parotid gland
TRANSCRIPT


SEMINAR
PAROTID GLAND
Presented By:-Dr. Amrita Rastogi
M.D.S 1st Year

CONTENTS INTRODUCTION
PAROTID CAPSULE
SURFACE MARKING
EXTERNAL FEATURES
DEVELOPMENT
RELATIONS
STRUCTURE WITHIN THE PAROTID GLAND
PROCESSES

PAROTID DUCT
NERVE SUPPLY
LYMPHATIC DRAINAGE AND LYMPH NODES
HISTOLOGY
FUNCTIONS OF PAROTID GLAND
CLINICAL CONSIDERATIONS
ROLE OF PUBLIC HEALTH DENTIST
CONCLUSION
REFERENCES

INTRODUCTION [1] [2] [3] The salivary glands in mammals are a group of
compound exocrine glands, glands with ducts, that
produce saliva.
They are:
• Parotid gland
• Sub mandibular gland
• Sublingual gland
• Minor salivary glands

Parotid region contains the largest serous salivary
gland and the “queen of the face”, the facial nerve.
Parotid gland(Para=around; otic=ear) is the largest
major salivary gland.
Parotid gland contains vertically disposed blood
vessels and horizontally situated facial nerve and
various branches.

Paired parotid glands lying largely below the
external acoustic meatus between mandible and
sternocleidomastoid muscle and it also projects
forwards on the surface of masseter.
Sternomastoid
External acousticmeatus
Ramus of mandible

Occupies the deep hollow
behind the ramus of the
mandible.
Wedge-shaped when viewed
externally , with the base
above & the apex behind the
angle of the mandible.

On the surface of the masseter, smalldetached part lies between zygomatic archand parotid duct called as Accessory parotidgland or ‘socia parotidis’

• It is irregular, wedge shaped, and unilobular.
Parotid is 14-28 grams in weight and provides 60-
65% of total salivary volume.
• Dimensions:-
averaging 5.8 cm ( craniocaudal dimension),
3.4 cm (ventraldorsal dimension).
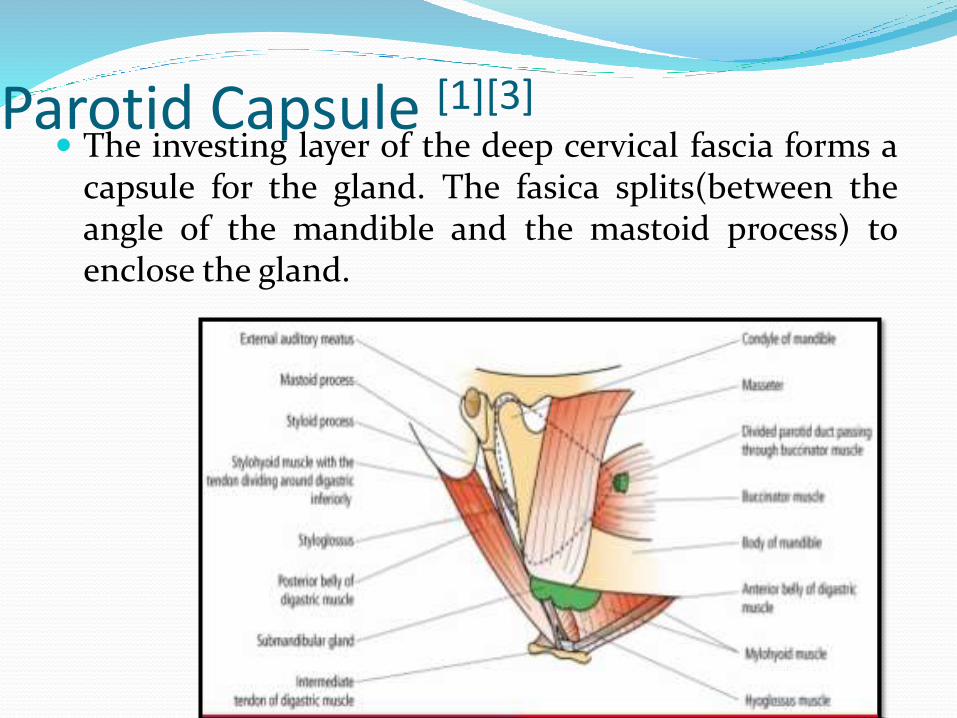
Parotid Capsule [1][3] The investing layer of the deep cervical fascia forms a
capsule for the gland. The fasica splits(between theangle of the mandible and the mastoid process) toenclose the gland.
Consists of :-
1) Superficial layer – It is thick and adherent to gland.
It extends from the masseter and
Sternocliedomastoid to the Zygoma,
2) Deep layer – It is thin and is attached to the styloid
process, the mandible and the tympanic plate.
A portion of the deep lamina extending between the
styloid process and the mandible, is thickened to form
the stylomandibular ligament which separates the parotid
glands from submandibular salivary gland.
The attachments of the Parotid fascia include :
Anterior – Mandible
Inferior – Stylomandibular ligament
Posterior –Styloid process

