patient problems associated with immediate and delayed rehospitalization
TRANSCRIPT

PATIENT PROBLEMS ASSOCIATED WITH IMMEDIATE AND DELAYED
REHOSPITALIZATION
J e r o m e M. Siegel, Ph.D. Cather ine St. Clair, Ph.D.
Patients from two types of inpatient settings, a city hospital ward and a voluntary admissions ward in a nonprofit hospital, were interviewed after immediate (under 6 weeks) or delayed (over 6 months) rehospitalization. Anxiety and other signs of internal distress were the commonest causes of rehospitalization. Less often re- ported were problems associated with treatment or severe behavioral difficulties independent of psychosis. Chart review of these rehospitalized patients showed little recognition of their internal distress which deserved more therapeutic atten- tion in the effort to avoid rehospitalization. The early returnees presented a picture of discouragement rather than psychopathology per se, whereas hallucinations and medication problems were more often mentioned by late returnees.
Problems of anxiety and depression most frequently led to readmission to the small voluntary ward, in contrast t o the public acting-out behavior of early re- cidivists to the large city ward. Hallucinations were the major problem of both groups of late returnees, suggesting that both time OUt of hospital and ward admis- sion policies may be neglected reasons for rehospitalization. Delayed rehospitaliza- tion was not correlated with social competence.
This r epor t is in tended to serve two purposes: (1) to review the litera- ture on problems associated with recidivism in psychiatric patients, and (2) to describe a research study that examines the problems o f early re turnees (rehospitalization within 6 weeks o f discharge) and later re turnees (over 6 months in the communi ty pr ior to rehospitalization).
Rehospitalization is a cont inuing possibility for psychiatric patients who have requ i red inpat ient care. One- th i rd or more (some estimates ex- ceed 40%) o f a given cohor t o f inpatients will be readmi t ted within a year o f discharge, and in five years the n u m b e r may rise over two-thirds if the
Reprint requests should be sent to Dr. Jerome M. Siegel, Division of Research and Evalua- tion, Hahnemann Community Mental Health/Mental Retardation Center, 314 N. Broad St., Philadelphia, Pennsylvania, 19102.
The authors wish to express appreciation to Drs. P. Evans Adams and Arnold Goldman, and to Denise Ahman, James Concannon, Jane Gershaw, Michael Goldstein, John Plummer, Stephen Shelly, Stanley Silver, and Philip Weinberg.
204 PSYCHIATRIC QUARTERLY, VOL 49(3) 1977

205
J, M. SIEGEL AND C. ST.CLAIR
population is predominately schizophrenic (see Anthony et al. 2 and PauP 1 for two recent reviews of the recidivism literature).
Research determining which patients become recidivists has been ex- tensive in the past decade. Studies have investigated the relationship of rehospitalization to the patients' demographic and background variables, to symptoms and ward behavior, and to community adjustment. Social competence (particularly as indexed by marital status), and length of previ- ous hospitalization seem to be the two most effective predictors of re- cidivism. That is, patients who have never been married, and patients who have previously spent longer periods in the hospital, are most likely to return. Symptomatology and hospital behavior do not effectively predict subsequent need for rehospitatization. 4' 8 Patients who become isolates after release, adult patients living in parental homes, and patients whose behavior burdens those with whom they reside are more likely to become recidivists.5, 10 There has also been considerable debate as to whether or not patients seen in aftercare are more likely to avoid further rehospitaliza- tion.2,11,~
As well as "who" returns, the question of what specific problems bring patients back has also been explored.
PROBLEMS OF RETURNEES
Research on the problems that cause return to the hospital has been difficult to evaluate for the following reasons: (1) different studies have approached the problems of categorizing reasons for return in different fashions making comparison between studies difficult; (2) data gathering in the various studies has ranged from the one extreme of exclusive self- report by the patients through the middle ground of consensual agreement between the patient, his significant others, and professionals, to the other extreme of evaluation by professionals of the patients' problems that caused return; and (3) some of the studies employed control groups of nonreturning patients permitting some comparison of returnees and non- returnees while others did not.
Of the studies employing control groups of nonreturning patients, Miller 9 found that the returning patients, their significant others, and their social workers agreed partially that psychiatric symptoms were the most common reasons for return (patients = 21%, significant others = 36%, social workers = 40%). Also reported by the patients only was that they were tricked or victimized into returning (19%), that they had experienced family conflict (15%), and that they had suffered from physical illness (14%). Comparisons of the returning patients with their nonreturning con- trols with regard to behavior on leave preceding release, indicated that even- tual returnees were more likely than nonreturnees to behave bizarrely.
Zolik, Levin, and Hubek 19 had social workers rate both returning and nonreturning patients on a large number of items which, though not prob- lems per se, permitted some translation into a problem-oriented

