paul dart md fca
TRANSCRIPT

Paul Dart MD FCA3495 Harris StreetEugene, OR 97405September 1, 2013
Federal Communications Commission
r.e. Comments on Notice of Inquiry, ET Docket No. 13-84
Dear Sirs,
I am part of a medical advisory group that has spent the last 18 months researching thecurrent medical literature on the biological or “non-thermal” effects of microwave radiofrequency transmissions, in an effort to assist the Eugene Water and Electric Board inmaking prudent decisions on their choices of technology as they consider installing anAMI infrastructure of RF–transmitting “smart” electric meters. This document containsthe product of our efforts—an extensive written review of the research to date onbiological effects of RF.
Also attached to this filing are five pdf documents from an audiovisual presentation onthis subject, illustrating research evidence for adverse effects including EHS(electrohypersensitivity syndrome), alterations in hormone physiology, DNA damage,cancer, infertility, and increased brain tumor risk from cell phones.
The FCC has not chosen to implement any safety standards regarding non-thermaleffects of microwave RF exposure. But the existing literature demonstrates that there issignificant cause for concern regarding the growing impacts of these exposures on thepublic. Research documenting their adverse biologic and health effects is robust now.The implications of this research cannot be discounted, and must not be ignored.
The FCC should request that the EPA impanel a Working Group composed of healthexperts who have no conflicts of interest with industry to review the scientific literatureon EMR. The Group should recommend biologically–based EMR standards that ensureadequate protection for the general public and occupational health based upon theprecautionary principle. Finally, the FCC should adopt the standards, testingprocedures, and appropriate precautionary warning language recommended by theWorking Group.
It would be indefensible at this time for the FCC to take any actions that may increaseexposure of the population to EMR from cell phones, base stations, Wi-Fi, Smart Metersand other RF or ELF–emitting devices. The current levels of exposure need to bereduced rather than increased further. The FCC must especially protect vulnerablegroups in the population including children and teenagers, pregnant women, men ofreproductive age, individuals with compromised immune systems, seniors, andworkers.
Sincerely yours,
Paul Dart MD FCA
Comments on Notice of Inquiry, ET Docket No. 13-84

Comments on Notice of Inquiry, ET Docket No. 13-84

BIOLOGICAL AND HEALTH EFFECTS OFMICROWAVE RADIO FREQUENCY
TRANSMISSIONS
A REVIEW OF THE RESEARCH LITERATURE
A REPORT TO THE STAFF AND DIRECTORS OFTHE EUGENE WATER AND ELECTRIC BOARD
June 4, 2013
Paul Dart, M.D.(lead author)
Kathleen Cordes, M.D.
Andrew Elliott, N.D.
James Knackstedt, M.D.
Joseph Morgan, M.D.
Pamela Wible, M.D.
Steven Baker(technical advisor)
Comments on Notice of Inquiry, ET Docket No. 13-84

Comments on Notice of Inquiry, ET Docket No. 13-84

EXECUTIVE SUMMARYThe FCC regulations for permissable exposures to microwave radio frequency
(RF) transmissions are only designed to protect against the thermal effects of high expo-sure levels. Representatives of the telecommunications industry usually assert thatthere is “no clear or conclusive” scientific evidence regarding the biological effects oflow level or “nonthermal” RF exposures. But in actuality, a large body of scientificresearch documents that RF exposures at low levels can produce adverse biological orhealth effects.
The installation of RF-transmitting “smart meters” by our electric utility couldsignificantly increase the level of RF exposure in Eugene’s residential neighborhoods.Such an increase carries potential health risks. The nature of these risks needs to becarefully considered before making a decision to deploy this technology.
Any decision-making process that ignores this possibility of harm could causesignificantly damage both to community health and to EWEB’s goodwill in thecommunity.
ELECTROHYPERSENSITIVITY (EHS)Microwave RF exposures can produce acute symptoms in some individuals.
These symptoms can include headache, sleep disturbance, difficulty in concentration,memory disturbance, fatigue, depression, irritability, dizziness, malaise, tinnitus,burning and flushed skin, digestive disturbance, tremor, and cardiac irregularities. Thissyndrome was described by Russian researchers in the 1950’s, who called it “microwavesickness”. Between 1953 and 1978 the Russian government purposefully targeted theU.S. embassy in Moscow with beams of microwave RF, producing symptoms ofmicrowave sickness in many embassy employees.
In recent years, the buildout of the wireless telecommunications infrastructurehas greatly increased the exposure of the general public to microwave RF, and this hasled to an increased number of individuals experiencing symptoms that are now referredto as “Electrohypersensitivity Syndrome” (EHS). Multiple research studies have showna correlation between these symptoms and residential exposure to radio, radar, and celltower transmissions.
The prevalence of EHS appears to be increasing, as the exposure of the public toRF continues to expand. Based on recent epidemiologic research, it would be reason-able to assume RF exposures provoke some sort of symptoms in between 3 and 5% ofthe population of Eugene at the current time. Any significant increase in residential RFexposure is likely to make these individuals more symptomatic, and to produce somenew cases of EHS by pushing some other individuals beyond their tolerance limit.
ALTERED PHYSIOLOGYLaboratory research in animal and human subjects has shown that “nonthermal”
levels of RF exposure can alter EEG, immune function, and hormone levels includingadrenal and thyroid hormones, testosterone, prolactin, progesterone.
Research shows that low levels of microwave RF exposure can reduce melatoninlevels in humans, and that some individuals are more sensitive than others to this effect.The adverse effects of nighttime RF exposure on melatonin secretion are particularydisturbing. The nocturnal rise in melatonin levels supports the natural function ofsleep, and disrupting this cycle can produce insomnia. Melatonin is an extremelypotent antioxidant, and helps to repair damaged DNA and heal the body from other
i
Comments on Notice of Inquiry, ET Docket No. 13-84

effects of oxidant stress.Melatonin is also protective against the growth of cancer cells, and disruption of
the circadian melatonin cycle has been shown to lead to increased tumor growth in avariety of cancer types. Women who have lower levels of nocturnal melatonin are atgreater risk for developing breast cancer. Reduced melatonin levels may also increasethe incidence of prostate cancer.
OXIDATIVE STRESS AND DAMAGED DNAIn contrast with Xrays and gamma rays, Microwave radiation does not have
sufficient power to directly break covalent bonds in DNA molecules. But microwaveRF can produce resonance interactions with ions and with charged macromolecules,and such interactions can significantly alter biochemical functions. A large body ofresearch has shown that microwave RF causes an increased production of free radicalsand reactive oxidant species in living tissues, and that this increased oxidant stressdamages DNA. This damage can and does occur at power levels well below thoselevels that could produce damage by thermal mechanisms.
Any chronic exposure to conditions that damage DNA can lead to an increasedrisk of cancer. Evidence of increased risk of certain types of cancer has been demons-trated in groups with occupational exposure to microwave RF, including radio techni-cians in private industry, military personnel, commercial airline pilots, and ham radiooperators. Elevated levels of cancer have been demonstrated in populations withincreased residential exposure to radio transmission towers. And in the last ten years,studies fro Israel, Germany, Austria, and Brazil have documented significant increasedin breast cancer and other cancers in individuals living less than 500 meters from cellphone towers, with measured exposure levels much lower than those permitted bycurrent FCC guidelines.
Research has also shown that RF exposure levels well within current guidelinescan cause DNA damage and reduced fertility in insects, birds, amphibians andmammals, and can lower sperm counts, sperm motility, and sperm motility in humanbeings.
RISKS OF CELL PHONE USECell phone use expanded dramatically in Europe and the United States in the late
1990’s. Early studies of the cancer risks of cell phone use were hampered by shortlatency periods of exposure. In general, studies funded by industry have reportedlower levels of risk than independently funded studies. But in the last four years, allbut the most poorly designed studies have shown an increased risk of brain tumorswith more than ten years of use—a level of exposure which appears to double the riskof brain tumor on the side of the head where the cell phone is customarily held. Thisrisk is higher in those who started using cell phones as children.
CONCLUSIONSExisting scientific research offers strong evidence that the chronic exposure of the
public to microwave RF transmissions produces serious acute and chronic health effectsin a significant portion of the population. These findings can be summarized in thefollowing precepts:
EXECUTIVE SUMMARY
ii
Comments on Notice of Inquiry, ET Docket No. 13-84

Basic Precepts for Residential Exposures to RF Transmissions: • Excessive RF exposure can cause acute problems (headaches, insomnia, fatigue,
vertigo, tinnitus, other symptoms of EHS).• Excessive RF exposure can also cause chronic problems (oxidative stress, cancer,
male infertility).• Constant RF transmission is probably harmful, even at low levels, and should be
avoided.• Frequent and repetitive intermittent transmissions are also probably harmful,
and should be avoided.• Nocturnal exposures are more problematic than daytime exposures, because of
RF’s potential to suppress nocturnal melatonin secretion and disturb sleep, andbecause night is the time when we rest and heal from stresses (including oxida-tive stress).
• Occasional and infrequent daytime exposures are much less likely to cause anincrease in chronic problems for the population at large.
• Occasional and infrequent daytime exposures are still likely to provoke acutesymptoms in a small percentage of the population.
EWEB should adopt a policy of minimizing their RF footprint in the community.A recognition of these precepts should lead EWEB to adopting a policy of mini-
mizing their infrastructure’s RF footprint in the community as much as possible duringregular operations. This doesn’t mean that staff would throw away their cell phonesand communicate by semaphore. But it would mean that instead of combatting or igno-ring the possibility that more RF in the community could cause harm, EWEB shouldacknowledge the potential risks of excessive residential exposure.
This would mean that such potential risks would be seriously considered in anydiscussion of the total risks and benefits involved (the “Total Bottom Line”), as EWEBdecides whether to use RF technology for any given purpose. If, after such a discussion,a considered decision is made to use RF technology, then these same potential risksshould be taken into serious consideration in determining how to use this technology ina manner that would minimize potential harm to the community.
In other words, don’t use RF when you don’t have to. Use hard-wired connec-tions wherever it is feasible to do so. And if you do use RF, design the infrastructure ina way that uses as little of it as possible.
In the final section of this report, we discuss the perspectives that such a policymight bring to a consideration of the available AMI technologies.
EXECUTIVE SUMMARY
iii
Comments on Notice of Inquiry, ET Docket No. 13-84

iv
Comments on Notice of Inquiry, ET Docket No. 13-84

TABLE OF CONTENTS
PREFACE vii
INTRODUCTION 1
ELECTROHYPERSENSITIVITY 9
RADIOFREQUENCY EFFECTS ON MELATONIN 23
RF EXPOSURE INCREASES OXIDATIVE STRESS AND DAMAGES DNA 31
CURRENT RESEARCH ON CELL PHONE USE AND BRAIN TUMOR 57
CONCLUSIONS AND RECOMMENDATIONS 67
v
Comments on Notice of Inquiry, ET Docket No. 13-84

vi
Comments on Notice of Inquiry, ET Docket No. 13-84

PREFACEThis paper represents the efforts of a group of physicians who have been in
private practice in Eugene for decades. Our concerns are for the health of our patientsas well as for our community as a whole.
When EWEB proposed installing a “mesh” smart meter network we becameconcerned. We know that there are people in this community who are highly sensitiveto electromagnetic fields. The installation of the smart meter mesh would makeEugene a much more hostile environment for these individuals.
We also know that chronic exposures to microwave radio frequency (RF) trans-missions can produce adverse long term physiological effects, even in individuals whodo not consciously experience acute symptoms from exposure to such electromagneticfields.
As we considered these issues, we were not sure if the policy makers at EWEBhad sufficient current and applicable scientific information upon which to rely, as theyevaluated the potential health effects of such an implementation. EWEB may havereferred to FCC guidelines, without considering that the FCC regulations on radiofrequency (RF) exposure are only designed to protect against the thermal effects ofextremely high level RF exposures, and do not attempt to define a safe level of protec-tion against other biological effects.
Because of these concerns, we have undertaken a sixteen month long investiga-tion of the scientific literature, in order to present what we feel is a valid scientific basisfor evaluating the potential health effects of a community-wide RF smart meter installa-tion. This paper presents our findings to you.
We have organized this report into six sections:1. An introduction into some of the issues involved in the “smart meter”
Advanced Metering Infrastructure. 2. A review of the scientific research documenting the existence of acute
reactions to “non-thermal” levels of RF exposure -- reactions which intheir most severe form are called electrohypersensitivity syndrome(EHS).
3. A review of the function of melatonin, of evidence that RF exposurecan suppress melatonin, and of the short and long term consequencesof melatonin suppression.
4. A review of the long term effects of RF exposure, especially theproduction of oxidative stress that can lead to DNA damage andincreased levels of cancer and infertility.
5. A review of current research regarding relationship of cellular andcordless telephone use to increased risk of brain tumors.
6. A discussion of our conclusions and recommendations to EWEB, basedon this review of the scientific literature.
vii
Comments on Notice of Inquiry, ET Docket No. 13-84

Comments on Notice of Inquiry, ET Docket No. 13-84

INTRODUCTIONAMI and the Smart Energy Grid
The Advanced Metering Infrastructure (AMI) technology is a key component ofthe smart energy grid that we heard discussed in very general terms in the 2008 presi-dential election. During the past two years, EWEB has been actively exploring thepossibility of installing AMI in Eugene.
EWEB staff have described several purposes for going to an AMI “smart meter”infrastructure, including the following:
Reducing operating costsRemote reading of meters would eliminate meter readers, allowing EWEB to
save substantial costs in employee time and benefits, vehicle use, and gasoline costs.Smart meters can also be used to turn power on and off remotely, saving labor andtravel costs when rentals become vacant or occupied.
Shifting time of useSmart meters can measure and record total power usage for several intervals
during the day. This will allow EWEB to bill customers more for electrical usage atpeak use hours, typically the early morning (when people are getting up, takingshowers, cooking breakfast) and late afternoon/early evening (when people returnhome from work, cook dinner, take showers, throw some clothes in the laundry, etc.).Time of use billing could create an incentive for customers to shift elective usage(laundry, recharging the electric car) away from peak usage hours.
Electrical utilities need enough generating capacity to meet peak demand. Redu-cing or restraining the growth of peak usage could reduce or slow the need to buildmore power generating capacity into the system.
Training customers to conserve electricitySmart meter technology can allow home owners to monitor their usage in real
time over a home network with the meter. EWEB hopes that this direct feedback willencourage people to reduce their energy consumption.
“Demand/Response” infrastructureEWEB has invested a great deal in wind power. But the wind tends to blow
hardest in the middle of the day and the middle of the night. At dawn and dusk (peakusage times for electrical consumers) the wind is more likely to calm down.
This creates a storage problem for the utility. When wind power production ishigh during the night, production can exceed demand, generating more electricity thancan be used locally or sold interstate.
One way to distribute and store this energy is to put it in your water heater. Twoway communication with your Smart Meter could allow the power company to turnyour water heater on for 15 minutes in the middle of the night or the middle of the day,at a time when it would otherwise not be on [they can’t turn it on for two hours, when itgets to the maximum heat setting the thermostat will turn it off]. EWEB would seekcustomers willing to volunteer to allow this arrangement.
With “demand/response” control, EWEB could store excess wind power as heatby turn on clusters of water heaters for 15 minutes, then turn them off and turn on otherclusters of water heaters, and continue to rotate the usage around the communityduring the middle of the night.
Page 1
Comments on Notice of Inquiry, ET Docket No. 13-84

Solar power generation creates another storage problem. Solar panel output canfluctuate rapidly during the day with changing cloud cover. Too sudden an increase inlocal production from multiple large panels could overload the grid. The AMI infra-structure would allow the utility to tell Smart Meters to turn off solar panel input intothe electrical grid. Again, this requires rapid two-way communication between theutility and the Smart Meter, and between the Smart Meter and the solar panel in thehouse.
From an engineering point of view, the simplest and cheapest way to install thiscommunications infrastructure is to have the meters communicate with the utility andwith the “smart appliances” in the home using wireless microwave radio technology.
The use of this wireless technology for AMI communications has generated agood deal of political heat in the last two or three years. To understand where this heathas come from, it is instructive to review the history of the Pacific Gas and ElectricCompany’s smart meter rollout in California.
PG&E in California, 2010 – 2011In 2010 and 2011 PG&E rolled out an AMI infrastructure in multiple cities in
California. The metering technology that they chose to install was the Silver SpringsAMI “smart meter”. These meters communicate with the utility by forming a “mesh”network in the neighborhood. The meters communicate with each other rather thanwith a central receiver, and pass data through this MESH network to the central collec-ting system of the electric utility.
The installation of such technology places a radio transmitter on every house inthe community. Concerns about the potential health effects of this residential RF expo-sure led several members of the California Assembly to request that the CaliforniaCouncil on Science and Technology (CCST) perform a study of whether current FCCstandards for Smart Meters were sufficiently protective of the public health, andwhether additional standards might be needed for such technology.
It should be noted that the regulatory standards established by the FederalCommunications Commission are based on defining safe levels against the thermaleffects of microwave radio frequency (RF) exposure (i.e. “Will it cook you?”) Forexample, the FCC has established Limits for Maximum Permissible Exposure (MPE).(FCC, 1999, page 15). The FCC has explicitly stated that they do not make any regula-tions or assurances whatsoever regarding the “nonthermal” biological effects ofmicrowave exposure (other physiologic effect besides heat damage). (Hankin, 2002)
The CCST released a report on “Health Impacts of Radio Frequency from SmartMeters” in January, 2011. (CCST, 2011) This report stated (on page 5) that Smart Meter-ing technology met the FCC standards for “safety against known thermally inducedhealth impacts”. It also stated (on page 4) that “To date, scientific studies have not identi-fied or confirmed negative health effects from potential non-thermal impacts of RF emissionssuch as those produced by existing common household electronic devices and smart meters. Notenough is currently known about potential non-thermal impacts of radio frequency emissions toidentify or recommend additional standards for such impacts.” The CCST report concludedthat “There is no evidence that additional standards are needed to protect the public from smartmeters.” (page 26)
When the Draft Version of this CCST report was released, several experts in thefield of research that studies the biological effects of RF communicated their disagree-
SECTION 1 – INTRODUCTION
Page 2
Comments on Notice of Inquiry, ET Docket No. 13-84
ment with the study’s conclusions. It was pointed out that the content of the CCSTdocument was in major part a repetition of a document produced by the industry-spon-sored Electric Power Research Institute a few weeks before (Tell, 2010), and that theanalysis of AMI smart meter exposure levels in the report was incorrect in its design.(Hirsch, 2011)
These experts offered evidence of multiple scientific studies documenting thenonthermal health impacts of RF. (Sage, 2011b) (Johansson, 2011) Independentresearch was presented to the CCST documenting that the Silver Springs metersproduced levels of household exposures significantly higher than levels shown to haveadverse health effects in current scientific research. (Sage, 2011a)
These objections from the scientific community did not alter the CCST’s stanceon smart meters, which continued to be installed in California.
What happened next in CaliforniaPG&E’s approach to the AMI rollout didn’t involve a lot of public education.
They just switched out the meters. And some people found that they were havingtrouble sleeping, or experiencing headaches, ringing in the ears, vertigo, or other symp-toms that hadn’t been bothering them before. Soon the internet was awash in anecdotalreports and commentary about these adverse effects. (emfsafetynetwork.org, 2011)
PG&E’s public posture was that the meters only transmitted for an average of 45seconds per day. They asserted that the total power output over time was well belowthe FCC guidelines for thermal risk, and well below that of other RF exposures in thecommunity. Videos began to crop up on You Tube showing that the picture wasn’t thatsimple (for example, http://www.youtube.com/user/thisirradiatedlife/featured).
Finally PG&E was served with a court order to provide clear documentation ofwhat the meters actually were doing. (Yip-Kikugawa, 2011) In the response to thatcourt order, PG&E provided documentation from the manufacturer of the meters thatthe average meter in the mesh network transmitted data signals to the utility 6 times aday, network management signals 15 times a day, timing signals 360 times a day, andbeacon signals to the mesh network 9,600 times a day. (Kim et al., 2011) This penciledout to an average of roughly 7 transmissions a minute, 24 hours a day, coming out ofevery meter in the community.
As reports of provoked symptoms increased, the situation became more andmore politically heated. Santa Cruz County banned the installation of smart meters.PG&E continued to install them, and the Santa Cruz County Sheriff’s office refused toenforce the ban. Individuals started purchasing refurbished analogue electric metersand swapping them out themselves, attempting to return the smart meters to the utility.PG&E publicly stated (a week or two before Christmas) that they would turn off thepower of anyone who removed a smart meter from their service box—but backed downfrom that threat due to public backlash.
By the end of 2011, multiple cities in California had either banned smart metersor placed a moratorium on their continued installation, and a lawsuit has been filedagainst PG&E with the California Public Utilities Commission. (Wilner, 2011)
EWEB’s Elster MESH AMI TrialIn 2010 EWEB set up a trial of AMI infrastructure, using the Elster REX2 Smart
Meter. Like the Silver Springs meter used by PG&E in California, the REX2 operates ona mesh network. The meters upload usage data to a central collection meter 4 to 6 times
SECTION 1 – INTRODUCTION
Page 3
Comments on Notice of Inquiry, ET Docket No. 13-84
a day, but transmit short beacon signals to the network several times a minute.EWEB stated on their website that these meters transmit “less than 10 seconds a
day”. But they were unable to state how frequently transmissions actually occurred. Inour communications with their public relations staff, we were told that Elster was un-willing to release this information. Information on the power output of these meters isavailable on the ELSTER website. (TUV Rheinland, 2010) But Elster does not discussthe actual frequency of transmission of the meters.
In January 2012 we used a Gigahertz Solutions HF35C analyzer to evaluate theoutput of one of these Elster meters in a residential neighborhood in Eugene.
Background RF signals coming through the neighborhood were measured in a360 degree circle around the monitoring position. The background RF averaged around4 microwatts/square meter (μW/m2), increasing to 8 or 10 μW/m2 when we aimed ourdirectional antenna at the radio towers on Blanton Heights or at a distant cell phonetower.
The Elster meter’s transmission rate was variable. In our observations, they aredefinitely transmitting several times a minute, sometimes 4 or 5 times a minute, andoccasionally in bursts of significantly higher frequency.
At 5 feet from the smart meter, the peak strength of the beacon signal coming offthe meter measured from 3800 to 11,000 μW/m2. At 20 feet from the meter, the powerdensity of the signal ranged from 362 to 493 μW/m2, with occasional bursts at higherpower output.
This means that at a distance of 20 feet the power of the signal coming out of theElster meter was about 100 times the power of the ambient background signal comingfrom any specific direction in the residential neighborhood.
This power density of 300+ to 400+ μW/m2 was greater than the signal strengthof the cell phone tower at 29th and Amazon, measured from about 200 meters away. Sofilling a neighborhood with a mesh network of the Elster smart meters would be similarto placing every house in that neighborhood closer than 200 meters from a cell phonetower, each house constantly being pinged by the chatter of multiple beacon signalsfrom the mesh.
This was disconcerting, since recent research has shown that people living within500 meters of a cell phone tower have increased incidence of headache, concentrationdifficulties, and sleep disorders, and also a significantly increased risk of some types ofcancer. (Khurana et al., 2010) (Levitt and Lai, 2010) (Yakymenko et al., 2011) (Altpeteret al., 2006) (Abdel-Rassoul et al., 2007)
When you put these facts together, it is not so surprising that the installation ofmesh smart meter networks in residential neighborhoods in California last year wasfollowed by a surge of anecdotal evidence regarding headaches, insomnia and otherhealth complaints. From a medical perspective, based on a familiarity with currentresearch on the biological effects of RF, this was a predictable consequence of PG&E’ssmart meter MESH network rollout.
Formation of our Advisory CommitteeBy late 2011 EWEB staff were working towards setting a specific timeline for
installing AMI in Eugene. From our perspective, the potential health risks of such aproject did not appear to have received any realistic discussion. EWEB’s web siteimplied that such risks were inconsequential. In January of 2012 EWEB’s Public Rela-
SECTION 1 – INTRODUCTION
Page 4
Comments on Notice of Inquiry, ET Docket No. 13-84

tions staff started to test a public relations campaign promoting the AMI project. Theirinitial presentation minimized the possibility any health risks from this exposure.
Some physician members of our group became involved in discussions withEWEB staff. In these discussions, we tried to learn more about the technologies underconsideration from EWEB engineers, and in turn we attempted to communicate ourconcerns about the potential health risks of this technology.
It became clear to us that EWEB staff did not have the time or the expertise toresearch this issue of health risks in any depth. Our sense of this was confirmed inApril of 2012, when EWEB management presented the AMI Business Case to the EWEBBoard. The discussion of “Potential Health Risks” in this document quoted governmentagency reports as if they were scientific studies, and stated that in an “attempt to discoverif there were any credible studies showing any health effect caused by long-term RF exposure inrelatively high dosages (e.g. exposures much greater than an AMI meter) . . . no conclusiveevidence was found that indicates that this higher magnitude RF exposure has created adversehealth impacts.”
EWEB is a locally owned utility with a lot of goodwill in the community. Wewere concerned that if EWEB continued forward without taking a deeper look at thisissue, decisions might be made that would have the potential to cause significant harmto the health of the community, or to create political strife that could significantlydamage EWEB’s local standing.
In an effort to help EWEB think this problem through in a more complete andconsidered fashion, we decided to form a group of physicians and other professionalswith scientific and engineering expertise. Over the past 16 months, our group hasstudied the scientific literature on the biological effects of microwave RF. This report isthe result of our efforts.
We hope that EWEB’s staff and Board will examine this information carefully,and that it will help them to make prudent choices as they consider the various AMItechnologies that are currently available to them.
SECTION 1 – INTRODUCTION
Page 5
Comments on Notice of Inquiry, ET Docket No. 13-84

