patient selection in clinical trials
TRANSCRIPT

Patient Selection in Clinical Trials
by
Arno Klaassen
August 20 1996Nr. 383
Information systemsDepartment of Computer ScienceUniversity of Nijmegen, The Netherlands
Urologic Informatics Center/BioMedical EngineeringDepartment of Urology
University Hospital Nijmegen, The Netherlands

Patient Selection in Clinical Trials UIC/BME research center
1

Patient Selection in Clinical Trials UIC/BME research center
2
Abstract
PROSYS is developed to support the development of clinical trial protocols. A part of thisclinical trial protocol is subject selection. In this thesis an attempt will be made to develop aninference mechanism for the selection of patients for a clinical trial. First there is given anintroduction into the medical science. After this a basic model for medical knowledge will bepresented. This model will be adapted to create a model that is able to define all kinds ofmedical knowledge and to store selection criteria. After this an inference mechanism will bedeveloped to store and develop the selection criteria needed according to a given studyobjective. This inference mechanism will be evaluated by creating a prototype for thedevelopment of selection criteria: SCDS (Selection Criteria Development System).
Keywords: Clinical trial, subject selection, study objective, urology

Patient Selection in Clinical Trials UIC/BME research center
3

Patient Selection in Clinical Trials UIC/BME research center
4
Table of Contents
LIST OF FIGURES.......................................................................................................................... 6
LIST OF TABLES ........................................................................................................................... 8
1 INTRODUCTION ....................................................................................................................... 10
1.1 CLINICAL TRIALS - CURRENT PROBLEMS IN PROTOCOL DESIGN ................................................. 101.1.1 Clinical trials.................................................................................................................. 101.1.2 Phases of clinical trials................................................................................................... 101.1.3 Clinical trial protocols.................................................................................................... 111.1.4 Problems in protocol design............................................................................................ 11
1.2 PROTOCOL DESIGN SYSTEM (PROSYS).................................................................................. 121.3 PROJECT DEFINITION ............................................................................................................... 151.4 SUMMARY............................................................................................................................... 15
2 DETERMINATION OF THE INCLUSION AND EXCLUSION CRITERIA FOR A NEWTRIAL ............................................................................................................................................ 16
2.1 INTRODUCTION ....................................................................................................................... 162.2 PROSYS-PART ....................................................................................................................... 222.3 KNOWLEDGE REPRESENTATION - THE DEVELOPMENT OF AN ONTOLOGY ..................................... 23
2.3.1 An extended ontology to model domain knowledge needed for the development of selectioncriteria .................................................................................................................................... 26
2.4 AN INFERENCE MECHANISM FOR DEVELOPING SELECTION CRITERIA............................................ 462.4.1 Preparation for the inference mechanism........................................................................ 482.4.2 Step 1: Deriving criteria based on the Study Objective ................................................... 502.4.3 Step 2: Developing criteria based on inference steps ...................................................... 522.4.4 Step 3: Trying to guarantee completeness of selection criteria ........................................ 55
2.5 SUMMARY............................................................................................................................... 57
3 SCDS: A SYSTEM FOR DEVELOPING SELECTION CRITERIA ....................................... 58
3.1 DATABASE DESIGN .................................................................................................................. 583.2 THE INFERENCE MECHANISM .................................................................................................... 583.3 EVALUATION........................................................................................................................... 593.4 ACCEPTANCE TEST .................................................................................................................. 603.5 SUMMARY............................................................................................................................... 61
4 DISCUSSION AND CONCLUSION .......................................................................................... 62
APPENDIX A: PSM....................................................................................................................... 64
APPENDIX B: BASIC ONTOLOGY FOR A CLINICAL TRIAL .............................................. 66
APPENDIX C: PERFORMANCE STATUS CRITERIA ............................................................. 70
APPENDIX D: HYDRA................................................................................................................. 72
APPENDIX E: LISA-D .................................................................................................................. 74
APPENDIX F: INITIAL POPULATION FOR THE INFERENCE MECHANISM ................... 76
GLOSSARY ................................................................................................................................... 82
REFERENCES............................................................................................................................... 84

Patient Selection in Clinical Trials UIC/BME research center
5

Patient Selection in Clinical Trials UIC/BME research center
6
List of figures
Figure 1: Information flow diagram......................................................................................13Figure 2: Overview of the information topics described in a protocol.....................................13Figure 3: Partial representation of dependencies....................................................................14Figure 4: Patient recruitment in a clinic that consistently performed at goal rate. ...................19Figure 5: Patient recruitment in a clinic that started slowly and then performed a greater than
goal rate.......................................................................................................................20Figure 6: Patient recruitment in a clinic that performed poorly. .............................................20Figure 7: Graphical representation of construction selection criteria ......................................23Figure 8: Ontology as developed by [d’Hollosy 1995]...........................................................25Figure 9: PSM model of the study objective..........................................................................32Figure 10: PSM model of the Patient Characteristics. ...........................................................35Figure 11: PSM model of the Disease Characteristics criteria. ..............................................38Figure 12: PSM model of the Environment Characteristics and Safety Criteria......................40Figure 13: PSM model for the development of selection criteria. ...........................................44Figure 14: Hydra syntax.......................................................................................................72

Patient Selection in Clinical Trials UIC/BME research center
7

Patient Selection in Clinical Trials UIC/BME research center
8
List of tables
Table 1: The information items in a clinical trial protocol .....................................................14Table 2: Items to consider as criteria for patient selection......................................................18Table 3: An example study objective points of interest. .........................................................31Table 4: ECOG performance status......................................................................................70Table 5: Karnofsky performance status ................................................................................70

Patient Selection in Clinical Trials UIC/BME research center
9

Patient Selection in Clinical Trials UIC/BME research center
10
1 Introduction
In this introduction a brief overview of this master science project is given. This introductionconsists of the following topics:
• Clinical Trials - Current problems in protocol design• PROtocol design SYStem (PROSYS)• Definition of this master science project
In clinical trial design a description of clinical trials is given. PROSYS, a knowledge basedsystem to support the development of clinical trial protocols will be pointed out and the relationbetween PROSYS and clinical trials is described. After this the definition of this master scienceproject is given.
1.1 Clinical Trials - Current problems in protocol Design
1.1.1 Clinical trials
Clinical research is performed to improve medical knowledge on for example the symptoms andcourse of diseases or to develop or improve treatments. One form of a clinical research study isa clinical trial. A clinical trial is an experimental study on medical products in human subjectsto establish the efficacy and safety of these products by investigating treatments and comparingthe outcomes in a group of patients treated with the treatment with those observed in acomparable group [d’Hollosy 1995, Meinert 1986].
1.1.2 Phases of clinical trials
A clinical trial is mostly conducted in different phases. These phases can be divided as follows[Pocock 1983, Spilker 1985]:
Phase 1: The first phase of a clinical trial is mainly focused on testing the safety of anew treatment. These tests are usually performed on a very small group ofhuman volunteers, except when a treatment is tested with a high level oftoxicity.
Phase 2: In the second phase the treatment is tested again, but as safe as possible, basedon the experience obtained during the first phase. The goal is to demonstratethe effect of the treatment on a small group of patients and to collect moreinformation on the safety of the treatment. In this phase, the risk is that a neweffective treatment does not show significant effects on the group examinedpatients and the testing of the treatment will not be continued. This is called aType II error, the probability of not detecting a significant difference whilethere is actually a difference.
Phase 3: The third phase is often the last phase to test a treatment. The treatment istested on a large group of patients compared to a control treatment. The goal isto investigate the balance between safety and efficacy of the treatment on theshort and long term. To some people the term ‘clinical trial’ is synonymous

Patient Selection in Clinical Trials UIC/BME research center
11
with a full-scale phase III trial, which is the most rigorous and extensive typeof scientific clinical investigation of a new treatment [Pocock 1983].
Phase 4: The fourth phase, which is not always performed, is to investigate the safetyand efficacy of the treatment on the long term. In this phase the treatment isalready an existing treatment for a particular disease. The term ‘phase 4 trials’is sometimes used to describe promotion exercise aimed at bringing a new drugto the attention of a large number of clinicians [Pocock 1983]. If this is thecase, this phase has limited scientific value and should not be considered as apart of clinical trial research.
1.1.3 Clinical trial protocols
Information on a clinical trial is fully described in a protocol. This includes the arguments,goals and design of the clinical trial. The purpose of creating a protocol for a clinical trial is tosafeguard the testing of a new treatment and to do some standardisation on testing a treatment.Also it provides some anchor points, at which one can see if a certain protocol part hassucceeded. The approval or ejection of a new trial by scientific and ethical committees is basedon the ethical and scientific contents of this protocol. After approval, the protocol is used bypeople who conduct the clinical trial.
A protocol should contain at least the following information [d’Hollosy 1995]:
• Introduction• Study objectives• Subject selection• Ethical aspects• Study design• Treatment(s)• Evaluation• Statistical aspects• Administration
1.1.4 Problems in protocol design
The development of a clinical trial protocol is a difficult process. Problems that can arise are:
• Incoherence between different protocol parts.• Ambiguity or incompleteness of information.• Errors in statistical design of the trial.
Because the development of a clinical trial protocol is a difficult process the protocol willusually be evaluated more than once. For example a draft protocol is evaluated by colleagues.This colleague makes several certain changes to the draft protocol. When the protocol has beenadapted the protocol must be evaluated once again before it can be sent to an ethical committee.These evaluations are time consuming, so developing a clinical trial protocol is quite a timeconsuming process.

Patient Selection in Clinical Trials UIC/BME research center
12
1.2 PROtocol design SYStem (PROSYS)
In the previous paragraph problems with protocol design have been pointed out. There hasmade an attempt to reduce these problems, by developing an information system that supportsprotocol design. The UIC/BME has started the development of a knowledge-based system thatshould support the development of clinical trial protocols in the future. Support of this systemshould avoid as much as possible the problems mentioned in the previous paragraph. The nameof this system is PROSYS (PROtocol design SYStem).
PROSYS is developed to computerise the development of clinical trial protocols. This supportshould lead to a complete and high quality protocol contains information that is:
• Complete• Unambiguous• Coherent• Correct
The second aim of the development of PROSYS is to fasten the approval of new clinical trials.Nowadays a clinical trial is often evaluated more than once due to not satisfying one or more ofthe above mentioned constraints. This extends the time of approval of a clinical trial. The ideais that the support of a computerised system as PROSYS improves the quality of first versionclinical trial protocols, which will fasten the approval of a new clinical trial. A new clinicaltrial can than be started as soon as possible.
Writing a research protocol for a new study is the development of this new study. If theprotocol contents and the order in which the relevant information for these contents should beobtained are known then this order describes the framework of the protocol preparationprocess.
There are several organisations that provide guidelines to write a well designed and completeresearch protocol for a clinical trial. Based on the guidelines for the preparation of EORTC1
cancer clinical trial protocols [Staquet 1980], the guidelines of the EEC2 [GCP 1990] and twoexisting already approved protocol in urological research [Prot1 1992, Prot2 1994] anoverview on the relevant contents of a clinical trial protocol has been made, which resulted in alist of 30 information blocks. The information blocks are concerned to only a few specifictopics [Figure 2]. The list of information items is shown in table 1 This list of informationblocks is used as foundation to develop PROSYS. The contents of this table are used todescribe the preparation process of the clinical trial protocol, that starts with working out theresearch objectives. A part of this process is shown in Figure 3. PROSYS is divided intoseveral parts, called PROSYS-parts. Each PROSYS-part is responsible for working out theprocess that results in the desired information. Each PROSYS-part can be seen as a stand aloneinformation system. All processes generate trial information that depends on the incominginformation of the involved information blocks. The incoming information can consist ofinformation from users or from other PROSYS-parts. The outgoing information of aninformation block serves as input for other PROSYS-parts or for users [Figure 1].
1 European Organisation for Research and Treatment on Cancer.2 European Economic Community.

Patient Selection in Clinical Trials UIC/BME research center
13
Figure 1: Information flow diagram
Figure 2: Overview of the information topics described in a protocol
Information topic Information blocksIntroduction 1. Description and prognosis of the disease
2. Current treatments3. Results of other, relevant, studies4. Rationale of the study
Study objectives 5. Title6. Research objectives
Subject selection 7. Inclusion and exclusion criteriaEthical aspects 8. Ethical study considerations
9. Informed consentStudy design 10. Study type (e.g., phase 2 study, phase 3 study, …)
11. Study design (e.g., double blind, cross-over, ..)12. Endpoints of the study
Miscellaneous
Introduction
Study objectives
Administration
Statistical aspects
Evaluation
Subject selection
Ethical aspects
Study design
Treatment(s)
PROTOCOL
User
Other PROSYS-part
Other PROSYS-part
PROSYS-part
OtherPROSYS-part
User

Patient Selection in Clinical Trials UIC/BME research center
14
Information topic Information blocksTreatment(s) 13. Detail description per treatment
14. Instructions to deal with adverse events (e.g., toxicities)15. Instructions to deal with deviations from the protocol (e.g., patient
withdrawal)Evaluation 16. Study variables and measuring methods
17. Measurement schedule18. Forms and procedures for data collection
Statistical aspects 19. Statistical method20. Significance level21. Sample size22. Study duration23. Randomisation method24. Stratification method
Administration 25. Registration method26. Administration with relation to the study participants (e.g., name and
professional background, participating centres , addresses, phonenumbers, function division in the study, co-ordination team, et cetera.)
27. Administration with relation to the study protocol (e.g., start date of thetrial, date(s) of protocol version(s), approval date(s)).
Miscellaneous 28. Quality control29. Additional information (e.g., finance, insurance)30. References
Table 1: The information items in a clinical trial protocol
Figure 3: Partial representation of dependencies
Research objectives Study type
Endpoints of the study Study variables andmeasurement methods
Detailed description pertreatment
Registration method Inclusion/exclusion criteria Measurement schedule
Forms and procedures fordata collection

Patient Selection in Clinical Trials UIC/BME research center
15
1.3 Project definition
The inclusion and exclusion criteria specify the human subjects from which data has to becollected. These inclusion and exclusion criteria are based on the research objectives and adetailed description for a treatment. The assignment of this master thesis is the following:
Defining and implementing of the knowledge and the reasoning process thatshould lead to the inclusion and exclusion criteria needed for new clinicaltrials.
This thesis consists of four chapters:
1. Introduction (this chapter)2. Determination of the Inclusion and Exclusion Criteria for a new Trial3. SCDS: a prototype for the development of selection criteria4. Discussion and Conclusion
Chapter two describes the development of the inclusion and exclusion criteria and is showingthe inference engine to develop these criteria.
Chapter three presents the prototype for the development of selection criteria. This prototype iscalled Selection Criteria Development System (SCDS).
1.4 Summary
In this chapter the world of clinical trials has been introduced to the reader. The aim of thischapter was to point out what a clinical trial is and to give an introduction into this masterscience project. For further information on clinical trials see [Meinert 1986, Pocock 1983,Sylvester 1995].

Patient Selection in Clinical Trials UIC/BME research center
16
2 Determination of the Inclusion and Exclusion criteria fora new Trial
2.1 Introduction
In clinical trials, new treatments are tested on human beings, mostly patients that are sufferingfrom the disease a new treatment is intended to. Human subjects are included in a clinical trialonly when satisfying a set of inclusion criteria and not satisfying any of the exclusion criteria.For each trial these criteria are developed to create the desired subject population.
Now an example is given of inclusion and exclusion criteria that are used in an existing PhaseIII trial [Win 122] to give an idea what is meant by inclusion and exclusion criteria. Theobjective of this study was to evaluate the value of the treatment Interleukin-2 in terms ofdisease free and overall survival of patients and their quality of life, after being treated againstcancer. The inclusion and exclusion criteria that were used are:
Inclusion criteria:
Patients will be eligible for participation in the study provided all the following criteriaare met:
• Histologically proven Renal Cell Carcinoma.• Patients should have undergone surgical resection of the primary tumour and
lymph nodes.• Nodal status N 1 or 2.• There should be no macroscopic residual disease.• Ambulatory performance status (ECOG 0-1; Karnofsky ≥ 80%3 ). Age < 70 years
old and a life expectancy greater than 3 months.• WBC ≥ 4.000, platelets ≥ 120.000 and HCT ≥ 30%.• Randomisation should occur within one month following surgery and treatment
should start between 4-6 weeks after surgery.
Exclusion criteria:
Patients will be excluded from participation in the study if one of the following criteriaare met:
• Any of the above criteria are not met.• Unstable angina pectoris or recent (6 months) myocardial infarction.• Evidence of active infections requiring antibiotic therapy.• Patients with major organ allografts (Interleukin-2 increase T-cell mediated
rejection and immunosuppressive agents are likely to reduce efficacy ofInterleukin-2).
• Patients with signs or symptoms of systemic metastatic Renal Cell Carcinoma.• Patients who require or are likely to require corticosteriods for intercurrent
disease.
3 See appendix C
Patient Selection in Clinical Trials UIC/BME research center
17
• Pregnant or lactating women.• Patients with previous malignancies, except for basal cell carcinoma of the skin or
cervical cancer.• Patients who receive radiation or chemotherapy.
In literature the phrase ‘selection criteria’ is synonym for the phrase ‘inclusion and exclusioncriteria’. In the remainder of this master thesis the phrase ‘selection criteria’ is used, becauseeach exclusion criterion can be written as a denial and would then be an inclusion criterion. Forexample, the inclusion criteria in [Win 122] ‘There should be no macroscopic residualdisease’ could be written as the exclusion criteria ‘Patient has macroscopic residual disease’.
Selection criteria used in a clinical trial should satisfy the following constraints:
• The selection criteria should guarantee ethics for the patients.• The selection criteria should guarantee complete safety for the patients.• The selection criteria should ensure a the selected patient population that is a good
reflection of the group for which the treatment is developed [Jeffcoat 1992].• The definition of the selection criteria should be precise and unambiguous.
Based on these constraints, except for the last constraint, the selection criteria can bedistinguished into several classes of criteria. These classes are [Spilker 1985]:
1) Characteristics of patients. In this class the characteristics of patients are defined. Forexample the age and life expectancy of the patient.
2) Characteristics of the disease and its treatment. In this class the characteristics ofthe patient‘s disease are recorded. For example, does the patient suffer from the diseaseor in what stage is the disease. Also the characteristics of the tested treatment andexclusion treatment’s are recorded.
3) Environmental and other factors. Sometimes special environment criteria are definedto detect a disease in a certain area. Also ethical criteria fall into this class. Forexample, has the patient signed the informed consent.
4) Safety criteria. In this class criteria are defined for examinations that are not clinicallyacceptable.
These classes of criteria are based on several points of interest. Spilker [Spilker 1985] statesitems that can lead to selection criteria for each class. Table 2 shows these items:
A. Characteristics of patients 1. Gender, e.g. patient should be of gender female. 2. Age, e.g. patient should have age older than 18. 3. Weight 4. Education 5. Race and/or ethic background 6. Social and economic status 7. Pregnancy and lactation, e.g. patient should have no pregnancy. 8. Use of tobacco; ingestion of caffeine and/or alcohol 9. Abuse of alcohol or drugs 10. Diet and nutritional status 11. Physiological limitation and genetic history 12. Surgical, anatomical, and/or emotional limitations