206
PATIENT PROBLEMS
framework. Comparison of returnees with nonreturnees revealed, among other differences, that the returnees were more likely to have problems with medication than nonreturnees. The returnee was also described as being more likely to have trouble getting along with his family.
From interviews with chronic state hospital patients, Sanders, Smith, and Weinmann 15 reported that bizarre behavior was a critical factor in the return of 41% of the patients. An additional 21% were self-referred after feeling either physically or mentally ill. Other critical factors included poor judgment in the handling of everyday affairs (9%), and being a burden on caretakers (9%). Threatening behavior toward self (6%) and others (6%) were critical factors also whereas 8% simply gave up, although there was nothing specifically wrong. The authors interpreted these data as indicat- ing that the majority of the patients had returned because of the recur- rence of psychiatric symptomatology. This interpretation received some support from the clinical charts that indicated that 60% of the returnees appeared overtly psychotic at the time of readmission.
In an attempt to extract the precipitating stresses associated with the above problem, Sanders et al recorded the number of complaints and difficulties mentioned by the patient in his own account of why he re- turned. Interpersonal difficulties, employment, physical condition, medi- cation problems, and recreation comprised the majority of the complaints. No attempt was made to include complaints of a symptomatic intrapsychic nature such as anxiety. A comparison of the returnees with a group of nonreturning patients on a large number of measures revealed very little difference between the two groups. Interpersonal problems did not dif- ferentiate them. There was, however, some tendency for returnees to be rated as more anxious than controls, although the authors indicated that psychiatric symptomatology in general was greater among nonreturnees than returnees at the time of original release.
In the final study which compared recidivists and a nonrecidivist group, Davis, Dinitz, and Pasamanick 3 reported a five-year follow-up on a group of schizophrenic patients. The problems of these patients, as indi- cated by a problem checklist filled out by significant others in the patient's life (spouses, relations), were bizarre speech, ideas, and acdons of the pa- tient which disrupted the household. Comparing recidivists and non- recidivists, it was found that recidivists were less cooperative with aftercare treatment staff and that medication seemed to be more of a problem for them than for the nonrecidivists.
There were two studies on the problems that caused return that did not involve a nonrecidivist control group. In the first, Spiegel and Keith- SpiegeP ~ questioned 100 V.A. hospital patients as to reasons for return. Nervousness was described as a primary problem by 42%, whereas 31% of the sample mentioned depression, physical health, and inability to find a job as problems. Almost as frequently cited were financial problems and strange thoughts (26%). Medication problems were mentioned by 15% of the sample, suicidal thoughts by 12%, and being bothered by voices, by 6%.
In the second study, Raskin and Dyson 14 reported on 45 consecutively

207
j . M. SIEGEL A N D C. S T . C L A I R
admitted schizophrenics with previous hospital histories. Information was sought from the patient, his therapist, his family, and from chart review as to reasons for this latest return. The major problems were impulsiveness, loneliness, hopelessness, and problems with therapists.
To summarize, a wide variety of problems besides the recurrence of psychiatric symptomatotogy have been mentioned by patients and those involved with them as reasons for return to the hospital. Self-report of the patients (as opposed to reports about the patients from significant others and professionals) places greater emphasis on physical illness, nervousness, depression, and finances. Reports about the patients tend to emphasize psychiatric symptoms, especially bizarre behavior, and problems with medication. Both patients and those involved with them agree as to the importance of interpersonal conflict, especially within the family, as an important factor in problems causing return.
THE TIMING OF REHOSPITALIZATION
In addition to the "who" and "why" of rehospitalization, research has also been conducted on the issue of "when" patients come back. The six- month period after hospital release seems to be the peak for readmissions. Davis et aP reported the majority of their returns in the six months after discharge. Paul's review 11 on chronicity cited five studies indicating the majority of rehospitalizations occurring within six months of discharge. However, Freeman and Simmons,:' Gurel, 7 and Miller 9 all provide ample evidence that readmissions continue well beyond this point.
In addition to the six months after release, the period 4-6 weeks after release also seems of importance, with many patients returning within this period? ,9,17
THE CURRENT STUDY
None of the studies cited above have compared immediate (6 weeks or less) and delayed returnees (6 months or more) on problems causing re- turn. To these authors' knowledge, there has also been no general research on these two groups of patients possibly disparate in other respects.* It would seem that patients who manage to survive in the community beyond the crucial 6-month period may have different patterns of problems caus- ing return than patients who return within 6 weeks of discharge. I f this proves to be the case, it may have important implications for treatment in the following fashion: The two groups of patients would seem to be the responsibility of different treatment staffs. Patients who return within a few weeks may be, in a sense, the "responsibility" of the hospital which
*Angr is t et al. 1 d ichotomized a n d r epo r t ed on a g r o u p of r e t u rnee s at 6 mon ths , bu t did not separately r epo r t immed ia t e re tu rnees , who were exc luded f rom the study.

208
P A T I E N T PROBLEMS
discharged them, while patients who return after 6 months are the "re- sponsibility" of Outpatient Clinics (at least in a treatment model presuppos- ing continuing care following hospitalization). Early returnees may indicate in their particular pattern of problems different areas of functioning with which hospital treatment might effectively deal prior to discharge. Problem areas where particular support is necessary may be indicated to outpatient clinic personnel responsible for immediate aftercare. Late returnees, on the other hand, may indicate in their particular patterns of problems dif- ferent areas of functioning with which Outpatient Clinics might effectively deal.
These two groups of patients may possibly differ in social competence, with patients who remain in the community longer more socially competent in the sense of being better able to deal with the problem of adjustment to the community. Platt and Spivack 12 have shown a relationship between greater problem-solving ability and social competence in psychiatric pa- tients.
Thus, the major purpose of this study is to see whether two particular groups of returnees (immediate and delayed) differ with respect to fre- quently mentioned problems relating to rehospitalization. The specific goals are (a) to look at similarities and differences in the problems causing return of immediate and delayed returnees, and (b) to attempt to specify therapeutic strategies for dealing with frequently mentioned problems. Both patients' self-reported and presenting problems noted on the hospital charts at readmission will be reviewed.
A subsidiary interest is a comparison of problems of patients returning to two different types of inpatient units, one located in a municipal hospital and the other in a nonprofit hospital, both providing aftercare through the same outpatient service. Responses of immediate and delayed returnees to the two units will be examined for possible differences, as will demographic characteristics.
Additional questions of interest include specifying the location of the problems (e.g., alone, with family, with friends, etc.) and the patients' at- titudes toward current and previous hospitalization.
The patients' skill at solving hypothetical real-life problems will also be assessed. It is hypothesized that long-term returnees will be socially more competent, as indicated by performance on the Means-Ends Problem- Solving Procedure (MEPS). The MEPS is a measure of the ability to cope with hypothetical real-life problem situations and has previously been re- lated to social competence. 12
METHODS
Setting and Patients
The sources of readmitted patients were two different psychiatric in- patient settings. Both are located in urban general hospitals and both offer