BIBLIOGRAPY
Abdel-Rassoul G, El-Fateh OA, Salem MA et al. Neurobehavioral effects among inhabi-tants around mobile phone base stations. Neurotoxicology (2007); 28(2):434-440.
Altpeter ES, Roosli M, Battaglia M, Pfluger D, Minder CE, Abelin T. Effect of short-wave(6-22 MHz) magnetic fields on sleep quality and melatonin cycle in humans: theSchwarzenburg shut-down study. Bioelectromagnetics (2006); 27(2):142-150.
CCST. Health Impacts of Radio Frequency From Smart Meters. California Council on Science and Technology (2011); 1-50. http://www.ccst.us/news/2011/20110111smart.php
EMF Safety Network. Smart Meter Health Complaints. (2011/10/17); 1-59.http://emfsafetynetwork.org/?page_id=2292
FCC. Questions and Answers about Biological Effects and Potential Hazards of Radio-frequency Electromagnetic Fields. OET Bulletin 56, Fourth Edition, FederalCommunications Commission, Office of Engineering and Technology. (1999); 1-38.http://transition.fcc.gov/Bureaus/Engineering_Technology/Documents/bulletins/oet56/oet56e4.pdf
Hankin N. Letter from N. Hankin, Center for Science and Risk Assessment, RadiationProtection Division, United States Environmental Protection Agency, to Ms. JaneNewton, President, The EMR Network. (2002); 1-3.
Hirsch D. Comments on the Draft Report by the California Council on Science andTechnology “Health Impacts of Radio Frequency from Smart Meters”.(2011); 1-11. http://www.ccst.us/projects/smart2/documents/letter8hirsch.pdf
Johansson O. Letter to California Public Utilities Commission (CPUC) re Smart Meters.(2011); 1-3. http://www.scribd.com/doc/59738917/Dr-Johansson-s-letter-re-SmartGrid-Smart-Meter-dangers-to-CPUC-7-9-2011
Khurana VG, Hardell L, Everaert J, Bortkiewicz A, Carlberg M, Ahonen M. Epidemiolo-gical evidence for a health risk from mobile phone base stations. Int J OccupEnviron Health (2010); 16(3):263-267.
Kim A, Chonda J, Law Department PGE. Pacific Gas and Electric Company’s Responseto Adminstrative Law Judge’s October 18, 2011 Ruling Directing It to FileClarifying Radio Frequency Information. (2011/11/1); http://sunroomdesk.com/wp-content/uploads/2011/11/PGERResponsesRFDataOpt-outalternatives_11-1-11-3pm.pdf
Levitt B, Lai H. Biological effects from exposure to electromagnetic radiation emitted bycell tower base stations and other antenna arrays. Environ Rev (2010); 18:369-395.
Milham S, Morgan LL. A new electromagnetic exposure metric: high frequency voltagetransients associated with increased cancer incidence in teachers in a Californiaschool. Am J Ind Med (2008); 51(8):579-586.
Sage C. Assessment of Radiofrequency Microwave Radiation Emissions from SmartMeters. ed. Santa Barbara, CA: Sage Associates, 2011a: 1-100. http://sagereports.com/smart-meter-rf/
Sage C. Letter of Comment on Smart Meter Report. Sage Associates, 2011b: 1-6.http://www.ccst.us/projects/smart2/documents/letter12sage.pdf
Sensus. FlexNet System Specifications. (AMR-456-R2). 2011a: http://www.sensus.com/documents/10157/32460/amr_456.pdf
SECTION 1 – INTRODUCTION
Page 6
Comments on Notice of Inquiry, ET Docket No. 13-84

Sensus. SUS-1004 FlexNet Brochure. 2011b: http://www.sensus.com/documents/10157/31649/SUS-1004_FlexNet_Brochure_seperated.pdf
Tell R. An Investigation of Radiofrequency Fields Associated with the Itron SmartMeter. EPRI 2010 Technical Report Electric Power Research Institute, (2010); 1-222.http://my.epri.com/portal/server.pt/gateway/PTARGS_0_2_1630_405_228188_43/http%3B/myepri10%3B80/EPRIDocumentAccess/popup.aspx?DeepLinking=false/000000000001021126
TUV Rheinland of North America. RF Exposure Report: Rex2 Power Meter. Elster Solu-tions, LLC. (2010); 1-3. http://www.naperville.il.us/emplibrary/Smart_Grid/RFexposurereport-RX2EA4.pdf
Wilner D. Wilner & Associates vs. Pacific Gas and Electric Company. Before the Cali-fornia Public Utilities Commission of the State of California. (2011/10/26); 1-19. http://docs.cpuc.ca.gov/published/proceedings/C1110028.htm
Yakymenko I, Sidorik E, Kyrylenko S, Chekhun V. Long-term exposure to microwaveradiation provokes cancer growth: evidences from radars and mobile communica-tion systems. Exp Oncol (2011); 33(2):62-70.
Yip-Kikugawa A. Administrative Law Judge’s Ruling Seeking Clarification. Before the Public Utilities Commission of the State of California. (2011/10/18): 1-4.http://docs.cpuc.ca.gov/EFILE/RULINGS/145652.PDF
SECTION 1 – INTRODUCTION
Page 7
Comments on Notice of Inquiry, ET Docket No. 13-84

Page 8
Comments on Notice of Inquiry, ET Docket No. 13-84

ELECTROHYPERSENSITIVITY“MICROWAVE SICKNESS"
Acute symptoms provoked by microwave radiation were first described byRussian medical researchers in the 1950’s. They described a constellation of symptomsincluding headache, ocular dysfunction, fatigue, dizziness, sleep disorders, dermato-graphism, cardiovascular abnormalities, depression, irritability, and memory impair-ment. (Liakouris, 1998)
In the years between 1953 and 1978 the Russian government harrassed the U.S.Embassy in Moscow by targeting it with radiation from a microwave transmitter.Concern about health effects led to a detailed study by A.M. Lilienfeld, an epidemiolo-gist at Johns Hopkins University. (Lilienfeld AM, 1979)
The abnormalities found in this study were an embarrassment to the U.S.government, since the levels of exposure experienced by embassy staff were in theorder of 2 to 28 microwatts/cm2, a level dramatically below the described U.S. safetystandards for microwave exposure. The conclusions of the study were altered to soft-pedal any abnormal findings. (Goldsmith, 1995b) (Cherry, 2000)
But outside epidemiologic analysis of the Lilienfeld report’s published datashowed that exposed embassy staff experienced a statistically significant excess ofseveral problems, including depression, irritability, difficulty in concentrating, memoryloss, ear problems, skin problems, vascular problems, and other health problems.Symptom incidence increased significantly with accrued years of exposure. (Golds-mith, 1995a) (Cherry, 2000)
THE EMERGENCE OF "ELECTROHYPERSENSITIVITY" AS A DIAGNOSISIn recent years the buildout of cellular communication networks has created a
markedly increased exposure of the public to RF transmissions. Each new generation ofcell phone technology has occupied a higher frequency on the microwave scale, withpotentially increasing impact on body physiology. (Cherry, 2002) As this has occurred,mounting evidence has pointed to the fact that a percentage of the population experi-ences adverse reactions associated with these exposures. The term “electrohypersensiti-vity” (EHS) has been used to describe a constellation of symptoms, including headache,sleep disturbance, difficulty in concentration, memory disturbance, fatigue, depression,irritability, dizziness, malaise, tinnitus, burning and flushed skin, digestive disturbance,tremor, and cardiac irregularities. Sleep disturbance, headache, nervous distress,fatigue, and concentration difficulties are the most commonly described symptoms.(Roosli et al., 2004)
These symptoms are identical to the symptoms of “microwave sickness”described by Russian physicians in the 1950’s.
SYMPTOMS PROVOKED BY TRANSMISSION TOWERSIn 2002, Santini reported significant increases in such symptoms in individuals
living closer than 300 meters to cell towers. (Santini et al., 2002) (Santini R, 2003) In Poland, Bortkiewicz found similar increases in symptoms among residents
near cell towers. Symptoms showed equal association to proximity of the tower,regardless of whether or not the subject suspected such a causal association. (Bortkie-wicz et al., 2004) (Bortkiewicz et al., 2012)
In two studies, Abelin and Altpeter found evidence of disruption of sleep cycle
Page 9
Comments on Notice of Inquiry, ET Docket No. 13-84

and melatonin physiology by RF transmission during the operation and subsequentshutdown of the short wave radio transmitter in Schwarzenburg, Switzerland. (Abelinet al., 2005) (Altpeter et al., 2006)
Figure 1: Percentage of subjects reporting symptoms, stratified by RF exposurelevels as measured in subject’s bedroom. (Hutter et al., 2006)
In a study done in urban and rural sites in Austria, Hutter found a clearly signifi-cant correlation between exposed signal power density and headaches and concentra-tion difficulties—despite the fact that maximum measured power densities were only4.1 mW/m2 (= 0.41 µW/cm2, well below established “safe” limits). (Hutter et al., 2006)
Figure 2: Percentage of subjects reporting symptoms, stratified by proximity tocity’s first cell phone tower. (Abdel-Rassoul et al., 2007)
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 10
Comments on Notice of Inquiry, ET Docket No. 13-84

In Egypt, a study of inhabitants living near the first cell phone tower in the city ofShebeen El-Kom found a significant increase in headaches, memory changes, dizziness,tremors, depressive symptoms, and sleep disturbance, with lower performance on testsof attention and short-term auditory memory. (Abdel-Rassoul et al., 2007)
Research at the military radar installation in Akrotiri, Cyprus, showed that resi-dents of exposed villages had markedly increased incidence of migraine, headache,dizziness, and depression, and significant increases in asthma, heart problems, andother respiratory problems. (Preece et al., 2007)
Studies in Murcia, Spain yielded similar findings, and based on measured expo-sures the authors suggested that safe levels of indoor exposure should not exceed1 µW/m2 (0.0001 µW/cm2) (Navarro et al., 2003) (Oberfeld et al., 2004)
In a study of residents of Selbitz, Bavaria, researchers found statistically signifi-cant increases in multiple health symptoms that demonstrated a dose-response relation-ship with cell phone tower transmissions. Individuals living within 400 meters of thecell phone tower had significantly more symptoms than those living > 400 meters fromthe tower. And individuals living within 200 meters of the tower had significantlyhigher symptoms than those living between 200 and 400 meters from the tower. (Egerand Jahn, 2010)
Two recent reviews provide a detailed overview of research in this area.(Khurana et al., 2010) (Levitt and Lai, 2010)
SYMPTOMS PROVOKED BY CELL PHONE USEMultiple studies of cell phone users in the last decade found evidence of a similar
pattern of symptoms to be provoked in some users. (Chia et al., 2000) (Oftedal et al.,2000) (Santini R, 2002) (Wilen et al., 2003) (Salama and Abou El Naga, 2004) (Al-Khlaiwi and Meo, 2004) (Balikci et al., 2005) (Balik et al., 2005) (Szyjkowska et al.,2005) (Meo and Al-Drees, 2005) (Soderqvist et al., 2008) (Landgrebe et al., 2009)(Hutter et al., 2010)
PHYSIOLOGY OF ELECTROHYPERSENSITIVITYA variety of research models have demonstrated that RF exposure does not have
a uniform effect on people. In many studies, a cohort of individuals has been identifiedthat has a more sensitive response to RF in one way or another.
Reduced heart rate variabilityIn one study, patients with symptoms consistent with EHS were found to have
dereased circadium changes in heart rate variability. (Lyskov et al., 2001) Similarchanges in HRV were found in another study where subjects self-identified as havingEHS symptoms from exposure to video display terminals, TV screens, fluorescentlights, or other electrical equipment. (Sandstrom et al., 2003) An occupational study ofRF plastic sealer workers also found alterations in heart rate compared to normalcontrols.
Fatigue and reduced melatoninIn the more recent Schwarzenberg study, the effect of RF exposure on producing
morning fatigue and reduced melatonin secretion was significantly greater in thesubjects whose general quality of sleep was below the median. (Altpeter et al., 2006)
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 11
Comments on Notice of Inquiry, ET Docket No. 13-84
EEG changesAlterations in EEG have been found in animals and in people with exposure to
both magnetic fields and cell phone transmission frequencies. (Marino et al., 2003)(Marino et al., 2004)
Nanou et al found the EEG response to be gender dependent after exposure bothto 900 MHz and 1800 MHz signals. (Nanou et al., 2005) (Nanou et al., 2009)
Bachman found EEG changes with 450 MHz microwave exposure in 25 to 30% ofhealthy volunteers (Bachmann et al., 2005) (Bachmann et al., 2006). In another study,EEG changes were 5 times as common in depressive subjects as in healthy controls.(Bachmann et al., 2007)
Landgrebe found decreased intracortical excitability in EEG after transcranialmagnetic stimulation in self-identified EHS patients, as compared with normal controls.(Landgrebe et al., 2007)
Schmidt found alteration in sleep EEG after exposure to a 900 MHz RF signalmodulated at two different frequencies, and noted a marked individual variation insensitivity to this effect. (Schmid et al., 2011)
Loughran found alterations in non-REM EEG after cell phone RF exposure.These alterations were consistently stronger in one subset of his study group, overmultiple tests. (Loughran et al., 2012)
Altered Immune FunctionExposure to both GSM and UMTS cellular transmissions at nonthermal exposure
levels have been shown to alter DNA repair mechanisms in lymphocytes. (Markova etal., 2005) (Belyaev et al., 2009) Multiple additional studies have demonstrated non-thermal biological effects of RF radiation on immune cell function, as reviewed here.(Johansson, 2007) (Johansson, 2009b)
One of the most intriguing findings is Johannson’s research showing that pati-ents with electrosensitivity have higher levels of mast cells in their skin, and that thesemast cells migrate closer to the skin surface. (Johansson, 2006) Mast cells are respon-sible for the itching, burning, and skin flushing that occurs after sunburn exposure. Thepresence of higher levels of mast cells in EHS patients provides an explanation for thesymptoms of flushed, itching, and burning skin on the face and other areas that isdescribed by these patients, who appear to be reacting to RF exposure like others mightreact to excessive sun exposure. Since mast cells are distributed throughout the body,the presence of mastocytosis in EHS patients may relate to some other symptoms aswell.
Hormonal ChangesChronic exposures to electromagnetic field effects have also been shown to cause
alterations in secretion of multiple hormones. A study published in 2007 showed thatphysiotherapists working with various electromagnetic treatment modalities had signi-ficantly elevated secretion levels of the stress hormones cortisol, adrenaline, and nor-adrenaline. (Vangelova et al., 2007)
Another study measured urinary secretion of the stress hormones adrenaline andnoradrenaline, along with levels of dopamine and phenylethylamine, prior to and overthe 1 1/2 years following the installation of a GSM cell phone tower in Rimbach,Bavaria. Levels of adrenaline and noradrenaline showed a significant increase over thefirst six months after exposure, and never returned to baseline levels. Responses
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 12
Comments on Notice of Inquiry, ET Docket No. 13-84

showed a proportional relationship to residential exposure levels, and were clearlypresent at levels as low as 60 to 100 microwatts/m2 (= 0.006 to 0.010 μW/cm2). Thissuggested a chronic stress effect of the GSM microwave signal on the population.(Buchner K, 2011)
Chronic adrenal stress will in time lead to decompensation and symptoms ofadrenal fatigue in a certain percentage of the population.
A recently published study evaluated human hormone profiles over six years ofexposure to the microwave RF emissions of GSM cell phones or cell phone towers.Findings included highly significant decreases in ACTH, cortisol, both T4 and T3thyroid hormones. In male subjects, serum testosterone levels gradually decreased withincreased time of exposure. In females, alterations in serum prolactin and progesteronelevels gradually increased over increased time of exposure. (Eskander et al., 2012)
Current ResearchOne of us had the opportunity this spring to visit the practice of Dr. Dominique
Belpomme, Professor of Oncology at Paris Descartes University, who is conductingresearch on electrohypersensitivity with the Association for Research and TreatmentsAgainst Cancer (ARTAC) in Paris. The ARTAC group has been following severalhundred patients with EHS over the last four years, and has documented that thesepatients have clear and consistent changes in oxidative metabolism, and also in bloodflow to the limbic system (as measured by doppler studies). Dr. Belpomme considersthese changes in the limbic system to directly correlate with many of the cognitivechanges (memory problems, difficulty with concentration, etc.) that are experienced bythese patients. The ARTAC group expects to publish a series of papers on their findingsduring the next year. (Dart, 2012)
PROVOCATION STUDIESOver the last ten years, many attempts have been made to evaluate the nature of
electrohypersensitivity through provocation studies. The limitations of these studieshave been discussed in detail in some recent papers. (Loughran et al., 2012) (Regel andAchermann, 2011)
Problems of methodology that have compromised many provocation studiesinclude:
• Many studies have been performed single-blind rather than double-blind.• Many studies divide the study group and normal controls based on the indivi-
dual’s self-identification as having (or not having) electrohypersensitivity.Since it is certainly possible for people to have reactions to EMF without beingaware of this connection, and since the entire population is exposed to EMF atthis point in time, it is difficult to be sure that the “control” group is indeedcomposed of “non-reactors”. This will tend to weaken the power of any studyset up in this fashion.
• Many studies evaluate whether or not the subject can discern when the RFsignal is present and when it is absent. Absence of the ability to make thisjudgement is taken as evidence that electrohypersensitivity does not exist. Thisis an extremely illogical assumption. A person can develop a headache duringor after an RF exposure without knowing when the signal is “on” or “off”, justas they can develop bacterial gastroenteritis without knowing what food wascontaminated with the bacteria. Having symptoms from RF and being a reli-
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 13
Comments on Notice of Inquiry, ET Docket No. 13-84

able RF meter are not the same thing.• Unspecified or inadequate control of background levels of RF/EMF is also a
problem with some “negative” studies. For example, one recent study (Kim etal., 2008) was performed with background RF levels in the study area of of 0.5,0.7, and 0.8 V/m from three different mobile phone service providers. Thisadds up to a reported 2.0 V/m of background RF, equivalent to several thou-sand microwatts/m2, which is well above threshold levels reported to causesymptoms in many sensitive individuals.
• Many studies assume that all patients who complain of EHS will react to anyconstant RF signal, and that they will react to it every time. Yet some studieshave demonstrated that patients vary in which frequencies they respond to, andthat patients can react more strongly to the starting and stopping of a signalthan they do to the presence of a steady signal.
• Furthermore, the assumption is often made that EHS symptoms will start whena signal is turned on, and stop when it turns off. These assumptions are proble-matic, since many patients with EHS report having symptoms that continue fora significant time (hours, in many cases) after a triggering exposure. Fewstudies discuss whether or not an adequate “washout time” was provided forbefore starting the study, or between provocational challenges. The absence ofsuch washout times seriously weakens the power of these studies.
In order to do a reliable RF provocation study with EHS exposure, it is necessaryto isolate the subjects from background RF levels, and to maintain them in this isolationfor long enough that they stop reacting to any prior exposures which they havereceived, before attempting to provoke a new reaction.
Some studies that are designed to address all these methodologic issues havefound clear evidence of electrosensitivity. For example, a study done in 1991 that wasperformed in an isolated EMF environment tested EHS patients with a variety of diffe-rent frequencies of RF stimulus, to determine their individual reactivity spectrum. 100patients who identified themselves as having electrohypersensitivity were tested singleblind with a variety of RF frequencies. 25 of these 100 patients showed an increase insymptoms of 20% over baseline, with no more than one placebo response.
These 25 patients were retested in a double blind setting with 25 healthy controls.16 of the 25 patients (64%) reacted to the positive challenges, which were performed at avariety of frequencies.
These 16 patients reacted to 53% of the 336 active challenges, and 7.5% of the 60blanks. No patient reacted to all tested frequencies. The 25 healthy controls had noreactions to challenges or to blanks.
Finally, these 16 patients were again tested in a double blind setting, each patientchallenged with the single frequency to which they were most sensitive. In this phaseof the study, the patients reacted 100% of the time to the active transmissions (with bothreported symptoms and autonomic changes on iriscorder) and did not report reactionsto the sham transmissions. (Rea et al., 1991)
It must be reiterated that having an adverse reaction to a provoking RF signaland having the ability to determine when the signal is “on” and when it is “off” are twocompletely different things. A recent double blind study demonstrated that a patientcan have consistent provocation of symptoms from a signal without having any clearawareness of when the signal is actually present. (McCarty et al., 2011)
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 14
Comments on Notice of Inquiry, ET Docket No. 13-84

These provocation studies involve short term exposures to the RF signal (typi-cally an hour or less). Since a great deal of the physiology research shows a morepowerful effect with chronic exposures, these short-term studies are probably not themost effective way to assess the clinical significance of reactions to RF.
PREVALENCE OF EHSResearch in Stockholm County, Sweden in 1997 found that 1.5% of the popula-
tion reported being hypersensitive to electrical or magnetic fields. (Hillert et al., 2002)In California in 1998, Levallois et al found that 3.2% of the adult population
reported being sensitive to sources of EMF. (Levallois et al., 2002) In Switzerland in 2004, researchers studying a representative sample of the Swiss
population found that 5% of the population had symptoms attributable to EHS, withsleep disorders and headaches being the most common reported symptoms. (Schreieret al., 2006)
In Austria in 2004, 2% of the population was estimated to have electrohypersen-sitivity. In a survey performed in Austria in 2008, 29.3% of respondents reportedhaving some sort of adverse response to electromagnetic pollution. Of this cohort, 2.1%reported intense disturbance, and 3.5% had experienced enough difficulty that they hadconsulted a physician about the problem. (Schrottner and Leitgeb, 2008)
Figure 3: The prevalence of electrohypersensitivity syndrome is increasing.(Hallberg and Oberfeld, 2006
In much of the world, exposure to microwave radio signals has continued tosignificantly increase since the early 1990’s. Reported electrosensitivity also appears tobe increasing over time. In 2006, Halberg and Oberfeld reviewed research on thissubject from 1985 forward, and estimated that if the trend in increased prevalence conti-nues, fifty percent of the population could be reporting adverse effects from EMF by theyear 2017 (Figure 1). (Hallberg and Oberfeld, 2006)
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 15
Comments on Notice of Inquiry, ET Docket No. 13-84

