Some beneficial effects of ACEi
and ARB may come from their association with decreased risk of UGIB 15.
Most of CKD patients died from CAD during the course of CKD progression and
only some of the CKD patients started chronic dialysis 17-19. In our study, the
proportion of patients who started chronic dialysis was higher than that of patients
who died. This was not only observed in our previous studies 1 20 but also in other
Page 11 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
cohort of CKD patients in Taiwan 21. The high prevalence of chronic dialysis in
Taiwan may be explained by an ethnic difference 22 or the effectiveness of
multidisciplinary care for CKD in Taiwan 21.
Diabetes was associated with the risk of chronic dialysis because diabetes is a
well-known confounder of dialysis. NSAIDs were also well-known risk factors for
UGIB and chronic dialysis 23, but we did not find any significant association of
NSAIDs and chronic dialysis. Aspirin, clopidogrel, warfarin were not associated with
the risk of chronic dialysis in patients with CAD, either. Steroids treatment was
relatively common in patients with CKD 24 but only 3% of patients took steroids in
this study. Steroids treatment was not associated with the risk of chronic dialysis in
this study. A limited number of patients who took these medications in this study may
explain this result. In addition, nausea and vomiting can be uremic symptoms 25 and
are indications of dialysis. Nausea and vomiting are common in patients with UGIB 26.
Although some CKD patients initiated dialysis because of UGIB-related nausea and
vomiting rather than uremic symptoms, the percentages of patients with nausea and
vomiting at the initiation of dialysis were similar among patients with UGIB and
those without. In addition, we excluded patients who underwent dialysis less than 3
months and discontinued dialysis because of a recovery of renal function.
Page 12 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
UGIB-related nausea/vomiting did not explain the association of UGIB and chronic
dialysis in this study.
The limitations of this study were its observational study design and the inclusion of
all patients in single hospital in Taiwan. This may limit the generalizability of our
finding to other ethnic groups. More studies of various ethnic groups and multiple
institutions are required to confirm our results. Patients of a CKD program were
analyzed in this study and therefore patient selection bias cannot be avoided. We also
recorded proton-pump inhibitor treatment for UGIB but did not find any beneficial
effect of proton-pump inhibitor in decreasing risk of chronic dialysis and all-cause
mortality. In spite of the limitations, this is the first study that shows an association of
UGIB and chronic dialysis, independent of all confounders of chronic dialysis. This
suggests that UGIB not only leads to acute kidney injury but also results in long-term
consequence of irreversible kidney injury in this population.
Conclusions
Upper gastrointestinal bleeding is associated with increased risk of chronic dialysis in
patients with chronic kidney disease stages 3-5 and not receiving dialysis. This
association is independent of age, gender, basal renal function, diabetes, hemoglobin,
albumin, and urine protein levels. More studies will be warranted to investigate if
Page 13 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
prevention of UGIB may slow the progression of CKD and delay the need of dialysis
in patients with CND-ND.
Acknowledgments
This study was supported in part by This study is supported in part by Taiwan
Ministry of Health and Welfare Clinical Trial and Research Center of Excellence
(MOHW105-TDU-B-212-133019) and China Medical University Hospital
(DMR-101-019 & DMR-102-015). The funders had no role in study design, data
collection and analysis, decision to publish, or preparation of the manuscript.
Contribution of Authors
Study concept, design, and acquisition of data: CC Liang; analysis, interpretation of
data, and drafting of the manuscript: CY Chou; critical revision of the manuscript for
important intellectual content: CT Chang, IK Wang; study supervision: CC Huang
Conflict of interest statement
The results presented in this paper have not been published previously in whole or
part. The authors have no conflicts of interest regarding the design or publication of
this study.
Data sharing statement
Page 14 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
None
Page 15 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
References
1. Liang CC, Wang SM, Kuo HL, et al. Upper gastrointestinal bleeding in patients with
CKD. Clin J Am Soc Nephrol 2014;9(8):1354-9.
2. Yang JY, Lee TC, Montez-Rath ME, et al. Trends in acute nonvariceal upper
gastrointestinal bleeding in dialysis patients. J Am Soc Nephrol
2012;23(3):495-506.
3. Sood P, Kumar G, Nanchal R, et al. Chronic kidney disease and end-stage renal
disease predict higher risk of mortality in patients with primary upper
gastrointestinal bleeding. Am J Nephrol 2012;35(3):216-24.
4. Åhsberg K, Höglund P, Staël von Holstein C. Mortality from peptic ulcer bleeding:
the impact of comorbidity and the use of drugs that promote bleeding. Alimentary
pharmacology & therapeutics 2010;32(6):801-10.
5. Leontiadis GI, Molloy-Bland M, Moayyedi P, et al. Effect of comorbidity on
mortality in patients with peptic ulcer bleeding: systematic review and meta-analysis.
Am J Gastroenterol 2013;108(3):331-45; quiz 46.
6. Moreau R, Lebrec D. Acute renal failure in patients with cirrhosis: perspectives in
the age of MELD. Hepatology 2003;37(2):233-43.
7. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of
macrovascular events in patients with type 2 diabetes in the PROactive Study
(PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised
controlled trial. Lancet 2005;366(9493):1279-89.
8. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes
mellitus and impaired glucose tolerance. Arch Intern Med 2005;165(8):863-7.
9. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for
hypertension: population study. BMJ 2000;320(7233):479-82.
10. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate
glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Annals of internal medicine
1999;130(6):461-70.
11. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a
competing risk. J Am Stat Assoc 1999;94(446):496-509.
12. Evans DW, Ryckelynck JP, Fabre E, et al. Peritonitis-free survival in peritoneal
dialysis: an update taking competing risks into account. Nephrology, dialysis,
transplantation : official publication of the European Dialysis and Transplant
Association - European Renal Association 2010;25(7):2315-22.
13. Bechade C, Guittet L, Evans D, et al. Early failure in patients starting peritoneal
dialysis: a competing risks approach. Nephrology, dialysis, transplantation : official
publication of the European Dialysis and Transplant Association - European Renal
Page 16 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Association 2014;29(11):2127-35.
14. Liang CC, Muo CH, Wang IK, et al. Peptic ulcer disease risk in chronic kidney
disease: ten-year incidence, ulcer location, and ulcerogenic effect of medications.
PloS one 2014;9(2):e87952.
15. Chou CY, Wang SM, Chang PH, et al. Angiotensin II receptor blocker prevents
upper gastrointestinal bleeding in hypertensive patients with chronic kidney disease
not on dialysis. Int J Clin Pract 2015.
16. Hsu TW, Liu JS, Hung SC, et al. Renoprotective effect of
renin-angiotensin-aldosterone system blockade in patients with predialysis
advanced chronic kidney disease, hypertension, and anemia. JAMA Intern Med
2014;174(3):347-54.
17. Winkelmayer WC, Levin R, Avorn J. Chronic kidney disease as a risk factor for
bleeding complications after coronary artery bypass surgery. Am J Kidney Dis
2003;41(1):84-9.
18. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death,
cardiovascular events, and hospitalization. N Engl J Med 2004;351(13):1296-305.
19. Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of
chronic kidney disease to kidney failure. JAMA 2011;305(15):1553-9.
20. Chen IR, Wang SM, Liang CC, et al. Association of walking with survival and RRT
among patients with CKD stages 3-5. Clin J Am Soc Nephrol 2014;9(7):1183-9.
21. Wang SM, Hsiao LC, Ting IW, et al. Multidisciplinary care in patients with chronic
kidney disease: A systematic review and meta-analysis. European journal of internal
medicine 2015;26(8):640-5.
22. Xu R, Zhang L, Zhang P, et al. Comparison of the prevalence of chronic kidney
disease among different ethnicities: Beijing CKD survey and American NHANES.
Nephrology, dialysis, transplantation : official publication of the European Dialysis
and Transplant Association - European Renal Association 2009;24(4):1220-6.
23. Plantinga L, Grubbs V, Sarkar U, et al. Nonsteroidal anti-inflammatory drug use
among persons with chronic kidney disease in the United States. Ann Fam Med
2011;9(5):423-30.
24. Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D,
PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the
study to evaluate early kidney disease. Kidney Int 2007;71(1):31-8.
25. Murtagh FE, Addington-Hall JM, Edmonds PM, et al. Symptoms in advanced renal
disease: a cross-sectional survey of symptom prevalence in stage 5 chronic kidney
disease managed without dialysis. J Palliat Med 2007;10(6):1266-76.
26. Roderick PJ, Wilkes HC, Meade TW. The gastrointestinal toxicity of aspirin: an
overview of randomised controlled trials. Br J Clin Pharmacol 1993;35(3):219-26.
