pediatric parapharyngeal lesions: criteria for malignancy
TRANSCRIPT
International Journal of Pediatric Otorhinolaryngology 77 (2013) 1955–1959
Contents lists available at ScienceDirect
International Journal of Pediatric Otorhinolaryngology
journa l homepage: www.e lsev ier .com/ locate / i jpor l
Pediatric parapharyngeal lesions: Criteria for malignancy
Lobna El Fiky a,*, Tamer Shoukry b,**, Ossama Hamid c,1
a Ain Shams University, 48 Ibn El Nafees Street, 6th District, Madinet Nasr, 11371 Cairo, Egyptb Ain Shams University, 15 El Khalifa El Maamoun Street, Heliopolis, Cairo, Egyptc Ain Shams University, 50 El Hegaz Street, Heliopolis, Cairo, Egypt
A R T I C L E I N F O
Article history:
Received 5 April 2013
Received in revised form 10 September 2013
Accepted 13 September 2013
Available online 1 October 2013
Keywords:
Parapharyngeal space tumors
Pediatric head neck malignancy
Neurogenic tumors
Metastatic head neck tumors
A B S T R A C T
Introduction: Parapharyngeal space (PPS) pediatric lesions represent a heterogeneous group of
uncommon neoplasms of both benign and malignant nature. These tumors tend to be locally advanced
by the time they are diagnosed; consequently, an early presumptive diagnosis of malignancy is of utmost
importance.
Objective: To highlight the occurrence of malignant PPS tumors in pediatric population, to determine
their incidence and to describe probable warning clues for diagnosis.
Patients and methods: The charts of 23 pediatric patients with PPS swellings were retrospectively
reviewed to analyze clinical and pathologic data. We describe possible criteria to suspect malignancy by
clinical and radiological examination.
Results: Twenty-three patients presented with neoplastic lesions in the PPS, benign tumors in 43.5% and
malignant in 56.5%. Malignancy was suspected in 13 cases according to combined clinical and
radiological criteria: a painless intraoral and neck swelling in children below one year old, presentation
with cranial nerve palsy, nasopharyngeal mucosal or sub-mucosal irregular lesion, the presence of
multiple lymph nodes with no evidence of infection, and adjacent bony skull base destruction with
intracranial extension.
Conclusion: Occurrence of malignancy in PPS tumors in the pediatric population is not uncommon.
Clinicians should deliberately look for associated secondary signs that predict malignancy. The surgeon
must understand the pathological spectrum of tumors of this space and the proper use of imaging studies
to make a preoperative diagnosis. This allows for planning of a sound surgical approach and a proper
preoperative counseling.
� 2013 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
Parapharyngeal tumors are rare tumors of the head and necklocated in a complex anatomical region [1–4]. Nonetheless, theparapharyngeal space (PPS) is of particular importance, for thediversity of structures it houses and thus the varied nature of thetumors it can contain [1,2,5,6]. The clinical presentation of thesetumors is always subtle, which hinders early diagnosis with astandard physical examination [1,3,7].
A lesion in the PPS can arise primarily within the space or morecommonly extend secondarily from the surrounding fascialcompartments or can represent metastatic disease [2,5,8,9]. Most
* Corresponding author. Tel.: +20 2 2741840; fax: +20 2 6708390;
mobile: +20 127461137.** Corresponding author. Tel.: +20 1007233186.
E-mail addresses: [email protected], [email protected] (L. El Fiky),
[email protected], [email protected] (T. Shoukry),
[email protected] (O. Hamid).1 Tel.: +20 1222145199/128487849; fax: +20 2 26394964.
0165-5876/$ – see front matter � 2013 Elsevier Ireland Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.ijporl.2013.09.010
available studies in the literature discuss PPS tumors in the adultpopulation. In children, there are a wide variety of tumors thatcan be found as miscellaneous case reports [10–14]. Unlikeadults, there are differences in pathomorphologic spectrum ofpediatric PPS tumors [15]. The salivary gland tumors andparagangliomas that dominate in adult population are extremelyrare in pediatric population where the most common tumor to beencountered is that of neurogenic origin [14]. Both benign andmalignant tumors may arise from any structure contained withinthe PPS in adults as well as pediatric population [6,12,16,17].Nevertheless, the diagnostic and surgical challenges of PPSlesions in children are much more delicate than in adultpopulation [10,18] (Table 1).
