pediatric neuropsychology case studies || the energizer bunny meets shirley temple: attention...
TRANSCRIPT

Chapter 15
The Energizer Bunny Meets Shirley Temple:
Attention Deficit Hyperactivity Disorder,
Combined Type
Michael J. Zaccariello
‘‘She will not sit still and be quiet! She just goes and goes nonstop.’’ Jenna’s
exasperated mother moaned during the initial clinical interview. Her voice was
tinged with both frustration and guilt over her reactions to her daughter’s behavior
that occasionally resulted in abrupt, sharp rebukes. In addition, Jenna herself had
begun to realize that something was ‘‘wrong.’’ This previously effervescent and
optimistic child began to remark that she was stupid and dumb and was being
ridiculed by peers at school.
Historically, Jenna was a highly energetic toddler who talked excessively.
Although never significantly or consistently oppositional or argumentative, her
behavior became increasingly more difficult to control as she grew older. Jenna’s
mother noted that she literally played all day long and seemingly never tired. In
addition, it was impossible for her to sit down appropriately for longer than a few
minutes at a time. She constantly fidgeted, kicked her legs, or touched objects.
Cognitively, she had extreme difficulty staying focused and on-task, and needed
frequent redirection or a quiet, nonstimulating environment to complete work. She
had a tendency to be impulsive, rushing through her school assignments, which
resulted in careless mistakes. She had organizational problems in her day-to day-
activities (e.g., frequently losing objects or articles of clothing). Academically, she
had always been an average to above average student, but starting in the second
grade she began to demonstrate some struggles in mathematics, spelling, and
handwriting. Her mother’s perception was that Jenna’s difficulties in these academ-
ic areas were not reflective of a skill deficit but, rather, extreme problems with
sustained focus and impulsivity.
Medically, Jenna was in perfect health, and both language and motor develop-
mental milestones were reached within normal limits. She had no significant
problems with vision, hearing, eating, or sleeping. She was prescribed no medica-
tion at the time of the evaluation.
Socially, Jenna was described as an outgoing and engaging child who enjoyed
horseback riding and any outdoor activities. She lived with her parents and an older
J.N. Apps et al. (eds.), Pediatric Neuropsychology Case Studies: 141
From the Exceptional to the Commonplace.# Springer Science þ Business Media, LLC 2010

brother who had been diagnosed with Attention Deficit Hyperactivity Disorder-
Primarily Inattentive Type (ADHD-I) by a pediatric neuropsychologist. The home
environment was described as positive and loving.
Jenna’s parents requested a neuropsychological evaluation to identify her pattern
of cognitive strengths and weaknesses. However, their prime concern was her
increasing restlessness and difficulties with attention. They were also concerned
with the emotional toll of social ridicule because of her high energy behavior. Her
parents questioned if she met formal criteria for Attention Deficit Hyperactivity
Disorder (ADHD) and wished for professional corroboration of their suspicion.
Jenna had never undergone a neuropsychological evaluation, and her mother
was curious about her overall cognitive skill set. Consequently, a broad approach
was taken, with a focus on attention and mental executive function measures.
Measures of attention are thought to assess one’s ability to direct and maintain
focus on a task. Executive functions are considered a related construct and involve
higher-ordered, goal-directed abilities that are organizational or supervisory in
nature. This cluster of abilities allows one to engage in abstract reasoning, prob-
lem-solving, judgment, cognitive flexibility, planning, and organization. Utilizing
feedback to correct responses, inhibit inappropriate behavior, and sustain one’s
attention is also considered in this area. Specific domains that were assessed
included intellectual ability, fine motor functions, attention, executive functions,
language fluency, visual-spatial abilities, and comprehensive academic skills de-
velopment. Behavioral ratings scales completed by both Jenna’s teacher and par-
ents were included as a critical foundation of the assessment.