Page 17 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Page 18 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Legends
Figure 1. Cumulative incidence of chronic dialysis in patients with and without upper
gastrointestinal bleeding (UGIB) using competing-risks regression with adjustments
for age, gender, renal function, diabetes, hemoglobin, albumin, and urine
protein/creatinine ratio. The primary event was chronic dialysis and the competing
event was all-cause mortality.
Figure 2. Upper gastrointestinal bleeding (UGIB) may accelerate the progression of
chronic kidney disease (CKD) and further increase the risk of chronic dialysis. In this
interactive scheme of UGIB and CKD, aggravating factors include anemia, diabetes,
and hypoalbuminemia, and protective factors contain a higher glomerular filtration
rate (GFR) and uses of angiotensionogen converting enzyme inhibitor (ACEi)/
angiotensin II receptor blocker (ARB).
Page 19 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Table 1. Clinical characteristics and outcomes according to upper gastrointestinal bleeding
Basal characteristics Total
n=3126
UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.8 1.0-4.3 2.8 0.8-4.3 2.4 0.9-4.1 0.38
Chronic dialysis n(%) 989 31.6 751 27.4 238 61.5 <0.01
Mortality n(%) 197 6.3 152 5.6 45 11.6 <0.01
Age (year) 65 ±14 64 ±14 68 ±12 <0.01
Male n(%) 1691 54.1 1476 53.9 215 55.6 0.54
Primary kidney disease
Diabetes 1141 36.5 968 35.3 173 44.7
<0.01 CGN 1059 33.9 938 34.3 121 31.3
Hypertension 520 16.6 476 17.4 44 11.4
CAD 380 12.2 324 11.8 56 14.5 0.14
eGFR (ml/min/1.73 m2) 21 11-37 21 11-38 16 9-28 <0.01
BMI (kg/m2) 24.2 ±4.1 24.2 ±4.1 24.1 ±3.9 0.51
Hemoglobin (g/dl) 10.6 ±2.4 10.7 ±2.4 10.1 ±2.3 <0.01
BUN (mg/dl) 48 ±31 48 ±31 54 ±31 <0.01
Creatinine (mg/dl) 3.8 ±2.9 3.7 ±2.8 4.3 ±2.9 <0.01
Calcium (mg/dl) 9.1 ±0.7 9.1 ±0.7 9.1 ±0.8 0.77
Phosphorus (mg/dl) 4.6 ±1.4 4.5 ±1.4 4.6 ±1.2 0.26
Albumin (g/dl) 3.4 ±0.6 3.5 ±0.6 3.3 ±0.6 <0.01
ACR (g/g) 0.6 0.1-2.2 0.5 0.1-2.0 1.6 0.2-3.5 0.08
PCR (g/g) 1.4 0.5-3.6 1.3 0.5-3.4 2.2 0.9-4.5 <0.01
Medications n(%)
Steroids 106 3.4 97 3.5 9 2.3 0.21
NSAIDs 61 2.0 50 1.8 11 2.8 0.18
Aspirin 351 11.2 305 11.1 46 11.9 0.66
Clopidogrel 94 3.0 83 3.0 11 2.8 0.84
Warfarin 64 2.1 52 1.9 12 3.1 0.12
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate
using MDRD formula, BMI: body mass index, BUN: blood urea nitrogen, ACR: urine
albumin/creatinine ratio, PCR: urine protein/creatinine ratio, NSAIDs: non-steroidal
anti-inflammatory drugs
Page 20 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
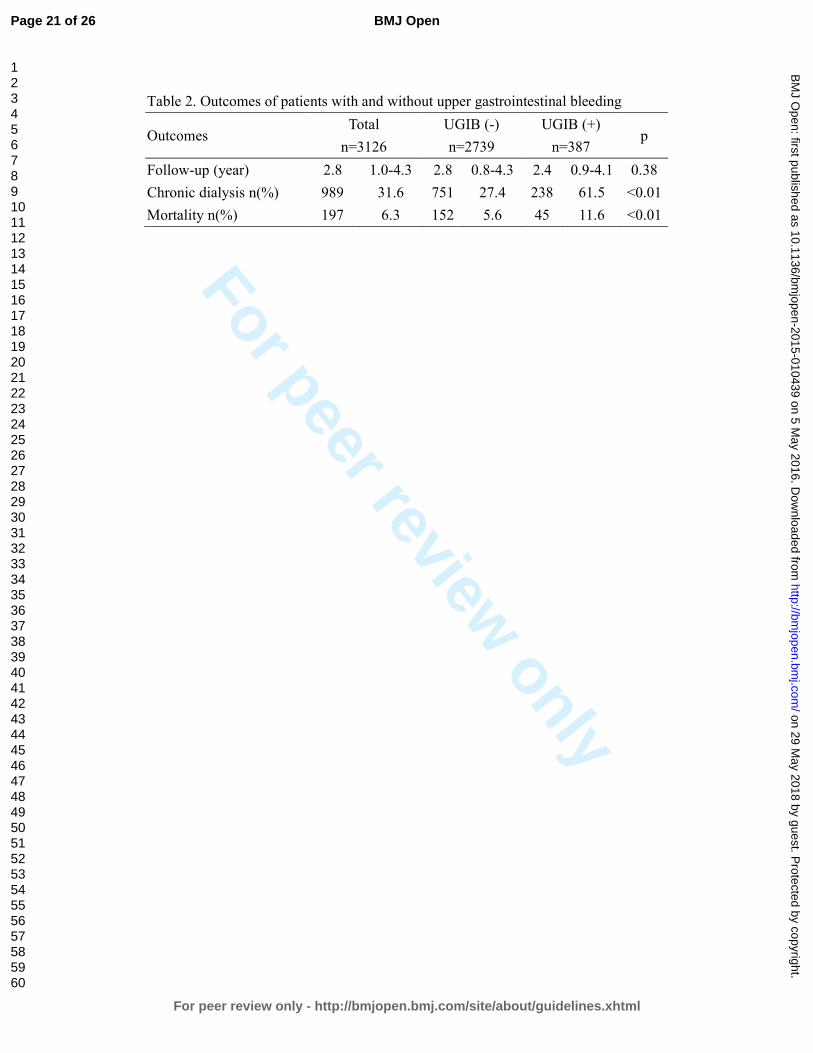
For peer review only
Table 2. Outcomes of patients with and without upper gastrointestinal bleeding
Outcomes Total
n=3126
UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.8 1.0-4.3 2.8 0.8-4.3 2.4 0.9-4.1 0.38
Chronic dialysis n(%) 989 31.6 751 27.4 238 61.5 <0.01
Mortality n(%) 197 6.3 152 5.6 45 11.6 <0.01
Page 21 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
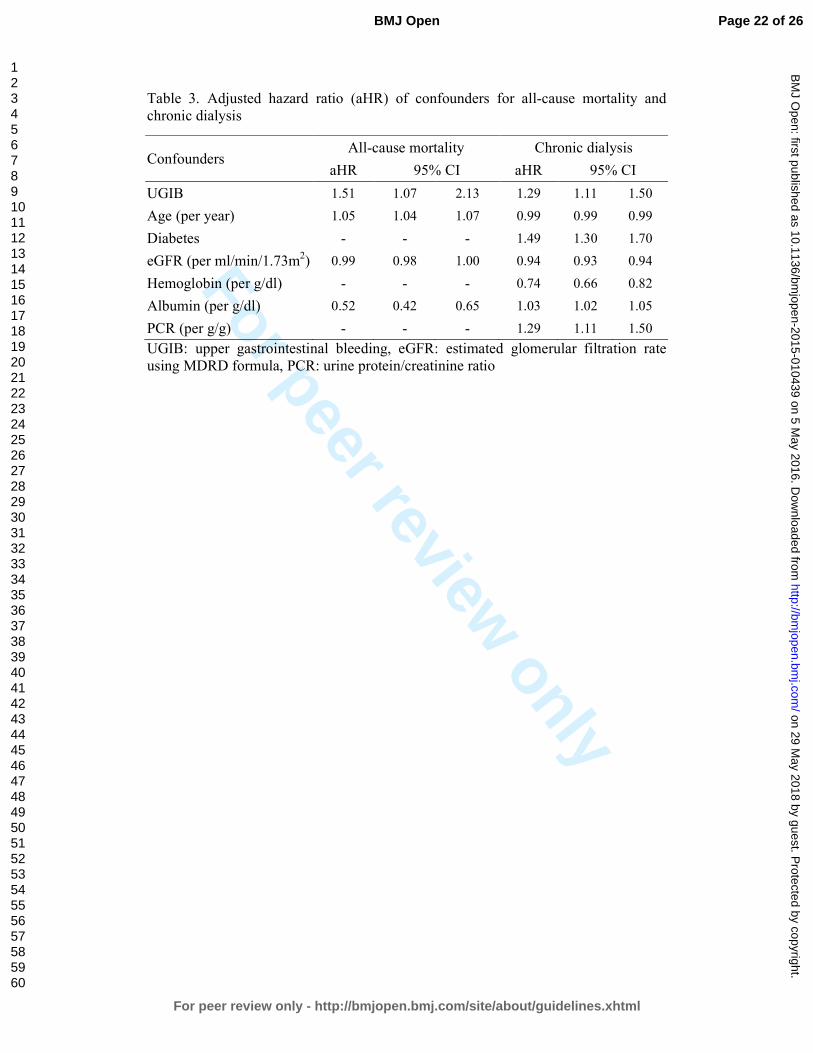
For peer review only
Table 3. Adjusted hazard ratio (aHR) of confounders for all-cause mortality and chronic dialysis
Confounders All-cause mortality Chronic dialysis
aHR 95% CI aHR 95% CI
UGIB 1.51 1.07 2.13 1.29 1.11 1.50
Age (per year) 1.05 1.04 1.07 0.99 0.99 0.99
Diabetes - - - 1.49 1.30 1.70
eGFR (per ml/min/1.73m2) 0.99 0.98 1.00 0.94 0.93 0.94
Hemoglobin (per g/dl) - - - 0.74 0.66 0.82
Albumin (per g/dl) 0.52 0.42 0.65 1.03 1.02 1.05
PCR (per g/g) - - - 1.29 1.11 1.50
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate using MDRD formula, PCR: urine protein/creatinine ratio
Page 22 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Figure 1
196x145mm (300 x 300 DPI)
Page 23 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
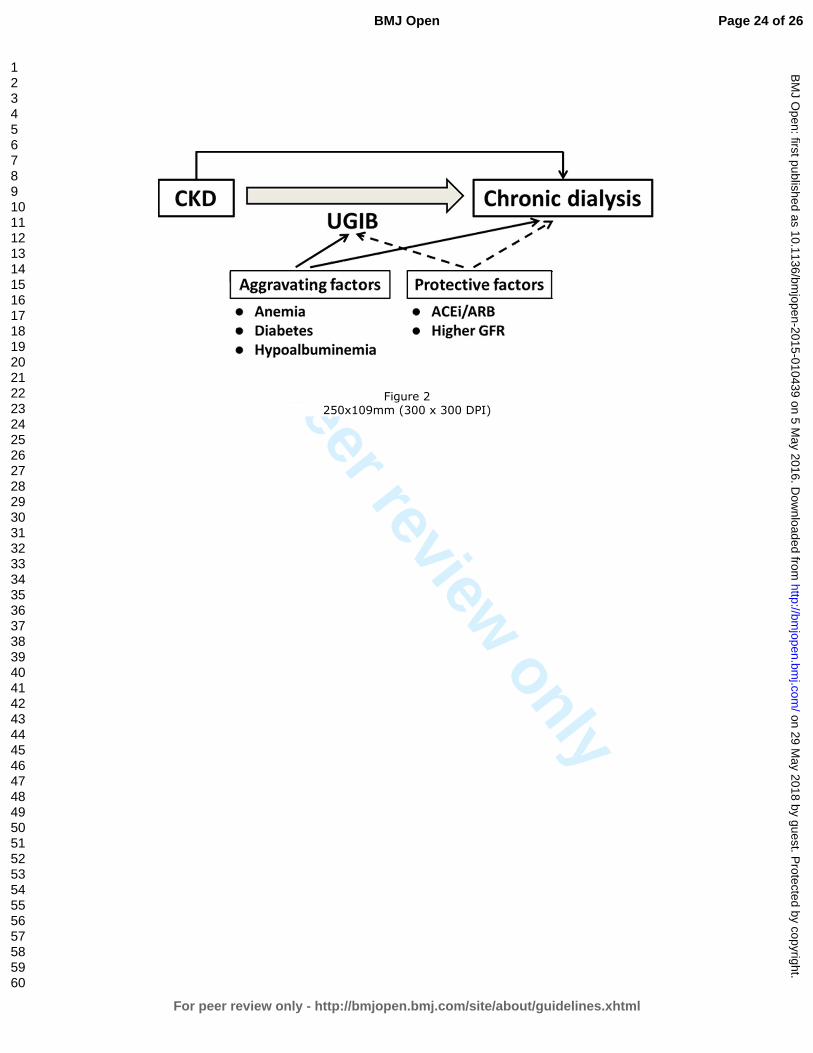
For peer review only
Figure 2
250x109mm (300 x 300 DPI)
Page 24 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
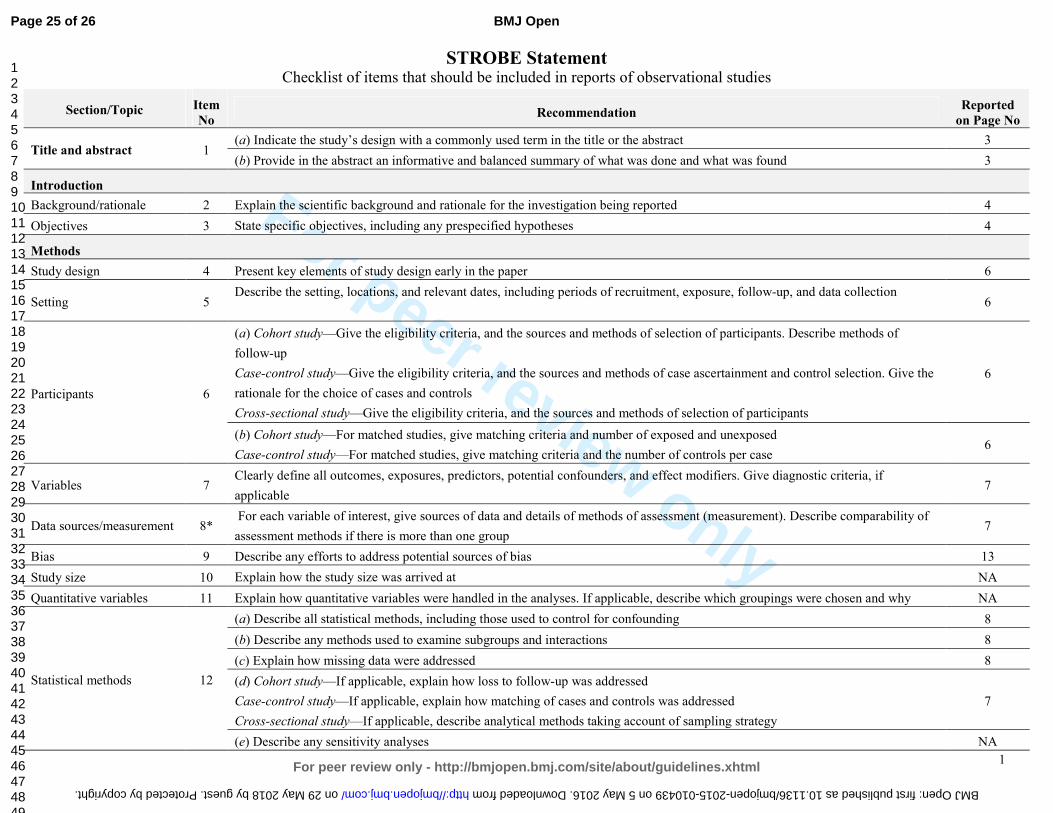
For peer review only
1
STROBE Statement Checklist of items that should be included in reports of observational studies
Section/Topic Item