Patient Selection in Clinical Trials UIC/BME research center
18
13. Hypersensitivity to a study drug or test 14. Other drug and nondrug allergies
B. Characteristics of the disease and its treatment 1. Disease being evaluated 2. Concomitant drugs 3. Previous drug and nondrug treatment 4. Washout period of nonstudy drugs or nondrug treatments 5. History of other diseases 6. Present clinical status 7. Previous hospilazations
C. Environmental and other factors 1. Patient recruitment and co-operation, e.g., patient should have signed informed
consent. 2. Participation in another dug study 3. Participation in another part of this study or in any other study using this study
drug 4. Institutional or environmental status 5. Occupation, e.g., patient should have occupation doctor. 6. Geographical location, e.g. patient should have residence Holland 7. Litigation and disability
D. Safety criteria 1. Physical examination 2. Clinically acceptability 3. ECG, e.g. Patient should have passed ECG 4. EGG 5. Ophthalmologic and laboratory examinations
Table 2: Items to consider as criteria for patient selection.
Selection criteria are used to select patients for a clinical trial during a patient recruitmentperiod. When selecting patients for a clinical trial, one must have in mind the number ofpatients that is needed to show the significance of the tested treatment or to reject the treatmentbased on the results of the clinical trial. This number of patients is called sample size and iscomputed on base of statistical aspects. There are four factors that play a role in computing thesample size [Collins 1984]:
• The outcome measures.• Magnitude of clinically important differences between outcome measures.• Amount of variation in the outcome measures in the study population.• Drop-out rate, where drop-out rate is defined as the number of study patients who fail
to complete the required follow-up for reasons that cannot definitely be attributed totreatment outcome in relation to the number of patients that entered the clinical trial.This drop-out rate is hardly to predict. Reasons for drop-out are usually that a patient’scondition has changed and continuing the trial may jeopardise the patient’s health orthe patient does not want to co-operate anymore.
If the selection criteria are too strict, or the sample size is too high, problems can occur increating the desired patient population and this mostly leads to the problem that fewer patientswere recruited in the desired recruitment interval than defined by the sample size.
This problem can be resolved in three ways:

Patient Selection in Clinical Trials UIC/BME research center
19
1) Extending the trial.2) Adapting the trial protocol.3) Terminating the trial.
The first method of solving the problem is the least severe. The most common reason a study isextended is that fewer patients enrolled than was expected (Figure 5 and Figure 6] after thepatient recruitment period. It is usually necessary only to increase the allowable recruitmenttime and not to modify the protocol [Spilker 1985, Tu 1993]. This because there are normallyenough patients to include in the clinical trial, but the designers underestimated the time neededto find these suitable patients.
When the patient recruitment period is extended and there are still not enough patients recruitedthe problem is mostly resolved by adapting the study protocol. If patient recruitment went muchslower than expected, it is likely that it will be difficult to select enough patients for a trial[Figure 6]. It should be possible to make adjustments to the selection criteria to render patientseligible for the clinical trial. Confirmation of eligibility may require more than one evaluation,due to changes in a patient’s condition. In this situation, identifying an eligible participant for aclinical trial is a dynamic and time-consuming process [Tu 1993].
The third, last and most severe method of resolving the problem is an early termination of thetrial. The clinical trial is than terminated due to the small number of patients included in theclinical trial. Sometimes a clinical trial can start with fewer patients than specified by thesample size, but the risk is that this trial will lose its value due to the lacking significance of theresults of the clinical trial.
In Figure 4, Figure 5, Figure 6 three illustrations are presented of patient recruitment. Thesefigures are based on the Beta-blocker Heart Attack Trial [Friedman 1985]. In Figure 4 anillustration of a clinical trial is given that was well designed; the patient recruitment wentaccording to the clinical trial protocol. In Figure 6 an illustration is presented of patientrecruitment that had a bad start, but after this went above goal ratio and an illustration isshown of a poorly designed patient recruitment.
Figure 4: Patient recruitment in a clinic that consistently performed at goal rate.

Patient Selection in Clinical Trials UIC/BME research center
20
Figure 5: Patient recruitment in a clinic that started slowly and then performed a greater thangoal rate.
Figure 6: Patient recruitment in a clinic that performed poorly.

Patient Selection in Clinical Trials UIC/BME research center
21
If the chosen selection criteria are too relaxed, the clinical trial will be less reliable and lessgeneralizable due to variation in patient characteristics of the selected patients. Thus, theoptimal set of selection criteria is the set of criteria that is as broad as possible to permitadequate enrolment and generalizability, but narrow enough to exclude those who are unlikelyto be affected by the intervention.
Summarised, in the development of selection criteria there are thus two extremes [Spilker1985]. In this section these extremes will be pointed out and their advantages anddisadvantages will be displayed. The first extreme is the highly restricted selection criteria.
Advantages:• This set provides more precise comparison of the test and control treatments.• The results of the trial are less likely to be effected by the population variability.
Disadvantages:• This set increases cost and time required for patient recruitment.• This set limits generalizability of the study findings, because there will be a very
homogeneous group of the patients and the characteristics of the patients will notmuch differ.
The other extreme is minimally restrictive selection criteria.
Advantages:
• This set makes patient recruitment easier• This set provides a base for wider generalisation of findings.
Disadvantages:
• This set may obscure treatment effects because of variability in composition of thestudy population.
• The results of a trial may be confusing, especially if an observed effect appears tobe associated with a subgroup of patients in the study and the subgroup is toosmall to yield a reliable treatment comparison.
• Potentially more eligible patients may be overlooked, due to the wide variety inpatient characteristics.
In this master thesis a knowledge based system is developed to support the development ofselection criteria. These criteria are developed for a first draft protocol. This is done because itis allowed to add selection criteria after the clinical trial protocol has been approved by acommittee, so it is recommended to create a set of selection criteria that is not too strict. Theuser can alter these criteria or add new ones to create a stricter set of selection criteria when theconductor of the clinical trial sees that there are many potential study objects and wants to addcriteria to assure a more homogeneous sample population.
Patient Selection in Clinical Trials UIC/BME research center
22
2.2 PROSYS-part
The UIC/BME has started the development of a knowledge based information system, calledPROSYS (see section 1.2). PROSYS should support the development process of clinical trialprotocols to improve the quality of first draft protocols. This should lead to a decrease in timeneeded to develop such protocols.
PROSYS consists of several partitions called PROSYS-parts. These parts can be seen as amodule of PROSYS or as a stand-alone information system. This master thesis will befocussed on the development of the PROSYS-part for the support of the development of theselection criteria. This PROSYS-part will use information to develop selection criteria. Thismethod of information development is best described as a knowledge based information systemand thus the PROSYS-part for the support of the development of selection criteria will be aknowledge based information system.
The development of a knowledge based system consists of several stages. First sampleknowledge is created and the relations in this sample knowledge must be discovered. Accordingto these relations, a knowledge model is developed to define the structure of these relations.After this the real knowledge must be collected and then this model can be populated using theknowledge from daily practice. After this, the inference mechanism has to be formulated.
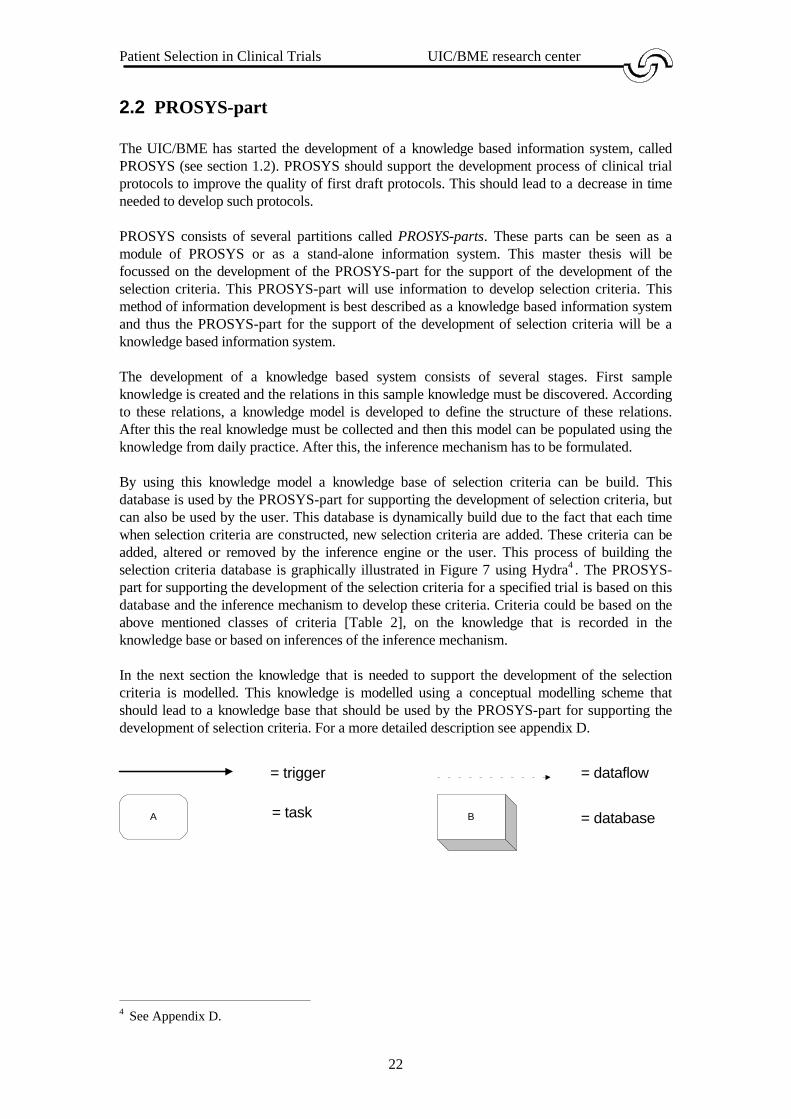
By using this knowledge model a knowledge base of selection criteria can be build. Thisdatabase is used by the PROSYS-part for supporting the development of selection criteria, butcan also be used by the user. This database is dynamically build due to the fact that each timewhen selection criteria are constructed, new selection criteria are added. These criteria can beadded, altered or removed by the inference engine or the user. This process of building theselection criteria database is graphically illustrated in Figure 7 using Hydra4 . The PROSYS-part for supporting the development of the selection criteria for a specified trial is based on thisdatabase and the inference mechanism to develop these criteria. Criteria could be based on theabove mentioned classes of criteria [Table 2], on the knowledge that is recorded in theknowledge base or based on inferences of the inference mechanism.
In the next section the knowledge that is needed to support the development of the selectioncriteria is modelled. This knowledge is modelled using a conceptual modelling scheme thatshould lead to a knowledge base that should be used by the PROSYS-part for supporting thedevelopment of selection criteria. For a more detailed description see appendix D.
4 See Appendix D.
= trigger
= taskA
= dataflow
B = database

Patient Selection in Clinical Trials UIC/BME research center
23
Figure 7: Graphical representation of construction selection criteria
2.3 Knowledge representation - the development of an ontology
In this master thesis the following definitions are used [Webster 1983]:
• Data: Data consist of facts such as words, numbers, etc. Used for reasoning,discussion or calculation.
• Information: When data is given a certain meaning the data with meaning is calledinformation. For example, when one concludes from a body temperature of 39
�
Celsius that a patients has fever, than body temperature of 39�
Celsius is calledinformation.
• Knowledge: When information is used to create other information, the information thatwas used to create this new information is called knowledge.
A knowledge base is a conceptual model that is populated with knowledge. Such a conceptualmodel is called an ontology5 . By using an ontology knowledge can be represented inknowledge base [Gruber http]. To develop the knowledge base that is needed by the inferencemechanism to construct the selection criteria an ontology is needed to conceptualise the domainknowledge.
Certain decisions have to be made during the development of an ontology. Here, these decisionsare based on the following criteria [Mars 1991, d’Hollosy 1995]:
• Expressiveness: It should be possible to represent all possible knowledge that isneeded in the application domain.
• Economy: It should be possible to represent all possible knowledge with as few aspossible concept classes and relations.
• Efficiency: It should be possible to perform the inference rules on the knowledge asefficient as possible.
5 The term ontology is borrowed from philosophy, in which it refers to the subject of existence. InArtificial Intelligence the term ontology is a description (like a formal specification of a program) ofconcept classes and relation classes that are used to conceptualise knowledge [Gruber 1993-2].
Developing selection criteria
KnowledgeBaseUser
PROSYS-part
InferenceMechanismInference
Mechanism

Patient Selection in Clinical Trials UIC/BME research center
24
• Flexibility: It should be possible to add, modify and remove knowledge easily.• Uniformity: The naming of concept classes should join the common terminology of the
application domain.
An ontology defines the structure of knowledge. Such a structure is defined by defining conceptclasses and relation classes between these concept classes. This structure can graphically berepresented using a modelling scheme. One can take for example a PSM-scheme6 forrepresenting an ontology.
The base for the ontology of this application is the ontology as developed by [d’Hollosy 1995].This ontology has an overlap with the construction of selection criteria due to the fact that theontology of [d’Hollosy 1995] already covers concept classes as State and Treatment Method.So the decision is made to adapt this ontology to a knowledge model for the development ofselection criteria. This basic and adapted ontology will be modelled using PSM. In PSM theconcept classes are called entity types and the relation classes are called fact types. In Figure 8the ontology developed by [d’Hollosy 1995] is modelled. For the a formal description of thisontology see Appendix B.
6 PSM (Predicator set model) is an extension of NIAM. For more information see Appendix A.

Patient Selection in Clinical Trials UIC/BME research center
25
Figure 8: Ontology as developed by [d’Hollosy 1995].
Anatomical Referent(AR-name)
comprisesbeing_part_of
PO1
being_kind_of
being_generalisation_of
KO1
having_function_towards occurring_in
HFT2
Material KO2
being_generalisation_of
being_kind_ofPO4
being_part_ofcomprises
Treatment Method(TM-name)
Evaluation Method(EM-name)
Instrument(IN-name)
Variabele(VAR-name)
State(ST-name)
being_kind_of
KO3
being_generalisation_of
being_kind_of
KO5
being_generalisation_of
being_kind_of
KO7
being_generalisation_of
being_kind_of
KO4
being_generalisation_of
being_kind_of
KO6
being_generalisation_of
PO3
comprisesbeing_part_of
PO5
comprisesbeing_part_of
PO2
comprisesbeing_part_of
HFT1
having_function_towardsoccurring_in
US1
uses
being_used_by
US2
uses
being_used_by
US3
usesbeing_used_by
US4
uses
being_used_by
CS1
causes
being_caused_by
CS2
causes
being_caused_by
CS3being_caused_by
causes
CS4
causes
being_caused_by
being_caused_by
causes
CS5
EB1
evaluates
being_evaluated_by
EB2evaluates
being_evaluated_by
HV1
having_variable
being_variable_of
FI2
can_be_found_in_state
being_state of
HV2
having_variable
being_variable_of
FI1
can_be_found_in_state
being_state_of
DB1
definesbeing_defined_by
DB2
being_defined_by
defines
HV3
being_variable_ofhaving_variable

Patient Selection in Clinical Trials UIC/BME research center
26
2.3.1 An extended ontology to model domain knowledge needed forthe development of selection criteria
In Figure 8, the ontology as developed by [d’Hollosy 1995] is presented. This model will beextended now. To model knowledge on selection criteria, several things like characteristics of adisease, or the study type of a clinical trial should be known, because certain selection criteriadepend of this information (see 2.1). To model this knowledge 6 new concept classes and 7 newrelation classes are added to the basic ontology.
The 6 new concept classes are:
Concept class: Study Type (STP)Description: For the development of the selection criteria it is necessary to know
for what phase the clinical trial is. This is always one of the followingphases: Phase I, Phase II, Phase III or Phase IV.
Examples: In Phase I the first experiments in human subjects are primarilyconcerned with drug safety, not efficacy, and are usually performedon volunteers, so selection criteria on disease characteristics aremostly not needed here. After studies in normal volunteers, the initialtrials in patients will also be of the Phase I type [Pocock 1983].
Argumentation: The reason of adding the concept class ‘Study Type’ is that whenconducting a clinical trial the selection criteria depend on the studytype. In a Phase I clinical trial there are normally only safety criteria,because a new treatment is tested on volunteers and the aim of thestudy is not to establish efficacy, but to test the safety of this newtreatment. Thus, the study type influences the construction of theselection criteria and is therefore added to the knowledge model.
Concept class: Study Objective (SO)Description: One needs to know which hypothesis has to be proven to support the
development of selection criteria. Selection criteria will depend onthis hypothesis.
Examples: If the study objective is to observe a certain disease in children, then alogical selection criterion would be ‘age < 18’.
Argumentation: A clinical trial is created according to the study objective that statesthe hypothesis that one wants to prove when conducting the trial. Theconstruction of the selection criteria is aimed at creating ahomogeneous group of patients that is suitable to test the hypothesis.Thus the study objective influences the construction of the selectioncriteria and is therefore added to the knowledge model.
Concept class: Selection CriteriaDescription: Selection criteria are used to include or exclude a potential trial
subject in or from a clinical trial. As mentioned above there are fourdifferent classes of selection criteria (see Table 2). These classes aresubclasses of the concept class Selection Criteria and will bemodelled accordingly; patient characteristics criteria (PC), diseasecharacteristics criteria (DC), Environment characteristics criteria(EC) and Safety criteria (SF). These Selection Criteria can be

Patient Selection in Clinical Trials UIC/BME research center
27
designed, altered or removed by the inference mechanism.Examples: Age > 18 (PC), has fever (DC), lives in Holland (EC), has signed
informed consent (EC), absent deep tendon reflexes (SF).Argumentation: The reason of adding this concept class is that when selecting patients
for a clinical trial, this is done by means of selection criteria. Theseselection criteria are developed by the inference engine or the user,thus there must be a concept class to store these developed selectioncriteria in.
Concept class: Selection Criteria SetDescription: This class is the super class of the concept class Selection Criteria.
This class contains (non empty) sets of selection criteria that are usedin a protocol.
Examples: {‘age > 18’, ‘Age < 65’, ‘signed informed consent’, ‘proven RenalCell Carcinoma’}
Argumentation: Selection Criteria are used to include or exclude a patient in a clinicaltrial. A part of the protocol is the patient recruitment. Patients arerecruited by matching their characteristics to a specified set ofselection criteria that should guarantee the safety of the patients and asample population that reflects the hypothesis being tested.
Concept class: Value (VAL)Description: This concept class is only connected to the concept class Variable.
Each variable must have a value connected to that variable. There arethree kinds of values: numbers, dates and text. Boolean values can berepresented using zero for false and for true. To support this, theconcept class Value consists of three subclasses: Text (String),Date-code (Date) and Number (Nr).
Examples: Age numbers (Nr). Occupation text (String), birth date (Date).Argumentation: When dealing with variables, one must have in mind that a variable
can have different values, therefore the concept class Variable mustbe connected with a class of values called Value.
Concept class: Operator (OP)Description: This concept class is only connected to the concept class Variable.
Each variable must have a value connected to that variable. Torepresent something like: age > 18, the concept class Operator isintroduced.
Examples: >, <.Argumentation: When dealing with variables, one must have in mind that a variable is
often a limit and therefore the variable must be attached to some kindof operator.
There are also seven new relation classes. These relation classes are needed to represent therelations between the concept classes.
Relation class: influences (INF)Explanation: The way in which a study objective is created is
influenced by the study type. In the reasoningprocess this study type must be taken into account