209
j . M. SIEGEL AND C. ST.CLAIR
aftercare through the same outpatient service. Unit A is a small, voluntary admissions ward with an average length of stay of 16-17 days. It is an attractive setting with semiprivate rooms for 14 patients, and a high staff- patient ratio. Unit B* is located in a municipal hospital, and hence accepts involuntary commitments and uninsured patients, and therefore potential disposition problems. Its two wards contain 54 beds and the average length of stay is about 30 days.
The patients studied were 86 readmitted patients whose length of stay in the community prior to readmission qualified them for inclusion in the study, which ran for a period of one year, and who were able and willing to cooperate in an interview situation. Of these patients, 47 were readmitted to Ward A and 39 were readmitted to Ward B. Of the Ward A patients, 8 were immediate (early) returnees (6 weeks or less) and 39 were delayed (late) returnees (6 months or more). Of Ward B patients, 13 were early and 26 were late returnees. Early returnees thus totalled 21, and late returnees, 65. A description of the patients' demographic characteristics will be found under Results.
Methods of Measurement
Readmission Questionnaire. The questionnaire was comprised of 19 problems selected from the literature review on reasons for rehospitaliza- tion. Patients were asked to indicate which of these problems had been in any way responsible for their return to the hospital. Next, they were asked to rank order the three problems most responsible for their readmission from the group of problems they had chosen. Additional questions con- cerned the manner of return to the hospital, perception of help received in past hospitalizations, need for help at last discharge, and guilt about return.
Chart Review. In order to obtain a possibly more objective account (than the patients' self-reports) of the three problems most responsible for the patients' readmissions, the intake charts were rated by the two authors. The ratings were done independently for each patient, and without knowl- edge of the subject's hospital history or time since last hospitalization. The procedure employed a listing from the intake record of the three problems that seemed most responsible for the patient's readmission. During the ratings, it became apparent to both raters that problems other than those 19 included in the questionnaire were beginning to appear with some fre- quency (e.g., public disturbance, drug overdose, suicidal ideation) and seven new problems were added to the revised questionnaire.
A revised version consisting of the original 19 problems plus 7 additional problems derived from the chart review was given to 29 patients. The added problems did not discriminate the groups.
Agreement between the two raters was generally high. The disagree- ment per problem ranged from zero to 21 percent. The two raters resolved
*Unit B is no longer in operation.

210
PATIENT PROBLEMS
all disagreements through discussion with the following rules: (a) any men- tion of medication problems in the chart was always included in the top three problems in order to indicate the frequency of the residents' percep- tions of this problem; (b) the "assault" problem was broadened to include assaulting gestures (e.g., flourishing a knife) as well as actual assaults; (c) when "depression" was noted as present, it was not included by the raters if suicide (both ideation and actual attempts) was mentioned, and the patient could be clearly rated as having two other salient problems; and (d) an overdose was listed under "overdose," rather than "suicide attempt," unless the chart specifically mentioned that an overdose was deliberately taken in a suicide attempt.
Means'-Ends Problem-Solving (MEPS). The MEPS procedure measures the ability to plan, in a stepwise fashion, means to reach a stated goal. Specifically, subjects are presented with an interpersonal problem situation in the form of a very brief story, consisting of a beginning and an end, and are asked to complete the story by making up a middle portion.
The subject's response is scored for the number of instrumental acts which enable the story protagonist to reach the stated goal. Individual story scores are summarized to provide a single total score. The following story is a sample: "Mr. C. had just moved in that day and didn't know anyone. Mr. C. wanted to have friends in the neighborhood. The story ends with Mr. C. having many good friends and feeling at home in the neighborhood. You begin the story with Mr. C. in his room immediately after arriving in the neighborhood." The acceptable means for this story would be: (a) visit neighbors, (b) give a party, (c)join a neighborhood organization, etc. These would be scored as relevant means. In contrast, the response "he stayed in his room and watched his neighbors walk down the street" or "he was a nice man so he had many friends" would be unacceptable responses. The number of responses which were not effective in reaching the stated goal were also examined. Four situations from the MEPS were employed (cf. Platt, Spivack, and Bloom la stories 3, 6, 7, and 8).
Procedure Subjects were interviewed on the two inpatient units. The readmission questionnaire was administered first and the MEPS second. The procedure usually took less than one hour and was generally completed in one session.
RESULTS
Demographic Variables and Psychiatric History
The four groups of patients were immediate (early) returnees (rehos- pitalized within 6 weeks of previous discharge) and delayed (late) returnees (6 months or more since last hospitalization) interviewed on Wards A and B. There were some significant demographic differences between them.