No Recommendation
Reported
on Page No
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 3
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4
Objectives 3 State specific objectives, including any prespecified hypotheses 4
Methods
Study design 4 Present key elements of study design early in the paper 6
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection
6
Participants 6
(a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of
follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the
rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable 7
Data sources/measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of
assessment methods if there is more than one group 7
Bias 9 Describe any efforts to address potential sources of bias 13
Study size 10 Explain how the study size was arrived at NA
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why NA
Statistical methods 12
(a) Describe all statistical methods, including those used to control for confounding 8
(b) Describe any methods used to examine subgroups and interactions 8
(c) Explain how missing data were addressed 8
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
7
(e) Describe any sensitivity analyses NA
Page 25 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from
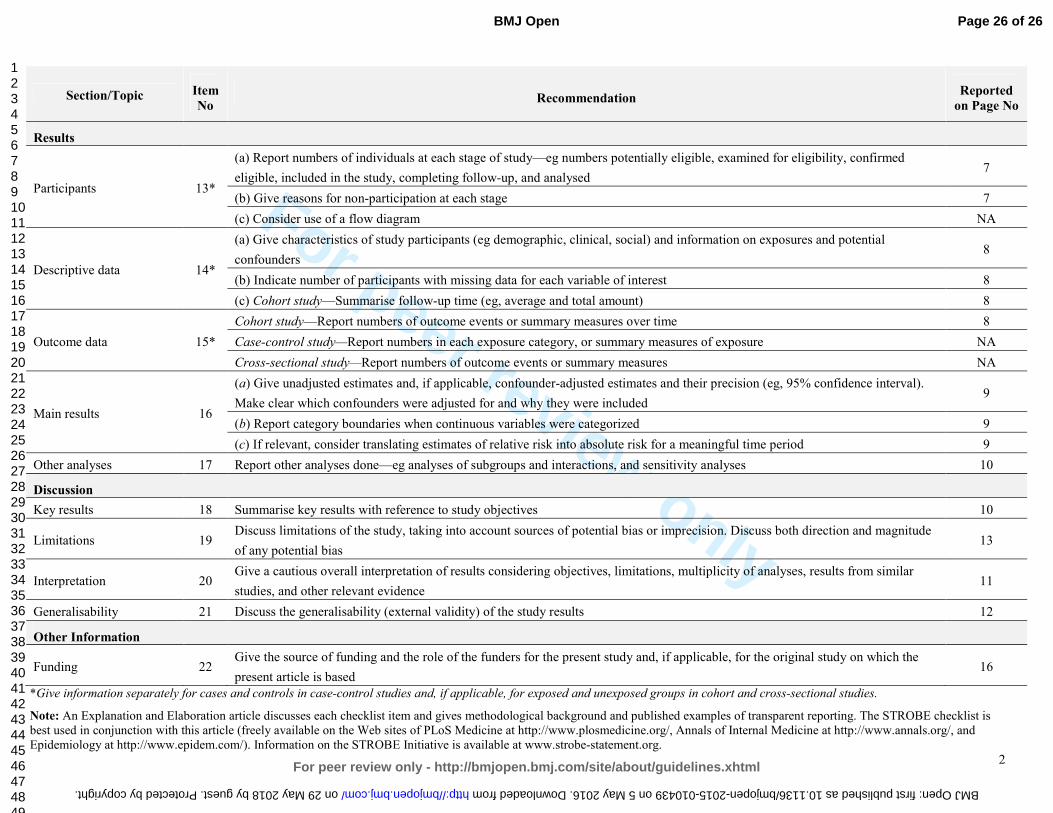
For peer review only
2
Section/Topic Item
No Recommendation
Reported
on Page No
Results
Participants 13*
(a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed
eligible, included in the study, completing follow-up, and analysed 7
(b) Give reasons for non-participation at each stage 7
(c) Consider use of a flow diagram NA
Descriptive data 14*
(a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders 8
(b) Indicate number of participants with missing data for each variable of interest 8
(c) Cohort study—Summarise follow-up time (eg, average and total amount) 8
Outcome data 15*
Cohort study—Report numbers of outcome events or summary measures over time 8
Case-control study—Report numbers in each exposure category, or summary measures of exposure NA
Cross-sectional study—Report numbers of outcome events or summary measures NA
Main results 16
(a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval).
Make clear which confounders were adjusted for and why they were included 9
(b) Report category boundaries when continuous variables were categorized 9
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period 9
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 10
Discussion
Key results 18 Summarise key results with reference to study objectives 10
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude
of any potential bias 13
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar
studies, and other relevant evidence 11
Generalisability 21 Discuss the generalisability (external validity) of the study results 12
Other Information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the
present article is based 16
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is
best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and
Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 26 of 26
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from

For peer review only
Upper gastrointestinal bleeding as a risk factor for dialysis and all-cause mortality: a cohort study of chronic kidney
disease patients in Taiwan
Journal: BMJ Open
Manuscript ID bmjopen-2015-010439.R3
Article Type: Research
Date Submitted by the Author: 13-Apr-2016
Complete List of Authors: Liang, Chih-Chia; China Medical University Hospital, Division of Nephrology Chou, Che-Yi; China Medical University Hospital, Division of Nephrology Chang, Chiz-Tzung; China Medical University Hosptial, Division of
Nephrology Wang, I-Kuan; China Medical University Hospital, Division of Nephrology Huang, Chiu-Ching; China Medical University Hospital, Department of Internal Medicine
<b>Primary Subject Heading</b>:
Renal medicine
Secondary Subject Heading: Renal medicine
Keywords: Chronic renal failure < NEPHROLOGY, Gastroduodenal disease < GASTROENTEROLOGY, Dialysis < NEPHROLOGY
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on 29 M