With the advent of CT scan and MRI, the radiological evaluationof the PPS lesions has advanced markedly providing an improvedunderstanding of the anatomy and allowing improved differentialdiagnosis based on characteristic displacement of fascial planes[7,9,19,20]. Imaging studies of this region must be obtained beforeattempting biopsy or excision, as vascular lesions may present inthe PPS [21].
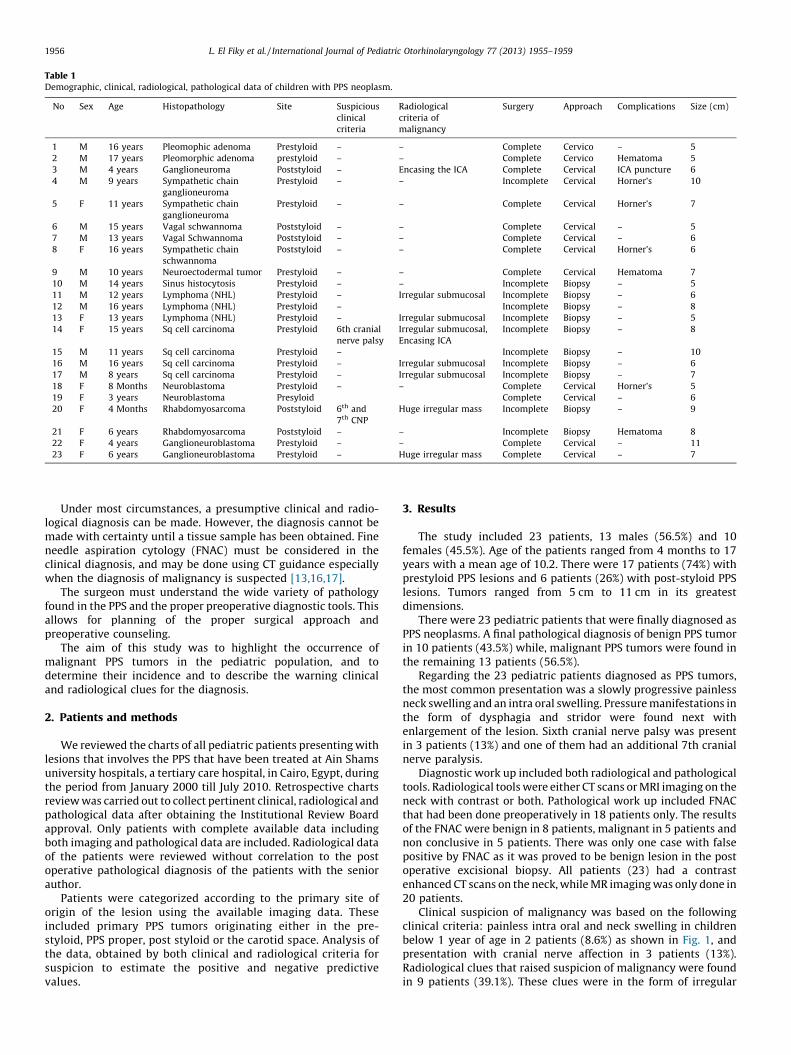
Table 1Demographic, clinical, radiological, pathological data of children with PPS neoplasm.
