patho lab trans -butch
TRANSCRIPT
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 1/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 1 of 6
LEXI-ADI-GILLIAN-BUTCH
OUTLINEI. Gross Specimen
a. Renal Cell Carcinomab. Wilm’s Tumor c. Renal Dysplasia
d. Chronic Pyelonephritise. Nephrolithiasisf. Kidney Hydronephrosisg. Benign Prostatic hyperplasiah. Transitional / urothelial cell
carcinomaII. Microscopic Specimen
a. Chronic protatitisb. NPHc. Prostatic adenocarcinomad. Papillary urothelial carcinomae. Chronic cyst itis
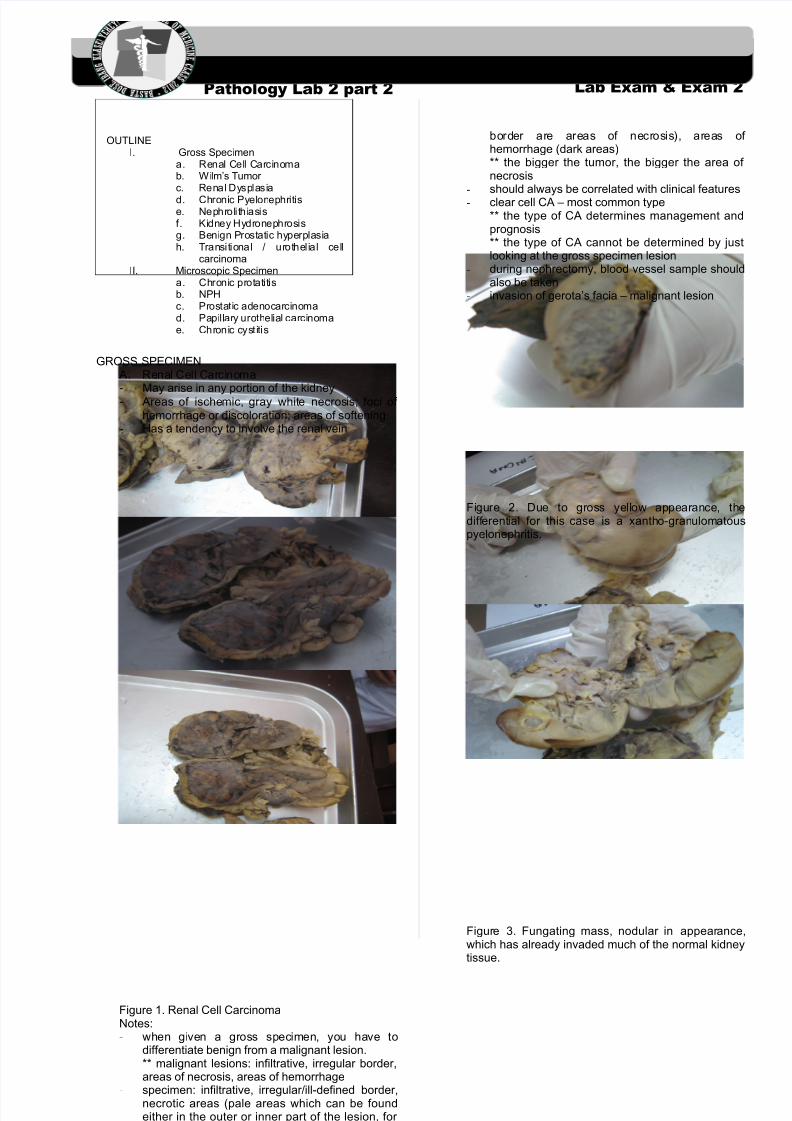
GROSS SPECIMENA. Renal Cell Carcinoma-
May arise in any portion of the kidney- Areas of ischemic, gray white necrosis; foci of hemorrhage or discoloration; areas of softening
- Has a tendency to involve the renal vein
Figure 1. Renal Cell CarcinomaNotes:- when given a gross specimen, you have to
differentiate benign from a malignant lesion.** malignant lesions: infiltrative, irregular border,areas of necrosis, areas of hemorrhage
- specimen: infiltrative, irregular/ill-defined border,necrotic areas (pale areas which can be foundeither in the outer or inner part of the lesion, for the gross specimen shown in the lab the outer
border are areas of necrosis), areas of hemorrhage (dark areas)** the bigger the tumor, the bigger the area of necrosis
- should always be correlated with clinical features
-clear cell CA – most common type** the type of CA determines management andprognosis** the type of CA cannot be determined by justlooking at the gross specimen lesion
- during nephrectomy, blood vessel sample shouldalso be taken
- invasion of gerota’s facia – malignant lesion
Figure 2. Due to gross yellow appearance, thedifferential for this case is a xantho-granulomatouspyelonephritis.