Patient Selection in Clinical Trials UIC/BME research center
28
when creating the selection that are criteria basedon the study objective.
Relations:Study Type influences StudyObjective
e.g., Study Type ‘Phase I’ influences StudyObjective ‘Safety of paracetamol’.
Relation class: having value (HVAL)Explanation: The concept class Value was developed to provide
values to the concept class Variable. The relationclass having value connects a variable with itsassociated value.
Relations:Variable having value Value e.g., Variable ‘Gender’ having operator ‘=’,
having value Value ‘Female’.
Relation class: is subject of (ISO)Explanation: The study objective is a sentence that can be
divided in several points of interest. Thisdeviation is done by attaching subjects to thestudy objective. These subjects are called pointsof interest. To connect these points of interestwith its associated study objective, the relationclass is subject of is developed.
Relations:State is subject of StudyObjective
e.g., State ‘Renal Cell Carcinoma’ being subjectof Study Objective ‘Evaluating quality oflife having Renal Cell Carcinoma’.
Treatment Method is subject ofStudy Objective
e.g., Treatment Method ‘surgical resection’ beingsubject of Study Objective ‘Evaluating thequality of life after having treated RenalCell Carcinoma with surgical resection’.
Variable is subject of StudyObjective
e.g., Variable ‘quality of life’ being subject ofStudy Objective ‘Evaluating quality of lifehaving Renal Cell Carcinoma’.
Relation class: is restriction of (RVAR)Explanation: The study objective is a sentence that can be
divided in several points of interest. Thisdeviation is done by attaching subjects to thestudy objective. One of these subjects can also bea restriction on the population, for example age.This relation class is added to represent theserestrictions..
Relations:Having Value is restriction ofStudy Objective
e.g., Having Value (Variable ‘Age’, Operator ‘>’,Value ‘18’) being_restriction_of StudyObjective ‘Evaluating quality of life ofadults having Renal Cell Carcinoma’.
Patient Selection in Clinical Trials UIC/BME research center
29
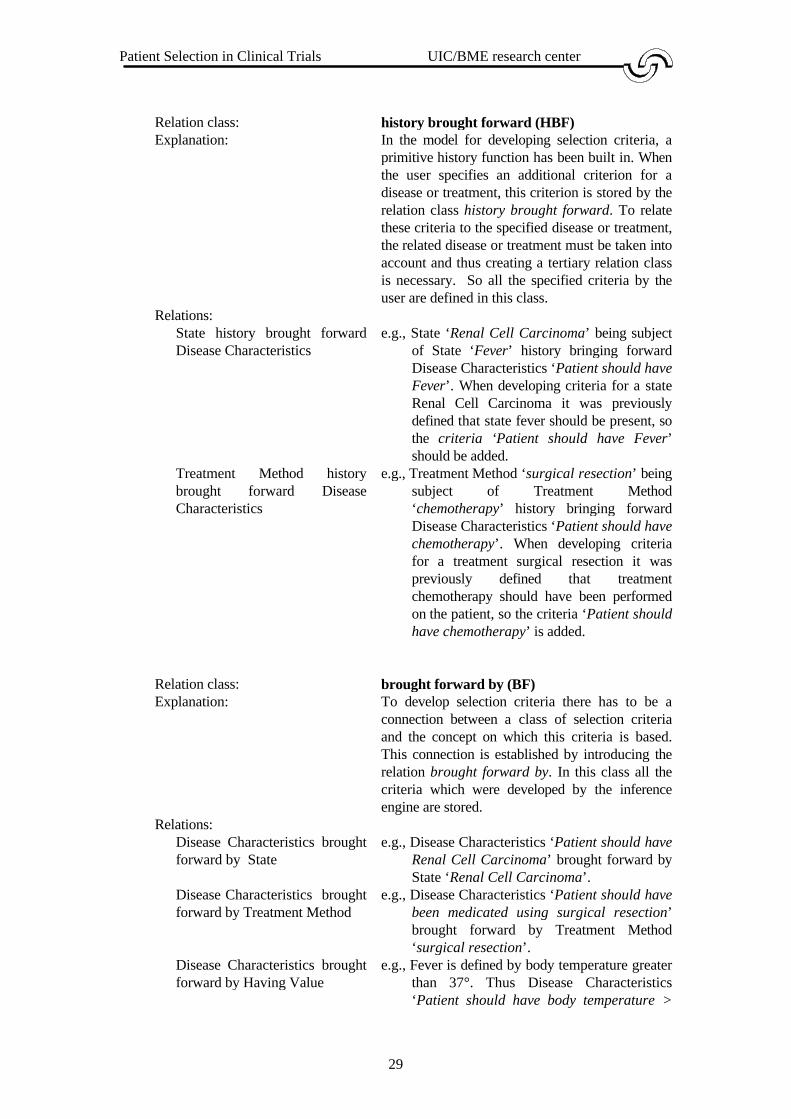
Relation class: history brought forward (HBF)Explanation: In the model for developing selection criteria, a
primitive history function has been built in. Whenthe user specifies an additional criterion for adisease or treatment, this criterion is stored by therelation class history brought forward. To relatethese criteria to the specified disease or treatment,the related disease or treatment must be taken intoaccount and thus creating a tertiary relation classis necessary. So all the specified criteria by theuser are defined in this class.
Relations:State history brought forwardDisease Characteristics
e.g., State ‘Renal Cell Carcinoma’ being subjectof State ‘Fever’ history bringing forwardDisease Characteristics ‘Patient should haveFever’. When developing criteria for a stateRenal Cell Carcinoma it was previouslydefined that state fever should be present, sothe criteria ‘Patient should have Fever’should be added.
Treatment Method historybrought forward DiseaseCharacteristics
e.g., Treatment Method ‘surgical resection’ beingsubject of Treatment Method‘chemotherapy’ history bringing forwardDisease Characteristics ‘Patient should havechemotherapy’. When developing criteriafor a treatment surgical resection it waspreviously defined that treatmentchemotherapy should have been performedon the patient, so the criteria ‘Patient shouldhave chemotherapy’ is added.
Relation class: brought forward by (BF)Explanation: To develop selection criteria there has to be a
connection between a class of selection criteriaand the concept on which this criteria is based.This connection is established by introducing therelation brought forward by. In this class all thecriteria which were developed by the inferenceengine are stored.
Relations:Disease Characteristics broughtforward by State
e.g., Disease Characteristics ‘Patient should haveRenal Cell Carcinoma’ brought forward byState ‘Renal Cell Carcinoma’.
Disease Characteristics broughtforward by Treatment Method
e.g., Disease Characteristics ‘Patient should havebeen medicated using surgical resection’brought forward by Treatment Method‘surgical resection’.
Disease Characteristics broughtforward by Having Value
e.g., Fever is defined by body temperature greaterthan 37°. Thus Disease Characteristics‘Patient should have body temperature >

Patient Selection in Clinical Trials UIC/BME research center
30
37°’ brought_forward_by Having Value(Variable ‘body temperature’, Operator ‘>’,Value ‘37°)’.
Disease Characteristics broughtforward by Evaluation Method
e.g., Disease Characteristics ‘Patient should havebeen examined using no x-ray’s’brought_forward_by Evaluation Method ‘x-ray’s’.
Patient Characteristics broughtforward by Having Value
e.g., Patient Characteristics ‘Patient should be ofgender female’ brought forward by HavingValue (Variable ‘gender’, Operator ‘=’,Value ‘female’).
Patient Characteristics broughtforward by Material
e.g., Patient Characteristics ‘Patient should be ofno hypersensitive against B’ broughtforward by Material ‘B’.
Environment Criteria broughtforward by Having Value
e.g., Environment Characteristics ‘Patient shouldhave residence Holland’ brought forwardby Having Value (Variable ‘Residence’,Operator ‘=’, Value ‘Holland’).
Safety Criteria brought forwardby Having Value
e.g., Safety Criteria ‘Patient should have deeptendon reflexes present’ brought forward byHaving Value (Variable ‘deep tendonreflexes’, Operator ‘=’, Value ‘present’).
Relation class: is exclusion of (EX)Explanation: To develop criteria based on an exclusion
treatment or state, an exclusion should beintroduced. The decision was made to create arelation class just for exclusions instead ofcreating a concept class. The advantage of thisapproach is that it is simple to model criteriabased on exclusion states or treatments.
Relations:State is exclusion of StudyObjective
e.g., State ‘Fever’ being exclusion of StudyObjective ‘Renal Cell Carcinoma and nothaving fever’.
Treatment Method is exclusionof Study Objective
e.g., Treatment Method ‘chemotherapy’ beingexclusion of Study Objective ‘Patients beingtreated with surgical resection and nothaving undergone chemotherapy’.
Treatment Method is exclusionof Treatment Method
e.g., Treatment Method ‘chemotherapy’ beingexclusion of Treatment Method ‘radiation’.
State is exclusion of TreatmentMethod
e.g., State ‘Fever’ being exclusion of TreatmentMethod ‘surgical resection’.
Also a new relation to an already existing relation class is added:
Relation class: is part of (PO)Relations:
Selection Criteria is part ofSelection Criteria Set
e.g., Selection Criteria ‘PC1’ is part of SelectionCriteria Set {‘PC1’, ’DC1’, ‘DC2’}.

Patient Selection in Clinical Trials UIC/BME research center
31
Due to the complexity of the extension, this extension will be presented in three phases:
• First, the concept class Study Objective will be explained and the relation betweenStudy Objective and other concept classes will be explained. After this, an example ofa population for this model will be given.
• Secondly, the subclasses of the concept class Selection Criteria are explained and therelation between these subclasses and other concept classes will be explained. Thesemodels will present a model of constructing the selection criteria for that subclass.After this, example populations for these models are given.
• The concept classes Study Type and Value are integrated in the concept classes StudyObjective and Selection Criteria and will not be modelled independently. The conceptclass Study Objective and the subclasses of the concept class Selection Criteria havebeen explained and an overview of the complete extension will be given.
Construction of the concept class Study Objective:
In considering study objectives, the study objective can be divided in several points of interest.For example:
Comparing the efficacy of a treatment for headaches ,not having migraine, usingparacetamol or a placebo drug A on female humans younger than 18 in a clinicalPhase III trial.
This objective can be divided into the following points of interest:
Treatment: Treatment Method ‘Paracetamol’Treatment Method ‘A’
State: State ‘Headache’no State ‘Migraine’
Study Type: Study Type ‘Phase III’Variable to be measured: Variable ‘Efficacy’Target: Variable ‘Gender’ having Value ‘female’
Variable ‘Age’ having Value < ‘18’
Table 3: An example study objective points of interest.
For the construction of the selection criteria it is not necessary to know the relation between thedifferent points of interest of the study objective, because the criteria are based on the treatmentmethods and disease used for the study objective. These points cannot be derived automatically,due to the lacking technology of natural language recognition. Thus, these points of interesthave to be supplied by the user or by another PROSYS-part. In Table 3 points of interest to thestudy objective of an example trial are mentioned. According to this table, a study objective canbe divided in several parts. Now these several parts and the study objective will be modelledusing PSM and an example population will be given.

Patient Selection in Clinical Trials UIC/BME research center
32
Figure 9: PSM model of the study objective.
As an example the following study objective used in Table 3 is used (SO for short). This studyobjective could be defined in terms of the PSM model and leads to the following population ofthe PSM model:
Pop(State) = ‘Headache’‘Migraine’
Pop(Study Objective) = ‘SO’
Pop(Treatment Method) = ‘Paracetamol’‘A’
Pop(Study Type) = ‘Phase III’
Pop(Variable) = ‘Age’‘Gender’
Pop(Value) = ‘18’‘female’
Pop(Operator) = <=
Pop(ISO1) = applying_to being_subject_of‘SO’ ‘Headache’
Pop(ISO2) = applying_to being_subject_of‘SO’ ‘Paracetamol’
Study Type(STP-name)
Value
State(ST-name)
Variable(VAR-name)
TreatmentMethod
(TM-name)
Study Objective(SO-name)
INF
ISO3
HVAL
ISO2
ISO1applying_tobeing_subject_of
influences
being_influenced_by
applying_to
applying_to
having_value
being_value_of
being_subject_of
being_subject_of
EX2
applying_to_exclusion
being_exclusion_of
EX1
applying_to_exclusionbeing_exclusion_of
Operator(OP-name)
being_operator_ofRVAR
with_restriction
being_restriction_of

Patient Selection in Clinical Trials UIC/BME research center
33
‘SO’ ‘A’
Pop(ISO3) = applying_to being_subject_of‘SO’ ‘Efficacy’
Pop(RVAR)
= with_restriction
being_restriction_ofhaving_value being_operator_of being_value_of
‘SO’ ‘Gender’ = ‘female’‘SO’ ‘Age’ < ‘18’
Pop(HVAL) = having_value being_operator_of being_value_of‘Gender’ = ‘female’
‘Age’ < ‘18’
Pop(INF) = being_influenced_by influences‘SO’ ‘Phase III’
Pop(EX1) = ∅
Pop(EX2) = with_exclusion being_exclusion_of‘SO’ ‘Migraine’
Now, by means of a formal model, the text of a study objective can be transformed into formalparts. In the according PROSYS-part the information on the treatment methods, states andvariables should be obtained from another PROSYS-parts or from the user.
Construction of the concept class Selection Criteria:
Table 2 showed the items that could lead to selection criteria for each class. These classes were[Spilker 1985]:
1) Characteristics of patients.2) Characteristics of the disease and its treatment.3) Environmental and other factors.4) Safety criteria.
These classes are described independently due to differences in developing selection criteria foreach class.
When dealing with knowledge based systems it is useful when the system uses knowledge thatwas defined in the past. When a criterion is defined by a user, this criterion is linked to a stateor treatment. When in another objective this state or treatment is used, this criterion will beadded automatically.
If a knowledge based system uses a kind of history function, the proposed selection criteriawould be better in the future due to a kind of learning function. This function should recordcriteria that were defined by the user and these criteria should be evaluated after the protocolhas been approved by a committee. The criteria that were actually used should than be recorded

Patient Selection in Clinical Trials UIC/BME research center
34
for future use. The model for developing selection criteria should thus be able to record somekind of history of old selection criteria. To provide knowledge that is necessary to implementsuch a kind of history, the user will be able to add criteria. The user is able to add all kinds ofcriteria. When a future objective is based on the same treatment or state, these defined criteriacould then be used.
Construction of the concept class Patient Characteristics:
In the concept class Patient Characteristics selection criteria are developed based on thecharacteristics of patients that one wants to include in the clinical trial. From the studyobjective mentioned in Table 3, the following points of interest to the patient characteristics canbe concluded:
• Variable ‘Gender’ having Value ‘female’ (PC1).• Variable ‘Age’ having Value < ‘18’ (PC2).• Treatment Method ‘A’ uses Material ‘B’ (PC3).
These points of interest should lead to the following patient characteristics criteria:
• Patient should be of gender female.• Patient should be of age < 18.• Patient should be of not hypersensitive against B.
According to the mentioned example, the patient characteristics criteria are based on thefollowing points on interest:
• Variable: If a point of interest is Age greater than 18, then this leads to the criteria:Age greater than 18.
• Material: A point of interest to the study objective is the treatment method that is goingto be evaluated. In most case a treatment method uses materials. If the patient hashypersensitivity towards this material he should be excluded from the trial because theresults of the screenings could be inaccurate, or the patient's health could be injeopardy.

Patient Selection in Clinical Trials UIC/BME research center
35
Figure 10: PSM model of the Patient Characteristics.
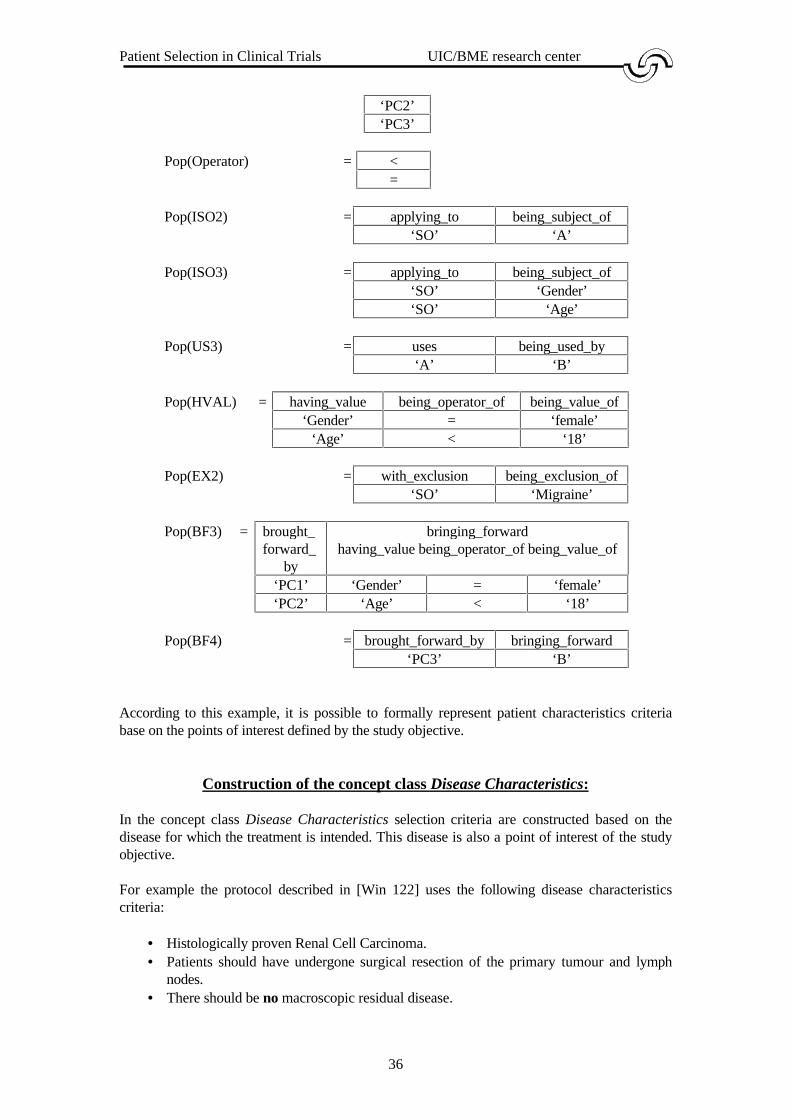
Now the PSM model of the patient characteristics criteria will be populated using the followingpatient characteristics criteria PC1, PC2 and PC3 and the study objective used in Table 3 andthe extra information that a treatment A uses material B:
Pop(Material) = ‘B’
Pop(Study Objective) = ‘SO’
Pop(Treatment Method) = ‘A’
Pop(Variable) = ‘Age’‘Gender
Pop(Value) = ‘18’‘female’
Pop(Patient Characteristics) = ‘PC1’
Study Objective(SO-name)
PatientsCharacteristics
(PC-name)
Material(MA-name)
TreatmentMethod
(TM-name)
ValueVariable
(VAR-name)
having_value being_value_ofHVAL
BF4brought_forward_by
bringing_forward
BF3 brought_forward_by
bringing_forward
ISO2 US3uses being_used_by
being_subject_of
applying_to
ISO3
being_subject_ofapplying_to
Operator(OP-name)
being_operator_of
EX2
being_exclusion_ofwith_exclusion
Patient Selection in Clinical Trials UIC/BME research center
36
‘PC2’‘PC3’
Pop(Operator) = <=
Pop(ISO2) = applying_to being_subject_of‘SO’ ‘A’
Pop(ISO3) = applying_to being_subject_of‘SO’ ‘Gender’‘SO’ ‘Age’
Pop(US3) = uses being_used_by‘A’ ‘B’
Pop(HVAL) = having_value being_operator_of being_value_of‘Gender’ = ‘female’
‘Age’ < ‘18’
Pop(EX2) = with_exclusion being_exclusion_of‘SO’ ‘Migraine’
Pop(BF3) = brought_forward_
by
bringing_forwardhaving_value being_operator_of being_value_of
‘PC1’ ‘Gender’ = ‘female’‘PC2’ ‘Age’ < ‘18’
Pop(BF4) = brought_forward_by bringing_forward‘PC3’ ‘B’
According to this example, it is possible to formally represent patient characteristics criteriabase on the points of interest defined by the study objective.
Construction of the concept class Disease Characteristics:
In the concept class Disease Characteristics selection criteria are constructed based on thedisease for which the treatment is intended. This disease is also a point of interest of the studyobjective.
For example the protocol described in [Win 122] uses the following disease characteristicscriteria:
• Histologically proven Renal Cell Carcinoma.• Patients should have undergone surgical resection of the primary tumour and lymph
nodes.• There should be no macroscopic residual disease.

