patient experience strategy - uhs · the patient experience strategy 2012-2016 our clinical,...
TRANSCRIPT
1
Patient Experience Strategy December 2012 – December 2016
2
“Putting the patient first… it’s in our DNA” Introduction & Background to the Strategy Patients tell us that good hospital care depends on getting the basics right. It is important to patients to receive good nutrition and hydration, to feel safe and cared for, to have care provided in clean and pleasant environments, and to feel trust and confidence in those caring for them. With over 10,000 patient episodes every month, our goals for providing a high quality, consistently positive patient experience may be ambitious but they are essential. Our highest priority is to provide care, treatment and facilities to meet the fundamental needs of patients, relatives and carers who use our services. We are determined to build on the success of delivering the previous patient experience strategy over the last 3 years. We believe a high quality care environment and appropriate support is a key part of the healing process, and this needs to be underpinned with clear standards for care. In this document, the reader will find the trust’s strategy for improving patient experience has been refreshed and updated. The revised strategy sets out the trust’s vision and goals for improving patient experience over the next four years (2012 to 2016). The strategy is aimed at adults, children, young people and women and their partners accessing maternity services.
Our Values In 2011, the trust developed a new set of values which underpin everything we do. They are currently being launched trust wide. The values are:
Patients First Working together
Fresh Thinking
Patients and families lie at the heart of everything we do. Their experience of the hospital, and their perceptions of the trust, are our measures of success.
The Patient Experience Strategy 2012-2016
Our clinical, technical and support staff are all crucial to providing
successful services. We work together for
maximum effect, and collaborate to make internal boundaries invisible to patients.
We incorporate new ideas, technologies and greater
efficiencies in the services we provide. We value research and education as drivers of future innovation and development, and also recognise our individual responsibilities for improvement.
We aim to make these values ‘what we do’ and ‘who we are’ - in essence they are to become our “DNA;” they building blocks of our organisation. They help us to inspire, develop and support every staff member to live the values for every patient, every colleague, every day.
These values are about us all helping each other to deliver great patient experience more consistently – involving people who use our services, their families, carers, staff and partners in continuing to improve the experience people have using and delivering our services.
This strategy provides us with a detailed blueprint of how we are putting “Patients First”. We know we have not yet achieved our goal of providing a positive patient experience for everyone who accesses our services; but we want to change our culture; the way we do things and increasingly be able to say that our healthcare professionals, managers and staff work in true partnership with patients, family and carers in delivering the best healthcare possible.

3
Our Staff Our staff are our biggest asset. We understand that in order to deliver a good patient experience, we also have to ensure a positive staff experience. Many of the themes in this strategy apply directly to staff as well as patients, and are detailed in our human resource policies and strategies.
Defining Patient Experience Currently, there are several definitions of patient experience which reflect that patients are very clear about what makes a good and poor experience. A positive patient experience is defined by the Department of Health as:
We therefore want people who use our services to experience care and treatment which is:
Welcoming Dignified Kind Respectful
Gentle Safe Personal Compassionate
Informative Sensitive Comforting Understanding
Caring Helpful Reassuring Supportive
Why Improve Patient Experience? Goodrich and Cornwall (2008) set out the case for why it is necessary to have a clear strategy for improving patient experience, in terms of clinical outcomes and the success of the organisation:
Improving patient experience makes good sense for patients because: • The reduction of anxiety and fear can speed the healing process and shorten
patient’s length of stay and decrease their acuity levels
• The provision of information reduces post operative complications
• Good communication/information enables people to (self) manage their illnesses more effectively
• Effective communication improves treatment and medications compliance
Improving patient experience makes good business sense because: • Patients are increasingly using the internet to rate their experience, affecting
organisational reputations
• The NHS choice programme has expanded under the Liberating the NHS reform programme (DoH 2012), further empowering patients to choose services perceived to provide the best care and treatment
“Getting good treatment in a comfortable, caring and safe environment, delivered in a calm and reassuring way; having information to make choices, to feel confident and feel in control; being talked to and listened to as an equal and being treated with honesty, respect and dignity”. (DoH, 2009) It is a moral and human imperative to protect people when they are sick, weak and vulnerable. This strategy sets out our intentions to improve patient experience across all trust departments and specialties over the next 4 years. It includes newborns, babies, children, young people, adults and older people – in short, every patient, relative and carer who comes into contact with our services will be impacted by the goals laid out in this strategy.