Figure 3. Fungating mass, nodular in appearance,which has already invaded much of the normal kidneytissue.
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 2/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 2 of 6
LEXI-ADI-GILLIAN-BUTCH
Figure 4. The tumor has already spread to theperirenal fat.
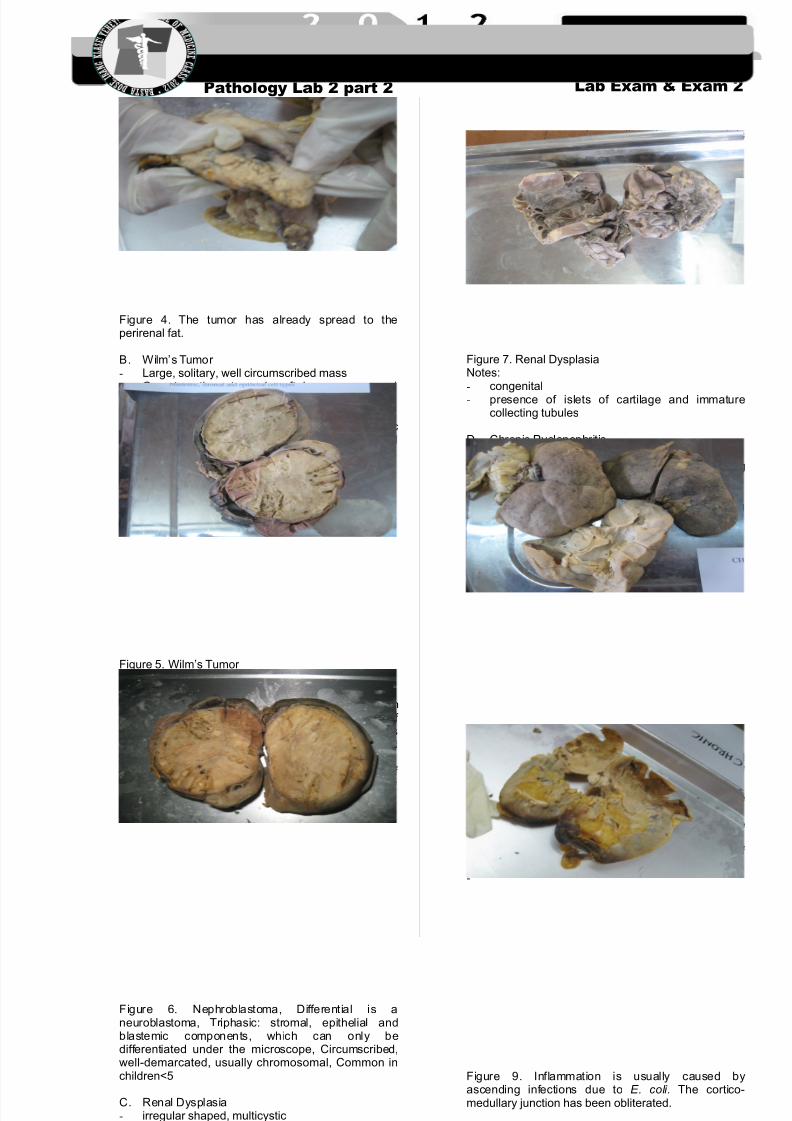
B. Wilm’s Tumor - Large, solitary, well circumscribed mass- On cut sections, tumor is soft, homogenous, and
tan to gray with occasional foci of hemorrhage,cyst formation and necrosis
- On microscopic sections, classic triphasiccombination of blastemic stromal and epithelialcell types
Figure 5. Wilm’s Tumor Notes:- common in children- specimen: smooth, homogenous lesion
occupying the entire renal parenchyma, foci of hemorrhage (minimal areas of hemorrhage ascompared to the renal cell CA specimen) andcyst
- may be triphasic (classical type): composed of
blastema, epithelial cells, stroma; biphasic; or anaplastic
Figure 6. Nephroblastoma, Differential is aneuroblastoma, Triphasic: stromal, epithelial andblastemic components, which can only bedifferentiated under the microscope, Circumscribed,well-demarcated, usually chromosomal, Common inchildren<5
C. Renal Dysplasia- irregular shaped, multicystic- cysts vary in size
- due to an abnormality in metanephricdifferentiation
Figure 7. Renal DysplasiaNotes:- congenital
- presence of islets of cartilage and immaturecollecting tubules
D. Chronic Pyelonephritis- kidneys are irregular scarred- coarse, discrete, corticomedullary scar overlying
in a dilated, blunted or deformed calyx- kidneys are smaller than usual- ureter is dilated and thickened, a finding
consistent with chronic vesicoureteral reflux
Figure 8. Chronic PyelonephritisNotes:- specimen: granular surface with scarring, small