GOVERNMENTAL RESPONSEThe various forms of research described above have provided strong support for
the fact that RF/EMF exposures can produce symptoms in human beings and that thereis a percentage of the population that is more sensitive to this effect. Continuedresearch is suggesting that this is not a static situation—that the prevalence of electro-hypersensitivity is a growing over time.
By the middle of the last decade, various government agencies were attemptingto define the scope of the problem. (Irvine, 2005)
The rollout of mobile phone technology occurred earlier in scandinavia than inother places in the world, and governmental recognition of EHS as a health problemoccurred earlier there than in other places. By the year 2000, EHS was recognized as adisability by the Swedish government. (Ministers, 2000)
In Stockholm, individuals with EHS can receive municipal support to reduce thepresence of and penetration of EMF/RF into their homes. The construction of a villagewith houses specifically designed to mitigate this problem is being considered. Patientswith EHS have the legal right to receive mitigations in their workplace, and some hospi-tals have build low EMF hospital rooms for use by such patients. (Johansson, 2006)
Various government reports or reviews on the question of electrohypersensiti-vity have been commissioned in the last few years. (Aringer et al., 1997) (Irvine, 2005)And legislation to address the problem has been proposed in some countries. (Snoy,2011) (Parliamentary Assembly, 2011) Many libraries and schools in europe havebanned WiFi due to concerns about health effects on employees and on the public.
REGULATORY RESPONSERegulations on exposure limits vary dramatically from country to country. In
general, exposure limits have been mandated at a lower level in Russia and easternEurope, where research on the health effects of RF exposure has been performed for alonger period of time. (Repacholi et al., 2012)
The regulatory standards established by the FCC and the World Health Organi-zation are based on defining safe levels against the thermal effects of RF (i.e. damagefrom being cooked by high levels of microwave exposure). The FCC has not establishedexposure standards for potential nonthermal or biological effects of microwave expo-sure. (Hankin, 2002)
For example, the FCC has established Limits for Maximum Permissible Exposure(MPE). For the general population, the permissible level of exposure at 900 MHz is 600μW/cm2, and at 1800 MHz is 1000 μW/cm2. (FCC, 1999) These exposure levels werelast updated in 1996, and are considered to be protective against thermal effects ofmicrowave radiation. However, current scientific research shows that these permissiblelevles of exposure are hundreds of times higher than the threshold levels for adverse“nonthermal” biological effects.
For the past ten years, the WHO has consistently equivocated on the issue ofrecognizing nonthermal biological effects from microwave RF exposure, despite themounting research evidence of health problems and health risks produced by currentlevels of public exposure.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 16
Comments on Notice of Inquiry, ET Docket No. 13-84
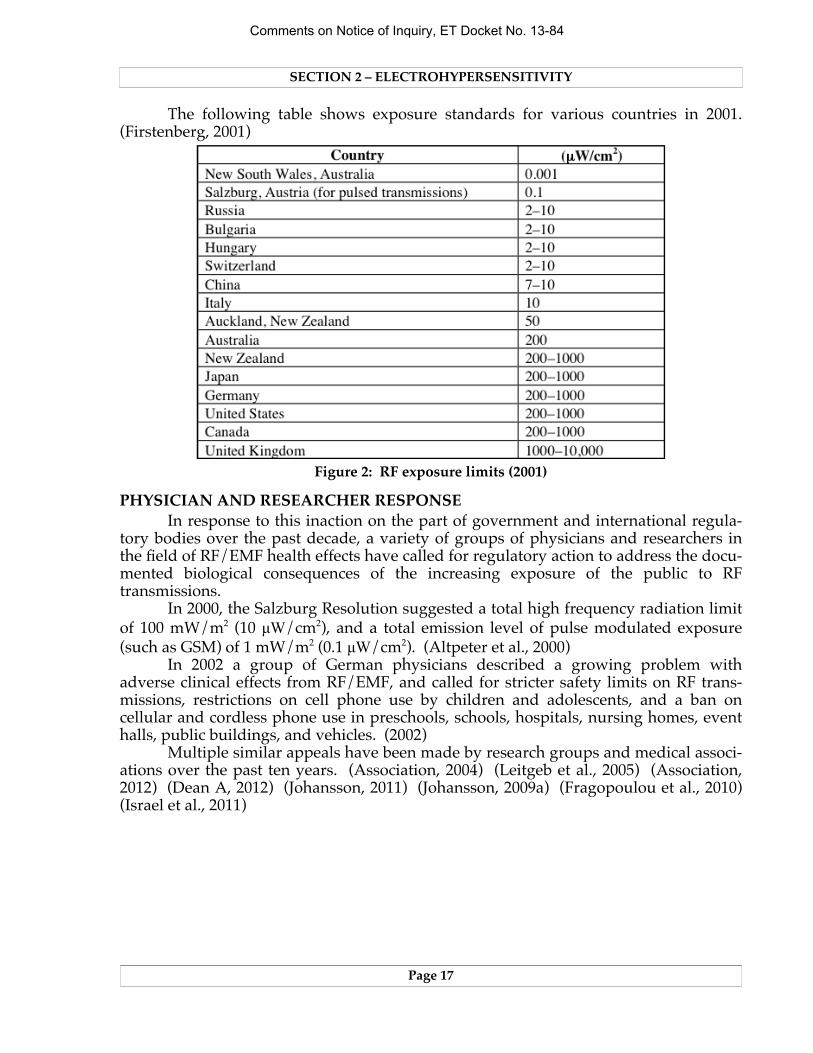
The following table shows exposure standards for various countries in 2001.(Firstenberg, 2001)
Figure 2: RF exposure limits (2001)
PHYSICIAN AND RESEARCHER RESPONSEIn response to this inaction on the part of government and international regula-
tory bodies over the past decade, a variety of groups of physicians and researchers inthe field of RF/EMF health effects have called for regulatory action to address the docu-mented biological consequences of the increasing exposure of the public to RFtransmissions.
In 2000, the Salzburg Resolution suggested a total high frequency radiation limitof 100 mW/m2 (10 µW/cm2), and a total emission level of pulse modulated exposure(such as GSM) of 1 mW/m2 (0.1 µW/cm2). (Altpeter et al., 2000)
In 2002 a group of German physicians described a growing problem withadverse clinical effects from RF/EMF, and called for stricter safety limits on RF trans-missions, restrictions on cell phone use by children and adolescents, and a ban oncellular and cordless phone use in preschools, schools, hospitals, nursing homes, eventhalls, public buildings, and vehicles. (2002)
Multiple similar appeals have been made by research groups and medical associ-ations over the past ten years. (Association, 2004) (Leitgeb et al., 2005) (Association,2012) (Dean A, 2012) (Johansson, 2011) (Johansson, 2009a) (Fragopoulou et al., 2010)(Israel et al., 2011)
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 17
Comments on Notice of Inquiry, ET Docket No. 13-84

BIBLIOGRAPHY
Abdel-Rassoul G, El-Fateh OA, Salem MA et al. Neurobehavioral effects among inhabi-tants around mobile phone base stations. Neurotoxicology (2007); 28(2):434-440.
Abelin T, Altpeter E, Roosli M. Sleep Disturbances in the Vicinity of the Short-WaveBroadcast Transmitter Schwarzenburg. Somnologie (2005); 9:203-209.
Al-Khlaiwi T, Meo SA. Association of mobile phone radiation with fatigue, headache,dizziness, tension and sleep disturbance in Saudi population. Saudi Med J (2004);25(6):732-736.
Altpeter E, Blackman C, Cherry N et al. Salzburg Resolution. International Conferenceon Cell Tower Siting. Salzburg (2000): 1-2. http://www.iemfa.org/images/pdf/Salz-burg_Resolution.pdf
Altpeter ES, Roosli M, Battaglia M, Pfluger D, Minder CE, Abelin T. Effect of short-wave(6-22 MHz) magnetic fields on sleep quality and melatonin cycle in humans: theSchwarzenburg shut-down study. Bioelectromagnetics (2006); 27(2):142-150.
Aringer L, Cunningham J, Gobba F et al. Possible health implications of subjectivesymptoms and electromagnetic fields. European Commission DG-V 1997:18. Bergq-vist U, Vogel E, eds. 1997: 1-125. https://gupea.ub.gu.se/dspace/bitstream/2077/4156/1/ah1997_19.pdf
Guideline of the Austrian Medical Association for the diagnosis and treatment of EMFrelated health problems and illnesses (EMF syndrome). Austrian Medical Asso-ciation (2012); http://www.magdahavas.com/wordpress/wp-content/uploads/2012/06/Austrian-EMF-Guidelines-2012.pdf
Bachmann M, Kalda J, Lass J, Tuulik V, Sakki M, Hinrikus H. Non-linear analysis of theelectroencephalogram for detecting effects of low-level electromagnetic fields. MedBiol Eng Comput (2005); 43(1):142-149.
Bachmann M, Lass J, Kalda J et al. Integration of differences in EEG analysis revealschanges in human EEG caused by microwave. Conf Proc IEEE Eng Med Biol Soc(2006); 1:1597-1600.
Bachmann M, Hinrikus H, Aadamsoo K et al. Modulated microwave effects on indivi-duals with depressive disorder. Environmentalist (2007); 27(4):505-510.
Balik HH, Turgut-Balik D, Balikci K, Ozcan IC. Some ocular symptoms and sensationsexperienced by long term users of mobile phones. Pathol Biol (Paris) (2005);53(2):88-91.
Balikci K, Cem Ozcan I, Turgut-Balik D, Balik HH. A survey study on some neurolo-gical symptoms and sensations experienced by long term users of mobile phones.Pathol Biol (Paris) (2005); 53(1):30-34.
Belyaev IY, Markova E, Hillert L, Malmgren LO, Persson BR. Microwaves from UMTS/GSM mobile phones induce long-lasting inhibition of 53BP1/gamma-H2AX DNArepair foci in human lymphocytes. Bioelectromagnetics (2009); 30(2):129-141.
Bortkiewicz A, Gadzicka E, Szyjkowska A et al. Subjective complaints of people livingnear mobile phone base stations in Poland. Int J Occup Med Environ Health (2012);25(1):31-40.
Bortkiewicz A, Zmyslony M, Szyjkowska A, Gadzicka E. [Subjective symptomsreported by people living in the vicinity of cellular phone base stations: review].Med Pr (2004); 55(4):345-351.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 18
Comments on Notice of Inquiry, ET Docket No. 13-84

Buchner K EH. Changes of Clinically Important Neurotransmitters under the Influenceof Modulated RF Fields--A Long-term Study under Real-life Conditions. Umwelt-Medizin-Gesellschaft (2011); 24(1):44-57.
Cherry N. Evidence of Health Effects of Electromagnetic Radiation, To the AustralianSenate Inquiry into Electromagnetic Radiation (2000): 1-84. http://www.neil-cherry.com/documents 90_m1_EMR_Australian_Senate_Evidence_8-9-2000.pdf
Cherry N. EMR Spectrum Principle (2002): 1-11. http://www.neilcherry.com/documents/90_p3_EMR_Spectrum_Principle_paper.pdf
Chia SE, Chia HP, Tan JS. Prevalence of headache among handheld cellular telephoneusers in Singapore: a community study. Environ Health Perspect (2000);108(11):1059-1062.
Dean A, Rea W, Smith C, Barrier A. American Academy of Environmental MedicinePosition Paper on Electromagnetic and Radiofrequency Fields Effect on HumanHealth (2012); http://aaemonline.org/emfpositionstatement.pdf
Eger H, Jahn M. Specific Health Symptoms and Cell Phone Radiation in Selbitz(Bavaria, Germany) -- Evidence of a Dose-Response Relationship. umwelt-medizin-gesellschaft (2010); 23:1-20.
Eskander EF, Estefan SF, Abd-Rabou AA. How does long term exposure to base stationsand mobile phones affect human hormone profiles? Clin Biochem (2012);45(1-2):157-161.
FCC. Questions and Answers about Biological Effects and Potential Hazards of Radio-frequency Electromagnetic Fields. ed. Federal Communications Commission,Office of Engineering and Technology (1999): 1-38.
Firstenberg A. Radio Wave Packet. Cellular Phone Task Force (2001): 1-8.http:/www.goodhealthinfo.net/radiation/radio_wave_packet.pdf
Fragopoulou A, Grigoriev Y, Johansson O et al. Scientific panel on electromagnetic fieldhealth risks: consensus points, recommendations, and rationales. Rev EnvironHealth (2010); 25(4):307-317.
Goldsmith JR. Epidemiologic Evidence of Radiofrequency Radiation (Microwave)Effects on Health in Military, Broadcasting, and Occupational Studies. Int J OccupEnviron Health (1995a); 1(1):47-57.
Goldsmith JR. Where the trail leads. Ethical problems arising when the trail of professi-onal work leads to evidence of a cover-up of serious risk and mis-representation ofscientific judgemnt concerning human exposures to radar. Eubios Journal of Asianand International Bioethics (1995b); 5(4):92-94.
Hallberg O, Oberfeld G. Letter to the editor: will we all become electrosensitive? Electro-magn Biol Med (2006); 25(3): 189-191.
Hankin N (Center for Science and Risk Assessment, Radiation Protection Division,United States Environmental Protection Agency) To Ms. Jane Newton, President,The EMR Network (2002): 1-3
Hillert L, Berglind N, Arnetz BB, Bellander T. Prevalence of self-reported hypersensiti-vity to electric or magnetic fields in a population-based questionnaire survey.Scand J Work Environ Health (2002); 28(1):33-41.
Hutter HP, Moshammer H, Wallner P et al. Tinnitus and mobile phone use. OccupEnviron Med (2010); 67(12):804-808.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 19
Comments on Notice of Inquiry, ET Docket No. 13-84

Hutter HP, Moshammer H, Wallner P, Kundi M. Subjective symptoms, sleepingproblems, and cognitive performance in subjects living near mobile phone basestations. Occup Environ Med (2006); 63(5):307-313.
Irish Doctors Environmental Association. IDEA Position on Elecro-Magnetic Radiation.(2004); http://www.ideaireland.org/emr.htm
Interdisziplinare Gesellschaft fur Umweltmedizin e.V. Freiburger Appeal. (2002);http://web.archive.org/web/20070930041008/http://www.emrnetwork.org/news/IGUMED_english.pdf
Irvine N. Definition, Epidemiology and Management of Electrical Sensitivity. Report for the Health Protection Agency Centre for Radiation, Chemical and Environmental Hazards,Radiation Protection Division, Chilton, Didcot, Oxfordshire, United Kingdom (2005); HPA-RPD-010: 1-42. http://www.hpa.org.uk/web/HPAwebFile/HPAweb_C/1194947416613
Israel M, Ivanova M, Zaryabova V. Criticism of the philosophy for development of stan-dards for non-ionizing radiation. Environmentalist (2011); 31(2):121-129.
Johansson O. Electrohypersensitivity: state-of-the-art of a functional impairment. Elec-tromagn Biol Med (2006); 25(4):245-258.
Johansson O. Evidence for Effects on the Immune System. Bioinitiative Report (2007);Section 8:186-224. http://www.bioinitiative.org/
Johansson O. The London Resolution. Pathophysiology (2009a); 16(2-3):247-248.Johansson O. Disturbance of the immune system by electromagnetic fields-A potentially
underlying cause for cellular damage and tissue repair reduction which could leadto disease and impairment. Pathophysiology (2009b); 16(2-3):157-177.
Johansson O. Letter to California Public Utilities Commission (CPUC) re Smart Meters(2011).
Khurana VG, Hardell L, Everaert J, Bortkiewicz A, Carlberg M, Ahonen M. Epidemiolo-gical evidence for a health risk from mobile phone base stations. Int J OccupEnviron Health (2010); 16(3):263-267.
Kim DW, Lee JH, Ji HC, Kim SC, Nam KC, Cha EJ. Physiological effects of RF exposureon hypersensitive people by a cell phone. Conf Proc IEEE Eng Med Biol Soc(2008):2322-2325.
Landgrebe M, Frick U, Hauser S, Hajak G, Langguth B. Association of tinnitus and elec-tromagnetic hypersensitivity: hints for a shared pathophysiology? PLoS One (2009);4(3):e5026 (1-6).
Landgrebe M, Hauser S, Langguth B, Frick U, Hajak G, Eichhammer P. Altered corticalexcitability in subjectively electrosensitive patients: results of a pilot study. J Psy-chosom Res (2007); 62(3):283-288.
Leitgeb N, Schrottner J, Bohm M. Does “electromagnetic pollution” cause illness? Aninquiry among Austrian general practitioners. Wien Med Wochenschr (2005);155(9-10):237-241.
Levallois P, Neutra R, Lee G, Hristova L. Study of self-reported hypersensitivity to elec-tromagnetic fields in California. Environ Health Perspect (2002); 110(Suppl4):619-623.
Levitt B, Lai H. Biological effects from exposure to electromagnetic radiation emitted bycell tower base stations and other antenna arrays. Environ Rev (2010); 18:369-395.
Liakouris AG. Radiofrequency (RF) Sickness in the Lilienfeld Study: An Effect of Modu-lated Microwaves? Archives of Environmental Health (1998); 53(3):236-238.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 20
Comments on Notice of Inquiry, ET Docket No. 13-84

Lilienfeld AM LGM, Cauthen J, Tonascia S, Tonascia J. Evaluation of health status offoreign service and other employees from selected eastern European embassies.Foreign Service Health Status Study, Final Report; Contract No. 6025-619037 (NTISpublication P8-288 163/9) (1979); 1-447.
Loughran SP, McKenzie RJ, Jackson ML, Howard ME, Croft RJ. Individual differencesin the effects of mobile phone exposure on human sleep: Rethinking the problem.Bioelectromagnetics (2012); 33(1):86-93.
Lyskov E, Sandstrom M, Hansson Mild K. Neurophysiological study of patients withperceived ‘electrical hypersensitivity’. Int J Psychophysiol (2001); 42(3):233-241.
Marino AA, Nilsen E, Chesson ALJ, Frilot C. Effect of low-frequency magnetic fields onbrain electrical activity in human subjects. Clin Neurophysiol (2004);115(5):1195-1201.
Marino AA, Nilsen E, Frilot C. Nonlinear changes in brain electrical activity due to cellphone radiation. Bioelectromagnetics (2003); 24(5):339-346.
Markova E, Hillert L, Malmgren L, Persson BR, Belyaev IY. Microwaves from GSMmobile telephones affect 53BP1 and gamma-H2AX foci in human lymphocytesfrom hypersensitive and healthy persons. Environ Health Perspect (2005);113(9):1172-1177.
McCarty DE, Carrubba S, Chesson AL, Frilot C, Gonzalez-Toledo E, Marino AA. Elec-tromagnetic Hypersensitivity: Evidence for a Novel Neurological Syndrome. Int JNeurosci (2011); 670-676.
Meo SA, Al-Drees AM. Mobile phone related-hazards and subjective hearing and visionsymptoms in the Saudi population. Int J Occup Med Environ Health (2005);18(1):53-57.
Nanou E, Hountala C, Maganioti A et al. Influence of a 1,800 MHz electromagnetic fieldon the EEG energy. Environmentalist (2009); 29(2):205-209.
Nanou E, Tsiafakis V, Kapareliotis E. Influence of the Interaction of a 900 MHz Signalwith Gender on EEG Energy: Experimental Study on the Influence of 900 MHzRadiation on EEG. Environmentalist (2005); 25:173-179.
Navarro E, Segura J, Portolés M, Gómez-Perretta C. The Microwave Syndrome: A Preli-minary Study in Spain. Electromagn Biol Med (2003); 22(2-3):161-169.
Nordic Council of Ministers. The Nordic Adaptation of Classification of Occupationally Related Disorders (Diseases and Symptoms) to ICD-10 (2000). http://www.norden.org/en/publications/publikationer/2000-839
Oberfeld G, Navarro E, Portoles M, Maestu C, Gomez-Perretta C. The Microwave Syn- drome -- Further Aspects of a Spanish Study. (2004):1-8.http://www.powerwatch.org.uk/pdfs/20040809_kos.pdf
Oftedal G, Wilen J, Sandstrom M, Mild KH. Symptoms experienced in connection withmobile phone use. Occup Med (Lond) (2000); 50(4):237-245.
Parliamentary Assembly, Council of Europe. Resolution 1815: The potential dangers ofelectromagnetic fields and their effect on the environment. (2011):1-4.http://www.cellphonetaskforce.org/wp-content/uploads/2012/01/eres1815.pdf
Preece AW, Georgiou AG, Dunn EJ, Farrow SC. Health response of two communities tomilitary antennae in Cyprus. Occup Environ Med (2007); 64(6):402-408.
Rea WJ, Pan Y, Fenyves EJ et al. Electromagnetic-Field Sensitivity. Journal of Bioelectricity(1991); 10(1-2):241-256.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 21
Comments on Notice of Inquiry, ET Docket No. 13-84

Regel SJ, Achermann P. Cognitive performance measures in bioelectromagneticresearch--critical evaluation and recommendations. Environ Health (2011); 10(1):10.
Repacholi M, Grigoriev Y, Buschmann J, Pioli C. Scientific basis for the Soviet andRussian radiofrequency standards for the general public. Bioelectromagnetics (2012);33(8):623-633.
Roosli M, Moser M, Baldinini Y, Meier M, Braun-Fahrlander C. Symptoms of ill healthascribed to electromagnetic field exposure--a questionnaire survey. Int J HygEnviron Health (2004); 207(2):141-150.
Salama OE, Abou El Naga RM. Cellular phones: are they detrimental? J Egypt PublicHealth Assoc (2004); 79(3-4):197-223.
Sandstrom M, Lyskov E, Hornsten R et al. Holter ECG monitoring in patients withperceived electrical hypersensitivity. Int J Psychophysiol (2003); 49(3):227-235.
Santini R SP, Le Ruz P, Danze J, Seigne M. Survey Study of People Living in the Vicinityof Cellular Phone Base Stations. Electromagnetic Biology and Medicine (2003);22(1):41-49.
Santini R SM, Bonhomme-Faivre L, Fouffet/Elsa Defrasne S, Sage M. Symptoms Experi-enced by Users of Digital Cellular Phones: A Study of a French EngineeringSchool. Electromagnetic Biology and Medicine (2002); 21(1):81-88.
Santini R, Santini P, Danze JM, Le Ruz P, Seigne M. [Investigation on the health ofpeople living near mobile telephone relay stations: I/Incidence according todistance and sex]. Pathol Biol (Paris) (2002); 50(6):369-373.
Schmid MR, Loughran SP, Regel SJ et al. Sleep EEG alterations: effects of differentpulse-modulated radio frequency electromagnetic fields. J Sleep Res (2011); (Apr12):1-9.
Schreier N, Huss A, Roosli M. The prevalence of symptoms attributed to electromag-netic field exposure: a cross-sectional representative survey in Switzerland. SozPraventivmed (2006); 51(4):202-209.
Schrottner J, Leitgeb N. Sensitivity to electricity--temporal changes in Austria. BMCPublic Health (2008); 8:310-316.
Snoy T. Visant à faire reconnaître les patients atteints d’électro-hypersensibilité.Chambre des Representats de Belgique. (2011): 1-8.http://www.next-up.org/pdf/Proposition_de_Resolu-tion_Therese_Snoy_Visant_a_faire_reconnaitre_les_patients_atteints_d_electro_hypersen-sibilite_Chambre_des_Repesentants_Belgique_20_07_2011.pdf
Soderqvist F, Carlberg M, Hardell L. Use of wireless telephones and self-reported healthsymptoms: a population-based study among Swedish adolescents aged 15-19years. Environ Health (2008); 7:18. http://www.ehjournal.net/content/7/1/18
Szyjkowska A, Bortkiewicz A, Szymczak W, Makowiec-Dabrowska T. [Subjectivesymptoms related to mobile phone use--a pilot study]. Pol Merkur Lekarski (2005);19(112):529-532.
Vangelova K, Israel M, Velkova D, Ivanova M. Changes in excretion rates of stresshormones in medical staff exposed to electromagnetic radiation. Environmentalist(2007); 27(4):551-555.
Wilen J, Sandstrom M, Hansson Mild K. Subjective symptoms among mobile phoneusers--a consequence of absorption of radiofrequency fields? Bioelectromagnetics(2003); 24(3):152-159.
SECTION 2 – ELECTROHYPERSENSITIVITY
Page 22
Comments on Notice of Inquiry, ET Docket No. 13-84

RADIOFREQUENCY EFFECTS ON MELATONINTHE FUNCTION OF MELATONIN
Many physiologic functions in the human body are entrained in a circadiumrhythm, fluctuating through the day/night cycle. The hormone melatonin, secreted bythe pineal gland, is a key agent in coordinating these physiologic responses throughoutthe body. (Zawilska et al., 2009)
The entrainment of melatonin secretion with the day/night cycle is maintainedby the suprachiasmatic nucleus in the hypothalamus, which receives input on thepresence of light from the retina via the retinohypothalamic tract. In the presence ofambient light, melatonin secretion is suppressed. In the absence of ambient light, mela-tonin secretion increases. So melatonin secretion is high during the nighttime hours,peaking shortly after midnight. Higher melatonin levels are part of what makes us feel“sleepy” at night. Exposure to light during the nighttime hours will lead to a rapidsuppression of melatonin secretion by the pineal gland, and this can cause disruption ofsleep and derangement of the circadium rhythm.
Since the length of the day varies seasonally, melatonin also provides our physio-logy with information and influence produced by the different seasons of the year. Thisseasonal influence was obviously more profound prior to the widespread introductionof artificial electric lighting.
The circadian rhythm of high nocturnal melatonin levels supports the naturalfunction of sleep, and disruption of this rhythm by bright light at night, night shiftwork, or travel to different time zones can produce sleep disturbances.
Melatonin is one of the most potent antioxidant molecules in the human body,and acts to reduce reactive oxidative processes in the body. Melatonin can quench thedamaging free radical activity produced by inflammation. The presence of elevatedmelatonin at night is therefore a key factor in the healing and rejuvenating functionsthat we associate with “a good night’s sleep”.
Many body processes (serum cortisol levels, body temperature, patterns of diges-tive function, etc.) have a circadian rhythm that is coordinated by the timing signal ofmelatonin secretion. Melatonin has a protective effect on the health of the gastrointes-tinal tract. Melatonin is also protective against the growth of cancer cells, and disrup-tion of the circadian melatonin cycle has been shown to lead to increased tumor growthin a variety of cancer types. (Reiter et al., 2011)
Research has clearly demonstrated that melatonin inhibits the proliferation, inva-siveness, and metastasis of human breast cancer cells. Women who have lower levels ofnocturnal melatonin are at greater risk for developing breast cancer. (Schernhammer etal., 2008) (Schernhammer and Hankinson, 2009) Breast cancer is more common inindustrialized societies, and geographically the incidence of breast cancer is stronglyassociated with higher levels of “light-at-night”. (Kloog et al., 2008) (Kloog et al., 2010)
Current research suggests that disruption of nocturnal melatonin signals by“light at night” can promote both the development and the growth of breast cancer.(Hill et al., 2011) (Stevens, 2009) In 2007 the International Agency for Research onCancer declared night shift work to be a probable carcinogen. Subsequent epidemio-logic research continues to support this finding. (Bonde et al., 2012)
Recent research has also suggested similar associations between “light at night”and the incidence of prostate cancer. (Kloog et al., 2009)
Page 23
Comments on Notice of Inquiry, ET Docket No. 13-84