Conceptual Diagnostic Background
With the introduction of the Diagnostic and Statistical Manual of Mental Disorders,
Third Edition, in 1980, delineation was made between the presence and absence of
hyperactive symptoms in children with attentional difficulties. Current diagnostics
further clarified this distinction into three types: primarily inattentive (ADHD-I),
primarily hyperactive-impulsive (ADHD-H), and combined (ADHD-C). However,
some recent studies have questioned the diagnostic accuracy of the current categor-
ical subtypes of ADHD and propose more of a dimensional model (Frazier, Young-
strom, & Naugle, 2007). Prevalence studies indicate that ADHD (devoid of a
specific subtype) is diagnosed three times as often in boys than girls in community
samples. This discrepancy rises to five to nine times more often in clinic-referred
groups. It is thought that ADHD-C occurs more often in boys and that ADHD-I
tends to be diagnosed more in girls. As children age, hyperactive symptoms
typically dissipate, but inattention symptoms can remain prominent. In a sense,
one does not typically outgrow ADHD.
There has been much debate in the literature concerning the usefulness
and relevance of neuropsychological tests in the diagnosis of ADHD. Although
a comprehensive review of this issue is beyond the scope of this brief case,
142 M.J. Zaccariello

indications suggest that the most scientific and powerful diagnostic indicator of
ADHD is a significant level of inattention or hyperactive symptoms as reported on
behavioral rating scales.
So, this begs the question, what is the point of a comprehensive neuropsycho-
logical evaluation of a child with ADHD features? Although not necessarily
diagnostic, a neuropsychological evaluation can provide a snapshot of how signifi-
cantly inattention or hyperactivity interacts with performance in other cognitive and
academic domains. Once such areas have been identified, specific recommenda-
tions beyond those typically given for ADHD can be outlined in the report to
maximize a child’s learning potential (Tables 15.1–15.3).
Test Results
On formal testing, Jenna presented as an absolutely delightful and pleasant young
girl. She readily engaged in conversation and expressed an appropriate range of
emotion throughout the evaluation. Her social interactions were appropriate, and
she spontaneously demonstrated a very kind and helpful attitude (e.g., picking up
dropped items).
In terms of her approach to testing, there was significant evidence of motor
restlessness throughout the evaluation, coupled with moderate levels of distracti-
bility, inattentiveness, and impulsivity. She had extreme difficulty sitting upright
and still in her seat. She frequently fidgeted, got out of her chair, rubbed the walls,
and looked at herself in an one-way mirror. Rather frequently, she reached for test
stimuli before being told to do so and/or blurted out answers before receiving
Table 15.1 Intellectual
Wechsler Intelligence Scale for Children – Fourth Edition Scorea Percentile
Full Scale IQ 113 81st
General Ability Index 111 77th
Verbal Comprehension Index 99 47th
Similarities (10)
Vocabulary (8)
Comprehension (12)
Perceptual Reasoning Index 121 92nd
Block Design (12)
Picture Concepts (14)
Matrix Reasoning (14)
Working Memory Index 110 75th
Digit Span (11)
Letter-Number Sequencing (13)
Processing Speed Index 109 73rd
Coding (12)
Symbol Search (11)a Standard score, (scaled score), [T-score], {z-score}.
15 The Energizer Bunny Meets Shirley Temple 143

Table 15.2 Academic achievement
Woodcock Johnson Tests of Achievement – Third Edition Score Percentile
Broad reading 108 71st
Letter-word identification 110 75th
Passage comprehension 100 51st
Reading fluency 108 70th
Basic reading skills 109 73rd