kidney, blunting of calyx (hallmark), thickening of
ureter wall due to reflux- causes: recurrent UTI and chronic obstructive
diseases- thyroidization – lumen filled with colloid-like
material- kidney becomes nonfunctional requiring dialysis if
both kidneys are affected-
Figure 9. Inflammation is usually caused byascending infections due to E. coli. The cortico-medullary junction has been obliterated.
E. Nephrolithiasis
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 3/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 3 of 6
LEXI-ADI-GILLIAN-BUTCH
- favoured sites of formation are within the renalcalyces and pelvis, thus causing dilatation and if multiple, may thin out the renal parenchyma
- most stone (75%) are calcium containing(calcium oxalate, calcium phosphate); 15% areso-called triple stones (magnesium ammoniumphosphate).
Figure 10. NephrolithiasisNotes:- specimen: dilated calyx, atrophic renal
parenchyma which is replaced with fat- types of stone: (1) calcium, (2) triple
phosphate/magnesium ammoniumphosphate/struvite stone
- treatment: laser to convert the stone into powder - type of necrosis: coagulative necrosis wherein
the original morphology is retained- urinalysis: presence of blood (hematuria) and
crystals
** renal cell CA may also present with hematuria** how to differentiate renal cell CA andnephrolithiasis? conduct urine cytology (lowsensitivity)** urine cytology: centrifuge urine sample → getthe sediments → stain with hematoxylin eosin(H&E)
- ureterolithiasis – kidney is still intact
F. Kidney Hydronephrosis- enlargement may be slight or massive
- kidney transformed into a thin-walled cystic
structure- striking parenchymal atrophy- blunting of apices of the pyramids
Figure 11. Kidney HydronephrosisNotes:- specimen: atrophy of parenchyma replaced with
