pathology of hiv & opportunistic...
TRANSCRIPT

Integrated Course
Microbiology & Pathology
Pathology
of
HIV & Opportunistic
infections
Jaroslava Dušková
Inst. Pathol. ,1st Med. Faculty, Charles Univ. Prague

Neuroimmunoendocrine
Regulations
Adrenals
Immune cells
TNF
IL-6
IL-1
Glucocorticoids
CRF
ACT
H
IL-1 neuronal
synapses
n.vagus
+corticotherapy !

The reflex arc of axon reflex has neither an
integration center nor any synapse
Def.: a reflex resulting from
a stimulus applied to one
branch of a nerve, which
sets up an impulse that
moves
centrally to the point of
division of the nerve, where
it
is reflected down the other
branch to the effector organ
• Blood vessels, sweating
glands and mast cells are
most important effectors of
axon reflex in the skin
Mevlut YAPRAK: The axon reflex. Neuroanatomy (2008) 7: 17–19

Procaccini C. et al.: Neuro-endocrine networks controlling immune system in health and disease.
Frontiers in Immunology , 2014, 5, 143,1-10
Neuroimmunoendocrine Regulations

Pathology of AIDS
Direct HIV effect
Opportune infections
Neoplastic processes

HIV-Related Lymphadenopathy – HIVRL
persistent generalized HIVRL >3mth duration
absence of other agent causing lymphadenopathy
histological evidence of follicular hyperplasia
BIOPSY
dif. dg.: HIV-Related Lymphadenopathy – HIVRL
infection
lymphoma
Kaposi sarcoma

ARC enlarged germinal centre

ARC hypercellular parafollicular zone

sclerosed & collapsed lymphoid follicle AIDS

Angiofollicular hyperplasia AIDS

Neuropathology of AIDS
Direct HIV effect HIV encephalitis
leucoencephalopathy
vacuolar myelopathy
neuropathy
myopathy
vasculitides, AIDS-Dementia complex, HIV-associated progressive encephalopathy of childhood

Portals of Entry to CNS
hematogenous (pyemia, sepsis, viremia)
directly
via plexus chorioideus
local source
directly (trauma)
bone melting (sinusitis, otitis)
vv. emissariae
along nerves (filla olfactoria)


HIV
encephalitis

HIV encephalitis

Pathology of AIDSOpportune infections
parasites: toxoplasmosis
mycoses, mycobacteria, spirochetes: Aspergillus, Candida, Cryptococcus
Mycobacterium avium intracellulare
Mycobacterium tuberculosis
Treponema pallidum
viral Cytomegalovirus
Herpes simplex
Herpes zoster
Polyoma PML
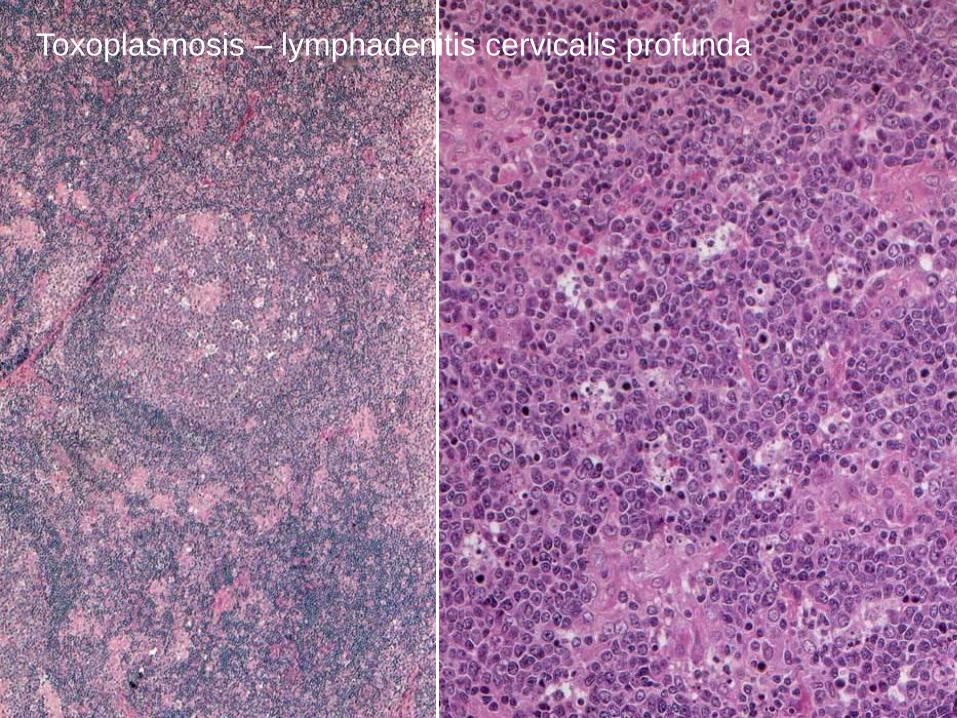
Toxoplasmosis – lymphadenitis cervicalis profunda