4
• Hospitals suffer financial penalties when the quality of care is poor
• A positive patient experience affects staff experience and can impact on recruitment and retention
• Poor staff-patient communication can lead to higher litigation costs
• Providing a good patient experience ensures organisations meet their statutory and regulatory obligations
This strategy has been developed within the context of a number of key reports, regulatory requirements and legislation. A summary of these can be found in appendix A. In 2012, both the Department of Health and the National Institute for Clinical Excellence (NICE) published core documents which include national standards for patient experience, and a DoH framework for patient experience (appendices D and E refer). This strategy incorporates all elements of both of these documents as well as those required in the NHS constitution and regulatory standards.
What do patients, family & carers want & need? Patient views backed by research, tell us that in addition to receiving the best possible treatment, patients want and expect:
• A safe and clean environment • To be treated as individuals, with dignity and respect for their culture, lifestyles and
beliefs
• To have their voice heard, to be valued for their knowledge and skills and to be able to exercise real choice about treatments and services
• To receive detailed high quality written and/or verbal information about their condition
and possible treatment, given in an honest, timely and sensitive manner at all stages of the patient pathway
• To know what options are available to them under the NHS, voluntary and independent
sectors, including access to self-help and support groups, complementary therapy services and other information
• To know that they will undergo only those interventions for which they have given
informed consent
• To have good face-to-face communication with health and social care professionals
• To know that services will be well co-ordinated
• To know that their physical symptoms will be managed in a way that is acceptable to them & is consistent with their clinical situation & clinicians’ current expertise
• To receive emotional support from professionals who are prepared to listen to them and are capable of understanding their concerns
• To receive support and advice on financial and employment issues
• To know their beliefs and values will be respected and supported through appropriate
spiritual care
• To receive support to enable them to explore spiritual issues
• To receive care at the end of life that meets their individual preferences and needs
5
• To be assured that their family and carers will be supported throughout the illness and in bereavement
• To be cared for in an environment where there are sufficient, well trained staff to meet
their needs.
Our approach to improving patient experience
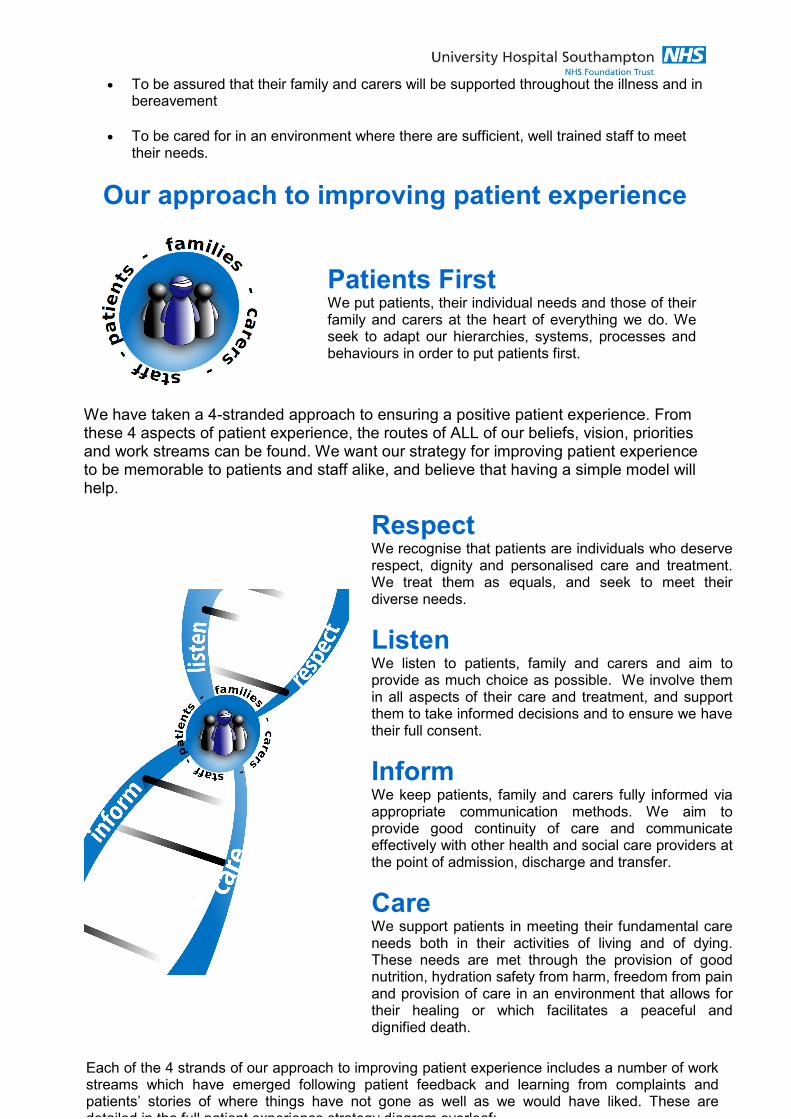
We have taken a 4-stranded approach to ensuring a positive patient experience. From these 4 aspects of patient experience, the routes of ALL of our beliefs, vision, priorities and work streams can be found. We want our strategy for improving patient experience to be memorable to patients and staff alike, and believe that having a simple model will help.
Patients First We put patients, their individual needs and those of their family and carers at the heart of everything we do. We seek to adapt our hierarchies, systems, processes and behaviours in order to put patients first.
Respect We recognise that patients are individuals who deserve respect, dignity and personalised care and treatment. We treat them as equals, and seek to meet their diverse needs.
Listen We listen to patients, family and carers and aim to provide as much choice as possible. We involve them in all aspects of their care and treatment, and support them to take informed decisions and to ensure we have their full consent.
Inform We keep patients, family and carers fully informed via appropriate communication methods. We aim to provide good continuity of care and communicate effectively with other health and social care providers at the point of admission, discharge and transfer.
Care We support patients in meeting their fundamental care needs both in their activities of living and of dying. These needs are met through the provision of good nutrition, hydration safety from harm, freedom from pain and provision of care in an environment that allows for their healing or which facilitates a peaceful and dignified death.
Each of the 4 strands of our approach to improving patient experience includes a number of work streams which have emerged following patient feedback and learning from complaints and patients’ stories of where things have not gone as well as we would have liked. These are detailed in the full patient experience strategy diagram overleaf:

6
Our model for improving patient experience

7
How our work streams will deliver improved patient experiences in 2013 - 2014:
Respect: Milestones for 2013/14 Providing excellent customer care
Delivery of a customer care training programme to outpatient staff with subsequent roll out to other wards and departments.
Compassionate care Implementing values based recruitment and selection processes.
Privacy & dignity Refreshing the privacy signs on bed curtains and developing a policy for chaperoning.
Same sex accommodation
Continued delivery of the 2012/13 same sex accommodation milestone plan (see trust website for details)
Equality & Diversity Delivering the actions to ensure compliance with the NHS Equality Delivery Scheme by April 2013
Transforming UHS Culture
Launch of a new work programme to embed the trust’s values and identify/translate these values into behaviours for all staff.
Vulnerable Adults Delivering the plan for safeguarding adults, including revising training approaches, updating the mental capacity policy and undertaking root cause investigations on all safeguarding alerts.
Vulnerable Children Continuing to build on the success of the safeguarding children strategy
Providing emotional & spiritual support
Develop innovative training to equip staff to provide compassionate care and effective emotional support to patients, families, carers and staff alike. Delivering our spiritual care policy.
Listen: Milestones for 2013/14 Choice Review the patient experience of the choose and book system and work
with general practitioner colleagues to improve this.
Active participation & Involvement
Deliver the patient and public involvement strategy and annual plan
Consent Continue to train staff in the use of mental capacity assessments in relation to informed consent
Experience Based Co-design
Deliver the Experience Based Co-Design (EBD) project.
Patient surveys Review and reform the methods for using real time surveys to gain patient satisfaction and opinion data. Increase the number of surveys completed at ward and department level.
Feedback Develop systems to capture patient feedback from a variety of sources and ensure learning and action from key themes.
Friends and Family Test
Deliver the DoH Friends and Family test project on time and in budget. Ensure robust plans in place to ensure UHS is in the upper quartile for the national FFT benchmark. Support clinical areas with lowest net promoter scores by understanding data.

9
Inform: Milestones for 2013/14 Continuity of care Verbal information
Develop a named registered nurse/midwife system where this is not currently operational. Review medical teams and the running of the hospital out of hours
Communication Deliver the annual Patient Improvement Framework targets, ensuring effective patient communication (verbal and written)
Written Information Refresh the policy and delivery plan for written & accessible information
Access and admission
Set standards for patient letters and roll these out to all care groups
Transfer and discharge
Set a regular programme of surveys in place for patients who have been discharged
Family and visitors Consult on and develop a new visiting policy.
Carers Roll out the Carer’s Information Trolley project into all relevant care groups. Implement the Carer Assessment Form in all relevant clinical areas. Hold at least one carers listening event.
Care: Milestones for 2013/14 Personal care Set and launch clear standards for the provision of personal care and
hygiene
Pain management Deliver actions to improve pain management, including roll out of the pain assessment tool to ALL care groups.
Nutrition and hydration
Finalise and launch the trust’s nutrition and hydration strategy and continue to deliver the plans for improving nutrition and catering
Spiritual care Refresh the spiritual care policy and update spiritual care link nurses. Monitoring referrals and activity across care groups.
Bereavement care Develop and deliver a bereaved relatives experience survey.
End of life care Continue to implement the trust’s end of life care strategy
Healing environment Set the direction of the estates and maintenance strategy with clear priorities for improving ward/department environments
Assurance Involve patients, members of the public and governors in reviewing the quality of the trust’s clinical services using tools such as the Clinical Accreditation Scheme and 15 Steps model.
Organisational and Personal Engagement
Implement a programme using the IPSOS MORI Patient Experience Self Assessment Tool at many different staff group and team levels, in order to see rapid improvement in the culture and behaviours which contribute to a positive patient experience.