211
J. M. SIEGEL AND C. ST.CLAIR
Compared with the combined late returnees, the 21 early returnees were younger (30.86 years + 10.06, vs. 36.48 years -+ 13.31, p < .05), but were of both sexes and both major races. The 65 late returnees tended to be older, two-thirds female (nonsignificant trend), and 70%* black (p < .05). Considering the four groups separately, the one unusual group is the early returnee group to the small voluntary admission ward (A), whose average education level beyond high school contrasted significantly (p < .05) with the 9th grade education of all the other groups. This education level finding gives some indication that the early returnees to Ward A were socially more competent compared to the other three groups.
The four groups did not differ on readmission diagnosis, marital status, or average number of previous hospitalizations. About half of each group was initially diagnosed as schizophrenic at readmission. Marital status, a powerful predictor of both readmission and premorbi~t social competence, does not discriminate these groups (all groups are about 40-50% "never married"), nor does number of previous hospitalizations (the median for all groups is three to four). However, there was a distinct difference on -residence of adult patients in their parents' homes (another indicator of social competence): the younger and better educated early returnees to the small Ward A had all left the parental home, compared to an extreme of 40% of the delayed returnees to the city hospital who were still living in the parental home at an average age of 40 years (p < .025).
In summary, the four groups appeared to come from similar psychiat- ric populations. One of the early returnee groups was significantly more socially competent than any of the other three groups as judged by educa- tional achievement and residence outside the parental home.
Patient Reports of Problems Leading to Readmission
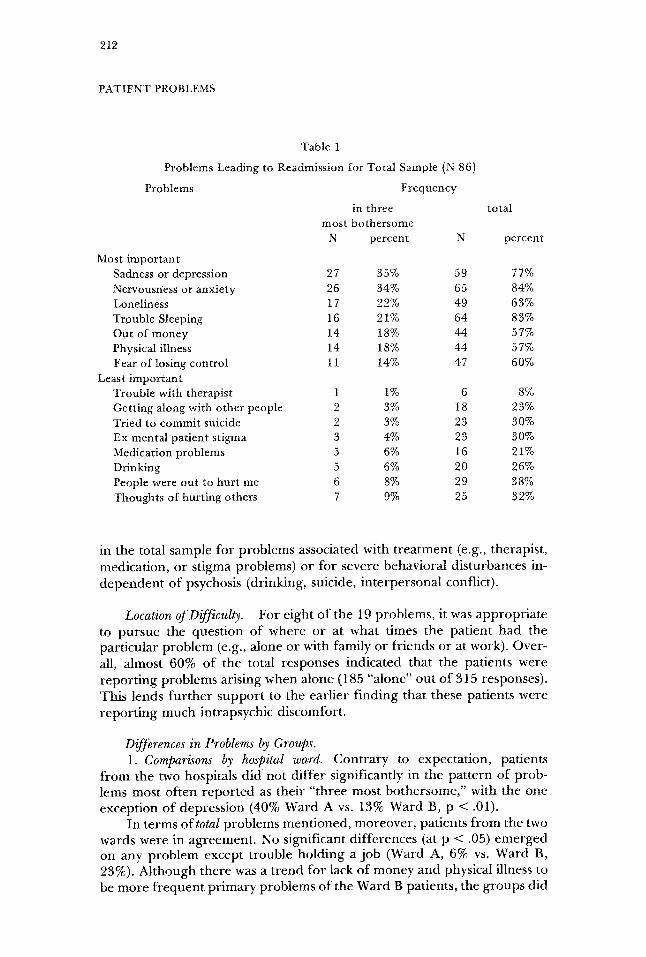
Most and Least Important Problems (all groups combined). Patients were asked to indicate the three most bothersome problems responsible for their return to the hospital from the list of total problems that they had pre- viously indicated had caused their readmission. Table 1 shows the prob- lems leading to readmission. At the top are the problems that were most frequently cited as among the "three most bothersome" problems, while below are those least frequently cited as among the "three most bother- some." The numbers in the left hand column refer to the "most bother- some" frequencies. Also shown in the table (in the right hand columns) are the total number of times a problem was mentioned by one of the 86 patients even if he did not later include it as among his "three most bother- some."
Note that the total group (combined over type of hospital unit and time of readmission) was most concerned with problems of internal dis- tress, such as depression, anxiety, and loneliness. There was little concern
*All p values shown for percentage differences result from a z test for proportions.
212
PATIENT PROBLEMS
Table 1
Problems Leading to Readmission for Total Sample (N 86)
Problems Frequency
in three total most bothersome
N percent N percent
Most important Sadness or depression 27 35% 59 77% Nervousn~ess or anxiety 26 34% 65 84% Loneliness 17 22% 49 63% Trouble Sleeping 16 21% 64 83% Out of money 14 18% 44 57% Physical illness 14 18% 44 57% Fear of losing control 11 14% 47 60%
Least important Trouble with therapist 1 1% 6 8% Getting along with other people 2 3% 18 23% Tried to commit suicide 2 3% 23 30% Ex mental patient stigma 3 4% 23 30% Medication problems 5 6% 16 21% Drinking 5 6% 20 26% People were out to hurt me 6 8% 29 38% Thoughts of hurting others 7 9% 25 32%
in the total sample for problems associated with t rea tment (e.g., therapist, medication, or stigma problems) or for severe behavioral disturbances in- d e p e n d e n t o f psychosis (drinking, suicide, in te rpersonal conflict).
Location of Difficulty. For eight o f the 19 problems, it was appropr ia te to pursue the quest ion o f where or at what times the pat ient had the part icular problem (e.g., alone or with family or f r iends or at work). Over- all, almost 60% of the total responses indicated that the patients were r epor t ing problems arising when alone (185 "alone" out o f 315 responses). This lends fu r t he r suppor t to the earl ier f inding that these patients were repor t ing much intrapsychic discomfort .
Differences in Problems by Groups'. 1. Comparisons by hospital ward. Cont ra ry to expectat ion, patients
f rom the two hospitals did not d i f fer significantly in the pat tern o f prob- lems most of ten r epo r t ed as their " three most bo thersome," with the one except ion o f depress ion (40% Ward A vs. 13% Ward B, p < .01).
In terms of total problems ment ioned , moreover , patients f rom the two wards were in agreement . No significant di f ferences (at p < .05) e me rg e d on any prob lem except t rouble holding a job (Ward A, 6% vs. Ward B, 23%). Al though there was a t rend for lack o f money and physical illness to be more f r equen t p r imary problems o f the Ward B patients, the groups did

