parent information project report v0.2 - ministry of health
TRANSCRIPT

Parent Information Project Report

Citation: Ministry of Health. 2010. Parent Information Project. Wellington: Ministry of Health.
Published in March 2010 by the Ministry of Health
PO Box 5013, Wellington, New Zealand
ISBN 978-0-478-33935-2 HP 4967
This document is available on the Ministry of Health’s website: http://www.moh.govt.nz

Parent Information Project iii
Contents
Executive Summary vi
Introduction 1
What Information and Advice Do Parents Want? 4 What information and advice do New Zealand parents want? 4
What Information and Advice Do Parents Need? 6 What information and advice do New Zealand parents need? 6
What Methods of Providing Information to Parents Are Available? 8 Telephone 9 Internet 9 DVDs 10 Email 11 Radio and television 12 CD-ROMs 13 Printed material 13 What New Zealand professionals said 14
What Methods Do Parents Prefer? 16
The Use of the Internet by Parents 17 Why parents use the internet 17 Websites designed for use by parents and children 21
The Quality of Health Information Available on the Internet 22 Is the information true? 22 Is the information on websites understandable? 22 What future standards are there for health information? 23
Telephone Health Lines 24 What is telephone triage/teletriage? 24 Child health telephone lines 26 Maternal and child health lines in the USA 27 Overall findings 31
Text Messaging 32 Mobile phones 32
Support 35 What is peer support and why is it important? 35 Peer telephone interventions for new mothers 36 The experience of being a peer telephone supporter 37

Parent Information Project iv
Content of peer support interventions 38 Training and experience of peer supporters 39
Findings and Recommendations 40 Major findings in this report 40 Principle underpinning the recommendations 41 Recommendations for provision of Well Child telephone and internet services 41
Bibliography 43
Appendix 1: Questionnaire Used in Telephone Survey of Parents 67 A Information sought 68 B Sources used and usefulness of each 70 C Preferences for providers/sources 71 D Plunket/Well Child Tamariki ora 73 E Demographics 73 Conclusion 76 Termination 76
Appendix 2: Results of Telephone Survey of Parents 77 Parent Information Summary Report – 1 July 2009 77 Parent Information Survey Results – 1 July 2009 81
Appendix 3: Websites Designed for Use by Parents and Children 109 Australia 109 Canada 110 England 110 New Zealand 110 Scotland 111 USA 111 Podcasting 111 Internet quality criteria 112 Well Child 113 Australia parent websites 113 UK parent websites 113 New Zealand parent websites 114 Australia parentlines 115 McKesson 115 UK parentlines 115 USA parent websites 115 New Zealand parentlines 115 HTA 116 Canada parentlines 116 Canada parent websites 116 USA child health 116 USA parentlines 116
Parent Information Project v
List of Tables Table 1: Topics that parents had sought or been given information about 5 Table 2: New Zealand health professionals’ views on what information parents need (%) 7 Table 3: Overview of the telephone as a method of information delivery 9 Table 4: Overview of the internet as a method of information delivery 10 Table 5: Overview of DVDs as a method of information delivery 11 Table 6: Overview of email as a method of information delivery 11 Table 7: Overview of radio and television as methods of information delivery 12 Table 8: Overview of CD-ROMS as a method of information delivery 13 Table 9: Overview of printed material as a method of information delivery 14 Table 10: Extent to which New Zealand health professionals agree with their Australian
counterparts on methods of information delivery (%) 15 Table 11: New Zealand parents’ preferences for Well Child information sources and perceived
utility of those sources (%) 16 Table 12: Data from Dennis et al’s (2002) study of peer support on duration of breastfeeding 36 Table 13: Data from Dennis’s (2003) study of peer support on postnatal depression symptoms 37
List of Figures Figure 1: Delivery model for remote access to information and advice on demand 2

Parent Information Project vi
Executive Summary This report is the result of the Parent Information Project, which was carried out over 2008/09. This project aimed to determine the best ways to provide on-demand Well Child information, advice and support to parents. Well Child services focus on promoting the health and development of all children and providing support to parents. Services for sick or symptomatic children are specifically excluded from the definition of Well Child services. In reviewing the literature and surveying parents, we found that Well Child could not be discussed in isolation to other information and advice services for parents including teletriage. However, the analysis and recommendations that are made here are limited to the scope of Well Child information and advice services. Parents describe face-to-face contact with health professionals as the most important source of information. Therefore, provision of information and advice on demand is intended to complement rather than be a substitute for face-to-face Well Child services delivered in the community. The following questions are at the heart of this research. • What information and advice do parents want? • What information and advice do parents need? • How do they get that now? • How could they get that in the future? The delivery model for remote access to information and advice on demand that emerged from this project is made up of three components: support, access to services, and information. Each of these bundles of services can only be delivered through telecommunications systems, which then raises issues regarding access. Around the world, the internet is the second-most frequently used and second-most preferred source of health information for parents, after consulting their health care provider. Most parents find it a helpful resource, particularly to enhance knowledge and understanding of a particular condition. However, the distinction between the internet and telephone health services has become blurred and, in many cases overseas, meaningless. In the latter instances the telephone healthline and the website have been integrated and services that in the past were only available by telephone are now able to be accessed by email or text and delivered in that way too. The major finding of this project has been that parents need different kinds of information, in different forms, at different times. These information services need to be reliable, accurate and trusted, and to reinforce the information, advice and support that parents receive through related face-to-face services. Combining the findings from the Well Child Framework Review with the Parent Information Project, the Ministry of Health has concluded that a one-stop national Well Child information and advice service is an integral part of delivering Well Child services and that this service must be intimately linked to face-to-face Well Child services.

Parent Information Project vii
Telephone, website and DVD resources have been shown to be effective in delivering information, advice and support to parents. The Ministry is investigating how these services can be implemented to provide integrated Well Child information, advice and support services that include Well Child/Tamariki Ora visits, telephone, website and DVD services.

Parent Information Project 1
Introduction In 2006 the Ministry of Health commenced a review of the Well Child/Tamariki Ora Framework. The aim of the review was to see if the current schedule of services was meeting the needs of young children and their families/whānau. The review recommended that Well Child services should place a greater emphasis on addressing issues such as parent–infant attachment, postnatal depression and family violence. The review also found that there were opportunities to improve outcomes for young children and their families/whānau through better co-ordination and integration of the range of Well Child services that are currently provided. One of the projects resulting from the Well Child Review was the Parent Information Project. This project aimed to determine the best ways to provide Well Child information, advice and support to parents remotely and on demand. Because parents describe face-to-face contact as the most important source of information, provision of information and advice remotely and on demand is intended to complement rather than be a substitute for face-to-face Well Child services delivered in the community. In determining the best ways to provide Well Child information to parents, this project worked to answer the following questions. • What information and advice do parents want? • What information and advice do parents need? • How do they get that now? • How could they get that in the future? The project has involved four components: 1. a literature review to determine what is being done elsewhere and what works 2. a survey of parents to ask what information they want and how they are accessing
that now 3. consultation with professionals about what information parents need and how the
professionals currently provide that information 4. an interview with NHS Direct in the United Kingdom, the world’s largest provider of
telephone and web-based health information services, to gain insight into how it has set up its health information services.
The delivery model for remote access to information and advice on demand that has emerged from this project is shown in Figure 1 below. It is made up of three components: support, access to services, and information. Each of these bundles of services can only be delivered through telecommunications systems, which then raises issues regarding access. Irrespective of what information parents want, their ability to access it is the first hurdle they have to overcome. According to the most recent data available from Statistics New

Parent Information Project 2
Zealand (December 2006), only 2 percent of households in New Zealand have no access to a telecommunications system. These data along with the results of our surveys of parents and health professionals tell us that the majority of parents in New Zealand have the potential to access maternal and child health information and advice on demand. Figure 1: Delivery model for remote access to information and advice on demand
Access to services
Support Information
Information sources
WebsitesSupportCommunity resourcesAges and stagesSpecial interestsAudio
PodcastsCommunity radioTalkbackPre-recorded
AudiovisualDVDInteractive TVKioskNarrowcast TVVideoconferencingWebinars
Printed materialMultiple languagesEasy readLarger printBraille
Access to services
Telephone servicesTriageAdviceInformationAccess to servicesMaking arrangementsTransfer to other supportOut of hours services
Support
LMCs and WCPsHelplinesPeer supportWhānau
Around the world, the internet is the second-most frequently used and second-most preferred source of health information for parents, after consulting their health care provider, who is usually their general practitioner (GP). Most parents find it a helpful resource, particularly to enhance knowledge and understanding of a certain condition. However, clinicians are concerned about the poor quality of the information that parents read. There have been no effective and enduring health information quality initiatives to address this problem, so health professionals have responded by advocating that they

Parent Information Project 3
should guide their patients to reliable sources, and author material themselves for publication on the internet. More parents use websites than telephone health lines. That said, the distinction between internet and telephone health services has become blurred and, in many cases overseas, meaningless. In the latter instances the telephone helpline and the website have been integrated and services that in the past were only available by telephone are now able to be accessed and delivered by email or text. Research shows that parents need different information in different forms at different times. So we have also briefly discussed other methods for delivering information such as email, radio, television, CDs, DVDs and printed material. Each of these methods has limitations or attributes according to the individual circumstances of each parent. This report addresses each of the major research questions in turn, before discussing the main delivery methods for Well Child information and advice. It then makes recommendations for integrated telephone and website services that should be provided to meet the Well Child information needs of New Zealand parents.

Parent Information Project 4
What Information and Advice Do Parents Want? In order to specify the range of services for delivery of Well Child information and advice to parents in ways that do not involve face to face contact, we need to know what information and advice parents want. One of the most significant studies of child development and parenting information needs was the Australian Parenting Information Project, undertaken for the Australian Government in 2004 by the Centre for Community Child Health (CCCH 2004). Its report focuses on child development and parenting, and incorporates the views of parents, health care providers and information from the literature. The views of parents in Australia were sought via a national telephone survey and focus groups. Parents said that they sought information about the physical, intellectual, social and emotional development of a child and a recurrent theme was that this information was sought by ‘ages and stages’. The data generated by the parent survey strongly influenced the development of the website http://raisingchildren.net.au/. As can be clearly seen from the layout of its home page, it graphically reflects parents’ declared need for information about a child’s development over time. The execution of this website set a new standard for communicating child health information and advice.
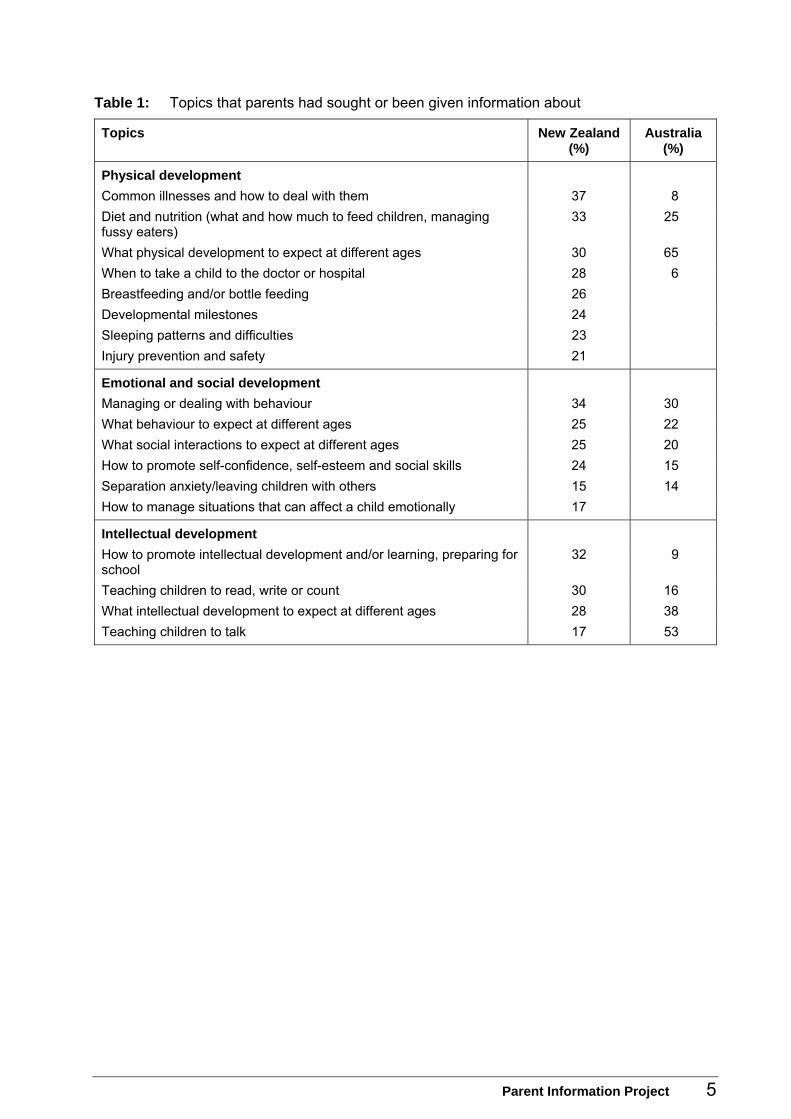
What information and advice do New Zealand parents want? We sought permission to replicate the survey questionnaire used in Australia. We modified the questionnaire to better reflect the aims of our research and the New Zealand context. A copy of the modified questionnaire is provided in Appendix 1. During April and May 2009, a national survey of over 800 New Zealand parents with children aged five years and under was conducted. The summary report and results of the survey are provided in Appendix 2. The most common child development topics that parents in New Zealand had sought or been provided with information about are listed in Table 1 below. The results for New Zealand parents in respect of information about emotional and social development mirror the results for Australia. However, in regard to the information New Zealand parents sought about physical and intellectual development, the results show slight differences from those for Australian parents. Overall, New Zealand parents appeared to want information about how they can promote their child’s wellbeing rather than on what development to expect at different ages and stages. However, the New Zealand results are also clustered over a much narrower range than the results from Australia, with the top 10 topics being separated by only 12 percentage points. This clustering would suggest that New Zealand parents want information about a greater number of child development topics than their Australian counterparts.
Parent Information Project 5
Table 1: Topics that parents had sought or been given information about
Topics New Zealand (%)
Australia (%)
Physical development Common illnesses and how to deal with them 37 8 Diet and nutrition (what and how much to feed children, managing fussy eaters)
33 25
What physical development to expect at different ages 30 65 When to take a child to the doctor or hospital 28 6 Breastfeeding and/or bottle feeding 26 Developmental milestones 24 Sleeping patterns and difficulties 23 Injury prevention and safety 21
Emotional and social development Managing or dealing with behaviour 34 30 What behaviour to expect at different ages 25 22 What social interactions to expect at different ages 25 20 How to promote self-confidence, self-esteem and social skills 24 15 Separation anxiety/leaving children with others 15 14 How to manage situations that can affect a child emotionally 17
Intellectual development How to promote intellectual development and/or learning, preparing for school
32 9
Teaching children to read, write or count 30 16 What intellectual development to expect at different ages 28 38 Teaching children to talk 17 53

Parent Information Project 6
What Information and Advice Do Parents Need? As part of its 2004 study (CCCH 2004) the Centre for Community Child Health questioned Australian child health professionals first about the content of information and support that parents need about their child’s development. In response, these professionals suggested that parents need: 1. greater understanding of child growth and development 2. greater understanding of basic parent craft (e.g., bathing, feeding) 3. techniques and routines around sleeping, feeding and settling 4. understanding of child safety, hygiene and nutrition 5. greater understanding of the importance of attachment, play and strong
relationships 6. assistance with behaviour and anger management 7. understanding of the differences among managing behaviour, discipline and
punishment 8. understanding of how to improve communication between each other and with
their child or children 9. greater understanding of the life implications associated with becoming a parent 10. support with managing day-to-day family life and financial pressures. In terms of process issues, the Australian professionals believed that parents need: 1. assurance about their parenting – that they are ‘doing okay’ 2. time to process and practise parenting skills 3. different information, in different forms, at different times 4. face-to-face relationships with professionals 5. consistent, credible messages 6. access to a range of services and support at different times.
What information and advice do New Zealand parents need? Members of the National Well Child/Tamariki Ora Clinical Advisory Group were asked to rate the above issues according to whether they would strongly disagree, disagree, agree or strongly agree that they represent the information and advice needs of parents. These ratings were sought to determine the extent to which the results from Australia in 2004 could be considered to apply in New Zealand five years later. It is clear from the data in Table 2 below that, overwhelmingly, New Zealand professionals agree or strongly agree with their Australian counterparts about the information needs of parents, in terms of both content and process. The high degree of agreement about the content of information supports this report’s citing of the Australian website raisingchildren.net.au as a model for communicating information about child health and development, and the resources available to parents.

