parkinson’s disease by rachel cheong. what is parkinson’s disease? refers to idiopathic/...
TRANSCRIPT

PARKINSON’S DISEASEBy Rachel Cheong

WHAT IS PARKINSON’S DISEASE?
Refers to Idiopathic/ Primary Parkinson’s Disease
Parkinsonism of unknown aetiology
Parkinsinonism= tremor at rest, stiffness, slowing of movement and postural instability.
Part of the Movement Disorders known as Akinetic-Rigid syndromes
Akinetic-Rigid Syndromes= slowed movement, increased tone
Dyskinesias= added, uncontrollable movements
Definition: Degenerative, progressive disease affecting the zona compacta of the substantia nigra in the basal ganglia associated with decreased levels of dopamine

Akinetic-Rigid Syndromes Dyskinesias
Idiopathic Parkinson’s Disease Essential tremor
Drug-induced Parkinsonism Chorea
MPTP-induced Parkinsonism Hemiballismus
Postencephalitic Parkinsonism Myoclonus
Parkinsonism-plus Tics
Wilson’s Disease Dystonias
Childhood akinetic-rigid syndromes
Paroxysmal dyskinesias

IDIOPATHIC PARKINSON’S DISEASE
Described in 1817 by James Parkinson- “The Shaking Palsy”
Prevalence: 65.6 per 100,000 to 125 per 100,000.
UK Incidence= approx. 128,000 cases
Incidence increases severely with age:
from 17.4 in 100,000 person years between 50 and 59 years of age to 93.1 in 100,000 person years between 70 and 79 years
Slightly more common in men
Insidious onset and progression
Studies suggest patients born in the spring have a higher incidence of PD
Characterized by accumulation of alpha-synuclein into Lewy bodies in the neurons as a hallmark

Related factors:
Nicotine: inverse relationship as acts like MAO-B inhibitors and stimulates dopamine
Caffeine may be protective
MPTP: methylphenyltetrahydropyridine (illicit stimulant/herbicides) causes severe parkinsonism
Encephalitis Lethargica: parkinsonism post-encephalitis
Genetics:
(a) Familial clusters of early-onset PD
(b) Mutations on Parkin gene on Chr 6 (under 40s; AR)
(c) α-synuclein gene mutation on Chr 2p13
(d) Ubiquitin carboxyl terminal hydrolase L1 (UCHL1) gene on Chr 4p14-16.3
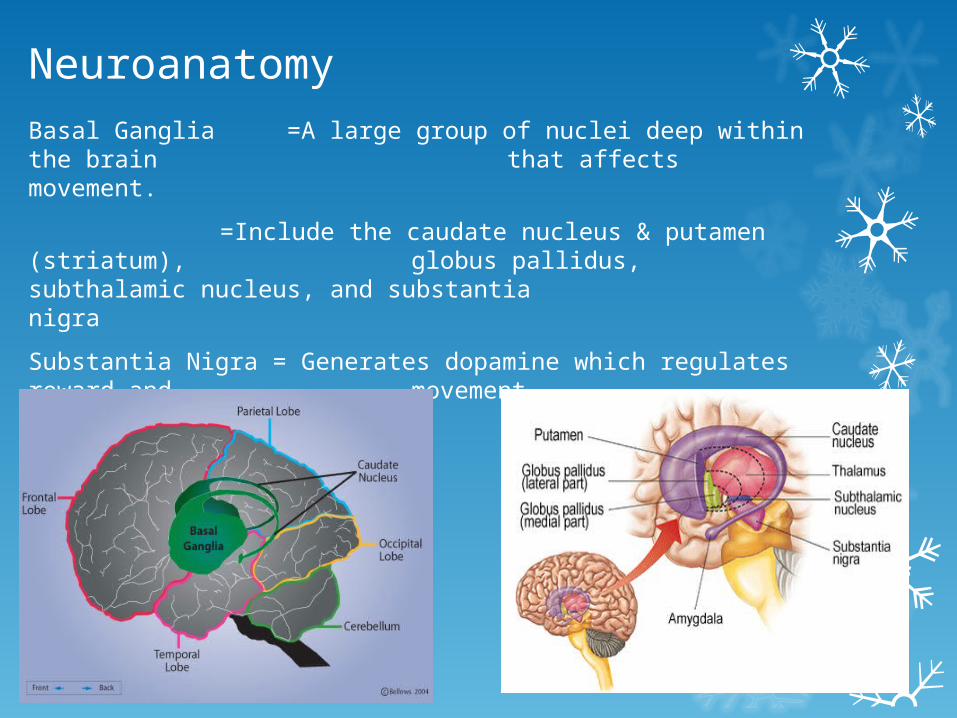
NeuroanatomyBasal Ganglia =A large group of nuclei deep within the brain
that affects movement.
=Include the caudate nucleus & putamen (striatum), globus pallidus, subthalamic nucleus, and substantia nigra
Substantia Nigra = Generates dopamine which regulates reward and movement.
PATHOPHYSIOLOGY•The basal ganglia and the cerebellum transmit information via the thalamus to the cerebral cortex to regulate movement.
•In a healthy brain, the neurons in the substantia nigra release dopamine into the striatum modulates neuronal activity affects movements + behaviours.
• In Parkinson's disease, there is a breakdown in the connection between the striatum (neuron cells die/become impaired) decreased dopamine levels
• Symptoms of Parkinson's disease appear after:
•60% - 80% of the neuronal cells become impaired or die.
•Striatal dopamine levels have decreased by 20% - 50% of normal levels
•Subsequently, globus pallidus interna and subthalamic nucleus begin to function abnormally Loss of control of motor function.
SIGNS & SYMPTOMS1. Tremor- 4-7Hz pill-rolling tremor at rest (decreases with action)
2. Rigidity- lead-pipe/plastic rigidity, more marked on one side; Cogwheeling when occurs with tremor.
3. Akinesia/ Bradykinesia- poverty/slowing of movement; difficulty initiating movement; loss of fine-finger movements; micrographia; mask-like facial expression; serpentine stare (decreased blinking)
4. Postural/Gait Change- Stooping (Simian); festinant/shuffling gait with poor arm swing; balance deterioratesfalls
5. Monotonous, tremulous speech slurring dysarthria anarthria
6. Cognitive decline
7. Depression, Apathy, Anxiety
8. GI Sx- constipation, heartburn, dribbling, dysphagia, weight loss, urinary difficulties
9. Others- greasy skins, excessive sweating
10. Insomnia

