parp inhibitors: usurping dna repair to target cancer lee schwartzberg md, facp chief medical...
TRANSCRIPT

PARP Inhibitors:PARP Inhibitors:Usurping DNA repair to target Usurping DNA repair to target
cancercancer
Lee Schwartzberg MD, FACP
Chief Medical Officer
The West Clinic

Question 1
DNA repair mechanisms are important in
1. Cancer cells only
2. Both cancer and normal eukaryotic cells
3. Predominantly in rapidly growing cells like bone marrow precursors
4. Predominantly cancer cells with BRCA mutations

Question 2
PARP inhibitors have demonstrated activity in:
1. BRCA 1 mutation carrier breast cancer
2. BRCA 2 mutation carrier breast cancer
3. Triple negative breast cancer
4. 1 and 3 only
5. 1 and 2 only
6. All of the above

All cells are under constant risk of All cells are under constant risk of DNA damageDNA damage
Ultraviolet light Ionizing radiation Man-made and natural chemicals Reactive oxygen species
most are generated “endogenously”
10,000 Single Strand Breaks/ cell/day ~100,000,000,000,000,000 DNA lesions in a
human body every day1-3
1. Jackson SP. Biochem Soc Trans 2001;29:655-6612. Lindahl T. Nature 1993;362:709-715
3. Jackson SP, Bishop CL. Drug Discovery World 2003;(Fall):41-45

Cellular Response To DNA Cellular Response To DNA DamageDamage

Cancer cells are highly susceptible Cancer cells are highly susceptible to DNA repair inhibitionto DNA repair inhibition Undergo deregulated proliferation
Less time for DNA repair than in normal cells Grow under stress, which causes ongoing DNA
damage Have DNA repair defects
P53, BRCA1, BRCA 2, ATM, Fanconi’s Anemia Allow growth despite ongoing genome instability
Are reliant on the DNA repair pathways they still retain

DNA Excision Repair MechanismsDNA Excision Repair Mechanisms

Lig3XRCC1
PolßPNK
Poly(ADP-Ribose) Polymerase (PARP)Poly(ADP-Ribose) Polymerase (PARP)
A key role in the repair of DNA single-strand breaks Through the base excision repair pathway (BER) Binds directly to sites of DNA damage Once activated, it uses NAD as a substrate, and generates
large, branched chains of poly (ADP-ribose) polymers on multiple target proteins
Recruits other DNA repair enzymes
PAR

Base Excision RepairBase Excision Repair

Inhibiting PARP-1 Increases Double-Strand DNA Inhibiting PARP-1 Increases Double-Strand DNA DamageDamage
PARP
Inhibition of PARP-1 prevents -recruitment of DNA repair enzymes-leads to failure of SSB repair-accumulation of SSBs
XRCC1
LigIII
PNK 1
pol β
During S-phase, replication fork
is arrested at site of SSB
DNA single strand break (SSB)damage
Degeneration into Double strand breaks

BRCA1 And 2 Are Required for Efficient BRCA1 And 2 Are Required for Efficient Repair of Double Stranded DNA BreaksRepair of Double Stranded DNA Breaks
DNA DSB
ATM/R
Ligase IVXRCC4
DNA-PKcs
Ku 70/80
ERCC1XRCC3
Rad 52/4RPA
Rad 51BRCA2
NBS1MRE11
Rad50BRCA1
H2AX
Non-homologous end-joining Homologous recombination
Predominant in G1Error-proneGross Genomic instability
Major pathway for repair Error-free
Cells with BRCA mutations are deficient in homologous recombination and lack the ability to efficiently repair DSBs.
Cancer cell death
Cellsurvival

The Concept of Synthetic LethalityThe Concept of Synthetic Lethality
(PARP)(BRCA)
Ashworth, A. J Clin Oncol; 26:3785-3790 2008

Farmer H et al. Nature 2005;434:917-920Personal communication, Alan Ashworth
BRCA1 and BRCA2 -/- cells are very BRCA1 and BRCA2 -/- cells are very sensitive to PARP inhibitionsensitive to PARP inhibition
BRCA2 +/-
BRCA2 -/-
Wild type
Log surviving fraction
0-4
-3
-2
-1
0
PARP inhibitor concentration (M)10-9 10-8 10-7 10-6 10-5 10-4
Control + PARP inhibitor
Control + PARP inhibitor
Wild type
BRCA2 -/-
Increased levels of chromosomal aberrations in PARP inhibitor treated BRCA2 -/- cells