Parent Information Project 7
There was also unanimity amongst New Zealand health professionals that parents need different information, in different forms, at different times. These clear results on the information that New Zealand parents want and need lead to consideration of the next question of how to communicate this information to parents. Table 2: New Zealand health professionals’ views on what information parents need (%)
Question Strongly disagree
Disagree Agree Strongly agree
1. Greater understanding of child growth and development
67 33
2. Greater understanding of basic parent craft (e.g., bathing, feeding)
14 86
3. Techniques and routines around sleeping, feeding and settling
14 86
4. Understanding of child safety, hygiene and nutrition
29 81
5. Greater understanding of the importance of attachment, play and strong relationships
43 57
6. Assistance with behaviour and anger management
57 43
7. Understanding of the differences among managing behaviour, discipline and punishment
14 86
8. Understanding of how to improve communication between each other and with their child or children
14 43 43
9. Greater understanding of the life implications associated with becoming a parent
43 57
10. Support with managing day-to-day family life and financial pressures
81 29
11. Assurance about their parenting – they are ‘doing okay’
16 84
12. Time to process and practise parenting skills 43 57 13. Different information, in different forms, at different
times 100
14. Face-to-face relationships with professionals 43 57 15. Consistent, credible messages 29 81 16. Access to a range of services and support at
different times 43 57
Parent Information Project 8
What Methods of Providing Information to Parents Are Available? Irrespective of what information parents want, their ability to access it is the first hurdle they have to overcome. The level of difficulty they experience in doing so is dictated by extrinsic factors such as the telecommunications systems available to them and by intrinsic factors such their hearing, sight and literacy. According to the most recent data available from Statistics New Zealand (December 2006), only 2 percent of households in New Zealand have no access to a telecommunications system. In regard to the main forms of telecommunications, 88 percent of all households have a fixed line telephone, 86 percent have a mobile phone, 72 percent have a computer and 64 percent have access to the internet. These data along with the results of our surveys of parents and health professionals tell us that the majority of parents in New Zealand have the potential to access child health information and advice on demand. There will always be small areas of the country where telecommunication systems will not be available. Special consideration must also be given to those parents who cannot access health information and advice for reasons of physical isolation, social isolation (ethnicity and language) and/or lack of money; or because of impaired hearing, impaired sight, impaired mobility etc. The optimal method of communicating information will inevitably vary between individuals. Someone who has a hearing disability, for example, is likely to get most value from information that is presented visually. On the other hand a person with impaired vision will appreciate information that is presented aurally – as will, for different reasons, someone with limited literacy. In determining effective methods of communicating information to parents, a further consideration is that individuals with limited health literacy lack the skills to obtain, process and understand basic information needed for health decisions. These individuals are less able to manage their own care and suffer worse health outcomes as a result. Limited health literacy is also associated with frequent hospitalisation, incomplete understanding of health issues and increased health care costs. Significant numbers of people are forced to seek health information in a non-native language and to navigate significant cultural barriers. The New Zealand Adult Literacy and Life Skills (ALL) survey (Satherley et al, 2008) looked at the distribution of literacy, numeracy and problem-solving among people aged 16 to 65. Of the adults surveyed, 43 percent had a literacy score (document and prose) of level 1 or 2. A level 1 or 2 score is defined as low literacy. A person with level one or two literacy may be able to comprehend words in isolation or simple sentences, but lacks the literacy skills to comprehend more complex passages of text or information. The literature review of communication channels from the Australian Parenting Information Project (CCCH 2004) is summarised below at some length because it

Parent Information Project 9
contains opinions and data that also appear in the latest literature about methods for delivering child health information and advice to parents on demand.
Telephone Telephone-based services can be delivered cheaply and are generally viewed favourably by parents, including parents of children with specific conditions. Advantages of this method of delivery for parents include savings of time and money on appointments, and easy access for rural families. Limitations include the lack of longitudinal contact with a professional, dependence on a telephone, limited use by lower income and less educated families, and difficulties likely to be experienced by non-English speaking families who try to use the service. Telephone information alone has not been shown to have an impact on parenting skills and child functioning. However, it can be a useful part of a multimedia parent training package that includes other strategies for communication such as written material and face to face services. The delivery of standardised instructions appears more effective than the use of ad hoc information. Table 3: Overview of the telephone as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• High satisfaction among parents using telephone helplines by professionals such as doctors and nurses
• Reduces time and cost of hospital appointments
• Reduces travel time and cost for rural families
• Increases access to quality care for families (often on 24-hour basis)
• Cheap to deliver
• Effective for behaviour management (e.g., school bullying) for parents of primary aged children
• Effective for parents of younger children (0–5 years)
• Limited uptake by low-income families
• Standardised instructions are more effective than ad hoc information
• Telephone services are best used to complement and support other strategies, e.g., written self-help material and face-to-face services
• Integration of telephone helplines with face-to-face services to improve longitudinal contact and continuity of care with health professionals
Internet Given the wealth of information available and the relative ease of accessibility for families, the internet can be an effective resource, provided families can identify reputable websites and accurate information. The main concern is for those parents with limited literacy who are unable to differentiate among websites based on the quality of the information or to understand the content of the information accessed. However, the barrier of written communication can now be addressed through turning the text into spoken words and the use of visual aids. These functions are also crucial for those with impaired sight or hearing, or those people for whom English is a second language. The critical point is that the language used in the text should be written in plain English and be simple enough to be accessible to the whole population.

Parent Information Project 10
There is a need for the government to develop effective consumer guidelines or an information authentication system to ensure that what parents access is quality information that is readable and trustworthy. Table 4: Overview of the internet as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Provides access to large amounts of information on many topics relating to parenting
• Provides information in a rich number of formats including text, voice, pictures and videos
• Not yet demonstrated • Improve accessibility of parent education materials, e.g., rapid and easy downloading of audio and visual clips
• Develop/disseminate guidelines to assist parents to distinguish credible, current and accurate advice from an authoritative source
DVDs Instructional DVDs have been effective in increasing patient knowledge in the short term when shown on specific topics in situations such as clinic waiting rooms. However, whether this increase is maintained over time is not known, as studies have focused on immediate information recall. Deep learning entails a parent being able to derive personal meaning from knowledge gained and being intrinsically motivated to alter their way of interacting with their child and the world. A combination of a DVD series and verbal discussion groups appears to be most effective in achieving such learning. For effective use with people of different cultures, it is important to seek advice on settings and cultural practices from representatives of the group(s) for whom it is intended and to use real-life situations and people.

Parent Information Project 11
Table 5: Overview of DVDs as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Can convey information in a consistent, interesting way particularly for complex topics
• Can form an effective part of a multimedia approach, with written information and/or verbal discussion groups
• Can circumvent reading/ literacy problems
• Readily dubbed in various languages
• Highly effective in improving parents’ knowledge of various child health issues
• Effective for improving relatively mild parent–child problems
• Can be effective in waiting rooms (with other distractions eliminated) for improving short-term parent knowledge on specific child health issues
• Longer or more intensive DVDs (e.g., an hour or more, or a series over several weeks) are effective in producing behavioural changes in problem parent–child interactions
• Effective for deep learning for parents who are strongly motivated to alter their way of interacting with their child and others, and who can derive personal meaning from the knowledge gained
• Best used in combination with other strategies, e.g., with short-term group education for self education; or as part of a multimedia parent training programme
• Effective for teaching parenting skills if used to model vignettes of desirable parent–child interactions, and accompanied by facilitator-led discussions
• Seek advice on settings and cultural practices from representatives of the group(s) for whom the DVD is intended, and use real-life situations and people
• Use culturally sensitive role models to demonstrate optimal behaviour. Imitation of modelled behaviour produces immediate learning if the model is seen as significant to the learner and the behaviour perceived as desirable with positive personal significance
Email Very little research is available on the use of email communication for delivering parenting information. Although it appears that it may have advantages for administrative staff in reducing telephone contact time with families, there are medico-legal and privacy issues to be considered. Table 6: Overview of email as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Reduces telephone contact time for administrative staff during busy periods, e.g., doctors’ clinics
• Provides electronic record of information sought by and provided to parents
• Not yet demonstrated • Medico-legal aspects relating to the Privacy Act 1993 need to be clarified before further implementation

Parent Information Project 12
Radio and television The use of mass media remains a controversial area. One factor of concern is the need to justify the costs of large campaigns given the difficulty involved in measuring effectiveness in terms of increased knowledge and behaviour change. Most campaigns appear to be effective in significantly increasing knowledge regarding health education issues, but the retention of this knowledge following the intervention is variable or not measured over the long term. Behavioural changes are much more difficult to achieve and measure. However, they are more likely to be achieved through sustained mass media campaigns involving several strategies, for example television programmes and additional support systems such as telephone helplines, resource centres and support groups. Cost benefits of programmes are also difficult to determine. However, several programmes have reported negative costs associated with unexpected increases in utilisation of existing health services. Table 7: Overview of radio and television as methods of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Can raise knowledge and awareness re important health issues and research findings
• Can quickly distribute messages to diverse audiences
• Can set agendas for individual and societal discourse
• Can influence behaviour • Can reach large
numbers of people quickly
• Can be entertaining as well as informative, e.g., television programmes
• Effective for increasing parental knowledge of child health issues
• Highly effective if used for screening campaigns
• Can result in significant changes in health service utilisation and associated costs
• Effective in producing short-term knowledge and behaviour changes
• Effective for parenting and child-related behaviour problems under optimal programming conditions
• Effective if television programmes are based on real-life situations with role models that public are able to strongly identify with
• Repetition of campaign message important in aiding knowledge recall
• Television programmes an effective medium in changing short-term behaviour especially when combined with another strategy, e.g., telephone helpline
• Use real-life case studies and culturally sensitive role models in television programmes
• Combine television with additional strategies such as telephone helplines, support groups and parent resource centres
• Need for study design to incorporate appropriate measures of behavioural outcomes as well as knowledge
• Further research needed on evaluation of optimal dose, intensity and length of campaign and population characteristics
• Sustained efforts over longer periods are more likely to have the desired behavioural impact than shorter, more intensive campaigns
• Ascertain the level of awareness in target group to proposed campaign message prior to intervention in order to avoid a ‘ceiling effect’

Parent Information Project 13
CD-ROMs The few studies that have contrasted technology-based education with traditional methods have tended to focus on students in higher education courses rather than parent education and have shown similar outcomes to traditional methods. Of those studies that have involved parents, very few were long term or contrasted various methods of instruction. Additional research is needed before conclusions can be drawn on the efficacy of CD-ROMs. Table 8: Overview of CD-ROMS as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Can be individualised because parents can seek information as needed
• Allows flexibility of learning, providing instruction at any time or place where a computer is available
• High levels of parental satisfaction on common child health issues such as management of nocturnal enuresis
• Is as effective as traditional teaching
• Effective in improving parents’ knowledge and perceptions but not in changing parenting behaviour
• More research into effectiveness with regard to parent education is needed
Printed material Informational handouts can be effective educational tools, particularly when they are accompanied by a personalised approach and advice. A personalised approach generally substantially increases people’s recall of the material presented, and its effectiveness in achieving its desired outcomes. In particular, it helps to engage parents’ interest and motivation, an essential step if handouts are to be effective teaching tools. Written material needs to be readable and readily understood. Informational literature should be written at or below the level of a person with limited literacy (average 8-year-old). The text should be simple, direct and focused. An understanding of cultural differences, particularly as they relate to parenting and early childhood, is critical to providing effective services in a multicultural society. Information and educational interventions generally tend to be based on mainstream culture. Differences in family expectations, communication and learning styles need to be identified and understood, and assessments, instructions and information adapted in culturally appropriate ways. Further research is needed to ascertain the most effective ways of achieving culturally sensitive family interventions.

Parent Information Project 14
Table 9: Overview of printed material as a method of information delivery
Positive features Evidence-based outcomes, best practice applications
Recommendations for effective implementation
• Improves recall and knowledge
• Reinforces verbal information
• Increases understanding, decreases anxiety and encourages compliance and self-management
Age-paced newsletters
• Common parental concerns addressed in relation to the child’s age, with emphasis on knowledge of development, parenting, health care, and emotional wellbeing
• Increases knowledge about development and parent–child relationships
• Increases parental self-confidence
• Effective for complex topics or teaching skills involving multiple steps, e.g., in behaviour management programmes
• A personalised approach in disseminating information improves effectiveness, rather than giving the written information by itself; e.g., discuss handouts during an appointment, rather than give without further instruction
• Important material should be presented first verbally and reinforced by written material
• Strategies such as a self-monitoring calendar and telephone reminders increase effectiveness
• Also effective if informational handouts are sent by mail in conjunction with a media campaign to raise parents’ interest in the intervention
• Resources need to be relevant and easily readable, written at the level of an average 8-year-old.
• Replace medical and technical jargon with everyday language where possible. Use short sentences, avoid prepositional phrases and passive tense
• Write for the desired health behaviour rather than for high-level knowledge
• Determine key points to achieve behavioural objectives. Limit the number of concepts
• Personalise the information by using ‘you’
What New Zealand professionals said Members of the National Well Child/Tamariki Ora Clinical Advisory Group were asked to rate the statements made in the Australian Government’s Parenting Information Project in 2004 regarding the role of each method of information delivery, as outlined above. These ratings were sought to determine the extent to which the methods used to communicate information to parents in Australia could be considered to apply in New Zealand, five years later. The results are listed in Table 10.

Parent Information Project 15
Table 10: Extent to which New Zealand health professionals agree with their Australian counterparts on methods of information delivery (%)
Methods Strongly disagree
Disagree Agree Strongly agree
Telephone 86 14 Internet 100 DVDs 81 29 Radio and TV 14 86 Printed materials 14 86
Among the New Zealand health professionals there was unanimous agreement about the role of the internet, telephone and DVDs as methods of information delivery. Bearing in mind that this project is about how Well Child information and advice can be provided to parents on demand, it can be concluded that the internet has a large role to play in conjunction with a telephone helpline. But this approach to delivery will only work well if it is aligned with how parents want to access information. The next section establishes what methods parents prefer.

Parent Information Project 16
What Methods Do Parents Prefer? The New Zealand and Australian telephone surveys of parents specifically asked them how useful they found each of the information, advice and support methods described in the previous section for accessing Well Child information. Parents were also asked about their preferences for each of these methods as possible sources of Well Child information in the future. The results are listed in Table 11. Table 11: New Zealand parents’ preferences for Well Child information sources and perceived
utility of those sources (%)
Information source Prefer* Useful**
Internet 52 86 Face-to-face communication with professional advisors 38 94 Telephone helplines – PlunketLine 32 94 Brochures or fact sheets on specific issues 22 80 Books 21 89 Telephone helplines – Healthline 20 86 Magazines 13 79 Television programmes 8 68 Videos or DVDs 7 58 Telephone helplines – Well Child Advice Line 6 93 Parenting support groups and networks 5 79 Newspaper articles 2 72
* Parents listed all preferred sources of Well Child information resulting in a total greater than 100% ** Combines responses of “very useful” and “useful” as sources of Well Child information. Over half of the New Zealand parents surveyed would prefer to access information about their child’s development on the internet. Other preferred sources of Well Child information for New Zealand parents are face-to-face communications with professional advisors (38 percent); telephone helplines especially PlunketLine (32 percent) and brochures or fact sheets on specific issues (22 percent). The high rating of face-to-face communication with health professionals and brochures or fact sheets is consistent with the Australian results. It should be noted that the role of Healthline for under five year olds is to assess, triage and provide information in relation to sick or symptomatic children, rather than to provide Well Child advice. Parents find face-to-face communication with health professionals and the current Well Child telephone services highly useful (93–94 percent). Although the internet is the most preferred source for information by parents, only 41 percent of New Zealand parents surveyed had used the internet as a source of Well Child information in the last six months. This suggests there is room for improvement in this method of delivery. This project is looking at the delivery of Well Child information, advice and support to parents, on demand, using methods that do not involve face-to-face contact. That in turn limits the scope of this report to those communication channels that are delivered by telecommunication systems. The next section examines the use of internet and telephone health lines by parents.