Patient Selection in Clinical Trials UIC/BME research center
37
• No unstable angina pectoris or recent (6 months) myocardial infarction.• No patients with signs or symptoms of systemic metastatic Renal Cell Carcinoma.• No patients who require or are likely to require corticosteriods for intercurrent disease.• No patients who receive radiation or chemotherapy.
From these disease characteristics criteria, the following points of interest can be concluded:
• State ‘Renal Cell Carcinoma’, no ‘systemic metastatic Renal Cell Carcinoma’, no‘macroscopic residual disease’, no ‘unstable angina pectoris’, no ‘recent (6 months)myocardial infarction’.
• Treatment Method ‘surgical resection’, no ‘corticoids’, no ‘radiation’, no‘chemotherapy’.
These points of interest could then be written as disease characteristics criteria using standardsentences:
• Patient should have Renal Cell Carcinoma (DC1).• Patient should have no systemic metastatic Renal Cell Carcinoma (DC2).• Patient should have no macroscopic residual disease (DC3).• Patient should have no unstable angina pectoris (DC4).• Patient should have no recent (6 months) myocardial infarction (DC5).• Patient should have been medicated using surgical resection (DC6).• Patient should have been medicated using no corticoids (DC7).• Patient should have been medicated using no radiation (DC8).• Patient should have been medicated using no chemotherapy (DC9)
According to this example, the selection criteria for the concept class Disease Characteristicsare based on the following points of interest:
• Treatment: This point of interest covers the treatment at which the clinical trial isaimed. Exclusion treatments could be defined as Study Objective with exclusionTreatment ‘A’. This could lead to automatic development of exclusion criteria fortreatments that could influence the result of the clinical trial.
• State: The disease that is being evaluated by conducting a clinical trial influences thedevelopment of Disease Characteristics criteria. Here could also exclusion states bedefined as Study Objective with exclusion State ‘State C’.
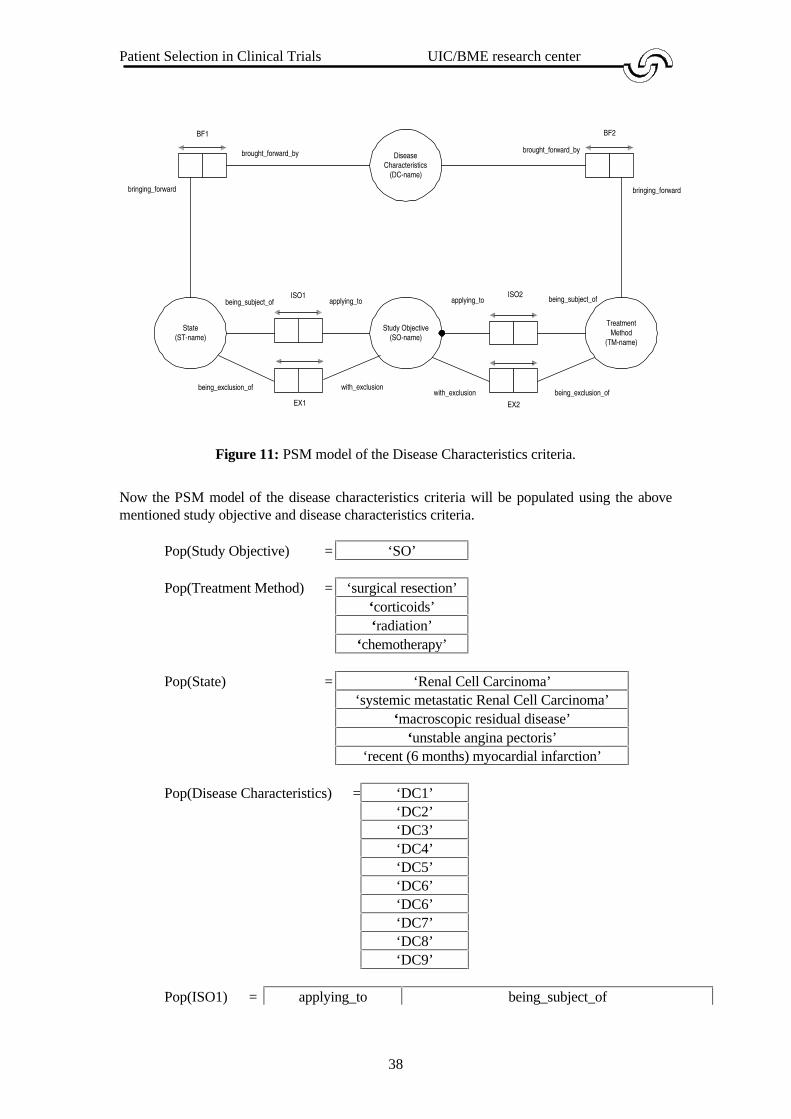
Figure 11 shows a PSM model of constructing the Disease Characteristics criteria.
Patient Selection in Clinical Trials UIC/BME research center
38
Figure 11: PSM model of the Disease Characteristics criteria.
Now the PSM model of the disease characteristics criteria will be populated using the abovementioned study objective and disease characteristics criteria.
Pop(Study Objective) = ‘SO’
Pop(Treatment Method) = ‘surgical resection’‘corticoids’‘radiation’
‘chemotherapy’
Pop(State) = ‘Renal Cell Carcinoma’‘systemic metastatic Renal Cell Carcinoma’
‘macroscopic residual disease’‘unstable angina pectoris’
‘recent (6 months) myocardial infarction’
Pop(Disease Characteristics) = ‘DC1’‘DC2’‘DC3’‘DC4’‘DC5’‘DC6’‘DC6’‘DC7’‘DC8’‘DC9’
Pop(ISO1) = applying_to being_subject_of
DiseaseCharacteristics
(DC-name)
Study Objective(SO-name)
State(ST-name)
TreatmentMethod
(TM-name)
brought_forward_bybrought_forward_by
BF1 BF2
ISO1 ISO2
bringing_forward bringing_forward
applying_toapplying_tobeing_subject_of being_subject_of
with_exclusion being_exclusion_ofEX2
with_exclusionbeing_exclusion_of
EX1
Patient Selection in Clinical Trials UIC/BME research center
39
‘SO’ ‘Renal Cell Carcinoma’
Pop(ISO2) = applying_to being_subject_of‘SO’ ‘surgical resection’
Pop(EX1) = with_exclusion being_exclusion_of‘SO’ ‘systemic metastatic Renal Cell Carcinoma’‘SO’ ‘macroscopic residual disease’‘SO’ ‘unstable angina pectoris’‘SO’ ‘recent (6 months) myocardial infarction’
Pop(EX2) = with_exclusion being_exclusion_of‘SO’ ‘corticoids’‘SO’ ‘radiation’‘SO’ ‘chemotherapy’
Pop(BF1) = brought_forward_by bringing_forward‘DC1’ ‘Renal Cell Carcinoma’‘DC2’ ‘systemic metastatic Renal Cell Carcinoma’‘DC3’ ‘macroscopic residual disease’‘DC4’ ‘unstable angina pectoris’‘DC5’ ‘recent (6 months) myocardial infarction’
Pop(BF2) = brought_forward_by bringing_forward‘DC6’ ‘surgical resection’‘DC7’ ‘corticoids’‘DC8’ ‘radiation’‘DC9’ ‘chemotherapy’
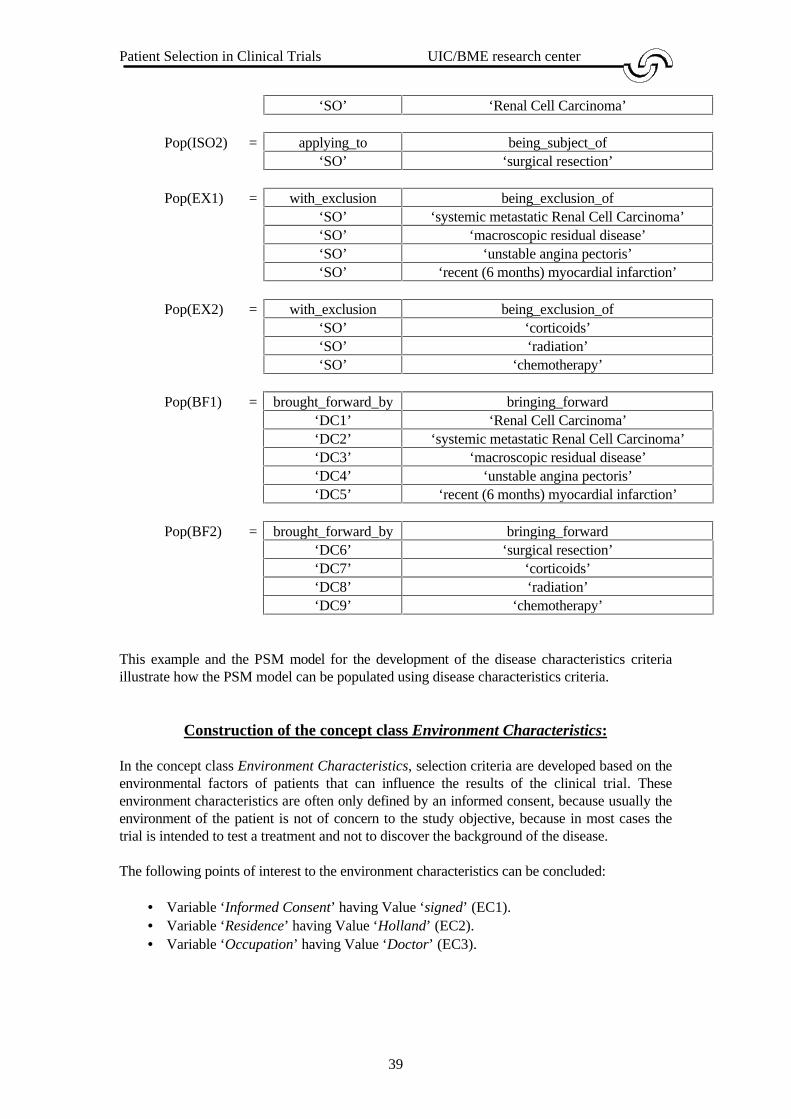
This example and the PSM model for the development of the disease characteristics criteriaillustrate how the PSM model can be populated using disease characteristics criteria.
Construction of the concept class Environment Characteristics:
In the concept class Environment Characteristics, selection criteria are developed based on theenvironmental factors of patients that can influence the results of the clinical trial. Theseenvironment characteristics are often only defined by an informed consent, because usually theenvironment of the patient is not of concern to the study objective, because in most cases thetrial is intended to test a treatment and not to discover the background of the disease.
The following points of interest to the environment characteristics can be concluded:
• Variable ‘Informed Consent’ having Value ‘signed’ (EC1).• Variable ‘Residence’ having Value ‘Holland’ (EC2).• Variable ‘Occupation’ having Value ‘Doctor’ (EC3).
Patient Selection in Clinical Trials UIC/BME research center
40
These points of interest should lead to the following environment characteristics criteria:
• Patient should have Informed Consent signed,• Patient should have residence Holland.• Patient should have occupation doctor.
According to the mentioned example, the environment characteristics criteria are based on thefollowing point of interest:
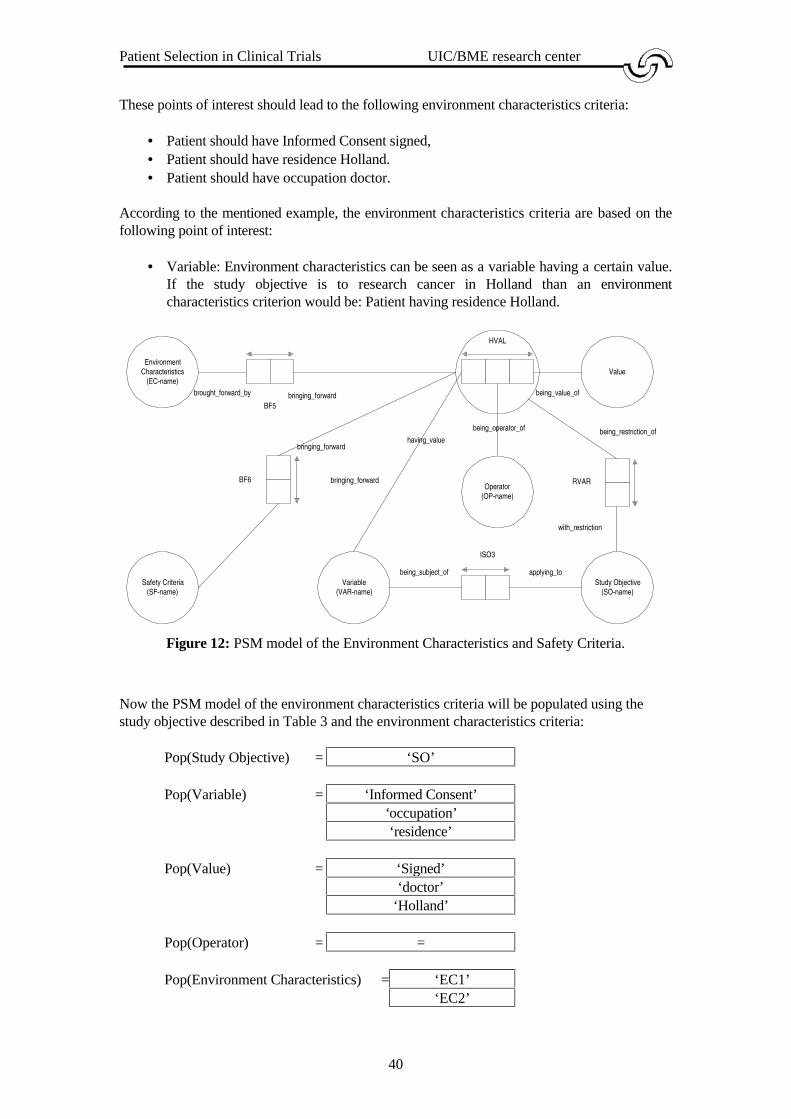
• Variable: Environment characteristics can be seen as a variable having a certain value.If the study objective is to research cancer in Holland than an environmentcharacteristics criterion would be: Patient having residence Holland.
Figure 12: PSM model of the Environment Characteristics and Safety Criteria.
Now the PSM model of the environment characteristics criteria will be populated using thestudy objective described in Table 3 and the environment characteristics criteria:
Pop(Study Objective) = ‘SO’
Pop(Variable) = ‘Informed Consent’‘occupation’‘residence’
Pop(Value) = ‘Signed’‘doctor’
‘Holland’
Pop(Operator) = =
Pop(Environment Characteristics) = ‘EC1’‘EC2’
EnvironmentCharacteristics
(EC-name)
Variable(VAR-name)
Value
Study Objective(SO-name)
BF5
brought_forward_by bringing_forward
ISO3
applying_tobeing_subject_of
HVAL
having_value
being_value_of
Safety Criteria(SF-name)
BF6
being_restriction_of
bringing_forward
Operator(OP-name)
being_operator_of
RVAR
with_restriction
bringing_forward

Patient Selection in Clinical Trials UIC/BME research center
41
‘EC3’
Pop(Safety Criteria) =�
Pop(ISO3) =�
Pop(RVAR)
= with_restriction
being_restriction_of
having_value being_operator_of being_value_of‘SO’ ‘Informed
consent’= ‘signed’
‘SO’ ‘occupation’ = ‘doctor’‘SO’ ‘residence’ = ‘Holland’
Pop(HVAL) = having_value being_operator_of being_value_of‘Informed consent’ = ‘signed’
‘occupation’ = ‘doctor’‘residence’ = ‘Holland’
Pop(BF5)
= brought_forward_by
bringing_forward
having_value being_operator_of being_value_of‘SO’ ‘Informed
consent’= ‘signed’
‘SO’ ‘occupation’ = ‘doctor’‘SO’ ‘residence’ = ‘Holland’
According to this example, it is possible to formally represent environment characteristicscriteria based on the points of interest defined by the study objective.
Construction of the concept class Safety Criteria:
Most patients receive a physical examination prior to entry into a clinical study [Spilker 1985].The selection criteria may list specific findings that are not acceptable for entry, e.g. thepatient's health could be jeopardised by participating in the trial. For example, the followingsafety criteria can be used:
• Variable ‘deep tendon reflexes’ having Value ‘present’ (SF1).• Variable ‘EGG’ having Value ‘normal’ (SF2).
These points of interest should lead to the following safety criteria:
• Patient should have deep tendon reflexes present.• Patient should have EGG normal.
According to this example, the safety criteria are based on variables having a certain value or acertain range. Figure 12 shows the PSM model for the development of the safety criteria.
Patient Selection in Clinical Trials UIC/BME research center
42
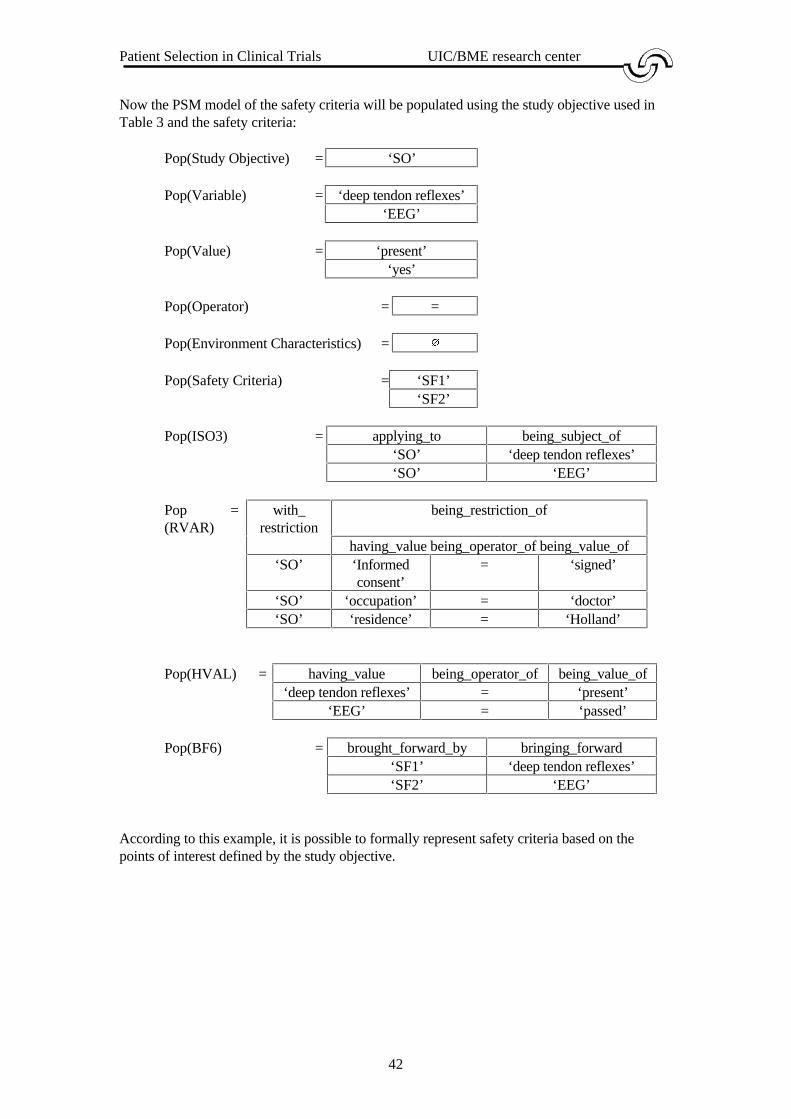
Now the PSM model of the safety criteria will be populated using the study objective used inTable 3 and the safety criteria:
Pop(Study Objective) = ‘SO’
Pop(Variable) = ‘deep tendon reflexes’‘EEG’
Pop(Value) = ‘present’‘yes’
Pop(Operator) = =
Pop(Environment Characteristics) =�
Pop(Safety Criteria) = ‘SF1’‘SF2’
Pop(ISO3) = applying_to being_subject_of‘SO’ ‘deep tendon reflexes’‘SO’ ‘EEG’
Pop(RVAR)
= with_restriction
being_restriction_of
having_value being_operator_of being_value_of‘SO’ ‘Informed
consent’= ‘signed’
‘SO’ ‘occupation’ = ‘doctor’‘SO’ ‘residence’ = ‘Holland’
Pop(HVAL) = having_value being_operator_of being_value_of‘deep tendon reflexes’ = ‘present’
‘EEG’ = ‘passed’
Pop(BF6) = brought_forward_by bringing_forward‘SF1’ ‘deep tendon reflexes’‘SF2’ ‘EEG’
According to this example, it is possible to formally represent safety criteria based on thepoints of interest defined by the study objective.