ay 2018 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-010439 on 5 May 2016. D
ownloaded from
For peer review only
Upper gastrointestinal bleeding as a risk factor for dialysis and
all-cause mortality: a cohort study of chronic kidney disease patients
in Taiwan
Chih-Chia Liang MD1,2,3,4, Che-Yi Chou PhD1,2,4, Chiz-Tzung Chang PhD1,2, I-Kuan
Wang MD1,2, Chiu-Ching Huang MD1,2,3
1Kidney Institute and Division of Nephrology, Department of Internal Medicine, China
Medical University Hospital, Taichung 404, Taiwan
2College of Medicine, China Medical University, Taichung 404, Taiwan
3Graduate Program of Translational Medicine, China Medical University, Taichung
404, Taiwan
4Chih-Chia Liang and Che-Yi Chou equally contribute to this work
Correspondence: Chiu-Ching Huang MD
Address of corresponding author: Kidney Institute and Division of Nephrology,
Department of Internal Medicine, China Medical University Hospital, No. 2, Yu-der
Road, North District, Taichung 40447, Taiwan
Tel: +886-4-22052121-3483, Fax: +886-4-22058883, E-mail: [email protected]
Running title: upper gastrointestinal bleeding and risk of chronic dialysis
Word count: Abstract: 253; Text: 2131
Page 1 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Abstract
Objective
Impaired renal function is associated with higher risk of upper gastrointestinal
bleeding (UGIB) in patients with chronic kidney disease and not on dialysis
(CKD-ND). It is unclear if UGIB increases risk of chronic dialysis. The aim of the
study was to investigate risk of chronic dialysis in CKD-ND patients with UGIB.
Setting
All CKD-ND stages 3-5 patients of a CKD program in one hospital between 2003 and
2009 were enrolled and prospectively followed until Sep 2012.
Primary and secondary outcome measures
Chronic dialysis (dialysis more than 3 months) started and all-cause mortality. The
risk of chronic dialysis was analyzed using Cox proportional hazard regression with
adjustments for age, gender, and renal function, followed by competing-risks analysis.
Results
We analyzed 3126 CKD-ND patients with a mean age of 65 ± 14 years in 2.8 years.
Of 3126 patients, 387 (12.4%) patients developed UGIB, 989 (31.6%) patients started
chronic dialysis, and 197 (6.3%) patients died. UGIB increased all-cause mortality
[adjusted Hazard Ratio (aHR): 1.51, 95% confidence interval (CI): 1.07- 2.13] and the
risk of chronic dialysis (aHR; 1.29, 95% CI; 1.11 - 1.50). The sub-distribution hazard
Page 2 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
ratio (SHR) of UGIB for chronic dialysis (competing event: all-cause mortality) was
1.37 (95% CI, 1.15-1.64) in competing-risks analysis with adjustments for age, renal
function, gender, diabetes, hemoglobin, albumin, and urine protein/creatinine ratio.
Conclusions
UGIB is associated with increased risk of chronic dialysis and all-cause mortality in
patients with CKD-ND stages 3-5. This association is independent of age, gender,
basal renal function, hemoglobin, albumin, and urine protein levels.
Keywords
chronic kidney disease, chronic dialysis, mortality, gastrointestinal bleeding,
Strengths and limitations of this study
� Upper gastrointestinal bleeding not only increases all-cause mortality but also
increases the risk of chronic dialysis in patients with chronic kidney disease.
� This association is shown in a cohort of CKD patients with adjustments for
confounders.
� The generalizability of this finding may be limited by one hospital and a single
ethnic group.
Page 3 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
Introduction
Upper gastrointestinal bleeding (UGIB) is a common gastrointestinal disorder in
patients with chronic kidney disease and not receiving dialysis (CKD-ND) 1 2. In
CKD-ND patients, the risk of UGIB is negatively associated with their renal function
1. UGIB not only increases the risk of hospitalization but also increases in-hospital
mortality in CKD-ND patients and CKD 5 patients on dialysis 3. The increased
all-cause mortality associated with UGIB is usually explained by the worsened
comorbid conditions caused by the UGIB3-5.