213
J. M. SIEGEL AND C. ST.CLAIR
not d i f fe r in expressed concern abou t in t rapsychic p rob lems in t e rms o f mos t f r equen t ment ion .
2. Comparisons by early vs. late readm~sion. T h e combined sample o f 86 pat ients was d ichotomized accord ing to t ime o f readmiss ion: 21 re tu r - nees within 6 weeks o f d ischarge ( immedia te or early) and 65 re tu rnees a f te r 6 mon t hs or m o r e in the c o m m u n i t y (delayed or late).
For bo th immed ia t e and delayed re tu rnees , "anxiety" (33% early and 23% late) and "depress ion" (43% a n d 23%, respectively) were the most b o t h e r s o m e prob lems . No d i f fe rences significant at p < .05 arose on the primary" p rob lems .
In t e rms of total t imes a p r o b l e m was cited, the re was also a g r e e m e n t as to the mos t f r equen t p rob lems , similar to the intrapsychic p rob l ems de- scribed as most c o m m o n in the total sample. However , some interes t ing d i f ferences e m e r g e d be tween early and late r e tu rnees (see Tab le 2). T h e early r e tu rnees were significantly m o r e likely to compla in o f difficulty with living a r r a n g e m e n t s (52% as o p p o s e d to only 29% o f the g r o u p that stayed longer in a communi ty , p < .05) and o f t rouble with a therapis t (19% of early vs. 3% of late, p < .025). S u p p o r t for these compla in ts is f ound in a t r end for m o r e o f the self-referrals back to the hospi tal to be early re tur - nees, who also admi t t ed when ques t ioned that they came back because "things got to be too much" fk)r t h e m ra the r than to a "place to get good t rea tment . " In contrast , the later r e tu rnees were significantly m o r e likely to compla in that they were hea r ing voices or seeing things (51% vs. only 14%
Problems
Table 2
Problems Discriminating a Immediate (Early) vs. Delayed (Late) Returns
Percent Percent early late
(N 21) (N 65) Z pb
aThe criterion for including a problem in the table was a percentage difference of ~ 10% be- tween early and late returns. The Ns shown are total frequency of mention per problem by each group.
bThe p values showns are for two-tailed tests, based on z test for proportions.
More common to early returnees Sadness/depression 81 65 1.40 n.s. Place to live, rent 52 29 1.94 .05 Stigma as ex mental patient 38 23 1.35 n.s. Finding a job 38 28 .90 n.s. Trouble with therapist 19 3 2.50 .01
More common to late returnees Heard voices/saw things 14 51 2.95 .002 Medication problems 5 23 1.88 .06 Holding a job 5 17 1.40 n.s. Trouble sleeping 67 77 .94 n.s.

214
P A T I E N T PROBLEMS
of the early group, p < .01) and of trouble with medication (23% vs. 5%, p < .10).
No other differences were large enough to attain statistical signifi- cance. The percentages that do differ by 10% or more are shown in Table 2, however, since they suggest an interesting hypothesis to pursue with a larger pool of early returnees. The group that was rehospitalized within 6 weeks, as compared to those who survived longer in the community, pre- sented a picture of discouragement rather than psychopathology per se. They more frequently complained of depression, trouble finding a job or living arrangements, discrimination because they were former mental pa- tients, and trouble with their therapists. In contrast, the late returnees, after 6 months or more in the community, more frequently mentioned serious symptoms (e.g., hallucinations), medication problems, trouble sleeping, and not being able to hold a job.
3. Early vs'. late readmission by hospital unit. Examination of the data suggested that there were enough differences between early and late pa- tient groups at the two hospitals to warrant separate examination of the four groups. However, total Ns of 8 and 13 in the two early groups make it difficult either to attain or to interpret statistical significance. Only prob- lems encompassing more than 25% of each group's own "most bother- some" responses will be presented for this reason.
Of the eight early returnees to the small voluntary unit (Ward A), six out of eight (75%) listed "depression," and four listed "anxiety," among their most prominent problems. The 39 late returnees to this same unit most often mentioned depression also, but in a much smaller proportion (33%, p < .05), and loneliness rather than anxiety was second, at 28%. Returnees to the same ward thus both rated depression as their primary problem, but place a differing value on anxiety (early) or loneliness (late) (p < .10 and p < .05, respectively), depending upon how long they had been out of the hospital.
As for the large nonvoluntary city unit (Ward B), the 13 early retur- nees' "most bothersome" reported problems were "physical illness" (38%), being "out of money" (13%), and "fear of losing control" (31%). The late returnees to this ward reported "nervousness/anxiety" (27%) as a major complaint and also "trouble sleeping" (31%), neither of which represents significantly different percentages from this ward's early group. However, the early group's emphasis on illness and loss of control are significantly different (at p < .05), although the emphasis on being out of money does not meet this criterion.
Note that these early return patients were thus claiming they were rehospitalized on a psychiatric ward primarily because they were physically ill and out of money. The only internal distress they admitted to in their "most bothersome" problems was fear of losing control. Contrast this to the self-reports of the other ward's early returnees, who were readmitted to a voluntary admissions ward and whose primary self-reported complaints were anxiety and depression. This distinction between the two groups, both