10
How we will deliver, monitor and report this strategy
Other trust strategies/policies with direct links to this patient experience strategy include:
- Trust 2020 Vision - Patient and Public Involvement Strategy - Patient Safety Strategy - Infection Prevention Strategy - Quality Governance Strategy - Nutrition & Hydration Strategy (under development) - End of Life Care Strategy - Spiritual care policy - Privacy, dignity and same sex accommodation policy - Workforce and Education Strategies
The nursing strategy is currently under development and will incorporate the DoH Chief Nurse’s vision and strategy for nursing (6C’s model), a draft summary of which can be found in appendix F.
Delivery of the strategy Annual Priorities for Patient Experience: The annual priorities for improving patient experience are set via the trust’s Patient Improvement Framework. Following analysis of learning from complaints and patient feedback, from consultation with patients and members of the public and in review with our commissioners, 5 top priorities for patient experience are set with associate improvement measures and targets. The annual plan for improving patient experience will incorporate the PIF priorities and other work streams as indicated in the strategy. Key groups and committees responsible for delivering this strategy: The Trust’s Quality Governance Steering Group (QGSG) is responsible on behalf of the Trust Executive Committee and ultimately Trust Board, for monitoring the delivery of this strategy. The trust’s Patient Experience Steering Group has been established for over 4 years and is responsible for the delivery of this strategy. It reports directly to the trust Quality Governance Steering group, and includes patient representation. A number of sub groups are established which report to this group on specific work streams. These include:
• Customer Care Group
• Nutrition Steering Group
• Environment Group
• End of Life Care Group
• Essence of Care Group
• Clinical Accreditation Scheme and Clinical Quality Dashboard Working Group Divisions and care groups each monitor local delivery of patient experience targets through their own boards and governance groups, and report progress via their QGSG reports. Patient Improvement Framework (PIF) plans are refreshed annually according to the resetting of the top 5 priorities for patient experience.

11
Staff Roles and Responsibilities We believe that each staff member, no matter what role they play, has core responsibilities for delivering a positive patient experience. We also expect staff to let us know when they feel unable to do this, either due to personal circumstances or because of lack of resources or inadequate systems and processes.
Monitoring Our Clinical Quality Dashboard provides clinical teams with information about key safety, experience, operational and staffing measures. Staff display results form the CQD in their clinical areas to keep colleagues, patients and members of the public up to date about their performance.
Reporting All patient experience metrics and KPIs are reported quarterly to PESG, QGSG, TEC and Trust Board. Appendix C details all of the measures currently in use for patient experience at the time of writing. Delivery of the Patient Experience Strategy is reported:
- annually in the Trust Annual Report - annually in the Trust Quality Account - quarterly in the in-depth patient experience report to Quality Governance Steering
Group, TEC and trust board. - Monthly at ward level in CQD displays
- Quarterly at divisional performance reviews
Strategy launch plans and next steps This strategy has undergone wide consultation and refinement with ALL key internal and external stakeholders. A formal launch plan is in place. This includes the use of leaflets and posters informing trust staff, patients, family and carers, as well as presentations at core brief and other groups, special publicity and media events and information on the trust’s website. We do hope you have enjoyed reading about our determined plans to improve patient experience. If you have any feedback on any aspect of this document, please contact the strategy author: Julia Barton, Associate Director of Nursing & Patient Experience [email protected] or via 023 8079 6179
EExxtteerrnnaall AAssssuurraannccee - CQC Regulation & Inspections - Commissioner Visits - PPI Visits e.g. HealthWatch
- Members Council Visits
- SHA Visits -- Delivery of the PCT Quality Contract & CQUINs
-NHSLA
PPaattiieenntt//CCaarreerr
FFeeeeddbbaacckk
- Surveys - Listening Clinics - Comment Cards - Patient Panels - Online Feedback - Email Feedback - Pals
- Complaints - NHS Choices
MMaannaaggeemmeenntt && LLeeaaddeerrsshhiipp
-Policies and guidelines -Clinical management structures -Appraisal and staff experience -Supervision -Whistle blowing policy/procedures
IInntteerrnnaall AAssssuurraannccee
- Annual Priorities (PIF)
- Patient Experience and PPI Strategies
- Patient Safety Strategy -Clinical Quality Dashboard
-Trust board reports and scrutiny
- Director of Nursing & Medical Director Exec walkabouts
-Matrons weekly peer reviews & night visits
-Board visits to clinical areas
-Board performance reviews
-(Serious) incident reporting & reviews
AAuuddiitt && MMoonniittoorriinngg
-Clinical effectiveness annual audit programme
-Essence of Care Standards & Audit programme
-Catering Audits -MUST audits -Cleaning Audits -Acuity Audits -VTE Audits -Infection Control audits and accreditation
- External Accreditation -Internal Accreditation - Observations of care