Surface Marking [5] The parotid gland is marked by joining the following
four points with each other.
a
b
c
d

a) The first point at theupper border of thehead of themandible.
b) The second pointjust above the centerof the massetermuscles.
c) The third pointposteroinferior toangle of mandible.
d) The fourth point isanterior border ofthe mastoid process.

External Features. [1] [2] [5]
The gland resembles a three sided pyramid. The apex
of the pyramid is directed downwards.
The gland has four surfaces:-
1) Superior (base of the pyramid)
2) Superficial
3) Anteromedial and
4) Posteromedial
The surfaces are separted by 3 borders:
a) Anterior b) Posterior and 3) Medial

Apex
Superior surface(Base)
Superficialsurface
Posterior border
Medial border
Anterior border
Development [5] [6] [7]
The parotid salivary glands appear early in the fourth week
of prenatal development and are the first major salivary
glands formed as an ectodermal furrow.
The epithelial buds of these glands are located on the inner
part of the cheek, near the labial commissures of the
primitive mouth.
These buds grow posteriorly toward the otic placodes of the
ears and branch to form solid cords with rounded terminal
ends near the developing facial nerve.

Later, at around 10 weeks of prenatal development,
these cords are canalized and form ducts, with the
largest becoming the parotid duct for the parotid
gland.
The rounded terminal ends of the cords form the
acini of the glands. Secretion by the parotid glands
via the parotid duct begins at about 18 weeks of
gestation. Again, the supporting connective tissue
of the gland develops from the surrounding
mesenchyme.

Relations [1] [2] [3]
The apex:
It overlaps the posterior belly of the diagastric and the
adjoining part of the carotid triangle. The cervical
branch of the facial nerve and the two divisions of the
retromandibular vein emerge through it.

The superior surface or base forms the upper end of
the gland :
It is small and concave. It is related to:
(a) The cartilagious part of the external acoustic
meatus.
(b) the posterior surface of the temporo mandibular
joint
(c) the superficial temporal vessels.
(d) the auriculotemporal nerve.

The superficial surface:
It is the largest of the four surfaces. It is covered with:
(a) Skin
(b) Superficial fascia containing the anteriorbranches of great auricular nerve, the perauricular orsuperficial parotid lymph nodes and the posteriorfibers of the platysma and risorius.
(c) the parotid fascia which is thick and adherent togland .
(d) a few deep parotid lymph nodes embedded in thegland.

The anteromedial surface:
It is grooved by posterior border of the ramus of the
mandible.
It is related to:
(a) The Masseter
(b) The lateral surface of temporomandibular joint.
(c) The posterior border of the ramus of the
mandible.
(d) The medial pterygoid.
(e) The emerging branches of the facial nerve.
The posteromedial surface:
It is moulded to the mastoid and styloid processes
and the structures attached to them.
They are related to:
(a)The mastoid process, with the sternocleidomastoid
and posterior belly of diagastric.
(b) The styloid process
The external carotid artery enters the gland through
this surface and internal carotid artery lies deep in the
styloid process.