fatty tissue- cause: chronic obstruction- kidney may rupture from trauma which may lead
to peritonitis since urine is detected as a foreignbody
- treatment: pathologic kidney is usually removed
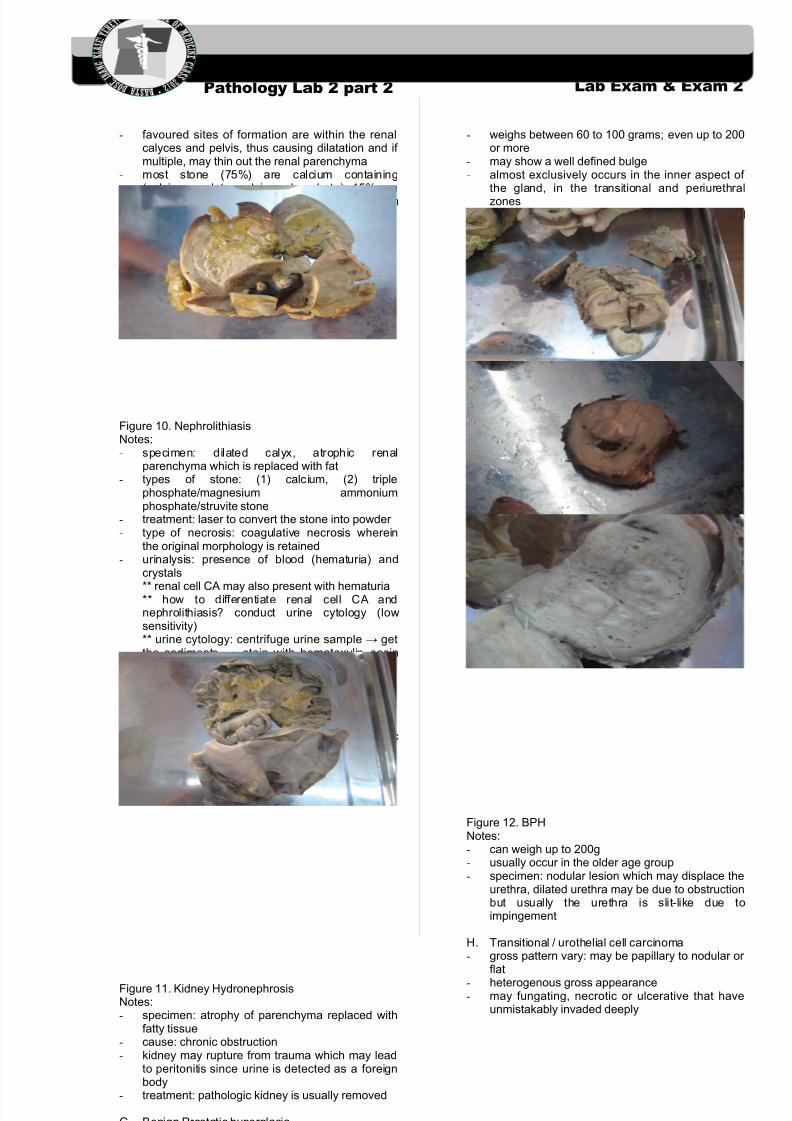
G. Benign Prostatic hyperplasia
- weighs between 60 to 100 grams; even up to 200or more
- may show a well defined bulge- almost exclusively occurs in the inner aspect of
the gland, in the transitional and periurethralzones
- Nodular enlargement may encroach the lateralwalls of the urethra to compress it into a slitlikeorifice
-
Figure 12. BPHNotes:- can weigh up to 200g- usually occur in the older age group- specimen: nodular lesion which may displace the
urethra, dilated urethra may be due to obstructionbut usually the urethra is slit-like due toimpingement
H. Transitional / urothelial cell carcinoma- gross pattern vary: may be papillary to nodular or
flat
-heterogenous gross appearance
- may fungating, necrotic or ulcerative that haveunmistakably invaded deeply
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 4/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 4 of 6
LEXI-ADI-GILLIAN-BUTCH
Figure 13. Transitional / urothelial cell carcinomaNotes:- normal bladder wall – smooth or trabeculated- specimen: fungating lesion (papillary), infiltrating
into the smooth muscle, black areas are due toIndia Ink stain which is used to determine the
depth of infiltration microscopically and assurgical lining of the section; along with thespecimen is the an atrophied uterus which ismeans the specimen came from a 50-60 year oldfemale
- management: surgical removal of the bladder and creation of a neobladder from the ilium
MICROSCOPIC SPECIMENA. Chronic protatitis
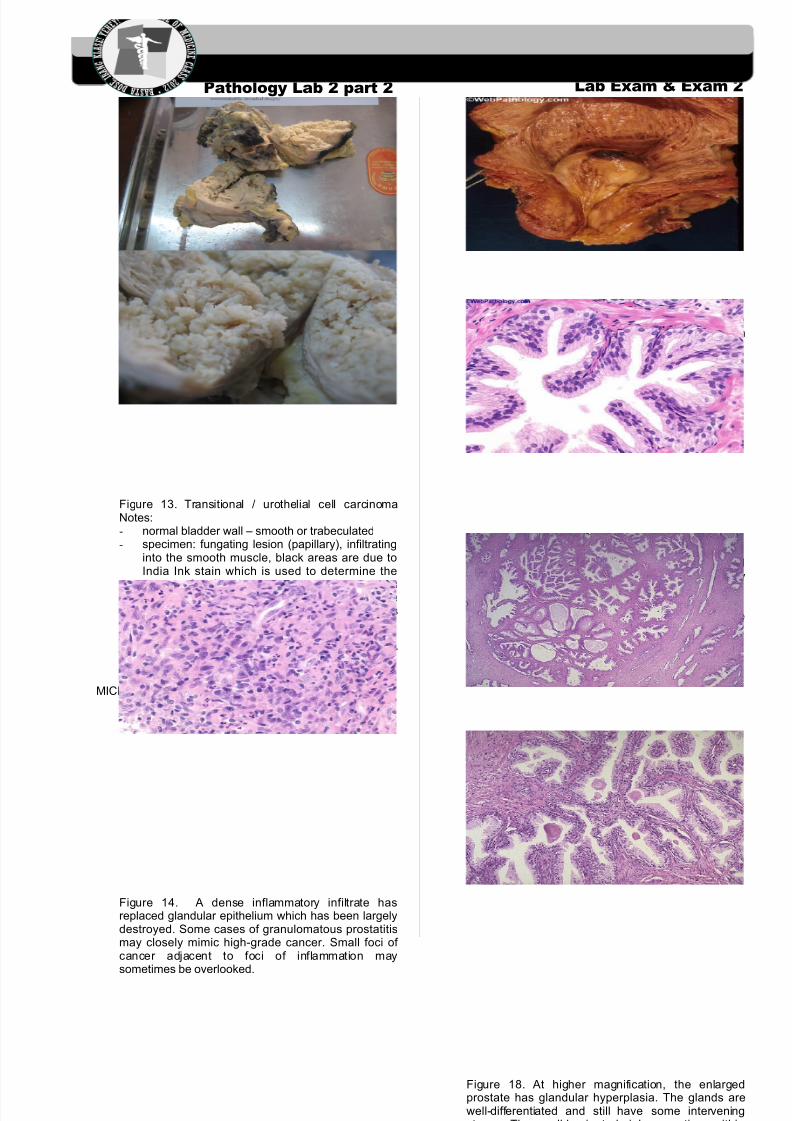