13
Appendix A: Key policy, regulatory and legislative documents which have informed this strategy
NHS Constitution (2010) (2012 draft revisions for consultation)
The Constitution describes the purpose, principles and values of the NHS and illustrates what staff, patients and the public can expect from the service. Since the Health Act came into force in January 2010, service providers and commissioners of NHS care have had a legal obligation to take the Constitution into account in all their decisions and actions. This strategy adheres to the NHS Constitution which sets out the common principles and values, which inform how the NHS is delivered, through establishing the rights, pledges and responsibilities for patients and staff.
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_113645.pdf
Equity and excellence: Liberating the NHS (2010)
and the
NHS Act (2012)
The NHS White Paper, Equity and Excellence: Liberating the NHS, sets out the Government's long-term vision for the future of the NHS. The vision seeks to:
• put patients at the heart of everything the NHS does;
• focus on continuously improving those things that really matter to patients - the outcome of their healthcare; and
• empower and liberate clinicians to innovate, with the freedom to focus on improving healthcare services
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_117794.pdf
Institute of Medicine’s (2001) 6 Domains of Quality
The Institute of Medicine’s widely accepted definitions of quality and patient centred care seem to say everything we believe to be important about providing high quality patient experience here at UHS
Safe, Effective, Timely, Efficient, Equitable & Patient Centred:
• Care delivered with compassion, empathy and responsiveness to individual patient needs, values and expressed preferences
• Care that is coordinated and integrated
• Care/treatment supported by the provision of information, communication and education
• Care which always seeks to achieve physical comfort
• Care underpinned by the provision of emotional support to relieve fear and anxiety
• The appropriate involvement of family and friends
http://www.talkingquality.ahrq.gov/content/create/sixdomains.aspx
2012/13 NHS Outcomes Framework, Domain 4: Quality Contract, CQUIN and QIPP
Ensuring that people have a positive experience of care
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_131723.pdf
Care Quality Commission Standards (2010)
The CQC quality standards detail what providers should do to comply with the section 20 regulations of the Health and Social Care Act 2008. Many of these standards in various domains directly relate to patient experience and are reflected in this strategy.
http://www.cqc.org.uk/sites/default/files/media/documents/gac_-_dec_2011_update.pdf
NICE Clinical Guideline 138 Patient Experience in Adult NHS Services (February 2012)
This clinical guidance offers evidence-based advice on ensuring a good
experience of care for people who use adult NHS services.
We have also published a quality standard describing high-quality care for
patients using adult NHS services in England.
http://www.nice.org.uk/nicemedia/live/13668/58283/58283.pdf
Monitor’s Compliance Framework 2012/13
Regulatory requirements for Foundation Trust, including inclusion of Annual Quality Account, Annual Plan and Report. Makes direct reference to patient involvement being at the core of trust quality strategies.
http://www.monitor-nhsft.gov.uk/sites/default/files/Compliance%20Framework%2030%20March%202012%20FINALv1.3.pdf http://www.monitor-nhsft.gov.uk/sites/default/files/Quality%20Governance%20Framework%20July%202010.pdf

14
High quality care for all (Darzi; DoH2008) (Next Stage review)
The vision this report sets out is of an NHS that gives patients and the public
more information and choice, works in partnership and has quality of care at
its heart – quality defined as clinically effective, personal and safe.
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_085828.pdf
The Kings Fund Point of Care Programme
Useful reports include: • Seeing the Person in the patient (Kings Fund 2009) • Making shared decision-making a reality: No decision about me without
me. (Kings Fund 2011) • Patient Choice: How patients choose and providers respond (Kings
Fund 2010) • Patient Preferences Matter: Stop the silent misdiagnosis (Kings Fund
2012) • Continuity of Care for Older Hospital patients (Kings Fund 2012)
http://www.kingsfund.org.uk/publications/the_point_of_care.html http://www.kingsfund.org.uk/publications/nhs_decisionmaking.html http://www.kingsfund.org.uk/publications/patient_choice.html http://www.kingsfund.org.uk/publications/patients_preferences.html http://www.kingsfund.org.uk/publications/continuity_of_care.html
Essence of Care (DoH 2010) The 12 essence of care benchmark standards for fundamental care were refreshed in 2010. The trust is currently piloting a trust wide version of the standards as part of its new Clinical Accreditation scheme
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/@ps/documents/digitalasset/dh_119978.pdf
NHS Equality Delivery System The EDS is designed to help NHS organisations improve equality performance, embed equality into mainstream NHS business and to help organisations meet their public sector
equality duties. http://www.eastmidlands.nhs.uk/about-us/inclusion/eds/ http://healthandcare.dh.gov.uk/equality-delivery-system/
DoH Framework for Patient Experience (2012)
In October 2011 the NHS National Quality Board (NQB) agreed on a working definition of patient experience to guide the measurement of patient experience across the NHS. This framework outlines those elements which are critical to the patients’ experience of NHS Services. See appendix E for details.
http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/@dh/@en/documents/digitalasset/dh_132788.pdf
Friends and Family Test (DoH, 2012)
Guidance on Implementing the Friends and Family Test (net promoter Score) for 2013-14.
https://www.wp.dh.gov.uk/publications/files/2012/10/NHS-Friends-and-Family-Test-Implementation-Guidance-v2.pdf
NHS Mandate (2012) The first Mandate between the Government and the NHS Commissioning Board, setting out the ambitions for the health service for the next two years,The NHS Mandate is structured around five key areas where the Government expects the NHS Commissioning Board to make improvements:
• Preventing people from dying prematurely
• Enhancing quality of life for people with long-term
conditions
• Helping people to recover from episodes of ill health or
following injury
• Ensuring that people have a positive experience of care
• Treating and caring for people in a safe environment and
protecting them from avoidable harm.
https://www.wp.dh.gov.uk/publications/files/2012/11/mandate.pdf