Anterior border
Separates superficial surface from anteromedial
surface.
Structures which emerge at this border
Parotid Duct
Terminal Branches of facial nerve
Transverse facial vessels
Posterior Border
Separates superficial surface from
posteromedial surface
Overlaps sternocleiodomastoid.
Medial Border
Separates anteromedial surface from
posteromedial surface
Related to lateral wall of pharynx

Structures within the Parotid Gland [2] [3] Arteries
• The external carotid artery
• The maxillary artery
• Superficial temporal vessels
• The posterior auricular artery
Superficial temporal Artery
Maxillary Artery
Posterior auricular artery
External carotid

Veins
The retromandibular veins is formed within thegland by the union of the superficial temporal andmaxillary veins. In the lower part of the gland, thevein divides into anterior and posterior divisionswhich emerge at the apex of the gland.
Superficial temporal Vein
Maxillary Vein
Post auricular Vein
External jugular vein
Common Facial Vein
Retromandibular vein
Posterior division Anterior division
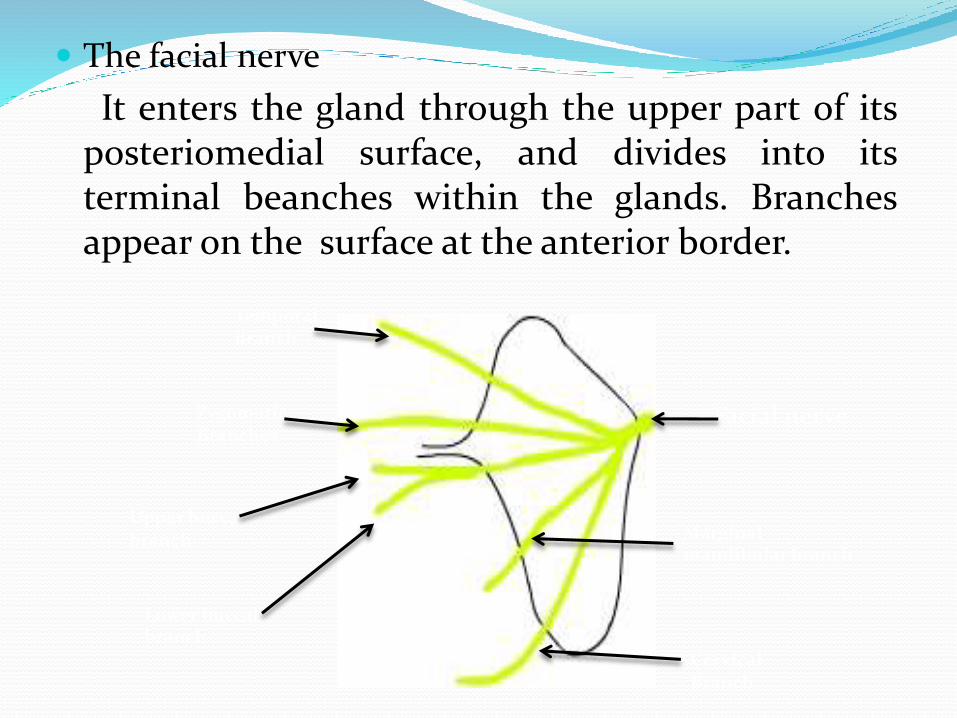
The facial nerve
It enters the gland through the upper part of itsposteriomedial surface, and divides into itsterminal beanches within the glands. Branchesappear on the surface at the anterior border.
Facial nerve
Temporal Branch
ZygomaticBranches
Upper buccal branch
Lower buccal branch
Marginal mandibular branch
Cervical Branch
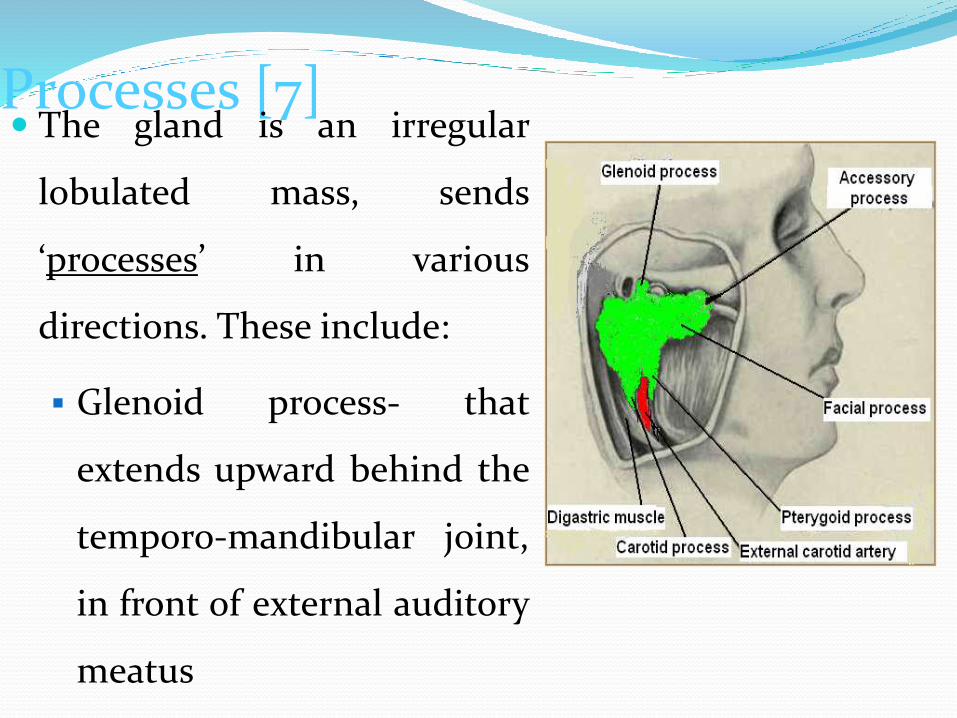
Processes [7] The gland is an irregular
lobulated mass, sends
‘processes’ in various
directions. These include:
Glenoid process- that
extends upward behind the
temporo-mandibular joint,
in front of external auditory
meatus