215
j. M. SIEGEL AND C. ST.CLAIR
of whom were rehospitalized within 6 weeks, emerges even more clearly in the intake review data to be presented below.
Chart Review on Primary Reasons for Rehospitalization
Primary reasons for rehospitalization were aiso categorized from in- take notes on these patients' hospital charts.
Total Sample. The problem most often identified in the residents' reports on the total group of 86 patients was hallucinations (N = 35 or 41%). Problems with medication (N = 20 or 23%), depression (N = 19 or 22%), and creating a public disturbance (N = 17 or 20%) were next. Assault against self (clear suicidal attempt, not just threat) or against other (active gesture) each appeared in the records at least 12 times (14%), and other "bizarre actions" 14 times (16%). In short, the majority of these problems most frequently mentioned at intake were public events. They make an interesting contrast to the patients' picture of internal misery as the most bothersome problem leading to rehospitalization, and support the conten- tion of some clinicians that a patient becomes a high risk for rehospitaliza- tion when his pathology becomes bothersome to others.
Just as striking is the absence of assignment of presenting problems to the categories of "loneliness," "trouble sleeping," and "out of money" since these three problems ranked among the most frequent and bothersome in the patients' self-reports. The most important difficulties leading to rehos- pitalization as perceived by the "objective" residents were clearly in a dif- ferent sphere from the patients' pictures of subjective discomfort.
Early vs. Late Readmissions by Hospital Unit. Once again clear dif- ferences are suggested between the early and late readmissions by hospital, even though the rating of these intake problems was controlled so that the chart reviewers did not know either the time or the ward of readmission. The two early groups were so small that caution must be exercised in interpreting results. However, these two groups emerged as very different in the blind chart rating. The criterion for discussion is problems common to more than 25% of each group. It is interesting that the Ward A early readmissions (already noted as younger and better educated), had."depres- sion," "trouble getting along with others," and "suicide attempt" as their prominent problems (50, 50, and 38%). In sharp contrast, the city hospital early group most often fell into the clearly visible categories "heard voices" (46 %), "assaulted others" (31%), and "public disturbance" (31%). Examina- tion of these percentage differences for significance showed that despite the small Ns the two early groups differed on depression (50 vs. 8%, p < .05), trouble getting along (38 vs. 8%, p < .10), assault (0 vs. 31%, p < . 10), and public disturbance (0 vs. 31%, p < . 10).
While the late group from the city ward was also high on "heard

216
PATIENT PROBLEMS
voices" (54%), their main problems were not assault or public disturbance but rather other nonviolent "bizarre actions" (31%) and medication prob- lems (27%). It is possible that this ward's early group did something con- spicuous to get rehospitalized, while the later returnees simply deteriorated following medication problems. (The late group from the smaller unit was harder to categorize with only hallucinations (36%) representing one- fourth of the problems.) The two late groups differ significantly on bizarre actions (31 vs. 8% in the city ward, p < .05) but not on medication (27 vs. 15%)
Additional Patient Data (Need for Help, Guilt, Problem-solving Ability)
The four groups did not differ significantly in the amount of help they felt they received the last time in the hospital (see Table 3). However, when asked how much help they felt they still required from doctors when they left, the early returnees from the voluntary admissions ward were signifi- cantly (p < .01) more likely than any other group to report that they felt they needed more help at discharge. This early group also expressed more guilt about coming back (p < .01). They were also significantly (p < .01) better able than the other three groups to provide numerous and relevant solutions for hypothetical real-life problems (see Table 4). Problem-solving ability has been demonstrated to be independent of intelligence 1~ but re- lated to prehospital social competence. 12 The MEPS results support the suggestion of the superior social competence of the Ward A early returnee group, as was demonstrated by their educational achievement. Note that this group also reported they needed more help at previous discharge, which may suggest better insight about their situation than the other groups.
Table 3
Mean Scores of Return Groups on Percept ions o f Help and Guil t
Ward A groups Ward B groups
I tem a Early Late Early Late
(iN 8) (N 36) (N 10) (N 21) F b
Helped last t ime in M 2.00 2.37 2.50 2.43 .54 n.s. hospital SD .76 .97 .71 .93
Still needed help M 2.63 1.69 .67 .91 6.71 at discharge SD .74 1.30 1.12 1.02
Gui l ty coming back M 2.13 .74 .91 .48 4.99 to hospital SD 1.25 1,04 1.22 .87
a Scoring: O Not at all, no help, no guilt; 1 Very little, a little, little; 2 Somewhat, some, some- what; 3 Very much, a lot, very, b N
bNeuman-Keuls tests following significant Fs discriminated Ward A early means only (p/ .01). C p .01.