No Sex Age Histopathology Site Suspicious
clinical
criteria
Radiological
criteria of
malignancy
Surgery Approach Complications Size (cm)
1 M 16 years Pleomophic adenoma Prestyloid – – Complete Cervico – 5
2 M 17 years Pleomorphic adenoma prestyloid – – Complete Cervico Hematoma 5
3 M 4 years Ganglioneuroma Poststyloid – Encasing the ICA Complete Cervical ICA puncture 6
4 M 9 years Sympathetic chain
ganglioneuroma
Prestyloid – – Incomplete Cervical Horner’s 10
5 F 11 years Sympathetic chain
ganglioneuroma
Prestyloid – – Complete Cervical Horner’s 7
6 M 15 years Vagal schwannoma Poststyloid – – Complete Cervical – 5
7 M 13 years Vagal Schwannoma Poststyloid – – Complete Cervical – 6
8 F 16 years Sympathetic chain
schwannoma
Poststyloid – – Complete Cervical Horner’s 6
9 M 10 years Neuroectodermal tumor Prestyloid – – Complete Cervical Hematoma 7
10 M 14 years Sinus histocytosis Prestyloid – – Incomplete Biopsy – 5
11 M 12 years Lymphoma (NHL) Prestyloid – Irregular submucosal Incomplete Biopsy – 6
12 M 16 years Lymphoma (NHL) Prestyloid – Incomplete Biopsy – 8
13 F 13 years Lymphoma (NHL) Prestyloid – Irregular submucosal Incomplete Biopsy – 5
14 F 15 years Sq cell carcinoma Prestyloid 6th cranial
nerve palsy
Irregular submucosal,
Encasing ICA
Incomplete Biopsy – 8
15 M 11 years Sq cell carcinoma Prestyloid – Incomplete Biopsy – 10
16 M 16 years Sq cell carcinoma Prestyloid – Irregular submucosal Incomplete Biopsy – 6
17 M 8 years Sq cell carcinoma Prestyloid – Irregular submucosal Incomplete Biopsy – 7
18 F 8 Months Neuroblastoma Prestyloid – – Complete Cervical Horner’s 5
19 F 3 years Neuroblastoma Presyloid Complete Cervical – 6
20 F 4 Months Rhabdomyosarcoma Poststyloid 6th and
7th CNP
Huge irregular mass Incomplete Biopsy – 9
21 F 6 years Rhabdomyosarcoma Poststyloid – – Incomplete Biopsy Hematoma 8
22 F 4 years Ganglioneuroblastoma Prestyloid – – Complete Cervical – 11
23 F 6 years Ganglioneuroblastoma Prestyloid – Huge irregular mass Complete Cervical – 7
L. El Fiky et al. / International Journal of Pediatric Otorhinolaryngology 77 (2013) 1955–19591956
Under most circumstances, a presumptive clinical and radio-logical diagnosis can be made. However, the diagnosis cannot bemade with certainty until a tissue sample has been obtained. Fineneedle aspiration cytology (FNAC) must be considered in theclinical diagnosis, and may be done using CT guidance especiallywhen the diagnosis of malignancy is suspected [13,16,17].
The surgeon must understand the wide variety of pathologyfound in the PPS and the proper preoperative diagnostic tools. Thisallows for planning of the proper surgical approach andpreoperative counseling.
The aim of this study was to highlight the occurrence ofmalignant PPS tumors in the pediatric population, and todetermine their incidence and to describe the warning clinicaland radiological clues for the diagnosis.
2. Patients and methods
We reviewed the charts of all pediatric patients presenting withlesions that involves the PPS that have been treated at Ain Shamsuniversity hospitals, a tertiary care hospital, in Cairo, Egypt, duringthe period from January 2000 till July 2010. Retrospective chartsreview was carried out to collect pertinent clinical, radiological andpathological data after obtaining the Institutional Review Boardapproval. Only patients with complete available data includingboth imaging and pathological data are included. Radiological dataof the patients were reviewed without correlation to the postoperative pathological diagnosis of the patients with the seniorauthor.
Patients were categorized according to the primary site oforigin of the lesion using the available imaging data. Theseincluded primary PPS tumors originating either in the pre-styloid, PPS proper, post styloid or the carotid space. Analysis ofthe data, obtained by both clinical and radiological criteria forsuspicion to estimate the positive and negative predictivevalues.
3. Results
The study included 23 patients, 13 males (56.5%) and 10females (45.5%). Age of the patients ranged from 4 months to 17years with a mean age of 10.2. There were 17 patients (74%) withprestyloid PPS lesions and 6 patients (26%) with post-styloid PPSlesions. Tumors ranged from 5 cm to 11 cm in its greatestdimensions.
There were 23 pediatric patients that were finally diagnosed asPPS neoplasms. A final pathological diagnosis of benign PPS tumorin 10 patients (43.5%) while, malignant PPS tumors were found inthe remaining 13 patients (56.5%).