Patient Selection in Clinical Trials UIC/BME research center
43
A model for developing selection criteria
In the previous paragraphs, models have been presented for each subclass of the concept classSelection Criteria. In this paragraph these models will be combined and the history functionwill be added to these models. Figure 13 shows a model for the development of selectioncriteria. This model has the following capabilities:
• To store selection criteria of any of the described selection criteria classes [Table 2].• To store disease characteristics criteria that are defined by the user. This function
provides a primitive kind of history function and provides the model a kind of learningcapability.
• To develop new selection criteria an inference mechanism is used. This mechanismuses the knowledge that is recorded according to the model.
In the following section, an inference mechanism will be developed. This inference mechanismand the knowledge model will be used to build the PROSYS-part for supporting thedevelopment of selection criteria.

Patient Selection in Clinical Trials UIC/BME research center
44
Figure 13: PSM model for the development of selection criteria.
Study Type(STP-name)
DiseaseCharacteristics
(DC-name)
PatientCharacteristics
(PC-name)
EnvironmentCriteria
(EC-name)
Safety Criteria(SF-name)
Selection CriteriaStudy Objective(SO-name)
Variable(VAR-name)
Value
Text(String)
Number(Nr)
State(ST-name)
TreatmentMethod
(TM-name)
Material(MA-name)
being_subject_of
ISO1
applying_to
influences
being_influenced_by
having_value
being_value_of HVAL
ISO2
ISO3
being_subject_of
being_subject_of
applying_to
applying_to
INF
brought_forward_by
bringing_forward
BF1
BF2
brought_forward_bybringing_forward
BF4
BF3
brought_forward_by
brought_forward_by
bringing_forward
bringing_forward
BF5
BF6
brought_forward_by
brought_forward_by
bringing_forward
bringing_forward
HBF2
HBF1
history_bringing_forward
history_brought_forward_by
history_bringing_forward
history_brought_forward_by
US3
uses being_used_by
PO6
being_part_of
comprises
Selection Criteria Set
being_subject_of
being_subject_of
Operator(OP-name)
being_operator_of
with_exclusion
being_exclusion_of
EX2
EX3
being_exclusion_ofwith_exclusion
with_exclusion
being_exclusion_of
EX4
EX1
with_exclusion
being_exclusion_of
Data-code(Date)
BF7brought_forward_by
bringing_forward
EvaluationMethod
(EM-name)
BF8
brought_forward_by
bringing_forward
RVAR
being_restriction_of
with_restriction

Patient Selection in Clinical Trials UIC/BME research center
45
Bridge-types are not modelled in the knowledge model, but the one to one relationship will bepresented in the population7 . The following relation classes represent the bridge-types:
• B-STP: Bridge between the concept class Study Type and its label type STP-name.• B-SO: Bridge between the concept class Study Objective and its label type SO-name.• B-STRING: Bridge between the concept class Text and its label-type String.• B-NR: Bridge between the concept class Number and its label type Int.• B-DC: Bridge between the concept class Disease Characteristics and its label type DC-
name..• B-PC: Bridge between the concept class Patient Characteristics and its label type PC-
name.• B-EC: Bridge between the concept class Environment Characteristics and its label type
EC-name.• B-SF: Bridge between the concept class Safety Criteria and its label type SF-name.
These bridge-types are needed by the reasoning mechanism to establish a link between anabstract and a concrete value. The reasoning will make use of a combined model presented inFigure 8 and Figure 13. These figures can be combined by the concept classes that are used inboth models. This is not explicitly done due to the
Figure 13 shows the graphical representation of an information structure, that is defined by:
� = {Material, Treatment Method, State, Selection Criteria, Selection Criteria Set,Disease Characteristics, Patient Characteristics, Environment Characteristics,Safety Criteria, Study Type, Study Objective, Variable, Value, Operator, Text,Number, MA-name, TM-name, ST-name, VAR-name, STP-name, SO-name,DC-name, PC-name, EC-name, SF-name, OP-name, String, Nr, INF, PO6, US3,ISO1, ISO2, ISO3, HBF1, HBF2, BF1, BF2, BF3, BF4, BF5, BF6, BF7, BF8,HVAL, RVAR, EX1, EX2, EX3, EX4}
£ = {MA-name, TM-name, ST-name, VAR-name, STP-name, SO-name, DC-name,PC-name, EC-name, SF-name, OP-name, String, Nr}
εε = {Material, Treatment Method, State, Selection Criteria, Disease Characteristics,Patient Characteristics, Environment Characteristics, Safety Criteria, StudyType, Study Objective, Variable, Value, Operator, Text, Number }
� = { INF, PO6, US3, ISO1, ISO2, ISO3, HBF1, HBF2, BF1, BF2, BF3, BF4,BF5, BF6, BF7, BF8, HVAL, RVAR, EX1, EX2, EX3, EX4 }
�= {Selection Criteria Set}
This model does not fulfil all requirements of a PSM-model. Several exceptions have beenmade. The fact-type is exclusion of defines an exclusion operator between two concepts. In thecase of the exclusions connected to the study objective, it would be a more elegant way tomodel this exclusion by using a concept class exclusion. This would make the relation classesEX1, EX2, EX3 and EX4 superfluous. In the case of a treatment method which is excluded bya state this would cause additional information to be recorded, because a relation has to beadded between the concept classes State and Treatment Method and also a relation between thisrelation and the concept class Exclusion. This would also be the case when a treatment methodis excluded by another treatment method, so in my opinion it easier to create an exclusion by arelation class than to create a new concept class, because it requires less information to berecorded.
7 See appendix A and [Hofstede 1994] for more information on bridge-types.

Patient Selection in Clinical Trials UIC/BME research center
46
Another exception to a PSM-model is the fact that in this model knowledge is inherited. This isdone by the inference mechanism. When the initial population is created, the selection criteriaclasses are empty for a specified study objective. By using inference steps, the inferencemechanism adds knowledge to the model based on knowledge already in the model. Theinference engine will populate the brought forward classes and will populate the classes ofselection criteria with structured knowledge. For example, a criterion based on an exclusionstate ‘Fever’ should be entered by the inference mechanism as ‘no Fever’. The advantage ofthis construction is that criteria are directly stored in the model and the model is better suited tobe a knowledge base. The disadvantage is that this is a case of redundancy. This would be aproblem when a selection criteria should be divided in atomic concepts. In this thesis this is notthe case and the inference mechanism is able to deduct the exclusion state by means ofbackward chaining. The selection criteria classes are populated by the inference mechanism andthe inference mechanism will therefore be responsible for the identification of the concepts thatare stored in the concept classes.
These exceptions are thus made to extend the power of the knowledge model. All side-effectshave been taken into account and the redundancy is controllable, so it is sound to use theseexceptions for the use of expressive power for the knowledge model.
The knowledge model has been described completely now and in the next section the inferencemechanism will be designed to develop the selection criteria.
2.4 An inference mechanism for developing selection criteria
At the beginning of the reasoning process only the concept class Study Objectives and a fewattached concept classes are populated. This population will be derived directly from the useror will be delivered by other PROSYS-parts. To develop the selection criteria, the inferenceengine will populate the rest of the model and thus develop the selection criteria using inferencesteps and sometimes interaction with the user.
There are several aspects that influence the development of the selection criteria:
• Study type: If the study type is Phase I, then there has to be interaction with the user toconfirm if there have to be made selection criteria for the classes patient characteristicsand disease characteristics.
• Study Objective: The study objective will be entered as a sentence into the system. Theuser has to point out which points on interest can be detected in the study objectivesand which variables have to be measured. Conflicting aspects in the points of interestshould be detected by the inference engine.
Generating a set of selection criteria consists of three steps:
1. Developing selection criteria based on the concepts that are connected to the studyobjective by the is subject of , with restriction and is exclusion of relations.
2. Developing selection criteria based on several inference steps for generating andretrieving knowledge. As long there is generated or retrieved new knowledge theinference steps are repeated.
3. Trying to improve the completeness of the selection criteria set by searching forstandard criteria and if these are not defined, defining them at this point.
Patient Selection in Clinical Trials UIC/BME research center
47
To show how the inference engine will populate this model, an initial population is given andthe inference steps will be explained using this sample population. The way in which the initialpopulation is created is the same way as in which the knowledge based system will create theinitial population. This initial population is defined in Appendix F.
Deriving the study objective:
The user will be asked to provide the study objective. This provision can be done by the user orby another PROSYS-part. After the study objective is analysed by the system e.g., the systemuses pattern matching to look for states, the study type, treatments and variables, the user willbe asked to confirm the points of interest. At this point the user is also able to alter, remove andadd the points of interest.
For example, the following study objective could be used:
“To evaluate the quality of life of female, not elderly adults who have been treatedwith Interleukin-1 and Interleukin-2 used to medicate the disease Renal CellCarcinoma and not having systemic metastatic Renal Cell Carcinoma in a phaseIII clinical trial.”
This sentence is very hard to understand, so the first step will be to write this complex sentenceis several straight forward sentences which than can be directly modelled. So to illustrate theinference engine, the following study objective is used:
• To evaluate the quality of life on patients treated with Interleukin-1 or Interleukin-2.• Patients having gender female and age greater than 18 and smaller than 65.• To evaluate the efficacy of Interleukin-1 and Interleukin-2.• Patients being treated with Interleukin-1 and Interleukin-2.• Patients having Renal Cell Carcinoma and not having systemic metastatic Renal Cell
Carcinoma.• Study type Phase III.
This natural language study objective can be presented in a more formal structure using LISA-D:
• Study Objective applying to Variable ‘quality of life’.• Study Objective with restriction (Variable ‘gender’, Operator ‘=’, Value ‘female’).• Study Objective with restriction (Variable ‘age’, Operator ‘>’, Value ‘18’).• Study Objective with restriction (Variable ‘age’, Operator ‘<’, Value ‘65’).• Study Objective applying to Variable ‘efficacy’.• Study Objective applying to Treatment Method ‘Interleukin-1’.• Study Objective applying to Treatment Method ‘Interleukin-2’.• Study Objective applying to State ‘Renal Cell Carcinoma’.• Study Objective with exclusion State ‘systemic metastatic Renal Cell Carcinoma’.• Study Objective being influenced by Study Type ‘Phase III’.

Patient Selection in Clinical Trials UIC/BME research center
48
Also the following knowledge is defined by another PROSYS-part:
• Treatment Method ‘Interleukin-1’ uses Material ‘etiocholanolone’.• Treatment Method ‘Interleukin-2’ uses Material ‘monocytes’.
Also several known side effects are also in the model provided by [d’Hollosy 1995]. Thereasoning mechanism should thus be able to take into account the knowledge from the modelprovided by [d’Hollosy 1995].
These structured sentences result in the population described in appendix F. In the nextsections, the inference steps are explained to develop the selection criteria. These inferencesteps use the models presented in Figure 8 and Figure 13. The initial population presented inappendix F will be used to clarify the inference steps.
2.4.1 Preparation for the inference mechanism
Before the inference mechanism can be developed there have to be defined several macros tosupport the addition of knowledge to the knowledge model. The first addition macro that ispresented in this thesis is a macro to add an instance to an abstract concept class. Also arelation must be added in its associated bridge type:
Macro BF_ST_Add8 :
Input: Exclusion: Value which states if the concept should be converted toan exclusion criterion. For example ‘no’.
Concept: The concept which the criterion aims. For example‘Fever’.
Inference step: BF_ST_Add (Exclusion, Concept) =State (in Disease Characteristics WITH DC-name Exclusion Concept)
Explanation: This macro is defined to add a selection criteria based on a state or excludedstate. The function in adds the abstract values to the concept and relationclasses and after this the concrete values are added to a label-type.
If it is necessary to add a criterion based on the excluded state ‘fever’ the following commandis executed:
BF_ST_Add (‘no’, ‘fever’)
8 BF_ST_Add = Add criterion Brought Forward by State
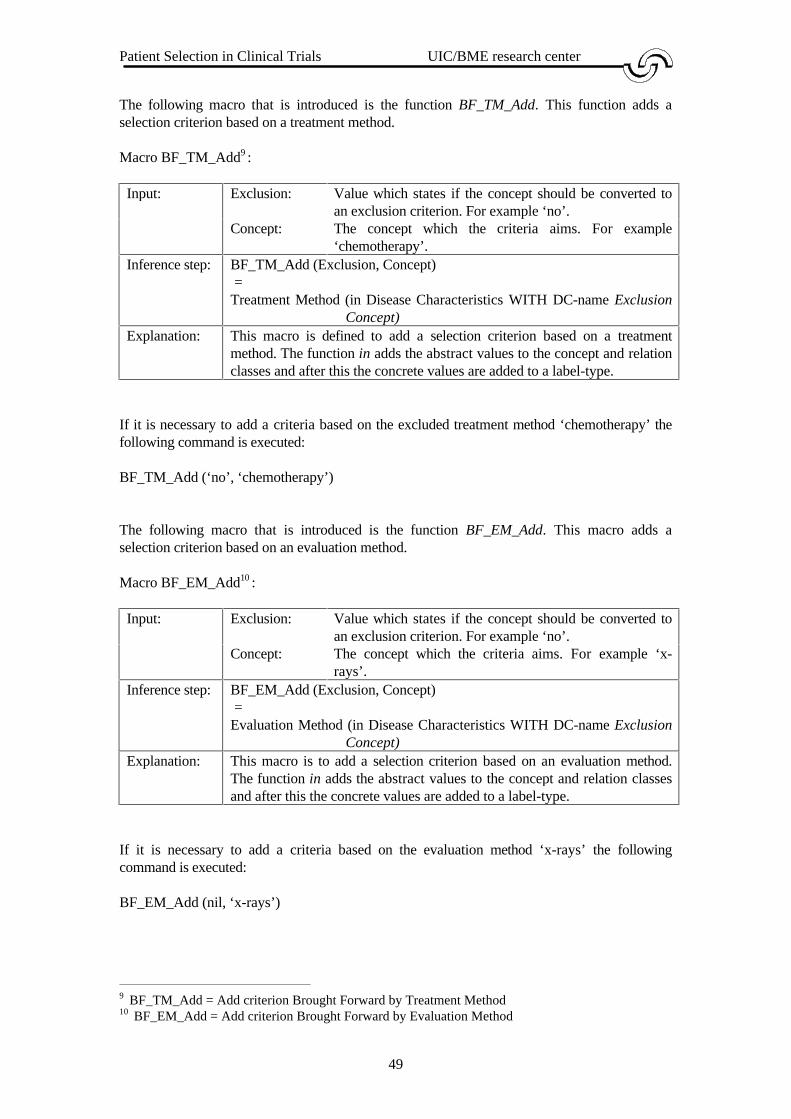
Patient Selection in Clinical Trials UIC/BME research center
49
The following macro that is introduced is the function BF_TM_Add. This function adds aselection criterion based on a treatment method.
Macro BF_TM_Add9 :
Input: Exclusion: Value which states if the concept should be converted toan exclusion criterion. For example ‘no’.
Concept: The concept which the criteria aims. For example‘chemotherapy’.
Inference step: BF_TM_Add (Exclusion, Concept) =Treatment Method (in Disease Characteristics WITH DC-name Exclusion
Concept)Explanation: This macro is defined to add a selection criterion based on a treatment
method. The function in adds the abstract values to the concept and relationclasses and after this the concrete values are added to a label-type.
If it is necessary to add a criteria based on the excluded treatment method ‘chemotherapy’ thefollowing command is executed:
BF_TM_Add (‘no’, ‘chemotherapy’)
The following macro that is introduced is the function BF_EM_Add. This macro adds aselection criterion based on an evaluation method.
Macro BF_EM_Add10 :
Input: Exclusion: Value which states if the concept should be converted toan exclusion criterion. For example ‘no’.
Concept: The concept which the criteria aims. For example ‘x-rays’.
Inference step: BF_EM_Add (Exclusion, Concept) =Evaluation Method (in Disease Characteristics WITH DC-name Exclusion
Concept)Explanation: This macro is to add a selection criterion based on an evaluation method.
The function in adds the abstract values to the concept and relation classesand after this the concrete values are added to a label-type.
If it is necessary to add a criteria based on the evaluation method ‘x-rays’ the followingcommand is executed:
BF_EM_Add (nil, ‘x-rays’)
9 BF_TM_Add = Add criterion Brought Forward by Treatment Method10 BF_EM_Add = Add criterion Brought Forward by Evaluation Method
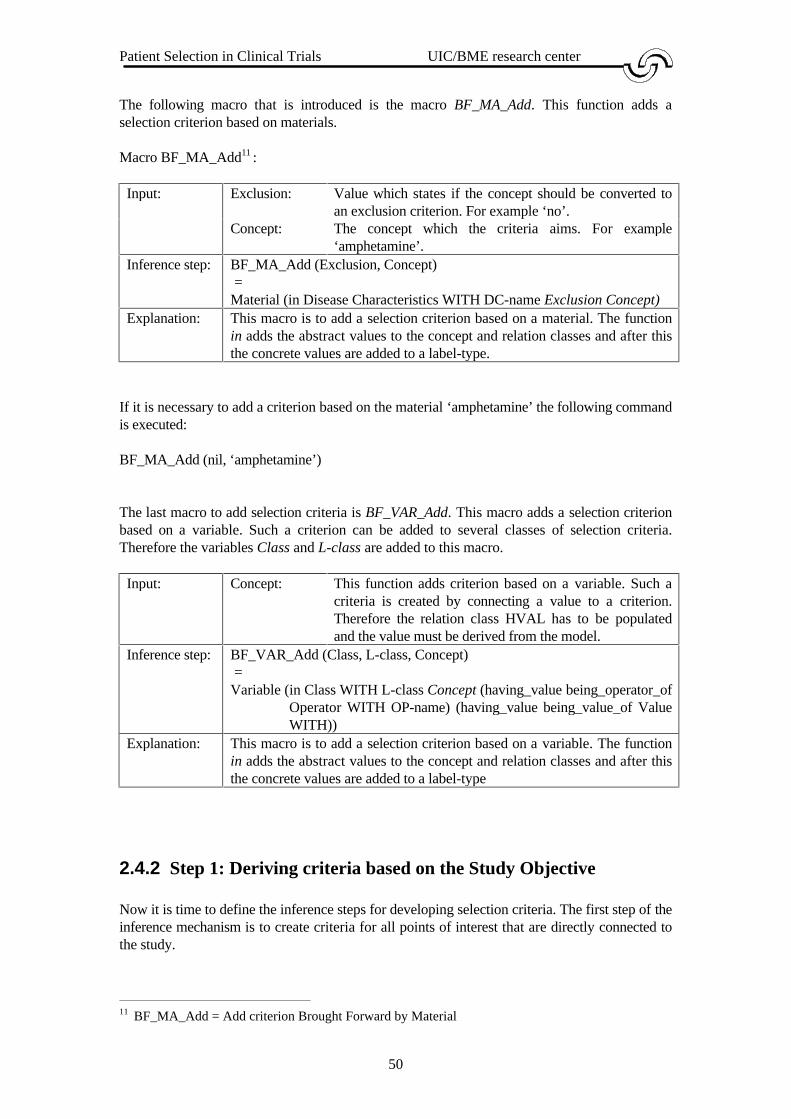
Patient Selection in Clinical Trials UIC/BME research center
50
The following macro that is introduced is the macro BF_MA_Add. This function adds aselection criterion based on materials.
Macro BF_MA_Add11 :
Input: Exclusion: Value which states if the concept should be converted toan exclusion criterion. For example ‘no’.
Concept: The concept which the criteria aims. For example‘amphetamine’.
Inference step: BF_MA_Add (Exclusion, Concept) =Material (in Disease Characteristics WITH DC-name Exclusion Concept)
Explanation: This macro is to add a selection criterion based on a material. The functionin adds the abstract values to the concept and relation classes and after thisthe concrete values are added to a label-type.
If it is necessary to add a criterion based on the material ‘amphetamine’ the following commandis executed:
BF_MA_Add (nil, ‘amphetamine’)
The last macro to add selection criteria is BF_VAR_Add. This macro adds a selection criterionbased on a variable. Such a criterion can be added to several classes of selection criteria.Therefore the variables Class and L-class are added to this macro.
Input: Concept: This function adds criterion based on a variable. Such acriteria is created by connecting a value to a criterion.Therefore the relation class HVAL has to be populatedand the value must be derived from the model.
Inference step: BF_VAR_Add (Class, L-class, Concept) =Variable (in Class WITH L-class Concept (having_value being_operator_of
Operator WITH OP-name) (having_value being_value_of ValueWITH))
Explanation: This macro is to add a selection criterion based on a variable. The functionin adds the abstract values to the concept and relation classes and after thisthe concrete values are added to a label-type
2.4.2 Step 1: Deriving criteria based on the Study Objective
Now it is time to define the inference steps for developing selection criteria. The first step of theinference mechanism is to create criteria for all points of interest that are directly connected tothe study.
11 BF_MA_Add = Add criterion Brought Forward by Material

Patient Selection in Clinical Trials UIC/BME research center
51
When structuring the study objective five kinds of criteria can be distinguished:
• The states at which the study objective aims must be a symptom of the patient. Thesestates must thus lead to disease characteristics criteria.
• The states that may not be present which are derived from the study objective mustalso lead to disease characteristics criteria. A reason for the definitions of suchexclusions could be that a certain state could interfere with the treatment or even couldjeopardise the patient’s health.
• The treatments that are used during the execution of the clinical trial. These treatmentsmust lead to disease characteristics criteria.
• The treatments which could interfere with the tested treatments and may not have beenperformed on the patients and are defined by the study objective must also lead todisease characteristics criteria.
• The restrictions of the study population that are connected to the study objective mustalso lead to selection criteria.
Step 1.1: States that are connected to the study objective
Uses: Text of the study objective so-text.Creates: Disease characteristics criteria which are based on states that are
connected to the study objective.Inference step: BF_ST_Add (nil, so-text IS NAME OF Study Objective applying_to
State WITH ST-name)Explanation: This step generates the states that are connected to the study objective
and creates selection criteria of these states.
Step 1.2: Exclusion states that are connected to the study objective
Uses: Text of the study objective so-text.Creates: Disease characteristics criteria which are based on exclusion states that
are connected to the study objective.Inference step: BF_ST_Add (‘no’, so-text IS NAME OF Study Objective
with_exclusion State WITH ST-name)Explanation: This step generates the exclusion states that are connected to the study
objective and creates selection criteria of these states.
Step 1.3: Treatments that are connected to the study objective
Uses: Text of the study objective so-text.Creates: Disease characteristics criteria which are based on treatments that are
connected to the study objective.Inference step: BF_TM_Add (nil, so-text IS NAME OF Study Objective applying_to
Treatment Method WITH TM-name)Explanation: This step generates the treatment methods that are connected to the
study objective and creates selection criteria of these treatmentmethods.