Parent Information Project 17
The Use of the Internet by Parents The internet is now the single largest source of health information with over 100,000 sites offering health information (Hargrave et al 2006; Wilson 2002). In the USA, 66 percent of the adult population use the internet (Mackert et al 2009) and in the UK 64 percent regularly access the internet (Sim et al 2007). According to the latest New Zealand Census data, 64 percent of households regularly use the internet and 86 percent of them have mobile phones (Statistics New Zealand 2006).
Why parents use the internet The internet is the second-most frequently used and second-most preferred source of health information for parents after health care providers (D’Alessandro et al 2004; Goldman and Macpherson 2006; Tuffrey and Finlay 2002; Wainstein et al 2006). Most parents find internet health information a helpful resource, particularly to enhance knowledge and understanding of a condition. These experiences have been determined by a number of surveys, some of which are summarised below. Boston et al’s study in 2005 aimed to determine the prevalence of internet medical searches by parents prior to their child’s surgical procedure and evaluate whether internet-based health information influences parents’ medical decisions on behalf of their children. The researchers found that the internet information influenced the medical decisions taken by about half of the parents surveyed. The conclusion from their research was, first, that physicians remain the most important source of information that guides a parent or patient in their decision-making. Secondly, the ideal for involving the internet in this process would be for surgeons to direct parents or patients to a few trusted internet sites and be prepared to discuss this information. In another study Kind et al (2005) examined the circumstances for lower socioeconomic communities. This study recruited parents from a community health centre in an urban, largely African American neighbourhood whose inhabitants were predominantly of low income and low education level. Caregivers were provided with access to online health information in the waiting rooms of community-based health centres. What they found striking was the large percentage of low-income, lower-education parents who do use the internet, have used it for finding health information, and strongly agree that they would use the internet to make health decisions. Amongst the studies by paediatricians about the use of the internet by parents, three recent ones – by Sim et al (2007), Khoo et al (2008) and Wainstein et al (2006) – are summarised below.
Parents attending outpatient clinics in London (Sim et al 2007) In 2005 parents attending outpatient clinics in London were asked to complete a questionnaire regarding internet use in seeking more information about their child’s condition. Just over half of the parents surveyed had accessed to the internet to seek

Parent Information Project 18
more information about their child’s condition. Ninety percent used the name of a specific condition as a keyword, with most parents (75 percent) using Google for their search engine. When asked what they searched the internet for, 89 percent were seeking more information, just over half were looking for possible long-term outcomes, medical treatments or complications and a third were looking for support groups. Almost all parents (94 percent) in Sim’s study said they found the internet useful, 84 percent felt they better understood their child’s condition after using the internet and 37 percent felt reassured. Of those who did not find the internet useful, half found little or no information, 38 percent found too much information and 13 percent felt that the information was too technical. Sim et al concluded that: • the internet is a useful educational tool in teaching parents about their child’s
condition • the best way to ensure that parents have access to quality and accurate information
on the internet is for paediatricians to provide it themselves.
Parents attending the emergency department at the Royal Children’s Hospital in Melbourne (Khoo et al 2008) Khoo et al (2008) surveyed the parents of patients presenting to the paediatric emergency department of the Royal Children’s Hospital in Melbourne in 2006/07 to determine where parents find information. They found that parents used a large number and wide variety of health information for their children, with GP/health professionals, the internet and family/friends being the most used. Although the internet was used frequently by parents, they still mostly used and trust information from their GP/health professional. The trustworthiness of internet information improved when the website was authored by the Royal Children’s Hospital. Most parents with internet access said they would value more guidance when searching for health information. The three suggestions contained in the questionnaire were all well received by respondents, which were: • a written information prescription of reliable websites from a doctor or nurse
(95 percent) • pamphlets and advertising (88 percent) • a professional medical informatics specialist (61 percent). After being shown a flow chart for ‘vomiting in children’, most parents (91 percent) said that they would definitely or probably follow the advice of such a treatment flow chart if it was available online from the Royal Children’s Hospital. The authors recommended that web-based algorithms for home treatment and health-care seeking behaviour should be explored further.
Parent Information Project 19
Parents’ internet access after appointments at the Sydney Children’s Hospital (Wainstein et al 2006) Wainstein et al (2006) looked at why parents use the internet by collecting data about their information seeking after they had met their doctor. Almost all parents (97 percent) wanted to know more about the information that was given to them by their doctor, most (75 percent) wanted to reduce their anxiety about what their doctor had told them and over half had unanswered questions or were seeking alternative therapies.
Effect of internet use on access to health services (Bouche and Migeot 2008) Given the extent to which parents are using the internet to gather health information, a question that arises is whether it leads them to consult professionals more often. Bouche and Migeot (2008) investigated the relationship between parental use of the internet to seek health information and primary care utilisation for their preschool child. They found that there was no relationship between information seeking and primary care utilisation, and that the internet seemed to be used as a supplement to health services rather than as a replacement. They thought it likely that improvement in health would occur for those who use the internet to seek health information which, in the long term, would eventually lead to saving in health costs.
The influence of internet use by parents on subsequent Well Child visits (Christakis et al 2006) This section concludes with a discussion about research undertaken by Christakis et al (2006). This research forms the basis for the recommendation of a new way of engaging New Zealand parents in the services offered by the Well Child Framework. In terms of offering Well Child information and advice to a parent on demand, the proposed new approach builds on the findings of all of the studies above on the many reasons why parents consult the internet and it addresses the issues of information prescription and authentication. The proposed new method also forms the basis for ‘making arrangements’ whereby visits to Well Child providers can be arranged, confirmed or altered. Christakis et al (2006) successfully showed that parents could influence the content of their Well Child visit through directed use of an internet site before the visit. The researchers also showed that this approach increased the likelihood that parents would adopt preventive measures. In the USA, paediatricians spend less than 10 minutes of Well Child visits discussing preventive care (LeBaron et al 1999; Reisinger and Bires 1980). There are numerous barriers to delivering paediatric preventive care including lack of time and knowledge, clinician forgetfulness (Stange et al 1994, 1998) and information overload (Battista and Lawrence 1998; Frame 1992). A typical visit can be consumed by a long list of topics seen as important to providers or organisations, leaving minimal time for discussion of concerns most relevant to parents.

Parent Information Project 20
Moreover providers may not use adult learning theory in counselling parents, opting instead for a quick run-through of topics (Knowles et al 2005). Parents may leave confused, overwhelmed or distracted by the amount of information conveyed during the visit (Schor 2004). In general, parents infrequently help to set the agenda for Well Child visits and often they leave without the information they sought initially (Bethell et al 2004; Hickson et al 1983; Wainstein et al 2006; Young et al 1998). Changing provider behaviour has proved difficult, especially with respect to preventive health maintenance (Davis et al 1995; Oxman et al 1995). However, patients themselves have been shown to be effective in motivating provider behaviour change (Davis et al 1995). Informing patients which questions to ask their doctor before a scheduled visit has improved the quality of adult diabetes care (Greenfield et al 1985, 1988; Kaplan et al 1989). But similar studies among healthy children are generally lacking. Traditional means of engaging patients have relied on mailings, telephone calls, or face-to-face contact. The capacity of the internet has not been explored even though it is vastly cheaper as a method of information delivery than these traditional means. Christakis et al enrolled children aged 0 to 11 years in a randomised controlled trial of a tailored website, MyHealthyChild, which provided information on prevention topics before a scheduled Well Child visit. There were two components of their intervention: 1. providing information to parents about prevention topics 2. communicating to physicians the topics that were of interest to parents. Families were assigned to one of four groups: usual care (control), prevention topics only (content only), prevention topics and notifying the physician (content and notification), or notifying the physician only (notification only). Before their child’s check, 93 percent of all parents in the study visited the website. Outcomes were determined with telephone follow-up surveys conducted two to four weeks after the visit. Parents in the ‘notification only’ and ‘content and notification’ groups reported discussing more prevention topics with their provider. Parents in the ‘content only’ and ‘content and notification’ groups reported implementing more prevention topic suggestions such as the use of a safety device. The success of the trial by Christakis, and all the evidence that has been collated from elsewhere about parents’ information and advice needs, lead to the recommendation that an equivalent of the MyHealthyChild website should be created for New Zealand parents. This web-based parent information service will: • be the source of up-to-date and accurate information about the Well Child
Framework • address the issues of information prescription and authentication • engage New Zealand parents in the services offered by the Well Child Framework

Parent Information Project 21
• provide a facility for visits with Well Child providers to be arranged, confirmed or altered.
Websites designed for use by parents and children The internet was searched for websites designed for use by parents in Australia, Canada, USA, England and Scotland. This report has focused on those that provide good examples to influence the design of a New Zealand child health website, and/or contain particular examples of service delivery. The addresses of websites of note are provided in Appendix 3. As discussed in the Introduction, the distinction between internet-based health information and advice services and telephone health services has become blurred and, in many cases overseas, meaningless because the telephone helpline and the website have been integrated. In the latter cases services that in the past were only available by telephone are now able to be accessed by email or text and in some cases delivered in that way too. Based on the evidence from overseas, this report recommends that the New Zealand Child Health website should be integrated with the Well Child Telephone Advice Service. Text messaging is discussed further on in the report. This report also recommends that the use of text messaging should be explored within this integrated package of services.
Parent Information Project 22
The Quality of Health Information Available on the Internet Assessment of the quality of information available on the internet depends on establishing whether the information is true and whether it is understandable.
Is the information true? A team of US physicians determined that only one in five of the links provided by the first results page of 14 search engines led to relevant content and fewer than half the clinical components of each subject were covered accurately and substantively (Berland et al 2001). The presence of common, low-quality information on the internet opens the way for the distribution of less valuable information, particularly because some users may bother to check the credibility of websites or may lack the background knowledge to judge the quality of presented information (Eysenbach et al 2002). Kaimal et al (2008) used Google and Yahoo search engines to find six obstetric topics of interest or concern to patients. They examined 350 websites, of which only 5 percent were sponsored by gynaecologists/obstetricians. They suggested that clinicians should create a list of websites that appear to have appropriate, unbiased information and provide this list to patients. With this list, patients could be more likely to access accurate health information. In addition, if their patients find these resources useful, physicians will transmit this message to their profession’s leaders increasing the likelihood that resources will be devoted to developing standardised patient education information.
Is the information on websites understandable? Health officials throughout the world are confronted by the challenge of limited literacy (Gray et al 2005), with half or more of the world’s adult population possessing limited ability to understand and act on information (Manning and Dickens 2006; Nielsen-Bohlman et al 2004). The Children’s Partnership evaluated 1000 websites and found only 10 of them were accessible to adults with limited literacy (Lazarus and Mora 2000). The scale of the problem has prompted a number of individuals and institutions to try to work around individual’s limited health literacy by using internet technologies (Homewood 2004), traditional media campaigns (Jorm et al 2005) and interpersonal channels (Wilkin and Ball-Rokeach 2006). Amongst these, digital media are recognised as having potential because of their adaptability, relative cost-effectiveness and accessibility (Eysenbach 2007). Davis et al (1994) note that a significant amount of public health information (educational and instructional material) requires a higher reading level than most parents have achieved and that information should probably be written at a level lower than a high school reading age if most parents are to be expected to read it.

Parent Information Project 23
Children’s health care will be compromised if physicians incorrectly assume that all parents can read and understand health-related material. In Davis et al’s study two-thirds of parents could not read at more than ninth grade level, and more than one-quarter of parents read at less than a seventh grade level. In New Zealand, almost half (43 percent) of adults are estimated to have limited literacy (Satherley et al, 2008). Therefore, to be understandable to a wide range of parents, health information should be written for an audience with a reading age of about 8 years of age.
What future standards are there for health information? This section has recorded that clinicians are concerned about the poor quality of much of the health information presented on the internet. The response of clinicians has been that they should guide their patients by informing them of reliable online sources and that they should author material for publication on the internet. We recommend as a short-term response that the Ministry of Health should: • be responsible for creating or adopting/accrediting authoritative health information,
and then freely distribute it to relevant New Zealand websites • publish lists of reliable sources of web health information. There is, however, a new approach in the UK that formalises the responsibility of health professionals to advise their patients about suitable health information. It proposes that health professionals should prescribe appropriate health information in a somewhat similar way to their prescription of suitable medication or treatment. ‘Information prescription’ is likely to be the health information response by the UK Department of Health to overcome the problem of widespread availability of unreliable information. However, prescription depends on accreditation. The UK Government has created an accreditation scheme standard for health and social information. This report recommends that the Ministry of Health considers adopting exactly the same approach in New Zealand.
Parent Information Project 24
Telephone Health Lines Telephone health lines have been in operation around the world for at least 20 years. The largest is NHS Direct in the UK, which handles 6 million calls per year. Even though little is known about their clinical effectiveness or cost-effectiveness, the number and size of telephone health lines is expanding. In general, national health lines are consulted by about 8 percent of the population each year. However, the rate of use is strongly affected by the level of marketing activity to create awareness of the service, the time of year (i.e., more calls in winter) and the prevalence of disease (e.g., in response to an epidemic). Telephone health line services around the world are usually provided by specially trained nurses who often use call handling technology and computerised protocols to assist them in helping callers. Telephone health lines deliver a wide range of services. The usual starting point for the conversation with the caller is triage. In respect of a child health related call, the pathways of care for the caller include: • dispatch of an ambulance in emergency cases • transfer to the national triage service for symptomatic callers • receiving information and advice about their child’s development • referral to locally available services and support, or • a routine visit to a Well Child practitioner. The greatest change over the last two decades in delivering health services using methods that do not involve face-to-face contact is the complete integration of a health information website with its associated telephone service. This development has occurred because telephone and website in combination can deliver services that neither channel can do alone. An important driver has been that the cost of service delivery by website is significantly lower than that incurred when the same or equivalent service is delivered by telephone, which uses highly qualified and specially trained nurses. An example is NHS Direct, which is now completely integrated with its companion health website, NHS Choices. This combined service delivered 30 million health transactions to members of the public in England in 2008.
What is telephone triage/teletriage? Triage in health services is the process of sorting patients into order of priority for treatment (Fortune 2001). Teletriage services may also include the provision of information, guidance with making a health decision, and symptom management to facilitate self-directed and informal care if appropriate. Within the context of Well Child services, teletriage involves determining if a call is in response to a sick or well child. GPs and other health professionals have long used telephony to provide advice to patients and to prioritise office visits for non-urgent issues (Leasure 1998).