Regarding the 23 pediatric patients diagnosed as PPS tumors,the most common presentation was a slowly progressive painlessneck swelling and an intra oral swelling. Pressure manifestations inthe form of dysphagia and stridor were found next withenlargement of the lesion. Sixth cranial nerve palsy was presentin 3 patients (13%) and one of them had an additional 7th cranialnerve paralysis.
Diagnostic work up included both radiological and pathologicaltools. Radiological tools were either CT scans or MRI imaging on theneck with contrast or both. Pathological work up included FNACthat had been done preoperatively in 18 patients only. The resultsof the FNAC were benign in 8 patients, malignant in 5 patients andnon conclusive in 5 patients. There was only one case with falsepositive by FNAC as it was proved to be benign lesion in the postoperative excisional biopsy. All patients (23) had a contrastenhanced CT scans on the neck, while MR imaging was only done in20 patients.
Clinical suspicion of malignancy was based on the followingclinical criteria: painless intra oral and neck swelling in childrenbelow 1 year of age in 2 patients (8.6%) as shown in Fig. 1, andpresentation with cranial nerve affection in 3 patients (13%).Radiological clues that raised suspicion of malignancy were foundin 9 patients (39.1%). These clues were in the form of irregular

[(Fig._3)TD$FIG]
Fig. 3. MRI on the neck, axial cuts showing a huge parapharyngeal lesion causing
posterior displacement of the neck vessels.
[(Fig._4)TD$FIG]
[(Fig._1)TD$FIG]
Fig. 1. CT scan on the neck with contrast, axial cuts of a 2 years old child, with
compromised airway by huge intra oral swelling on the left side.
L. El Fiky et al. / International Journal of Pediatric Otorhinolaryngology 77 (2013) 1955–1959 1957
pharyngeal mucosa or sub-mucosal lesion that is extending to thePPS in 5 patients (21.7%) as shown in Figs. 2 and 3. Otherradiological clues included multiple lymph nodes with no evidenceof infection in 2 patients (8.6%) as shown in Fig. 4, adjacent bonydestruction with intra cranial extension in 2 patients (8.6%) asshown in Fig. 5 and encasement of the internal carotid artery in 2patients (8.6%) as shown in Fig. 6.
Combining both clinical and radiological clues for themalignancy suspicion, a total of 9 out of the 13 patients withmalignant PPS tumors were accurately suspected. Using thesecriteria, four patients were false negative as they were notsuspicious of malignancy. One patient was a false positive result asit proved to be a paraganglioma encasing the internal carotid
[(Fig._2)TD$FIG]Fig. 2. MRI on the neck, T1 WI, coronal cuts showing a huge left parapharyngeal
mass with irregular surface caused by a submucosal lesion.
artery (patient 3). When calculating these combined clinical andradiological clues for raising suspicion of malignancy, the positivepredictive value was 90% and the negative predictive value was69.2%. The low figure of the negative predictive value make it isdifficult to accurately define the nature of the tumor without theexcisional biopsy.
Operative intervention in PPS tumors included nasopharyngealbiopsy in four patients (17.3%) while incisional biopsy were done infive patients (21.7%) in order to reach a pathological diagnosis.Transcervical approach was used in the remaining 14 patients(60.8%) aiming for complete excision. Complete macroscopicresection was accomplished in 12 patients (52.17%), whileincomplete removal was done in 2 patients (8.6%).
Fig. 4. Coronal cuts MRI on the neck T1 WI, showing multiple cervical lymph nodes
with no evidence of infection.

[(Fig._5)TD$FIG]
Fig. 5. CT scan on the neck, axial cuts with contrast showing huge parapharyngeal
lesion with posterior encroachment over the anterior surface of the cervical spines
causing irregular surface (Bony destruction).
L. El Fiky et al. / International Journal of Pediatric Otorhinolaryngology 77 (2013) 1955–19591958
Operative complications included one patient with internalcarotid artery puncture during dissection of ganglioneuroma thatwas encasing the artery in a four years old child. The vessel wasencased by the tumor and extremely attenuated as shown in Fig. 6.Primary repair was immediately done, without the need for bloodtransfusion and there were no post operative neurologic deficit.However, complete removal of the tumor could not be achieved.Post operative complications included a hematoma collection inthree patients (13%), and Horner’s syndrome in four patients(17.3%).