ELECTROMAGNETIC AND RADIOFREQUENCY EXPOSURES CAN REDUCE MELATONIN PRODUCTION IN THE PINEAL GLAND
In the 1990’s, the Swiss government conducted a series of studies of sleep qualitynear the Swiss national short wave radio transmission tower in Schwarzenburg. Thesestudies were initiated after the government received a petition stating that many resi-dents living near the transmitter were experiencing problems including nervousness,headache, sleep disturbance, and fatigue.
!O/2:()!PS!G%:1*!E1)).!T/7*:(<#$3)!8/*+!>O!)6.'7:()!#*!E3+8#(F)$<:(2;!E8/*F)(1#$%;!Figure 1: Sleep Disturbance by Proximity Zone in the Schwarzenburg Study.
(Cherry, 2002)
!#$%&'(! )*! +,-(.'(-/,0-(! '(123$,0-4$/! 5,'! 61((/!+$-3&'7208(! 23! 68492':(07&'%!9$34!Figure 2: Sleep Disturbance by Exposure Levels in the Schwarzenburg Study.
(Cherry, 2002)In these studies, a statistically significant increase in sleep disturbance was found
in residents living closer to the towers. Difficulty in maintaining sleep correlated withtransmission field strength, at exposure levels as low as 0.1 nanowatts/cm2. (Cherry,2002) (Abelin et al., 2005)
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 24
Comments on Notice of Inquiry, ET Docket No. 13-84

!#$%&'(! "*! 61((/! I$-3&'7208(! $0! /(,/1(! (;/,-(I! 3,! 2! -4,'3.92L(! '2I$,! -323$,0-!94$84!Figure 3: Reduction in Sleep Disturbance with Interruption of Tower Transmis-
sion in the Schwarzenburg Study. (Cherry, 2002)During an interval when the transmitter was turned off for three days, statisti-
cally significant reductions in sleep disturbance were found in both the high and thelow exposure groups (Figure 3). Note that Group C showed a reduction in sleep distur-bance with absence of the signal, despite the fact that signal strength in Zone Caveraged only 0.0004 μW/cm2 (4 μW/m2).
The Schwarzenburg transmission tower was shut down permanently in 1998. Ina final research project, sleep quality and salivary melatonin levels were measured in agroup of 54 community residents for an interval before and after the end of radiotransmission.
Baseline sleep quality was assessed by analysis of sleep diary records, andsubjects were stratified into two groups classified as either “poor” or “good” sleepers.Salivary melatonin samples were collected before breakfast, lunch, tea, dinner, andbefore bed. Subjects recorded morning tiredness and sleep quality, time of fallingasleep, and duration of sleep. Exposure levels were calculated for each subjects home.
During the baseline exposure period, scores of morning tiredness directly corre-lated with increased levels of exposure, and melatonin excretion levels were reduced bya factor of 0.90 for each mA/m of increase magnetic field exposure level. Peak mela-tonin excretion times were delayed by 4.4 minutes for every 1 mA/m increase in expo-sure level.
After shutdown of the transmitter, subjects’ morning fatigue scores improved by1.74 units for each 1 mA/m of reduced exposure, and melatonin excretion levelsincreased by a factor of 1.15 per mA/m of reduced exposure. (Altpeter et al., 2006)
The Schwarzenburg shutdown study’s findings were remarkable for two additi-onal reasons. First, there were no other significant levels of short wave radio exposurein the community at the time of the study. So this study provides a true eliminationand challenge test of RF exposure effects on a fairly large group of people in theirnormal environment. Such a study setting was difficult to arrange at that time, and
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 25
Comments on Notice of Inquiry, ET Docket No. 13-84

would be even more difficult to achieve today, as the number of sources of RF exposurein our communities have increased markedly with the rollout of the wireless telecom-munications infrastructure.
Second, the stratification of the study group into “poor” and “good” sleepersallowed recognition of an important additional finding. Improvements in sleep qualityand melatonin secretion levels after transmitter shutdown were significantly greater in“poor” sleepers than they were in “good” sleepers. This evidence supports the hypo-thesis that some individuals may be more sensitive to the effects of microwave expo-sure, a condition that has been called “electrohypersensitivity” or EHS.
Multiple additional studies in a variety of settings have demonstrated an effect ofvarious forms of EMF/RF on melatonin physiology. Several comprehensive reviews ofthis research have been published in the last few years. (Cherry, 2002) (Davinipour andSobel, 2007) (Davanipour and Sobel, 2009)
Performing large long-term studies of RF effects on humans in a sleep laboratorysetting would be prohibitively difficult both logistically and financially. But severalrecent laboratory studies in animals have demonstrated suppression of melatonin byprolonged pulsed microwave RF exposures.
Kesari et al. exposed Wistar rats to 2.45 GHz mobile phone transmissions, 2hours daily for 45 days, at a calculated SAR of 0.9 W/Kg. Pineal melatonin levels weresignificantly reduced in exposed animals. (Kesari et al., 2011)
Kumar et al. repeated this experiment with 2.5 GHz exposures of 2 hours per dayfor 60 days, at a much lower exposure level (power density of 0.21 mW/cm2, calculatedSAR of 0.014 W/kg). Even at this low level of exposure (= 210 mW/cm2), serum mela-tonin levels were significantly reduced in exposed animals. (Kumar et al., 2011)
Figure 4: Serum melatonin levels in sham (black) and exposed (grey) Wistar ratsafter 2 hours daily exposure for 60 days to 2.45 GHz RF transmission at 0.21
milliwatts/cm2. (from Kumar et al., 2011)In another study, Kesari found significant reduction in pineal melatonin levels in
rats exposed to 2.45 GHz mobile phone transmissions, 2 hours daily for 45 days, at apower density of 0.21 mW/cm2 (calculated SAR of 0.014 W/kg). (Kesari et al., 2012)
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 26
Comments on Notice of Inquiry, ET Docket No. 13-84

CONSEQUENCES OF REDUCTION OF MELATONIN LEVELS BY MICROWAVE RF EXPOSURE
Reduction of melatonin levels by exposure to radio transmissions could beexpected to cause sleep disturbance. Research findings like the Schwarzenburg studiesstrongly support this conclusion.
But melatonin has also been found to be protective against promotion of sometypes of cancer. If suppression of melatonin by “light at night” and night shift work canincrease risk of breast cancer (as discussed above), then suppression of melatonin byradio transmissions could also be expected to increase cancer risk. Recently publishedresearch studies strongly support this conclusion.
A study in Israel found women living within 350 meters of a cell phone tower tohave over 10 times greater risk of cancer than the community as a whole (p < 0.0001).(Wolf and Wolf, 2004)
A study of cancer patients in Germany found a 3.29 times greater risk of cancer(p < 0.01) in patients with residence closer than 400 meters to a cell pone tower. Risk ofbreast cancer was 3.4 times greater, and average age of diagnosis of breast cancer was19 years earlier. (Eger et al., 2004)
In a case/control study of cancer patients residing near a cell phone transmissiontower in Austria, those with external residential exposures of greater than 1000 μW/m2
(> 0.1 μW/cm2) had a a breast cancer risk that was 23 times higher (p = 0.0007) andbrain tumor risk was 121 times higher (p = 0.001) than controls. (Oberfeld, 2008)
A recent study from Brazil found a clearly elevated relative risk of cancer mor-tality at residential distances of 500 meters or less from cell phone transmission towers.(Dode et al., 2011)
Several recent published reviews discuss the multiple epidemiologic studies thathave shown an association between residential RF exposure from microwave transmis-sion towers and increased breast cancer risk. (Cherry, 2005) (Khurana et al., 2010)(Levitt and Lai, 2010) (Yakymenko et al., 2011) We will discuss this issue morethoroughly in Section 3.
RAISING THE LEVEL OF RADIOFREQUENCY TRANSMISSION IN RESIDENTIAL NEIGHBORHOODS CARRIES SIGNIFICANT RISKS
Unlike visible light, microwave radio transmissions penetrate walls and humanbodies. They are not easily blocked out by window blinds or eye shades. If microwaveradio waves can disrupt melatonin secretion in a portion of the population, then a signi-ficant increase in nocturnal RF transmission levels in a residential neighborhood wouldbe expected to produce an increase in sleep problems, and over the long run, anincrease in the incidence of breast and prostate cancer. The first evidence of such aneffect would be a significant increase in complaints of sleep disruption. It might requireseveral years of exposure for the increase in cancer incidence to reveal itself.
If we use complaints of sleep disruption as a marker for this effect, we cansuspect that the recent installation of MESH-networking smart meters in California andin other municipalities around the world has pushed many residential areas across athreshold, producing chronodysruption in a significantly increased portion of the popu-lation. The early evidence for this is that these smart meter rollouts have been followedby a dramatic increase in complaints of sleep difficulties received by physicians, bypublic utility commissions, and in postings on the internet.
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 27
Comments on Notice of Inquiry, ET Docket No. 13-84

BIBLIOGRAPHY
Abelin T, Altpeter E, Roosli M. Sleep Disturbances in the Vicinity of the Short-WaveBroadcast Transmitter Schwarzenburg. Somnologie (2005); 9:203-209.
Altpeter ES, Roosli M, Battaglia M, Pfluger D, Minder CE, Abelin T. Effect of short-wave(6-22 MHz) magnetic fields on sleep quality and melatonin cycle in humans: theSchwarzenburg shut-down study. Bioelectromagnetics (2006); 27(2):142-150.
Bonde JP, Hansen J, Kolstad HA et al. Work at night and breast cancer - report onevidence-based options for preventive actions. Scand J Work Environ Health (2012);online first. doi:10.5271/sjweh.3282:1-11.
Cherry N. EMF/EMR Reduces Melatonin in Animals and People. (2002):1-14.http://www.neilcherry.com/documents.php
Cherry N. Electromagnetic Radiation causes cancer: the implications for breast cancer.(2005):1-39. http://www.neilcherry.com/documents.php
Davanipour Z, Sobel E. Long-term exposure to magnetic fields and the risks ofAlzheimer’s disease and breast cancer: Further biological research. Pathophysiology(2009); 16(2-3):149-156.
Davinipour Z, Sobel E. Magnetic Field Exposure: Melatonin Production; Alzheimer’sDisease; Breast Cancer. Bioinitiative Report (2007); Section 12:425-495.http://www.bioinitiative.org/
Dode AC, Leao MM, Tejo Fde A et al. Mortality by neoplasia and cellular telephonebase stations in the Belo Horizonte municipality, Minas Gerais state, Brazil. SciTotal Environ (2011); 409(19):3649-3665.
Eger H, Hagen K, Lucas B, Vogel P, Voit H. The Influence of Being Physically Near to aCell Phone Transmission Mast on the Incidence of Cancer. Umwelt Medizin Gesell-schaft (2004); 17(4):1-7.
Hill SM, Blask DE, Xiang S et al. Melatonin and associated signaling pathways thatcontrol normal breast epithelium and breast cancer. J Mammary Gland Biol Neoplasia(2011); 16(3):235-245.
Kesari KK, Kumar S, Behari J. 900-MHz microwave radiation promotes oxidation in ratbrain. Electromagn Biol Med (2011); 30(4):219-234.
Kesari KK, Kumar S, Behari J. Pathophysiology of microwave radiation: effect on ratbrain. Appl Biochem Biotechnol (2012); 166(2):379-388.
Khurana VG, Hardell L, Everaert J, Bortkiewicz A, Carlberg M, Ahonen M. Epidemiolo-gical evidence for a health risk from mobile phone base stations. Int J OccupEnviron Health (2010); 16(3):263-267.
Kloog I, Haim A, Stevens RG, Barchana M, Portnov BA. Light at night co-distributeswith incident breast but not lung cancer in the female population of Israel. Chrono-biol Int (2008); 25(1):65-81.
Kloog I, Haim A, Stevens RG, Portnov BA. Global co-distribution of light at night(LAN) and cancers of prostate, colon, and lung in men. Chronobiol Int (2009);26(1):108-125.
Kloog I, Stevens RG, Haim A, Portnov BA. Nighttime light level co-distributes withbreast cancer incidence worldwide. Cancer Causes Control (2010); 21(12):2059-2068.
Kumar S, Kesari KK, Behari J. The therapeutic effect of a pulsed electromagnetic field onthe reproductive patterns of male Wistar rats exposed to a 2.45-GHz microwavefield. Clinics (Sao Paulo) (2011); 66(7):1237-1245.
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 28
Comments on Notice of Inquiry, ET Docket No. 13-84

Levitt B, Lai H. Biological effects from exposure to electromagnetic radiation emitted bycell tower base stations and other antenna arrays. Environ Rev (2010); 18:369-395.
Oberfeld G. Environmental Epidemiological Study of Cancer Incidence in the Munici-palities of Hausmannstätten & Vasoldsberg (Austria). Provincial Government ofStyria, Department 8B, Provincial Public Health Office, Graz, Austria (2008): 1-10.
Reiter RJ, Rosales-Corral S, Coto-Montes A et al. The photoperiod, circadian regulationand chronodisruption: the requisite interplay between the suprachiasmatic nucleiand the pineal and gut melatonin. J Physiol Pharmacol (2011); 62(3):269-274.
Schernhammer ES, Berrino F, Krogh V et al. Urinary 6-sulfatoxymelatonin levels andrisk of breast cancer in postmenopausal women. J Natl Cancer Inst (2008);100(12):898-905.
Schernhammer ES, Hankinson SE. Urinary melatonin levels and postmenopausal breastcancer risk in the Nurses’ Health Study cohort. Cancer Epidemiol Biomarkers Prev(2009); 18(1):74-79.
Stevens RG. Working against our endogenous circadian clock: Breast cancer and electriclighting in the modern world. Mutat Res (2009); 680(1-2):106-108.
Wolf R, Wolf D. Increased Incidence of Cancer Near a Cell-Phone Transmitter Station.International Journal of Cancer Prevention (2004); 1(2):1-19.
Yakymenko I, Sidorik E, Kyrylenko S, Chekhun V. Long-term exposure to microwaveradiation provokes cancer growth: evidences from radars and mobile communica-tion systems. Exp Oncol (2011); 33(2):62-70.
Zawilska JB, Skene DJ, Arendt J. Physiology and pharmacology of melatonin in relationto biological rhythms. Pharmacol Rep (2009); 61(3):383-410.
SECTION 3 – MICROWAVE RF EFFECTS ON MELATONIN SECRETION
Page 29
Comments on Notice of Inquiry, ET Docket No. 13-84

Page 30
Comments on Notice of Inquiry, ET Docket No. 13-84

RADIOFREQUENCY EXPOSURE INCREASESOXIDATIVE STRESS AND DAMAGES DNA
Over the past 20 years, a great deal of research evidence has accrued whichdemonstrates that EMF and RF can alter cellular physiology.
INDUCTION OF STRESS PROTEINSWhen cells are stressed in a way that damages DNA in cells, an early response of
the cellular physiology is to increase the production of proteins involved in the repair ofthese structures. These repair proteins are called stress proteins or “heat shock”proteins (since early research models used heat to stress the cells). Increased produc-tion of these proteins are direct evidence of physiologic stress and damage to cell DNA,as they represent the effort of the cell to protect against and repair that damage.
The physiologic stressors that trigger this response stimulate specific regions onthe cell’s chromosome. These regions initiate the transcription of the stress responsegenes that encode for these repair proteins.
In the late 1990’s research demonstrated that EMF exposures can produce thesestress proteins. (Lin et al., 1997) (DiCarlo et al., 1998)
Further research demonstrated that EMF/RF stimulation promotes gene trans-cription at different promotion sites than those triggered by heat stress (Lin et al., 1998)(Lin et al., 1999), and that this promotion by EMF/RF can occur at power levels that arenot high enough to produce thermal changes in the cells. (DiCarlo et al., 1999) (Weis-brot et al., 2003) (Blank and Goodman, 2004) (Blank, 2007)
Subsequent research has shown that at DNA transcription sites activated by lowlevel EMF and RF exposure, higher levels of exposure can lead to single or doublestrand breakage of the DNA chain. (Blank and Goodman, 2009)
Current research confirms production of the stress protein response bymicrowave signals in the 900 MHz and 1800 MHz bands. (Cao et al., 2011) (Jiang et al.,2012) (Calabro et al., 2012)
DNA DAMAGEMany research studies performed in the last decade have demonstrated that
radio frequency radiation at nonthermal levels can produce fragmentation of DNA.In 2003, Ivancsits reported that intermittent low frequency EMF could cause
single and double strand breaks in DNA at magnetic flux densities as low as 35 micro-tesla, well below levels producing thermal effects. Effects were time and dose depen-dent. (Ivancsits et al., 2003)
This work was confirmed in 2004 in a study showing that 24 to 48 hour expo-sures to a 0.01 mT 60 hz magnetic field could produce single and double strand DNAcleavage, apoptosis, and necrosis of brain cells in rats. These effects could be blockedwith antoxidants, suggesting that free radicals played a role in the damage process. (Laiand Singh, 2004)
Subsequent research demonstrated that these effects also could be produced bynonthermal effects of radiofrequency microwave exposures—at power levels that werebelow the levels producing thermal effects—and that this nonthermal damage could beprevented by administration of antioxidant free radical scavengers. (Adlkofer, 2006)
Page 31
Comments on Notice of Inquiry, ET Docket No. 13-84

The results of in vitro studies on DNA damage from EMF/RF are variable, sincedifferent cell types have different sensitivities to these effects. (Schwarz et al., 2008)Several detailed reviews of these studies have been published in the last five years.These reviews document multiple studies showing production of DNA damage at lowpower densities, with more prolonged exposure times producing more significanteffects. (Lai, 2007) (Ruediger, 2009) (Phillips et al., 2009) (Levitt and Lai, 2010)
Current research continues to validate these findings. For example, Cam andSyhand found an increase in the production of single strand DNA breaks in hair rootcells following 15 to 30 minutes of mobile phone use. (Cam and Seyhan, 2012)
Figure 1: Comet Assay of DNA fragmentation in rat brains, produced byprolonged exposure to microwave RF. (Kesari et al., 2010a)
Kesari et. al. exposed Wistar rats to 2.45 GHz frequency at 0.34 mW/cm2 powerdensity (340 μW/cm2, whole body SAR ~ 0.11 W/Kg), 2 hours a day for 35 days, anddemonstrated increased double strand DNA breakage (p ≤ 0.0002) in brain tissue. Thiswas accompanied by decreased activity levels of glutathione peroxidase (p < 0.005) andsuperoxide dismutase (p < 0.006), and increased catalase activity (p < 0.006) suggestingthat the microwave exposure produced severe oxidative stress. (Kesari et al., 2010a)
Kumar et. al. exposed Wistar rats to 50 GHz continuous source microwave trans-mission, 2 hours a day for 45 days, with a power density of 0.86 μW/cm2 (calculatedSAR 8.0 x 10-4 W/kg). Other rats were exposed to 10 GHz, 2 hours a day for 45 days,power density 0.214 mW/cm2 (214 μW/cm2, SAR 0.014 W/kg). Both forms of exposureproduced significantly altered levels of reactive oxygen species, antioxidant enzymeactivity, and blood cell micronuclei formation, demonstrating the production of oxida-tive stress with genotoxic effects. (Kumar et al., 2010)
RF EXPOSURE PRODUCES OXIDATIVE STRESSIt is a truism among apologists for the telecommunications industry that
microwave radiofrequency transmissions cannot possibly cause cancer, because theenergy of a photon of this wavelength is not powerful enough to directly break an ionic
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 32
Comments on Notice of Inquiry, ET Docket No. 13-84

bond the way an xray can, and therefor could not possibly cause mutations in DNA.Such an argument sounds like good physics, but it isn’t good biology. Ionizing radia-tion is only one way to cause the mutations in DNA that can produce cancer.
Chronic inflammation can cause cancer. Cigarette smoke can cause cancer.Toxins and autoimmune disease can cause cancer. One common pathway shared bythese causes is that they produce an inflammatory response in the body that increasesthe activity of free radicals (reactive oxygen species). These free radicals produce oxida-tive damage in the tissues.
This oxidative activity is the tool that our bodies use to destroy foreign bacteria,which can be completely broken up—DNA and all—and digested by our immunesystem. Free radicals are an important defensive weapon for our bodies, but an excessof oxidative activity can lead to damage of our own tissues. Such excesses have beenassociated with many chronic problems including autoimmune disease, heart disease,and some forms of cancer. Every week another article is published suggesting thattaking antioxidants may be protective against some of these problems.
The mechanisms through which EMF/RF increase oxidative stress in livingtissues have not been clearly elucidated, although some ideas have been proposed.(Liboff, 2010) (Georgiou, 2010)
But in the last decade, the scientific research clearly established that EMF and RFexposure cause an increase in reactive oxygen species in living tissues, leading tooxidant damage of DNA. (Shiroff, 2008)
Figure 2: Depletion of antioxidants in RF-exposed rat brains, after exposure to 2.45GHz, 2 h a day for 35 days at 0.34 mW/cm2 power density, 2.45 GHz frequency.
(Kesari et al., 2010a)Studies cited above document that microwave RF exposures at very low power
densities produce oxidant stress accompanied by DNA damage. (Kesari et al., 2010a)(Kumar et al., 2010)
Other recently published studies also show that RF exposure can increaseoxidant stress and tissue damage in brain tissue (Maaroufi et al., 2011) (Avci et al.,2012), liver tissue (Guler et al., 2012), white blood cells (Lu et al., 2012), and human sali-vary glands (Hamzany et al., 2012).
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 33
Comments on Notice of Inquiry, ET Docket No. 13-84
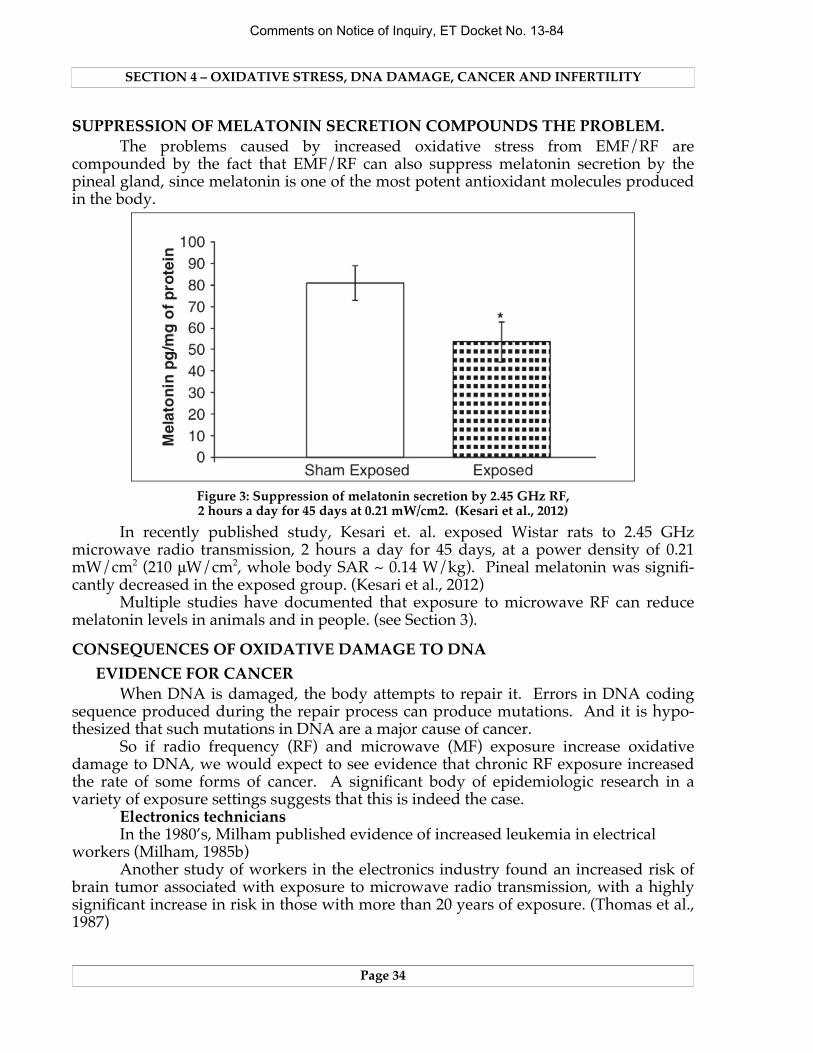
SUPPRESSION OF MELATONIN SECRETION COMPOUNDS THE PROBLEM.The problems caused by increased oxidative stress from EMF/RF are
compounded by the fact that EMF/RF can also suppress melatonin secretion by thepineal gland, since melatonin is one of the most potent antioxidant molecules producedin the body.
Figure 3: Suppression of melatonin secretion by 2.45 GHz RF,2 hours a day for 45 days at 0.21 mW/cm2. (Kesari et al., 2012)
In recently published study, Kesari et. al. exposed Wistar rats to 2.45 GHzmicrowave radio transmission, 2 hours a day for 45 days, at a power density of 0.21mW/cm2 (210 μW/cm2, whole body SAR ~ 0.14 W/kg). Pineal melatonin was signifi-cantly decreased in the exposed group. (Kesari et al., 2012)
Multiple studies have documented that exposure to microwave RF can reducemelatonin levels in animals and in people. (see Section 3).
CONSEQUENCES OF OXIDATIVE DAMAGE TO DNAEVIDENCE FOR CANCER
When DNA is damaged, the body attempts to repair it. Errors in DNA codingsequence produced during the repair process can produce mutations. And it is hypo-thesized that such mutations in DNA are a major cause of cancer.
So if radio frequency (RF) and microwave (MF) exposure increase oxidativedamage to DNA, we would expect to see evidence that chronic RF exposure increasedthe rate of some forms of cancer. A significant body of epidemiologic research in avariety of exposure settings suggests that this is indeed the case.
Electronics techniciansIn the 1980’s, Milham published evidence of increased leukemia in electrical
workers (Milham, 1985b)Another study of workers in the electronics industry found an increased risk of
brain tumor associated with exposure to microwave radio transmission, with a highlysignificant increase in risk in those with more than 20 years of exposure. (Thomas et al.,1987)
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 34
Comments on Notice of Inquiry, ET Docket No. 13-84