Dialysis may be needed in patients with CKD-ND when UGIB leads to decreased
intravascular volume and the subsequent pre-renal acute kidney injury 6. Furthermore,
UGIB episodes may be the last straw for progression of CKD and may lead to chronic
dialysis if CKD-ND patients do not recover from acute kidney injury. However, the
long-term effect of UGIB on the risk of chronic dialysis in patients with CKD-ND is
not clear. The aim of the study was to investigate the risk of chronic dialysis after
UGIB in patients with CKD-ND.
Materials and Methods
Patient enrollment
All patients in the outpatient-based CKD program of China Medical University
Hospital (CMUH) from June 2003 to December 2009 were included. The CKD
Page 4 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
program included patients with CKD-ND stages 3-5 diagnosed by nephrologists and
no exclusion criteria were applied. The CKD program supported by National Health
Insurance Taiwan includes clinical endocrinologists, nephrologists, CKD nurses,
dietitians, and social workers. The purpose of the CKD program is to monitor the
progression of CKD patients. Laboratory measurements and CKD education are
performed at least four times a year. The UGIB was identified from review of medical
records and the date of UGIB was recorded. All patients were followed to the date of
initiation of chronic dialysis including hemodialysis and peritoneal dialysis, loss to
follow-up, death, or until September 2012. There were two patients who received a
kidney transplant and these two patients were excluded in the analysis because the
timing of kidney transplantation was not related to uremic symptoms. As we aimed to
investigate risk of chronic dialysis, patients who received dialysis less than 3 months
and patients who discontinued dialysis because of a recovery of renal function were
excluded.
Definition and measurements
UGIB was defined as melena, hematemesis, or the presence of red blood in gastric
lavage fluid, together with observation of a bleeding lesion or a lesion likely to have
bled on endoscopy of the upper digestive tract 1. Coronary artery disease (CAD) was
defined as a positive exercise test, angiographic findings of at least one stenosis of
Page 5 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
more than 50%, or positive findings on scintigraphy.7 Diabetes mellitus was defined
as use of insulin, use of oral anti-diabetic medication, or a fasting plasma glucose
level of 126 mg/dl or more.8 Hypertension was defined as taking antihypertensives
without regard to the actual measurement of blood pressure, or having a systolic blood
pressure reading greater than 140 mm Hg or a diastolic blood pressure reading greater
than 90 mm Hg.9 Patients’ primary kidney disease including diabetes nephropathy,
chronic glomerulonephritis (CGN), and hypertensive nephropathy was diagnosed by
the primary care physician and was recorded at enrollment.
Each patient’s body mass index (BMI), blood urea nitrogen (BUN), and creatinine
were measured at enrollment. Serum calcium, phosphorus, albumin, urine
albumin/creatinine ratio (ACR), and urine protein/creatinine ratio (PCR) were
measured in 3 months after enrollment. Estimated glomerular filtration rate (eGFR)
was calculated using the MDRD Collaboration formula.10 The formula for white or
other race was used because the patients were all Chinese. The time-varying analysis
used an average of three eGFR measurements. Medications associated with a higher
risk of UGIB, including steroids, non-steroidal anti-inflammatory drugs (NSAIDs),
aspirin, clopidogrel and warfarin, were recorded based on the review of medical
records.
Outcomes measurements
Page 6 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
The CKD nurses recorded the outcomes (dialysis for more than 3 months or mortality)
and date of the outcomes in the computerized case-management system. The CKD
nurses also checked patients’ status in the computerized medical record system in
CMUH and contacted patients who did not return to the outpatient every 6 months.
The percentage of patients who were lost to follow-up was 6% in the CKD program.
The outcomes were validated by a study nurse through a review of medical records
and the study nurse was blinded to the aim of the study, and other physicians
performed the analysis.
Statistical analysis
Data were reported as mean ± standard deviation, median (interquartile range), or
frequency (percentage) as appropriate. All continuous variables were tested using
skewedness and kurtosis test for their normality. Data were analyzed using Student’s t
test for parametric variables, Kolmogorov-Smirnov test for non-parametric variables,
or chi-square test for categorical variables. Factors with a p-value < 0.05 in
univariable Cox proportional hazard regression and risk factors of chronic dialysis in
the literature were considered as possible confounders. Possible confounders for
all-cause mortality and chronic dialysis were analyzed using multivariable Cox
proportional hazard regression. An adjusted hazard ratio (aHR) and 95% confidence
Page 7 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
intervals (CI) of aHR in multivariable Cox regression with adjustments for age,
gender, and eGFR were calculated. We utilized competing-risks analysis 11 with
adjustments for confounders identified in Cox regression because the risk of chronic
dialysis may be overestimated if patients’ death was not taken into consideration 12 13.
An adjusted sub-distribution HR (aSHR) and 95% CI of aSHR were calculated in
competing-risks analysis with adjustments for age, gender, eGFR, and confounders
for chronic dialysis. The primary outcome was defined as chronic dialysis and the
competing event was patient’s death in the competing-risks analysis. All analyses
were performed using Stata version 13 SE (StataCorp, TX, USA) and a p-value < 0.05
was considered statistically significant.
Ethical considerations
Internal review board approval (DMR 99-IRB-301) was obtained for the review of
medical records, and the need for informed consent was waived.
Results
Patient characteristics
We identified 3126 patients with CKD-ND stages 3–5 including 1691 males and 1435
female, aged 65±14 years (Table 1). Diabetes nephropathy and chronic
glomerulonephritis (CGN) were the major forms of primary kidney disease. The basal
eGFR of the patients was 21 (11-37) ml/min/1.73m2 and the urine PCR was 1.4 (0.5 -
Page 8 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
3.6) g/g at enrollment. Patients with UGIB were older and more often had diabetes, a
lower eGFR, a lower hemoglobin, a higher BUN, a higher creatinine, and a lower
serum albumin. They, however, had similar use of steroid, NSAIDs, aspirin,
clopidogrel, and warfarin. There were no differences in serum calcium and phosphate
levels in the patients with UGIB and the patients without. The times of follow-up
were similar in the patients with UGIB and the patients without (p = 0.38, Table 2).
The proportion of the patients with UGIB who started chronic dialysis was higher
than that of the patients without UGIB (61.5% vs. 27.4%, p < 0.01). Patients with
UGIB were associated with a higher all-cause mortality than patients without UGIB
(11.6% vs. 5.6%, p < 0.01).
Upper gastrointestinal bleeding and risk of mortality
UGIB was independently associated with higher all-cause mortality (Table 3) with an
aHR of 1.51 (95% CI: 1.07 - 2.13, p = 0.02). Patients’ age, eGFR, and serum albumin
were independently associated with all-cause mortality. The aHR was 1.05 for every
one additional year (95% CI: 1.04 – 1.07, p < 0.01), 0.99 for every ml/min/1.73m2 of
eGFR (95% CI: 0.0.98-1.00, p < 0.01), and 0.52 per g/dl of serum albumin (95% CI:
0.42 – 0.65, p < 0.01). Diabetes, CAD, hemoglobin, and PCR were not associated
with all-cause mortality. Use of steroid, NSAIDs, clopidogrel, and warfarin were not
Page 9 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
associated all-cause mortality, either.
Upper gastrointestinal bleeding and risk of chronic dialysis
UGIB was associated with an increased risk of chronic dialysis with an aHR of 1.29
(95% CI: 1.11-1.50, p < 0.01). Diabetes was independently associated with increased
risk of chronic dialysis with an HR of 1.49 (95% CI: 1.30 - 1.72, p < 0.01).
Hemoglobin and serum albumin were associated with lower risk of chronic dialysis.
PCR was associated with increased risk of chronic dialysis with an HR of 1.29 (95%
CI: 1.11-1.50) per 1g/g. Steroids, NSAIDs, clopidogrel, and warfarin were not
associated with the risk of chronic dialysis. The aSHR of UGIB for chronic dialysis
was 1.37 (95% CI: 1.15-1.64, p < 0.01) in competing-risks analysis with adjustments
for age, gender, eGFR, diabetes, hemoglobin, albumin, and PCR. The cumulative
incidence of chronic dialysis in patients with UGIB and those without is shown in
Figure 1.
Discussion
In this cohort of patients with CKD-ND stages 3-5, UGIB was associated with higher
risk of chronic dialysis. The association of UGIB and risk of chronic dialysis were
further validated using competing-risks analysis. The competing-risks analysis was
Page 10 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
critical to this study because UGIB was associated with increased all-cause mortality.
