patient, provider, and system interventions to …acknowledgements –it took a village...
TRANSCRIPT
PATIENT, PROVIDER, AND SYSTEM
INTERVENTIONS TO PROMOTE EQUITY
AMONG VULNERABLE VETERAN
POPULATIONS
Society of Behavioral Medicine 37th Annual Meeting
Washington, DC
April 2, 2016
Leg0fenris. Oh brother where art thou. https://flic.kr/p/9wuc1h / CC BY-NC-ND 2.0

Peter Murphy. Me against myself.
https://flic.kr/p/9Q4xUk; CC BY-ND 2.0
Parker Knight. Long Beach VA Hospital.
https://flic.kr/p/7B5Cos; CC BY 2.0
Theodore Lee. War Veteran.
https://flic.kr/p/p3PPQc; CC BY-NC-ND 2.0
The U.S. Army. Virginia.
https://flic.kr/p/4v3Py2; CC BY 2.0.
Don DeBold. Vietnam Veteran’s Memorial.
https://flic.kr/p/cm6L8Y; CC BY-NC-ND.

JnL. Bike Wheel. https://flic.kr/p/4JKSG; CC BY-SA 2.0.
Male Gringo. Funky Spokes Bike Repair. https://flic.kr/p/7RkwC5; CC BY-NC 2.0.

EVALUATION OF A NETWORK-WIDE
EFFORT TO REDUCE RACIAL
DISPARITIES IN HYPERTENSION
Leslie R.M. Hausmann, PhD
Core Investigator, CHERP
VA Pittsburgh Healthcare System
Assistant Professor of Medicine
University of Pittsburgh

Disclosures/Funding
• The views expressed here are mine and do not represent
those of the Department of Veterans Affairs or the United
States Government.
• I have no financial conflicts to disclose.
• This work was undertaken as quality improvement
supported with funding from the VA Office of Health Equity
and VISN 4 (XVA 72-183; PI: Hausmann).
Acknowledgements – It took a village
• Operations, Clinical, and Research Partners:• VHA Office of Health Equity
• Veterans Integrated Service Network (VISN) 4
• VA Pittsburgh Healthcare System, Center for Health Equity Research
and Promotion (CHERP)
• Individuals:
Keri L. Rodriguez George Brown Christopher M. Mannozzi
Maria K. Mor Matthew J. Chinman Matthew F. Muldoon
Kelly H. Burkitt Charlene David Lisa Red
Walter J. Clark Beth Ann Gibson Genna Toth
David S. Macpherson Kenneth T. Jones Uchenna S. Uchendu
Michael J. Fine Judith Long

Goals for the Next 15 Minutes
• Review how this project came to be
• Summarize the evaluation aims and methods
• Report major qualitative and quantitative findings
• Share future recommendations

Veterans Integrated Service Network (VISN) 4

Project Origin
• VISN 4 included objectives to reduce disparities in
performance plan for Fiscal Year (FY) 2013
• Develop a VISN-wide Race Disparity Dashboard
• Use the Dashboard to identify opportunities for quality
improvement

VISN 4 Race Disparity Dashboard –
Initial Findings
Black-White Differences in 19 Primary Care Quality Measures as of April 20, 2013
VISN 4 Disparities Objectives for FY14
• Carry out a VISN-wide quality improvement effort to
reduce racial disparities in hypertension (HTN) control
• Specific target: Reduce the number black Veterans with
severe (i.e., Stage 2) HTN
• Why black Veterans?
• Target for HTN control (80% with BP<140/90) was met for
whites, but not blacks
• Why Stage 2 HTN (BP>160/100)?
• Greater risk for vascular morbidity

The VISN 4 Hypertension Racial
Disparities Project was Born
• VISN Project Lead appointed (based in Pittsburgh)
• Task: Coordinate efforts across VISN
• Facility Project Leads appointed at each VA Medical
Center (VAMC)
• Task: Oversee project activities at their VAMC and
Community Based Outpatient Clinics (CBOCs)

Step 1 – GAIR Analysis
• Identify factors underlying black-white HTN disparities at
each facility
• Providers not using current clinical GUIDELINES
• Lack of patient ADHERENCE to medication and lifestyle
modification
• Provider clinical INERTIA (a lack of urgency) in treating
patients with HTN
• Patient RESISTANCE to standard medication management
• Formulate local action plans based on GAIR analysis
Step 2 (and 3 and 4…) –
Implement Local Action Plans• VISN Project Lead served as a model and provided
support
• Facility Project Leads carried out local activities
• VISN provided tools to generate lists of patients with
Stage 2 HTN
• Lists could be sorted by race, last BP, provider, etc.
• VISN also distributed monthly progress reports

Evaluation Opportunity –
VISN 4 / CHERP / OHE Partnership
• CHERP partnered with VHA
Office of Health Equity
(OHE) and VISN 4 to
document the process and
impact of this network-wide
effort to reduce race
disparities in HTN

Evaluation Aims
• Describe HTN control intervention strategies implemented
and barriers to implementation
• Assess impact of intervention strategies on disparities in BP
control among black and white Veterans with HTN

Methods – Qualitative
• CHERP qualitative expert documented VISN and local
facility project-related calls
• Conducted semi-structured telephone interviews with
facility project leaders
• Coded meeting and interview notes for barriers and
strategies using modified grounded theory approach

Methods – Quantitative
• Used data abstracted from electronic medical records to
assess change in BP for black and white Veterans
• Used multi-level regression models to examine how
intervention strategies were related to changes in BP
disparities

Qualitative Findings, Part 1 –
Barriers to Implementation
• 19 different barriers identified
• Range=2-9, Median=4
• Fell into 4 categories (# facilities)
• Project implementation barriers (8)
• Patient-level barriers related to HTN management (6)
• Provider-level barriers related to HTN management (5)
• System-level barriers related to HTN management (6)

Qualitative Findings, Part 2 –
Strategies Used to Reduce Disparities
• 22 specific strategies identified
• Range=4-10, Median=6
• Fell into 7 broad categories (# facilities)
• Provider education (9)
• Use lists of patients with Stage 2 HTN (8)
• Patient outreach (5)
• Patient education about BP management (4)
• Increase uptake of existing services (3)
• Establish new type of HTN appointment (2)
• Modify Computerized Patient Record System to prompt
action (2)

Quantitative Findings –
Did BP Change?