A case/control study of brain cancer deaths in Maryland found a threefoldgreater brain cancer incidence in electrical or electronic engineers and technicians,compared to the reference population. (Lin et al., 1985)
A study of leukemia rates in different occupational groups in the U.S. Navyshowed increased leukemia risk in electrician’s mates. (Garland et al., 1990)
Figure 4: Mortality (1950–1974) in U.S. Navy Korean War Veterans, stratified by in-service levels of occupational radar exposure. (Cherry, 2002a, after Robinette, 1980)
A study performed for the U.S. military published data comparing a cohort of20,000 Korean War veterans with higher occupational exposure levels to RF/MW expo-sure to 208,000 Korean war veterans with minimal occupational exposure during theirservice years. Mortality statistics were reviewed for the interval between 1950 and 1974.(Robinette et al., 1980) This data shows that the group with the highest rated occupa-tional exposure level (aviation electronic technicians) had a significantly higher totaldeath rate during the study period, and a higher death rate from disease, from malig-nancy, and from lymphatic and hematopoetic malignancies. (Goldsmith, 1997a)
A study of Polish career military personnel from 1971 – 1985 showed double therisk of cancer in personnel with occupational exposure to RF/MW transmission, ascompared other personnel. The exposed cohort had higher morbidity rates for GIcancers (Observed versus Expected Ratio = 3.19 – 3.24), brain tumors (OER = 1.91), andhematopoetic malignancy (OER = 6.31), including chronic myelocytic leukemia (OER =13.9), acute myeloblastic leukemia (OER = 8.62), and non-Hodgkin’s lymphoma (OER =5.82). (Szmigielski, 1996)
Radio OperatorsIncreased rates of acute myeloid leukemia and of other lymphatic malignancies
have been found in large population based studies of amateur radio operators (Milham,1985a) (Milham, 1988a) (Milham, 1988b).
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 35
Comments on Notice of Inquiry, ET Docket No. 13-84

Figure 5: Analysis of leukemia deaths in male members of the American RadioRelay League resident in Washington and California, 1971 – 1983. (Milham, 1985a)
Another study of female radio and telegraph operators in Norway found anincreased incidence of breast cancer in this group as compared to the standardized inci-dence rate in the female population of that country. (Tynes et al., 1996)
Police radar operatorsTwo studies have shown increased rates of testicular cancer (Davis and Mostofi,
1993), and of testicular cancer and melanoma (Finkelstein, 1998) in police officers withoccupational exposure to handheld radar.
Airline pilotsAirline pilots have significant occupational exposure to RF/MF (radio frequency
and microwave frequency) transmissions.A study of U.S. Air Force personnel showed an increased risk of brain tumors
associated with increasing rank, and associated with estimated exposures to bothmicrowave radio and low frequency radio transmissions. No increased risk associatedwith exposure to ionizing radiation was found in this study population. (Grayson, 1996)
A study of commercial airline pilots in Iceland found an increased risk of malig-nant melanoma. (Rafnsson et al., 2000) Another study with Danish pilots showedincreased risk of total cancer, melanoma, other skin cancers, and acute myeloidleukemia in commercial airline cockpit crews. (Gundestrup and Storm, 1999) Neither ofthese studies specifically controlled for RF/MF exposures as compared to other expo-sures (cosmic rays, tropical sun on the beach, etc.) incurred by flying personnel.
However, an extensive study of German commercial airlines crews (including6,017 cockpit and 20,757 cabin crew members) showed an increased brain cancer risk forcockpit crew and an increased all cancer risk for cockpit crew with more than 30 yearsemployment compared to those with under 10 years of employment. Notably, theseincreased risk were not found in cabin crew members, who share equal exposure tocosmic rays and tropical beaches, but are farther from the radios. (Zeeb et al., 2010)
U.S. Embassy Moscow 1953 – 1976From the 1950’s to the mid-1970’s the U.S. Embassy in Moscow was exposed to a
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 36
Comments on Notice of Inquiry, ET Docket No. 13-84

constant low intensity radar signal, as a form of harassment by the Russian government.The exposure level on the outside of the west facade of the building was measured at 5microwatts/cm2, and was present for 9 hours a day. Since the wall and windows atte-nuated the signal, inside exposure levels were likely to be in the range of 0.02 to 0.1μW/cm2.
The State Department contracted an epidemiologic analysis potential healtheffects on exposed personnel and their dependents, which was performed by A.M. Lili-enfeld M.D., and epidemiologist at John’s Hopkins University. This report waspublished including all of the tabulated raw data. (Lilienfeld AM, 1979)
The report as finally released stated as a conclusion that personnel “suffered noill effects” from the microwave exposure. However, the published conclusions differedfrom the original conclusions written by Dr. Lilienfeld, and evidence suggests that thefinal conclusions were “whitewashed”. (Goldsmith, 1997b) One can presume that thismight have been done to avoid embarrassment of the federal government, since anyharm, if produced, would have been produced at levels of exposure orders of magni-tude less than those exposure levels permitted by United States FCC guidelines.
A hematologic study performed on employees at the Moscow embassy wassubmitted to the U.S. government in October, 1976. This study showed significantabnormalities in hematologic parameters in this group, in comparison with studies offoreign service workers in the United States. (Goldsmith, 1997a)
The published data from the Lilienfield study of Moscow embassy workers andtheir dependents has subsequently been analyzed by other epidemiologists and foundto show a statistically significant increase in total adult and childhood cancers, in breastcancer, and in childhood leukemia. (Goldsmith, 1995) (Cherry, 2002a)
Residential exposure to Radio/TV Transmission towersBy the late 1990’s, a significant body of epidemiologic literature had accumulated
that demonstrated an association between exposure to radar and RF radiation and theoccurrence of certain types of cancer.
Evidence for association between radio transmission tower exposures and adultand/or childhood leukemia has been reported in studies from Hawaii (Maskarinec etal., 1994) and Australia (Hocking et al., 1996).
A study from England shows an increased risk of adult leukemia in those resi-ding within two kilometers of the transmission tower, and decreased risk of leukemia,skin cancer, and bladder cancer with increased distance of residence from the tower.(Dolk et al., 1997b) A follow-up study involving multiple other sites in England alsoshowed a statistically significant decline in risk of adult leukemia with increasingdistance of residence from transmission sites. (Dolk et al., 1997a) (Hocking et al., 1998)
A study in Rome evaluated the incidence of adult and childhood leukemia as afunction of residential proximity to the Vatican Radio transmission tower. Pediatricleukemia cases were more common than expected at less than 6 kilometers from thetower, and significantly elevated in adult men living within 2 km of the tower. Adultmale leukemia mortality and childhood leukemia rates showed a significant decreasewith increasing distance between tower and residence. (Michelozzi et al., 2002)
A study of cancer incidence in proximity to the Sutro radio/TV tower in SanFrancisco also showed a strong correlation of exposure and incidence of several types ofchildhood cancer. (Cherry, 2002b) This study was notable for its rigor in analyzing theactual exposure levels around the tower in relation to the data set. Power density/
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 37
Comments on Notice of Inquiry, ET Docket No. 13-84

exposure levels around UHF and VHF broadcasting antennae are not distributed in asimple and symmetrical regression (“with the square of the distance”). Transmissionexposure levels form a series of peaks and valleys around these antennae, and theantennae can be arranged to focus more power in one direction than another, aiming astronger signal at the target audience in a population center. Studies that fail to takethis distribution into account and assume that exposure is in direct ratio to distance willmix higher and lower exposure groups together, diluting the power of the study andunderestimating true risk in relation to exposure.
In another paper, Dr. Cherry analyzes this issue in detail, and uses his more rigo-rous approach to review and refine the analysis of data from many of the earlier studieson health effects of radio/TV broadcast towers. His analysis strengthens the evidencefor increased cancer risk from these exposures. (Cherry, 2002a)
A large population case/control study in south Korea looked at 1928 leukemiapatients and 956 brain cancer patients under 15 years of age who were diagnosedbetween 1993 and 1999 at 14 large hospitals in Korea. These cases were matched with3082 age matched patients who received respiratory disease diagnoses (primarilyasthma) at the same hospitals during the study period. Case and control exposurelevels were calculated for 31 transmitters in South Korea that had a transmission powergreater than 20 kW, using a mathematical model that was correlated with field testing.Children residing within 2 kilometers of a transmission tower had a significantlyincreased risk of leukemia as compared to children with residence greater than 20 kmfrom the tower (OR 2.15, 95% CI = 1.00 to 4.67). (Ha et al., 2007)
Residential Exposure to Cell Phone Tower (Base Station) TransmissionsWith the dramatic rollout of commercial cell phone service in the 1990’s, large
segments of the population became exposed to significantly higher levels of microwaveRF exposure due to the installation of cell phone towers in urban areas. Several recentpapers have reviewed the significant evidence for ill effects from these urban exposures.(Khurana et al., 2010) (Yakymenko et al., 2011) (Kumar, 2010)
Netanyu, IsraelWolf and Wolf studied rates of cancer incidence during the second year of opera-
tion of a 1500 watt 850 MHz cell phone tower in Netanya, Israel. The study group wascomposed of 622 individuals who had lived in area A, within 350 meters of the tower,for the previous 3 to 7 years. A control group of 1,222 individuals living in an outlyingarea B was also studied.
During the study year, 8 cases of cancer occurred in the study group, and 2 casesoccurred in the control group. The cancer rate for the entire town was 31 cases per10,000. Relative cancer rates for females was 10.5 for the study group, 0.6 for the controlgroup, and 1.0 for the town as a whole (P < 0.0001).
Signal power densities of the tower’s transmissions in the homes of the cancercases ranged from 0.3 – 0.5 μW/cm2. [note that FCC limits are 600 – 1000 μW/cm2.]
In the year following the close of the study, another 8 new cases of canceroccurred in area A, and another 2 cases occurred in area B. (Wolf and Wolf, 2004)
Naila, GermanyA cell phone transmission tower was placed in the town of Naila, Germany, in
1993. Eger, Hagen, et. al. reviewed the medical health records from 1994 to 2004 foraround 1000 residents of the municipality (roughly 90% of the population). All
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 38
Comments on Notice of Inquiry, ET Docket No. 13-84

included patients had been living at the same address during the entire 10 years ofobservation.
Over the course of the entire study period, patients living in an inner area within400 meter of the transmission tower had 2.27 times the relative risk of cancer incidence,compared to patients living more than 400 meters from the tower (p < 0.05). Cancerpatients in the inner residential area also developed cancer an average of 8.5 yearsearlier in life than did cancer patients residing in the more distant area.
For the years 1999 to 2004 (after 5 years of tower operation) the relative risk ofcancer incidence in residents less then 400 meters from the tower increased to 3.29 (p< 0.01). Relative risk of breast cancer was 3.4 in the inner area, where average age ofdiagnosis was 50.8 years, compared to 69.9 years in the outer area. (Eger et al., 2004)
Hausmannstätten and Vasoldsberg, AustriaOberfeld performed a case/control study of cancer patients in the municipalities
of Hausmannstätten and Vasoldsberg, Austria. All subjects had resided within 1,200meters of an analogue cell phone tower that operated between 1984 and 1997 in themunicipalities.
Figure 6: Odds ratio of cancer incidence, stratified by exposure levels(exterior to dwelling) in μW/m2. (Oberfeld, 2008)
Residential outdoor exposure levels were measured, and three different case/control groups were assessed, for case exposure levels outside the residence of 10 – 100μW/m2 (= 0.001 – 0.01 μW/cm2)), 100 – 1000 μW/m2 (= 0.01 – 0.1 μW/cm2), and greaterthan 1000 μW/m2 (> 0.1 μW/cm2). respectively. The reference exposure level for thecontrol group was less than 10 μw/m2 (= 0.001 μW/cm2). [Note that FCC thermal safetylimits are 6,000,000 to 10,000,000 μW/m2.]
Cancer risk for all cancers was significantly elevated for all three elevated expo-sure categories, and was 5 to 8 times higher in the >1000 μW/m2 (> 0.1 μW/cm2) cate-
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 39
Comments on Notice of Inquiry, ET Docket No. 13-84
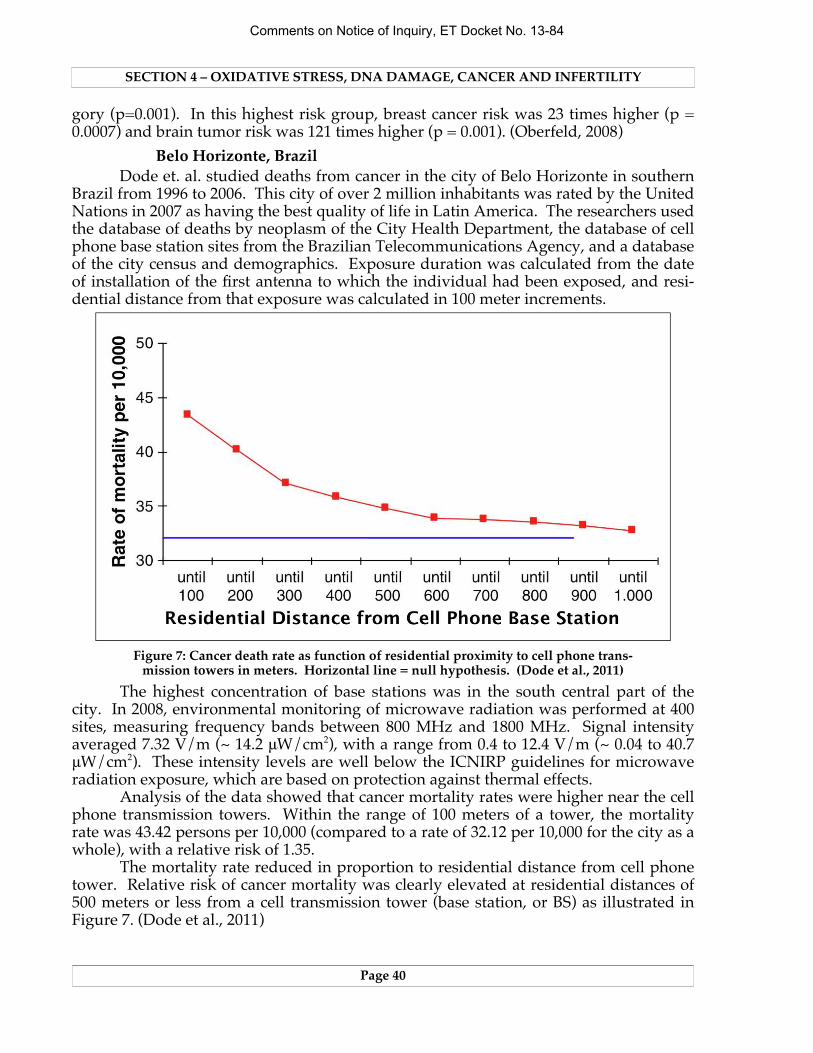
gory (p=0.001). In this highest risk group, breast cancer risk was 23 times higher (p =0.0007) and brain tumor risk was 121 times higher (p = 0.001). (Oberfeld, 2008)
Belo Horizonte, BrazilDode et. al. studied deaths from cancer in the city of Belo Horizonte in southern
Brazil from 1996 to 2006. This city of over 2 million inhabitants was rated by the UnitedNations in 2007 as having the best quality of life in Latin America. The researchers usedthe database of deaths by neoplasm of the City Health Department, the database of cellphone base station sites from the Brazilian Telecommunications Agency, and a databaseof the city census and demographics. Exposure duration was calculated from the dateof installation of the first antenna to which the individual had been exposed, and resi-dential distance from that exposure was calculated in 100 meter increments.
Figure 7: Cancer death rate as function of residential proximity to cell phone trans-mission towers in meters. Horizontal line = null hypothesis. (Dode et al., 2011)
The highest concentration of base stations was in the south central part of thecity. In 2008, environmental monitoring of microwave radiation was performed at 400sites, measuring frequency bands between 800 MHz and 1800 MHz. Signal intensityaveraged 7.32 V/m (~ 14.2 μW/cm2), with a range from 0.4 to 12.4 V/m (~ 0.04 to 40.7μW/cm2). These intensity levels are well below the ICNIRP guidelines for microwaveradiation exposure, which are based on protection against thermal effects.
Analysis of the data showed that cancer mortality rates were higher near the cellphone transmission towers. Within the range of 100 meters of a tower, the mortalityrate was 43.42 persons per 10,000 (compared to a rate of 32.12 per 10,000 for the city as awhole), with a relative risk of 1.35.
The mortality rate reduced in proportion to residential distance from cell phonetower. Relative risk of cancer mortality was clearly elevated at residential distances of500 meters or less from a cell transmission tower (base station, or BS) as illustrated inFigure 7. (Dode et al., 2011)
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 40
Comments on Notice of Inquiry, ET Docket No. 13-84

TaiwanLi et. al. performed a case/control study of 2606 children age 15 or less who were
diagnosed with a neoplasm in Taiwan between 2003 and 2007. Each case was matchedwith 30 controls. Residential exposure of cases and controls was calculated based onthe annual power density in watt-years per kilometer squared for each of the 367 towns-hips in Taiwan, averaged out for the 5 year period prior to diagnosis in the townshipwhere the subject resided at time of diagnosis.
This study is notable for the large number of cases and controls, which shouldincrease the power of the study. On the other hand, if elevated microwave exposure isassociated with cancer risk, assuming that power density of cell phone tower transmis-sions is constant throughout each township would serve to minimize the effects ofhigher exposure levels closer to the towers, minimizing the distinction between higherand lower cohorts, and diluting the power of the study.
Case/control analyses were performed for “all cancer types”, for leukemia, andfor brain neoplasm. Odds ratio for cases of “all cancer types” with calculated exposuregreater than median exposure value of controls were significantly elevated at 1.13 (95%CI = 1.01 to 1.28). Odds ratio for cases of leukemia with calculated exposure greaterthan median exposure value of controls were elevated at 1.23 (95% CI = 0.99 to 1.52).Odds ratio for cases of brain neoplasm with calculated exposure greater than medianexposure value of controls were slightly elevated at 1.14 (95% CI = 0.83 to 1.55). (Li etal., 2012)
EVIDENCE FOR IMPAIRMENT OF FERTILITYToxic exposures that damage DNA can cause cancer. They can also cause
damage to the production of healthy eggs and sperm, leading to infertility. Ifmicrowave RF exposure causes oxidative damage to DNA, this should lead to measu-rable alterations in function of reproductive function and fertility. Current research isbeginning to prove the presence of this effect.
Laboratory studies in insectsIn 2004, Panagopoulos et. al. demonstrated that exposure to a modulated GSM
900 MHz cell phone signal for 6 continuous minutes daily for two days decreased thefertility of both male and female fruit flies (Drosophila melanogaster). Exposure powerdensity was ~ 0.436 milliwatts/cm2 (= 436 μW/cm2). (Panagopoulos et al., 2004)
In a later study, Panagopoulos et. al. exposed Drosophila fruit flies to a cellphone transmitting GSM 900 MHz at 0.40 mW/cm2 (= 400 μW/cm2—Group 1) or GSM900 MHz at 0.29 mW/cm2 (= 290 μW/cm2—Group 2), or DCS 1800 MHz at 0.29 mW/cm2 (= 290 μW/cm2—Group 3). Transmission exposures were 6 consecutive minutesper day for six days. The exposure induced fragmented DNA during oogenesis. Celldeath scores in the ovaries of female flies were 63% in Group 1, 45% in Group 2, and39% in Group 3, as compared to 7.8% in the sham and control groups. (Panagopoulos etal., 2007)
Subsequent research exposed Drosophila fruit flies to GSM 900 MHz or DCS1800 MHz signals for signal durations of 1 to 21 minutes a day for five consecutive days,at a power density of 10 μW/cm2. Impairment of fertility increased linearly with dura-tion of exposure (see figure 2). Even at 1 minute of exposure a day, fertility was signifi-cantly decreased in exposed versus sham exposure specimens (p < 0.00001). (Panago-poulos and Margaritis, 2010)
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 41
Comments on Notice of Inquiry, ET Docket No. 13-84

Figure 8: Decreased fertility of fruit flies at exposure level of 10 μW/cm2.(Panagopoulos and Margaritis, 2010)
In another study using a GSM 900 MHz cell phone signal at 0.35 mW/cm2 (= 350μW/cm2), six minutes of daily exposure was divided into one, two, or three minutesegments, spaced 10 minutes apart. This was compared with one 6 minute constantexposure and with two 3 minute exposures spaced 6 hours apart. DNA damage andcell death in the intermittent exposures sequenced 10 minutes apart was essentially thesame as with the constant 6 minute exposure (p > 0.92), and markedly higher than inthe sham group (p < 10-8). The group with divided exposures 6 hours apart had less celldeath than the more frequently exposed group, but still showed significantly higherinfertility than the control group (p < 0.002). (Chavdoula et al., 2010)
In yet another study, the Panagopoulos group evaluated influence of GSM 900MHz and 1800 MHz cell phone transmissions on Drosophila fertility using exposures of6 minutes per day for 6 days, at exposure distances varying from 0 to 100 cm. Theywere able to demonstrate an adverse effect on fertility for all exposures at all powerdensities greater than or equal to 1 μW/cm2. (Panagopoulos et al., 2010)
Recently Panagopoulos published another study demonstrating that exposure toa GSM 900 MHz modulated cell phone transmissions at ~0.35 mW/cm2 (= 350 μW/cm2)for 6 minutes during ovarian development can seriously retard ovarian maturation andreduce final size of ovaries in Drosophila fruit flies. (Panagopoulos, 2012)
Laboratory studies in animalsMagras and Xenos placed caged mice at various locations in an antenna park in
Thessaloniki, Greece, at locations with RF power densities ranging from 168 nW/cm2 (=0.168 μW/cm2) to 1053 nW/cm2 (= 1.053 μW/cm2). The mice lived in these locations forsix months, during which time they were mated repeatedly. Numbers of newborns perlitter decreased progressively, and ended with complete infertility by the fifth matingcycle. This infertility was not reversible with removal to an unexposed laboratory envi-ronment. (Magras and Xenos, 1997)
Meo et. al. exposed Wistar rats to cell phone transmissions for either 30 or 60
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 42
Comments on Notice of Inquiry, ET Docket No. 13-84

minutes a day for 3 months, and then measured serum testosterone levels. Testosteronelevels decreased with increased duration of exposure, and the difference in testosteronelevel between subjects and controls was statistically significant in the 60 minutes perday group (p < 0.02) (Meo et al., 2010)
Otitoloju et. al. evaluated sperm head morphology in laboratory rats that wereexposed to cell tower transmissions at two locations with mean RF exposure levels of489 ± 43 mV/m (~ 0.6 μW/cm2) and 625 ± 25 mV/m (~ 0.10 μW/cm2). A control groupwas held in a laboratory with RF exposure levels of 59 ± 17 mV/m (~ 0.001 μW/cm2).After six months of exposure, exposed rats showed mean sperm head abnormalities of40% and 46%, versus 2% in control animals. (Otitoloju et al., 2010)
Kesari and Behari exposed male Wistar rats to 50 GHz continuous microwaveradiation at a power density of 0.86 μW/cm2 (calculated SAR 8 x 10-4 W/kg), 2 hours aday for 45 days. Sperm cells showed significant reductions of glutathione peroxidaseand superoxide dismutase activity (p ≤ 0.05) and increased catalase activity (p < 0.02),consistent with a significant increase in oxidative stress. Histone kinase activity wasalso increased (p < 0.016), and and significantly increased apoptosis (programmed celldeath) and alteration in phases of sperm development were also present. (Kesari andBehari, 2010)
In a similar study, Kesari et. al. confirmed a significant increase in cell deaththrough apoptosis, reduced sperm count, and reduced protein kinase C activity in maleWistar rats exposed to cell phone transmissions 2 hours daily for 35 days. Exposurepower densities ranged from 0.1 – 2.0 mW/cm2 (= 100 – 2000 μW/cm2, calculated SAR0.9 W/kg. (Kesari et al., 2010b)
In 2011 and 2012 Kumar and Kesari published four additional papers documen-ting the adverse effects of 10 GHz microwave exposure (2 hours daily for 45 days atpower density of 0.21 mW/cm2 (= 210 μW/cm2, SAR 0.014 W/kg) on fertility in maleWistar rats. These studies document significant levels of pathological change includingincreases in reactive oxygen species, increased apoptosis (cell death) in sperm cells andaltered sperm cell cycle (Kumar et al., 2011), increased free radical formation, decreasedactivity of glutathione peroxidase and superoxide dismutase, increased activity of cata-lase and malondialdehyde, decreased histone kinase (Kesari et al., 2011), reduced testos-terone levels, shrinkage of seminiferous tubules and testicular size, distortion of spermstructure, decreased number and weight of progeny (Kesari and Behari, 2012), forma-tion of micronuclei bodies in lymphocytes, DNA strand breakage, altered levels ofhistone kinase, altered percentage of spermatogenic phases, and (again) reduced testos-terone levels and shrinkage of seminiferous tubules. (Kumar et al., 2012)
In 2012, Atasoy et. al. published a study of rats exposed to a WiFi router(802.11.g, 2.437 GHz) for 20 weeks, 24 hours a day. Histological and immunohistoche-mical examinations of the rats’ testes showed evidence of DNA damage compared tocontrols (p < 0.05) and decreased activity levels of antioxidants (catalase and glutat-hione peroxidase, p < 0.05). (Atasoy et al., 2012)
Other animal studiesExperimental laboratory evidence clearly demonstrates that microwave RF radia-
tion can adversely effect reproduction in insects and animals. Some evidence tosupport this is also available from studies of animals exposed to RF in their naturalenvironment.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 43
Comments on Notice of Inquiry, ET Docket No. 13-84