Patient Selection in Clinical Trials UIC/BME research center
52
Step 1.4: Exclusion treatments that are connected to the study objective
Uses: Text of the study objective so-text.Creates: Disease characteristics criteria which are based on exclusion treatments
that are connected to the study objective.Inference step: BF_TM_Add (‘no’, so-text IS NAME OF Study Objective
with_exclusion Treatment Method WITH TM-name)Explanation: This step generates the exclusion treatment methods that are directly
connected to the study objective and creates selection criteria of thesetreatment methods.
Step 1.5: Variables that are connected to the study objective
Uses: Text of the study objective so-text.Creates: Selection criteria which are based on variables connected to the study
objective.Inference step: BF_VAR_Add (Class, L-Class, so-text IS NAME OF Study Objective
applying_to Variable having_value Value being_value_of WITHVAR-name)
Explanation: This step generates the variables that are connected to the studyobjective and are connected to a value. These variables lead to selectioncriteria of several selection criteria. Class and L-class are thecorresponding classes of criteria in which a certain criteria belongs.
2.4.3 Step 2: Developing criteria based on inference steps
In this section criteria will be developed based on inference steps. These inference steps canalso be combined to a more powerful inference step. The inference mechanism will try to inferas much as possible and thus combining inference steps to develop more criteria. The numberof inference steps seems little, but this is deliberately done due to the fact that there would be tomany selection criteria and overlap between criteria. Also this thesis is only a support to thedeveloper of selection criteria, and should thus be easy to read and try to create a set ofminimally restrictive selection criteria, so thus will enable the user to stricten the set ofselection criteria.
Also the inference mechanism will try to avoid recursivity as much as possible due to the factthat recursivity could lead to too many selection criteria. For example, if the patient may not behypersensitive against material A and Material A is part of Material B and Material C, thefollowing criteria could be added:
• Patient should not be hypersensitive against A.• Patient should not be hypersensitive against B.• Patient should not be hypersensitive against C.
This example shows that there are developed three criteria that are based on one point ofinterest and should actually be defined by one criterion. So the inference mechanism should bevery careful when using recursivity.

Patient Selection in Clinical Trials UIC/BME research center
53
Step 2.1: A treatment method which is excluded by another treatment method
Uses: Treatment method that is investigated in the clinical trial.Creates: Retrieves treatments that are excluded by treatments used in the clinical
trial directly or indirectly.Inference step: treatment IS NAME OF Treatment Method with_exclusion Treatment
Method WITH)Explanation: When the treatment method that is investigated in the clinical trial
excludes several other treatment methods, these treatment methodsshould lead to Disease Characteristics criteria. This investigatedtreatment can also be a treatment that was retrieved by an earlier stepof the inference mechanism.
Step 2.2: A state which is excluded by a treatment method
Uses: Treatment method that is investigated in the clinical trial.Creates: Retrieves states that are excluded by treatments used in the clinical trial
directly or indirectlyInference step: treatment IS NAME OF Treatment Method with_exclusion State
WITHExplanation: When the treatment method that is investigated in the clinical trial
excludes several states, these states should lead to DiseaseCharacteristics criteria. This investigated treatment can also be atreatment that was retrieved by an earlier step of the inferencemechanism.
Step 2.3: A state defined by another state
Uses: State or Excluded state that is investigated in the clinical trial.Creates: Retrieves states or exclusion states defined by another state or
exclusion state.Inference step: state IS NAME OF State being_defined_by State WITHExplanation: When the treatment method that is investigated in the clinical trial
excludes a state and this state is defined by another state, both thesestates should lead Disease Characteristics criteria. This state orexcluded state can also be retrieved by an earlier step of the inferencemechanism.
Step 2.4: A treatment method that uses materials
Uses: Treatments under investigation.Creates: Patient Characteristics criteria based on materials.Inference step: BF_MA_Add (‘no’, treatment IS NAME OF Treatment Method uses
Material WITHExplanation: When the treatment method that is investigated in the clinical trial uses
materials, Patient Characteristics criteria should be defined to ensurethat a patient is not hypersensitive against these materials. Thesetreatments can also be retrieved by an earlier step of the inferencemechanism.
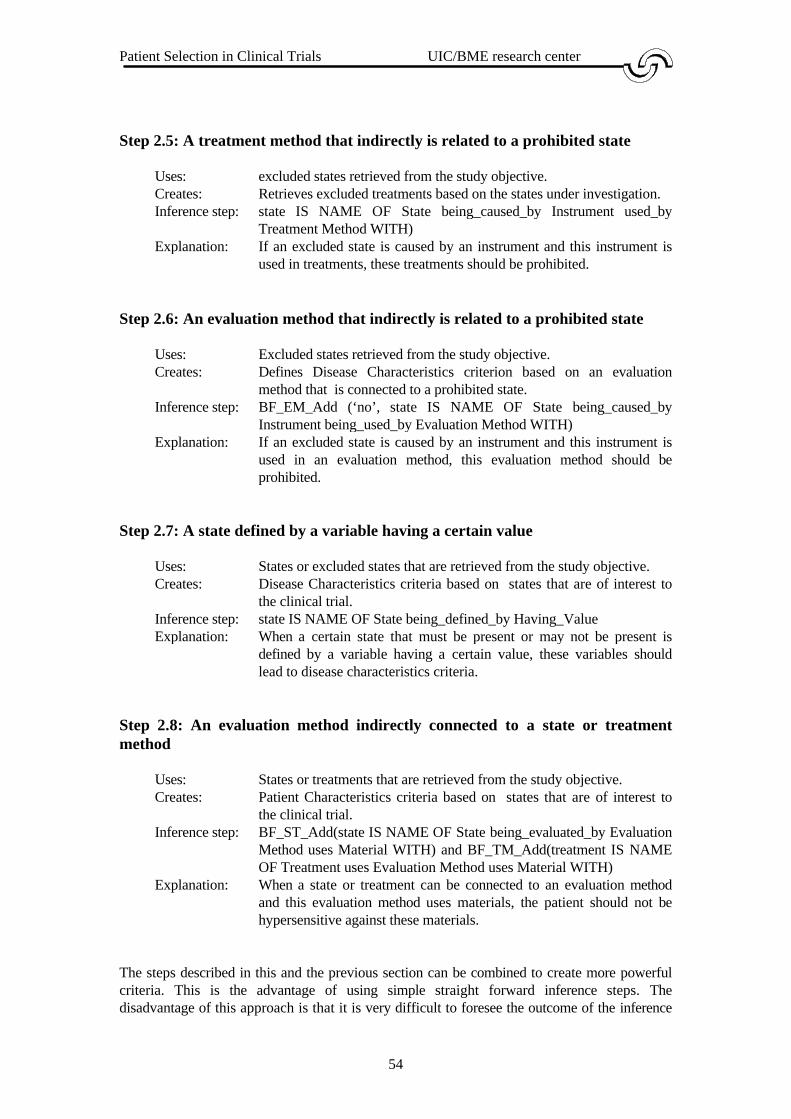
Patient Selection in Clinical Trials UIC/BME research center
54
Step 2.5: A treatment method that indirectly is related to a prohibited state
Uses: excluded states retrieved from the study objective.Creates: Retrieves excluded treatments based on the states under investigation.Inference step: state IS NAME OF State being_caused_by Instrument used_by
Treatment Method WITH)Explanation: If an excluded state is caused by an instrument and this instrument is
used in treatments, these treatments should be prohibited.
Step 2.6: An evaluation method that indirectly is related to a prohibited state
Uses: Excluded states retrieved from the study objective.Creates: Defines Disease Characteristics criterion based on an evaluation
method that is connected to a prohibited state.Inference step: BF_EM_Add (‘no’, state IS NAME OF State being_caused_by
Instrument being_used_by Evaluation Method WITH)Explanation: If an excluded state is caused by an instrument and this instrument is
used in an evaluation method, this evaluation method should beprohibited.
Step 2.7: A state defined by a variable having a certain value
Uses: States or excluded states that are retrieved from the study objective.Creates: Disease Characteristics criteria based on states that are of interest to
the clinical trial.Inference step: state IS NAME OF State being_defined_by Having_ValueExplanation: When a certain state that must be present or may not be present is
defined by a variable having a certain value, these variables shouldlead to disease characteristics criteria.
Step 2.8: An evaluation method indirectly connected to a state or treatmentmethod
Uses: States or treatments that are retrieved from the study objective.Creates: Patient Characteristics criteria based on states that are of interest to
the clinical trial.Inference step: BF_ST_Add(state IS NAME OF State being_evaluated_by Evaluation
Method uses Material WITH) and BF_TM_Add(treatment IS NAMEOF Treatment uses Evaluation Method uses Material WITH)
Explanation: When a state or treatment can be connected to an evaluation methodand this evaluation method uses materials, the patient should not behypersensitive against these materials.
The steps described in this and the previous section can be combined to create more powerfulcriteria. This is the advantage of using simple straight forward inference steps. Thedisadvantage of this approach is that it is very difficult to foresee the outcome of the inference

Patient Selection in Clinical Trials UIC/BME research center
55
mechanism also certain criteria can be developed in multiple ways. Although the user sees onlythe first occurrence of this criterion, it increases the time needed to develop selection criteria.
The inference mechanism will will until it rans out of input. This could be described in thefollowing statement:
while new knowledge found in previous loop dobegin
generate criteria based on step 1;retreive knowledge and generate criteria base on step 2;
end
A simple example of the inference mechanism could for example be:
Knowledge:
• State st1 is subject of Study Objective so1.• State st1 is defined by State st2.
This knowledge will be used to create criteria as follows:
First run:• Step 1.1: State st1 leads to criterion Patient should have st1.• Step 2.3: The mechanism finds the rule State st1 is defined by State st2. Now st2 is
added to the list of states that should lead to criteria. If st1 was an excluded state, thenst2 is also an excluded state.
• All knowledge is processed and some new knowledge is found, so the mechanismcontinues with the second run.
Second run:• Step 1.1: State st2 leads to criterion Patient should have st2.• No new knowledge is found so the inference mechanism will exit.
The inference mechanism processes all the other steps in a similar way, except for step 2.4 and2.6. These steps produce knowledge that cannot be directly connected to the study objective, sothese steps will generate criteria directly without interference of step 1.
2.4.4 Step 3: Trying to guarantee completeness of selection criteria
It is very difficult to guarantee completeness of selection criteria, but to make sure that certainimportant selection criteria are defined, these criteria will be used as default criteria, e.g. ifthese criteria are not already defined, they will be defined by this step.
Step 3.1: A performance status criterion should always be defined
Uses: Safety criteria based on the study objective.Creates: Safety criterion based on a performance status if this criterion is not
Patient Selection in Clinical Trials UIC/BME research center
56
already defined.Inference step: BF_VAR_Add (Safety Criteria, SF-name, ‘performance status’ IS
NAME OF Variable)Explanation: A performance status that states that the patient’s status of life is
sufficient is very important when including a patient in a clinical trial.
Step 3.2: An age criterion should always be defined
Uses: Environment Criteria based on the study objective.Creates: Environment Criterion that guarantees an explicit definition of an age
criterion.Inference step: BF_VAR_Add (Environment Criteria, EC-name, ‘age’ IS NAME OF
Variable)Explanation: Age is an important factor is accepting a clinical trial, thus an age
criterion has to be defined. In most trials, an age criterion is notdefined. In this case it is assumed that only adults will be included in aclinical trial. Testing on children is normally prohibited except whenthere is a good reason to test a medication on children.
Step 3.3: An informed consent criterion should always be defined
Uses: Environment criteria based on the study objective.Creates: Environment criterion that ensures that the patient has given his or her
approval.Inference step: BF_VAR_Add (Environment Criteria, EC-name, ‘informed consent’ IS
NAME OF Variable )Explanation: An informed consent is necessary to point out the risqué’s to the patient
and to get is approval. In this way the patient is not able to start alawsuit when a treatment has unknown side-effects.
Step 3.4: Pregnant or lactating women should always be excluded from the trialunless specified otherwise
Uses: Patient characteristics based on the study objective.Creates: Patient characteristics criterion which ensures that pregnant or
lactating are not participating in the trial except when explicitly definedotherwise.
Inference step: BF_VAR_Add (Patient Characteristics, PC-name, ‘pregnant orlactating’ IS NAME OF Variable)
Explanation: When the treatment method that is investigated in the clinical trial usesmaterials. Baby’s are always extremely sensitive, and testing atreatment on pregnant or lactating women could jeopardise a baby’shealth.
Step 3.5: A life expectancy criterion should always be defined
Uses: Patient characteristics based on the study objective.Creates: A patient characteristics criterion specifying that the patient lives at

Patient Selection in Clinical Trials UIC/BME research center
57
least as long to complete the trial.Inference step: BF_VAR_Add (Patient Characteristics, PC-name, ‘life expectancy’ IS
NAME OF Variable)Explanation: When it is likely that a patient dies before the ending of a study, not
only the testing on the patient was incomplete and partially unusable,but it also influences the outcome of the trial in a negative way.Therefore the patient should live a least as long to survive the trial.
Step 3.6: Patients with chronic manic depressions should always be excludedfrom the trial unless specified otherwise
Uses: Safety criteria based on the study objective.Creates: Safety criteria that ensures that patients suffering from chronic manic
depressions are not participating in the study unless specifiedexplicitly.
Inference step: BF_VAR_Add (Safety Criteria, SF-name, ‘chronic manic depressions’IS NAME OF Variable)
Explanation: A patient’s state of mind can influence the working of a treatment,therefore patient’s suffering from a chronic manic depression areprohibited from participating in the clinical trial, except when explicitlydefined otherwise,
These six criteria should ensure that certain criteria that are mostly implicitly defined should bepart of the set of selection criteria that is created. This third step has to be made to ensure thatseveral important criteria are always defined.
2.5 Summary
In this chapter the knowledge base is created for the development of selection criteria. Thisknowledge base has the capability to store all kinds of medical knowledge and to store theknowledge that is defined by the study objective. According to this study objective, selectioncriteria are developed by the inference mechanism.
This inference mechanism consists of three major steps. The first step is simple, but will beused more often than would be expected. Due to the fact that the inference mechanism retrievesknowledge recursively, these steps will be executed more than once. This step will definitelyend sometime. Due to the fact that there are only a limited number of concepts, the inferencemechanism will eventually run out of input.
This inference mechanism could be improved by defining more relations and medicalknowledge such as side-effects and probability functions. This would require a major adaptionto the knowledge base and will maybe be an option for the future.

Patient Selection in Clinical Trials UIC/BME research center
58
3 SCDS: a system for developing selection criteria
In this chapter the knowledge base and inference mechanism developed in chapter 2 will beevaluated by developing a prototype for the support of the development of selection criteria.This program is called SCDS (Selection Criteria Development System). This program is astand-alone version of a system for the support of the development of selection criteria, butwith minor adaptions can also be used as the PROSYS-part for subject selection. Thisprototype can also be used to build a knowledge base of medical knowledge.
3.1 Database design
The database model was developed using the modelling method PSM. The decision was madeto translate this model directly to a database model. Decisions had to be made:
Keys:
In PSM abstract keys are defined as st1. This is not possible in a database, so this key hasbeen transformed in the following foreign key:
(Concept Type Concept Index)
For example, st1 would be defined as (‘ST’,1).
Database naming:
When developing the knowledge model, concept classes and relation classes were defined.Several fact-types belong to the same relation class. For example, the fact-types ISO1,ISO2, ISO3 and ISO4 belong to the relation class ISO. Each concept class results in aseparate database. For each concept class there is also a separate database.
PSM makes use of generalisation. To deal with this generalisation, a field is added to thesuper-class which states the sub-class to which a concept belongs to.
Constraints:
PSM makes use of constraints to define certain restrictions to the study population. In adatabase model this is very hard. The decision has been made to implement these constraintsin the procedures for adding to the knowledge base.
These were the exeptions that were used to design the databases for SCDS. In the followingsection, some decisions of programming will be pointed out and after this the program will beevaluated by using the initial population presented in Appendix F.
3.2 The inference mechanism

Patient Selection in Clinical Trials UIC/BME research center
59
The inference mechanism will be implemented as defined in the previous section. To providethe inference mechanism to detect if a certain concept was already used, the inferencemechanism will use buffers. For each point of interest the inference mechanism will use twobuffers:
• Knowledge buffer: This buffer holds the knowledge that should be used in theinference mechanism.
• Used knowledge buffer: This buffer hold the knowledge that is already used by theinference mechanism and should not be used again.
The initial knowledge for the knowledge buffers is the knowledge that is directly connected tothe study objective. The result of the inference mechanism is a set of criteria that can bealtered by the user. Also there is an explanation facility available that lists the inference stepsused to create the selected selection criterion.
The inference mechanism is defined in LISA-D queries. These defined inference steps have tobe translated to the programming language used to write the prototype. The inference steps aretranslated into procedures These LISA-D terms have been translated into procedures. Theprototype contains documentation on how the LISA-D queries are translated into procedures.
The output of the inference mechanism is a set of selection criteria. This set is connected to thestudy objective and stored in the database model. After building this prototype, it can be tested.Testing the inference mechanism will show if the defined inference steps have the desiredoutput. An acceptance test of the prototype will be held to see if it is clear that the prototypecan be used as a stand-alone program for the development of selection criteria. After this, theprototype can be used for the support of the development of selection criteria and with minorchanges it can be integrated into PROSYS to serve as the PROSYS-part for supporting thedevelopment of selection criteria.
3.3 Evaluation
As explained in Appendix E there has been defined an initial population. The study objectivethat is used in this evaluation is the following:
To evaluate the quality of life of patients born in 1981and suffering from Renal CellCarcinoma (not Metastatic Renal Cell Carcinoma), who have been treated withChemotherapy.
From this study objective the following points of interest can be conducted:Treatment: ChemotherapyState: Renal Cell CarcinomaExcluded State: Metastatic Renal Cell CarcinomaRestrictions: Date of birth ≥ 1-1-81
Date of birth ≤ 31-12-81
The inference mechanism will make use of the relations defined in the knowledge base and willalso make use of relations that are already defined in another knowledge base. These relationsare:

Patient Selection in Clinical Trials UIC/BME research center
60
State ‘Fever’ caused by Instrument ‘X-ray instrument’State ‘Fever’ caused by Instrument ‘PSA-meter’Treatment ‘Radiotherapy’ uses Instrument ‘PSA-meter’State ‘Fever’ defined by State ‘Shivvering’State ‘Fever’ defined by Restriction (‘Body temperature’,’>‘,’37’)Evaluation Method ‘X-rays’ uses Instrument ‘X-ray instrument’Evaluation Method ‘X-rays’ uses Material ‘Radioactive fluid’
Now the inference mechanism will be used and according to the inference steps defined in theprevious chapter. The following set of criteria is generated by the inference mechanism:
‘Patient should have Renal Cell Carcinoma’ step 1.1‘Patient should have no Metastatic Renal Cell Carcinoma step 1.2‘Patient should have been treated with Chemotherapy’ step 1.3‘Patient should not have been treated with Radiotherapy’ steps 2.5, 1.4 or
steps 2.2, 1.4‘Patient should have no Fever’ steps 2.1, 1.3‘Patient should not be hypersensitive against GCSI’ step 2.4‘Patient should not be hypersensitive against M_VAC’ step 2.4‘Patient should not have been evaluated with X-rays’ step 2.6‘Patient should have no shivvering’ steps 2.3, 1.1‘Patient should not have Body temperature > 37’ steps 2.1, 2.7, 1.5‘Date of birth >= 1-1-81’ step 1.5‘Date of birth <= 31-12-81’ step 1.5‘Patient should not be hypersensitive against Radio active fluid’ step 2.8
Steps 3.1 to 3.6 have not been taken into account this step, because these steps are merely tosafeguard a complete set of selection criteria instead of really generating criteria. These criteriathat were created are the criteria that also were defined on paper. Testing with otherpopulations give also the expected criteria, so it is sound to assume that the prototype workscorrectly.
This example is only a small one, but with this small example
3.4 Acceptance test
The prototype is tested by the UIC/BME and seems to have the desired output. The prototypeprovides several functions such as:
• Defining a study objective and the points of interest• Defining a knowledge base on medical knowledge consisting of relations between
concepts• Loading and storing the developed study objective and set of selection criteria• Generating criteria• Altering criteria• Printing the developed set of selection criteria• On line help which provides the user with a simple help on almost every topic

Patient Selection in Clinical Trials UIC/BME research center
61
The UIC/BME has used the prototype and has stated that the prototype is easy to use and withminor changes can be integrated with PROSYS. The program seems to do what it is intendedto, so the UIC/BME has accepted the prototype as a prototype for supporting the developmentof selection criteria.
3.5 Summary
In this chapter an overview is given of SCDS, the prototype for supporting the development ofselection criteria. This overview consists of a database definition, a description of the inferencemechanism, an evaluation of the prototype and an acceptance test.
With the tested study objective, SCDS generated the expected criteria and one could assumethat the inference mechanism is implemented correctly and SCDS can be used to support thedevelopment of selection criteria. Also it has proven that a complex medical task can bespeeded up and improved by buidling a support system for the medical expert.

Patient Selection in Clinical Trials UIC/BME research center
62
4 Discussion and Conclusion
In this thesis an attempt has been made to develop an inference mechanism for the developmentof selection criteria for urological use. An existing model for storing medical knowledge hasbeen adapted to support the development of these selection criteria.
In chapter 2 this extended model has been presented and an inference mechanism wasdeveloped to generate selection criteria for a specified study objective. This inferencemechanism consists of three major steps in which the criteria have been developed. These stepscontain simple sub-steps, but due to the use of recursion there has been created a powerfulinference mechanism with several advantages en disadvantages. The advantages are that itconsist of simple steps, it is easily maintainable and can make use of a wide range of medicalknowledge.
The disadvantages are that due to the simple steps, criteria can be developed in different waysand this slows down the generation process. Also it is very hard to foresee the outcomes of ageneration process. Especially when there is a lot of knowledge base there could be developed alot of selection criteria.
In chapter 3 a prototype for the development of selection criteria was introduced, called SCDS.This prototype evaluates the inference mechanism. Due to the use of PSM and LISA-D theknowledge base and the inference mechanism could almost be directly translated into a workingmodel.
This prototype proves that it is possible to support the development of selection criteria bymaking use of a computer. Not only does this support speed up the time needed to develop suchcriteria, but it is also clear why certain criteria should be defined. So by making use of such asupport system, one is able to record experience from a medical expert who develops selectioncriteria. Interaction with a medical expert will always be needed, but this medical expert couldreally benefit from such a prototype.
It is my opinion that the knowledge base and the inference mechanism could be adapted tocreate an inference mechanism that creates a stricter set of selection criteria and also could beused to derive other knowledge like side-effects of a treatment. To stricten the set of developedselection criteria one should have more medical background to have a deeper insight in thedevelopment of selection criteria.
This inference mechanism combined with the inference mechanism of PROSYS could create asystem that is unique in urological medical science. PROSYS has proven that the time neededto complete difficult medical tasks can be reduced by making use of a support system. Not onlydoes this speed up the time needed for the development of a clinical trial, but is also does somestandardisation in creating a clinical trial and thus improves the quality of first draft clinicaltrial protocols.
Further research should be done to investigate if more similar tasks could be speeded up byusing an inference mechanism and also to investigate if this system could be ported to othermedical departments.

Patient Selection in Clinical Trials UIC/BME research center
63

Patient Selection in Clinical Trials UIC/BME research center
64
Appendix A: PSM
The Predicate Set Model (PSM) is developed at the University of Nijmegen. It is an extensionto the well-known NIAM model and has several new features like schema-types, specialisation,generalisation, sequence type and several constraints. In this appendix a short overview of PSMis given. For a more detailed description see [Hofstede 1994].
In relation two the ontology a concept class is represented by an object-type and a relation classis represented by a fact-type.
A An entity type A representing a class of abstract objects
A(L)
An entity type A and corresponding label type L, representing aclass of concrete objects. There is also an one-to-onerelationship between A and (L). This notation is an abbrovationfor the relation ship between A and (L).
A fact type f representing a relationship consisting of two roles,p and q, each connected to an object type
Two object types, where object type A inherits the properties ofobject type B (generalisation) and instances of B areautomatically instances of A
f qp
B A
A (L)f qp
A fact type f with a uniqueness constraint, showing that itconcerns a one-to-many relationship
B A
A fact type f with a uniqueness constraint, showing that itconcerns a many-to-many relationship
f qp
f qp
Two object types, where object type B inherits the properties ofobject type A (specialisation) and instances of B areautomatically instances of A

Patient Selection in Clinical Trials UIC/BME research center
65
A(L)
f qp A fact type f with a total role constraint, showing that eachinstance of object type A must take part in fact type f
A(L)
f qp
gsr
A fact type f with a total role constraint, showing that eachinstance of object type A must take part in fact type f or facttype g (inclusive or)
B(L)
A
C(M)
Object type A inherits the properties of object type B and objecttype C (multiple inheritance) and instances of B and C areautomatically instances of A, whereas instances of B can notbe instances of C (disjunct)
AAn instance of object type B consist of a (non empty) set ofinstances of object type A.
B
PSM without graphical constraints is called an information structure. This informationstructure can be formally represented using the following basic components [Hofstede 1994]:
• A nonempty finite set �� of object types. �
= £ ∪∪ εε ∪∪ �
.• A set £ of label types. Label types are also object types: £ ⊆⊆ �� .• A set εε of entity types Entity types are also object types: εε ⊆⊆ �� .• A set
� of fact types. Fact types are also object types:
� ⊆⊆ �� .
• A set �
of power types. Power types are also object types: �
⊆⊆ �� .
In an information structure £, εε and �
do not share elements: £ ∩∩ εε ∩∩ �
∩∩ �
= ∅∅.
Patient Selection in Clinical Trials UIC/BME research center
66
Appendix B: Basic ontology for a clinical trial
In the modelling scheme each object type is member of a certain concept class and each facttype is member of a certain relation class. For the basic ontology as been developed by[d’Hollosy 1996] there are 7 concept classes and 9 relation classes. A short and informaldescription of these classes is given below:
There are 7 concept classes and are defined as follows:
Concept class: Anatomical Referent (AR)Description: An organism or a concrete or abstract part of an organism.Examples: human being, hand, palm of the hand.
Concept class: Material (MA)Description: There are two kinds of material; Inorganic Material (IMA) and
Organic Material (OMA).Examples: liquid (IMA) , gas (IMA), blood (OMA), skin (OMA).
Concept class: Variable (VAR)Description: A characteristic of a concept that can appear as a study variable in a
clinical trial.Examples: body temperature, name, drug dose.
Concept class: State (ST)Description: The situation in which an anatomical referent can be found at a certain
moment. A state is present or not present.Examples: dead, fever, happy.
Concept class: Treatment Method (TM)Description: A method aimed to change the state in which an anatomical referent is
found.Examples: surgery, therapy.
Concept class: Evaluation Method (EM)Description: A method to calculate variable values or the presence of a state.Examples: method to measure blood pressure of fever.
Concept class: Instrument (IN)Description: A tool that is used to perform the evaluation method or a treatment.Examples: X-ray machine, needles, thermometer.
In the previous paragraph the concept classes were defined and explained. In this paragraph therelation classes between these concept classes will be stated. A relation is a function betweentwo concept classes to establish a link between two concepts. A description of these 9 relationclasses is given below:
Relation class: is kind of (KO)Relations:
Anatomical Region being kind ofAnatomical Region
e.g., Anatomical Region ‘stomach’ being kind ofAnatomical Region ‘digestive organ’.

Patient Selection in Clinical Trials UIC/BME research center
67
Material being kind of Material e.g., Material ‘urine’ being kind of Material’excretion product’.
Treatment Method being kind ofTreatment Method
e.g., Treatment Method ‘massage’ being kind ofTreatment Method ‘physiotherapy’.
Evaluation Method being kind ofEvaluation Method
e.g., Evaluation Method ‘gastroscopy’ being kindof Evaluation Method ‘endoscopy’.
Instrument being kind ofInstrument
e.g., Instrument ‘Celsius thermometer’ beingkind of Instrument ‘thermometer’.
Variable being kind of Variable e.g., Variable ’patients name’ being kind ofVariable ‘identification variable’.
State being kind of State e.g., State ‘broken leg’ being kind State ‘bonefracture’.
Relation class: is part of (PO)Relations:
Anatomical Region being part ofAnatomical Region
e.g., Anatomical Region ‘arm’ being part ofAnatomical Region ‘human body’.
Material being part of Material e.g., Material ‘salt’ being part of Material‘urine’.
Anatomical Region being part ofMaterial
e.g., Anatomical Region ‘ephiteel cell’ being partof Material ‘epitheel tissue’.
Treatment Method being part ofTreatment Method
e.g., Treatment Method ‘stitching’ being part ofTreatment Method ‘surgery’.
Evaluation Method being part ofEvaluation Method
e.g., Evaluation Method ‘Measuring weight’being part of Evaluation Method ‘physicalexamination’.
Relation class: has a function towards (HFT)Relations:
Anatomical Region havingfunction towards Material
e.g., Anatomical Region ‘bladder’ havingfunction towards Material ‘urine’.
Anatomical Region havingfunction towards AnatomicalRegion
e.g., Anatomical Region ‘brain’ having functiontowards Anatomical Region ‘nervesystem’.
Relation class: Uses (US)Relations:
Treatment Method usesInstrument
e.g., Treatment Method ‘surgery’ usesInstrument ‘surgical instruments’.
Evaluation Method usesInstrument
e.g., Evaluation Method ‘measuring bodytemperature’ uses Instrument ‘clinicalthermometer’.
Treatment Method uses Material e.g., Treatment Method ‘drug treatment’ usesMaterial ‘drug’.
Evaluation Method usesMaterial
e.g., Evaluation Method ‘urography’ usesMaterial ‘contrast liquid’.

Patient Selection in Clinical Trials UIC/BME research center
68
Relation class: (possible) Causes (CS)Relations:
Material (possible) causes State e.g., Material ‘paracetamol’ (possible) causesState ‘painless head’.
Treatment Method (possible)causes State
e.g., Treatment Method ‘massage’ (possible)causes State ‘painless muscles’.
Evaluation Method (possible)causes State
e.g., Evaluation Method ‘Urography’ (possible)causes State ‘shock’.
Instrument (possible) causesState
e.g., Instrument ‘needle’ (possible) causes State‘bruise’.
State causes (possible) State e.g., State ‘cancer’ (possible) causes State‘death’.
Relation class: is evaluated by (EB)Relations:
Variable being evaluated byEvaluation Method
e.g., Variable ‘length’ being evaluated byEvaluation Method ‘measuring’.
State being evaluated byEvaluation Method
e.g., State ‘bone fracture’ being evaluated byEvaluation method ‘x-ray scanning’.
Relation class: has variable (HV)Relations:
Anatomical Region havingvariable Variable
e.g., Anatomical Region ‘human body’ havingvariable Variable ‘body temperature’.
State having variable Variable e.g., State ‘fever’ having variable Variable ‘bodytemperature’.
Material having variableVariable
e.g., Material ‘fluid’ having variable Variable‘quantity’.
Relation class: can be found in state (FI)Relations:
Anatomical Region can be foundin State
e.g., Anatomical Region ‘ankle’ can be found inState ‘swollen’.
Material can be found in State e.g., Material ‘Water’ can be found in State‘frozen’.
Relation class: is defined by (DB)Relations:
State being defined by Variable e.g., State ‘fever’ being defined by Variable ‘bodytemperature’.
State being defined by State e.g., State ‘flu’ being defined by State ‘fever’.
Now there will be given a formal description of the information structure and of the relationclasses used in the ontology. For a brief description of the syntax used in the PSM-model andthe development of an information structure see Appendix A.
Patient Selection in Clinical Trials UIC/BME research center
69
Figure 8 shows the graphical representation of an information structure, that is defined by:
� = { Anatomical Referent, Material, Treatment Method, Evaluation Method,
Instrument, State, Variable, AR-name, TM-name, EM-name, IN-name, ST-name,VAR-name, KO1, KO2, KO3, KO4, KO5, KO6, KO7, PO1, PO2, PO3, PO4,PO5, CS1, CS2, CS3, CS4, CS5, CS5, EB1, EB2, HV1, HV2, HV3, FI1, FI2,DB1, DB2, HFT1, HFT2, US1, US2, US3, US4}
£ = { TM-name, EM-name, IN-name, ST-name, VAR-name}εε = { Anatomical Referent, Material, Treatment Method, Evaluation Method, State,
Instrument, Variable }�
= { KO1, KO2, KO3, KO4, KO5, KO6, KO7, PO1, PO2, PO3, PO4, PO5, CS1,CS2, CS3, CS4, CS5, CS5, EB1, EB2, HV1, HV2, HV3, FI1, FI2, DB1, DB2,HFT1, HFT2, US1, US2, US3, US4}
Now there will be given a formal description of the relation classes also called fact types.
is part of = { (x, y) | x, y ∈ ε }is kind of = { (x, y) | x, y ∈ ε }is evaluated by = { (x, y) | x ∈ ε, y ∈ Evaluation Method, x ≠ y}has variable = { (x, y) | x ∈ ε, y ∈ Variable, x ≠ y }can be found in state = { (x, y) | x ∈ ε, y ∈ State, x ≠ y }(possible) causes = { (x, y) | x ∈ ε, y ∈ State }is defined by = { (x, y) | x ∈ ε, y ∈ Variable ∪ State }has a function towards = { (x, y) | x, y ∈ ε }uses = { (x, y) | x ∈ ε, y ∈ Material ∪ Instrument }
This formal description of the relation classes will be used for the reasoning process. Thefollowing bridge-types12 are also implicitly defined in Figure 8:
• B-ST: Bridge between the concept class State and its label type ST-name.• B-TM: Bridge between the concept class Treatment Method and its label type TM-
name.• B-MA: Bridge between the concept class Material and its label type MA-name.• B-VAR: Bridge between the concept class Variable and its label type VAR-name.• B-AR: Bridge between the concept class Anatomical Referent and its label type AR-
name.• B-EM: Bridge between the concept class Evaluation Method and its label type EM-
name.• B-IN: Bridge between the concept class Instrument and its label type IN-name.
These bridge types are needed by the reasoning process to establish a link between a concretean abstract value.
12 See appendix A for more information on bridge-types.

Patient Selection in Clinical Trials UIC/BME research center
70
Appendix C: Performance status criteria
Grade 0: Able to carry out all normal activity without restriction.Grade 1: Restricted in physically strenuous activity but ambulatory and ably to carry
out light work.Grade 2: Ambulatory and capable of all self-care but unable to carry out any work; up
and about more than 50% of walking hours.Grade 3: Capable of only limited self-care, confined to bed or chair for more than 50%
of walking hours.Grade 4: Completely disabled; cannot carry out any self-care, totally confined to bed or
chair.
Table 4: ECOG performance status
100 % normal; no complaints90 % able to carry on normal activities; minor signs or symptoms of disease80 % normal activity with effort70 % cares for self; unable to carry on normal activity or to do active work60 % ambulatory; requires some assistance in activities of daily living and selfcare50 % requires considerable assistance of frequent medical care40 % disabled; requires special care and assistance30 % severe disabled; hospilazations indicated though death not imminent20 % very sick; hospilazations and active supportive treatment10 % moribund0 % dead
Table 5: Karnofsky performance status

Patient Selection in Clinical Trials UIC/BME research center
71

Patient Selection in Clinical Trials UIC/BME research center
72
Appendix D: Hydra
In PSM and LISA-D only static aspects can be represented. Task structures focus solely ondynamic aspects of a Universe of Discourse. Naturally, dynamic and static aspects of aUniverse of Discourse do not exist independently. The execution of tasks may lead topopulation changes. Task structures are used to model processes of data acquisition. In thisappendix, a transaction modelling technique called Hydra is defined in which interactionsbetween processes and data can be modelled. Hydra is based on task structures, LISA-D andPSM, and as such constitutes a complete information modelling technique. In this appendix ashort overview of Hydra is given. For a more detailed description see [Hofstede 1995].
Figure 14: Hydra syntax
M
Task A is part of Supertask M
Task A trigger Task B to perform someaction
M
A
Supertask M is divided in several tasks.The execution of supertask M starts withtask A.
ATransaction task named A
B
B i s a d a t a b a s e t h a t i s u s e d b y(transaction) tasks to add, alter or removedata to or from this database
A
A B
B A
Database B is input for Task A

Patient Selection in Clinical Trials UIC/BME research center
73

Patient Selection in Clinical Trials UIC/BME research center
74
Appendix E: LISA-D
Once an information structure has been developed in PSM, it can be described with LISA-D(Language for Information Structure and Access Descriptions) [Hofstede 1995-1, Hofstede1995-2]. LISA-D can be considered as a redesign of RIDL (Reference and IDea Language)[Troyer 1984], but exceeds the capabilities of RIDL by far. LISA-D can be used to expressqueries and constraints. The semantics of LISA-D are based on path expressions, which are anextension of relational algebra emphasising concatenations of relations. Sentences in LISA-Dare called information descriptors.
The basis for LISA-D information descriptors is names used in a PSM scheme, e.g., the namesof the object types, the names of the fact types, the names of the predicators, etc. This basis canbe used to build other information descriptors, e.g., is_born_in and State can becombined as the information descriptor is_born_in State and this can be expanded intoPresident is_born_in State. The corresponding PSM scheme is as follows:
For each PSM component special path expressions and LISA-D operators are defined. Theseare summed up in the following table:
President Stateborn_in being_
birthstate_of
Birthstate
LISA-D expression / path expression PSM componentX object type Xp predicator p
P← reverse of path expression Pf P isolation of the front element of path
expression PP � Q concatenation of Q to P, provided
there P is connected to QP ∪ Q union of P and QX p Y object types X and Y connected to
each other by means of a fact type inwhich p is a predicator
L IS-NAME-OF X label type L connected to object typeX by means of a bridge type
X IN Y element type X and power type Yconnected to each other by means of
fact type ∈x
X INVOLVED-IN f object type X participating in fact typef
X NOT INVOLVED-IN f object type X not participating in facttype f
f OF X fact type f in which object type Xparticipates