Letter-word identification 110 75th
Word attack 106 66th
Broad math 120 91st
Calculation 113 80th
Applied problems 126 96th
Math fluency 103 59th
Broad written language 104 60th
Spelling 103 58th
Writing samples 104 60th
Writing fluency 102 55th
Academic skills 110 75th
Academic applications 112 78th
Academic fluency 106 65th
Table 15.3 Other cognitive functions
Tests Scorea Percentile
Attention-Deficit Hyperactivity Disorder RatingScale – Fourth Edition
Home Version
Total >99th
Hyperactivity-impulsivity 97th–98th
Inattention 98th–99th
School Version
Total 95th–96th
Hyperactivity-impulsivity 94th–95th
Inattention 94th–95th
Achenbach Child Behavior Checklist
Parent Form
Anxious/depressed [63] 90th
Withdrawn/depressed [50] 50th
Somatic complaints [53] 62nd
Social problems [50] 50th
Thought problems [58] 79th
Attention problems [80] >97th
Rule-breaking behavior [55] 69th
Aggressive behavior [60] 84th
Teacher’s Report Form
Anxious/depressed [50] 50th
Withdrawn/depressed [50] 50th
Somatic complaints [50] 50th
(continued)
144 M.J. Zaccariello
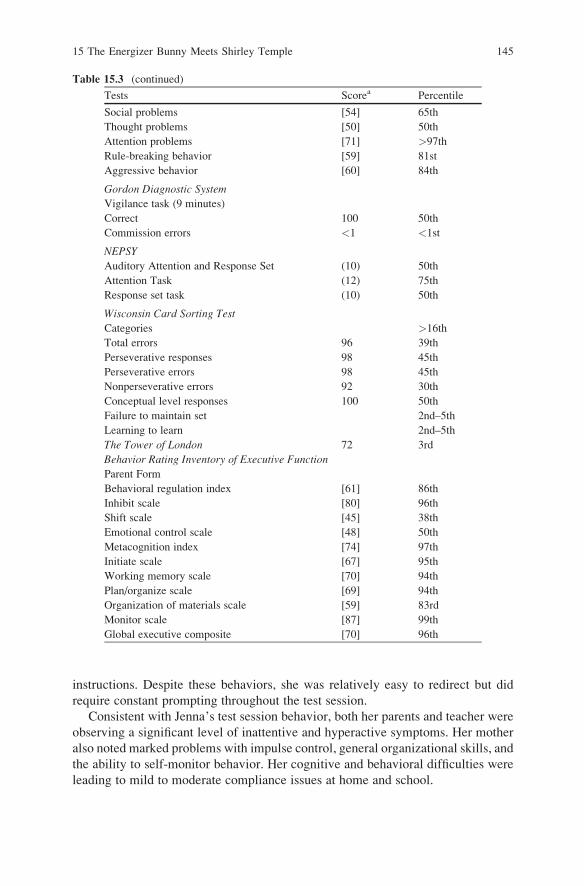
instructions. Despite these behaviors, she was relatively easy to redirect but did
require constant prompting throughout the test session.
Consistent with Jenna’s test session behavior, both her parents and teacher were
observing a significant level of inattentive and hyperactive symptoms. Her mother
also noted marked problems with impulse control, general organizational skills, and
the ability to self-monitor behavior. Her cognitive and behavioral difficulties were
leading to mild to moderate compliance issues at home and school.
Table 15.3 (continued)
Tests Scorea Percentile
Social problems [54] 65th
Thought problems [50] 50th
Attention problems [71] >97th
Rule-breaking behavior [59] 81st
Aggressive behavior [60] 84th
Gordon Diagnostic System
Vigilance task (9 minutes)
Correct 100 50th
Commission errors <1 <1st
NEPSY
Auditory Attention and Response Set (10) 50th
Attention Task (12) 75th
Response set task (10) 50th
Wisconsin Card Sorting Test
Categories >16th
Total errors 96 39th
Perseverative responses 98 45th
Perseverative errors 98 45th
Nonperseverative errors 92 30th
Conceptual level responses 100 50th
Failure to maintain set 2nd–5th
Learning to learn 2nd–5th
The Tower of London 72 3rd
Behavior Rating Inventory of Executive Function
Parent Form
Behavioral regulation index [61] 86th
Inhibit scale [80] 96th
Shift scale [45] 38th
Emotional control scale [48] 50th
Metacognition index [74] 97th
Initiate scale [67] 95th
Working memory scale [70] 94th
Plan/organize scale [69] 94th
Organization of materials scale [59] 83rd
Monitor scale [87] 99th
Global executive composite [70] 96th
15 The Energizer Bunny Meets Shirley Temple 145
A quick glance at Jenna’s neuropsychological profile revealed that most of her
scores were average to above average. Overall intellectual ability was high average
with a significant strength in nonverbal intellectual ability relative to her solidly
average verbal intellectual ability. She had little difficulty on specific tests of
language, visual-spatial processing, or fine motor dexterity. Her academic skills
development was progressing at the expected rate with no evidence of deficit in any
academic domain.
A different picture emerged on tests of attention and mental executive function.
Her test scores ranged from average to impaired. Jenna had difficulty on most tasks
where she had to rely on self-regulation strategies to successfully negotiate the
measure and did not have the examiner encouraging her to remain attentive. She
was impulsive, which resulted in a high number of mistakes. In addition, she
displayed a weakness in being able to change problem solving strategies efficiently.