Figure 14. A dense inflammatory infiltrate hasreplaced glandular epithelium which has been largelydestroyed. Some cases of granulomatous prostatitismay closely mimic high-grade cancer. Small foci of cancer adjacent to foci of inflammation maysometimes be overlooked.
B. Nodular prostatic hyperplasia
Figure 15. Hyperplasia of the median lobe of theprostate produces a polypoid mass that protrudes inthe bladder lumen.
Figure 16. The luminal contour shows tufts andpapillary infoldings of glands. The tall secretory
epithelial cells have pale clear cytoplasm and uniformround or oval nuclei. Prominent nucleoli are not seen.Fibromuscular stroma and any basal cells can beidentified.
Figure 17. BPH can involve both glands and stroma,though the former is usually more prominent. Here, alarge hyperplastic nodule of glands is seen.
Figure 18. At higher magnification, the enlargedprostate has glandular hyperplasia. The glands arewell-differentiated and still have some interveningstroma. The small laminated pink concretions within
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 5/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 5 of 6
LEXI-ADI-GILLIAN-BUTCH
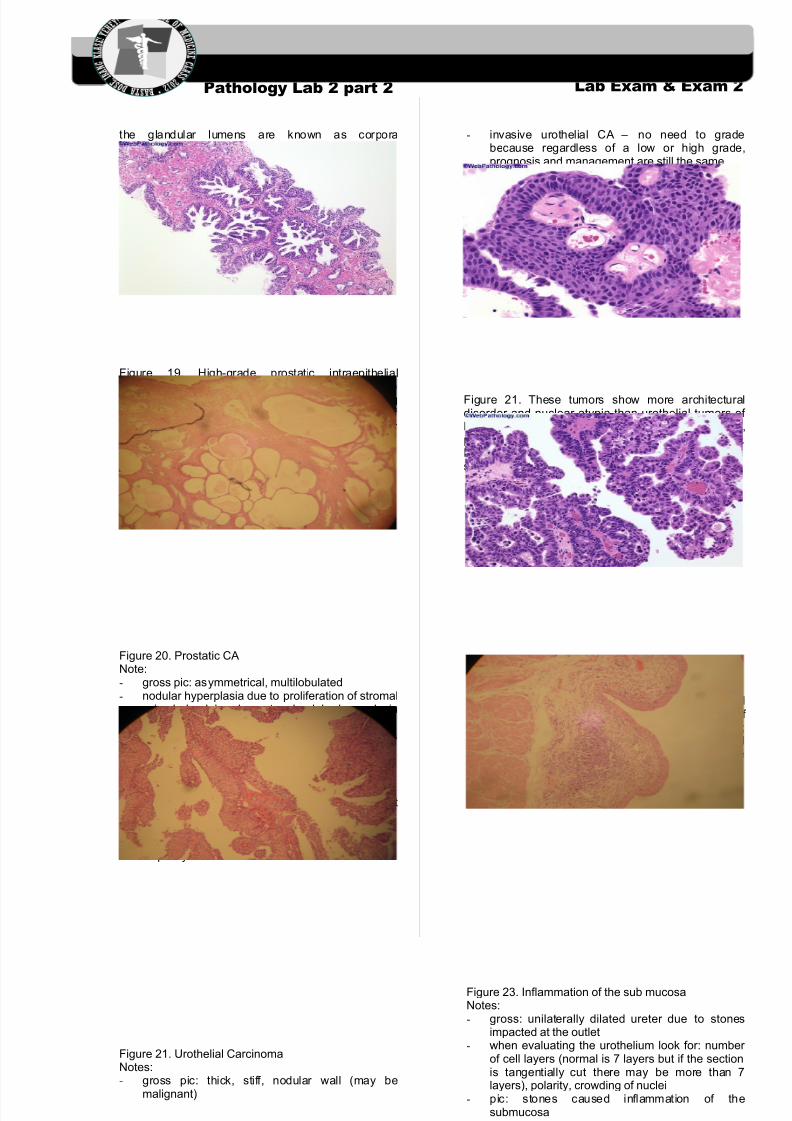
the glandular lumens are known as corporaamylacea.
C. Prostatic adenocarcinoma
Figure 19. High-grade prostatic intraepithelialneoplasia (PIN) consists of intermediate to large sizepreexisting glands with proliferative changes resultingin hyperchromatic appearance. Note the small foci of cancer adjacent to PIN on the upper left and lower right.
Figure 20. Prostatic CANote:- gross pic: asymmetrical, multilobulated- nodular hyperplasia due to proliferation of stromal
or/and glandular elements; glandular hyperplasiagrossly appear as cystic spaces
- adenocarcinoma – cells are trying to form glandswhich fuse together
- gleason grading: grades 1-3 = distinct glandsgrade 4 = fused glands