Candidosis

Candidosis oesophagi

Intertrigo

Toxoplasmosis cerebri cyst

Toxoplasmosis

Toxoplasmosis stereotactic brain biopsy

methenamine silver (sputum)
Cryptococcosis
polychrome (CSF)

Cryptococcosis
PAS


Candidosis vaginae


Candidosis - sputum

Candidosis – BAL polychrome // methenamine silver)

Aspergilosis pulmonum

TBC pulmonum cavernosa

Aspergillosis sputum
fruiting head
polychrome

Aspergilloma

Aspergillosis BAL ( methenamine silver)


Mucor BAL (polychrome)

Chinen K, Tokuda Y, Sakamoto A, Fujioka Y.:
Fungal infections of the heart:
a clinicopathologic study of 50 autopsy cases.
Pathol Res Pract. 2007;203(10):705-15.
cardiac fungal infection (CFI) incidence is increasing
a grim prognosis
an early diagnosis and aggressive therapy
among a total of 4396 autopsy cases 50 CFI patients (1.1%)
32 males and 18 females - mean age of 65.5 years
underlying diseases for CFI included solid malignant neoplasms (n=23), hematologic disorders (n=10), chronic renal diseases (n=7), liver diseases (n=5), diabetes mellitus (n=5), and other
none of the patients was diagnosed to have CFI antemortem!
most patients (n=45) demonstrated multi-organ fungal infections with myocardial involvement
causative pathogens were Candida (n=36), Aspergillus (n=9), Mucor (n=4), and Cryptococcus (n=1).

Progressive Multifocal
Leucoencephalopathy
PME
luxol blue

Cytomegalovirosis

CMV

Herpes anogenitalis

Herpes

Herpes labialis

B8467/12
Gingivostomatitis herpetica,
obj. 4x
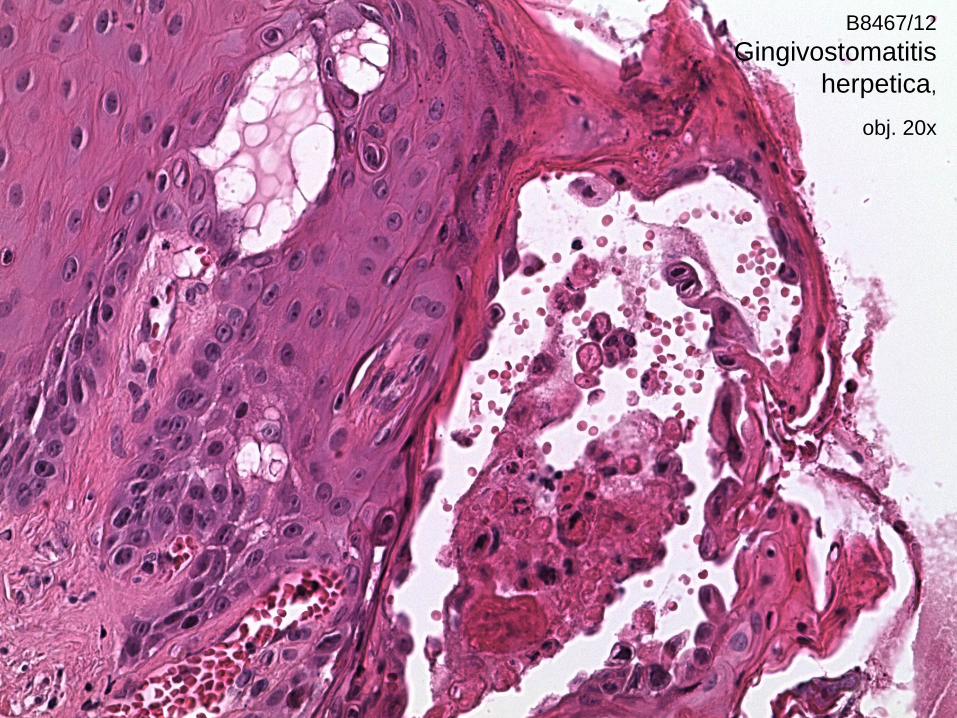
B8467/12
Gingivostomatitis
herpetica,
obj. 20x