Figure 9: Impaired fertility in white storks nesting near cell phone towers.(Balmori, 2005)
Balmori studied a white stork population that was nesting near a cluster of cellphone towers in in Valladolid, Spain. Power densities at ground level ranged from 10μW/cm2 at 50 meters from the towers to 1 μW/cm2 at 100 meters distance and a tenthsof a μW/cm2 at 150 to 200 meters distance. Total breeding productivity was signifi-cantly reduced at nests closer than 200 meters, compared to nests farther than 300meters from the towers. (Balmori, 2005)
Balmori performed bird counts at 30 locations during 40 visits to Valladolid,Spain, over the interval between October 2002 and May 2006, and measured mean elec-tric field strength at each counting site. Bird population density declined significantlyover the observation period (p = 0.0037), and population density was significantly lowerin areas with higher electric field strength (p = 0.0001). (Balmori and Hallberg, 2007)
Balmori also studied reproductive success of common frogs (Rana temporaria) ata breeding site 140 meters from a cluster of cell phone towers. Electric field intensitiesmeasured at 1.8 to 3.5 V/m (~0.9 to 3.2 μW/cm2). Some eggs were in enclosures thatwere permeable to microwave radiation, and others were shielded in grounded Faradaycages. Exposed eggs showed asynchronous growth with varying tadpole size and a90% mortality rate, while shielded eggs developed synchronously with a 4.2% mortalityrate. (Balmori, 2010a)
Much more work needs to be done on in vivo studies of the effects of microwave cellular transmissions on animals and plants. Two reviews of the existing research havebeen published. (Balmori, 2009) (Balmori, 2010b)
Human studiesHuman sperm counts have been declining for decades. In 1992 Carlsen et. al.
published a meta-review of 61 studies published between 1938 and 1991, with 14,947subjects. They found a decreased in mean sperm count from 113 million/ml to 66million/ml (p < 0.0001) between 1940 and 1990, with a decrease in seminal volume from
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 44
Comments on Notice of Inquiry, ET Docket No. 13-84

3.40 ml to 2.75 ml (p = 0.027). Additionally, the percentage of men with sperm counts< 20 million/ml increased over this time period, while the percentage of men withsperm counts > 100 million/ml decreased. The incidence of testicular cancer increasedbetween two and fourfold during this interval. (Carlsen et al., 1992)
Carlsen’s analysis produced controversy initially. But subsequent analysis hasshown that their results were essentially correct. Analytic approaches to their data setthat refined the analysis to adjust for bias of various kinds have continued to supportthe validity of their conclusions. (Swan and Elkin, 1999)
In another meta-analysis, Swan et. al. looked at 54 of the most robust studies inthe Carlsen data set, and at 47 additional studies, covering studies from 28 countriesover a total time interval from 1934 to 1996. They found a rate of decrease in spermcounts of 0.80 million/ml per year in North America and 3.13 million/ml per year inEurope/Australia. (Swan et al., 2000)
And more recent studies have shown that this downward trend in sperm countsis continuing. Jorgensen et. al. found decreasing levels in sperm concentration, totalsperm count, and percentage of morphologically normal sperm in Finnish men born in1987 versus 1982 – 83 versus 1979 – 1981. (Jorgensen et al., 2011) Sperm counts in NewZealand sperm donors decreased 50% between 1987 and 2007, an average of 2.5% peryear. (Shine et al., 2008)
In the early 1990’s, it was hypothesized that this decrease in sperm counts andincrease in testicular pathology might be due to exposure of male embryos to exoge-nous estrogens (DES, pesticide residues, plasticizers like Bisphenol A, etc.) early indevelopment. (Sharpe and Skakkebaek, 1993) (Carlsen et al., 1995) (Irvine, 1997)
In 1994, Abell et. al. described higher sperm counts in members of a Danishorganic farmer’s association, as compared with Danish men who had occupationalexposures to xenoestrogens. (Abell et al., 1994) Jensen et. al. found a 43.1% highersperm concentration (p = 0.033) in 55 members of Danish organic foods associationswho ate at least 25% organic foods, as compared with 141 normal controls. (Jensen et al.,1996)
Multiple studies in animal models have shown that in utero exposures to estro-genic chemicals can alter testicular health and function. Regional variations in spermcount and testicular cancer rates suggest the possibility of environmental influences. Arecent paper by Nordkap et. al. reviews current perspectives on this subject. (Nordkapet al., 2012)
On the other hand, estrogenic xenobiotic chemicals have been present in the foodchain since the 1950’s. Adverse clinical effects of these exposures have been discussedsince the early 1960’s. (Randolph, 1962) Unless the human body burden of these chemi-cals has continued to significantly increase over the last 50 years, we would expect theinfluence of this effect on sperm counts to plateau.
But sperm counts have not plateaued. They have continue to decrease throug-hout the developed world. A recent study of 26,609 french partners of totally infertilewomen seeking in vitro fertilization found a 32.2% decrease in sperm concentrationbetween 1989 and 2005, with projected sperm counts for a 35 year old man droppingfrom 73.6 million/ml to 49.9 million/ml. (Rolland et al., 2012)
This continued trend should be a cause for significant alarm. The World HealthOrganization defines sperm counts above 20 million/ml as normal. But studies haveshown that couples take longer to get pregnant at sperm counts below 40 to 55 million/
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 45
Comments on Notice of Inquiry, ET Docket No. 13-84

ml. (Bonde et al., 1998) (Guzick et al., 2001) (Slama et al., 2002) In Israel, a recent studyof sperm donors showed that over the last 10 to 15 years the average sperm count hasdropped from 106 million/ml to 68 million/ml, an average decrease of 2.5 million/ml(0.8%) per year. 15 years ago, 66% of sperm donations were of acceptable quality; usingthe same criteria, at the current time only 18% of donations would be of acceptablequality. (Haimov-Kochman et al., 2012)
As discussed above, studies in insects and animals have demonstrated thatmicrowave radio exposure at remarkably low power densities can have an adverseeffect on male fertility. With the rollout of cellular and WiFi infrastructure, exposure tothese radio frequencies has increased dramatically in the last 20 years. Would it bereasonable to ask if such exposures have played a role in the continued decrease in malefertility that has occurred during this time period? The result of several recent studiessuggests that the answer to this question is “Yes”.
Erogul et. al. split human sperm samples and exposed one part to signal from a900 MHz cell phone. They found statistically significant decreases in motility of spermin the exposed samples. (Erogul et al., 2006)
Fejes et. al. measured semen quality in a cohort of 371 subjects where confoun-ding factors had been excluded, and found a significant decrease in sperm motility (p< 0.01) in individuals with talk time > 60 minutes/day versus talk time < 15 minutes/D.Decreased sperm motility also correlated with increased duration of cell phoneownership in months. (Fejes et al., 2005)
Figure 10: Decrease in sperm count (5), motility (6), viability (7) and normalmorphology (8) with increased cell phone talk time. (Agarwal, 2008)
Agarwal et. al. studied semen quality in 361 subjects, divided into four groupsbased on daily cell phone usage (no use, < 2 hours/day, 2 to 4 h/D, > 4 h/D). Theyfound that sperm count, motility, viability, and percent normal morphology all decre-ased with increased cell phone use. (Agarwal et al., 2008)
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 46
Comments on Notice of Inquiry, ET Docket No. 13-84

Figure 11: Sperm exposed in vitro to 1.8 GHz (SAR = 27.5 W/kg) for 16 hours @21ºC (isothermal conditions). (De Iuliis et al., 2009)
De Iuliis et. al. exposed human sperm to 1.8 GHz microwave radio transmis-sions. Statistically significant decreases in sperm motility and vitality were demonstrateat exposure levels as low as 1.0 W/kg (p < 0.01). This study also found an increase inreactive oxygen species, oxidative damage to DNA, and DNA fragmentation, that wasnot dependent on thermal effects. (De Iuliis et al., 2009)
Figure 12: A) Production of ROS with increasing levels of microwave RF .B) Production of ROS with increasing levels of temperature.
(De Iuliis et al., 2009)
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 47
Comments on Notice of Inquiry, ET Docket No. 13-84

Figure 13: Sperm damage from exposure to laptop computer WiFi transmission.(Avendano et al., 2011).
Another recent study the effects of exposing motile sperm to 4 hours of WiFitransmission at a position 3 cm beneath a laptop computer, at power densities between0.45 and 1.05 μW/cm2. Temperature was maintained at a constant 25ºC. Exposed speci-mens showed a statistically significant decrease in sperm progressive motility, and asignificant increase in non-motile sperm and in sperm DNA fragmentation. (Avendanoet al., 2011)
The fact that multiple recent studies have demonstrated the ability of microwaveRF exposure to cause nonthermal damage sperm function and sperm DNA with shortexposure times and quite low exposure levels—the FCC exposure limit is 1000 μW/cm2—should be a source of grave concern. The presence of constantly transmittingWiFi networks in homes and schools may be much less innocuous than is generallysupposed.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 48
Comments on Notice of Inquiry, ET Docket No. 13-84

BIBLIOGRAPHY
Abell A, Ernst E, Bonde JP. High sperm density among members of organic farmers’association. Lancet (1994); 343(8911):1498.
Adlkofer F. Risk Evaluation of Potential Environmental Hazards from Low EnergyElectromagnetic Field Exposure Using Sensitive In Vitro Methods. Bioelectromagne-tics (2006); 331-354.
Agarwal A, Deepinder F, Sharma RK, Ranga G, Li J. Effect of cell phone usage on semenanalysis in men attending infertility clinic: an observational study. Fertil Steril(2008); 89(1):124-128.
Atasoy HI, Gunal MY, Atasoy P, Elgun S, Bugdayci G. Immunohistopathologicdemonstration of deleterious effects on growing rat testes of radiofrequency wavesemitted from conventional Wi-Fi devices. J Pediatr Urol (2012); March 30.
Avci B, Akar A, Bilgici B, Tuncel OK. Oxidative stress induced by 1.8 GHz radiofrequency electromagnetic radiation and effects of garlic extract in rats. Int J RadiatBiol (2012); 88(11):799-805.
Avendano C, Mata A, Sanchez Sarmiento CA, Doncel GF. Use of laptop computersconnected to internet through Wi-Fi decreases human sperm motility and in-creases sperm DNA fragmentation. Fertil Steril (2012); 97(1):39-45.
Balmori A. Electromagnetic pollution from phone masts. Effects on wildlife. Pathophysi-ology (2009); 16(2-3):191-199.
Balmori A. Mobile phone mast effects on common frog (Rana temporaria) tadpoles: thecity turned into a laboratory. Electromagn Biol Med (2010a); 29(1-2):31-35.
Balmori A, Hallberg O. The urban decline of the house sparrow (Passer domesticus): apossible link with electromagnetic radiation. Electromagn Biol Med (2007);26(2):141-151.
Balmori A. Possible Effects of Electromagnetic Fields from Phone Masts on a Populationof White Stork. Electromagn Biol Med (2005); 24(2):109-119.
Balmori A. The incidence of electromagnetic pollution on wild mammals: A new“poison” with a slow effect on nature? Environmentalist (2010b); 30(1):90-97.
Blank M. Evidence for Stress Response (Stress Proteins). Bioinitiative Report (2007);Section 7:146-185. http://www.bioinitiative.org/
Blank M, Goodman R. Comment: a biological guide for electromagnetic safety: thestress response. Bioelectromagnetics (2004); 25(8):642-8.
Blank M, Goodman R. Electromagnetic fields stress living cells. Pathophysiology (2009);16(2-3):71-78.
Bonde JP, Ernst E, Jensen TK et al. Relation between semen quality and fertility: a popu-lation-based study of 430 first-pregnancy planners. Lancet (1998);352(9135):1172-1177.
Calabro E, Condello S, Curro M et al. Modulation of heat shock protein response in SH-SY5Y by mobile phone microwaves. World J Biol Chem (2012); 3(2):34-40.
Cam ST, Seyhan N. Single-strand DNA breaks in human hair root cells exposed tomobile phone radiation. Int J Radiat Biol (2012); 88(5):420-424.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 49
Comments on Notice of Inquiry, ET Docket No. 13-84

Cao Y, Xu Q, Jin ZD, Zhou Z, Nie JH, Tong J. Induction of adaptive response: pre-expo-sure of mice to 900 MHz radiofrequency fields reduces hematopoietic damagecaused by subsequent exposure to ionising radiation. Int J Radiat Biol (2011);87(7):720-728.
Carlsen E, Giwercman A, Keiding N, Skakkebaek NE. Evidence for decreasing qualityof semen during past 50 years. BMJ (1992); 305(6854):609-613.
Carlsen E, Giwercman A, Keiding N, Skakkebaek NE. Declining semen quality andincreasing incidence of testicular cancer: is there a common cause? Environ HealthPerspect (1995); 103(Suppl 7):137-139.
Chavdoula ED, Panagopoulos DJ, Margaritis LH. Comparison of biological effectsbetween continuous and intermittent exposure to GSM-900-MHz mobile phoneradiation: Detection of apoptotic cell-death features. Mutat Res (2010);700(1-2):51-61.
Cherry N. Health Effects in the vicinity of Radio/TV towers and mobile phone basestations. (2002a):1-40. http://www.neilcherry.com/documents.php
Cherry N. Childhood Cancer in the vicinity of the Sutro Tower, San Francisco.(2002b):1-22. http://www.neilcherry.com/documents.php
Davis RL, Mostofi FK. Cluster of testicular cancer in police officers exposed to hand-held radar. Am J Ind Med (1993); 24(2):231-233.
De Iuliis GN, Newey RJ, King BV, Aitken RJ. Mobile phone radiation induces reactiveoxygen species production and DNA damage in human spermatozoa in vitro.PLoS One (2009); 4(7):e6446 (1-9).
DiCarlo AL, Farrell JM, Litovitz TA. A simple experiment to study electromagnetic fieldeffects: protection induced by short-term exposures to 60 Hz magnetic fields. Bioe-lectromagnetics (1998); 19(8):498-500.
DiCarlo AL, Farrell JM, Litovitz TA. Myocardial protection conferred by electromag-netic fields. Circulation (1999); 99(6):813-816.
Dode AC, Leao MM, Tejo Fde A et al. Mortality by neoplasia and cellular telephonebase stations in the Belo Horizonte municipality, Minas Gerais state, Brazil. SciTotal Environ (2011); 409(19):3649-3665.
Dolk H, Elliott P, Shaddick G, Walls P, Thakrar B. Cancer incidence near radio and tele-vision transmitters in Great Britain. II. All high power transmitters. Am J Epidemiol(1997a); 145(1):10-17.
Dolk H, Shaddick G, Walls P et al. Cancer incidence near radio and television transmit-ters in Great Britain. I. Sutton Coldfield transmitter. Am J Epidemiol (1997b);145(1):1-9.
Eger H, Hagen K, Lucas B, Vogel P, Voit H. The Influence of Being Physically Near to aCell Phone Transmission Mast on the Incidence of Cancer. Umwelt·Medizin·Gesell-schaft (2004); 17(4):1-7.
Erogul O, Oztas E, Yildirim I et al. Effects of electromagnetic radiation from a cellularphone on human sperm motility: an in vitro study. Arch Med Res (2006);37(7):840-843.
Fejes I, Zavaczki Z, Szollosi J et al. Is there a relationship between cell phone use andsemen quality? Arch Androl (2005); 51(5):385-393.
Finkelstein MM. Cancer incidence among Ontario police officers. Am J Ind Med (1998);34(2):157-162.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 50
Comments on Notice of Inquiry, ET Docket No. 13-84

Garland FC, Shaw E, Gorham ED, Garland CF, White MR, Sinsheimer PJ. Incidence ofleukemia in occupations with potential electromagnetic field exposure in UnitedStates Navy personnel. Am J Epidemiol (1990); 132(2):293-303.
Georgiou C. Oxidative stress-induced biological damage by low-level EMFs: mecha-nism of free radical pair electron spinpolarization and biochemical amplification.In: Giuliani L, Soffritti M, eds. Non-thermal Effects and Mechanisms of InteractionBetween Electromagnetic Fields and Living Matter -- An ICEMS Monograph.Fidenza, Italy: Mattioli, (2010):63-113. http://www.ramazzini.it/ricerca/publications.asp
Goldsmith JR. Epidemiologic Evidence of Radiofrequency Radiation (Microwave)Effects on Health in Military, Broadcasting, and Occupational Studies. Int J OccupEnviron Health (1995); 1(1):47-57.
Goldsmith JR. Epidemiologic evidence relevant to radar (microwave) effects. EnvironHealth Perspect (1997a); 105(Suppl 6):1579-1587.
Goldsmith JR. TV broadcast towers and cancer: the end of innocence for radiofrequencyexposures. Am J Ind Med (1997b); 32(6):689-692.
Grayson JK. Radiation exposure, socioeconomic status, and brain tumor risk in the USAir Force: a nested case-control study. Am J Epidemiol (1996); 143(5):480-486.
Guler G, Tomruk A, Ozgur E et al. The effect of radiofrequency radiation on DNA andlipid damage in female and male infant rabbits. Int J Radiat Biol (2012);88(4):367-373.
Gundestrup M, Storm HH. Radiation-induced acute myeloid leukaemia and othercancers in commercial jet cockpit crew: a population-based cohort study. Lancet(1999); 354(9195):2029-2031.
Guzick DS, Overstreet JW, Factor-Litvak P et al. Sperm morphology, motility, andconcentration in fertile and infertile men. N Engl J Med (2001); 345(19):1388-1393.
Ha M, Im H, Lee M et al. Radio-frequency radiation exposure from AM radio transmit-ters and childhood leukemia and brain cancer. Am J Epidemiol (2007);166(3):270-279.
Haimov-Kochman R, Har-Nir R, Ein-Mor E et al. Is the quality of donated semen deteri-orating? Findings from a 15 year longitudinal analysis of weekly sperm samples.Isr Med Assoc J (2012); 14(6):372-377.
Hamzany Y, Feinmesser R, Shpitzer T et al. Is Human Saliva an Indicator of theAdverse Health Effects of Using Mobile Phones? Antioxid Redox Signal (2012); ePubahead of print.
Hocking B, Gordon I, Hatfield G, Grain H. Re: “Cancer incidence near radio and televi-sion transmitters in Great Britain. I. Sutton Coldfield transmitter. II. All high powertransmitters”. Am J Epidemiol (1998); 147(1):90-91.
Hocking B, Gordon IR, Grain HL, Hatfield GE. Cancer incidence and mortality andproximity to TV towers. Med J Aust (1996); 165(11-12):601-605.
Irvine DS. Declining sperm quality: a review of facts and hypotheses. Baillieres ClinObstet Gynaecol (1997); 11(4):655-671.
Ivancsits S, Diem E, Jahn O, Rudiger HW. Intermittent extremely low frequency electro-magnetic fields cause DNA damage in a dose-dependent way. Int Arch OccupEnviron Health (2003); 76(6):431-436.
Jensen TK, Giwercman A, Carlsen E, Scheike T, Skakkebaek NE. Semen quality amongmembers of organic food associations in Zealand, Denmark. Lancet (1996);347(9018):1844.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 51
Comments on Notice of Inquiry, ET Docket No. 13-84

Jiang B, Nie J, Zhou Z, Zhang J, Tong J, Cao Y. Adaptive response in mice exposed to900 MHz radiofrequency fields: primary DNA damage. PLoS One (2012);7(2):e32040.
Jorgensen N, Vierula M, Jacobsen R et al. Recent adverse trends in semen quality andtestis cancer incidence among Finnish men. Int J Androl (2011); 34(4 Pt 2):e37-e48.
Kesari KK, Behari J. Microwave exposure affecting reproductive system in male rats.Appl Biochem Biotechnol (2010); 162(2):416-428.
Kesari KK, Behari J. Evidence for mobile phone radiation exposure effects on reproduc-tive pattern of male rats: role of ROS. Electromagn Biol Med (2012); 31(3):213-222.
Kesari KK, Behari J, Kumar S. Mutagenic response of 2.45 GHz radiation exposure onrat brain. Int J Radiat Biol (2010a); 86(4):334-343.
Kesari KK, Kumar S, Behari J. Mobile phone usage and male infertility in Wistar rats.Indian J Exp Biol (2010b); 48(10):987-992.
Kesari KK, Kumar S, Behari J. Effects of radiofrequency electromagnetic wave exposurefrom cellular phones on the reproductive pattern in male Wistar rats. Appl BiochemBiotechnol (2011); 164(4):546-559.
Kesari KK, Kumar S, Behari J. Pathophysiology of microwave radiation: effect on ratbrain. Appl Biochem Biotechnol (2012); 166(2):379-388.
Khurana VG, Hardell L, Everaert J, Bortkiewicz A, Carlberg M, Ahonen M. Epidemiolo-gical evidence for a health risk from mobile phone base stations. Int J OccupEnviron Health (2010); 16(3):263-267.
Kumar G. Report on Cell Tower Radiation Submitted to Secretary, DOT, Delhi. (2010):1-50. http://www.ee.iitb.ac.in/~mwave/GK-cell-tower-rad-report-DOT-Dec2010.pdf
Kumar S, Behari J, Sisodia R. Influence of electromagnetic fields on reproductive systemof male rats. Int J Radiat Biol (2012); epub Nov 13:1-8
Kumar S, Kesari KK, Behari J. Evaluation of genotoxic effects in male Wistar ratsfollowing microwave exposure. Indian J Exp Biol (2010); 48(6):586-592.
Kumar S, Kesari KK, Behari J. Influence of microwave exposure on fertility of male rats.Fertil Steril (2011); 95(4):1500-1502.
Lai H. Evidence for Genotoxic Effects (RFR and ELF Genotoxicity). Bioinitiative Report(2007); Section 6:1-43. http://www.bioinitiative.org/
Lai H, Singh NP. Magnetic-field-induced DNA strand breaks in brain cells of the rat.Environ Health Perspect (2004); 112(6):687-694.
Levitt B, Lai H. Biological effects from exposure to electromagnetic radiation emitted bycell tower base stations and other antenna arrays. Environ Rev (2010);18(NA):369-395.
Li CY, Liu CC, Chang YH, Chou LP, Ko MC. A population-based case-control study ofradiofrequency exposure in relation to childhood neoplasm. Sci Total Environ(2012); 435-436:472-478.
Liboff A. Weak low-frequency electromagnetic fields are biologically interactive. In:Giuliani L, Soffritti M, eds. Non-thermal Effects and Mechanisms of InteractionBetween Electromagnetic Fields and Living Matter -- An ICEMS Monograph.Fidenza, Italy: Mattioli, (2010): 51-61. http://www.ramazzini.it/ricerca/publications.asp
Lilienfeld AM LGM, Cauthen J, Tonascia S, Tonascia J. Evaluation of health status offoreign service and other employees from selected eastern European embassies.Foreign Service Health Status Study, Final Report; Contract No. 6025-619037 (NTISpublication P8-288 163/9) (1979); 1-447.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 52
Comments on Notice of Inquiry, ET Docket No. 13-84
Lin H, Blank M, Goodman R. A magnetic field-responsive domain in the human HSP70promoter. J Cell Biochem (1999); 75(1):170-176.
Lin H, Han L, Blank M, Head M, Goodman R. Magnetic field activation of protein-DNAbinding. J Cell Biochem (1998); 70(3):297-303.
Lin H, Opler M, Head M, Blank M, Goodman R. Electromagnetic field exposure inducesrapid, transitory heat shock factor activation in human cells. J Cell Biochem (1997);66(4):482-488.
Lin RS, Dischinger PC, Conde J, Farrel KP. Report on the relationship between the inci-dence of brain tumors and occupational electromagnetic exposure. J Occup Med(1985); 27:413-419.
Lu YS, Huang BT, Huang YX. Reactive Oxygen Species Formation and Apoptosis inHuman Peripheral Blood Mononuclear Cell Induced by 900 MHz Mobile PhoneRadiation. Oxid Med Cell Longev (2012); Article ID 740280:1-8.
Maaroufi K, Save E, Poucet B, Sakly M, Abdelmelek H, Had-Aissouni L. Oxidativestress and prevention of the adaptive response to chronic iron overload in thebrain of young adult rats exposed to a 150 kilohertz electromagnetic field. Neuro-science (2011); 186:39-47.
Magras IN, Xenos TD. RF radiation-induced changes in the prenatal development ofmice. Bioelectromagnetics (1997); 18(6):455-461.
Maskarinec G, Cooper J, Swygert L. Investigation of increased incidence in childhoodleukemia near radio towers in Hawaii: preliminary observations. J Environ PatholToxicol Oncol (1994); 13(1):33-37.
Meo SA, Al-Drees AM, Husain S, Khan MM, Imran MB. Effects of mobile phone radia-tion on serum testosterone in Wistar albino rats. Saudi Med J (2010); 30(8):869-873.
Michelozzi P, Capon A, Kirchmayer U et al. Adult and childhood leukemia near a high-power radio station in Rome, Italy. Am J Epidemiol (2002); 155(12):1096-1103.
Milham SJ. Silent keys: leukaemia mortality in amateur radio operators. Lancet (1985a);1(8432):812.
Milham SJ. Mortality in workers exposed to electromagnetic fields. Environ Health Pers-pect (1985b); 62:297-300.
Milham SJ. Increased mortality in amateur radio operators due to lymphatic and hema-topoietic malignancies. Am J Epidemiol (1988a); 127(1):50-54.
Milham SJ. Mortality by license class in amateur radio operators. (1988b);128(5):1175-1176.
Nordkap L, Joensen UN, Blomberg Jensen M, Jorgensen N. Regional differences andtemporal trends in male reproductive health disorders: semen quality may be asensitive marker of environmental exposures. Mol Cell Endocrinol (2012);355(2):221-230.
Oberfeld G. Environmental Epidemiological Study of Cancer Incidence in the Munici-palities of Hausmannstätten & Vasoldsberg (Austria). Provincial Government ofStyria, Department 8B, Provincial Public Health Office, Graz, Austria (2008):1-10.http://www.emf-health.com/PDFreports/Austrianstudy.pdf
Otitoloju AA, Obe IA, Adewale OA, Otubanjo OA, Osunkalu VO. Preliminary study onthe induction of sperm head abnormalities in mice, Mus musculus, exposed toradiofrequency radiations from global system for mobile communication basestations. Bull Environ Contam Toxicol (2010); 84(1):51-54.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 53
Comments on Notice of Inquiry, ET Docket No. 13-84