PARP Inhibitors in Clinical PARP Inhibitors in Clinical DevelopmentDevelopment
Differing chemical structures
Differing toxicity
Differing schedules and routes of administration
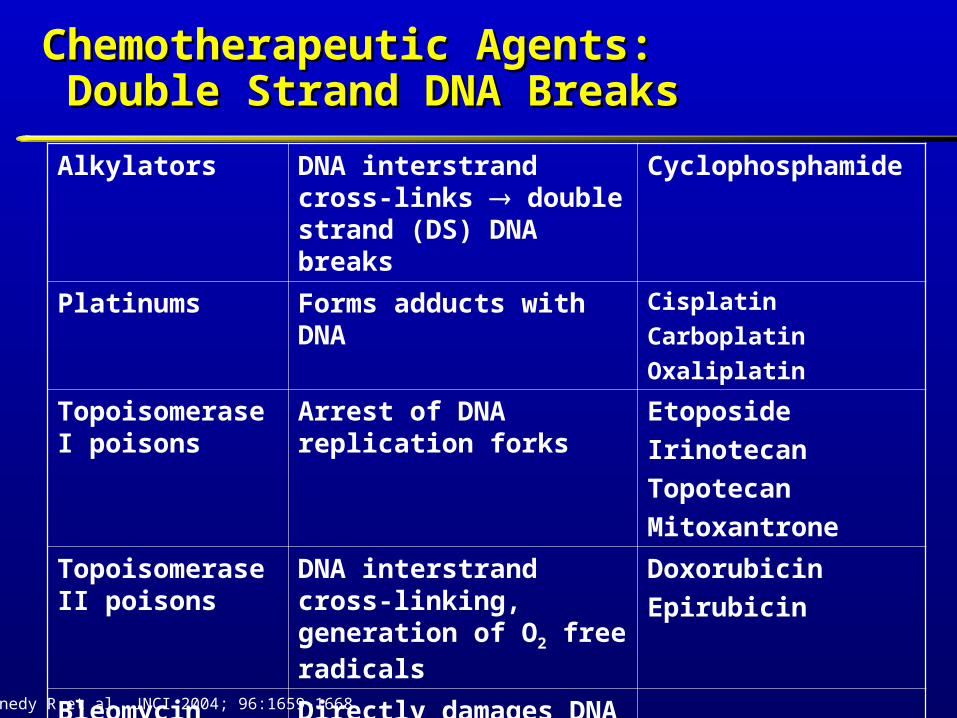
Chemotherapeutic Agents:Chemotherapeutic Agents: Double Strand DNA Breaks Double Strand DNA Breaks
Alkylators DNA interstrand cross-links double strand (DS) DNA breaks
Cyclophosphamide
Platinums Forms adducts with DNA Cisplatin
Carboplatin
Oxaliplatin
Topoisomerase I poisons
Arrest of DNA replication forks
Etoposide
Irinotecan
Topotecan
Mitoxantrone
Topoisomerase II poisons
DNA interstrand cross-linking, generation of O2 free radicals
Doxorubicin
Epirubicin
Bleomycin Directly damages DNA DS DNA breaks
Kennedy R et al. JNCI 2004; 96:1659-1668

PARP Inhibitors in BRCA 1/2 PARP Inhibitors in BRCA 1/2 Mutated TumorsMutated Tumors

Phase I Trial of Olaparib in Phase I Trial of Olaparib in Patients with Solid TumorsPatients with Solid Tumors
Escalation and expansion phase, n = 60 Recommended phase II dose: 400 mg PO BID Toxicities
Nausea (32%), fatigue (30%), vomiting (20%), taste alteration (13%), anorexia (12%), anemia (5%)
Clinical activity = 12/19 patients with BRCA mutations
Tumor BRCA No. of pts Response
Breast 2 2 1 CR, 1 SD
Ovarian 1 or 2 8 8 PRs
Fallopian tube 1 1 PR
Prostate 2 1 PR
Fong PC et al. N Engl J Med 2009; 361:123-134