Facial process- that
extends anteriorly
onto the masseter
muscle
Accessory process
(part)- small part of
facial process lying
along the parotid duct

Pterygoid process-that
extends forward from the
deeper part, lies between
the medial pterygoid
muscle & the ramus of
mandible
Carotid process-that lies
posterior to the external
carotid artery

Parotid Duct [5] [6] [8]
ductus parotideus; Stensen’s duct
It is thick walled and about 5cm long
and 5 mm in diameter
Carries saliva to the oral cavity.
Course :-
Forms by the union of smaller duct from the
gland and run forwards and slightly downward on
the masseter.

Relations
Superiorly:
(a) Accessory parotid gland.
(b) upper buccal branch of the facial nerve.
(c) the transverse facial vessels.
Inferiorly:
(a) The lower buccal branch of the facial nerve.

At the anterior border of the masseter, it turns
medially and pierces:
(a) the buccal pad of fat.
(b) the buccalpharyngeal fascia
(c) the buccinator
“Because of the oblique course of the duct through
the buccinator infaltion of the duct is prevented
during blowing.”
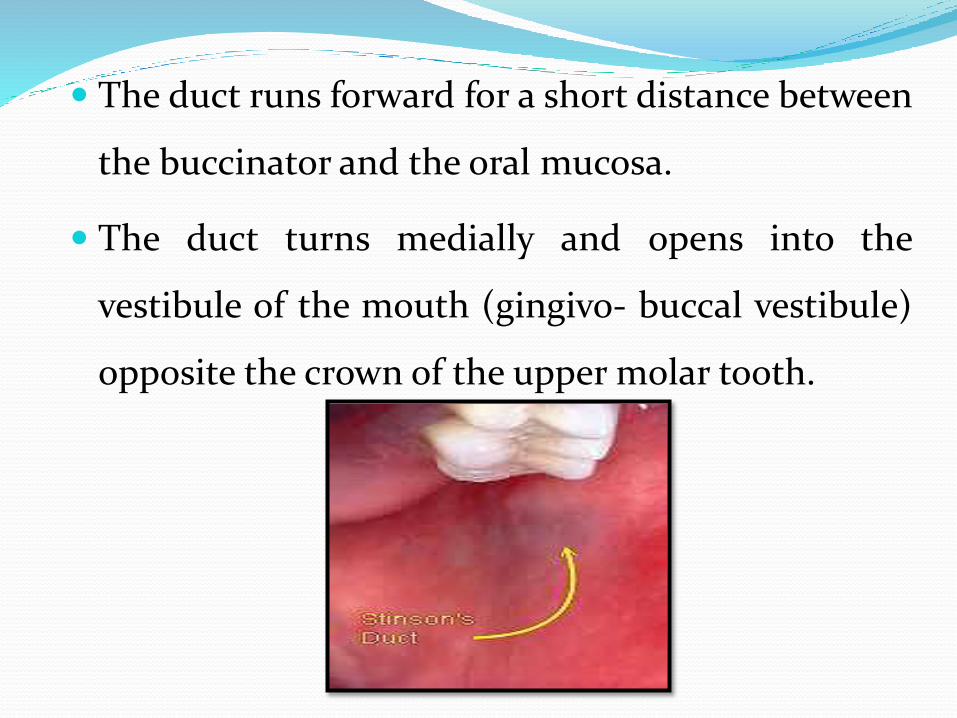
The duct runs forward for a short distance between
the buccinator and the oral mucosa.
The duct turns medially and opens into the
vestibule of the mouth (gingivo- buccal vestibule)
opposite the crown of the upper molar tooth.
Nerve Supply [1] [5] [9]
PARASYMPATHETIC(SECRETOMOTOR)
SUPPLY-derived from auriculo temporal nerve
Its stimulation produces watery secretion.
They reaches the gland through the
auriculotemporal nerve.
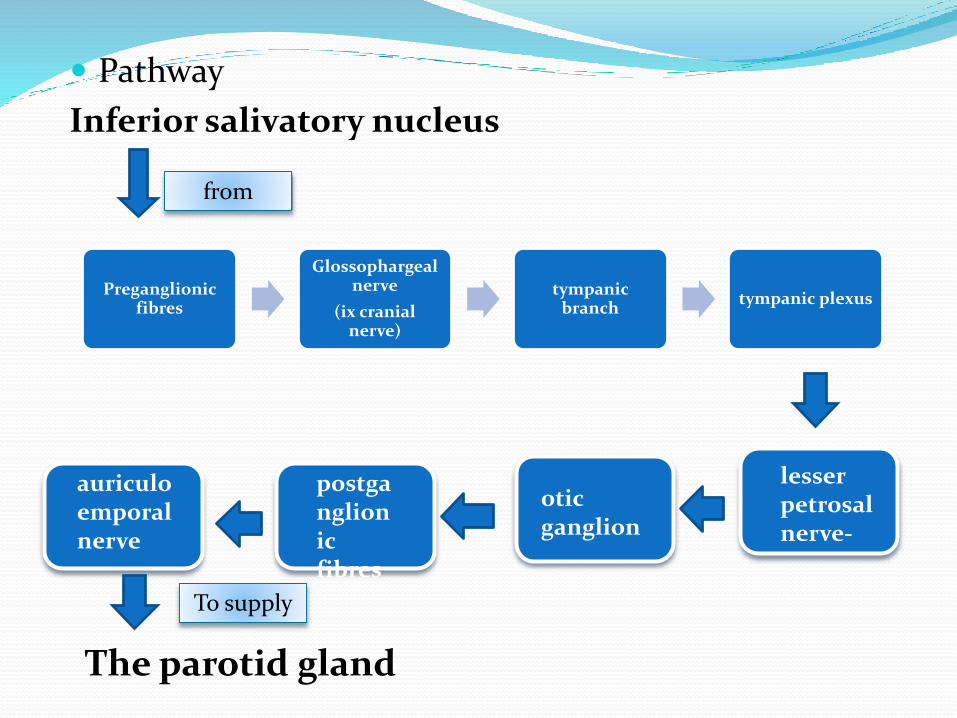
Pathway
Inferior salivatory nucleus
Preganglionicfibres
Glossophargealnerve
(ix cranial nerve)
tympanic branch
tympanic plexus
from
lesser petrosalnerve-
oticganglion
postganglionic fibres
auriculoemporalnerve
The parotid gland
To supply

SYMPTHETIC SUPPLY- they are vasomotor, and
are derived from the plexus around the external
carotid artery.
Stimulation produces thick sticky secretion.
SENSORY NERVES-comes from the
auriculotemporal nerve, but the parotid fascia is
innervated by the sensory fiberes of the great
auricular nerve.

