part d and hospice
DESCRIPTION
Part D and Hospice. Judi Lund Person, MPH Jason Kimbrel, PharmD, BCPS Greg Dyke, RPh Joan Harrold, MD, MPH , FAAHPM, FACP Nancy Bridgman, Omnicare. Objectives. Update on Part D Changes at your hospice Admissions Collect Part D information from beneficiary Written materials - PowerPoint PPT PresentationTRANSCRIPT
Part D and Hospice
Judi Lund Person, MPHJason Kimbrel, PharmD, BCPS
Greg Dyke, RPhJoan Harrold, MD, MPH, FAAHPM, FACP
Nancy Bridgman, Omnicare

Objectives• Update on Part D• Changes at your hospice
– Admissions• Collect Part D information from beneficiary• Written materials• Giving staff the words
– Medication management• Documentation of reason for unrelated• Discontinuation of meds
• Review standardized form and draft instructions• FY2015 Hospice Wage Index proposed rule – Part D section• Questions

How did we get here?
• OIG report issued in 2012• Findings of $33 M in claims (FY2009) paid by Part D after
beneficiary elects hospice – four classes of drugs• Additional analysis by CMS Center for Program Integrity• Ongoing and intense discussions about the “intersection
between Part D and hospice” with CMS Part D and CMS Part A since summer 2013
• Final guidance issued by CMS on March 10 2014• Proposed regulations for hospice and Part D issued on
May 2 2014 for FY2015
Components of Final Guidance
• Considered to be “subregulatory guidance” without CMS enforcement
• Part D and hospice confusion• “Be ready by” date of May 1, 2014 – some Part D
plans implemented earlier
• Repeated reference to 2014 guidance– FY2015 Hospice Wage Index proposed rule posted on May
2 references changes to Part D/Hospice intersection

CMS Statements
• We expect drugs covered under Part D for hospice beneficiaries will be unusual and exceptional circumstances.
• 1983 Hospice final rule (48 FR 56010) was that the hospice benefit provides virtually all care for the terminally ill individual
• It is a comprehensive, holistic approach to treatment that recognizes that the impending death of an individual necessitates a change from curative to palliative care.
• NOTE: NHPCO continues to work with CMS on definitions and interpretations.

Key Issues
• Hospice physician’s responsibility. • Must document “why” the drug is unrelated –
form calls it “Rationale for Treatment”• Can the Part D plan override the hospice’s
decisions?• How will the hospice initiate communication
with the Part D plan?• How can hospices begin using the
standardized form?

ADMISSION PROCESS CHANGES

Admission Process
• Talk to patients and families about the changes in Part D coverage
• Evaluate pre-admission med regimen • Review patient admission packet for changes• Provide letter to patients and families describing
change• Provide letter patients and families can take to
pharmacy with hospice contact information• Collect information on Part D from patient/family• Collect information on preferred pharmacy

Finding a Patient’s Part D Plan
• Three ways– Ask for the patient’s Part D card during admission
• Collect patient’s insurance number, Part D plan name, any other numbers on the card and any contact phone number
• PREFERRED METHOD– Contact the pre-hospice medication dispenser
(preferred pharmacy) for Part D coverage information – Request that the pharmacy submit an E1 query to the
CMS Transaction Facilitator, which identifies: • Name and contact information of Part D plan sponsor• Takes time, depends on pharmacy workflow• Accuracy rate = 70%

Referral Sources
• Letter explaining Part D changes• Ongoing communication about coordination
with hospice• Close communication between Hospice and
SNF PRIOR TO ordering medications – Expected in regulations for both hospice and SNF– Review payment responsibility– May protect SNF from difficulties with LTC
pharmacy