DIAGNOSISo Clinical diagnosis
o NICE recommends using the UK Parkinson's Disease Society (PDS) Brain Bank Criteria for diagnosis:
• Step 1: diagnosis of Parkinsonian syndrome
Bradykinesia + ≥ 1 of : Muscular rigidity.4- to 6-Hz resting tremor.Postural instability not caused by primary visual, vestibular, cerebellar or proprioceptive dysfunction.
• Step 2: exclusion criteria for Parkinson's disease:History of CVA/ step-wise progression/ head trauma/ /
autonomic+cerebellar Sx/ Exposure to known drugs/ Negative response to Dopa trial/ Early severe
dementia

Step 3: supportive prospective positive criteria of Parkinson's disease
Three or more are required for the diagnosis of definite PD:
Unilateral onset.
Rest tremor present.
Progressive disorder.
Persistent asymmetry affecting the side of onset most.
Excellent response (70-100%) to L-dopa.
Severe L-dopa-induced chorea.
L-dopa response for five years or more.
Clinical course of ten years or more.
Hyposmia.
Visual hallucinations.

Investigations
To exclude other causes
CT/MRI: Exclude supratentorial tumours, normal pressure hydrocephalus and extensive subcortical vascular pathology.
Positron emission tomography (PET) scanning: with fluorodopa to localise dopamine deficiency in the basal ganglia
Transcranial sonography: differentiate PD from atypical or secondary Parkinsonian disorders, for early diagnosis of PD and for detection of subjects at risk for PD.
Genetic testing- eg, Huntington's gene, single-gene mutations in familial PD
Olfactory testing: differentiate PD from other Parkinsonian disorders
For young-onset or atypical disease: measurement of ceruloplasmin levels (Wilson's disease) and syphilis serology.