Panagopoulos DJ, Karabarbounis A, Margaritis LH. Effect of GSM 900-MHz mobilephone radiation on the reproductive capacity of Drosophila melanogaster. Electro-magnetic biology and medicine (2004); 23(1):29-43.
Panagopoulos DJ. Effect of microwave exposure on the ovarian development ofDrosophila melanogaster. Cell Biochem Biophys (2012); 63(2):121-132.
Panagopoulos DJ, Chavdoula ED, Margaritis LH. Bioeffects of mobile telephony radia-tion in relation to its intensity or distance from the antenna. Int J Radiat Biol (2010);86(5):345-357.
Panagopoulos DJ, Chavdoula ED, Nezis IP, Margaritis LH. Cell death induced by GSM900-MHz and DCS 1800-MHz mobile telephony radiation. Mutat Res (2007);626(1-2):69-78.
Panagopoulos DJ, Margaritis LH. The effect of exposure duration on the biological acti-vity of mobile telephony radiation. Mutat Res (2010); 699(1-2):17-22.
Phillips JL, Singh NP, Lai H. Electromagnetic fields and DNA damage. Pathophysiology(2009); 16(2-3):79-88.
Rafnsson V, Hrafnkelsson J, Tulinius H. Incidence of cancer among commercial airlinepilots. Occup Environ Med (2000); 57(3):175-179.
Randolph TG. Human Ecology and Susceptibility to the Chemical Environment.Charles C Thomas, Springfield IL (1962); 1-148.
Robinette CD, Silverman C, Jablon S. Effects upon health of occupational exposure tomicrowave radiation (radar). Am J Epidemiol (1980); 112(1):39-53.
Rolland M, Le Moal J, Wagner V, Royère D, De M, J. Decline in semen concentrationand morphology in a sample of 26 609 men close to general population between1989 and 2005 in France. Human Reproduction (2012); Dec 4 ahead of print.
Ruediger HW. Genotoxic effects of radiofrequency electromagnetic fields. Pathophysio-logy (2009); 16(2-3):89-102.
Schwarz C, Kratochvil E, Pilger A, Kuster N, Adlkofer F, Rudiger HW. Radiofrequencyelectromagnetic fields (UMTS, 1,950 MHz) induce genotoxic effects in vitro inhuman fibroblasts but not in lymphocytes. Int Arch Occup Environ Health (2008);81(6):755-767.
Sharpe RM, Skakkebaek NE. Are oestrogens involved in falling sperm counts and dis-orders of the male reproductive tract? Lancet (1993); 341(8857):1392-1395.
Shine R, Peek J, Birdsall M. Declining sperm quality in New Zealand over 20 years. N ZMed J (2008); 121(1287):50-56.
Shiroff V. DNA and Chromosome Damage: A Crucial non-thermal Biological Effect ofMicrowave Radiation. In Effects of Wireless Communication Technologies (Broc-hure 3): How Susceptible are Genes to Mobile Phone Radiation? Competence Initi-ative for the Protection of Humanity, Environment and Democracy (2008):1-61.http://www.kompetenzinitiative.net/broschuerenreihe/brochure-series/english/index.html
Slama R, Eustache F, Ducot B et al. Time to pregnancy and semen parameters: a cross-sectional study among fertile couples from four European cities. Hum Reprod(2002); 17(2):503-515.
Swan SH, Elkin EP. Declining semen quality: can the past inform the present? Bioessays(1999); 21(7):614-621.
Swan SH, Elkin EP, Fenster L. The question of declining sperm density revisited: ananalysis of 101 studies published 1934-1996. Environ Health Perspect (2000);108(10):961-966.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 54
Comments on Notice of Inquiry, ET Docket No. 13-84

Szmigielski S. Cancer morbidity in subjects occupationally exposed to high frequency(radiofrequency and microwave) electromagnetic radiation. Sci Total Environ(1996); 180(1):9-17.
Thomas TL, Stolley PD, Stemhagen A et al. Brain tumor mortality risk among men withelectrical and electronics jobs: a case-control study. J Natl Cancer Inst (1987);79(2):233-238.
Tynes T, Hannevik M, Andersen A, Vistnes AI, Haldorsen T. Incidence of breast cancerin Norwegian female radio and telegraph operators. Cancer Causes Control (1996);7(2):197-204.
Weisbrot D, Lin H, Ye L, Blank M, Goodman R. Effects of mobile phone radiation onreproduction and development in Drosophila melanogaster. J Cell Biochem (2003);89(1):48-55.
Wolf R, Wolf D. Increased Incidence of Cancer Near a Cell-Phone Transmitter Station.International Journal of Cancer Prevention (2004); 1(2):1-19.
Yakymenko I, Sidorik E, Kyrylenko S, Chekhun V. Long-term exposure to microwaveradiation provokes cancer growth: evidences from radars and mobile communica-tion systems. Exp Oncol (2011); 33(2):62-70.
Zeeb H, Hammer GP, Langner I, Schafft T, Bennack S, Blettner M. Cancer mortalityamong German aircrew: second follow-up. Radiat Environ Biophys (2010);49(2):187-194.
SECTION 4 – OXIDATIVE STRESS, DNA DAMAGE, CANCER AND INFERTILITY
Page 55
Comments on Notice of Inquiry, ET Docket No. 13-84

Page 56
Comments on Notice of Inquiry, ET Docket No. 13-84

CURRENT RESEARCH ONCELL PHONE USE AND BRAIN TUMOR RISK
INTRODUCTIONTo be complete, any review of the health hazards of microwave radio exposures
must include a discussion of the research on possible associations between cell phoneusage and brain tumors.
This research is a hot topic politically. Cell phone use has permeated our society,and no one wants to think that use of a cell phone is going to increase their personal risk(or their child’s personal risk) of acquiring a terrifying disease.
The rollout of the cellular communications infrastructure has also created anextremely profitable industry. The telecommunications industry made $3.1 trillion ingross profits in 2010. (Plunkett Research, 2012) This industry has a powerful incentiveto downplay the health effects of EMF, and has funded a good deal of research thatserves to further that aim. Some studies regarding cell phones and brain tumors havebeen funded in large part by the telecommunications industry. These industry-designed studies have generally concluded that the use of cell phones does not create ahealth hazard. And these negative reports have received wide coverage in the newsmedia. However, the study designs funded by industry are more likely to useunblinded protocols and to underestimate risk, as compared to studies funded bypublic bodies. (Levis et al., 2012)
When powerful financial interests are at play, industry funding of favorableresearch studies is often used to influence the political and scientific playing field.We’ve seen this play out in pharmaceutical research, where several recent scandals havehighlighted the distorting effects of corporate financing on research outcomes. In thepast few decades the production of research providing favorable (to corporate interests)results has become something of a science in itself, with corporations essentially gamingthe academic system, funding studies designed to produce favorable outcomes for theirproducts, and hiding studies that do not support their interests. The peer reviewprocess of the scientific journals has not proved to be an adequate defence against thisproblem. (Smith, 2005)
In the research on cell phones and brain tumors, the situation is furtherconfounded by the fact that cell phone usage has only become wide spread in the last 15years or so. The first digital cell phone infrastructure was pioneered in Scandinavia,and the first research that raised concerns about cell phone cancer risks was producedin Sweden in the late 1990’s. But environmental influences that promote cancer gene-rally take years to do so.
Take the question of the potential risk of cell phone use by teenagers. Does thiscell phone use increase the risk of brain tumors later in life? The mass market for cellphone use by teenagers really started after 1995, and extended use of cell phones to surfthe web ballooned after the introduction of the iPhone in 2007. Looking for brain cancertoday in 30 year olds who started using a cell phone in 1997 would be similar to lookingfor lung cancer today in 30 year olds who started smoking in 1997 (and who would bemost likely to develop lung cancer in their 50’s or 60’s).
This means we cannot find great reassurance in “negative” cell phone cancer riskstudies performed 8 or 10 years ago. And similarly, any “positive” findings of cellphone cancer risk to date should produce real concern, since it is possible that they areidentifying only the early cases of a larger problem.
Page 57
Comments on Notice of Inquiry, ET Docket No. 13-84

Three major and ongoing research studies have been performed in the last 10years. One is the INTERPHONE Study, which is funded in major part by the telecom-munications industry. A second study which received much recent media attention isthe “Danish Cohort” study. A third body of research has been produced by the Hardellgroup in Sweden, a research group with no financial support from the telecommunica-tions industry.
THE INTERPHONE STUDYThe INTERPHONE Study is a large standard protocol study of brain and sali-
vary gland tumor risk in relation to mobile telephone use, with branches of the studybeing performed in 13 countries, and combined together to increase the statisticalpower of the results. This study was funded in major part by the wireless communica-tions industry.
The first major summary of this research was published in 2010. This “case-control” study looked at patients with brain tumors (2708 glioma cases, 2409 menin-gioma cases) and matched controls, and compared their estimated cell phone usage todetermine if regular cell phone usage increased the odds of being a brain tumor patient.The authors concluded that “Overall, no increase in risk of either glioma or menin-gioma was observed in association with use of mobile phones.” (Group, 2010)
This reported result was then widely quoted by the press and government agen-cies like the World Health Organization (IARC, 2010) as demonstrating the lack of riskof wireless technology.
However, this study defined a member of the risk group as any subject who “hadan average of at least one call per week for a period of 6 months”. This definition of “regularcell phone use” diluted the risk pool out with lower risk individuals to the point that nodifference between risk and control groups was visible in the study.
Interestingly, the study did report its statistics stratified by total time of reporteduse, and the top decile (greater than 1640 hours use over a ten year interval, averagingout as greater than 3 hours a week) had an increased risk of certain tumors. Individualswho accrued that greater than 1650 hours of use over a 1 to 4 year interval (rangingfrom 8 to over 30 hours a week) had a markedly higher odds ratio of meningioma (OR4.80) or glioma (OR 3.27).
In the discussion of their data showing increased risk within the higher usagegroup, the authors failed to consider the possibility that this data showed a real risk.Instead, they discounted this trend of increased risk in the heavier users, stating thatvarious “biases and errors limit the strength of the conclusions we can draw from theseanalyses and prevent a causal interpretation.” And it is this “biases and error’s”comment that has been quoted by industry apologists in subsequent publications,rather than the study’s actual statistical findings of increased odds of brain tumor withcell phone talk time greater than 3 hours a week over a ten year period, or greater than8 hours a week over a 1 to 4 year period.
The discrepancy between actual data and concluding discussion in this studywas not highlighted by mass media coverage of this study. One must assume thatreporters read the abstract rather than the complete article, and accepted the author’sconclusions without question. Other researchers in the field were more critical in theirassessments of the INTERPHONE project as compared to other published literature onthe subject (Morgan, 2009), and pointed out that the INTERPHONE data really did
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 58
Comments on Notice of Inquiry, ET Docket No. 13-84

document an increased risk, consistent with studies published by researchers in thefield that were more independent from industry funding sources. (Hardell et al., 2011a)(Levis et al., 2011)
A more recent study from the INTERPHONE group found an increased risk foracoustic neuroma in individuals with > 1640 hours of talk time over up to 5 years ofexposure (OR = 2.79, 95% CI = 1.51 – 5.16). For those subjects who routinely used theircell phone on the same side of the head where they had the acoustic neuroma, the oddsratio was 3.74 (95% CI 1.58 – 8.83). (Cardis and Schüz, 2011)
The most recent study from the INTERPHONE group showed increased oddsratio of glioma and meningioma with greater than 10 years of mobile phone use. Theauthor’s conclusions acknowledged this finding, but stated that “the uncertainty ofthese results requires that they be replicated before a causal interpretation can bemade”. This is an interesting comment, considering that this study result itself wasessentially a replication of the actual findings of the earlier INTERPHONE study.(Cardis et al., 2011)
THE DANISH STUDYA study from Denmark on the risk of mobile phones and brain tumors was
published in the British Medical Journal in 2011. The conclusions of this study werethat “there were no increased risks of tumors of the central nervous system, providinglittle evidence for a causal association”. (Frei et al., 2011)
This study was widely quoted in the media and by government organizations asrefuting the link between cell phones and brain tumors, with headlines like BBC News:“Mobile phone brain cancer link rejected.” (Triggle, 2011)
In this case-control study, the risk group was composed of native Danes who hadacquired a cell phone contract prior to 1995. However, any prior to 1995 corporateusers were excluded from the risk group (this was 32% of the original cohort). Alsoexcluded were all prior to 1995 subscribers who were less than 18 years old at the timethey obtained their first subscription. The study did not determine how often membersof the risk group used their phones, or make any determination as to exposure toportable phones in the home for risk or control group members.
The control group was composed of all Danes aged 30 or older and born after1925 in Denmark. This of course means that the control group included all the earlycorporate subscribers (whom we might call the “power users”), and also included the85% of Danes who obtained a cell phone after 1995.
This contamination of the control group with large numbers of cell phone usersmade the conclusions of the study essentially meaningless. To the BMJ’s credit, lettersthat pointed this out were printed in the same issue with the original article (but appa-rently not read by the members of the press). (Khurana, 2011) (Philips and Lamburn,2011)
The net result of all this was that the public was falsely reassured by mediareports of a peer reviewed article in a prestigious medical journal, when the negativeconclusions of that article were essentially meaningless. (Soderqvist et al., 2012)
THE HARDELL GROUP STUDIESThe first digital cell phone network (2G) was launched in Finland in 1991, and
the cell phone communication infrastructure expanded widely in Scandinavia duringthat decade. In the late 1990’s case reports of brain tumors in cell phone users lead to
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 59
Comments on Notice of Inquiry, ET Docket No. 13-84

the first of multiple studies produced by the Hardell research group in Sweden. In thiscase control study of data collected between 1994 and 1996 from 233 living patients withbiopsy-verified brain tumors, no clear distinction could be established between cellphone users and nonusers in the patient population, but a trend was observed of in-creased odds of tumor presence in the temporal or occipital lobe on the same side of thehead habitually used to listen to the cell phone. (Hardell et al., 1999)
In 2002 Hardell et al. published another and larger case control study of 649brain tumor cases diagnosed between January 1997 and June 2000. This study (andsubsequent studies by the Hardell group) looked at exposure from both cellular phonesand mobile (cordless) phones connected to land lines. Cumulative hours of cell phoneuse was calculated from questionnaires about phone usage habits. Increased risk ofbrain tumor was found for ipsilateral use (phone habitually on same side of head asbrain tumor site) with both analogue and digital cellular phones and for cordlessphones. Increased risk was also seen for increased duration of exposure. (Hardell et al.,2002)
Another expanded case control study with 1617 brain tumor patients diagnosedbetween 1997 and 2000 was published later that year showed similar findings, with thehighest calculated risk being for ipsilateral acoustic neuroma in analog cellular phoneusers (the older technology). (Hardell et al., 2002)
Hardell et al. analyzed this same data set of 1617 patients for incidence of vesti-bular schwannoma (VS), and found an increased odds ratio for VS associated with theuse of analogue cell phones. They found that the incidence of VS in Sweden had signifi-cantly increased during the time period from 1960 to 1998, with more of this increaseoccurring during from 1980 to 1998. All other brain tumors taken together had alsoshowed a significant yearly increase between 1960 and 1998. (Hardell et al., 2003)(Hardell et al., 2003)
In 2006 and 2007, Hardell et al. published several more studies of brain tumorpatients diagnosed between 1997 and 2003. Cell phones had been in wide use for alonger interval of time, and their data allowed evaluation of latency periods of > 10years duration, and risk for subjects with first cell phone use at < 20 years of age.Cumulative lifetime use of > 2,000 hours showed elevated odds ratios for analog,digital, and cordless phones, and increased risk for malignant tumors with ipsilateralexposure. Risk of malignant tumors was more pronounced in individuals with first cellphone use at less than 20 years of age. (Hardell et al., 2006) (Hardell et al., 2006a)(Hardell et al., 2006b) (Mild et al., 2007)
Later in 2006, Hardell et al. published a pooled review of their data from all six oftheir previous case control studies. (Hardell et al., 2006) And they have subsequentlypublished three more papers updating and consolidating their earlier findings. (Hardelland Carlberg, 2009) (Hardell et al., 2010) (Hardell et al., 2011b)
CRITIQUES AND REVIEWSIn 2004 Kundi et al. published a review of 9 existing epidemiologic studies on the
relationship between cell phone use and brain tumor risk, and found that all studiesapproaching reasonable latencies of exposure time showed an increased relative risk(range 1.3 to 4.6) of brain tumor in cell phone users, with highest overall risk foracoustic neuroma (RR 3.5) and uveal melanoma (RR 4.2) (Kundi et al., 2004)
In 2007 Hardell et al. published a meta-analysis of two cohort studies and 15 case
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 60
Comments on Notice of Inquiry, ET Docket No. 13-84
control studies on the association between long-term use of cell phones and braintumor. They found increased risk for acoustic neuroma and glioma with ≥ 10 years ofexposure, with higher risk of tumor on the exposed side of the head. (Hardell et al.,2007a)
Hardell, Mild, and Kundi published exhaustive reviews of the existing literatureon this subject in 2007 in the Bioinitiative Report. (Hardell et al., 2007b) (Kundi, 2007)
In 2008, Hardell et al. published two meta-analyses of the existing case controlstudies in the literature including ten studies on glioma and nine studies on acousticneuroma. They found “a consistent pattern of association between mobile phone useand ipsilateral glioma and acoustic neuroma using ≥ 10 years latency period”. (Hardellet al., 2008)
In another meta-analysis published in 2009, Hardell et al. again found “a consis-tent pattern of an increased risk for glioma and acoustic neuroma after > 10 year mobilephone use . . . with highest risk found in the age group < 20 years at time of first use ofwireless phones.” (Hardell et al., 2009)
In a 2009 review, Ahlbom et al. stated that existing studies “do not demonstratean increased risk within approximately 10 years of use for any tumor of the brain”. In away, this statement is a somewhat backhanded acknowledgement of the fact that thepublished research to that date clearly does show increased risk with greater than 10years of use. (Ahlbom et al., 2009)
In 2009 Khurana et al. published a metanalysis of the eleven existing long-termepidemiologic studies on cell phone use and brain tumor risk that met these criteria:Publication in a peer reviewed journal; inclusion of subjects with greater than 10 yearsof cell phone use; analyzing “laterality” of cell phone usage in relation to brain tumorincidence. Their conclusion was that “using a cell phone for ≥ 10 years approximatelydoubles the risk of being diagnosed with a brain tumor on the same (“ipsilateral”) sideof the head as that preferred for cell phone use”. (Khurana et al., 2009)
In 2011 the WHO/International Agency for Research on Cancer (IARC) classifiedradiofrequency electromagnetic fields as “possibly carcinogenic to humans (Group 2B),based on an increased risk for glioma, a malignant type of brain cancer, associated withwireless phone use”. (WHO, 2011) (Baan et al., 2011)
In 2012, Levis et al. published an analysis of published case control studies,pooled analyses, and meta-analyses on head tumor risk with mobile phone use. Theyfound that “in studies funded by public bodies, blind protocols give positive resultsrevealing cause-effect relationships between long-term latency or use of mobile phones(cellulars and cordless) and statistically significant increases of ipsilateral risk of braingliomas and acoustic neuromas, with biological plausibility. In studies funded or co-funded by the cellphone companies non-blind protocols give overall negative resultswith systematic underestimation of risk; however, also in these studies a statisticallysignificant increase in risk of ipsilateral brain gliomas, acoustic neuromas, and parotidgland tumours is quite common when only subjects with at least 10 years of latency orexposure to mobile phones (only cellulars) are considered.” (Levis et al., 2012)
CONCLUSIONSThe current epidemiological research shows that greater than 10 years of cell
phone use incurs a significantly increased risk of ipsilateral brain tumor (glioma ormeningioma). This risk is greater in individuals that start using cell phones as children.
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 61
Comments on Notice of Inquiry, ET Docket No. 13-84

This means that the RF exposure guidelines for cell phone use cannot be consi-dered to be adequately protecting the public.
In light of these findings, current public policy that essentially ignores biologicalor “nonthermal” levels of RF exposure need to be reconsidered and revised, in order tosignificantly reduce the risk to the public health that is produced by these technologies.
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 62
Comments on Notice of Inquiry, ET Docket No. 13-84

BIBLIOGRAPHY
Ahlbom A, Feychting M, Green A, Kheifets L, Savitz DA, Swerdlow AJ. Epidemiologicevidence on mobile phones and tumor risk: a review. Epidemiology (2009);20(5):639-652.
Baan R, Grosse Y, Lauby-Secretan B et al. Carcinogenicity of radiofrequency electro-magnetic fields. Lancet Oncol (2011); 12(7):624-626.
Cardis E, Armstrong BK, Bowman JD et al. Risk of brain tumours in relation to esti-mated RF dose from mobile phones: results from five Interphone countries. OccupEnviron Med (2011); 68(9):631-640.
Cardis E, Schüz J. Acoustic neuroma risk in relation to mobile telephone use: results ofthe INTERPHONE international case-control study. Cancer Epidemiol (2011);35(5):453-464.
Frei P, Poulsen AH, Johansen C, Olsen JH, Steding-Jessen M, Schuz J. Use of mobilephones and risk of brain tumours: update of Danish cohort study. BMJ (2011);343(d6387.
Hardell L, Nasman A, Pahlson A, Hallquist A, Hansson Mild K. Use of cellular telep-hones and the risk for brain tumours: A case-control study. Int J Oncol (1999);15(1):113-116.
Hardell L, Hallquist A, Mild KH, Carlberg M, Pahlson A, Lilja A. Cellular and cordlesstelephones and the risk for brain tumours. Eur J Cancer Prev (2002); 11(4):377-386.
Hardell L, Mild KH, Carlberg M. Case-control study on the use of cellular and cordlessphones and the risk for malignant brain tumours. Int J Radiat Biol (2002);78(10):931-936.
Hardell L, Mild KH, Carlberg M. Further aspects on cellular and cordless telephonesand brain tumours. Int J Oncol (2003); 22(2):399-407.
Hardell L, Hansson Mild K, Sandstrom M, Carlberg M, Hallquist A, Pahlson A. Vesti-bular schwannoma, tinnitus and cellular telephones. Neuroepidemiology (2003);22(2):124-129.
Hardell L, Carlberg M, Mild KH. Case-control study of the association between the useof cellular and cordless telephones and malignant brain tumors diagnosed during2000-2003. Environ Res (2006); 100(2):232-241.
Hardell L, Mild KH, Carlberg M, Soderqvist F. Tumour risk associated with use ofcellular telephones or cordless desktop telephones. World J Surg Oncol (2006);4(74):1-10.
Hardell L, Carlberg M, Hansson Mild K. Pooled analysis of two case-control studies onthe use of cellular and cordless telephones and the risk of benign brain tumoursdiagnosed during 1997-2003. Int J Oncol (2006a); 28(2):509-518.
Hardell L, Carlberg M, Hansson Mild K. Pooled analysis of two case-control studies onuse of cellular and cordless telephones and the risk for malignant brain tumoursdiagnosed in 1997-2003. Int Arch Occup Environ Health (2006b); 79(8):630-639.
Hardell L, Carlberg M, Soderqvist F, Mild KH, Morgan LL. Long-term use of cellularphones and brain tumours: increased risk associated with use for > or =10 years.Occup Environ Med (2007a); 64(9):626-632.
Hardell L, Mild K, Kundi M. Evidence for Brain Tumors and Acoustic Neuromas. BioI-nitiative Report (2007b); Section 10(2): 317-343. http://www.bioinitiative.org
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 63
Comments on Notice of Inquiry, ET Docket No. 13-84