Phase II Trial of Olaparib in BRCA-deficient Phase II Trial of Olaparib in BRCA-deficient Metastatic Breast CancerMetastatic Breast Cancer
Eligibility
Confirmed BRCA1 or 2 mutation
Stage IIIB/C or IV BC after progression ≥ 1 prior chemotherapy for advanced disease
Cohort 2*
Olaparib 100 mg po bid (maximal PARP inhibition)
28-day cycles
Cohort 1
Olaparib 400 mg po bid (MTD)
28-day cycles
* Following an interim review, patients in the 100 mg bid cohort were permitted to crossover to receive 400 mg bid
(Non-randomized sequential cohorts)
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)
Primary Endpoint: Response rate

Olaparib 400 mg BID(n = 27)
Olaparib 100 mg BID(n = 27)
Grade 1/2 Grade 3 Grade 1/2 Grade 3
Fatigue 15 (56) 4 (15) 15 (56) 2 (7)
Nausea 11 (41) 5 (19) 15 (56) 0
Vomiting 7 (26) 3 (11) 6 (22) 0
Headache 10 (37) 0 5 (19) 1 (4)
Constipation 6 (22) 0 8 (30) 0
Olaparib in BRCA-deficient Metastatic Breast Cancer: Select Toxicities
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)

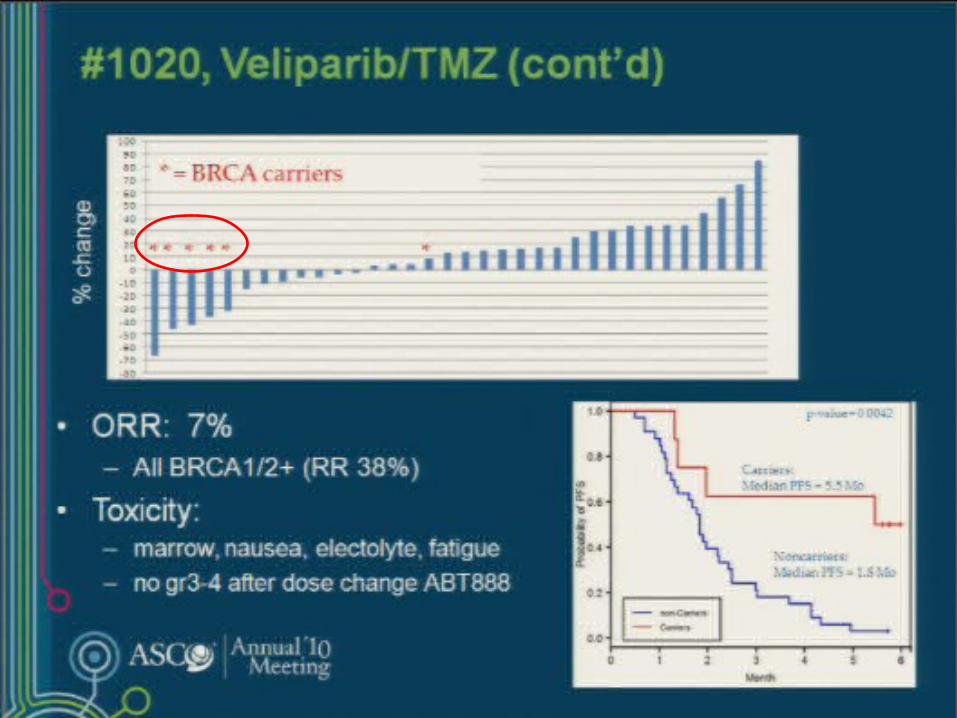