217
J, M. SIEGEL AND C. ST.CLAIR
Table 4
Mean Scores of Return Groups on Means-End Problems-Solving Stories
Ward A Ward B Score Early Late Early Late F a
Total means produced M 7.00 2.89 2.25 2.45 5.42 b SD 2.97 2.81 2,93 2.39
Irrelevant means/ M .17 2.07 2.50 2.00 4.14 b no means SD ,4t 1.46 1.38 1.38
a Neuman-Keuls tests discriminated Ward A Early means from all other at p ~ . 0 1 . b p .01
DISCUSSION
Of the problems leading to readmission, "anxiety/nervousness" was the most tYequently mentioned. Almost 85% of all subjects mentioned it as a problem associated with rehospitalization, and over one-third listed it as one of their three "most bothersome" problems. "Sadness/depression" was also frequently mentioned by over 75% of the patients and ranked as among the most bothersome by about 35%. This finding on most bother- some problems is similar to that of Spiegel and Keith-Spiege116 as pre- viously described. Of the other frequently mentioned problems in the cur- rent study, being out of money and physical illness were endorsed by 57% as among their three most bothersome problems. Other prominent prob- lems of the eight early returnees to Ward A were loneliness, trouble sleep- ing, and fear of losing control; five may be considered primarily reflective of internal distress.
Among the least frequently mentioned problems were trouble with therapist or medication, and problems in the interpersonal sphere such as trouble getting along with others. In terms of the area of location of their difficulties (alone or with others), the patients also indicated generally that they were more frequently distressed when alone than when being with others.
The emphasis on intrapsychic complaints in this largely schizophrenic, multihospitalized group may suggest that more severely disturbed inpa- tients have, during the course of their career as chronic patients, experi- enced a gradual diminishment of their interpersonal sphere (fewer and fewer contacts with people) to the point where there are so few meaningful contacts with others that interpersonal problems are not a prominent pos- sibility. Another possible explanation is that these chronic patients may be "process" schizophrenics whose interpersonal interaction has always been limited.
This pattern of complaints of internal distress in this largely schizo- phrenic sample of patients seems to indicate the need for therapeutic ap- proaches that focus on the patient's intrapsychic distress when alone.

218
PATIENT PROBLEMS
"Anxiety/nervousness," as mentioned above, was the most frequent prob- lem mentioned. Sanders et al. 15 in a study previously cited, reported that their returning chronic patients were somewhat more anxious than the nonreturning chronic patients in their study, although in general there was little other difference between the two groups. This may suggest that the ability to learn to manage one's own anxiety level may be a crucial element in being able to remain in the community. Techniques are available to aid discharged inpatients in dealing more effectively with their own anxiety, such as the behavior therapy technique of systematic desensitization? 8
There is also some indication from the results of the current study that the patients' preoccupation with their subjective distress, physical concerns, and money problems were not salient fbr the psychiatric residents who interviewed the patients on readmission. This may be unfortunate since we may be losing sight of the fact that providing support around problems of internal distress may be of crucial importance in keeping patients in the community.
Medication problems have been seen as an area of particular concern by many investigators. Studies by Zolik et al. 19 and Davis et al. a gave some indication that medication problems are more often a factor in patients' recidivism than patients actually report themselves. In the current study, only 16 of these 86 seriously disturbed patients even mentioned it as a problem, of whom all but one were late returnees. Only five listed it among their most important concerns. That the patients may have been underes- timating medication problems is supported by studies previously cited by Spiegel and Keith-Spiegel 1~ and Sanders et al? ~ which also had compara- tively small numbers of patients reporting medication problems.
Related to the low incidence of patients mentioning medication prob- lems is the issue of so few patients mentioning problems with therapists. Does the low incidence of therapist problems reflect satisfaction with therapists, or the relative unimportance of therapists in the patients' daily lives, or failure to remain actively in treatment with therapists? I f the latter is true, then a therapeutic strategy focused on improving continuity of care after discharge is more salient than focusing on the medication problem per se. A chronic patient not actively engaged in some type of supervised aftercare is obviously going to develop "medication problems" very quickly.
Regarding differences between early and late returnees, the litany of complaints more common to early returnees suggests an inability to adjust to the social situations outside the hospital, rather than the overt psychotic symptoms complained of more frequently by late returnees. Early retur- nees were more likely to report difficulties that seemed objectively related to the situation of being just released from a mental hospital. The most prominent of these difficulties included finding a place to live, the om- nipresent "sadness/depression," the stigma of being an exmental patient, and trouble with therapist. Late returnees, on the other hand, were more likely to report the recurrence of florid psychiatric symptomatology such as hallucinations.
When data from the residents' intake notes were examined, further