Hardell L, Carlberg M, Soderqvist F, Hansson Mild K. Meta-analysis of long-termmobile phone use and the association with brain tumours. Int J Oncol (2008);32(5):1097-1103.
Hardell L, Carlberg M. Mobile phones, cordless phones and the risk for brain tumours.Int J Oncol (2009); 35(1):5-17.
Hardell L, Carlberg M, Hansson Mild K. Epidemiological evidence for an associationbetween use of wireless phones and tumor diseases. Pathophysiology (2009);16(2-3):113-122.
Hardell L, Carlberg M, Hansson Mild K. Mobile phone use and the risk for malignantbrain tumors: a case-control study on deceased cases and controls. Neuroepidemio-logy (2010); 35(2):109-114.
Hardell L, Carlberg M, Hansson Mild K. Re-analysis of risk for glioma in relation tomobile telephone use: comparison with the results of the Interphone internationalcase-control study. Int J Epidemiol (2011a); 40(4):1126-1128.
Hardell L, Carlberg M, Hansson Mild K. Pooled analysis of case-control studies onmalignant brain tumours and the use of mobile and cordless phones includingliving and deceased subjects. Int J Oncol (2011b); 38(5):1465-1474.
IARC. Brain tumour risk in relation to mobile telephone use: results of the INTERP-HONE international case-control study. Int J Epidemiol (2010); 39(3):675-694.
INTERPHONE Study Group. Brain tumour risk in relation to mobile telephone use:results of the INTERPHONE international case-control study. Int J Epidemiol (2010);39(3):675-694.
Khurana VG. Questions about selection, exposure, and tumour incidence. BMJ (2011);343(d7893; author reply d7912.
Khurana VG, Teo C, Kundi M, Hardell L, Carlberg M. Cell phones and brain tumors: areview including the long-term epidemiologic data. Surg Neurol (2009);72(3):205-14; discussion 214-5.
Kundi M. Evidence for Brain Tumors (Epidemiological). Bioinitiative Report (2007);Section 10(2): 344-380. http://www.bioinitiative.org
Kundi M, Mild K, Hardell L, Mattsson MO. Mobile telephones and cancer--a review ofepidemiological evidence. J Toxicol Environ Health B Crit Rev (2004); 7(5):351-384.
Levis AG, Minicucci N, Ricci P, Gennaro V, Garbisa S. [Mobile phones and headtumours: it is time to read and highlight data in a proper way]. Epidemiol Prev(2011); 35(3-4):188-199.
Levis AG, Minicuci N, Ricci P, Gennaro V, Garbisa S. Mobile Phones and HeadTumours: A Critical Analysis of Case-Control Epidemiological Studies. Open Envi-ronmental Sciences (2012); 6(1-12.
Mild KH, Hardell L, Carlberg M. Pooled analysis of two Swedish case-control studieson the use of mobile and cordless telephones and the risk of brain tumoursdiagnosed during 1997-2003. Int J Occup Saf Ergon (2007); 13(1):63-71.
Morgan LL. Estimating the risk of brain tumors from cellphone use: Published case-control studies. Pathophysiology (2009); 16(2-3):137-147.
Philips A, Lamburn G. Updated study contains poor science and should be disregarded.BMJ (2011); 343(d7899; author reply d7912).
Plunkett Research L. Telecommunications Industry Overview, (2012).http://www.plunkettresearch.com/telecommunications-market-research/industry-statistics
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 64
Comments on Notice of Inquiry, ET Docket No. 13-84

Smith R. Medical Journals Are an Extension of the Marketing Arm of PharmaceuticalCompanies. PLoS Medicine (2005); 2(5):0364-0366.
Soderqvist F, Carlberg M, Hardell L. Review of four publications on the Danish cohortstudy on mobile phone subscribers and risk of brain tumors. Rev Environ Health(2012); 27(1):51-58.
Triggle N. Mobile phone brain cancer link rejected. BBC News, (2011, October 20).http://www.bbc.co.uk/news/health-15387297
WHO. IARC Classifies Radiofrequency Electromagnetic Fields as Possibly Carcinogenicto Humans. World Health Organization, Press Release, 31 May 2011:http://www.iarc.fr/en/media-centre/pr/2011/pdfs/pr208_E.pdf
SECTION 5 – CELL PHONE USE AND BRAIN TUMOR RISK
Page 65
Comments on Notice of Inquiry, ET Docket No. 13-84

Page 66
Comments on Notice of Inquiry, ET Docket No. 13-84

CONCLUSIONS AND RECOMMENDATIONSADVERSE BIOLOGICAL EFFECTS—THE SCIENTIFIC EVIDENCE
In the previous sections we have reviewed the increasingly robust body of scien-tific evidence that excessive RF exposure can cause both acute and chronic adversebiological effects:
ACUTE EFFECTSIn susceptible individuals, excessive RF exposure can provoke acute symptoms.
The most common symptoms are sleep disturbance, headache, irritability, fatigue, andconcentration difficulties. Other symptoms may include depression, dizziness, tinnitus,burning and flushed skin, digestive disturbance, tremor, and cardiac irregularities.
As physicians, some of us have seen patients who are experiencing this problem,and are aware of the connection with RF exposure. Research suggests that 3 to 5% ofthe population fit into this category. If this is the case, there may be 4,700 people inEugene who react to RF exposure in some way, and know it.
These symptoms are not uncommon in the population, of course. And in allprobability there are many other people in Eugene who are having problems withinsomnia or fatigue--problems provoked by EMF exposures--but are unaware of theconnection between cause and effect.
Any significant increase in RF exposure in our residential areas will make theseindividuals more symptomatic. Such increases are likely to push additional individualsabove their tolerance threshold, producing new cases of these problems. If increased RFlevels from repeated daily transmissions between smart meters and their control towerspushed an additional 1% of the community into acute reactivity to RF exposures, thiswould mean an additional 1500 people in our city with insomnia, headaches, fatigue,ringing in the ears, or other debilitating symptoms.
CHRONIC EFFECTSChronic exposure to RF can also cause chronic physiologic changes, including
altered endocrine function (both melatonin and other hormones), and increased oxidantstress that can lead to increased levels of cancer and male infertility. The public isalready being subjected to increased levels of RF from wireless communications. In-creasing the total load of transmission further will increase the occurrence of theseadverse consequences.
PERSPECTIVE AS WE MOVE FORWARDAt the beginning of the last century, people began to use vehicles powered by
internal combustion engines that burned gasoline. Gasoline power was cheap andconvenient, and greatly increased the mobility of the population. And the companiesthat sold the gas and the cars made a lot of money.
This use of fossil fuels has had long term consequences--increased atmosphericCO2 which through the greenhouse effect would lead to global climate change. Initi-ally, these consequences went unrecognized. Then the scientific community began topredict and measure them.
Public acknowledgement of these consequences has gone through several stages.First, the science was ignored. Then the science was attacked or denied by those whoseeconomic interests were threatened by it. Public recognition of the problem is onlyarriving as the long term consequences of climate change are beginning to be felt.
Page 67
Comments on Notice of Inquiry, ET Docket No. 13-84

The use of wireless communications technology is following a similar trajectory.Wireless communication is convenient, and increases our mobility. The installation ofwireless networks is also significantly cheaper than installation of hard-wired networks.And the companies that provide these networks and the tools that we use to accessthem are making a great deal of money.
For decades, the biological consequences of this form of communication wentunrecognized by both the public and the scientific community. As scientific evidence ofbiological and health effects began to emerge, this evidence was initially ignored bygovernment regulating bodies, the media, and the public. As this evidence is gettingharder to ignore, it is now being attacked or denied by the telecommunicationsindustry. Wide public recognition of the problem and the science that describes it willarrive as the problem becomes more severe, and more people get sick.
The previous sections of this report describe the increasing body of science thatclearly demonstrates the existence of adverse biological effects from chronic RF expo-sure. It is important for EWEB’s Board and staff to recognize that this science is real,and that the science isn’t going to go away. As the wireless communications infra-structure continues to grow, the magnitude and duration of public exposure are goingto continue to increase, and the number of people with acute or chronic effects from thisexposure will continue to grow. As recognition of the problem by the public increases,exposures and infrastructure that are currently unquestioned will become politicallyunacceptable.
EWEB has moved slowly in the process of investigating AMI technology. Recog-nition of the potential health effects of excessive RF exposure to the public should causethis appraisal to become even more deliberate and circumspect. EWEB needs to avoidinvesting millions of dollars on infrastructure that becomes part of the problem.Instead, EWEB needs to think about making engineering choices that recognize thisproblem, and seek to become a part of its solution.
RECOMMENDATIONSBASIC PRECEPTS FOR RESIDENTIAL EXPOSURES TO RF TRANSMISSIONS• Excessive RF exposure can cause acute problems (headaches, insomnia, fatigue,
vertigo, tinnitus, other symptoms of EHS).• Excessive RF exposure can also cause chronic problems (oxidative stress, cancer,
male infertility).• Constant RF transmission is probably harmful, even at low levels, and should be
avoided.• Frequent and repetitive intermittent transmissions are also probably harmful,
and should be avoided.• Nocturnal exposures are more problematic than daytime exposures, because of
RF’s potential to suppress nocturnal melatonin secretion and disturb sleep, andbecause night is the time when we rest and heal from stresses (including oxida-tive stress).
• Occasional and infrequent daytime exposures are much less likely to cause anincrease in chronic problems for the population at large.
• Occasional and infrequent daytime exposures are still likely to provoke acutesymptoms in a small percentage of the population.
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 68
Comments on Notice of Inquiry, ET Docket No. 13-84
Based on our review of the existing science, we suggest that the above basicprecepts be considered when thinking about residential exposures to microwave RFtransmissions. We consider this to be important for the population at large, and evenmore important for those in our community who suffer from symptoms of electrohy-persensitivity. For all of us, our homes are the place where we rest and where we sleep,where we rejuvenate ourselves from the stresses of the wider world. It is important thatour residential environments be a place where this can occur. Our homes need to bepart of the solution, not part of the problem.
EWEB SHOULD ADOPT A POLICY OF MINIMIZING THEIR RF FOOTPRINT IN THE COMMUNITY
A recognition of these precepts should lead EWEB to adopting a policy of mini-mizing their infrastructure’s RF footprint in the community as much as possible duringregular operations. This doesn’t mean that staff would throw away their cell phonesand communicate by semaphore. But it would mean that instead of combatting or igno-ring the possibility that more RF in the community could cause harm, EWEB shouldacknowledge the potential risks of excessive residential exposure.
This would mean that such potential risks would be seriously considered in anydiscussion of the total risks and benefits (the “Total Bottom Line”) in deciding whetherto use RF technology for any given purpose. If, after such a discussion, a considereddecision is made to use RF technology, then these same potential risks should be takeninto serious consideration in determining how to use this technology in a manner thatwould minimize potential harm to the community.
In other words, don’t use RF when you don’t have to. Go hard-wired whereverit is feasible to do so. And if you do use RF, design the technology to use as little of it aspossible.
Current engineering choices in AMI technology have not been designed withthese goals in mind, since the industry has not had an practical incentive to recognizethe problem and to “work the problem”. But EWEB as a purchaser of technology couldchoose to push vendors towards designing and providing hardware options that wouldaddress these goals. This would put EWEB in the position of being part of the solutionrather than just another part of the problem.
FLAWS IN THE CONCEPT OF “OPTING OUT”It has been suggested that people who have problems with EHS or concerns
about health exposures to RF can be taken care of by creating an “opt out” program,allowing them to decline the installation of a smart meter on their home. This sugges-tion overlooks some obvious and important problems:
• You can’t “opt out” of exposure to your neighbor’s meter, that is ten feet awayfrom your bedroom window.
• You can’t “opt out” of all the meters on the wall of your rental apartmentcomplex. Or the ones on the wall of the complex right across the alley from yourapartment.
• You can’t “opt out” of exposure to the meter on the other side of your bedroomwall if you are a baby in a crib.
• You can’t “opt out” of exposure to transmissions from the radio tower 100 metersfrom your house.
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 69
Comments on Notice of Inquiry, ET Docket No. 13-84

The idea of an “opt out” program is an effort to address the concerns of peoplewho are personally worried about RF exposures, either because they are aware ofhaving acute reactions to these exposures, or because they have a general concern aboutthe acute or chronic effects from such exposure.
But a voluntary “opt out” program does not protect the community at large fromadverse effects that they are unaware of and unconcerned about. For example, thecurrent research shows that cancer rates are higher in residences near cellular transmis-sion towers. Most people don’t know this. How does a voluntary “opt out” programhelp the person who develops breast cancer three years after installation of a transmis-sion tower across the street from her house? She didn’t know it was a problem . . .
DISCUSSION OF THE TECHNOLOGY OPTIONSHow would adopting these precepts and goals play out in practice? Several
factors come into consideration:• The scientific evidence on biological effects of RF, summarized in the basic
precepts listed above.• The various possible functional goals of the AMI program:
– Reducing operating costs by reading and switching meters remotely.– Training customers to conserve electricity.– Shifting time of use by measuring and billing time of day usage.– Absorbing fluctuations in renewable energy supply by “demand/response”
control of usage.• The different AMI technologies that are available.
When our committee puts our best understanding of these three factors intoconsideration, and look at each choice in AMI technology through this combined frameof reference, the discussion runs something like this:
MESH NetworkFrom a biological point of view, AMI meters that are transmitting several times a
minute can be considered to be an essentially constant source of RF exposure. Wherethese networks have been established in the last two years, large increases in reportedacute symptoms have occurred. We think it is medically probable that that this techno-logy will be found to cause an increase in chronic health problems, including increasedcancer, once sufficient time has passed for this to occur.
EWEB staff has already explored and tested a MESH option and chosen not to goforward on that path. We applaud EWEB’s decision to steer away from this technology.
Powerline Communications (PLC)From a public health point of view, PLC is less problematic than an RF AMI
communication technology. And PLC could be used to reduce operating costs, traincustomers to conserve electricity using in-house monitors, and record and transmit timeof day usage measurements to the utility.
EWEB has turned away from the choice of PLC for two main reasons. Firstly,because it won’t allow measurement of water meter readings, limiting the reduction ofoperating costs from elimination of meter reading. Secondly, because PLC as currentlydesigned does not have the bandwidth to sustain rapid “demand/response” controlcommunications.
There are some other technical considerations that make PLC infrastructure moreawkward to set up in an environment where some transmission wires are on poles and
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 70
Comments on Notice of Inquiry, ET Docket No. 13-84
others are underground.If “demand/response” was not on the table, and if a Total Bottom Line analysis
of the options included the potential health costs of using RF technology, the financialanalysis of the PLC option might look different than it did in the AMI Business Caseprepared by EWEB staff last April. A decision to read the water meters once every 3months rather than monthly could also realize additional savings, if this option wasunder serious consideration.
Fiber Optic CommunicationsFiber optic communication between the utility and the house meter is an ideal
solution from a health/environmental point of view, providing ample bandwidthwithout RF transmission. However, this technology would be quite expensive to install,especially in the parts of Eugene where the power grid is underground. The cost mightbe prohibitive for EWEB at this point in time. Like PLC, fiber optics would not commu-nicate with the water meters.
Tower Communications Network (SENSUS)The engineering system that EWEB is currently considering is the SENSUS
company’s technology, where central towers communicate directly with the meters onthe houses. SENSUS owns the sole rights to a certain transmission frequency on thecommunications bandwidth. This allows them to use more powerful radios on thesmart meters, strong enough to communicate directly with a transmission towerwithout requiring that the message be passed from meter to meter across a MESHnetwork. The community would be divided into about 13 zones, each of which wouldhave a communication tower placed on an existing EWEB property within the zone,and these towers would communicate directly with the house electric meters and withradios on the house water meters.
With 88,000 electric meters and 52,000 water meters in the city, an average zonewould have 6770 electric meters and 4000 water meters in the zone. How long a trans-mission interval would be required for a tower to collect the data from 10,770 meters?We don’t know the answer to this question, and EWEB engineers may not know either,until they set up a trial system and test it out. But clearly, the RF footprint created bythis sort of system could vary significantly, depending on how the system was used.
It is routine for utilities to collect data from these systems four times a day. Butthis routine was developed without consideration of the potential health risks of exces-sive RF transmission in the community. And usage data does not need to be collectedthis frequently to achieve the main goals of the AMI program. From a practical point ofview, the utility will continue to bill once a month, and in theory could remotely collectthat usage data once a month, minimizing the community’s exposure to frequent andrepetitive RF transmissions.
We think usage data should be collected from these meters at an interval of onceevery two to four weeks, with transmission occurring during the daytime hours. Trans-mission events at this level of infrequency would represent a minimal increase in the RFexposure to the community, and would be unlikely to significantly increase the risk ofchronic health problems in the community.
Each data transmission event would still be likely to provoke acute symptoms inindividuals with EHS who lived near these transmission towers. But if these eventsoccurred at an interval of once every two weeks or longer, and at a predictable time of
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 71
Comments on Notice of Inquiry, ET Docket No. 13-84

day, this might be a manageable level of exposure for those individuals.In our informal discussions with EWEB engineers, we have been told that they
have looked into the issue of data collection frequency, and that the longest that theycould go between data collection events with the SENSUS system would be about threeand one half days.
This would appear to be a case where the technology has not been designed withan eye to minimizing RF transmission. Six daily time-of-use intervals times 30 daysequals 180 intervals of usage data. We think that if an iPod can store 64 gigabytes ofmusic, it ought to be possible to give a smart meter enough memory to store 180readings before transmitting them to the utility. We would recommend that EWEB asktheir potential vendors to provide a meter with enough memory to store two to fourweeks of data, to enable the minimal RF footprint that we are recommending.
Tower communications and the water metersWater usage is billed once a month, and a single monthly reading of the meters
would collect this data with minimal RF exposure to the community. Again, this datacollection should occur in the day time, not in the middle of the night.
Tower communications and “demand/response” From a public health perspective, the use of the system for “demand/response”
load control is more problematic. As we understand it, a lot of this transmission wouldoccur at night, when wind power production is high and demand is low. Towerswould be transmitting every 15 minutes, to turn one cohort of water heaters on andanother cohort off. And the protocols required by the grid would require a two waycommunication with each meter in the cohort, acknowledging that house’s participationin the cohort at that time.
This will involve a good deal of transmission in the system every 15 minutes,both from the towers potentially talking to hundreds of meters across the neighbor-hood, and from the 2 watt radios on each house in the cohort talking back to the tower.
Communication of this frequency from the towers would be a significant additi-onal layer of frequent nocturnal RF signal exposure to the residences within a fewhundred meters of the towers.
And enough cohorts of houses are involved, the transmissions from the meterson the houses could also increase the signal density in the residential areas enough todisrupt melatonin and sleep in a percentage of the population.
We think that this frequent level of activity in the demand/response systemwould be a significant additional RF burden on the community. It would make life inthe residential area significantly more difficult for those individuals in the communitythat is currently already having acute problems. It would probably cause the onset ofacute symptoms in a small percentage of the population who are not currently experi-encing them. And it would be likely to further increase the incidence of chronic adverseRF effects in our community.
Demand/response and the in-home “Zigbee” networkOnce the AMI smart meter on the house gets a demand/response signal from the
control tower, it must tell the water heater in the house to turn on. Existing technologydoes this through wireless communication over a “Zigbee” WiFi network in the home.This network is maintained by constant transmissions of signals between the meter andthe Zigbee appliances in the home network, 24 hours a day.
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 72
Comments on Notice of Inquiry, ET Docket No. 13-84

The research that we’ve reviewed above shows that biological effects can beproduced by low power levels of RF exposure, and that prolonged, constant exposurescan have effects even at extremely low exposure levels.
For demand/response to work in the community, at least 20% of the homes inthe community will need to volunteer for the program, and have it set up in theirhouses. In undertaking to install demand/response infrastructure in its current form,EWEB would be making several presumptions:
• A presumption that the Zigbee system is low enough in power that it won’tcause any harm.
• A presumption that public acceptance should be good, since the public at largeisn’t really concerned about the health effects of RF at this time.
• A presumption that since most people have WiFi now anyway, they aren’t goingto be concerned about the additional exposure.
• A presumption that because the system will be voluntary, so no one can or willcomplain about involuntary exposure.While it may be true that the public isn’t that worried at present, and that many
people have WiFi in their homes and aren’t worried about it at all, we do not think thatEWEB can assume that this will continue to be the case throughout the investment life-time of the installed demand/response infrastructure.
As we’ve discussed in the prior sections, signals of WiFi power are strongenough to cause severe symptoms in individuals with EHS. Several hours of WiFiexposure has been shown to cause damage to healthy sperm. The general public isunaware of these facts. But we think that this is less likely to be the case 8 or 10 yearsfrom now, much less 20 years from now. As increased exposure to wireless RF commu-nications causes more health problems in the population, and the scientific evidence ofthis effect continues to become more robust, public attitudes about this exposure aregoing to change. Within 20 years, the public—especially parents with young children—will be much less open to having constant WiFi signal in their homes. If this assump-tion is correct, the purchase of many millions of dollars in demand/response infra-structure that is based on wireless in-home communications would appear to be anunwise investment.
The “demand/response” infrastructure is still immatureWe think that the “demand/response? infrastructure is still immature. This tech-
nology may be mature from an engineering point of view, in that “it works”. But froma public health perspective, it is completely immature. We state this because the tech-nology has been designed around RF communications (because this infrastructure isquicker and cheaper to set up than a hard wired system) without any consideration ofthe health effects of exposure to excessive or prolonged RF transmissions, and withoutany considered effort to engineer the hardware or the software protocols in a way thatwould minimize such exposures.
The Zigbee network is a case in point. In modern construction, most electricmeters are sitting on the outside of the circuit breaker box. Within that breaker box,there are dedicated circuits with hard-wired connections to the electric water heater, theelectric stove, and the electric clothes drier.
Why not set up communications between these utilities with powerline commu-nications protocols over these hard-wired connections? All it would take would be
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 73
Comments on Notice of Inquiry, ET Docket No. 13-84
some intelligent technology in the 220 circuit breakers for the appliances, and a smartswitch at the other end of the circuit, and connections to the network controls in thesmart meter that is plugged into the breaker box. All this could be done withoutputting any RF transmission into the house?
Why hasn’t this been done yet? Because a wireless solution is easier to install?Because changing the hard wiring would require changing electrical codes? Because noone thinks it’s necessary to get this clever, since no one is worried about RF exposures?
Solutions like this could be created, if industry and government had enoughincentive to work the problem, rather than to deny the existence of the problem. Untilsuch alternatives to constant in-home RF exposure are developed, we think that EWEBwould be wise to avoid getting married to this technology. Developing demand/response using a constantly transmitting in-home RF network will mean investing agreat deal of money in infrastructure that is likely to become extremely unpopularwithin the next 10 to 15 years. What we look at now as “quick and cheap” will come tobe viewed as “quick and dirty”.
Other communication optionsWe’ve been told that the powerline communication option is not a feasible solu-
tion for demand/response control, since it lacks the bandwidth necessary for rapidcommunications between server and meters.
We think that serious consideration should be given to the potential use ofbroadband internet connections for demand/response communications. We unders-tand that EWEB does not have the financial power to build their own fiberoptic networkat this time. But in 2010, 82% of the households in our part of the state had broadbandinternet connections, and this proportion continues to grow. Would it be technicallypossible to use these wired internet connections to communicate with the vast majorityof the electric meters in our city, rather than building a new wireless infrastructure todo the job? Broadband internet communications would certainly have the bandwidthto do this, and a demand/response system is not expected to require the participationof every household in the community. If we acknowledge the health risks of RFcommunication (especially the robust night-time communication expected for demand/response control), then an internet-based demand/response control system should begiven serious consideration.
IN CONCLUSIONWe hope that our report and recommendations will be helpful to EWEB staff, the
EWEB Board of Governors, and to members of our community. We think that review ofthis information should allow a more realistic appraisal of the health risks involved inestablishing an AMI network that utilizes microwave RF communication. Such ameasured and realistic appraisal is a necessary part of the Total Bottom Line Analysisthat EWEB has promised to bring to any major initiative in our community.
This is a lengthy document, and discusses complex issues. We would welcomethe opportunity to meet with EWEB staff and members of the Board, in order to give amore extensive audiovisual presentation and clarification of this material, and toanswer any questions that you wish to ask us about this research.
We hope to be part of an ongoing dialogue about the potential health effects ofRF technology, as EWEB continues to deliberate on the various choices that they facewith the AMI program.
SECTION 6 – CONCLUSIONS AND RECOMMENDATIONS
Page 74
Comments on Notice of Inquiry, ET Docket No. 13-84

Comments on Notice of Inquiry, ET Docket No. 13-84