grade 5 = no glands visiblescore = predominating grade + second mostpredominant grade
- LM pic: pleomorphic hyperchromatic nuclei
D. Papillary urothelial carcinoma
Figure 21. Urothelial CarcinomaNotes:- gross pic: thick, stiff, nodular wall (may be
malignant)
- invasive urothelial CA – no need to gradebecause regardless of a low or high grade,prognosis and management are still the same
- LM: fibrovascular core
a. Low-grade
Figure 21. These tumors show more architecturaldisorder and nuclear atypia than urothelial tumors of low malignant potential. The nuclear size, shape,polarity, and chromatin show greater variability.Mitoses are still infrequent. Umbrella cells can still beseen.
b. High-grade
Figure 22. These tumors display total architecturaldisorganization and significant cytologic atypia of urothelium. There is loss of nuclear polarity;considerable variation in nuclear size, shape, andchromatin content; mitoses are frequent and may beabnormal. Umbrella cells are usually absent.
E. Chronic cystitis
Figure 23. Inflammation of the sub mucosaNotes:- gross: unilaterally dilated ureter due to stones
impacted at the outlet- when evaluating the urothelium look for: number
of cell layers (normal is 7 layers but if the sectionis tangentially cut there may be more than 7layers), polarity, crowding of nuclei
- pic: stones caused inflammation of thesubmucosa
8/14/2019 Patho Lab Trans -butch
http://slidepdf.com/reader/full/patho-lab-trans-butch 6/6
Pathology Lab 2 part 2
OS 214 Excretory Module Pathology Department
Lab Exam & Exam 2
March 11, 2009 | WED Page 6 of 6
LEXI-ADI-GILLIAN-BUTCH
a. Papillary Cystitis
Figure 24. Proliferation of vessels and accumulationof edema fluid and inflammatory cells in the laminapropria has created papillary configuration focally.Distinction from papillary urothelial carcinoma isimportant.