Lympatic Drainage [9] [10] Lymph drains first to the parotid nodes and from there
to the upper deep cervical nodes.

Parotid lymph nodes The parotid lymph nodes lie partly in the superficial fascia and
partly deep to the deep fascia over the parotid gland.
They drain:-
(a) the temple
(b) the side of the scalp
(c) the lateral surface of the auricle
(d) the external acoustic meatus
(e) the middle ear
(f) the parotid gland

(g) the upper part of cheek
(h) parts of the eyelids
(i) orbit
Efferents from these nodes pass to the upper
groups of the deep cervical nodes.

Histology [4] [7] The salivary glands are a
group of compound exocrine
glands secreting saliva.
Salivary glands are composed
of serous and mucous acini, the
proportions of which
determine the type of salivary
secretion from each duct.

The Secretory Unit
– Acinus (serous, mucous, mixed)
– Myoepithelial cells
– Intercalated duct
– Striated duct
– Excretory duct

The parotid gland is a pure serous gland.
All acinar cells are similar in structure to the serous
cells. In the infants, however, a mucous secretory units
may be found.
The intercalated ducts of the parotid gland are long
and branching and numerous in striated ducts.
The connective tissue septa in the parotid contain
numerous fat cells, which increases in number with
age and leave an empty space in histological sections.

Functions of parotid glands [9]
[10] [11]
Protection of the oral cavity and oral enviroment: the
constant secretion of saliva prevents desiccation of oral
cavity.
Lubrication and cleansing oral cavity:
provides a washing action to flush away debris
and nonadherent bacteria and provide
lubrication for smooth and sliding movement.
Initiation of starch digestion: the action of
amylase on ingested carbohydrate to produce
glucose and maltose in the mouth.
Immunological: defensive substance in saliva are
the immunoglobulins. The perdominant salivary
immunoglobulin is IgA.
Parotid gland is the largest, provides 65% of the
total salivary volume. Normal outflow is 1-2L/day.

Clinical considerations [9] Diseases of parotid gland
1) Congenital
Aplasia or atresia- any one or group of salivary
glands may be absent, unilaterally or bilaterally.
Aplasia occurs for unkown reasons in conjunction
with other development defects such as hemifacial
microsomia, the LADD syndrome and mandibulo-
facial dysostosis.

Salivary loss leads to increased caries, burning
sensation, oral infections, taste aberrations and
difficulty with denture retention.

2) AcquiredInfective
MumpsBacterial sialadentitis
AutoimmuneSjögren's syndrome
InflammatorySialadenitis
NeurologicalFrey's syndrome

Neoplastic
Salivary gland neoplasm
Idiopathic
Sialolithiasis
Sialadenosis
Mumps [10]
Its a viral disease of the human species, caused by
the mumps virus Paramyxovirus.
Transmitted by direct contact, droplet spread, or
contaminated objects.
Painful swelling of the parotid gland.

Fever and headache are the
main symptoms of mumps,
together with malaise and
anorexia. Other symptoms of
mumps can include dry
mouth, sore face and/or ears
and occasionally in more
serious cases, loss of voice.

It was a common childhood diseases worldwide.
The disease is generally self-limiting, running its
course before receding, with no specific treatment
apart from controlling the symptoms with pain
medication.
Bacterial parotitis [11] [16]
It can be acute, chronic and recurrent.
The most common pathogens associated with
acute bacterial parotitis are Staphylococcus aureus
and anaerobic bacteria. The predominant
anaerobes include gram-negative bacilli.
It often occurs in the setting of debilitation,
dehydration, and poor oral hygiene, particularly
among elderly postoperative patient

Once an abscess has formed
surgical drainage is required. The
choice of antimicrobial depends
on the etiologic agent.
Maintenance of good oral hygiene,
adequate hydration, and early and
proper therapy of bacterial
infection of the oropharynx may
reduce the occurrence of
suppurative parotitis.