Parent Information Project 25
Factors motivating the rise in more formalised telephone health line programmes include: • the volume of emergency department visits • a desire to minimise inappropriate health care visits • shorter hospital stays, resulting in more acutely ill clients in the community • people’s demand for and access to health information • enhanced continuity of health care services outside regular hours • advances in information and communication technologies • the need for equitable access to health services for those with limited mobility and/or
living in remote locations (Department of Health UK 2000; Glasper 1993; Hogenbirk et al 2002; Larson-Dahn 2001; Mullett 2000; O’Connell et al 2001; Price Waterhouse Coopers 2001; Romanow 2002).
Despite the wide range of activities, little is known about the overall effectiveness of telephone health services. Reviews suggest that nurse telephone consultation provided alone or combined with other self-care and informal care resources reduces health professionals’ workload, encourages self-care and informal care for health problems and decreases health care costs without increasing adverse outcomes (Stacey 2002). To ensure programme quality, telephone health services need: • practitioners with specialised education in teletriage and access to continuing
education opportunities • a documentation system to ensure that the interactions and services provided are
recorded; ideally, the documentation should be integrated with that of other health services such as the caller’s personal practitioner
• clinical protocols that guide practitioners’ responses to calls and enhance the quality of the interaction
• continuous quality improvement programmes to ensure the delivery of high-quality service and an early response to potential problems (Coleman 1997).
Regulating organisations recommend that nurses providing telephone health services have specialised knowledge, skills and judgement. The process that nurses use during the telephone interaction includes assessing the health issue and individual capacity, communicating effectively with active listening, making relevant decisions with the caller, determining access to appropriate resources and evaluating the process and outcomes. Many telephone health services provide training for their nurses as part of the orientation process, have a system to formally document the calls and include a medical consultant on staff. In more formal health line programmes, nurses work in shifts to provide services as part of their regular duties and not as an addition to daytime responsibilities.
Parent Information Project 26
Child health telephone lines The purpose of this project has been to produce an evidence base for the specification of Well Child information, advice and support services for parents of a child aged five years or younger. The research has established that there are three distinctly different child health information purposes to be achieved via telephone. One is telephone triage and advice for a child with trauma or symptoms that concern the parent. Telephone triage of children with a suspected illness is excluded from the definition of community Well Child services and so is outside of the scope of this report. Another is provision of advice and guidance that relates to healthy development of the child, and that in particular focuses on the Well Child Framework. The third is guiding parents to authoritative sources of Well Child information. This report examines the literature in respect of Well Child-related telephone health services.
Child health telephone lines from a nursing perspective The main challenge in telephone health services is the difficulty of accurately assessing a situation with limited sensory input. It is different from face-to-face assessments as information is gathered through a limited conversation on the phone. The assessments are often made in a crisis and one must rely on the client for information that may be inaccurate or incomplete (Canadian Nurses Association 2000; Canadian Nurses Protective Society 1997; Edwards 1994; McMullen 1998). In relation to child health telephone services, the conversation is usually with a parent or caregiver. When their child is ill, many parents feel insecure and seek assistance in sorting out their child’s medical problem (VanDinter 2000). It can be a challenge to accurately assess the severity of the situation when dealing with an anxious parent or caregiver. Greenberg (2000a) evaluated an established nurse-run telephone service in a paediatric outpatient setting. The study found that nurses were valued for their listening and communication skills, their ability to extract information from the caller, and their ability to impart information in a way that the particular patient could understand. There is no indication in the literature as to what skills a telenurse must possess. There appears to be consensus that the nurse must have a minimum of three to five years’ nursing experience, preferably in a variety of settings, as well as exceptional interpersonal skills and superior communication skills both verbally and in writing. In addition, possessing knowledge of community resources and an ability to work well under pressure are assets in practice (Canadian Nurses Association 2000; Coleman 1997; Hoare et al 1999; VanDinter 2000).
Responding to calls about children Forty percent of calls to NHS Direct are about children. Monaghan et al (2003) saw a need to identify whether nurses with specific paediatric qualifications differ in dealing with triage calls about children. In particular, they sought to determine whether there was a difference in call length and outcomes when triaging children who presented with rash or fever by telephone. In New Zealand, there is a distinction between the roles of

Parent Information Project 27
Well Child and paediatric nurses. Paediatric nurses specialise in delivery of nursing care to unwell children or children with chronic conditions usually within hospitals or outpatient clinics. Well Child nurses specialise in community child health nursing, which includes health promotion and education, screening and surveillance, and provision of support to the child and family. Currently, all Well Child calls are required to be handled by a Well Child specialist nurse. Calls about sick or symptomatic children are handled by nurses with specific training in teletriage. Monaghan et al found in a sample of child health calls to NHS Direct that the mean length of calls handled by registered paediatric nurses was significantly shorter than that of other registered nurses. Both groups of nurses referred to triage outcomes groups with similar frequency (i.e. similar frequency of call dispositions by call type). These results do not explain why there is a difference in call length between paediatric and other registered nurses. Monaghan et al consider it likely that nurses having undergone paediatric nursing education are able to assess children more quickly. Nurses reach conclusions by focusing on contextually bound nuances which are the components of expertise. Nurses, from telephone training onwards, are encouraged to try to build pictures in their ‘mind’s eye’ of the child and their environment (Edwards 1994, 1998). This approach is supported by Pettinari and Jessopp (2001) who demonstrated that visualisation work is intimately tied to interactional practices of nurses and callers. The ability to get the essential information on which to make a decision rests on the ‘packaging’ of the questions. This means that the nurse needs to extract the vital information by adjusting the types of question to an appropriate level for the caller to understand and be able to respond. Monaghan et al (2003) argue that only then will the nurse be able to make an appropriate and safe decision. The visualisation will elicit a faster response if the nurse has encountered a situation before and in a variety of contexts. Yanovski et al (1992) state that the correct decisions seemed to be determined by the interpretation of the information collected, and not by the number or type of questions asked, and that experience played an important part in triage. Monaghan’s and Yanovski’s findings suggest that nurses with more experience and specialisation in dealing with particular types of health issues are likely to be more efficient in providing similar telephone health services. Although Monaghan’s research is in respect of paediatric nurses, the principle they have demonstrated appears to support continuation of the need for Well Child-related telephone calls to be answered by Well Child trained and experienced nurses.
Maternal and child health lines in the USA Summarised below are examples of different types of child health lines from the USA – toll-free hotlines, Parent Line, a nurse-managed paediatric community clinic and teletriage provided by children’s hospitals.

Parent Information Project 28
Toll-free hotlines The toll-free hotlines in the USA were originally created for prenatal assistance alone but now cover a wide range of early childhood issues (Booth et al 2004). They began operating in the 1980s as Medicaid was expanding eligibility for pregnant women. Many states supported toll-free lines to ensure that low-income women had access to referrals for prenatal care. The federal Maternal and Child Health Block Grant programme required states to establish a toll-free line with a strong focus on helping children enrol in Medicaid. These lines had to provide families with, at a minimum, information on health care practitioners, Medicaid providers and other relevant health-related providers in the state. Although the country’s maternal and child hotlines operate independently of one another, a national 800 number (1-800-311-BABY) maintained by the Maternal and Child Health Bureau automatically connects callers to their state line. Some states have gone so far as to link their toll-free numbers to a greater number of community-based services. Booth et al also recommended that a website should be established for each line to make the information more easily accessible. The most frequent queries to these hotlines have involved health insurance (85 percent), child development concerns (38 percent), parenting and child rearing (27 percent) and children with emotional or mental health needs (25 percent). The majority of hotlines are available only during normal business hours, with provision for leaving messages after-hours. A fraction of them offer access 24 hours a day, seven days a week. Most of the hotlines are staffed by social workers and health professionals, and in some cases parents. Many have staff that speak other languages or provide translation services for non-English-speaking families. For the deaf or hearing impaired, over 60 percent of the hotlines offer text facilities. Callers can expect to be provided with information specific to their question or a referral to another health line or community-based agency. Many states avoid duplication by sharing operators, facilitating three-way calling, or co-locating staff from the various lines. In addition to federal funding, the hotlines sometimes receive financial support from other sources. In some states, early intervention programmes and the Supplemental Nutrition Program for Women, Infants, and Children also provide funding.
Parent Line Parent Line resulted from a five-year trial of a telephone intervention to reduce low birthweight and preterm births. In that study, low-income pregnant women were randomised to telephone contact (intervention) or usual care (control) groups (Moore and Krowchuk 1997). Women in the intervention group received one or two calls a week from a nurse when they were between 24 and 37 weeks’ gestation. The content of the calls included an assessment of potential signs of preterm labour, fluid intake, nutrition, smoking, and
Parent Information Project 29
substance use when appropriate. Nurses also helped the intervention group to address issues and problems in their lives and to contact appropriate community resources. There was a 26 percent decrease in the number of low birthweight births and a 27 percent reduction in births prior to 36 completed weeks’ gestation when compared with the control group. For African American mothers who were in the intervention group, there was a 44 percent decrease in low birthweight births and preterm births. Women who received telephone support during the study frequently asked that the calls continue after birth so Moore and Krowchuk sought funding for such a service. The immediate catalyst for Parent Line was a programme in North Carolina called Smart Start. In addition to funding Parent Line, Smart Start provides community-based family outreach and service co-ordination, therapeutic services for children whose parents are in substance abuse treatment, parenting materials for all parents, vision screening for low-income children, transportation services, a fathers’ peer counselling programme, nutrition outreach education to low-income communities and a number of other early childhood services. The goal of Parent Line is to improve the health and development of children from birth to five years of age through a combination of three strategies: 1. a weekly or fortnightly call from a nurse to the child’s parent to address specific
age-related health and development issues 2. a telephone hotline that any parent in the community can use to ask a question
about child health and development or to locate appropriate community resources 3. for parents lacking telephones, weekly home visits from an outreach worker. Although children are the focus of Parent Line, the nurses recognise that when parent needs are unmet, child needs are also likely to suffer, so parents’ issues are also topics for Parent Line discussions. Moore and Krowchuk conclude that implementation of a programme such as Parent Line could result from expansion of nursing practice by a nurse entrepreneur who seeks funding from public or private sources, or could result from an expansion of a current programme in a hospital or community agency.
Nurse-managed paediatric community clinic A nurse-managed health centre model was developed in response to growing demand for accessible primary care in the community and as a result of the expanded role of the advanced practice nurse in primary care (Kinsey and Buchanan 2002). These health centres are managed by nurses in partnership with the communities they serve. They are part of a safety net that provides health care to the underinsured and other vulnerable populations (Hanson-Turton 2005). They provide holistic health care and patient-centred health promotion and disease prevention.

Parent Information Project 30
A study by Beaulieu and Humphreys (2008) looked at the impact of implementing a nurse telephone advice service within one of these centres. The situation at the particular centre involved was complicated by the fact that up to half of the callers are Spanish speaking. In addition, many of the callers are grandparents who have their own health problems. A bilingual, bicultural nurse with previous experience in paediatric health care was hired and given additional training in paediatric telephone advice and triage. Comparisons were made between the experiences of a pre-implementation sample of patients and post-implementation group of parents/caregivers. Two statistically significant differences between groups were found. The first concerned the main reason for calling the clinic: the post-implementation group was more likely to call regarding concern about a health problem or for advice (70 percent compared with 30 percent of the pre-implementation group). The other regarded the importance placed on shared decision-making between the nurse and parent/caregiver: the entire post implementation group said this feature was important (compared with 80 percent of the pre-implementation group). The results of the introduction of the telephone advice nurse were: • provision of prompt, consistent, high-quality care to ethnically diverse children and
families • more balanced clinic flow (morning and afternoon equally busy) • greatly reduced burden on providers to respond to clinic calls • involvement as part of the team to manage the care of a child (e.g., a child having an
asthma attack) both in the clinic and at home or elsewhere • providing an unexpected continuity between patients and providers that was
particularly evident in children and families with the most complex needs and unstable circumstances.
Telephone services offered by children’s hospitals As the paediatric health care environment in the USA becomes more competitive, many children’s hospitals are seeking ways to strengthen their relationships with and increase the loyalty of referring physicians, patients and parents (Lewin 1995; Poole and Schmitt 1993). As part of this effort, many children’s hospitals have developed telephone advice programmes (Pert et al 1996). These programmes are generally delivered by paediatric nurses using standardised protocols. They provide both after-hours telephone advice to parents regarding children who have been referred by physicians, and telephone advice to the general public as part of a health information line (Anders 1997; Fox-Gleissman et al 1995; Poole 1999; Wolcott et al 1995). High levels of satisfaction and some improvements in physician allegiance have been described among physician users of telephone advice programmes. Telephone advice programmes may also increase patient satisfaction through the provision of credible,
Parent Information Project 31
consistent, useful and rapid responses to parental questions and concerns (Poole and Schmitt 1993; Young et al 1998).
Overall findings What this review of the literature reveals is that delivery of nurse-led telephone information and advice services has expanded over the last two decades. These services offer a clinically effective and cost-effective way to assess the needs of children and parents and provide valuable information and advice in response to questions and concerns from parents. Overseas, child health and development lines tend to have been set up at the community level and are integrated with similar community health services. The advantages of this model over a national service are that parents are more likely to be linked with other services in their community, access to a child’s health record is more likely and continuity of care with their community health provider is improved. However, in countries that employ this model, suggested enhancements include linking these community child health and development lines through a national 0800 number to improve access and integrating the service more strongly with other community services. In New Zealand, telephone triage services of symptomatic people of all age groups are delivered nationally within the continuum that extends from primary health care, through after hours to emergency services. Telephone triage of children with a suspected illness is excluded from the definition of community Well Child services. New Zealand is in the unique position of having the majority of community Well Child services delivered by one national organisation. This structure provides an opportunity to completely integrate Well Child telephone advice with community Well Child services whilst retaining the added advantages of providing this service via one national Well Child telephone line. Therefore, this report recommends that Well Child telephone advice should sit within the package of services delivered in the Well Child programme and be intimately linked to the other Well Child services being delivered within the community.

Parent Information Project 32
Text Messaging Amongst the tools potentially available to a parent, the mobile telephone and the computer have the richest communication and education functionality because they are able to present information to a parent in written form, as spoken words or as images. However, there is no longer a clear distinction between these two devices. The sources of information available to a parent, and the ease with which it can be shared with others, has dramatically changed as a result of mobile telephones. These devices are now common and they are profoundly affecting how people socialise too. Many of these phones are able to access the internet. The wireless technology that they employ enables users to receive information at a speed and with a richness of image quality that was previously restricted to television. The limitation of needing a fixed broadband cable connection has gone, and with it the restraint that a parent could only get information when they were at a particular place with an internet connection. It is the computer and mobile telephone that have enabled the phenomenon of social networking which depends on immediate access between people irrespective of location. Social networking employs blogs, chat rooms, wikis, bulletin boards, podcasts, text messaging, email, internet telephony (e.g., Skype), exchanging of audiovisual material, automatic text to word conversion, automatic translation of text from one language to another, and so on. (For further information on these social networking terms, see http://www.commoncraft.com/store/socialmedia for three-minute tutorials.) Because of the popularity of social networking, particularly amongst young people, a large provider of health services in the USA, Humana, is studying the ways in which it can be mobilised to support health-seeking behaviour. In particular, it is studying the notion that health and entertainment should be linked. Its precept is that by creating a culture where healthy behaviour is cool, people will then want to be healthy and will be inspired to do things that are healthy. Humana is testing its claim that one route to changing culture is combining health and entertainment by developing health and wellness promotion programmes and looking for opportunities to integrate health entertainment. The fundamental drivers it is using are ‘eco health’, ‘social hubworking’ and ‘tracking and rewards system’ (e.g., personal health monitoring and feedback like wearing a watch).
Mobile phones Part of this project involved looking at the literature on the use of mobile phones for delivering health information and advice. Mobile phones have the potential to solve the problem of access to the information, irrespective of whether the person has a computer and irrespective of their access to broadband. Additionally, mobile telephones are able to be used by those with hearing difficulties via text and image, and by parents with limited sight through the delivery of information in audio form.
Mobile-based technologies have the potential to change the dynamics of monitoring and self-management (Pagliari et al 2005; Tachkara et al 2003). Examples are:

Parent Information Project 33
• an electronic meter linked with a mobile phone so that peak flow recordings and current symptoms can be sent to a central server accessible to both patients and their clinicians (Pinnock et al 2006)
• improved compliance with intensive insulin regimes in teenagers with diabetes (Franklin 2003)
• improved adherence to treatment in adults with hypertension (Friedman et al 1996) • reduced hospitalisation in people with heart failure (Louis et al 2003) • monitoring and increased confidence in self-management among people with asthma
(Rasmussen et al 2005; Ryan et al 2005). Texting (like email) can be a useful form of communication in non-urgent situations (D’Allessandro 2004), is time-saving for both health professional and patient, and reduces the telephone tag that frequently occurs when trying to make contact.
Text messaging – diabetes Franklin (2003) developed a novel support network (Sweet Talk) using a unique text messaging system to deliver diabetes information and support to young people. The Sweet Talk intervention uses a process of sequential goal-setting to increase a sense of self-efficacy for controlling diabetes (Bandura 1982). This approach is based on theories that health behaviour is influenced by patients understanding the severity of their disease and the benefits of changing behaviour; and that providing reminders, feedback and support reinforces positive behaviour change. Patients are encouraged to use the system to ask questions related to their diabetic care. If patients have questions that they do not wish to leave until the next clinic visit or find difficult to ask in clinic settings, they may be encouraged to use text messaging as this may be less intimidating than face-to-face dialogue with their doctor (Gustafson and Pal 1999; Marrero 2000).
Text messaging – improving outpatient attendance In a study by Downer et al (2006), parents of patients of the Royal Children’s Hospital in Melbourne who were scheduled to attend an outpatient clinic appointment were sent a text message reminder. Ninety percent of these patients attended their appointment. Eighty percent of the patients in the control group attended their appointment. Appointments that patients fail to attend or do not attend are a significant and widespread problem in the health system. Not only do they waste clinical and administrative resources, they also reduce revenue opportunities, increase waiting times for appointments and lengthen treatment times. Traditional reminder methods such as telephone calls and posted letters have high unit costs and require significant staff resources to administer. The cost of sending the text message reminders over the three-month study period was A$5,164. This total equates to A$0.25 per success, significantly lower than the cost of sending letters, post cards or automated telephone messages.