Mycobacterium avium intracellullare

Bendayan D, Litman K, Hendler A, Polansky V.: Liver tuberculosis
in an HIV patient: diagnosis and management.Indian J Tuberc. 2010 Jul;57(3):152-6.
Pulmonary and Tuberculosis Department, Shmuel Harofe Hospital, Beer Yaakov, Israel
Hepatic involvement is common in miliary and extra-pulmonary
tuberculosis but is usually clinically silent.
A patient that presented with prolonged fever and hepatomegaly.
Liver biopsy revealed non-necrotizing granulomas that led in turn to the
diagnosis of generalized tuberculosis and HIV infection.
Diagnosis of hepatic tuberculosis requires a high degree of suspicion
especially in AIDS patients who show atypical presentations.
Good results have been obtained with the four drug regimen.

Pneumocystis jiroveci pneumonia

„Snowball“ with
icicle effect
Pneumocystis
jiroveci

Trichomoniasis

Steven I. Hajdu, MD, FIAC
Memorial Sloan-Kettering
Cancer Center, USA
(dressed in three layers of
protective garbs to do an
AIDS autopsy)

Most Common Malignant
Neoplasms in AIDS Patients
Kaposi sarcoma HHV 8
malignant lymphoma HHV 8, EBV
(undiff. large B cell extranodal)
squamous cell carcinoma HPV

Kaposi´s sarcoma KSHV, HHV-8
Sarcoma idiopathicum multiplex haemorrhagicum Kaposi
Four
forms • Classic (not HIV ass), Ashkenazy Jews, old,
localized
• Endemic African KS , young and children,
LN and viscera spread, aggressive
• Transplantation ass. LN and viscera spread,
aggressive
• HIV infected LN and viscera spread, aggressive


Sarcoma Kaposii
HHV-8

Sarcoma Kaposii

Kaposi sarcoma

Kaposi sarcoma

dr. Moritz Kaposi
• dr. Moritz Kohn born in
Kaposvar Hungary 1837
• associate of Prof. Hebra 1865
• dating Martha Hebra 1867
• changing his name to Kaposi
1871
• changing his religion 1872
• described sarcoma idiopathicum
multiplex haemorrhagicum 1872
• married Martha Hebra 1872
• died Vienna 1902

Schulz TF.:
The pleiotropic effects
of Kaposi's sarcoma herpesvirus.
J Pathol. 2006 Jan;208(2):187-98.
Kaposi's sarcoma herpesvirus HHV8
an essential factor in the pathogenesis of – Kaposi's sarcoma (KS)
– multicentric Castleman's disease (MCD)
– primary effusion lymphoma (PEL)
– an occasional involvement in bone marrow hypoplasia
haemophagocytic syndrome
Other disease associations are unconfirmed or controversial.
HHV8-associated disease is of particular importance
in immunosuppressed individuals, in particular in patients with HIV infection and transplant recipients.

nH ML (colon and mesenterium involved)

Neuropathology of AIDS -
tumours
Primary cerebral lymphoma
mostly B type
often multicentric
EB virus proven in some
Kaposi sarcoma (HHV8 related)
exceptionally meta to CNS