The final pathological diagnosis proved to be benign in 10patients, representing 43.5% of tumors. Benign tumors includedtwo patients with pleomorphic adenoma, three patients ofschwannoma, three patients of ganglioneuroma, one patient withwell differentiated neuroectodermal tumor and one patient withsinus histocytosis. Malignant tumors accounted for 56.5% oftumors. Malignant tumors included lymphoma in three patients,four patients with squamous cell carcinoma, two patients with
[(Fig._6)TD$FIG]Fig. 6. CT scan on the neck with contrast, axial cuts showing complete encasement
of the internal carotid artery with the parapharyngeal lesion in a 4 years old child
with ganglioneuroma.
neuroblastoma, two patients with rhabdomyosarcoma, and gang-lioneuroblastoma in two patients.
Malignant lesions were confirmed and staged after pathologicalevaluation. Chemotherapy was given for seven patients, radio-therapy was given for five patients, and a combination ofradiotherapy and chemotherapy was given for four patients.Follow up of the patients with malignancy ranged from 23 to 64months post operatively. Three patients died from the disease,while four patients had recurrence and received further treatment.Remission with no evidence of recurrence was achieved in sixpatients that were alive and free of the disease.
4. Discussion
A large array of unusual PPS lesions present in childhood [17].Because tumors in the PS are rare, the exact incidence of suchtumors is very difficult to determine [22]. Congenital lesions aswell as infections are by far more common in children than tumors[4,15].
On the other hand, the common benign salivary gland tumorsthat occur in adult population are extremely rare in children in thePPS. This was in accordance with our series as we had only 2patients with pleomorphic adenoma. Nevertheless, both benignand malignant tumors may arise from any structure containedwithin the space [14,21]. Malignant tumors however, tend to bemore common in the pediatric group. In a review of literature,pediatric malignant PPS lesions accounted for 67% of patients withPPS tumors encountered [10]. In the current series, malignancywas found in 56.5% of all tumors encountered being more commonthan benign tumors.
Variability of malignant tumors includes soft tissue tumors,neurogenic tumors, lymphomas, sarcomas, metastases and naso-pharyngeal carcinoma as well as other uncommon lesions [13].Such a histopathologic spectrum must modify the preoperativediagnosis and surgical treatment [10].
Making a diagnosis of malignancy involving PPS is usuallydifficult and delayed especially in children [15,17,23]. Manyreasons contribute to such occurrence. The clinical presentation isusually insidious, minimal, vague and versatile [1,2,9,18,19,22]. Itis also difficult to elicit clinical findings in such an age. The deeplysituated position of the PPS, and the difficult examination of theoropharynx, needs a relatively long time until the pathology isunveiled [1,14,21].
At the same time, malignancy in the PPS can easily mimicinfection or normal lymphoid hypertrophy of adenoidal tissue.Nasopharyngeal and intraoral growth requires differentiation fromthe more common inflammatory illness of the adenoidal andtonsillar infection, which is more common in such an age [10,20].
Children with malignancies might also present with symptomsand signs that mimic infection including fever [15,24]. It is not rarethat a PPS malignancy present asymptomatic [9,17]. Finally, due tothe rarity of these PPS malignant lesions and the age of the patients,we usually consider malignancy a remote possibility.
In order to avoid this delay in the diagnosis of pediatric PPSmalignant lesions, we raised the clinical and radiological clues thatmight help in earlier diagnosis of malignant lesions in the PPSamong the pediatric population. The clinical clues that were usedin the prediction of malignancy were, below 1 year age, cranialnerve affection on presentation. The radiological clues ofmalignancy were, asymmetrical mucosal or submucosal nasopha-ryngeal lesion, presence of large multiple lymph nodes, extra-parenchymal extension, perineural invasion and skull base lesion[1,2,7,16,17].