15
Appendix B: Individual, Team & Organisational factors affecting patient experience( Goodrich & Cornwall, 08) Factors Affecting Patient Experience at the Individual Level
Organisational Human
Staff Staff Patient
Education, training & qualifications Morale
Clinical need
Induction/preparation Experience Mental & physical capacity
Job description Health Status Ability to speak for self
Accountability Tiredness, stress, well-being Spoken English
Delegated responsibilities Professional and personal attitudes & values
Age
Permanent v. temporary status Support Social Status
Support Active family or other support
Supervision
Appraisal
Spoken English
Depression, Anxiety or fear
Factors affecting patient experience at team level
Organisational Human
Performance management and measures Leadership
Governance and Accountability Morale
Division of labour Communication
Clarity/conflicts over job boundaries Experience in team
Access to IT Flexibility
Operating procedures Team ethos and values
Record keeping
Skill mix
Deployment
Capacity management – match between supply and demand
Stability of staffing- e.g. vacancies and use of bank, agency and locums
Priorities
Factors at Organisational Level needed to protect patients (Adapted from HCC 2008, in Goodrich and Cornwall, 2008))
Technical Human
Set Direction Open culture in which staff are able to voice
concerns
Ensure delivery Culture for effective team-working
Maintain governance Enabling and supportive leadership & management styles
Have adequate information about trends and potential issues at ward/specialist level
Expect and encourage professional staff to speak out on behalf of patients

16
Appendix C: Metrics and Performance Indicators for Patient Experience
National and Local Surveys
• Friends and Family Test (FFT)
(2013/14)
• Accident and Emergency
Department Survey
• National Inpatients Survey
• National Cancer Patient
Experience Survey
• Maternity Patient Experience
Survey
• Discharge survey
• Bereaved relatives survey
• National Outpatient Survey
2011/12: progress against Plan
• Children And Young People local
real-time survey
• Stroke inpatient real-time survey
• Diabetes – national survey (audit)
• Carers survey
• Staff survey
Patient Feedback KPIs: What are patients telling us about
our services?
• Overall satisfaction with care
• Overall satisfaction with care for older people) (over 65s)
• Recommend hospital to family and friends (FFT)
• Privacy and Dignity
• Noise at night from staff
• Trust and confidence in nurses
• National and Local CQUINs for Patient Experience
• Complaints
o Number received
o Response Times
o Number returned dissatisfied
o Referrals to the Ombudsman
• Concerns (PALS)
o Number received resolved by next working day
o Number received not resolved by next working day
o PALS enquiries
• Communication – primary and secondary complaints
received
• Staff Attitudes – primary and secondary complaints received
Patient Experience Improvement KPIs: How are
we improving our services and learning from
patient feedback?
• Nutrition, hydration and catering
o MUST screening
o MUST Care Plans in place
o Mealtimes assistance
o Hospital food
o Mealtimes assistance
o Protected mealtimes in place
• Same sex accommodation
o Non clinically justified breaches
o Clinically Justified breaches
o Patients perceptions of sharing
• Vulnerable Adults
o CQUIN for dementia
o Safeguarding Adult Alerts
o DOLS Breaches
• Clinical accreditation scheme
o Number of wards reviewed
o Number of wards accreditated