Parent Information Project 34
This report recommends that novel forms of delivery of Well Child information, advice and support, such as those described above, should be trialled and evaluated as part of implementing integrated telephone and website services for Well Child. Text messaging – Information service Many service providers are exploring the use of text messaging to complement their services, which may be delivered face-to-face, by telephone and/or by website. The use of text messaging as part of these services is seen as a method to increase accessibility of information, to promote services and to reduce demand on other services by sending reminders and responding clients in a less resource intensive way. One good example within the government sector is Career Services, which provides career advice to individuals through face-to-face services, an 0800 number, and website including chat rooms, twitter and email. Career Services has also trialled the use of text messaging with young adults and has found this to be an economical and effective method for communicating information. The Ministry proposes to build on the experience of other services and pilot text messaging as appropriate within the integrated child health telephone and website service.

Parent Information Project 35
Support As the Introduction stated, support is one of three key components required to meet the Well Child information and advice needs of a parent. This final section takes account of recent literature about peer support from Australia, Canada, UK and USA. Telephone peer support is widely available through helplines. It has the advantage of offering greater accessibility and potentially more availability than face-to-face contact and it is extensively used in the voluntary sector.
What is peer support and why is it important? The most thorough definition of peer support describes a peer as a created source of support, internal to a community, who shares salient target population similarities (e.g., age, ethnicity, health concern or stressor) and possesses specific knowledge that is concrete, pragmatic and derived from personal experience rather than formal training (Dennis et al 2002). Peer support has also been defined as the giving of assistance and encouragement by an individual considered equal. Within a health care context, peer support is the provision of emotional, appraisal and informational assistance by a created social network member who possesses experiential knowledge of a specific behaviour or stressor and similar characteristics to the target population (Dennis 2003). Dennis defines each of the above components of assistance as follows.
• Emotional support includes expressions of care, encouragement, attentive listening, reflection, reassurance and usually the absence of criticism.
• Appraisal support involves the communication of information that is pertinent to self-evaluation and encompasses expressions that affirm the appropriateness of emotions, cognitions and behaviours.
• Informational support is the provision of knowledge relevant to problem-solving. The need for peer support arises because health professionals alone are unable to address all of the health care needs of patients (Department of Health 2000). Peer interventions have been applied to disease-related, prevention and health promotion topics (Dennis et al 2002). A range of approaches such as individual one-to-one sessions, self-help/support groups, online computer-mediated groups, and telephone contact have been used. Such interventions are intended to meet the support and informational needs of patients, as well as to relieve the pressure on mainstream health services. Peer interventions tend to involve peer/lay individuals with knowledge gained through experience who extend embedded social networks and complement professional health services (Dennis 2003). There is evidence that offering support to other people can be beneficial for the helper, as well as the person being helped. For the helper, volunteering can result in:

Parent Information Project 36
• improved physical health (Moen et al, 1989; Schwartz and Sprangers, 1999) • increased feelings of self-worth (Hainsworth and Barlow, 2001, Mowbray et al, 1996
and Omoto et al, 2000) • reduced depressive symptoms (Hainsworth and Barlow, 2001) • improved communication skills (Mowbray et al, 1996) • changes in self-management behaviours (Barlow et al, 2005). Dale et al (2008) examined the effects seven randomised control trials of peer support telephone calls on physical and psychological health, and on health behaviours. In all seven studies the intervention was delivered by telephone to participants in their homes. These interventions were aimed at: • improving depressive symptoms in women at high risk for post-partum depression
(Dennis 2003) • increasing self-efficacy and improving diet in people recovering from a myocardial
infarction or angina (Carroll 2006; Heller 1995) • encouraging breastfeeding in primiparous, breastfeeding women over 16 years old
(Dennis et al 2002) • increasing mammography usage in women aged over 40 years (Calle 1994; Duan
2000) • increasing self-efficacy in people with type 2 diabetes (Dale 2007). The seven studies described a wide variety of methods for recruiting peer advisors including through local support groups, flyers, advertisements and word of mouth, local churches and rehabilitation services.
Peer telephone interventions for new mothers From the studies reviewed by Dale et al we have chosen the two by Dennis (2002, 2003), which examined the impact of peer support telephone calls for new mothers. Both studies provided emotional, appraisal and information support.
Breastfeeding support Dennis et al (2002) investigated the efficacy of peer telephone support on the duration of breastfeeding. The intervention was a call within 48 hours of hospital discharge, followed by calls as frequently thereafter as the mother deemed necessary. Rates of exclusive breastfeeding were determined using self-report questionnaires developed for the study. Table 12: Data from Dennis et al’s (2002) study of peer support on duration of breastfeeding
Outcome Duration Intervention group Control group
4 weeks 92% 84% 8 weeks 85% 75%
Mothers breastfeeding
12 weeks 81% 67%

Parent Information Project 37
As Table 13 shows, significantly more mothers in the peer support group than in the control group continued to breastfeed exclusively at three months post partum. Mothers reported that having a peer supporter available when difficulties were experienced (i.e., on demand), increased their confidence, decreased their concerns and assisted them in reaching their breastfeeding goals. Women who received peer support telephone interventions were more satisfied with their method of infant feeding compared with the control group. Also 85 percent of mothers in the intervention group stated that, if offered, they would choose to have a peer supporter again.
Postnatal depression support Dennis (2003) also investigated the efficacy of peer support telephone calls on post-partum depression. The intervention was a call within 48 to 72 hours of hospital discharge, followed by calls as frequently thereafter as the mother deemed necessary. The primary outcome measure was depressive symptoms determined using the Edinburgh Postnatal Depression Scale (EPDS). A score greater than 12 indicates that the person is likely to suffer from postnatal depression. Table 13: Data from Dennis’s (2003) study of peer support on postnatal depression symptoms
Outcome Timing of assessments Intervention group Control group
4 weeks 45% 73% EPDS >9 8 weeks 35% 73%
4 weeks 10% 41% EPDS > 12 8 weeks 15% 52%
As Table 14 shows, the depressive scores of women who received telephone peer support were significantly reduced when compared with the control group. At the four-week assessment, 41 percent of mothers in the control group scored higher than 12 on the Edinburgh Scale compared with only 10 percent in the intervention group. At the eight-week assessment, 52.4 percent of the mothers in the control group scored higher than 12 on the Edinburgh Scale compared with 15 percent of mothers in the experimental group. In a post hoc analysis, the frequency and occurrence of peer volunteer interactions were not correlated with Edinburgh Scale scores at the eight-week assessment. This finding suggests that there was not a simple ‘dose effect’ between the amount of the intervention received and its benefit.
The experience of being a peer telephone supporter Three of the studies reviewed by Dale et al (2008) provided qualitative data reporting the peers’ experience of providing support (Carroll 2006; Dale 2007; Dennis et al 2002). The three key themes that emerged were that peer supporters: 1. needed to feel that they were of help to the recipient

Parent Information Project 38
2. valued the sharing of experience 3. sometimes felt confronted by their own anxieties and vulnerability. In the study by Dennis et al (2002), supervision was perceived positively by many peer supporters. Dale (2007) reported that a few peer volunteers felt that more guidance and feedback would have been helpful, particularly in the early stages of the intervention. The need for constant proactive support and regular calls from the training facilitator was emphasised, even though the peer volunteers could themselves contact someone at any time.
Content of peer support interventions Content analysis of the interventions from these studies confirmed the three themes of peer support as informational support, appraisal support and emotional support, as defined by Dennis (2003). There was evidence that informational support may be effective in encouraging dietary change in patients’ post-myocardial infarction (Heller 1995) and in increasing mammography usage in women aged over 40 years (Calle 1994; Duan 2000). There was also evidence that a combination of informational, appraisal and emotional support contributed to the intervention’s effectiveness when targeting more complex behaviours and conditions, such as encouraging breastfeeding in new mothers (Dennis et al 2002) and improving depressive symptoms in women at high risk for post-partum depression (Dennis 2003). However, emotional support alone failed to encourage recovery behaviours in people post-myocardial infarction (Carroll 2006), and emotional and appraisal support was not effective in increasing self-efficacy or improving glycaemic control in people with type 2 diabetes (Dale 2007). These limitations on the success of this approach suggest that emotional and/or appraisal peer telephone support may need to be combined with informational support to have a beneficial effect on more complex health behavioural changes. The review concluded that those studies that included informational support (with or without appraisal support and emotional support) emerged as being more effective than those that lacked an informational support component. It seems doubtful that informational support by peers ever occurs in the absence of at least some emotional or appraisal support. The social interaction implicit in all types of peer support may be particularly important, even when the main intent of a peer telephone intervention is the imparting of information. As described above, peer support was effective in providing support to mothers to increase the continuation of breastfeeding (Dennis et al 2002). Most of the women receiving support (75 percent) had a college or university education. The extent to which this intervention would have been effective in a less educated or more socially disadvantaged population is unknown. A shared cultural, educational and socioeconomic background may be important in contributing to the impact of peer support telephone calls.

Parent Information Project 39
Training and experience of peer supporters There have been few comparisons of different approaches to telephone support within the same study. No studies have compared ‘novice’ peer supporters and more experienced supporters. It is possible that with increasing experience, peer supporters become more effective in their support. Conversely, increasing experience may lead to a loss in peer effect if greater experience is associated with an increase in para-professionalism. The studies reviewed did not report the extent of telephone support experience that peers had prior to entering the trials. In the UK, the National Institute for Health and Clinical Excellence (NICE) recommends a change in the way breastfeeding support is delivered, from a reactive to a proactive service. It recommends that all new mothers (particularly those who are least likely to start and continue to breastfeed) are called by a peer supporter within 48 hours of returning home from hospital (or 48 hours after a home birth) (NICE 2008). It also recommends that commissioners and managers of maternity and children’s services ensure that peer supporters: • attend a recognised, externally accredited training course in breastfeeding peer
support • offer new mothers ongoing support according to their individual needs, which could
be delivered face-to-face, via telephone or through local groups • can consult a health professional and are provided with ongoing support • gain appropriate child protection clearance. Dale et al’s review found insufficient information about the training of peers to reach an understanding of the levels of training or support required to meet the different target needs and populations to produce optimal performance. It is recommended that peer support initiatives should be included in the integrated Well Child website, telephone and community services. However, given some of the questions that remain regarding training and essential qualities of peer support programmes, it is also recommended that these initiatives are trialled and evaluated prior to widespread roll-out.

Parent Information Project 40
Findings and Recommendations The findings and recommendations presented here are primarily about parents’ information, advice and support needs from a Well Child focus. The present systems are fragmented and a parent is confronted with a bewildering array of sources of information, not all of which are accurate. These proposals for the way in which these services are delivered are intended to make it easier for parents to access Well Child information and services. This report strongly supports the integration of telephone and internet services for effective delivery of the Well Child Framework and provision of information and advice services to a parent (whether face-to-face or on demand).
Major findings in this report Health professionals in New Zealand agree with their Australian counterparts on the content of Well Child information and support that parents need. This content also mirrors the type of Well Child information that parents say that they want, with the most important being information on what parents can do to promote their child’s development and what development to expect at different ages. In terms of process issues, New Zealand health professionals agree that parents need different information, in different forms, at different times; consistent, credible messages; face-to-face relationships with professionals; and access to a range of services and support at different times. New Zealand parents preferred sources of Well Child information are the internet (52 percent); face-to-face communications with professional advisors (38 percent); telephone helplines especially PlunketLine (32 percent) and brochures or fact sheets on specific issues (22 percent). Parents find face-to-face communication with health professionals and the current Well Child telephone services highly useful (93–94 percent). While parents rank the internet as their most preferred source of information, only 41 percent of New Zealand parents surveyed had used the internet as a source of Well Child information in the last six months suggesting there is room for improvement in this method of delivery. There was unanimous agreement amongst New Zealand health professionals about the importance of the internet as a source of information for parents. Parents agree, with over half listing the internet as their preferred source for Well Child information. The main theme that came through was that no matter what the source of the information, it needed to be consistent and true, reinforcing the information received through other sources. International evidence suggests that parents can successfully use the internet to supplement or influence the content of their face-to-face contacts with a health professional. This form of internet use can enhance the Well Child visit for the parents and increase the rate at which parents adopt preventive measures.

Parent Information Project 41
Overseas, access to health information has been broadened and the consistency of that information has been improved by integrating telephone health lines with websites. This project adopts the same recommendation of integration of telephone and website information services for provision of Well Child information to parents. The report also highlights that for provision of support to be effective, it requires three components: informational, emotional and appraisal. These components can most effectively be delivered by a ‘peer’, defined as somebody integral to a person’s community. These findings, along with the recommendations for better integration from the Well Child Framework Review, provide the rationale for the conclusion that provision of Well Child information and support via telephone or website is an integral part of the Well Child programme.
Principle underpinning the recommendations A parent of a child under the age of five years needs a combination of Well Child services on demand, which include information, support and the making of arrangements for face-to-face services. The remotely accessed services recommended in this report are intended to complement face-to-face Well Child services delivered in the community rather than to replace them.
Recommendations for provision of Well Child telephone and internet services Delivery of Well Child information, advice and support to parents on demand should be integrated with Well Child/Tamariki Ora services that are being delivered in the community. Parents should have access to consistent, on-demand Well Child information and advice via telephone, website, DVD and printed materials. The Ministry of Health should be the source of all authoritative health information in either of the following ways: • directly through the authoring of fact sheets, podcasts etc by the Chief Advisor, Child
Health • via accreditation and information prescription of reputable information sources, e.g.,
kidshealth. The website model from Christakis et al (2006) should be adopted as the basis for dissemination of all Well Child information and advice. The results would be the creation of a Child Health website that: • is the one true source of Well Child information for parents • is modelled on the following websites:
– http://raisingchildren.net.au/ – http://www.nhs.uk/nhsdirect/Pages/nhsdlanding.aspx – http://www.netmums.com/h/n/SUPPORT/HOME/ALL/464// – http://www.aboutmyhealth.org/

Parent Information Project 42
– http://www.thelowdown.co.nz/#/home/ • is integrated with the Well Child telephone health line • provides maternal and child health support, advice and information to a parent by
telephone and responds to emails and texts as if the ‘caller’ had used the phone • provides information about the Well Child Framework, anticipatory guidance and
‘ages and stages’ information that is relevant to individual parents and their children • makes maternal and child health arrangements between a parent and a provider and
delivers reminders by text message • has web-based algorithms for home treatment and health care behaviour • provides details of availability of maternal and child health services local to the
parent’s community, in an approach similar to Netmums in the UK and Raisingchildren in Australia
• makes the website material available in a wide variety of languages (e.g., using text conversion services provided free of charge by AltaVista and Yahoo) and as audio via automatic conversion of text
• operates web-based blogs, bulletin board and forums for parents • delivers information and advice in audiovisual formats, e.g., webinars, DVDs, video
clips and interactive TV • acts as a portal with links to other reputable child health websites as prescribed by
the Ministry of Health. Based on the evidence from overseas, this report recommends that the Child Health website should be integrated with the Well Child telephone line. It also recommends that the Child Health website and Well Child telephone line should sit within the package of services delivered in the Well Child programme and be intimately linked to the other Well Child services being delivered within the community. Opportunities for networking between the national Well Child telephone advisory service and its staff and various single purpose support lines dealing with Well Child topics should also be considered. This report recommends that novel forms of delivery of Well Child information, advice and support via mobile phone and text messaging should be trialled and evaluated as part of implementing integrated telephone and website services for Well Child. The integrated Well Child information and advice services should foster, encourage and support a vibrant network of support groups that are operated by parents as volunteers (breastfeeding, parenting, mental health, special needs). Different models for delivery of peer support (e.g., via telephone, website, parent groups) should be explored and evaluated, as should the potential of social networking.