Primary cerebral B cell lymphoma

Well Differentiated Squamous Cell Carcinoma In an AIDS Patient

SIL H

Huppmann AR, Orenstein JM.: Opportunistic disorders of the
gastrointestinal tract in the age of highly active
antiretroviral therapy.Hum Pathol. 2010 Dec;41(12):1777-87.
Department of Pathology, George Washington University Medical Center, Washington, DC 20037, USA.
Since the 1996 advent of highly active antiretroviral therapy (HAART) the incidence of most opportunistic disorders in the developed world has declined but not disappeared.
The number of new yearly HIV infections (about 55,000) and the total number of US infections (more than 1.1 million) remain very significant.
Opportunistic GI disorders were diagnosed in 442 endoscopies performed since 1996 as before, but at about one half the rate. – The esophagus - Candida.
– Helicobacter pylori - the most common gastric infection
– The small bowel still showed cytomegalovirus (CMV), cryptosporidia, and Mycobacterium avium complex (MAC) infections.
– Large bowel infections were CMV, cryptosporidiosis, MAC, and spirochetosis
– Cases of adenovirus, bacterial colitis, Kaposi sarcoma, and lymphoma were still diagnosed.

F68, CLL biopsy in an immunocompromised patient
Two rapidly growing tumours on the right
upper and lower extremity.
Excisions: 33x18x22 mm and 23x14x14 mm

Bone marrow July 2014 Chronic Lymphatic Leukemia
HE PAX 5

Liver November 2016 Chronic Lymphatic Leukemia
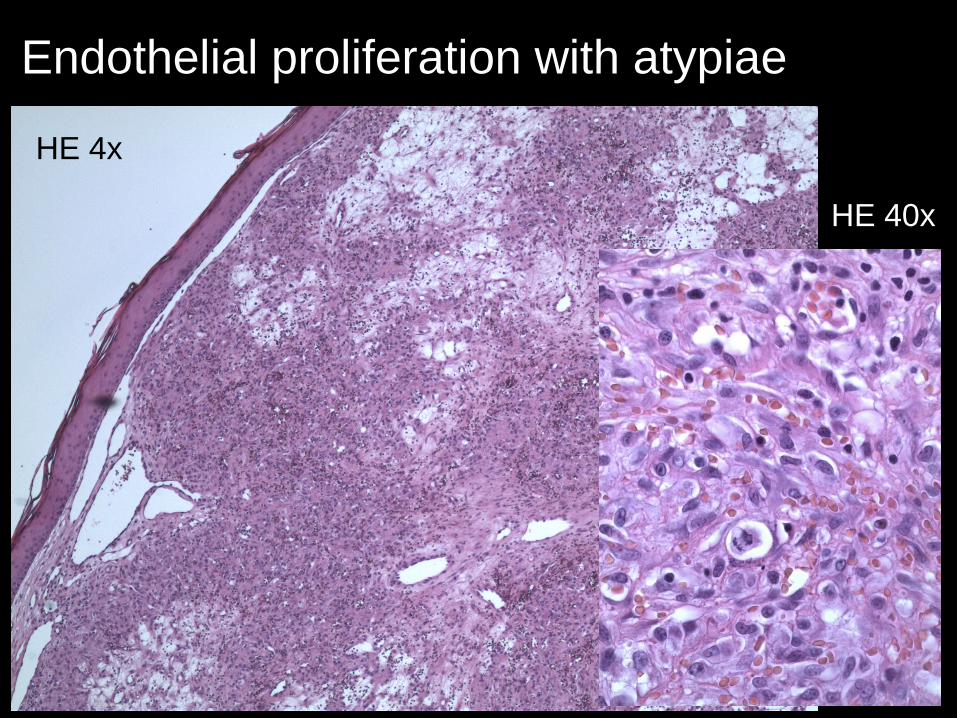
Endothelial proliferation with atypiae
HE 4x
HE 40x

Endothelial markers positive
CD 31
ERG 1

ImmunohistochemistryKSHV (HH8) -
Ki-67 (MIB1) 10%

Warthin Stary impregnation 40x

Biopsy report
Florid vascular proliferations with
impregnation positive rods
Most probably bacillary angiomatosis
Reactive proces caused by bacteria
Bartonella sp.
PSEUDOTUMOUR !!!