219
J. M. SIEGEL AND C. ST.CLAIR
distinctions emerged. First, presenting problems of the early groups from the two inpatient wards were quite different, although both groups were clearly effective in achieving early rehospitalization. The voluntary ward early returnees were most frequently cited as showing depression, suicidal ideation, and trouble getting along with others. In contrast, the city hospital early returnees displayed public acting-out behaviors in effecting rehos- pitalization: hallucinations, assault, and creating a public disturbance. To the extent that administrative policies toward rehospitalization differ at the two hospitals, both groups may be demonstrating an accurate perception of how sick one must be to effect a quick readmission. That is, a depressed patient might be rather easily readmitted to a small voluntary unit, where~is at the city hospital residents are more likely to give the recidivist medication and send him home unless he is actively bothering society. These patients have already averaged more than three hospitalizations, and they dearly "know the ropes." If our inference is accurate about the discouragement in the self-reports of the early returnees, this interpretation of the behaviors noted in the chart review appears even more likely.
The residents' notes on the readmission of the late patients are clearly different in quality from those on the early returnees. Both late groups are characterized by hallucinations. Bizarre but nonviolent behavior and medi- cation problems also characterized the city ward patients who remained in the community over six months. In contrast to the public acting-out of the early city ward returnees, a deterioration effect following a medication halt is suggested for these late readmissions. Do these patients returning after 6 months tire of medication as a way of life, or decide they are well because they have not been hospitalized for so long, and thus stop medication? The fact that only in the late patients' se/f-reports medication is important lends further support to this distinction found in the residents' notes.
Finally, the distinctiveness of the ward A (voluntary admissions) retur- nees from the other groups constituted one of the most interesting findings of the study. This small group was clearly a socially more competent group, as indicated by its educational attainment and its problem-solving skills. It was also the group that reported retrospectively that it needed more help at the time of the previous discharge, and was somewhat more guilty about having to return to the hospital than the other three groups. These patients also tended to be younger than the others and though largely unmarried, to have made the break from the parental home. It was hypothesized origi- nally that it would be the long-term (delayed) returnees who would appear as socially more competent on demographic measures as well as on the problem-solving measure, because the ability to remain out of the hospital six months or more might be seen as another indication of social compe- tence. This hypothesis was not confirmed. Greater social competence seemed related to the combination of a very brief stay in the community and readlnission to the voluntary ward. It may be that these early returnees felt that they could have benefitted from a longer period of hospitalization, and their prompt return to the hospital was an adaptive response to their continuing state of distress. They did indicate that they felt that they

220
PATIENT PROBLEMS
n e e d e d m o r e he lp at d i scharge . I n any case, they d i f f e r as radical ly f r o m
the ear ly r e t u r n e e s to the city hosp i ta l as to e i t h e r late g r o u p .
R E F E R E N C E S
1. Angrist S, Lefton M, Dinitz S, Pasamanick B: Women After Treatment: A Study of FoTwer Mental Patients and Their Normal Neighbors. New York, ApptetonrCentury-Crofts, 1968.
2. Anthony WA, Buell SS, Sharratt S, Althoff ME~ Efficacy of psychiatric rehabilitation. Psychol Bull 78:)t47-456, 1972.
3. Davis AE, Dinitz S, Pasamanick B: The prevention of hospitalization in schizophrenia: five years after an experimental program. AmJ Orthopsychiatry 42:375-388, 1972.
4. Ellsworth RB: Non-professionals in Psychiatric Rehabilitation. New York, Appleton- Century-Crofts, 1968.
5. Freeman HE, and Simmons OG: The Mental Patient Comes Home. New York, Wiley & Sons, 1963.
6. Graft H, Kenig L, Radoff G: Prejudice of upperclass therapists against lower-class pa- tients. Psychiatr Q 45:475-489, 1971.
7. Gurel, L: A forward-looking backward glance: An overview of past, present, and pro- jected program evaluation staff research. Presented at the 12th Annual Conference on VA Cooperative Studies in Psychiatry, Denver, April, 1967.
8. Harakal CM, Goldman C: Further psychiatric contacts of former inpatients in one year following discharge. Research and Evaluation Report No. 18. Philadelphia, Hahnemann Medical College and Hospital, 1972.
9. Miller D. Worlds that fail. Part I: Retrospective analysis of mental patients' careers. California Mental Health Research Monograph, 1965, No. 6.
10. Orlinsky N, D'Elia E: Rehospitalization of the schizophrenic patient. Arch Gen Psychiatry 10:47-54, 1964.
11. Paul GL: Chronic mental patient: Current status-future directions. Psychol. BuU 71:81-94, 1969.
12. Platt J J, Spivack G: Social competence and effective problem-solving thinking in psychiat- ric patients.J Clin Psyehol 28:3-5, 1972.
13. Platt J J, Spivack G, Bloom M: Means-ends Problem-solving (MEPS): Manual and Tentative Norms. Philadelphia, Department of Mental Health Sciences, Hahnemann Medical Col- lege and Hospital, 1971.
14. Raskin M, Dyson WL: Treatment problems leading to readmissions of schizophrenic patients. Arch. Gen. Psychiatry 19:356-360, 1968.
15. Sanders R, Smith RS, Weinman BS: Chronic Psychoses and Recovery. San Francisco, Jossey- Bass, 1967.
16. Spiegel DE, Keith-Spiegel P: Why we came back: A study of patients readmitted to a mental hospital. Merit Hyg 53:433-437, 1969.
17. Spiegel D, Younger J: Life outside the hospital: A view from patients and relatives. Merit Hyg 56:9-20, 1972.
18. Zeisset RM: Desensitization and relaxation in the modification of psychiatric patients; interview behavior.J Abnorm Psychol 73:18-24, 1968.
19. Zolik ES, Levin I, Hubek P: Comprehensive community care and patient rehospitaliza- tion. Proceedings of the 78th Annual Convention of the American Psychological Associ- ation, 503-504, 1970.