Parent Information Project 43
Bibliography 10th Annual National Telephone Triage Conference. 2003. Telephone triage 2003. San Anselmo, CA: TeleTriage Systems. URL: http://www.teletriage.com/conference/index.html
Abdullah AS, Mak YW, et al. 2005. Smoking cessation intervention in parents of young children: a randomised controlled trial. Addiction 100(11): 1731–40.
Ad Hoc Committee on Health Literacy. 1999. Health Literacy: Report of the Council on Scientific Affairs. Journal of the American Medical Association 281: 552–7.
Adkins JW, Storch EA, et al. 2006. Home-based behavioral health intervention: use of a telehealth model to address poor adherence to type-1 diabetes medical regimens. Telemedicine Journal and E-Health 12(3): 370–2.
Adler KG. 2006. Web portals in primary care: an evaluation of patient readiness and willingness to pay for online services. Journal of Medical Internet Research 8(4): e26.
Advisory Committee on Health Infostructure. 2000. National Health Technical Infostructure: Blueprint and preliminary tactical plan: Blueprint report: Consultation document. Ottawa: Health Canada.
Alberta Heritage Foundation for Medical Research. 1998. Telephone Nurse Triage Services. Edmonton: The Foundation.
Allen RD (ed). 1990. The Concise Oxford Dictionary of Current English. 8th ed. Oxford: Clarendon Press.
American Nurses Association. 1999a. Competencies for Telehealth Technologies in Nursing. Washington: American Nurses Association Publishing.
American Nurses Association. 1999b. Core Principles on Telehealth. Washington: American Nurses Association Publishing.
American Nurses Association. 2001. Developing Telehealth Protocols: A blueprint for success. Washington: American Nurses Association Publishing.
Anders G. 1997. Triage by phone. Wall Street Journal 4 February, A1.
Anderson GD, Nelson-Becker C, et al. 2005. A patient-centered health care delivery system by a university obstetrics and gynecology department. Obstetrics and Gynecology 105(1): 205–10.
Aslam N, Bowyer D, Wainwright A, et al. 2005. Evaluation of internet use by paediatric orthopaedic patient and the quality of information available. Journal of Pediatric Orthopaedics Part B, 14: 129–33.
Awadallah S, Halaweish I, et al. 2006. Tele-echocardiography in neonates: utility and benefits in South Dakota primary care hospitals. South Dakota Medicine: The Journal of the South Dakota State Medical Association 59(3): 97–100.
Baker D, Parker R, Williams M, et al. 1998. Health literacy and the risk of hospital admission. Journal of General Internal Medicine 13(12): 850–1.
Bandura A. 1982. Self-efficacy mechanism in human agency. American Psychologist 37: 122–147.
Bandura A. 1989. Social cognitive theory. Annals of Child Development 6: 1–60.

Parent Information Project 44
Barbour J. 2005. Internet sites for parents children and young people. In: R Wootton and J Batch (eds) Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press.
Barger SE, Nugent KE, Bridges W. 1993. Schools with nursing centers: a year follow-up study. Journal of Professional Nursing 9: 7–13.
Barlow J, Coren E. 2001. Parent-training programmes for improving maternal psychosocial health. Evidence-based Nursing 4(81).
Barlow J, Coren E, Stewart-Brown S. 2005. Parent-training programmes for improving maternal psychosocial health. Campbell Systematic Reviews.
Battista RN, Lawrence RS. 1988. Implementing preventive services. American Journal of Preventive Medicine 4: 1–194.
Beall MS, Golladay GJ, Greenfield ML, et al. Use of the internet by pediatric orthopaedic outpatients. Journal of Pediatric Orthopedics 22: 261–4.
Beaulieu R, Humphreys J. 2008. Evaluation of a telephone advice nurse in a nursing faculty managed pediatric community clinic. Journal of Pediatric Health Care 22(3): 175–81.
Belman S, Chandramouli V, et al. 2005. An assessment of pediatric after-hours telephone care: a one-year experience. Archives of Pediatrics and Adolescent Medicine 159(2): 145–9.
Bensink M, Wootton R, et al. 2007. Investigating the cost-effectiveness of videotelephone based support for newly diagnosed paediatric oncology patients and their families: design of a randomised controlled trial. BMC Health Services Research 7: 38.
Bentley PJ, Turner VF, Hodgson SA, et al. 2005. A central role for the health call centre. Australian Health Review 29(4): 435–8.
Berland GK, Elliott MN, Morales LS, et al. 2001. Health information on the internet: accessibility, quality and readability in English and Spanish. Journal of the American Medical Association 285(20): 2612–21.
Bernhardt JM, Felter EM. 2004. Online pediatric information seeking among mothers of young children: results from a qualitative study using focus groups. Journal of Medical Internet Research 6(1).
Bethell C, Reuland CH, Halfon N, et al. 2004. Measuring the quality of preventive and developmental services for young children: national estimates and patterns of clinicians’ performance. Pediatrics 113(suppl): 1973–83.
Birch S, Glasper EA, et al. 2005. GP views of nurse-led telephone referral for paediatric assessment. British Journal of Nursing 14(12): 667.
Bird B, Zarum R, Renzi F. 2001. Emergency medicine resident patient care documentation using a handheld computerised device. Academic Emergency Medicine 8(12): 1200–03.
Black KL. 2007. Standardisation of telephone triage in pediatric oncology. Journal of Pediatric Oncology Nursing 24(4): 190–9.
Blake J. 2006. Supporting anxious parents in search of internet information. Nursing Times 102(19): 24–6.
Bloggapedia. Child Health Blog Posts. URL: http://www.bloggapedia.com
Parent Information Project 45
Bogin J. 2006. Enhancing developmental services in primary care: the Help Me Grow experience. Journal of Developmental and Behavioral Pediatrics 27(1 Suppl): S8–12; discussion S17–21.
Bolli S, Melle GV, et al. 2005. After-hours paediatric telephone triage and advice: the Neuchatel experience. European Journal of Pediatrics 164(9): 568–72.
Booth M, Brown T, et al. 2004. Dialing for help: state telephone hotlines as vital resources for parents of young children. Issue Brief (Commonwealth Fund) (787): 1–12. URL: http://www.cmwf.org
Borowitz SM, Rittband L. 2001. Using the internet to teach parents and children about constipation and encopresis. Med Informatics and the Internet in Medicine 264(4): 283–95.
Boston M, Ruwe E, et al. 2005. Internet use by parents of children undergoing outpatient otolaryngology procedures. Archives of Otolaryngology -- Head and Neck Surgery 131(8): 719–22.
Bouche G, Migeot V. 2008. Parental use of the internet to seek health information and primary care utilisation for their child: a cross-sectional study. BMC Public Health 8: 300.
Boulton AJM. 1993. DCCT: implications for diabetes care in the UK. Diabetic Medicine 10: 687.
Bower DJ, Barry N, et al. 2005. Designing and implementing e-health applications in the UK’s National Health Service. Journal of Health Communication 10(8): 733–50.
Boyer EW, Lapen PT, et al. 2007. Dissemination of psychoactive substance information by innovative drug users. Cyberpsychology and Behavior 10(1): 1–6.
Bristol S. 1993. Telephone advice for parents of newborns. Nebraska Nurse 26(1): 8–9.
Britt DW, Norton JD, et al. 2006. Equity in the development of telemedicine sites in an Arkansas high-risk pregnancy programme. Journal of Telemedicine and Telecare 12(5): 242–5.
Britton C, McCormick FM, et al. 2007. Support for breastfeeding mothers. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD001141/frame.html
Burns N, et al. 2001. The Practice of Nursing Research Conduct, Critique, and Utilisation. Philadelphia: WB Saunders.
Callahan CW, Malone F, et al. 2005. Effectiveness of an internet-based store-and-forward telemedicine system for pediatric subspecialty consultation (Brief record). Archives of Pediatrics and Adolescent Medicine 159(4): 389–93.
Calle EE, Miracle-McMahill HL, Moss RE, et al. 1994. Personal contact from friends to increase mammography usage. American Journal of Preventive Medicine 10: 361–6.
Canadian Nurses Association. 2000. Telehealth: great potential or risky terrain? Nursing Now: Issues and Trends in Canadian Nursing 9. URL: http://www.cna-nurses.ca/pages/issuestrends/nrgnow/telehealth_great%20potential.htm
Canadian Nurses Protective Society. 1997. Telephone advice. infoLAW 6(1): 1–2.
Carey M. The role of a statewide information and referral (I&R) system in enhancing the access of children and their families to developmental programs and services. Journal of Developmental and Behavioral Pediatrics 27(1 Suppl): S13–6; discussion S17–21.

Parent Information Project 46
Carmona RH. 2006. Health literacy: a national priority. Journal of General Internal Medicine 21(8): 803.
Carroll D, Rankin S. 2006. Comparing interventions in older unpartnered adults after myocardial infarction. European Journal of Cardiovascular Nursing 5(1): 83–89.
Castillo Riquelme MC, Lord J, et al. 2004. Cost-effectiveness of digital photographic screening for retinopathy of prematurity in the United Kingdom (structured abstract). International Journal of Technology Assessment in Health Care 20(2): 201–13.
CCCH. 2004. Parenting Information Project. Centre for Community Child Health, Royal Children’s Hospital Melbourne. Available in five volumes from Australian Government Department of Family and Community Services website. URL: http://www.facs.gov.au/pip
Centennial College. 2003. Certificate program in nursing telepractice. Scarborough, ON. URL: http://www.centennialcollege.ca/telehealth
Chamberlain LB, Merewood A, et al. 2005. Calls to an inner-city hospital breastfeeding telephone support line. Journal of Human Lactation 21(1): 53–8.
Chambers A, Hennessy E, et al. 2006. Longitudinal trends in quality of life after starting home parenteral nutrition: a randomised controlled study of telemedicine. Clinical Nutrition (Edinburgh, Scotland) 25(3): 505–14.
Chan S, Lam TH. 2006. Protecting sick children from exposure to passive smoking through mothers’ actions: a randomized controlled trial of a nursing intervention. Journal of Advanced Nursing 54(4): 440–9.
Chapman DJ, Damio G, et al. 2004. Effectiveness of breastfeeding peer counselling in a low-income, predominantly Latina population: a randomised controlled trial. Archives of Pediatrics and Adolescent Medicine 158(9): 897–902.
Charnock D, Shepperd S. 1999. DISCERN on the internet. URL: http://www.discern.org.uk
Chen LE, et al. 2000. Pediatric surgery on the internet: is the truth out there? Journal of Pediatric Surgery 35(8): 1179–82.
Chiang MF, Jiang L, et al. 2007. Interexpert agreement of plus disease diagnosis in retinopathy of prematurity. Archives of Ophthalmology 125(7): 875–80.
Chiang MF, Keenan JD, et al. 2005. Assessment of image-based technology: impact of referral cutoff on accuracy and reliability of remote retinopathy of prematurity diagnosis. AMIA: Annual Symposium Proceedings 126–30.
Chiang MF, Starren J, et al. 2006. Remote image based retinopathy of prematurity diagnosis: a receiver operating characteristic analysis of accuracy. British Journal of Ophthalmology 90(10): 1292–6.
Chiang MF, Wang L, et al. 2007. Telemedical retinopathy of prematurity diagnosis: accuracy, reliability, and image quality. Archives of Ophthalmology 125(11): 1531–8.
Chiari G, Vanelli M. 2005. Telephone and hot lines: a tool delivering clinical care. Acta Bio-Medica de l Ateneo Parmense 76(Suppl 3): 75–80.
Chisholm MA, Fair J, Spivey CA. 2007. Health literacy and transplant patients and practitioners. Public Health 121(10): 800–803.
Christakis DA, Zimmerman FJ, Rivara FP, et al. 2006. Improving pediatric prevention via the internet: a randomised, controlled trial. Pediatrics 118: 1157–66.

Parent Information Project 47
Cicutto L, Ashby M. 2007. The importance of a community-based asthma helpline. Journal of Asthma 44(9): 705–10.
Coleman A. 1997. Where do I stand? Legal implications of telephone triage. Journal of Clinical Nursing 6(3): 227–31.
College of Nurses of Ontario. 2000. A standard for telephone practice. Nursing and You 2(4). URL: http://www.cno.org/publications/ny/ny_vol2no4.html#4
Commission on the Future of Health Care in Canada, Romanow RJ. 2002. Building on Values: The future of health care in Canada – final report. Saskatoon: Commission on the Future of Health Care in Canada. URL: http://www.hc-sc.gc.ca/english/pdf/care/romanow_e.pdf
Cooper D, Arnold E, et al. 2005. The effect of deprivation, age and sex on NHS Direct call rates. British Journal of General Practice 55(513): 287–91.
Cooper DL, Smith GE, et al. 2007. The contribution of respiratory pathogens to the seasonality of NHS Direct calls. Journal of Infection 55(3): 240–8.
Cooper L, Hill M, Powe N. 2002. Designing and evaluating interventions to eliminate racial and ethnic disparities in health care. Journal of General Internal Medicine 17(6): 477–86.
Corpron CA, et al. 2001. Evaluation of pediatric surgery information on the internet. Journal of Pediatric Surgery 36(8): 1187–9.
Cragg DK, McKinley RK, Roland MO, et al. 1997. Comparison of out of hours care provided by patients’ own general practitioners and commercial deputising services: a randomised controlled trial. I: The process of care. British Medical Journal 314(7075):187–9. URL: http://bmj.bmjjournals.com/cgi/content/full/314/7075/187?
Customer Information Systems Inc for the Capital Health Authority. 2001. Capital Health Link: Consumer evaluation report. Final report. Edmonton: The Health Authority.
Dale J, Caramlau I, Docherty A, et al. 2007. Telecare motivational interviewing for diabetes patient education and support: a randomised controlled trial based in primary care comparing nurse and peer supporter delivery. Trials 28(8): 18.
Dale J, Caramlau IO, Lindenmayer A, et al. 2008. Peer support telephone calls for improving health (Review). The Cochrane Collaboration Issue 4.
D’Allesandro DM, Kreiter CD, et al. 2004. A randomised controlled trial of information prescription for pediatric patient education on the internet. Archives of Pediatrics and Adolescent Medicine 200(158): 857–62.
Dane AV, Schneider BH. 1998. Program integrity in primary and early secondary prevention: are implementation effects out of control? Clinical Psychology Review 18(1): 23–45.
Darnell JC, Hiner SL, Neill PJ, et al. 1985. After-hours telephone access to physicians with access to computerised medical records: experience in an inner-city general medicine clinic. Medical Care 23(1): 20–6.
Davidoff F, Florance V. 2000. The informationist: a new health professional? Annals of Internal Medicine 132.
Davis DA, Thompson MA, Oxman AD, et al. 1995. Changing physician performance: a systematic review of the effect of continuing education strategies. Journal of the American Medical Association 274: 700–705.
Davis KM, Heins JM, Fisher EB. 1997. Types of social support deemed important by participants in the DCCT. Diabetes 46: 352.