Olaparib in BRCA-deficient Olaparib in BRCA-deficient Metastatic Breast Cancer: ResultsMetastatic Breast Cancer: Results
ITT cohort 400 mg BID
N = 27
100 mg BID
N = 27
ORR 11 (41%) 6 (22%)
CR 1 (4%) 0
PR 10 (37%) 6 (22%)
Median PFS
5.7 mo
(4.6-7.4)
3.8 mo
(1.9 – 5.6)
Tutt A et al. J Clin Oncol 2009;27(18S):803s (abstr CRA501)
Best percent change from baseline in target lesions
by genotype
Median 3 prior lines of therapy
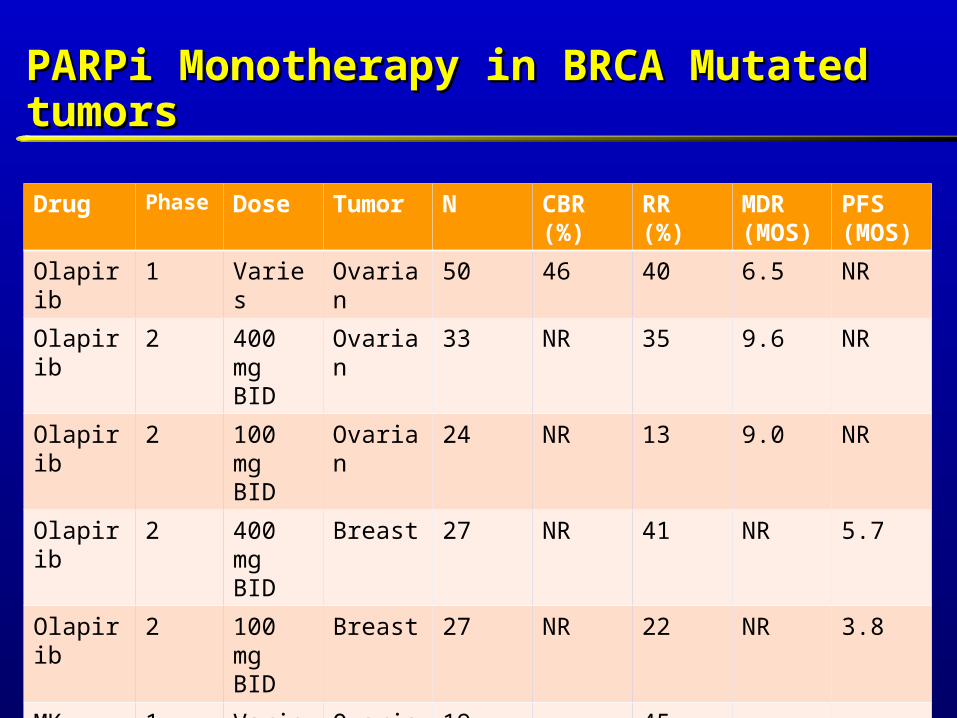
PARPi Monotherapy in BRCA Mutated PARPi Monotherapy in BRCA Mutated tumorstumors
Drug Phase Dose Tumor N CBR (%)
RR (%)
MDR (MOS)
PFS (MOS)
Olapirib 1 Varies Ovarian 50 46 40 6.5 NR
Olapirib 2 400 mg BID
Ovarian 33 NR 35 9.6 NR
Olapirib 2 100 mgBID
Ovarian 24 NR 13 9.0 NR
Olapirib 2 400 mgBID
Breast 27 NR 41 NR 5.7
Olapirib 2 100 mg BID
Breast 27 NR 22 NR 3.8
MK-4827
1 Varies Ovarian 19 45
MK-4827
1 Varies Breast 4 50
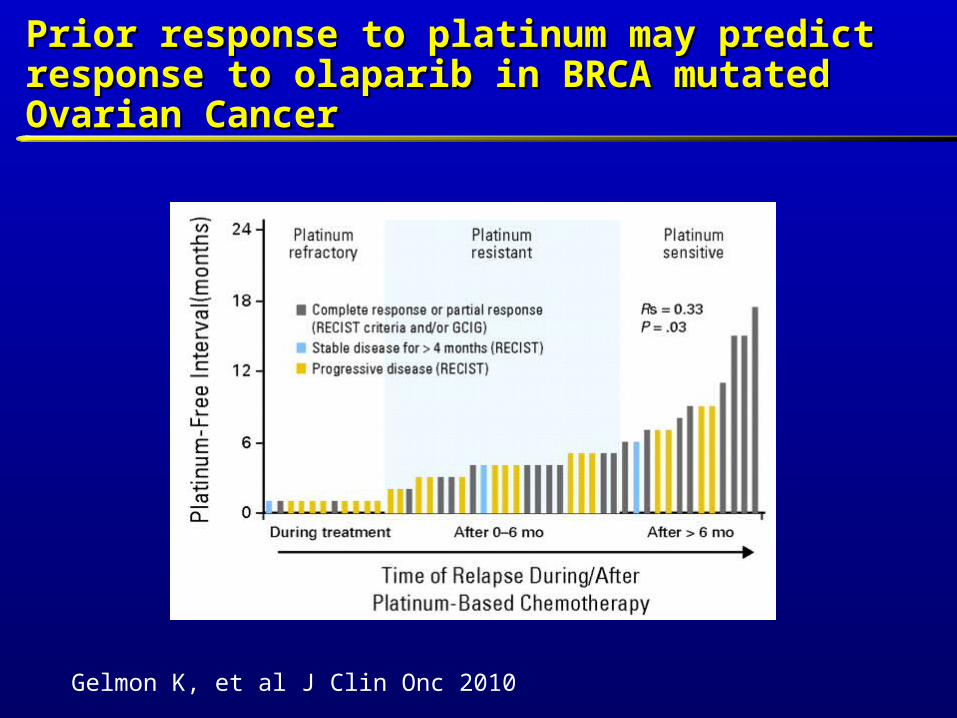
Prior response to platinum may predict response Prior response to platinum may predict response to olaparib in BRCA mutated Ovarian Cancerto olaparib in BRCA mutated Ovarian Cancer
Gelmon K, et al J Clin Onc 2010