17
Appendix D: Patient experience in adult NHS services: NICE Quality Standard (2012)
The NICE quality standard for patient experience defines best practice within this topic area. It provides specific, concise
quality statements, measures and audience descriptors to provide the public, health and social care professionals,
commissioners and service providers with definitions of high-quality care. There are 14 quality statements which
comprise the standard. The table below details the standard and the structure, process and outcome measures related
to this. Mapping to the UHS Patient Experience Strategy 4 themes is included.
Standard 1:
Patients are treated
with dignity, kindness,
compassion, courtesy,
respect,
understanding and
honesty.
UHS = RESPECT
Structure
Evidence of local arrangements to provide guidance to staff on how to treat patients with
dignity, kindness, compassion, courtesy, respect, understanding and honesty.
Outcome
Evidence from patient experience surveys and feedback that patients feel they have been
treated with dignity, kindness, compassion, courtesy, respect, understanding and honesty.
Standard 2:
Patients experience
effective interactions
with staff who have
demonstrated
competency in
relevant
communication skills.
UHS = INFORM
Structure
a) Evidence of local arrangements to ensure that annual appraisals or performance
assessments of staff include mentoring for and evaluating compliance with the NICE
guidance on patient experience.
b) Proportion of staff involved in providing NHS services who have compliance with the NICE
guidance on patient experience examined at their annual appraisal or performance
assessment.
Numerator - the number of staff in the denominator who have compliance with the NICE
guidance on patient experience examined at their annual appraisal or performance
assessment.
Denominator - the number of staff involved in providing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients feel staff
communicated with them in a clear and understandable way.
Standard 3.
Patients are
introduced to all
healthcare
professionals
involved in their care,
and are made aware
of the roles and
responsibilities of the
members of the
healthcare team.
UHS = INFORM
Structure
Evidence of local arrangements to ensure that patients are introduced to all healthcare
professionals involved in their care, and are made aware of the roles and responsibilities of
the members of the healthcare team.
Outcome
Evidence from patient experience surveys and feedback that patients were introduced to all
healthcare professionals involved in their care, and were made aware of the roles and
responsibilities of the members of the healthcare team.

18
Standard 4.
Patients have
opportunities to
discuss their health
beliefs, concerns and
preferences to inform
their individualised
care.
UHS = LISTEN
Structure
Evidence of local arrangements to ensure that patients have opportunities to discuss their
health beliefs, concerns and preferences, and these inform their individualised care.
Process
Proportion of patients given the opportunity to discuss their health beliefs, concerns and
preferences.
Numerator - the number of patients in the denominator who were given the opportunity to
discuss their health beliefs, concerns and preferences.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients feel they had
opportunities to discuss their health beliefs, concerns and preferences, and these informed
their individualised care.
Standard 5.
Patients are
supported by
healthcare
professionals to
understand relevant
treatment options,
including benefits,
risks and potential
consequences.
UHS = LISTEN &
INFORM
Structure
Evidence of local arrangements to ensure that healthcare professionals support patients to
understand relevant treatment options, including benefits, risks and potential consequences.
Outcome
Evidence from patient experience surveys and feedback that patients were supported by
healthcare professionals to understand relevant treatment options, including benefits, risks
and potential consequences.
Standard 6.
Patients are actively
involved in shared
decision making and
supported by
healthcare
professionals to
make fully informed
choices about
investigations,
treatment and care
that reflect what is
important to them.
UHS = LISTEN
Structure
a) Evidence of local arrangements to ensure that patients are actively involved in shared
decision making, including using the most effective way of communicating to maximise the
patient's participation in decisions.
b) Evidence of local arrangements to ensure that patients are supported to make informed
choices using risk communication and decision support, such as patient decision aids.
c) Evidence of local arrangements to ensure that information provided to facilitate shared
decision making is evidence-based, understandable and clearly communicated.
Process
a) Proportion of patients who were asked about any issues that may prevent them being
actively involved in decisions about their care.
Numerator - the number of patients in the denominator who were asked about any issues that
may prevent them being actively involved in decisions about their care.
Denominator - the number of patients accessing NHS services.
b) Proportion of patients supported to use an evidence-based patient decision aid.
Numerator - the number of patients in the denominator supported to use an evidence-based
patient decision aid.