Sjögren's syndrome [7] [8]
Chronic inflammation of the salivary glands may
also be an autoimmune disease known as Sjögren's
syndrome
The disease most commonly appears in people
aged 40–60 years, but it may affect small children.
Women versus men is approximately 9:1.
The involved parotid gland is enlarged and tender at
times.
The cause is unknown. The syndrome is often
characterized by excessive dryness in the eyes, mouth,
nose, vagina, and skin



Frey’s Syndrome [12] [13]
Also known as gustatory sweating or auriculo-
temporal nerve syndrome.
Commonly occurs after parotid surgery or trauma.
It reflects the aberrant innervation of sweat glands
on the face by regrowing parasympathetic
secretomotor axons that would have previously
innervated the parotid gland.

It is characterized by
o Sweating
oWarmth
oRedness of the face
as a result of salivary
stimulation by the smell or
taste of food
There is no effective treatment, but various options
are:-
Injection of Botulinum Toxin A.
Surgical transection of the nerve fibers (only a
temporary treatment).
Application of an ointment containing an
anticholinergic drug such as scopolamine.

Sialadenitis (sialoadenitis) [11] [12]
It is the inflammation of asalivary gland. It may besubdivided into acute, chronicand recurrent forms.
Acute
• sialolithiasis
• decreased flow (dehydration,post-operative, drugs)
• poor oral hygiene
• exacerbation of low grade chronicsialoadenitis
Clinical features
• Painful swelling
• Reddened skin
• Edema of the cheek, Periorbital region and neck
• low grade fever
• malaise
• raised ESR, CRP, leucocytosis
• purulent exudate from duct punctum

Chronic
• Clinical Features unilateral
• mild pain / swelling
• common after meals
• duct orifice is reddened and flow decreases
• may or may not have visible/palpable stone.
• Recurrent painful swellings

Treatment
• In chronic recurrent sialadenitis or chronic
sclerosing sialadenitis, acute attacks are managed
with conservative therapies such as hydration,
analgesics (mainly NSAIDs), sialogogues to
stimulate salivary secretion, and regular, gentle
gland massage.
• If infection is present, appropriate cultures should
be obtained, followed by empirical antibiotic
therapy initially, for example
amoxicillin/clavulanate or clindamycin which
cover oral flora.
If there are attacks more than approximately 3
times per year or severe attacks, surgical excision
of the affected gland should be considered.

Salivary gland neoplasm [7] [10] [12] [13]
Salivary gland cancer is a cancer that forms in tissues
of a salivary gland.
Salivary gland cancer is rare, with 2% of head and neck
tumors forming in the salivary glands, the majority in
the parotid.
Salivary gland neoplasms are classified by the World
Health Organization as primary or secondary, benign
or malignant, and by tissue of origin. This system
defines five broad categories of salivary gland
neoplasms.

Malignant epithelial tumors (e.g. acinic cell carcinoma,
mucoepidermoid carcinoma and adenoid cystic carcinoma,
salivary duct carcinoma)
Benign epithelial tumors (e.g. pleomorphic adenoma,
myoepithelioma and Warthin tumour, sebaceous
lymphadenoma)
Soft tissue tumors (Hemangioma)
Hematolymphoid tumors (e.g. Hodgkin lymphoma)
Secondary tumors.

MUCOEPIDERMOID CARCINOMA PLEOMORPHIC ADENOMA
HEMANGIOMA

Signs and symptoms
Signs include fluid draining from the ear,
pain, numbness, weakness, trouble
swallowing, and a lump.
The most common symptom of major
salivary gland cancer is a painless lump in
the affected gland, sometimes accompanied
by paralysis of the facial nerve.

Causes
The chief risk factor is chewing tobacco, followed by
smoking. Other risk factors include older age,
radiation therapy treatment to head or neck, and
being exposed to certain carcinogenic substances at
work.
Treatment
• Surgery with or without radiation.
• Radiation therapy.
• Chemotherapy.

Sialolithiasis [11] [12]
Sialolithiasis (also termed salivary calculi, or
salivary stones), is a condition where a calcified
mass forms within a salivary gland, usually in the
duct of the submandibular gland (also termed
"Wharton's duct"). Less commonly the parotid
gland.

Signs and symptoms
Signs and symptoms are variable and depend largely
upon whether the obstruction of the duct is complete
or partial, and resultant pressure created within the
gland. The development of infection in the gland also
influences the signs and symptoms.