PARP Inhibitors beyond BRCA PARP Inhibitors beyond BRCA mutation carriersmutation carriers

Triple Negative Breast Cancer Triple Negative Breast Cancer (TNBC)(TNBC)
‘Triple negative’: ER-negative, PR-negative, HER2-negative Depending on thresholds used to define ER and PR
positivity and methods for HER2 testing
TNBC accounts for 10–17% of all breast carcinomas
Significantly more aggressive than other molecular subtype tumors
Higher relapse rate than other subtypes No specific targeted therapy
Reis-Filho JS, et al. Histopathology 2008;52:108-118.

Characteristics Hereditary BRCA1 Triple Negative/Basal-Like1,2,3
ER/PR/HER2 status Negative Negative
TP53 status Mutant Mutant
BRCA1 status Mutational inactivation* Diminished expression*
Gene-expression pattern Basal-like Basal-like
Tumor histologyPoorly differentiated
(high grade)Poorly differentiated
(high grade)
Chemosensitivity to DNA-damaging agents
Highly sensitive Highly sensitive
TNBC Shares Clinical and Pathologic Features with TNBC Shares Clinical and Pathologic Features with BRCA-1-Related Breast Cancers (“BRCAness”)BRCA-1-Related Breast Cancers (“BRCAness”)
3Sorlie et al. Proc Natl Acad Sci U S A 2001;98:10869-744 Miyoshi et al. Int J Clin Oncol 2008;13:395-400
*BRCA1 dysfunction due to germline mutations, promoter methylation, or overexpression of HMG or ID44
1Perou et al. Nature. 2000; 406:747-7522Cleator et al.Lancet Oncol 2007;8:235-44

Targeting DNA Repair Pathway in Targeting DNA Repair Pathway in TNBCTNBC
Clustering analyses of microarray RNA expression have shown that familial BRCA-1 tumors strongly segregate with basal-like/ triple-negative tumors
Suggests that sporadic TNBC may have acquired defects in BRCA1-related functions in DNA repair
= BRCA1+ = BRCA2+
Basal-like
Sorlie T et al. PNAS 2003;100:8418-8423