UGIB can be a complication of uremia because of the uremic coagulopathy. In this
study, UGIB patients started chronic dialysis after a median of 1.2 (interquartile range:
0.7-1.3) years. Uremic coagulopathy associated UGIB therefore may not be one of the
uremic symptoms that required dialysis in these patients. In summary of our previous
studies 1 14 15 and this study (Figure 2), patients with CKD-ND were more at risk for
developing UGIB and UGIB may further accelerate the progression of CKD to
chronic dialysis. The common aggravating factors of CKD and UGIB are anemia16,
diabetes, and hypoalbuminemia1. In addition, higher GFR and uses of
angiotensinogen converting enzyme inhibitor (ACEi) or angiotensin II receptor
blocker (ARB) may protect UGIB in this scenario 15. Some beneficial effects of ACEi
and ARB may come from their association with decreased risk of UGIB 15.
Most of CKD patients died from CAD during the course of CKD progression and
only some of the CKD patients started chronic dialysis 17-19. In our study, the
proportion of patients who started chronic dialysis was higher than that of patients
who died. This was not only observed in our previous studies 1 20 but also in other
cohort of CKD patients in Taiwan 21. The high prevalence of chronic dialysis in
Taiwan may be explained by an ethnic difference 22 or the effectiveness of
Page 11 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
multidisciplinary care for CKD in Taiwan 21.
Diabetes was associated with the risk of chronic dialysis because diabetes is a
well-known confounder of dialysis. NSAIDs were also well-known risk factors for
UGIB and chronic dialysis 23, but we did not find any significant association of
NSAIDs and chronic dialysis. Aspirin, clopidogrel, warfarin were not associated with
the risk of chronic dialysis in patients with CAD, either. Steroids treatment was
relatively common in patients with CKD 24 but only 3% of patients took steroids in
this study. Steroids treatment was not associated with the risk of chronic dialysis in
this study. A limited number of patients who took these medications in this study may
explain this result. In addition, nausea and vomiting can be uremic symptoms 25 and
are indications of dialysis. Nausea and vomiting are common in patients with UGIB 26.
Although some CKD patients initiated dialysis because of UGIB-related nausea and
vomiting rather than uremic symptoms, the percentages of patients with nausea and
vomiting at the initiation of dialysis were similar among patients with UGIB and
those without. In addition, we excluded patients who underwent dialysis less than 3
months and discontinued dialysis because of a recovery of renal function.
UGIB-related nausea/vomiting did not explain the association of UGIB and chronic
dialysis in this study.
Page 12 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
The limitations of this study were its observational study design and the inclusion of
all patients in single hospital in Taiwan. This may limit the generalizability of our
finding to other ethnic groups. More studies of various ethnic groups and multiple
institutions are required to confirm our results. Patients of a CKD program were
analyzed in this study and therefore patient selection bias cannot be avoided. We also
recorded proton-pump inhibitor treatment for UGIB but did not find any beneficial
effect of proton-pump inhibitor in decreasing risk of chronic dialysis and all-cause
mortality. In spite of the limitations, this is the first study that shows an association of
UGIB and chronic dialysis, independent of all confounders of chronic dialysis. This
suggests that UGIB not only leads to acute kidney injury but also results in long-term
consequence of irreversible kidney injury in this population.
Conclusions
Upper gastrointestinal bleeding is associated with increased risk of chronic dialysis in
patients with chronic kidney disease stages 3-5 and not receiving dialysis. This
association is independent of age, gender, basal renal function, diabetes, hemoglobin,
albumin, and urine protein levels. More studies will be warranted to investigate if
prevention of UGIB may slow the progression of CKD and delay the need of dialysis
in patients with CND-ND.
Page 13 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Acknowledgments
This study was supported in part by This study is supported in part by Taiwan
Ministry of Health and Welfare Clinical Trial and Research Center of Excellence
(MOHW105-TDU-B-212-133019) and China Medical University Hospital
(DMR-101-019 & DMR-102-015). The funders had no role in study design, data
collection and analysis, decision to publish, or preparation of the manuscript.
Contribution of Authors
Study concept, design, and acquisition of data: CC Liang; analysis, interpretation of
data, and drafting of the manuscript: CY Chou; critical revision of the manuscript for
important intellectual content: CT Chang, IK Wang; study supervision: CC Huang
Conflict of interest statement
The results presented in this paper have not been published previously in whole or
part. The authors have no conflicts of interest regarding the design or publication of
this study.
Data sharing statement
None
Page 14 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
References
1. Liang CC, Wang SM, Kuo HL, et al. Upper gastrointestinal bleeding in patients with
CKD. Clin J Am Soc Nephrol 2014;9(8):1354-9.
2. Yang JY, Lee TC, Montez-Rath ME, et al. Trends in acute nonvariceal upper
gastrointestinal bleeding in dialysis patients. J Am Soc Nephrol
2012;23(3):495-506.
3. Sood P, Kumar G, Nanchal R, et al. Chronic kidney disease and end-stage renal
disease predict higher risk of mortality in patients with primary upper
gastrointestinal bleeding. Am J Nephrol 2012;35(3):216-24.
4. Åhsberg K, Höglund P, Staël von Holstein C. Mortality from peptic ulcer bleeding:
the impact of comorbidity and the use of drugs that promote bleeding. Alimentary
pharmacology & therapeutics 2010;32(6):801-10.
5. Leontiadis GI, Molloy-Bland M, Moayyedi P, et al. Effect of comorbidity on
mortality in patients with peptic ulcer bleeding: systematic review and meta-analysis.
Am J Gastroenterol 2013;108(3):331-45; quiz 46.
6. Moreau R, Lebrec D. Acute renal failure in patients with cirrhosis: perspectives in
the age of MELD. Hepatology 2003;37(2):233-43.
7. Dormandy JA, Charbonnel B, Eckland DJ, et al. Secondary prevention of
macrovascular events in patients with type 2 diabetes in the PROactive Study
(PROspective pioglitAzone Clinical Trial In macroVascular Events): a randomised
controlled trial. Lancet 2005;366(9493):1279-89.
8. Gottlieb DJ, Punjabi NM, Newman AB, et al. Association of sleep time with diabetes
mellitus and impaired glucose tolerance. Arch Intern Med 2005;165(8):863-7.
9. Lavie P, Herer P, Hoffstein V. Obstructive sleep apnoea syndrome as a risk factor for
hypertension: population study. BMJ 2000;320(7233):479-82.
10. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate
glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Annals of internal medicine
1999;130(6):461-70.
11. Fine JP, Gray RJ. A proportional hazards model for the subdistribution of a
competing risk. J Am Stat Assoc 1999;94(446):496-509.
12. Evans DW, Ryckelynck JP, Fabre E, et al. Peritonitis-free survival in peritoneal
dialysis: an update taking competing risks into account. Nephrology, dialysis,
transplantation : official publication of the European Dialysis and Transplant
Association - European Renal Association 2010;25(7):2315-22.
13. Bechade C, Guittet L, Evans D, et al. Early failure in patients starting peritoneal
dialysis: a competing risks approach. Nephrology, dialysis, transplantation : official
publication of the European Dialysis and Transplant Association - European Renal
Page 15 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Association 2014;29(11):2127-35.
14. Liang CC, Muo CH, Wang IK, et al. Peptic ulcer disease risk in chronic kidney
disease: ten-year incidence, ulcer location, and ulcerogenic effect of medications.
PloS one 2014;9(2):e87952.
15. Chou CY, Wang SM, Chang PH, et al. Angiotensin II receptor blocker prevents
upper gastrointestinal bleeding in hypertensive patients with chronic kidney disease
not on dialysis. Int J Clin Pract 2015.
16. Hsu TW, Liu JS, Hung SC, et al. Renoprotective effect of
renin-angiotensin-aldosterone system blockade in patients with predialysis
advanced chronic kidney disease, hypertension, and anemia. JAMA Intern Med
2014;174(3):347-54.
17. Winkelmayer WC, Levin R, Avorn J. Chronic kidney disease as a risk factor for
bleeding complications after coronary artery bypass surgery. Am J Kidney Dis
2003;41(1):84-9.
18. Go AS, Chertow GM, Fan D, et al. Chronic kidney disease and the risks of death,
cardiovascular events, and hospitalization. N Engl J Med 2004;351(13):1296-305.
19. Tangri N, Stevens LA, Griffith J, et al. A predictive model for progression of
chronic kidney disease to kidney failure. JAMA 2011;305(15):1553-9.
20. Chen IR, Wang SM, Liang CC, et al. Association of walking with survival and RRT
among patients with CKD stages 3-5. Clin J Am Soc Nephrol 2014;9(7):1183-9.
21. Wang SM, Hsiao LC, Ting IW, et al. Multidisciplinary care in patients with chronic
kidney disease: A systematic review and meta-analysis. European journal of internal
medicine 2015;26(8):640-5.
22. Xu R, Zhang L, Zhang P, et al. Comparison of the prevalence of chronic kidney
disease among different ethnicities: Beijing CKD survey and American NHANES.