We advocate that any clinical suspicion should be immediatelycomplemented by radiological evaluation and should consider thepresence of malignant lesion. This suspicion must be confirmed by

L. El Fiky et al. / International Journal of Pediatric Otorhinolaryngology 77 (2013) 1955–1959 1959
pathological examination. FNAC is an easy, rapid, and effectivemethod of predicting this myriad of lesions, though some grayzones prevail [22]. However, FNAC is sometimes difficult toperform in children, and its results are sometimes not reliable[1,2,9,10,12]. This should modify the diagnostic workup for analternative approach to reach a pathological diagnosis. Biopsies areindicated in the context of extirpation surgery. This usually can bedone in PPS tumors even if malignant in nature as they aresometimes well encapsulated and a safe macroscopic removal canbe achieved. Given the anatomical complexity of the PPS, theprognosis of infilterative lesions remain poor in spite of themeticulous surgical effort [10].
An incisional biopsy guided by frozen section to establish theproper pathological diagnosis and proceed accordingly is also aviable option [3,14]. Although a total removal of the lesion isdesirable, it should not be accomplished at the expense of injury ofvital nerves or vessels. In pediatric PPS malignant tumors, surgeonshould also take into account adjunctive therapeutic options suchas chemotherapy and radiotherapy to minimize surgical morbidityand to improve the prognosis [10].
Unfortunately, most malignancies of the PPS in childhood arehigh grade, a non Hodgkin’s lymphoma, undifferentiated squa-mous cell carcinoma, neuroblastoma or embryonal sarcomas andusually need adjunctive treatment for control, as they have a highrate of advanced loco-regional disease as well as metastatses [16].Although the prognosis of these tumors is grave, they areconsidered potentially curable especially in early stages. Thetherapeutic implications of a delayed diagnosis of a malignantlesion in this area can be significant. A high index of suspicion willlead to early biopsy, greatly improving the prognosis [20].
In conclusion, we should emphasize that malignant tumors aremore common than benign tumors in the PPS in the pediatricpopulation. Consideration of malignany in this age and site should beborn in mind. Primary malignant PPS tumors are usually neurogenicin origin in that age group. One should direct attention todeliberately look for distinctive suspicious features. Earlier diagnosiscan direct the patient to timely appropriate therapy. The surgeonmust understand the pathological spectrum of tumors of this spaceand the proper use of imaging studies to make a preoperativediagnosis. This allows for planning of a sound diagnostic andtherapeutic strategy and a proper preoperative counseling.
Conflict of interest
There is no conflict of interest of this study.
Acknowledgments
Authors thank all the staff of the ENT clinic at Demerdashhospital at the Faculty of Medicine of Ain Shams University fortheir cooperation. Also, all the medical secretary staff of the samehospital for their help in collecting the data of the patients andtheir medical records.
References
[1] V. Suarez-Fente, J.L. Liorente-Pendas, J. Gomez-Martinez, L.A. Garcia-Gonzalez,F. Lopez-Alvarez, C. Suarez-Nieto, Primary tumours of the parapharyngealspace. Our experience in 51 patients, Acta Otorrinolaringol. Esp. 60 (1)(2009) 19–24.
[2] K. Luna-Ortiz, J.E. Navarrete-Aleman, M. Granados-Garcia, A. Herrera-Gomez,Primary parapharyngeal space tumors in a Mexican cancer center, Otolaryngol.Head Neck Surg. 132 (2005) 587–591.
[3] K.R.W. Zhi, H. Zhou, Y. Wen, Y. Zhang, Management of parapharyngeal spacetumors, J. Oral Maxillofac. Surg. 67 (2009) 1239–1244.
[4] S. Saussez, T.D. Maesschalk, V. Mahillon, O. Filleul, S. Louryan, Second branchialcyst in the parapharyngeal space: a case report, Auris Nasus Larynx 36 (2009)376–379.
[5] P.M. Som, H.D. Curtin, Fascia and spaces of the neck, in: P.M. Som, H.D. Curtin(Eds.), Head and Neck Imaging, fouth ed., St. Louis: C.V. Mosby, 2003, pp. 1820–1824.
[6] R.C. Helmberger, S.P. Stringer, A.A. Mancuso, Rhabdomyoma of the pharyngealmusculature extending into the prestyloid parapharyngeal space, Am. J. Neuroa-diol. 17 (1996) 1115–1118.
[7] S. Shirakura, A. Tsunoda, K. Akita, T. Sumi, M. Suzuki, T. Sugimoto, et al., Para-pharyngeal space tumors: anatomical and image analysis finding, Auris NasusLarynx 37 (2010) 621–625.