Time Trends in Stage 2 HTN among
Black and White Veterans in VISN 4

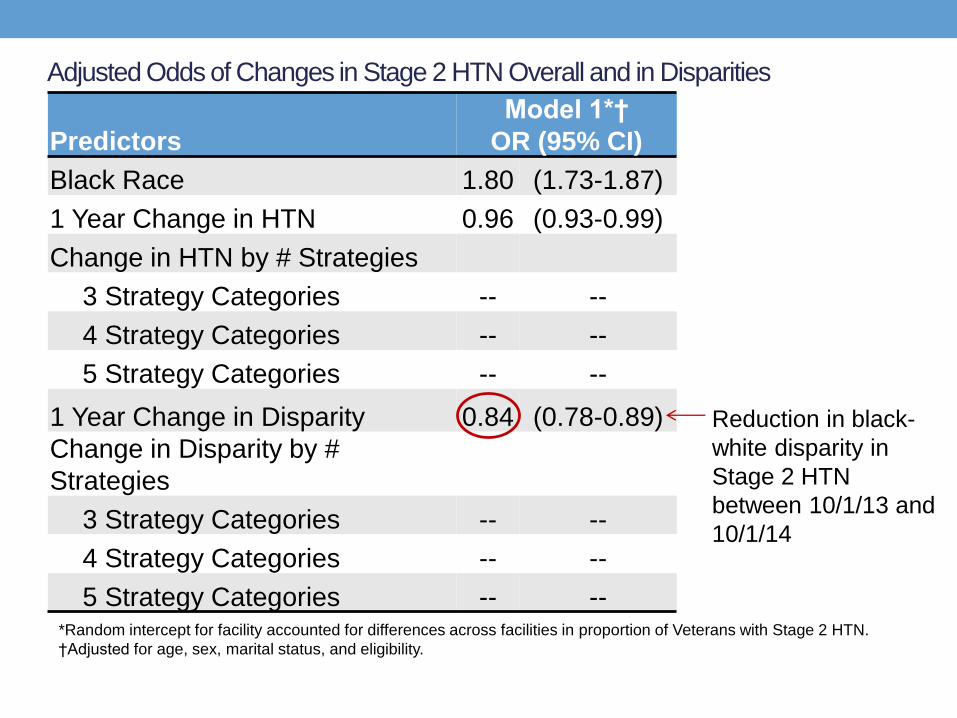
Adjusted Odds of Changes in Stage 2 HTN Overall and in Disparities
Predictors
Model 1*†
OR (95% CI)
Black Race 1.80 (1.73-1.87)
1 Year Change in HTN 0.96 (0.93-0.99)
Change in HTN by # Strategies
3 Strategy Categories -- --
4 Strategy Categories -- --
5 Strategy Categories -- --
1 Year Change in Disparity 0.84 (0.78-0.89)
Change in Disparity by #
Strategies
3 Strategy Categories -- --
4 Strategy Categories -- --
5 Strategy Categories -- --*Random intercept for facility accounted for differences across facilities in proportion of Veterans with Stage 2 HTN.
†Adjusted for age, sex, marital status, and eligibility.
Reduction in black-
white disparity in
Stage 2 HTN
between 10/1/13 and
10/1/14

Adjusted Odds of Change in Stage 2 HTN and Change in Disparities
Predictors
Model 1*†
OR (95% CI)
Model 2**†
OR (95% CI)
Black Race 1.80 (1.73-1.87) 1.81 (1.53-2.14)
1 Year Change in HTN 0.96 (0.93-0.99) -- --
Change in HTN by # Strategies
3 Strategy Categories -- -- 1.01 (0.96-1.07)
4 Strategy Categories -- -- 0.97 (0.93-1.01)
5 Strategy Categories -- -- 0.82 (0.76-0.89)
1 Year Change in Disparity 0.84 (0.78-0.89) -- --
Change in Disparity by #
Strategies
3 Strategy Categories -- -- 0.87 (0.79-0.95)
4 Strategy Categories -- -- 0.77 (0.70-0.85)
5 Strategy Categories -- -- 0.39 (0.27-0.56)*Random intercept for facility accounted for differences across facilities in proportion of Veterans with Stage 2 HTN.
**Facility-level random intercept for effect for Black race added to account for differences across facilities in proportion
of Black Veterans with Stage 2 HTN.
†Adjusted for age, sex, marital status, and eligibility.

Summary
• There were small VISN-wide reductions in the black-white
disparity in Stage 2 HTN over time.
• Facilities that used strategies from more intervention
categories showed significantly larger reductions in
disparities.

Future Recommendations
• Ensure that race, ethnicity, and other potential risk factors are
systematically recorded and made available.
• Include goals to reduce disparities in annual performance plans.
• Provide structure, leadership, and resources to support quality
improvement efforts that target disparities.
• Allow facilities to adopt action plans that fit their specific needs.
• Design performance metrics to ensure that they are acceptable
and interpretable to those who will be carrying out efforts.
• Incorporate a “formative evaluation” into project plans to identify
and address early implementation barriers.