Predictors of Response to Cisplatin in Predictors of Response to Cisplatin in TNBCTNBC
Silver, D. P. et al. J Clin Oncol; 28:1145-1153 2010
Phase II Study of the PARP inhibitor Iniparib in Phase II Study of the PARP inhibitor Iniparib in Combination with Gemcitabine/Carboplatin in Combination with Gemcitabine/Carboplatin in Triple Negative Metastatic Breast CancerTriple Negative Metastatic Breast Cancer
Background and Rationale
PARP1 Upregulated in majority of triple negative human breast cancers1
Iniparib (BSI-201)
Small molecule IV PARP inhibitor
Potentiates effects of chemotherapy-induced DNA damage
No dose-limiting toxicities in Phase I studies of BSI-201 alone or in combination with chemotherapy
Marked and prolonged PARP inhibition in PBMCs
O’Shaughnessy J, et al. NEJM 2011

Phase II TNBC Study: Treatment Schema Phase II TNBC Study: Treatment Schema
21-DayCycle
* Patients randomized to gem/carbo alone could crossover to receive gem/carbo + BSI-201 at disease progression
RANDOMIZE
BSI-201 (5.6 mg/kg, IV, d 1, 4, 8, 11)
Gemcitabine (1000 mg/m2, IV, d 1, 8)
Carboplatin (AUC 2, IV, d 1, 8)
BSI-201 (5.6 mg/kg, IV, d 1, 4, 8, 11)
Gemcitabine (1000 mg/m2, IV, d 1, 8)
Carboplatin (AUC 2, IV, d 1, 8)
Gemcitabine (1000 mg/m2, IV, d 1, 8)
Carboplatin (AUC 2, IV, d 1, 8)
Gemcitabine (1000 mg/m2, IV, d 1, 8)
Carboplatin (AUC 2, IV, d 1, 8)
RESTAGINGEvery 2 Cycles
Metastatic TNBCN = 120
1st -3rd line MBC Eligible

Safety – Hematologic ToxicitySafety – Hematologic ToxicityPhase II Gem Carbo +/- IniparibPhase II Gem Carbo +/- Iniparib
Gem/Carbo(n = 59)
BSI-201 + Gem/Carbo(n = 57)
Grade 2 Grade 3 Grade 4 Grade 2 Grade 3 Grade 4
Anemia, n (%)12
(20.3%)7 (11.9%)
0 (0.0%)
15(26.3%)
7 (12.3%)
0 (0.0%)
Thrombocytopenia, n (%) 7 (11.9%)6
(10.2%)6
(10.2%)4
(7.0%)6
(10.5%)7
(12.3%)
Neutropenia, n (%) 7 (11.9%)18
(30.5%)13
(22.0%)7 (12.3%)
18 (31.6%)
7(12.3%)
Febrile neutropenia, n (%)0
(0.0%)3
(5.1%)1
(1.7%)0
(0.0%)0
(0.0%)0
(0.0%)
RBC treatment*, n (%)5
(8.5%)5
(8.5%)2
(3.4%)3
(5.3%)5
(8.8%)2
(3.5%)
G-CSF Use, n (%)6
(10.2%)6
(10.2%)3
(5.1%)4
(7.0%)5
(8.8%)1
(1.8%)
*Transfusion and/or EPO use
O’Shaughnessy J, et al. NEJM 2011

Gem/Carbo(n = 59)
BSI-201 + Gem/Carbo(n = 57)
Grade 2 Grade 3 Grade 4 Grade 2 Grade 3 Grade 4
Nausea, n (%)10
(16.9%)2
(3.4%)0
(0.0%)7
(12.3%)0
(0.0%)0
(0.0%)
Vomiting, n (%)9
(15.3%)0
(0.0%)0
(0.0%)4
(7.0%)1
(1.8%)0
(0.0%)
Fatigue, n (%)10
(16.9%)6
(10.2%)0
(0.0%)10
(17.5%)1
(1.8%)0
(0.0%)
Neuropathy, n (%)2
(3.4%)0
(0.0%)0
(0.0%)1
(1.8%)0
(0.0%)0
(0.0%)
Diarrhea, n (%)6
(10.2%)1
(1.7%)0
(0.0%)1
(1.8%)1
(1.8%)0
(0.0%)
Safety – Non-Hematologic ToxicitySafety – Non-Hematologic ToxicityPhase II Gem Carbo +/- IniparibPhase II Gem Carbo +/- Iniparib
O’Shaughnessy J, et al. NEJM 2011