MEDICATION MANAGEMENT
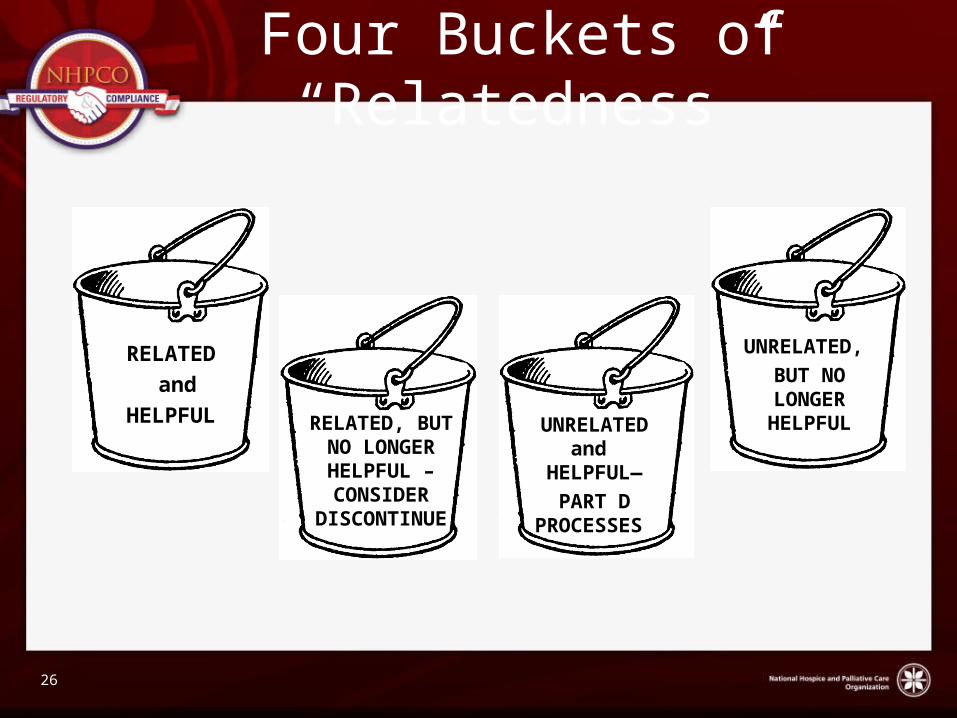
Four Buckets of “Relatedness”
RELATED and
HELPFUL UNRELATEDand
HELPFUL—PART D
PROCESSES
UNRELATED, BUT NO LONGER HELPFULRELATED,
BUT NO LONGER
HELPFUL – CONSIDER DISCONTIN
UE
26
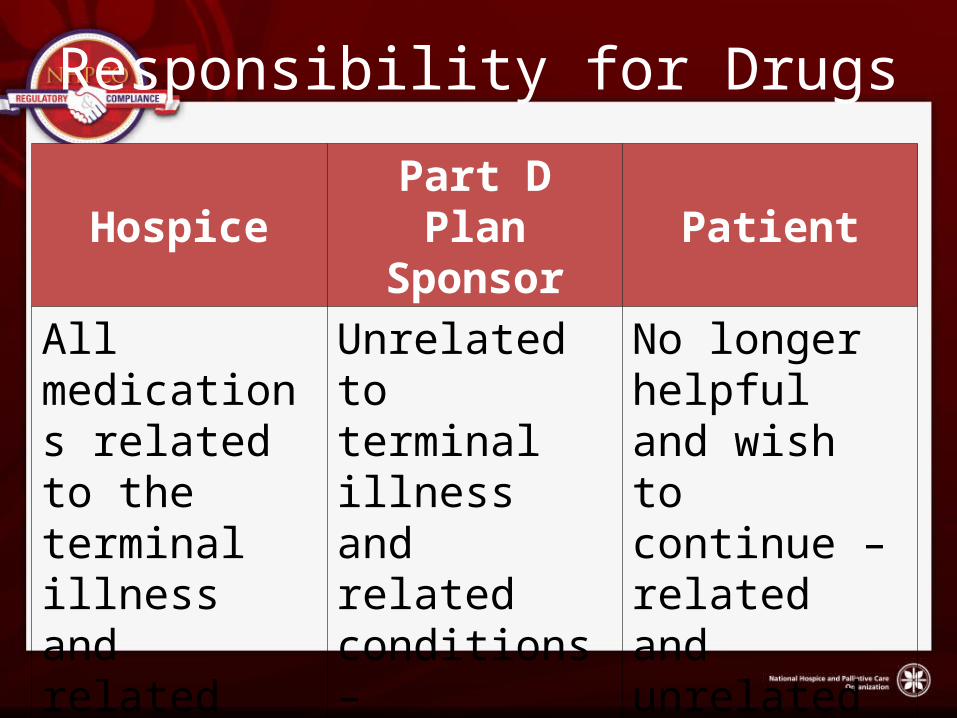
Responsibility for Drugs
Hospice Part D Plan Sponsor Patient
All medications related to the terminal illness and related conditions
Unrelated to terminal illness and related conditions – submitted to Part D plan for processing
No longer helpful and wish to continue – related and unrelated