Formulation and Recommendations
On the basis of the responses to behavioral questionnaires and test session behavior,
Jenna had significant inattention, distractibility, impulsivity, and motor restless-
ness, which were consistent with individuals diagnosed with ADHD-C. She could
not sit appropriately for longer than 10–15 min at a time and frequently reached for
test stimuli or blurted out answers.
Jenna was subsequently diagnosed with ADHD-C, which includes a mixture of
problems with behavioral inhibition, sustained attention, organization, consistency
of performance, and/or goal-directed behavior. ADHD-C is the most common form
of ADHD that arises in childhood in 3–7% of the population (American Psychiatric
Association, 2000). The symptoms of ADHD do not spontaneously disappear in the
majority of cases but can be treated to some extent with behavior management and/
or medication. Jenna’s combination of ADHD-C features included average intel-
lectual ability and average to above average underlying academic skills. Therefore
it would be realistic for her to attain average to above average performance in
school most of the time.
Although not directly assessed, another important finding concerned is the
Jenna’s emotional functioning. During the assessment, she acknowledged strug-
gles in school and admitted self-esteem issues related to her attentional prob-
lems. Studies have shown that 40% of children with ADHD show signs of either
depression and/or anxiety (Spencer, Biederman, & Wilens, 1999). It is vitally
important to address the behavioral and cognitive difficulties that children with
ADHD typically experience. However, professionals, caretakers, and school per-
sonnel should also be acutely aware of the impact and range that ADHD can have
on a child’s emotional and social well-being. Her parents were provided with
psychotherapy referrals, which they could use if her distress continued or worsened.
At least 75% of children with ADHD benefit from stimulant medication. Jenna’s
behavioral and cognitive presentation of ADHD symptoms make an evaluation for
stimulant medication routinely recommended. If she continues using the medica-
146 M.J. Zaccariello

tion over a long period of time, observation trials off medication for a week at a time
approximately twice during each school year would be useful to monitor her
ongoing benefit or need for the medication.
Standard suggestions for managing attention and organization problems in the
classroom included obtaining eye contact with Jenna prior to delivering directions.
It may be helpful to place a hand on her shoulder or arm and to be sure that
directions are clear, simply stated, and given one at a time. Delivering more com-
plex directions in brief, simple, numbered steps (e.g., ‘‘First, read pages 1–10;
second, answer questions 1–5; and third, check answers in the back of the book’’)
would also be helpful. If Jenna continues to have difficulty, writing down key
instructions and taping them to her desk may help cue her.
Presenting material in small, successive units that can be mastered hierarchically
would allow Jenna to maximize her attentional capacity, assist in organizing the
material to be learned, reduce the feeling of being overwhelmed by the material,
and develop greater self-confidence as she progresses through the material.
Jenna would need distractions minimized to the greatest extent possible in the
classroom (e.g., seating her at the front of the class and increased one-to-one contact
with the teacher), as well as regular feedback provided with concrete suggestions for
appropriate behaviors. It would also be helpful to provide consistency and structure
through daily schedules; standard seating arrangements; clearly defined class-
room expectations, rules and consequences; and clear places for necessary materi-
als, such as color-coded subject folders, and reinforcement for using organizers.
Jenna needs guided practice in planning how to complete assigned tasks (what
is needed, how to break tasks into manageable parts, estimating time needed for
each part) and to be assigned tasks or classroom duties that she can successfully
complete.
It would be helpful to provide other organizational checklists, such as steps to
get ready to go home after school, and to remind Jenna at the end of the day about
what she needs for home and the next day. Also, Jenna would benefit from pacing
her work and changing the pace or task frequently and from opportunities for
controlled movement.
Given Jenna’s inattentive and hyperactive tendencies, she would not always beexpected to perform at top efficiency level on timed tasks. Extra time can be given
strategically when needed, and curriculum requirements such as timed math tests
might be loosened or modified for her, but not omitted.
At home, Jenna needs more frequent attentional cueing. Adults should help her
break complex tasks into smaller steps. Commands should be given one or two at a
time, and longer sets of commands should be repeated, rehearsed, or written down.