Final Results:Final Results:Phase II: Gem Carbo +/- Iniparib in TNBCPhase II: Gem Carbo +/- Iniparib in TNBC
O’Shaughnessy J et.al. NEJM 2011

Final Results:Final Results:Phase II Gem Carbo +/- Iniparib in TNBCPhase II Gem Carbo +/- Iniparib in TNBC
O’Shaughnessy J, et.al. NEJM 2011

Phase I: Olaparib + Paclitaxel in 1Phase I: Olaparib + Paclitaxel in 1stst and 2and 2ndnd line MBC line MBC
BKG: Olaparib single agent activity in BRCA 1/2 mutated MBC
Olaparib + paclitaxel, N=19, 70% 1st line, unselected for BRCA mutations
33-40% RR; no CRs Median PFS: 5.2-6.3 months Hematologic toxicity high, requires G-CSF Dose reductions common Unclear whether combination be taken forward

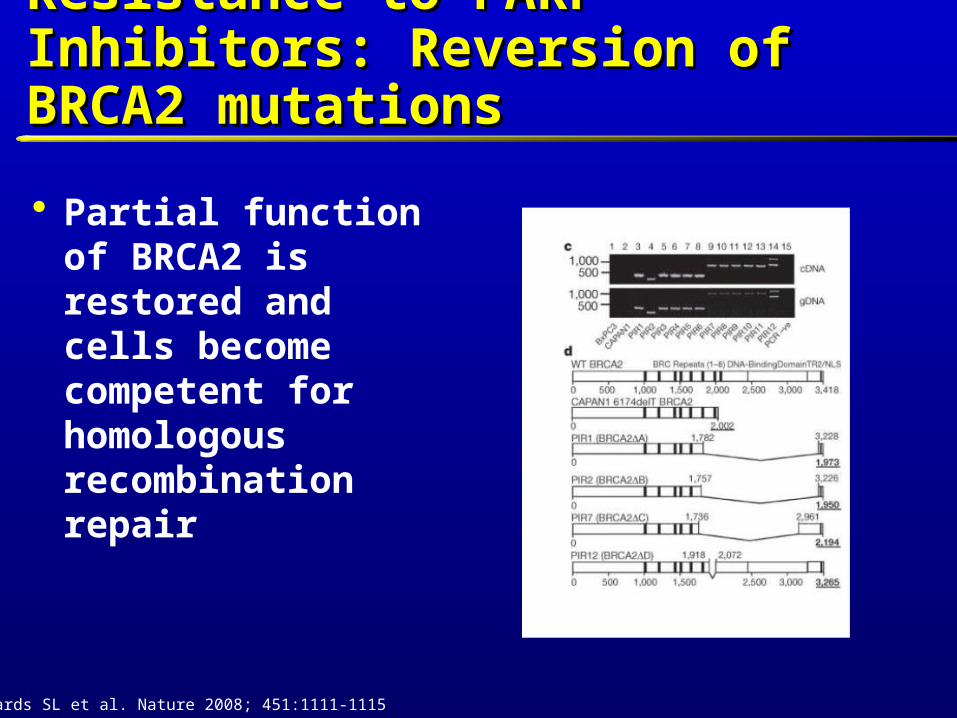
Resistance to PARP Inhibitors: Resistance to PARP Inhibitors: Reversion of BRCA2 mutationsReversion of BRCA2 mutations
Partial function of BRCA2 is restored and cells become competent for homologous recombination repair
Edwards SL et al. Nature 2008; 451:1111-1115

The Future of PARP inhibitors: The Future of PARP inhibitors: Many Unanswered QuestionsMany Unanswered Questions
Can we use these agents more broadly? To treat other tumors with specific DNA repair defects,
i.e. sporadic loss of BRCA 1/2, tumors with PTEN mutations
Challenge is to identify them
Timing of PARP inhibitor in relation to cytotoxic agent (before it, with it, how long to continue it?)
ConclusionsConclusions
Targeting DNA repair mechanisms in tumor cells is a rational target
PARP is an integral enzyme in DNA repair Multiple PARP inhibitors are available Preliminary results show activity in BRCA mutated
cancers (Breast and Ovarian) Preliminary results show activity of iniparib with
chemotherapy in TNBC Phase III results forthcoming