Nephrology, dialysis, transplantation : official publication of the European Dialysis
and Transplant Association - European Renal Association 2009;24(4):1220-6.
23. Plantinga L, Grubbs V, Sarkar U, et al. Nonsteroidal anti-inflammatory drug use
among persons with chronic kidney disease in the United States. Ann Fam Med
2011;9(5):423-30.
24. Levin A, Bakris GL, Molitch M, et al. Prevalence of abnormal serum vitamin D,
PTH, calcium, and phosphorus in patients with chronic kidney disease: results of the
study to evaluate early kidney disease. Kidney Int 2007;71(1):31-8.
25. Murtagh FE, Addington-Hall JM, Edmonds PM, et al. Symptoms in advanced renal
disease: a cross-sectional survey of symptom prevalence in stage 5 chronic kidney
disease managed without dialysis. J Palliat Med 2007;10(6):1266-76.
26. Roderick PJ, Wilkes HC, Meade TW. The gastrointestinal toxicity of aspirin: an
overview of randomised controlled trials. Br J Clin Pharmacol 1993;35(3):219-26.
Page 16 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Page 17 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Legends
Figure 1. Cumulative incidence of chronic dialysis in patients with and without upper
gastrointestinal bleeding (UGIB) using competing-risks regression with adjustments
for age, gender, renal function, diabetes, hemoglobin, albumin, and urine
protein/creatinine ratio. The primary event was chronic dialysis and the competing
event was all-cause mortality.
Figure 2. Upper gastrointestinal bleeding (UGIB) may accelerate the progression of
chronic kidney disease (CKD) and further increase the risk of chronic dialysis. In this
interactive scheme of UGIB and CKD, aggravating factors include anemia, diabetes,
and hypoalbuminemia, and protective factors contain a higher glomerular filtration
rate (GFR) and uses of angiotensionogen converting enzyme inhibitor (ACEi)/
angiotensin II receptor blocker (ARB).
Page 18 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Table 1. Clinical characteristics and outcomes according to upper gastrointestinal bleeding
Basal characteristics Total
n=3126
UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.8 1.0-4.3 2.8 0.8-4.3 2.4 0.9-4.1 0.38
Age (year) 65 ±14 64 ±14 68 ±12 <0.01
Male n(%) 1691 54.1 1476 53.9 215 55.6 0.54
Primary kidney disease
Diabetes nephropathy 1141 36.5 968 35.3 173 44.7
<0.01 CGN 1059 33.9 938 34.3 121 31.3
Hypertensive nephropathy 520 16.6 476 17.4 44 11.4
CAD 380 12.2 324 11.8 56 14.5 0.14
eGFR (ml/min/1.73 m2) 21 11-37 21 11-38 16 9-28 <0.01
BMI (kg/m2) 24.2 ±4.1 24.2 ±4.1 24.1 ±3.9 0.51
Hemoglobin (g/dl) 10.6 ±2.4 10.7 ±2.4 10.1 ±2.3 <0.01
BUN (mg/dl) 48 ±31 48 ±31 54 ±31 <0.01
Creatinine (mg/dl) 3.8 ±2.9 3.7 ±2.8 4.3 ±2.9 <0.01
Calcium (mg/dl) 9.1 ±0.7 9.1 ±0.7 9.1 ±0.8 0.77
Phosphorus (mg/dl) 4.6 ±1.4 4.5 ±1.4 4.6 ±1.2 0.26
Albumin (g/dl) 3.4 ±0.6 3.5 ±0.6 3.3 ±0.6 <0.01
ACR (g/g) 0.6 0.1-2.2 0.5 0.1-2.0 1.6 0.2-3.5 0.08
PCR (g/g) 1.4 0.5-3.6 1.3 0.5-3.4 2.2 0.9-4.5 <0.01
Medications n(%)
Steroids 106 3.4 97 3.5 9 2.3 0.21
NSAIDs 61 2.0 50 1.8 11 2.8 0.18
Aspirin 351 11.2 305 11.1 46 11.9 0.66
Clopidogrel 94 3.0 83 3.0 11 2.8 0.84
Warfarin 64 2.1 52 1.9 12 3.1 0.12
UGIB: upper gastrointestinal bleeding, CGN: chronic glomerulonephritis, eGFR:
estimated glomerular filtration rate using MDRD formula, CAD: coronary artery
disease, BMI: body mass index, BUN: blood urea nitrogen, ACR: urine
albumin/creatinine ratio, PCR: urine protein/creatinine ratio, NSAIDs: non-steroidal
anti-inflammatory drugs
Page 19 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
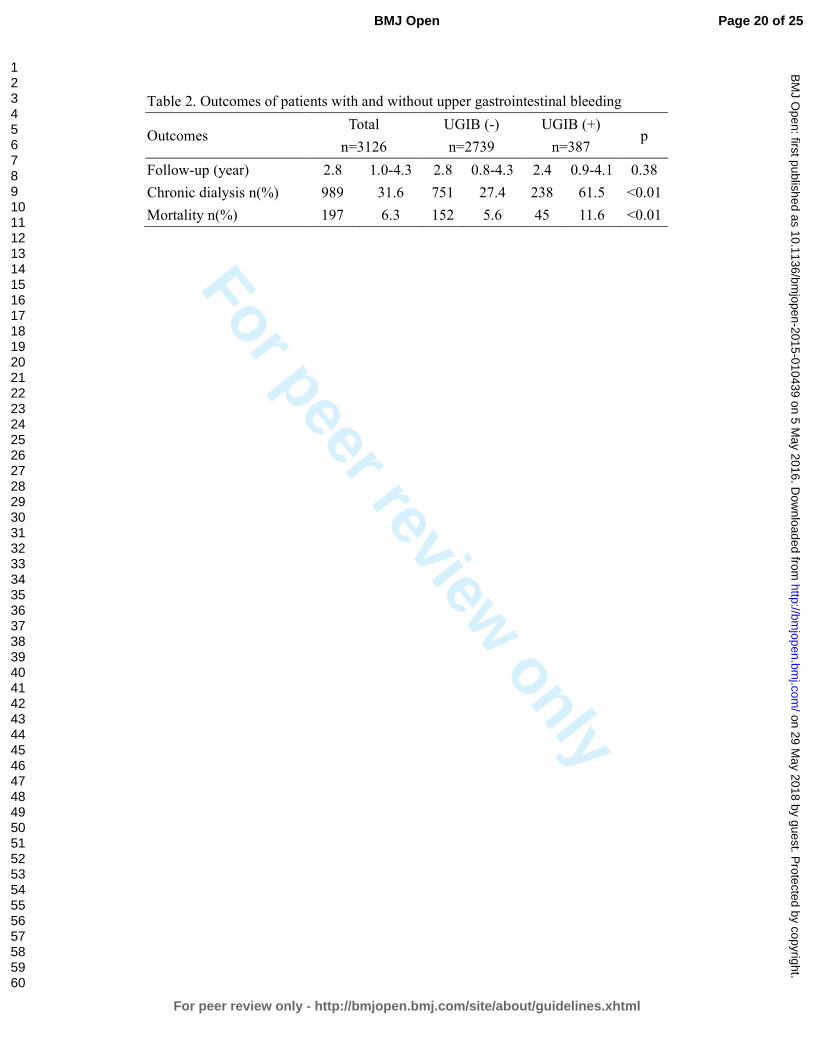
For peer review only
Table 2. Outcomes of patients with and without upper gastrointestinal bleeding
Outcomes Total
n=3126
UGIB (-)
n=2739
UGIB (+)
n=387 p
Follow-up (year) 2.8 1.0-4.3 2.8 0.8-4.3 2.4 0.9-4.1 0.38
Chronic dialysis n(%) 989 31.6 751 27.4 238 61.5 <0.01
Mortality n(%) 197 6.3 152 5.6 45 11.6 <0.01
Page 20 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
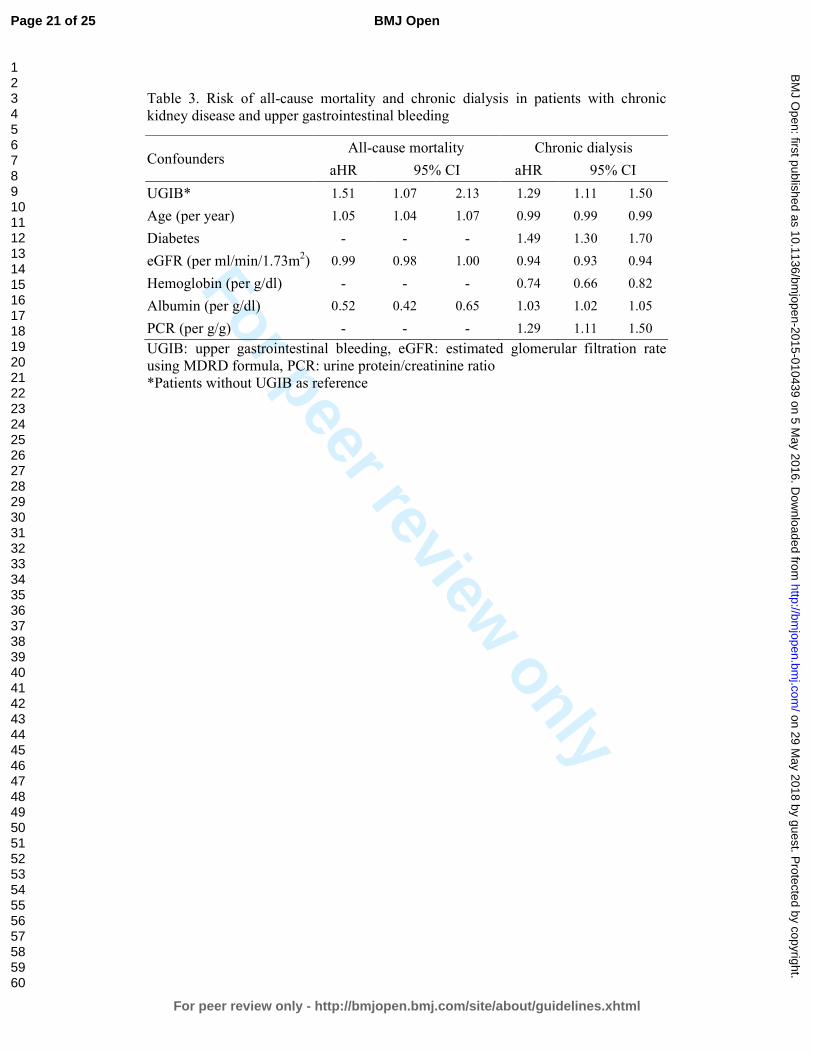
For peer review only
Table 3. Risk of all-cause mortality and chronic dialysis in patients with chronic kidney disease and upper gastrointestinal bleeding
Confounders All-cause mortality Chronic dialysis
aHR 95% CI aHR 95% CI
UGIB* 1.51 1.07 2.13 1.29 1.11 1.50
Age (per year) 1.05 1.04 1.07 0.99 0.99 0.99
Diabetes - - - 1.49 1.30 1.70
eGFR (per ml/min/1.73m2) 0.99 0.98 1.00 0.94 0.93 0.94
Hemoglobin (per g/dl) - - - 0.74 0.66 0.82
Albumin (per g/dl) 0.52 0.42 0.65 1.03 1.02 1.05
PCR (per g/g) - - - 1.29 1.11 1.50