[8] K. Rajagopal, A. Ramesh, S. Sreepathi, C. Shetty, CT Evaluation of parapharyngealmasses: pictorial assay, Int. J. Radiol. 10 (2) (2009).
[9] F. Bozza, M.G. Vigili, P. Ruscito, A. Marzetti, F. Marzetti, Surgical management ofparapharyngeal space tumours: results of 10-year follow-up, Acta Otorhinolar-yngol. Ital. 29 (2009) 10–15.
[10] I. Starek, V. Mihal, Z. Novak, D. Pospisilova, J. Vomacka, J. Vokurka, Pediatrictumors of the parapharyngeal space. Three case reports and a literature review,Int. J. Pediatr. Otorhinolaryngol. 68 (2004) 601–606.
[11] W. Ng, S.H. Chan, A.W.M. Lee, K.Y. Lau, T.K. Yau, W.M. Hung, et al., Parapharyngealextension of nasopharyngeal carcinoma: still a significant factor in era of modernradiotherapy? Int. J. Radiat. Oncol. Biol. Phys. 72 (4) (2008) 1802–1809.
[12] P.P. Singh, A. Sharma, N. Gupta, Parapharyngeal space lipoma, Indian J. Otolar-yngol. Head Neck Surg. 56 (2) (2004) 152–154.
[13] S. Vranic, S.K. Caughron, S. Djuricic, N. Bilalovic, S. Zaman, I. Suljevic, et al.,Hamartomas, teratomas and teratocarcinosarcomas of the head and neck: reportof 3 new cases with clinico-pathologic correlation, cytogenetic analysis, andreview of the literature, BMC Ear Nose Throat Disord. 8 (8) (2008).
[14] M.T. Brigger, S.E. Pearson, Management of parapharyngeal minor salivary neo-plasms in children: a case report and review, Int. J. Pediatr. Otorhinolaryngol. 70(2006) 143–146.
[15] Y.L.C. Lau, K. Tsui, A. Lee, Life-threatening airway obstruction: an unusualpresentation of a cervical mass during infancy, HK J. Paediatr. (New Series) 11(2006) 153–156.
[16] S. Sahraoui, A. Acharki, A. Benider, N. Bouras, A. Kahlain, Nasopharyngeal carci-noma in children under 15 years of age: a retrospective review of 65 patients, Ann.Oncol. 10 (1999) 1499–1502.
[17] P.J. Bradley, P.T. Bradley, K.D. Olsen, Update on the management of paraphar-yngeal tumours, Curr. Opin. Otolaryngol. Head 19 (2011) 92–98.
[18] H. Chijiwa, T. Mihoki, B. Shin, K. Sakamoto, H. Umeno, T. Nakashima, Clinicalstudy of parapharyngeal space tumours, J. Laryngol. Otol. 123 (Suppl. S 31) (2009)100–103.
[19] Satyawati, A.K. Gupta, V.L. Nehru, N.K. Kandelwal, S.B.S. Mann, Parapharyngealspace tumors: a radiological and surgical correlation, Indian J. Otolaryngol. HeadNeck Surg. 58 (2) (2006) 120.
[20] H.E. Stambuk, S.G. Patel, K.M. Mosier, S.L. Wolden, A.I. Holodny, Nasopharyngealcarcinoma: recognizing the radiographic features in children, Am. J. Neuroradiol.26 (2005) 1575–1579.
[21] R. Shahab, T. Heliwell, A.S. Jones, How we do it: a series of 114 primary pharyngealspace neoplasms, Clin. Otolaryngol. 30 (2005) 364–367.
[22] P. Mondal, N. Basu, S. Gupta, N. Bhattacharya, M. Mallick, Fine needle aspirationcytology of parapharyngeal tumors, J. Cytol. 26 (3) (2009) 102–104.
[23] G. El-Husseiny, A. Allam, Khafagy y, A. Kandil, A.Z. Belal, L. Shalaby, et al.,Nasopharyngeal carcinoma in children and adolescents, J. Egypt. Nat. CancerInst. 12 (3) (2000) 151–155.
[24] S.E. Forgie, J.L. Robinson, Pediatric malignancies presenting as a possible infec-tious disease, BMC Infect. Dis. 7 (44.) (2007).