19
Denominator - the number of patients accessing NHS services for whom there is a relevant
evidence-based decision aid.
Outcome
a) Evidence from patient experience surveys and feedback that patients found that the
information provided to facilitate shared decision making was understandable and clearly
communicated.
b) Evidence from patient experience surveys and feedback that patients feel able to make
decisions that reflect what is important to them.
Standard 7.
Patients are made
aware that they have
the right to choose,
accept or decline
treatment and these
decisions are
respected and
supported.
UHS = LISTEN
Structure
Evidence of local arrangements to ensure that patients are made aware of their right to
choose, accept or decline treatment and that these decisions are respected and supported.
Process
Proportion of patients made aware of their right to choose, accept or decline treatment.
Numerator - the number of patients in the denominator made aware of their right to choose,
accept or decline treatment.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients know about their right
to choose, accept or decline treatment and feel that their decisions were respected and
supported.
Standard 8. Patients
are made aware that
they can ask for a
second opinion.
UHS = LISTEN
Structure
Evidence of local arrangements to ensure that patients are made aware that they can ask for
a second opinion.
Process
Proportion of patients made aware that they can ask for a second opinion.
Numerator - the number of patients in the denominator made aware that they can ask for a
second opinion.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients know that they can ask
for a second opinion.
Standard 9.
Patients experience
care that is tailored to
their needs and
personal preferences,
taking into account
their circumstances,
Structure
Evidence of local arrangements to ensure that care is tailored to patients' needs and personal
preferences, taking into account their circumstances, their ability to access services and their
coexisting conditions.
Process

20
their ability to access
services and their
coexisting conditions.
UHS = RESPECT
The proportion of patients with care tailored to their needs and preferences, taking into
account their circumstances, their ability to access services and their coexisting conditions.
Numerator - the number of patients in the denominator who have care tailored to their needs
and preferences, taking into account their circumstances, their ability to access services and
their coexisting conditions
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that care was tailored to the patient's
needs and personal preferences, taking into account their circumstances, their ability to
access services and their coexisting conditions.
Standard 10.
Patients have their
physical and
psychological needs
regularly assessed
and addressed,
including nutrition,
hydration, pain relief,
personal hygiene and
anxiety.
UHS = CARE
Structure
Evidence of local arrangements to ensure that patients have their physical and psychological
needs regularly assessed and addressed.
Process
Proportion of patients who have their physical and psychological needs regularly assessed
and addressed.
Numerator - the number of patients in the denominator who have their physical and
psychological needs regularly assessed and addressed.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients feel their physical and
psychological needs were regularly assessed and addressed.
Standard 11.
Patients experience
continuity of care
delivered, whenever
possible, by the same
healthcare
professional or team
throughout a single
episode of care.
UHS = INFORM
& CARE
Structure
Evidence of local arrangements to ensure continuity of care and that, whenever possible,
patients see the same healthcare professional or team throughout a single episode of care.
Process
Proportion of patients seeing the same healthcare professional or team throughout a single
episode of care.
Numerator - the number of patients in the denominator seeing the same healthcare
professional or team throughout a single episode of care.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that, whenever possible, patients
saw the same healthcare professional or team throughout a single episode of care.
Standard 12.
Patients experience
coordinated care with
clear and accurate
information exchange
Structure
Evidence of local arrangements to support coordinated care through clear and accurate
information exchange between relevant health and social care professionals.

21
between relevant
health and social
care professionals.
UHS = INFORM
Outcome
Evidence from patient experience surveys and feedback that patients feel that information
about their care was shared clearly and accurately between relevant health and social care
professionals.
Standard 13.
Patients´
preferences for
sharing information
with their partner,
family members
and/or carers are
established,
respected and
reviewed throughout
their care.
UHS = INFORM
Structure
Evidence of local arrangements to ensure that patients' preferences for sharing information
with partners, family members and/or carers are established, respected and reviewed
throughout their care.
Process
Proportion of patients whose preferences for sharing information with partners, family
members and/or carers are established, respected and reviewed throughout their care.
Numerator - the number of patients in the denominator whose preferences for sharing
information with partners, family members and/or carers are established, respected and
reviewed throughout their care.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients' preferences for sharing
information with partners, family members and/or carers were established, respected and
reviewed throughout their care.
Standard 14.
Patients are made
aware of who to
contact, how to
contact them and
when to make
contact about their
ongoing healthcare
needs.
UHS = INFORM
Structure
Evidence of local arrangements to ensure that patients are made aware of who to contact,
how to contact them and when to make contact about their ongoing healthcare needs.
Process
Proportion of patients made aware of who to contact, how to contact them and when to make
contact about their ongoing healthcare needs.
Numerator - the number of patients in the denominator made aware of who to contact, how to
contact them and when to make contact about their ongoing healthcare needs.
Denominator - the number of patients accessing NHS services.
Outcome
Evidence from patient experience surveys and feedback that patients know who to contact,
how to contact them and when to make contact about their ongoing healthcare needs.

22
Appendix E: DoH Patient Experience Framework (Feb 2012)

23
Appendix F: A new national vision and strategy for nurses, midwives and care-
givers (DRAFT)

24
Version: FINAL
Status: 2012 refresh of 2008-2011 Patient Experience Strategy
Approved by: Trust Board December 2012
Date Approved: 19th December 2012
Author: Associate Director of Nursing & Patient Experience
Executive Leads Director of Nursing & OD/Medical Director
Name of Responsible
Committee
Patient Experience Steering Group
Date Issued: February 2013
Review Date: January 2016