parry romberg syndrome
TRANSCRIPT

Parry romberg syndrome
Neurocutaneous syndrome characterized by progressive shrinkage and degeneration of the tissues beneath the skin usually on only one side of face but occasionally extending to other parts of the body
The condition is often accompanied by significant neurological, ocular and oral signs and symptoms
Progressive facial hemiatrophy

There is an estimate that 1 in every 700.000 births present this syndrome
The earlier the onset of the disease, skeletal compromise is more likely, due to skeletal growth and development.
In 95% of the time, the face is compromised unilaterally
PRS is not a congenital disease with onset typically in the first or second decade of life
The syndrome usually affects more than one branch of the trigeminal nerve dermatomes of the trigeminal nerve, being V1 (ophthalmic division) damaged in 35% of the cases, V2 (maxillary division) in 45% and V3(mandibular division) in the remaining 20%.
Incidence

No genetic predispositions, no hereditary traits defined,no ethnic preferences
Nervous system hyperactivity ? Etiological hypothesis resume to
InfectionPeripheral trigeminal neuritis – a trigeminal neuritis would begin with episodes of pain followed by tissue atrophy.Sympathetic Hypothesis – based on an association among Horner Syndrome, pilomotor reflex alterations, unilateral mydriasis, vasomotor diseases, unilateral migraine and transpiring diseases
Etiology

The syndrome often begins with a circumscribed
patch of SCLERODERMA in the frontal region of the
scalp which is associated with a loss of hair and the
appearance of a depressed linear scar extending
down through the midface on the affected side.
This scar is referred to as a "coup de sabre"
lesion
Clinical features

“coup de sabre

The affected area extends progressively with the
atrophy of the skin, subcutaneous tissue, the muscles,
bones, cartilages, alveolar bone and soft palate on that
side of the face.
The mouth and nose are typically deviated towards the
affected side of the face
The process may eventually extend to involve
tissues between the nose and upper corner of lip,
the upper jaw ,the angle of mouth, the area around the
eye and brow, the ear, and/or the neck
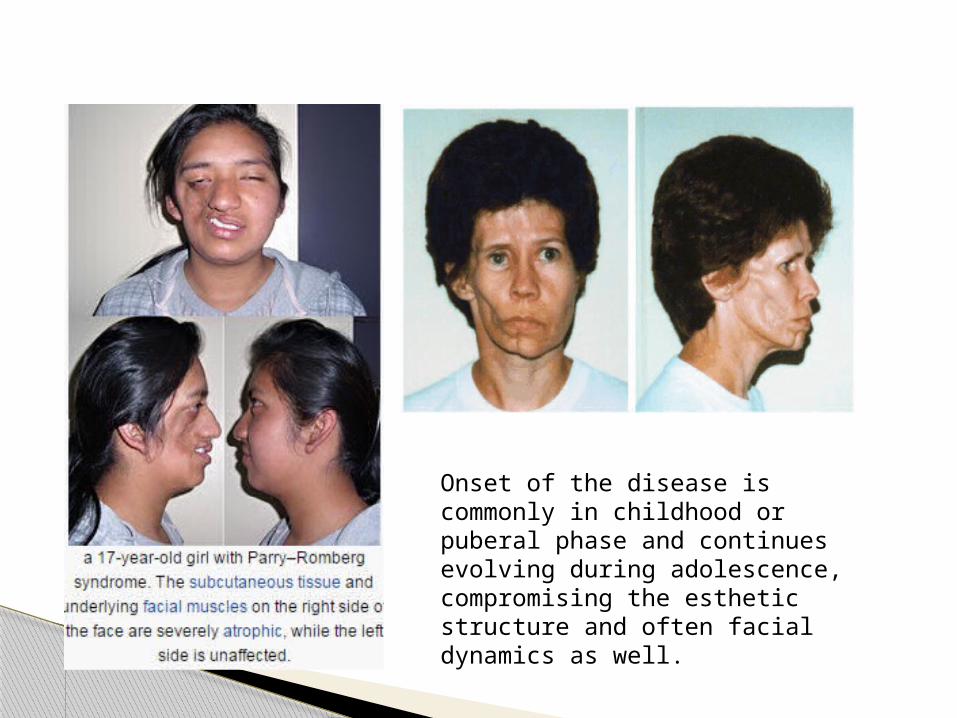
Onset of the disease is commonly in childhood or puberal phase and continues evolving during adolescence, compromising the esthetic structure and often facial dynamics as well.

Inigo et al proposed a classification for PRS based on skin, subcutaneous tissue and bony atrophy in trigeminal dermatomes:
A) Mild: Atrophy of skin and subcutaneous tissue of only one trigeminal dermatome. No bone involvement
B) Moderate: Two trigeminal dermatomes involved, no bony structures affected.
C) Severe: All three trigeminal territories affected or bone involvement. In the initial phases of the disease, there may be cutaneous hardness, hypercromia or hypocromia (similar to scleroderma) of skin, hair, Iris and even cicatricial alopecia
Classification
Systemic Associations
Neurological ocular
Seizures -most common
Migraneous crisis Aneurisms Cerebral atrophy Cerebral vascular
anomalies Facial muscular
spasms
Enophtalmia Uveitis Retinal vasculitis Paralysis of III cranial
nerve Glaucoma and eyelid
atrophy Mydriasis,miosis,
vasomotor or secretory reactions
oculo-pupillary phenomena

Treatment is divided into two philosophies: the first
consists in trying to stop the disease process through
immunosupression which also improve associated
symptoms, while the second regards the repair of
acquired deformities after stabilization of the disease
process. For such, many reconstructive and esthetic
procedures have been tried, such as free grafts,
microsurgery, flaps and alloplastic material
Treatment



BEFORE AFTER TREATMENT WITH MULTIPLE FAT GRAFTS
Parry Romberg Syndrome continues to be an
challenge for research in plastic surgery. It
represents an infirmity with an obscure etiology,
unknown physio-pathology, wide array of clinical
presentations, whose treatment still demands
more than one procedure