When will my hospice interact with a Part D plan?
• Role of hospice PBM• Role of contracted community pharmacy• Prescriptions written by unaffiliated prescriber– If not coordinated with the hospice, will be
rejected at pharmacy
• Understanding Part D “processing”
Medication Management
• Treatment decisions should not be driven by costs, as opposed to clinical appropriateness.
• CMS states:“Hospices should use thoughtful clinical judgment, with a patient-centered focus, when developing the hospice plan of care, including the recommendations for medication management.”
Reports from Beneficiaries
• Anecdotal reports from Medicare hospice beneficiaries
• They are not receiving medications related to their terminal illness and related conditions from their hospice
• One reason stated – “those medications are not on the hospice’s formulary”
16
Formulary
• Many hospices establish a formulary• Hospice can offer an alternative to drug not
on formulary– If patient declines, patient pays
• Formulary drug is not working?– Hospice must provide off-formulary drug as
alternative

Medication Review with Patients and Families
• Begin the discussion• Give staff the words for the conversation• Consider timing and prognosis of patient
ABN for Medications
• No ABN Required:– For medications that are not reasonable and
necessary and the hospice will not provide to the beneficiary
– Documentation in the medical record is strongly suggested
• ABN Required: – If the hospice provides and pays for a medication
even though it is not reasonable and necessary, an ABN must be issued in order to charge the beneficiary
Beneficiary Appeal Rights
• If the beneficiary feels that the Medicare hospice should cover the cost of the drug, the beneficiary may submit a claim for the medication directly to Medicare on Form CMS-1490S.
• Appeal: Use if claim is denied under the appeals process set forth in part 405, subpart I.
STANDARDIZED FORM AND INSTRUCTIONS

Standardized Form and Instructions
• Developed by National Council of Prescription Drug Plans (NCPDP) Hospice Task Group
• Cooperative effort between Part D plans, NHPCO and hospice providers
• “Hospice Status and Plan of Care for Medicare Part D A3 Reject Override”
Components of Form
• Hospice information
• Patient information– Diagnoses– Admit/discharge date
• Prescriber information– Includes unaffiliated notation
• Hospice PBM information• Signed by
– Hospice or– Prescriber
Unrelated medications•Name and strength•Dosing schedule•Quantity per month•Rational for treatmentMedications under hospice plan of care•Determination of responsible party
– Hospice– Patient
Patient Information
• Diagnoses– Primary– Secondary– Unrelated
• Admit/discharge date

Medications Unrelated
• Medication name and strength• Dosing schedule• Quantity per month• Rationale for treatment– Why drug is unrelated?– 1-2 sentences– Must provide clinical basis
Instructions for Form
• In draft form• Feedback from hospice providers and Part D
plans once the form is in use

Unanswered Questions
• Should beneficiary give up their Part D plan when they enroll in hospice?
• Can beneficiary re-enroll in Part D plan if discharged or revoke hospice benefit?
• List of Part D plan phone/fax numbers for hospice contacts?
• Can hospice interact with Part D plan as prescriber?
• Add questions to this list…

FY2015 HOSPICE WAGE INDEX PROPOSED RULE – PART D INCLUDED
FY2015 Hospice Wage Index Proposed Rule
• Proposed change in filing NOE– No more than 3 days after the date of election
• Propose a Notice of Termination or Revocation (NOTR)– No more than 3 days after live discharge or
revocation
• Considering requiring Part D sponsors to accept NOE and NOTR information as use for coverage until official CMS notification is received
New Proposed Definitions
• Terminal illness• Related conditions
• CMS asks for comments on definitions• Definitions, when final, will guide Part D
coverage for hospice patient medications

Independent Review Process
• CMS considering• Separate and distinct from the enrollee
appeals process • Independent Review Entity (IRE) decision
would be binding on both the Part D sponsor and the hospice
31
Resources
• NHPCO web page on Part D and Hospice• http://
www.nhpco.org/regulatory-compliance-hospices/part-d-and-hospice
• Compliance Guide• Sample Letters• Latest information