UGIB: upper gastrointestinal bleeding, eGFR: estimated glomerular filtration rate using MDRD formula, PCR: urine protein/creatinine ratio *Patients without UGIB as reference
Page 21 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from

For peer review only
Figure 1
196x145mm (300 x 300 DPI)
Page 22 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
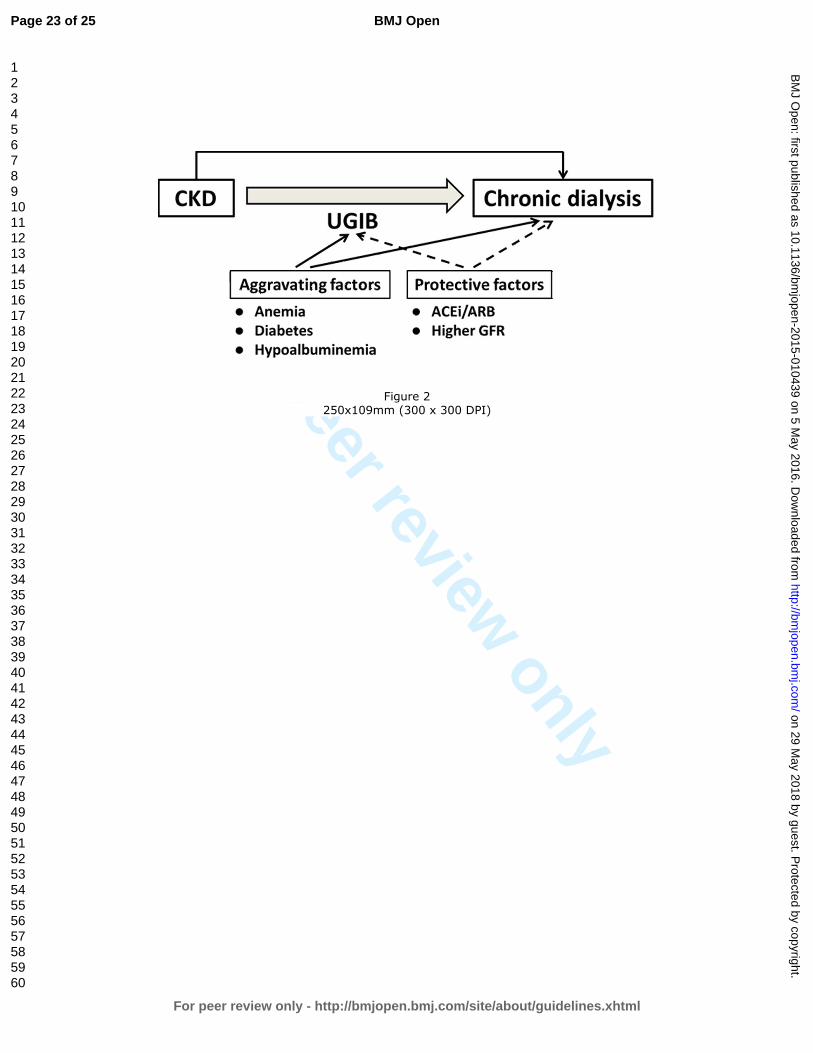
For peer review only
Figure 2
250x109mm (300 x 300 DPI)
Page 23 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-010439 on 5 M
ay 2016. Dow
nloaded from
For peer review only
1
STROBE Statement Checklist of items that should be included in reports of observational studies
Section/Topic Item
No Recommendation
Reported
on Page No
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 3
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4
Objectives 3 State specific objectives, including any prespecified hypotheses 4
Methods
Study design 4 Present key elements of study design early in the paper 6
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection
6
Participants 6
(a) Cohort study—Give the eligibility criteria, and the sources and methods of selection of participants. Describe methods of
follow-up
Case-control study—Give the eligibility criteria, and the sources and methods of case ascertainment and control selection. Give the
rationale for the choice of cases and controls
Cross-sectional study—Give the eligibility criteria, and the sources and methods of selection of participants
6
(b) Cohort study—For matched studies, give matching criteria and number of exposed and unexposed
Case-control study—For matched studies, give matching criteria and the number of controls per case 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable 7
Data sources/measurement 8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe comparability of
assessment methods if there is more than one group 7
Bias 9 Describe any efforts to address potential sources of bias 13
Study size 10 Explain how the study size was arrived at NA
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and why NA
Statistical methods 12
(a) Describe all statistical methods, including those used to control for confounding 8
(b) Describe any methods used to examine subgroups and interactions 8
(c) Explain how missing data were addressed 8
(d) Cohort study—If applicable, explain how loss to follow-up was addressed
Case-control study—If applicable, explain how matching of cases and controls was addressed
Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy
7
(e) Describe any sensitivity analyses NA
Page 24 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from

For peer review only
2
Section/Topic Item
No Recommendation
Reported
on Page No
Results
Participants 13*
(a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed
eligible, included in the study, completing follow-up, and analysed 7
(b) Give reasons for non-participation at each stage 7
(c) Consider use of a flow diagram NA
Descriptive data 14*
(a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders 8
(b) Indicate number of participants with missing data for each variable of interest 8
(c) Cohort study—Summarise follow-up time (eg, average and total amount) 8
Outcome data 15*
Cohort study—Report numbers of outcome events or summary measures over time 8
Case-control study—Report numbers in each exposure category, or summary measures of exposure NA
Cross-sectional study—Report numbers of outcome events or summary measures NA
Main results 16
(a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence interval).
Make clear which confounders were adjusted for and why they were included 9
(b) Report category boundaries when continuous variables were categorized 9
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period 9
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 10
Discussion
Key results 18 Summarise key results with reference to study objectives 10
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude
of any potential bias 13
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar
studies, and other relevant evidence 11
Generalisability 21 Discuss the generalisability (external validity) of the study results 12
Other Information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the
present article is based 16
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE checklist is
best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at http://www.annals.org/, and
Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 25 of 25
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on 29 May 2018 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-010439 on 5 May 2016. Downloaded from