Management NICE suggests specialist review every 6-12 months for clinical
monitoring and medication adjustment
Multidisciplinary management including specialist nurses, OT, physiotherapy, SALT, psychologists, social services
Pharmacological Treatment:
Levodopa
Dopamine agonists
MAO-BIs
COMT inhibitors
Amantadine
Apomorphine
Antimuscarinic drugs
Surgical Treatment
Palliative Care

Levodopa
Most effective/ most responsive
Given with a peripheral dopa-decarboxylase inhibitor, which prevents peripheral conversion to dopamine
Eg: Sinemet, Madopar
Use lowest effective dose, eg: Sinemet 62.5 mg TDS increased to 125 mg after two weeks
Adverse effects rare/mild: nausea, dizziness, weight loss
Dopamine agonists
Treats motor features
Used in early disease, younger patients
Can be adjuvant to Levodopa
More severe/common adverse effects than Levodopa
Non-ergot derivatives preferred, eg: pramipexole and ropinirole
Ergot-derivatives, eg: bromocriptine, cabergoline, lisuride and pergolide (Monitor renal function)

MAO-B Inhibitors
Eg: Selegiline, Rasagiline
Early treatment with selegiline alone can delay the need for levodopa therapy
Addition of selegiline to a levodopa/decarboxylase inhibitor combination is more effective when introduced at 5 years from onset
COMT Inhibitors
Eg: Entacapone, Tolcapone
Reversibly inhibit the peripheral breakdown of levodopa by the COMT enzyme
Increases the amount available for conversion to dopamine in the brain and reducing fluctuations in plasma levels.
Benefits patients with levodopa motor fluctuations

Antimuscarinic drugs
Eg: orphenadrine, procyclidine and trihexyphenidyl
Improves motor function but common neuropsychiatric and cognitive S/E
Reduces drug-induced Parkinsonism
Amantadine
monotherapy in early PD (for tremor or bradykinesia)
weak and short-lived benefit; used as adjuvant later
Apomorphine
Given subcutaneously
Used as a rescue agent in advanced disease to provide rapid but short-lived benefit for sudden, severe 'off' episodes
use intermittent injections to reduce 'off time' and continuous infusion to reduce 'off time' and dyskinesias

Surgical Treatment
Developed in the mid-twentieth century before the advent of effective medical therapy.
Recently enjoyed a resurgence
Pallidotomy
Subthalamic Surgery
Thalamic Surgery
Deep Brain Stimulation

Complications “Wearing Off Phenomenon” or “On-Off Fluctuations”
Dyskinesias
Depression & Anxiety
Hallucinations & Psychosis
Dementia
Compulsive Behaviours
Parkinsonian Crisis
-Acute akinesia
-rare but life-threatening complication
-sudden worsening of motor symptoms and severe akinesia.
-Triggers include infections, surgery, gastrointestinal disease and changes in medication.
-Acute akinesia is difficult to treat and often needs hospital admission

Parkinson’s Plus Syndrome Multiple System Atrophy
-Shy-Drager Syndrome
-autonomic dysfunction, parkinsonism, ataxia
Progressive Supranuclear Palsy
-Steele-Richardson-Olszewski syndrome
-Supranuclear ophthalmoplegia, neck dystonia, Parkinsonism, Pseudobulbar palsy, behavioral and cognitive impairment, imbalance and difficulties walking, frequent falls
Corticobasal Degeneration
-Parkinsonism, Alien Hand Syndrome, Apraxia, Aphasia
Pick’s Disease
-frontotemporal dementia, progressive nonfluent aphasia, impaired social conduct, passivity/anxiety

Case Scenario A 64 year old man attends his GP after his wife made him
come. For the last 6 months he has noticed that he is slowing down. It takes him a long time to do simple tasks like getting dressed. His hands are shaking all the time, more so on the right. His wife has noticed a change in his gait saying he shuffles when he walks. He has no past medical history of notes and is on no regular medication and has no known allergies. On examination he has a blank staring expression and marked rigidity of his limbs, more so on the right. He has resting pill rolling tremor. His gait is shuffling and festinant
What is your differential diagnosis?
What are the key Sx leading to your DDx?

References
NICE Guidelines http://www.nice.org.uk/nicemedia/live/10984/30088/30088.pdf
University of Minnesota- Neurology Teaching Webpage
Kumar & Clark Pg. 1144-1147
Oxford Handbook Pg. 368-369, 534
Patient Plus Reference http://www.patient.co.uk/doctor/parkinsons-disease-management
International Parkinson’s and Movement Disorders Society http://www.movementdisorders.org/disorders/parkinson.php