Patient Selection in Clinical Trials UIC/BME research center
75

Patient Selection in Clinical Trials UIC/BME research center
76
Appendix F: Initial population for the inference mechanism
In this appendix the initial population is created for the knowledge model shown in Figure 13.This results in the following population:
Pop(Study Objective) = so1
so2
Pop(SO-name’) = {‘To evaluate the quality of life and to evaluate theefficacy of patient's being treated with Interleukin-1compared to Interleukin-2 on females having age olderthan 18 and younger than 65, treated against Renalcell Carcinoma having no having systemic metastaticRenal Cell Carcinoma in a clinical trial Phase III .’,‘To evaluate the quality of life of patients born in1981 having Renal Cell Carcinoma (Not MetastaticRenal Cell Carcinoma) who have been treated withChemotherapy.’}
Pop(State) = st1
st2
st3
Pop(ST-name) = ‘Renal Cell Carcinoma’‘systemic metastatic Renal Cell Carcinoma’
‘Metastatic Renal Cell Carcinoma’
Pop(Treatment Method) = tm1
tm2
tm3
Pop(TM-name) = ‘Interleukin-1’‘Interleukin-2’
‘Chemotherapy’
Pop(Study Type) = stp1
Pop(STP-name) = ‘III’
Pop(Material) = ma1
ma2
ma3
ma4
Pop(MA-name) = ‘etiocholanolone’‘monocytes’
‘GCSI’‘M_VAC’

Patient Selection in Clinical Trials UIC/BME research center
77
Pop(Variable) = var1
var2
var3
var4
var5
Pop(VAR-name) = ‘quality of life’‘efficacy’‘gender’
‘age’‘Date of birth’
Pop(Value) = val1
val2
val3
val4
val5
Pop(Number) = val1
val2
Pop(Int) = ‘18’‘65’
Pop(Data-code) = val4
val5
Pop(Date) = ‘1-1-81’‘31-12-81’
Pop(Text) = val3
Pop(String) = ‘female’
Pop(Operator) = op1
op2
op3
Pop(OP-name) = <=>
Pop(Selection Criteria) = sc1
sc2
Pop(B-STP) = with_name being_name_ofstp1 ‘III’

Patient Selection in Clinical Trials UIC/BME research center
78
Pop(B-SO) = with_name being_name_ofso1 ‘To evaluate the quality of life and to
evaluate the efficacy of patients beingtreated with Interleukin-1 compared to
Interleukin-2 on females having ageolder than 18 and younger than 65,
treated against Renal cell Carcinomahaving no having systemic metastatic
Renal Cell Carcinoma in a clinical trialPhase III (SO1).’
so2 ‘To evaluate the quality of life ofpatients born in 1981 having Renal CellCarcinoma (Not Metastatic Renal CellCarcinoma) who have been treated with
Chemotherapy.’
Pop(B-ST) = with_name being_name_ofst1 ‘Renal Cell Carcinoma’st2 ‘systemic metastatic Renal Cell
Carcinoma’st3 ‘Metastatic Renal Cell Carcinoma’st4 ‘Fever’
Pop(B-TM) = with_name being_name_oftm1 ‘Interleukin-1’tm2 ‘Interleukin-2’tm3 ‘Chemotherapy’tm4 ‘Radiotherapy’
Pop(B-MA) = with_name being_name_ofma1 ‘etiocholanolone’ma2 ‘monocytes’ma3 ‘GCSI’ma4 ‘M_VAC’
Pop(B-VAR) = with_name being_name_ofvar1 ‘quality of life’var2 ‘efficacy’var3 ‘gender’var4 ‘age’var5 ‘Date of birth’
Pop(B-OP) = with_function being_function_ofop1 <op2 =op3 >
Pop(B-STRING) = with_name being_name_ofval3 ‘female’

Patient Selection in Clinical Trials UIC/BME research center
79
Pop(B-NR) = with_nr being_nr_ofval1 ‘18’val2 ‘65’
Pop(B-DATE) = with_date being_date_ofval4 ‘1-1-81’val5 ‘31-12-81’
Pop(INF) = being_influenced_by influencesso1 stp1
Pop(ISO1) = applying_to being_subject_ofso1 st1
so2 st1
Pop(ISO2) = applying_to being_subject_ofso1 tm1
so1 tm2
so2 tm3
Pop(ISO3) = applying_to being_subject_ofso1 var1
so1 var2
so1 var3
so1 var4
so2 var5
Pop(EX2) with_exclusion being_exclusion_ofso1 st2
so2 st3
Pop(EX3) with_exclusion being_exclusion_oftm3 tm4
Pop(EX4) with_exclusion being_exclusion_oftm3 st4
Pop(HVAL) = having_value being_operator_of being_value_ofvar3 op2 val3
var4 op1 val1
var4 op3 val2
var5 op1 val4
var5 op3 val5
Pop(US3) = uses being_used_bytm1 ma1
tm2 ma2
tm3 ma3
tm3 ma4

Patient Selection in Clinical Trials UIC/BME research center
80
This initial population will be used by the inference mechanism to develop selection criteria andthis population is intended to explain the generation process shown in chapter 3.

Patient Selection in Clinical Trials UIC/BME research center
81

Patient Selection in Clinical Trials UIC/BME research center
82
Glossary
Application Domain The universe of discourse where the knowledge has to beapplied.
Clinical Trial An experimental study on medical products in human subjectsto establish the efficacy and safety of these products byinvestigating their effects.
Clinical Trial Protocol A framework to conduct a clinical trial. The arguments, goalsand design of a clinical trial are presented in such a protocol.
Decision Support System An information system that is knowledge based and has aninference engine, but does not make decision but only gives arecommendation.
Hydra A transaction modelling technique, base on task structures.Inference Mechanism A set of rules that operates on knowledge and deducts new
knowledge from the knowledge base.Knowledge Base A database of facts called knowledge.Knowledge based model A model to define relations between facts, so that knowledge
can be stored in the model.Knowledge based system An information system that is based on knowledge, and creates
new knowledge by derivation.NIAM Natural language Information Analysing Method. A conceptual
modelling scheme.Ontology The structure of knowledge in a knowledge base.PROSYS PROtocol design SYStem. A knowledge-base system that
supports the development process of clinical trial protocols.PSM Predicate Set Model. A conceptual modelling scheme that is an
extension to NIAM. This scheme is developed at the Universityof Nijmegen. For more information see [Hofstede 1994].
Sample Size The number of patients that must complete a clinical trial.SCDS Selection Criteria Development System. The prototype to
evaluate the developed inference mechanism.Selection Criteria Also called inclusion and exclusion criteria, are rules that state
the demands the patients have to satisfy.UIC/BME The Urological Informatics Center/BioMedical Engineering
unit. This unit has developed PROSYS and this master scienceproject is

Patient Selection in Clinical Trials UIC/BME research center
83

Patient Selection in Clinical Trials UIC/BME research center
84
References
[Barreiro 1993] Barreiro, R .P Otero, R. Marin, J. Mira. A Modular Knowledge Basefor the Follow-Up of Clinical Protocols. Methods of Information inMedicine, Volume 32 pages 373-381, 1993.
[Brodie 1986] Michael L. Brodie, John Mylopoulos. Knowledge Bases andDatabases: Semantic vs. Computational Theories of Information. J.Clifford, New Directions for Database Systems, Chapter 13,Norwood, New Jersey, 1986.
[Clinical 1994] Clinical Epidemiology Unit. A Proposal for Structured Reporting ofRandomized Controlled Trials. JAMA, Volume 272 No. 24,Canada, 1994.
[Collins 1984] Joseph F. Collins. Planning patient recruitment; Fantasy andReality. Statistics in Medicine, Volume3, 435-443,1984.
[Culbert 28] Chris Culbert, Gary Riley, Robert T. Savely. An Expert SystemDevelopment Methodology that Supports Verification andValidation. ISA Transactions, Volume 28 No. 1.
[Dahl 1983] Veronica Dahl. Logic Programming as a Representation ofKnowledge. Simon Fraser University, Canada, 1983.
[Dassen 1991] Willem R. M. Dassen, Rob Mulleneers, Herman L. L. Frank. TheValue of an Expert System in Performing Clinical Drug Trials.Computed Biologic Medicine. Volume 21 No. 4 pages 193-198,1991.
[Debenham 1991] John Debenham. The Construction of Maintainable KnowledgeBases. The Next Generation of Information Systems; From Data toKnowledge, M. P. Popazoglou, Sydney, Australia, 1991.
[Dickersin 1990] Kay Dickersin, Karen Higgins, Curtis L. Meinert. Identification ofMeta-Analyses, the Need for Standard Terminology. ControlledClinical Trials, Volume 11 pages 52-66, 1990.
[Ellenberg 1995] Jonas H. Ellenberg. Clinical Trials. Clinical Neuropharmacology,Volume 8 No. 1, 1990.
[Falkenberg 1992] E. Falkenberg. Lecture notes Systems and Organizations. KatholiekeUniversiteit Nijmegen, 1992.
[Feigl 1995] Polly Feigl. Design of the Prostate Cancer Prevention Trial (PCPT).Controlled Clinical Trials Volume 16 pages 150-163, New York,1995.
[Franks 1988] Peter Franks, Clinical Trials. Family Medicine, Volume 20 No. 6,New York, 1988.

Patient Selection in Clinical Trials UIC/BME research center
85
[Friedman 1985] Friedman, Lawrence M. Fundamentals of clinical trials. 1985
[Gruber Http] Thomas R. Gruber. Ontolingua.http://ksl.stanford.edu/pub/knowledge/ontolingua /ontolingua.
[Gruber 1993-1] Thomas R. Gruber. A Translation Approach to Portable OntologySpecifications. 1993
[Gruber 1993-2] Thomas R. Gruber. Toward Principles for the Design of OntologiesUsed for Knowledge Sharing. Stanford Knowledge SystemsLaboratory, 1993.
[Hendriks 1994] P. Hendriks, D. Vriens, J. Benders. Reader Kennissystemen.Katholieke Universiteit Nijmegen, vakgroep Bedrijfswetenschappen,1994.
[Hofstede 1994] Arthur H.M. ter Hofstede. Dictaat IS1, Grondslagen vanInformatiesystemen 1. Katholieke Universiteit Nijmegen, vakgroepInformatica, 1994.
[Hofstede 1995] Arthur H.M. ter Hofstede. Dictaat IS2, Grondslagen vanInformatiesystemen 2. Katholieke Universiteit Nijmegen, vakgroepInformatica, 1995.
[d’Hollosy 1995] W. d’Hollosy. Protocol design System for Clinical Trials. UIC/BMEResearch Center AZN Nijmegen, 1995.
[d’Hollosy 1996] W. d’Hollosy. An Ontology to Conceptualize domain Knowledgeneeded to determine relevant Study Variables for new ClinicalTrials. Computers and Biomedical Research, 1996.
[Jeffcoat 1992] M. K. Jeffcoat. Principles and Pitfalls of Clinical Trials Design.Journal of Periodontal. Pages 1045-1051, 1992.
[Jorna 1992] R. J. Jorna, J. L. Simons. Kennis in Organisaties. 1992.
[Karp 1993] Peter D. Karp, Thomas Gruber, Fritz Mueller. A GenericKnowledge-Base Access Protocol. 1993.
[Koval 1987] J.J. Koval, L. M. Kwarciak, M. G. A. Grace, B. J. Lockwood. AComprehensive Database Management System for a Variety ofClinical Trials. Methods of Information in Medicine, Volume 26 No.1 pages 24-30, 1987.
[Lewis 1993] Roger J. Lewis. An Introduction to the Use of Interim Data Analysesin Clinical Trials. Annals of emergency medicine Volume 1469pages 129-135, Torrance, California, 1993.
[Ludwig 1990] Thomas Ludwig, Bernd Walter. Database Concepts for the Supportof Knowledge-Based Systems. Information Systems and ArtificialIntelligence, D. Karagounnon, Berlin, 1990.

Patient Selection in Clinical Trials UIC/BME research center
86
[Mars 1991] N. J. I. Mars. Inleiding Kennistechnologie. 1991.
[Malogolowkin 1989 Marcio H. Malogolowkin. Tracing Expert thinking in Clinical TrialDesign. Computers and Biomedical Research, Volume 22 pages 190-208, 1989
[Meinert 1986] Curtis L. Meinert. Clinical Trials; Design, Conduct and Analysis.1986
[Morrison 1991] L. M. Morrison, D. R. Small, E. S. Glen. Computer Applications ina Urology Department. British Journal of Urology, Volume 67 pages257-262, 1991.
[Peduzzi 1988] Peter Peduzzi. General Statistical Design Considerations ofRandomized Clinical Trials. Perspectives in Shock Research, pages61-70, 1988.
[Pocock 1983] Stuart J. Pocock. Clinical Trials. 1983.
[Prakken 1989] B. Prakken. Strategisch en Tactisch Informatiebeleid. 1989.
[Riegelman 1981] Richard K. Riegelman. Studying a Study and Testing a Test; How toread the Medical Literature. 1981.
[Rotmensz 1989] Nicole Rotmensz, Kris van Tongelen, Josette Renard. DataManagement and Clinical Trials. 1989.
[Seters 1993-1] Harrie van Seters. GIP1: Realisatie en Invoering. KatholiekeUniversiteit Nijmegen, vakgroep Informatica, 1993.
[Seters 1993-2] Harrie van Seters, Wil Lamain. GIP2: Ontwerp. KatholiekeUniversiteit Nijmegen, vakgroep Informatica, 1993.
[Seters 1994] Harrie van Seters, Wil Lamain, Tom van Weert. GIP4: Managementvan Analyse en Ontwerp. Katholieke Universiteit Nijmegen, vakgroepInformatica, 1994.
[Smith 1992] A. P. Smith. Design a Clinical Information System. BMJ, Volume305 pages 415-417, 1992.
[Spilker 1985] Bert Spilker. Guide to Clinical Studies and Development Protocols.1985.
[Sylvester 1995] Richard Sylvester. Almost everything that you wanted to know aboutthe Statistical Design and Analysis of Phase III Clinical Trials.EORTC Newsletter, Volume 11.1, 1995.
[Taylor 1990] D. W. Taylor, E. G. Bosch. CTS: A Clinical Trials Simulator.Statistics in Medicine, Volume 9 pages 787-801, 1990.
[Testa 1985] Marcia a. Testa, Donald C. Simonson. The Design and Structure ofClinical Research Information Systems. Journal of Medical Systems,

Patient Selection in Clinical Trials UIC/BME research center
87
Volume 9 No. 3, 1985.
[Troyer 1984] O.M.F. de Troyer, R. Meersman, F. Ponseart. RIDL userguide.International Centre for Information Analysis Services, Control DataBelgium. 1984.
[Tu 1993] S. W. Tu. A Methodology for Determing Patients’ Eligibility forClinical Trials. Methods of Information in Medicine, Volume 32pages 317-325, 1993.
[Tygstrup 1982] Niels Tygstrup, John M. Lachin, Erik Juhl. The Randomized ClinicalTrial and Therapeutic Decisions. 1982.
[Voynick 1988] Irene M. Voynick, Robert W. Makuch. The Design andImplementation of a Software System for Clinical Studies: AnIllustration Based on the Needs of a Comprehensive Cancer Centre.Journal of Medical Systems, Volume 12 No. 5, 1988.
[Webster 1983] Merriam-Webster Inc. Webster’s ninth new collegiate dictionary.1983
[Win 122] Werkgroep Immunotherapie Nederland (WIN). A Randomized PhaseIII Study with Adjuvant subcutaneous recombinant Interleukin-2versus no treatment in Patients with renal cell Carcinoma with noEvidence of disease after Tumornephrectomy andLymphadenectomy
[Wyatt 1991] Jeremy Wyatt. Computer-Based Knowledge Systems. The Lancet,Volume 338, 1991.

Patient Selection in Clinical Trials UIC/BME research center
88
Index
A
acceptance test ............................................60age ..............................................................17ambiguity ....................................................11application domain......................................23aspects
ethical ...............................................11; 13statistical..................................... 11; 13; 18
B
bridge type ..................................................45
C
classesconcept ...................................................26
clinicaltrial................................. 12; 15; 16; 18; 19trial protocol .....................................19; 21
clinical trial............................... 10; 11; 15; 16Phase I ....................................................10Phase II...................................................10Phase III ...........................................10; 16Phase IV .................................................11phases of .................................................10protocol................................. 10; 11; 12; 21protocol adaption ....................................19protocol design..................................10; 11
concept class .........................................26; 66concept classes ............................................24constraints....................................... 12; 17; 58criteria
classes of selection ..................................17disease characteristics .......................17; 36environment characteristics...............17; 39higly restricted selection..........................21inclusion/exclusion ......... 13; 14; 15; 16; 17minimally restricted selection..................21patient characteristics........................17; 34safety ................................................17; 41selection16; 17; 18; 19; 21; 23; 24; 26; 33; 43; 46
D
data.............................................................23database design ...........................................58decision support system...............................15design
statistical.................................................11drop-out rate ...............................................18
E
ECOG.........................................................70economy......................................................23efficacy..................................................10; 11efficiency.....................................................23
entity type................................................... 65entity types ................................................. 24error
type II..................................................... 10expressiveness ............................................ 23
F
fact type...........................................24; 64; 65flexibility .................................................... 23
G
generalisation ............................................. 64
H
Hydra ................................................... 22; 72
I
incoherence ................................................ 11incompleteness ........................................... 11inference mechanism .....22; 23; 43; 46; 48; 59information................................................. 23
block ................................................ 12; 13item........................................................ 12structure ........................................... 65; 68system .................................................... 12topic ....................................................... 13
informed consent .................................. 13; 18
K
Karnofsky................................................... 70knowledge ............................................ 15; 23
base .......................................12; 15; 22; 23based information system........................ 22based system..................................... 12; 21model ..................................................... 22representation......................................... 23
L
label type .................................................... 65life expectancy............................................ 16LISA-D ...................................................... 59
M
macro ......................................................... 48master science project ........................... 10; 15master thesis......................................... 21; 22master thesis definition............................... 15
N
NIAM......................................................... 64
O
object type .................................................. 65object-type .................................................. 64ontology...........................................23; 24; 26

Patient Selection in Clinical Trials UIC/BME research center
1
extended .................................................26
P
patientpopulation...............................................19recruitment .............................................17
patient recruitment .......................... 16; 18; 19performance
status ......................................................16pregnant or lactating women .......................17project definition .........................................15PROSYS ................................... 10; 12; 15; 22
-part..................................................12; 22protocol
design .....................................................12protocol design
guidelines ...............................................12protocol-part ...............................................11prototype .....................................................15PSM.............................. 24; 58; 64; 65; 68; 72
R
reasoning process ........................................15relation class .........................................31; 66relation classes ............................................24research objectives.................................12; 15
S
sample population....................................... 18sample size ......................................14; 18; 19SCDS ......................................................... 58specialisation .............................................. 64standarisation ............................................. 11study........................................................... 16
design............................................... 11; 13extension ................................................ 19objective ......................................11; 13; 16protocol adaption.................................... 19termination............................................. 19type ........................................................ 13
study objective ...........................13; 26; 31; 47study type ................................................... 26subject selection.................................... 11; 13
T
task............................................................. 72transaction.................................................. 72
U
UIC/BME ............................................. 12; 22uniformity................................................... 23