Parent Information Project 48
Davis TC, Mayeaux EJ, et al. 1994. Reading ability of parents compared with reading level of pediatric patient education materials. Pediatrics 93: 460–8.
Dawson A, Cohen D, et al. 1999. Domiciliary midwifery support in high-risk pregnancy incorporating telephonic fetal heart rate monitoring: a health technology randomised assessment (structured abstract). Journal of Telemedicine and Telecare 5(4): 220–30.
Dean BS, Decker MJ, et al. 2008. Condition HELP: a pediatric rapid response team triggered by patients and parents. Journal for Healthcare Quality 30(3): 28–31.
Delle Fave A, Massimini F. 2004. Parenthood and the quality of experience in daily life: a longitudinal study. Social Indicators Research 67(1–2): 75-106.
Dennis CL, Hodnett E, Gallop R, et al. 2002. The effect of peer support on breast-feeding duration among primiparous women: a randomised controlled trial. Canadian Medical Association Journal 166(1): 21–8.
Dennis CL. 2003 . The effect of peer support on post-partum depression: a pilot randomised controlled trial. Canadian Journal of Psychiatry 48(2): 115–24.
Dennis CL, Hodnett E. 2007. Psychosocial and psychological interventions for treating postpartum depression. URL http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD006116/frame.html
DePalma JA. 2008. Evidence needed to support home care in the future. Home Health Care Management and Practice 20(2): 186–8.
Department of Health (UK). 2000. Department of Health response to the independent review of GP out-of-hours services in England report “Raising standards for patients. New partnerships in out-of-hours care”. London: the Department. URL: htttp://www.doh.gov.uk/pdfs/oohgovresp.pdf
DeWalt DA, Berkman ND, Sheridan S, et al. 2004. Literacy and health outcomes: a systematic review of the literature. Journal of General Internal Medicine 19(12): 1228–39.
Dorchy H. 1994. Dorchy’s recipes – explaining the ‘intriguing efficacy of Belgian conventional therapy. Diabetes Care 17: 458–60.
Dornelas EA, Magnavita J, et al. 2006. Efficacy and cost-effectiveness of a clinic-based counseling intervention tested in an ethnically diverse sample of pregnant smokers. Patient Education and Counselling 64(1–3): 342–9.
Dowie R, Mistry H, et al. 2007. Telemedicine in pediatric and perinatal cardiology: economic evaluation of a service in English hospitals. International Journal of Technology Assessment in Health Care 23(1): 116–25.
Downer SR, Meara JG, et al. 2006. SMS text messaging improves outpatient attendance. Australian Health Review 30(3): 389–96.
Duan N, Fox SA, Pitkin Derose K, et al. 2000. Maintaining mammography adherence through telephone counselling in a church-based trial. American Journal of Public Health 90: 1468–71.
Dunnigan L. 2001. Info-Santé CLSC: an interface between the population and the health care system in Québec. Presented at the Canadian Telehealthcare Summit, 29 November 2001, Ottawa.
Dwyer S. 2008. From Early Pregnancy to Early Parenting: Antenatal education and transitions of maternal care in New Zealand. Wellington: Families Commission.
Edwards B. 1994. Telephone triage: how experienced nurses reach decisions. Journal of Advanced Nursing 19: 717–24.

Parent Information Project 49
Edwards B. 1998. Seeing is believing – picture building: a key component of telephone triage. Journal of Clinical Nursing 7: 51–7.
Eggleston PA, Butz A, et al. 2005. Home environmental intervention in inner-city asthma: a randomised controlled clinical trial. Annals of Allergy, Asthma and Immunology: Official publication of the American College of Allergy, Asthma and Immunology 95(6): 518–24.
Ells AL, PHOTOROP Study Group. 2005. Telemedicine screening for clinically significant retinopathy of prematurity: a multicenter clinical trial. Iovs 46ARVO E-abstract 3491.
Elwyn GJ, Kinnersley P, Rees J, et al. 1999. A nurse telephone triage system in an inner-city practice proved effective in assessing patients and reducing GP workloads. Nursing Times 95(23): 43.
Eysenbach G, Kohler C. 2002. How do consumers search for and appraise health information on the world wide web? Qualitative study using focus groups, usability tests, and in depth interviews. British Medical Journal 324: 573–7.
Eysenbach G, Powell J, Kuss O, et al. 2002. Empirical studies assessing the quality of health information for consumers on the world wide web. Journal of the American Medical Association 287(20): 2691–700.
Eysenbach G. 2007. Credibility of health information and digital media: new perspectives and implications for youth. In: M Metzger and A Flanagan (eds) Digital Media, Youth, and Credibility. Cambridge, MA: MIT Press.
Felix RJ, Jones KL, et al. 2004. Post marketing surveillance for drug safety in pregnancy: the Organization of Teratology Information Services project. Birth Defects Research 70(12): 944–7.
Ferguson R. 2005. Telephone help lines for parents. In: R Wootton and J Batch (eds) Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press.
Ferguson T. 2000. Online patient-helpers and physicians working together: a new partnership for high quality health care. British Medical Journal 321: 1129–32.
Ferris DG, Bishai DM, et al. 2004. Telemedicine network telecolposcopy compared with computer-based telecolposcopy (structured abstract). Journal of Lower Genital Tract Disease 8(2): 94–101.
Fisher-Jeffes L, Finlay F. 2006. Immunisation hotline calls as five-in-one vaccine introduced. Community Practitioner 79(4): 121–4.
Flesch R. 1948. A new readability yardstick. Journal of Applied Psychology 32: 221–33.
Fogler JA, Weber S, et al. 2007. Consultation needs in perinatal HIV care: experience of the National Perinatal HIV Consultation Service. American Journal of Obstetrics and Gynecology 197(3 Suppl): S137–41.
Fomous C, Miller N. 2006. The role of National Library of Medicine web sites in newborn screening education. Mental Retardation and Developmental Disabilities Research Reviews 12(4): 305–12.
Fortune T. 2001. Telephone triage: an Irish view. Accident and Emergency Nursing 9(3): 152–6.
Fosarelli P, Schmitt BD. 1987. Telephone dissatisfaction in pediatric practice: Denver and Baltimore. Pediatrics 80: 28–31.
Foster J, Jessopp L, Dale J. 1999. Concerns and confidence of general practitioners in providing telephone consultations. British Journal of General Practice 49(439): 111–13.

Parent Information Project 50
Fox-Gleissman D, Poole SR, Schmitt BD. 1995. Pediatric Telephone Triage and Advice Manual. Denver: Division of Pediatrics, The Children’s Hospital.
Frame PS. 1992. Health maintenance in clinical practice: strategies and barriers. American Family Physician 45: 1192–200.
Franco SM, Mitchell CK, Buzon RM. 1997. Primary care physician access and gatekeeping: a key to reducing emergency department use. Clinical Pediatrics 36(2): 63–8.
Franklin V, Waller A, Pagliari C, et al. 2003. “Sweet Talk”: text messaging support for intensive insulin therapy for young people with diabetes. Diabetes Technol Ther 5(6): 991–6.
Fraser HSF, Allen C, et al. 2007. Information systems for patient follow-up and chronic management of HIV and tuberculosis: a life-saving technology in resource-poor areas. Journal of Medical Internet Research 9(4): e29.
Friedman RH, Kaziz LE, Jette A. 1996. A telecommunications system for monitoring and counselling patients with hypertension: impact on medication adherence and high blood pressure control. American Journal of Hypertension 9: 285–92.
Gagliardi A, Jahad AR. 2002. Examination of instruments used to rate quality of health information on the internet: chronicle of a journey of a voyage with unclear destination. British Medical Journal 324: 569–73.
Gallagher TE. 2004. Augmentation of special-needs services and information to students and teachers ‘ASSIST’ – a telehealth innovation providing school-based medical interventions. Hawaii Medical Journal 63(10): 300–9.
Gay CL, Chapuis F, et al. 2006. Reinforced follow-up for children and adolescents with type 1 diabetes and inadequate glycaemic control: a randomised controlled trial intervention via the local pharmacist and telecare. Diabetes and Metabolism 32(2): 159–65.
Gazmararian J, Williams M, Peel J, et al. 2003. Health literacy and knowledge of chronic disease. Patient Education and Counselling 51(3): 267–75.
Gerber A, Lauterbach KW. 2005. Pediatric telephone triage and advice system. Justified only if saving costs? (Provisional record). Monatsschrift fϋr Kinderheilkunde 153(11): 1089–100.
Gibson S. 2002. Sweet talk – intensive diabetes support using SMS scheduling. Unpublished BSc (Hons) thesis. Division of Applied Computing, University of Dundee, Scotland.
Glasgow RE, Vogt TM, Boles SM. 1999. Evaluating the public health impact of health promotion interventions: the RE-AIM framework. American Journal of Public Health 89(9): 1322–7.
Glasper A. 1993. Telephone triage: a step forward for nursing practice? British Journal of Nursing 2(2): 108–9.
Goldman RA, Macpherson A. 2006. Internet health information use and e-mail access by parents attending paediatric emergency department. Emergency Medicine Journal 23: 345–48.
Goodenough B, Cohn RJ. 2004. Parent attitudes to audio/visual telecommunications in childhood cancer: an Australian study. Telemedicine Journal and e-Health 10(Suppl2): S-15–S-25.
Government of Saskatchewan. 2003. Healthline officially launched. Press release, 10 September, Regina. URL: http://www.gov.sk.ca/newsrel/releases/2003/09/10-641.html
Graham AL, Papandonatos GD. 2008. Reliability of internet- versus telephone-administered questionnaires in a diverse sample of smokers. Journal of Medical Internet Research 10(1): e8.
Parent Information Project 51
Graham ML, Ward B, et al. 2006. Rural parents, teenagers and alcohol: what are parents thinking? Rural and Remote Health 6(1): 383.
Grandinetti D. 1996. Patient telephone calls can drive pediatricians crazy. Medical Economics 15: 7–14.
Gray NJ, Klein PR, Powe N. 2005. Designing and evaluating interventions to eliminate racial and ethnic disparities in health care. Journal of Adolescent Health 37(3): 243.e1–e7.
Greenberg ME. 2000a. Telephone nursing: evidence of client and organizational benefits. Nursing Economics 18(3): 117–23.
Greenberg ME. 2000b. The domain of telenursing: issues and prospects. Nursing Economics 18(4): 220–2, 201.
Greenfield S, Kaplan S, Ware JE Jr. 1985. Expanding patient involvement in care. Annals of Internal Medicine 102: 520–8.
Greenfield S, Kaplan SH, Ware JE Jr, et al. 1988. Patients’ participation in medical care: effects on blood sugar control and quality of life in diabetes. Journal of General Internal Medicine 3: 448–57.
Gunning R. 1952. The Technique of Clear Writing. New York: McGraw-Hill International Book Co.
Gustafson DH, Hawkins R, Boberg E, et al. 1999. Impact of a patient-centred, computer-based health information/support system. American Journal of Preventive Medicine 16: 1–9.
GVU’s Tenth WWW User Survey Graphs. URL: http//www.cc.gatech.edu/gvu/user_surveys/survey-1998-10/graphs/use/Q110.htm.2003.
Hagan L, Morin D, Lépine R. 2000. Evaluation of telenursing outcomes: satisfaction, self-care practices, and cost savings. Public Health Nursing 17(4): 305–13.
Hage SJ. 1997. Triage: a refocused concept. Radiology Management 19(3):18–19.
Hainsworth J, Barlow J. 2001. Volunteers’ experiences of becoming arthritis self-management lay leaders: “It’s almost as if I’ve stopped aging and started to get younger!”. Arthritis Care and Research 45(4): 378-83.
Hall WA, Clauson M, et al. 2006. Effects on parents of an intervention to resolve infant behavioral sleep problems. Pediatric Nursing 32(3): 243–50.
Hallam L. 1994. Primary medical care outside normal working hours: review of published work. British Medical Journal 308(6923): 249–53. URL: http://bmj.bmjjournals.com/cgi/content/full/308/6923/249?
Hanauer D, Dibble E, Fortin J, et al. 2004. Internet use among community college students: implications in designing healthcare interventions. Journal of American College Health 52(5): 197–202.
Hanson RM, Exley BJ, et al. 2004. Paediatric telephone triage and advice: the demand continues. Medical Journal of Australia 180(7): 333–5.
Hansen-Turton. 2005. The nurse managed health center safety net: a policy solution to reducing health disparities. Nursing Clinics of North America 40: 729–38.
Hargrave DR, Hargrave UA, Bouffet E. 2006. Quality of health information on the internet in pediatric neuro-oncology. Neuro-oncology 8: 175–82.
Parent Information Project 52
Harper DC. 2006. Telemedicine for children with disabilities. Children’s Health Care 35(1): 11–27.
Harrison J. 2006. Pounds for Parents. Community Practitioner 79(7): 202.
Haviland L, Thornton AH, et al. 2004. Giving infants a great start: launching a national smoking cessation program for pregnant women. Nicotine and Tobacco Research 6 Suppl 2: S181–8.
Haycox A, Walley T. 1997. Pharmacoeconomics: evaluating the evaluators. British Journal of Clinical Pharmacology 43(5): 451–6.
Haynes RB, Ackloo E, et al. 2008. Interventions for enhancing medication adherence. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD000011/frame.html
Heller RF, Lim L, Valenti L, et al. 1995. A randomised controlled trial of community based counselling among those discharged from hospital with ischaemic heart disease. Australian and New Zealand Journal of Medicine 25(4): 362–4.
Hertz A, Gitterman B, Sherman H. 1998. Pediatric call centers and the practice of telephone triage and advice: critical success factors. American Academy of Pediatrics.
Hickson GB, Altemeier WA, O’Connor S. 1983. Concerns of mothers seeking care in private pediatric offices: opportunities for expanding services. Pediatrics 72: 619–24.
Hiller JE, Griffith E, et al. 2002. Education for contraceptive use by women after childbirth. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD001863/frame.html
Hirsh DA, Simon HK, et al. 2007. The host hospital 24-hour under referral rate: an automated measure of call-center safety. Pediatrics 119(6): 1139–44.
Hoare K, Lacoste J, Haro K, et al. 1999. Exploring indicators of telephone nursing quality. Journal of Nursing Care Quarterly 14(1): 38–46.
Hogenbirk JC, Pong RW, Chan BTB, et al. 2002. Evaluation of a Teletriage Pilot Project in Northern Ontario. Sudbury, ON: Centre for Rural and Northern Health Research.
Hohenhaus SM. 2005. An informal discussion of emergency nurses’ current clinical practice: what’s new and what works: danger with use of intravenous promethazine in the emergency department. Journal of Emergency Nursing 31(5): 465–7.
Homewood J. 2004. Consumer health information emails: content, metrics and issues. Aslib Proceedings: New Information Perspectives 56(3): 166–79.
Hopton J, Hogg R, McKee I. 1996. Patients account of calling the doctor out of hours: qualitative study in one general practice. British Medical Journal 313: 991–4.
Hornor G. 2005. Domestic violence and children. Journal of Pediatric Health Care 19(4): 206–12.
Howard D, Gazmararian J, Parker R. 2005. The impact of low health literacy on the medical costs of Medicare managed care enrolees. American Journal of Medicine 118(4): 371–7.
Humphreys J, Martin H, Roberts B, et al. 2004. Strengthening an academic nursing centre through partnership. Nursing Outlook 52: 197–202.
Ikemba CM, Kozinetz CA, Levitt M, et al. 2002. Internet use in families with children requiring cardiac surgery for congenital heart disease. Pediatrics 109: 419–22.
Iskander JK, Miller ER, et al. 2004. The role of the Vaccine Adverse Event Reporting System (VAERS) in monitoring vaccine safety. Pediatric Annals 33(9): 599–606.
Parent Information Project 53
Institute of Medicine. Crossing the quality chasm. URL: http://www.iom.edu/?id=5432?redirect=0
International Council of Nurses. 2001. International Standards for Telenursing Programmes. Geneva: The Council.
Jackson KM, Scott KE, et al. 2008. Cost-utility analysis of telemedicine and ophthalmoscopy for retinopathy of prematurity management. Archives of Ophthalmology 126(4): 493–9.
Jadad AR, Moore RA, Carroll D, et al. 1996. Assessing the quality of reports of randomised clinical trials: is blinding necessary? Controlled Clinical Trials 17(1): 1–12.
Jeffries P, Woolf S, Linde B. 2003. Technology-based vs traditional instruction. Nursing Education Perspectives 24(2): 70–74.
Johansen MA, Wootton R, et al. 2004. A feasibility study of email communication between the patient’s family and the specialist burns team. Journal of Telemedicine and Telecare 10(Suppl 1): 53–6.
Jones RA, Okely AD, et al. 2007. The HIKCUPS trial: a multi-site randomised controlled trial of a combined physical activity skill-development and dietary modification program in overweight and obese children. BMC Public Health 7: 15.
Jorm A, Christensen H, Griffiths K. 2005. The impact of beyondblue: the national depression initiative on the Australian public’s recognition of depression and beliefs about treatments. Australian and New Zealand Journal of Psychiatry 39(4): 248–54.
Kaimal AJ, Cheng YW, et al. 2008. Google obstetrics: who is educating our patients? American Journal of Obstetrics and Gynecology 198: 682e1–e5.
Kalichman SC, Benotsch E, et al. 2000. Health literacy and health related knowledge among persons living with HIV/AIDS. American Journal of Preventive Medicine 18(4): 325–31.
Kaplan SH, Greenfield S, Ware JE Jr. 1989. Assessing the effects of physician–patient interactions on the outcomes of chronic disease. Medical Care 27(suppl): S110–S127.
Kearney TE, Hiatt PH, et al. 2007. Alternative models for telephone response to pediatric poisonings. Prehospital Emergency Care 11(3): 284–92.
Keatinge D. 2006. Parents’ preferred child health information sources: implications for nursing practice. Australian Journal of Advanced Nursing 23(3): 13–18.
Keatinge D, Rawlings K. 2005. Outcomes of a nurse-led telephone triage service in Australia. International Journal of Nursing Practice 11(1): 5–12.
Keshavjee K, Lawson ML, Malloy M, et al. 2003. Technology failure analysis: understanding why a diabetes management tool developed for a personal digital assistant (pda) didn’t work in a randomised control trial. AMIA Annual Symposium Proceedings 889.
Kempe A, Dempsey C, Poole SR. 1999. Introduction of a recorded health information line into a pediatric practice. Archives of Pediatrics and Adolescent Medicine 153.
Keplar KE, Urbanski CJ, et al. 2005. Update on personal digital assistant applications for the healthcare provider. Annals of Pharmacotherapy 39(5): 892–907.
Khoo K, Bolt P, et al. 2008. Health information seeking by parents in the internet age. Journal of Paediatrics and Child Health 44(7–8): 419.
Kickbusch IS. 2001. Health literacy: addressing the health and education divide. Health Promotion International 16(3): 289–97.