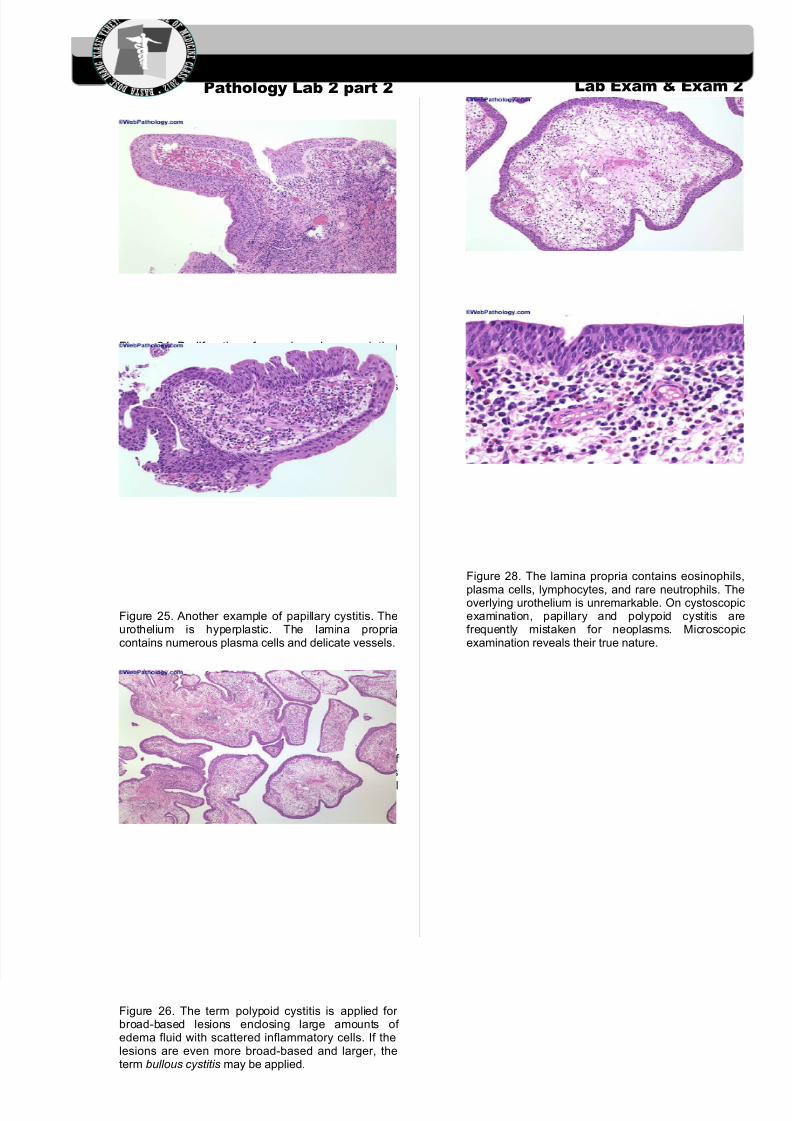
Figure 25. Another example of papillary cystitis. Theurothelium is hyperplastic. The lamina propriacontains numerous plasma cells and delicate vessels.
b. Polypoid Cystitis
- (Robbin’s) an inflammatory condition resultingfrom irritation to the bladder mucosa. Althoughindwelling catheters are the most commonly citedculprits, any injurious agent may give rise to thislesion. The urothelium is thrown into broad,bulbous, polypoid projections as a result of marked submucosal edema. Polypoid cystitis
may be confused with papillary urothelialcarcinoma both clinically and histologically
-
Figure 26. The term polypoid cystitis is applied for broad-based lesions enclosing large amounts of edema fluid with scattered inflammatory cells. If thelesions are even more broad-based and larger, theterm bullous cystitis may be applied.
Figure 27. The presence of edema fluid andinflammatory cells can be better appreciated in thisimage. The majority of the patients with polypoidcystitis have history of indwelling catheters.
Figure 28. The lamina propria contains eosinophils,
plasma cells, lymphocytes, and rare neutrophils. Theoverlying urothelium is unremarkable. On cystoscopicexamination, papillary and polypoid cystitis arefrequently mistaken for neoplasms. Microscopicexamination reveals their true nature.