Pain, which is intermittent, and may suddenly get
worse before mealtimes, and then slowly get better
(partial obstruction).
Swelling of the gland, also usually intermittent, often
suddenly appearing or increasing before mealtimes,
and then slowly going down (partial obstruction).

Tenderness of the involved gland.
Palpable hard lump, if the stone is located near the
end of the duct. If the stone is near the submandibular
duct orifice, the lump may be felt under the tongue.
Lack of saliva coming from the duct (total
obstruction).
Erythema (redness) of the floor of the mouth
(infection).
Pus discharging from the duct (infection).
Cervical lymphadenitis (infection).

Treatment
Non-invasive: For small stones, hydration, moist heat
therapy, NSAIDs (nonsteroidal anti-inflammatory drugs)
Some stones may be massaged out by a specialist.
Shock wave therapy (Extracorporeal shock wave
lithotripsy).
Minimally invasive: Sialendoscopy
Surgical
Supporting treatment: To prevent infection while
the stone is lodged in the duct, antibiotics are
sometimes used.

Role of public health dentist [15]
During the treatment of oral cancer affecting
salivary glands leading to surgical removal of the
glands, leads to decreased or no saliva secretion.
This increases the incidence of dental caries.
Patient under the high dose of radiation therapy
reduce the quality and quantity of normal saliva,
causing radiation caries.
Fluoride application
Maintaining the periodontal health.
Educating about proper nutrition and good oralhygiene.
Dentures reconstruction in case of altered oral tissue.
Educating and motivating people about tobaccocessation.

Conclusion The parotid glands are a pair of mainly serous salivary
glands located inferior and anterior to the external acoustic
meatus, draining their secretions into the vestibule of oral
cavity through the Stensen duct or parotid duct.
The parotid gland also secretes salivary alpha-amylase
(sAA), which is the first step in the decomposition of
starches during mastication.

Parotid gland is the largest, it provides 65% of the total
salivary volume. The serous cell predominates in the
parotid, making the gland secrete a mainly serous
secretory product.
Apart from viral infection, other infections, such as
bacterial, can cause parotitis (acute suppurative
parotitis or chronic parotiti). These infections may
cause blockage of the duct by salivary duct calculi or
external compression.
About 80% of tumors of the parotid gland are benign.
Surgical treatment of parotid gland tumors is
sometimes difficult because of the anatomical
relations of the facial nerve parotid lodge, as well as
the increased potential for postoperative relapse. Thus,
detection of early stages of a parotid tumor is
extremely important.

References 1) Guyton and Hall ;Textbook of medical physiology
9th edition pg no. 223-254.
2) Tortora-Derrickson; Principal of anatomy and
physiology,12th edition pg no. 112-114.
3) Chaudhuri; Concise medical physiology , 2nd
edition. Pg no. 34-36.
4) A.K.Jain Human physiology ,1st edition. Pg no. 454-
456.

5) K.Sembulingum,P.Sembulingum;Essentials of
medical physiology,4th edition pg no.555-557.
6) Burket’s ;Oral medicine ,11th edition pg. no. 211-213.
7) Principal of anatomy and physiology- tortora-
derrickson ,12th edition.
8) Richard Tencate ;ORAL HISTOLOGY-5th edition pg.
no. 339-342.
9) Robert M Bradley ;ESSENTIALS OF ORAL
PHYSIOLOGY pg. no. 221-223
10) G.Neil Jenkins ;The physiology and biochemistry of
the mouth, 4th edition pg.no. 11-13
11) Christopher L B Lavelle ;APPLIED ORAL
PHYSIOLOGY-2nd edition.
12) Greenberg& Glick ;BURKETS ORAL MEDICINE-
10th edition pg. no. 41-43
13) Shafer,Hine & Levy ;Textbook of Oral Pathology
6th edition pg. no. 134-144.
14) Saliva:its secretion,composition&functions.-
British Dental Journal 1992; 172:305

15) The effect of saliva on dental caries George K.
Stookey, MSD, PhD
10.14219/jada.archive.2008.0347 2008;139(suppl
2):11S-17SJADA
16) J Craniofac Surg. 2003 Jan;14(1):37-40.
Acute bacterial suppurative parotitis:
microbiology and management.