More frequent attentional cueing (e.g., ‘‘look at this now’’; ‘‘this is important to pay
attention to’’) in everyday life will be needed in the long run, and adults should try
to avoid becoming frustrated with this need. She should be given extra instruction in
organizational skills such as outlining, diagramming, planning a sequence of steps
in complex tasks, and taking strategic breaks during extended study time.
Jenna and her family would benefit from ongoing consultation with a psycholo-
gist who is knowledgeable about behavior management approaches for children
15 The Energizer Bunny Meets Shirley Temple 147

with ADHD symptoms. Family psychotherapy could also provide an opportunity to
work on family interaction issues, emotional issues, and/or peer interaction issues
that often accompany ADHD.
Jenna’s difficulties with abstract reasoning and logical problem-solving tasks
suggest that she may have difficulty with some complex, novel tasks. Specifically,
she may find it difficult to analyze the requirements of a task and apply effective
strategies toward a solution. As a result, she may get frustrated with the acquisition
of novel cognitive skills such as higher level academics.
Although not indicated at this time given her average to above average academic
skills development, with a diagnosis of ADHD, Jenna may be eligible to have an
Accommodation Plan prepared for her as mandated under Section 504 of the
Rehabilitation Act of 1973. This could be particularly important if her academic
performance begins to suffer due to her ADHD presentation as she progresses to
higher grades with greater requirements for attention and self-control. Many of the
specific attention and organization suggestions outlined could be incorporated into
an Accommodation Plan.
Additional Resources
Key Concepts and Terms
Attention The cognitive process of selectively concentrating on one aspect of the
environment while ignoring other things.
Executive functions Processes that are most involved in giving organization and
order to actions and behavior. Executive functions involve (1) strategic thinking
and future planning, (2) the ability to inhibit or delay responding, (3) initiating
behavior, and (4) shifting between activities flexibly.
References
Resources for Clinicians
American Psychiatric Association. (2004). Diagnostic and statistical manual of mental disorders(4th ed., Text revision). Washington, DC: American Psychiatric Association.
Barkley, R. A. (2006). Attention-deficit hyperactivity disorder. (3rd ed.). New York: Guilford
Press.
Cutting, L. E., & Denckla, M. B. (2003). Attention: Relationships between attention-deficit
hyperactivity disorder and learning disabilities. In H. L. Swanson, K. R. Harris, & S. Graham
(2003), Handbook of learning disabilities (pp. 125–139). New York: Guilford Press.
Ellison, P. (2005). School neuropsychology of attention-deficit/hyperactivity disorder. In R. C.
D’Amato, E. Fletcher-Janzen, & C. R. Reynolds (Eds.), Handbook of school neuropsychology(pp. 460–486). New Jersey: Wiley
148 M.J. Zaccariello

Frazier, T. W., Youngstrom, E. A., & Naugle, R. I. (2007). The latent structure of attention-deficit/
hyperactivity disorder in a clinic-referred sample. Neuropsychology, 21, 45–64.Spencer, T., Biederman, J., & Wilens, T. (1999). Attention-deficit/hyperactivity disorder and
comorbidity. Pediatric Clinics of North America, 46, 915–927.U.S. Department of Education, Office of Special Education Programs’ (OSEP), Individuals with
Disabilities Education Act (IDEA) web site: http://www.idea.ed.gov/explore/home
Resources for Families
A.D.D. Warehouse, www.addwarehouse.com/shopsite_sc/store/html/index.html. Provides general
information on Attention Deficit Hyperactivity Disorder and a comprehensive catalog of
books, tapes, and training materials.
Barkley, R. A. (2000). Taking charge of ADHD: The complete, authoritative guide for parents.
(2nd ed.) New York: Guilford Press.
Children with Attention Deficit Disorders (CHADD), http://www.chadd.org. Lecture programs,
parent support groups, and valuable information for parents and teachers.
Dawson, P., & Guare R. (2003). Executive skills in children and adolescents: A practical guide to
assessment and intervention. New York: Guilford Press.
Flick, G. L. (1996). Power parenting for children with ADD/ADHD: A practical parent’s guide for
managing difficult behaviors. Hoboken, New Jersey: Jossey-Bass.
Learning Disabilities Association of America, http://www.ldanatl.org
National Center for Learning Disabilities, http://www.ncld.org, www.schwablearning.org and
http://www.ldonline.org/.
15 The Energizer Bunny Meets Shirley Temple 149