Parent Information Project 54
Kincaid JP, Fishburne RP, Rogers RL, et al. 1975. Derivation of New Readability Formulas (Automated Readability Index, Fog Count and Flesch Reading Ease Formula) for Navy Enlisted Personnel. Research Branch Report 8-75, Millington, TN: Naval Technical Training, US Naval Air Station, Memphis, TN.
Kind T, Huang ZJ, et al. 2005. Internet and computer access and use for health information in an underserved community. Ambulatory Pediatrics 5(2): 117–21.
Kind T, Simon AE, et al. 2004. Can information prescription change parental attitudes and behaviours related to using the internet for health information resources? Archives of Pediatrics and Adolescent Medicine 200: 158. URL: http//archpedi.ama-assn.org
Kinsey K, Buchanan M. 2002. The nursing centre: a model of community health nursing practice. In: M Stanhope, J Lancaster (eds) Community and Public Health Nursing (5th edition). St Louis: Mosby.
Klasner AE, King WD, et al. 2006. Accuracy and response time when clerks are used for telephone triage. Clinical Pediatrics 45(3): 267–9.
Knowles MS, Holton EF, Swanson RA. 2005. The Adult Learner: The definitive classic in adult education and human resource development. Burlington, MA: Elsevier.
Kohler F, Schierbaum C, et al. 2005. Partnership for the heart: German-Estonian health project for the treatment of congenital heart defects in Estonia. Health Policy 73(2): 151–9.
Kopycka-Kedzierawski DT, Billings RJ. 2006. Teledentistry in inner-city child-care centres. Journal of Telemedicine and Telecare 12(4): 176–81.
Korsch BM. 1984. What do parents want to know? What do they need to know? Pediatrics 74(5): 917–19.
Krumm M, Huffman T, et al. 2008. Telemedicine for audiology screening of infants. Journal of Telemedicine and Telecare 14(2): 102–4.
Lai CH, Mallory SB. 2000. Internet use among parents of patients of a dermatology clinic. Pediatric Dermatology 17: 493–4.
Lajoie A, Koreen S, et al. 2008. Retinopathy of prematurity management using single-image vs multiple-image telemedicine examinations. American Journal of Ophthalmology 146(2): 298–309.
Lam F, Istwan NB, et al. 2003. Managing perinatal outcomes: the clinical benefit and cost-effectiveness of pharmacologic treatment of recurrent preterm labor (structured abstract). Managed Care 12(7): 39–46.
Lancaster T, Stead LF. 2005. Self-help interventions for smoking cessation. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD001118/frame.html
Lane JM, Addis ME. 2005. Male gender role conflict and patterns of help seeking in Costa Rica and the United States. Psychology of Men and Masculinity 6(3): 155–68.
Langer A, Farnot U, et al. 1996. The Latin American trial of psychosocial support during pregnancy: effects on mother’s wellbeing and satisfaction. Latin American Network For Perinatal and Reproductive Research (LANPER). Social Science and Medicine 42(11): 1589–97.
Larson-Dahn ML. 2001. Tel-eNurse Practice. Quality of care and patient outcomes. Journal of Nursing Administration 31(3): 145–52.
Last JM. 2001. A Dictionary of Epidemiology (4th ed). Oxford. UK: Oxford University Press.
Parent Information Project 55
Lattimer V, George S, Thompson F, et al. 1998. Safety and effectiveness of nurse telephone consultation in out of hours primary care: randomised controlled trial. British Medical Journal 317(7165): 1054–9. URL: http://bmj.bmjjournals.com/cgi/content/full/317/7165/1054
Lattimer V, Sassi F, George S, et al. 2000. Cost analysis of nurse telephone consultation in out of hours primary care: evidence from a randomised controlled trial. British Medical Journal 320(7241): 1053–7. URL: http://bmj.bmjjournals.com/cgi/reprint/320/7241/1053?
Laubscher B, Donatellio C. 2002. Use of a Swiss paediatric emergency department has grown. British Medical Journal 325: 389.
Lazarus W, Mora F. 2000. Online Content for Low-income and Underserved Americans: The Digital Divide’s new frontier, a strategic audit of activities and opportunities. Santa Monica, CA: The Children’s Partnership. URL: http://www.childrenspartnership.org/pub/low_income/index.html
LeBaron CW, Rodewald L, Humiston S. 1999. How much time is spent on well-child care and vaccinations? Archives of Pediatrics and Adolescent Medicine 153: 1154–9.
Leclerc B-S, Dunningan L, Cote H, et al. 2003. Caller’s ability to understand advice received from a telephone health line service: comparison of self-reported and registered data. Health Services Research 38: 2.
Lee AH. 2008. A pilot intervention for pregnant women in Sichuan, China on passive smoking. Patient Education and Counselling 71(3): 396–401.
Lee TJ, Guzy J, Johnson D, et al. 2002. Caller satisfaction with after-hours telephone advice: nurse advice service versus on-call pediatricians. Pediatrics 110(5): 865–72.
Leasure S. 1998. Telephone triage: a new way to provide health care in the outpatient setting. Surgical Services Management 4(12): 41–3.
Leese B, Young R. 1999. Disappearing GPs? Is there a crisis in recruitment and retention of general practitioners in England? Manchester, UK: National Primary Care Research and Development Centre, University of Manchester. URL: http://www.npcrdc.man.ac.uk
Leibowitz R, Day S, Dunt D. 2003. A systematic review of the effect of different models of after-hours primary medical care services on clinical outcome, medical workload, and patient and GP satisfaction. Family Practice 20(3): 311–7.
Leonard H, Slack-Smith L, et al. 2004. How can the internet help parents of children with rare neurologic disorders? Journal of Child Neurology 19(11): 902–7.
Lewin LS. 1995. Adapting your pediatric practice to changing health care system. Pediatrics 96: 799–804.
Lewis C, Packman A, et al. 2008. A phase II trial of telehealth delivery of the Lidcombe Program of Early Stuttering Intervention. American Journal of Speech-Language Pathology 17(2): 139–49.
Li J, Grigg M. 2007. Changes in characteristics of New Zealand Quitline callers between 2001 and 2005. New Zealand Medical Journal 120(1256): U2584.
Light PA, Hupcey JE, et al. 2005. Nursing telephone triage and its influence on parents’ choice of care for febrile children. Journal of Pediatric Nursing 20(6): 424–9.
Lindau ST, Tomori C, et al. 2002. The association of health literature with cervical cancer prevention knowledge and health behaviours in a multiethnic cohort of women. American Journal of Obstetrics and Gynecology 186(5): 938–43.

Parent Information Project 56
Loane MA, Bloomer SE, et al. 2001. A randomised controlled trial assessing the health economics of real-time teledermatology compared with conventional care: an urban versus rural perspective (structured abstract). Journal of Telemedicine and Telecare 7(2): 108–118.
Lord Darzi. 2008. High Quality Care For All: NHS Next Stage Review Final Report. Gateway reference: 10106. London: Department of Health.
Louis AA, Turner T, Gretton M, et al. 2003. A systematic review of telemonitoring for the management of heart failure. European Journal of Heart Failure 5: 583–90.
Mackert M, Love B, Whitten P. 2009. Patient education on mobile devices: and e-health intervention for low health literate audiences. Journal of Information Science 35(1): 82–93.
McClung HJ, Murray RD, Heitlinger LA. 1998. The internet as a source for current patient information. Pediatrics 101: e2.
McConnochie KM, Wood NE, et al. 2005. Telemedicine reduces absence resulting from illness in urban child care: evaluation of an innovation. Pediatrics 115(5): 1273–82.
McCrossan B, Morgan, et al. 2007. Assisting the transition from hospital to home for children with major congenital heart disease by telemedicine: a feasibility study and initial results. Medical Informatics and the Internet in Medicine 32(4): 297–304.
McCrossan BA, Grant B, et al. 2008. Diagnosis of congenital heart disease in neonates by videoconferencing: an eight-year experience. Journal of Telemedicine and Telecare 14(3): 137–40.
McDevitt J, Braun S, Noyes M, et al. 2005. Integrated primary and mental health care: evaluating a nurse-managed centre for clients with serious and persistent mental health. Nursing Clinics of North America 8: 779–90.
McDonald EM, Solomon BS, et al. 2006. Do urban parents’ interests in safety topics match their children’s injury risks? Health Promotion Practice 7(4): 388–95.
McKay HG, Feil EG, Glasgow RE, et al. 2003. Feasibility and use of an internet support service for diabetes self-management. Diabetes Education 24: 174–9.
McKinley RK, Cragg DK, Hastings AM, et al. 1997. Comparison of out of hours care provided by patients’ own general practitioners and commercial deputising services: a randomised controlled trial. II: The outcome of care. British Medical Journal 314(7075): 190–3. URL: http://bmj.bmjjournals.com/cgi/content/full/314/7075/190?
McKinley RK, Manku-Scott T, Hastings AM, et al. 1997. Reliability and validity of a new measure of patient satisfaction with out of hours primary medical care in the United Kingdom: development of a patient questionnaire. British Medical Journal 314(7075): 193–8. URL: http://bmj.bmjjournals.com/cgi/content/314/7075/193
McKinstrie F. 2006. Young minds. Community Practitioner 79(9): 271.
McKinstry B, Walker J, Campbell C, et al. 2002. Telephone consultations to manage requests for same-day appointments: a randomised controlled trial in two practices. British Journal of General Practice 52(477): 306–10.
McMullan M. 2006. Patients using the internet to obtain health information: how this affects patient-health professional relationship. Patient Education and Counseling 63: 24–8.
McMullen P. 1998. Telephone triage in women’s health care. Lippincott’s Primary Care Practice 2: 251–5.

Parent Information Project 57
Mahoney MR, Khamarko K, et al. 2008. Care of HIV-infected Latinos in the United States: a description of calls to the National HIV/AIDS Clinicians’ Consultation Centre. Journal of the Association of Nurses in AIDS Care 19(4): 302–10.
Manning DL, Dickens C. 2006. Health literacy: more choice, but do cancer patients have the skills to decode? European Journal of Cancer Care 15(5): 448–52.
Marcin JP, Ellis J, et al. 2004. Using telemedicine to provide pediatric subspecialty care to children with special health care needs in an underserved rural community. Pediatrics 113(1 Pt 1): 1–6.
Marcin JP, Nesbitt TS, et al. 2004. Use of telemedicine to provide pediatric critical care inpatient consultations to underserved rural Northern California. Journal of Pediatrics 144(3): 375–80.
Marcin JP, Schepps DE, et al. 2004. The use of telemedicine to provide pediatric critical care consultations to pediatric trauma patients admitted to a remote trauma intensive care unit: a preliminary report. Pediatric Critical Care Medicine 5(3): 251–6.
Marklund B, Silfverhielm B, Bengtsson C. 1989. Evaluation of an educational programme for telephone advisers in primary health care. Family Practice 6(4): 263–7.
Marrero DG. 2000. Computer assisted diabetes dietary self-management counseling. Medical Care 38: 1059–61.
Massin MM, Montesanti J, et al. 2006. Use of the internet by parents of children with congenital heart disease. Acta Cardiologica 61(4): 406–10.
Martens L. 2005. Electromagnetic safety of children using wireless phones: a literature review. Bioelectromagnetics Suppl 7: S133–7.
Mayo A, Chang BL, Omery A. 2002. Use of protocols and guidelines by telephone nurses. Clinical Nursing Research 11: 204.
Melzer SM, Poole SR. 1999. Computerised pediatric telephone triage and advice programs at children’s hospitals. Archives of Pediatrics and Adolescent Medicine 153: 858–63.
Milne RG, Horne M, et al. 2006. SMS reminders in the UK national health service: an evaluation of its impact on ‘no-shows’ at hospital out-patient clinics. Health Care Management Review 31(2): 130–6.
Mistiaen P, Poot E. 2006. Telephone follow-up, initiated by a hospital-based health professional, for postdischarge problems in patients discharged from hospital to home. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD004510/frame.html
Moen P, Dempster-McClain D, Williams RM Jr. 1989. Social integration and longevity: an event history analysis of women’s roles and resilience. American Sociological Review 54(4): 635–47.
Moher D, Jadad AR, Tugwell P. 1996. Assessing the quality of randomised controlled trials: current issues and future directions. International Journal of Technology Assessment in Health Care 12(2): 195–208.
Monaghan R, Clifford C, McDonald P. 2003. Seeking advice from NHS direct on common childhood complaints: does it matter who answers the phone? Journal of Advanced Nursing 42(2): 209–16.
Monteny M, Berger MY, et al. 2008. Triage of febrile children at a GP co-operative: determinants of a consultation. British Journal of General Practice 58(549): 242–7.

Parent Information Project 58
Moore ML, Krowchuk H. 1997. Parent Line: nurse telephone intervention for parents and caregivers of children from birth through age 5. Journal for Specialists in Pediatric Nursing 2(4): 179–84.
Morgan GJ, Grant B, et al. 2005. Supporting families of critically ill children at home using videoconferencing. Journal of Telemedicine and Telecare 11(Suppl 1): 91–2.
Mortensen HB, Villumsen J, Volund A, et al. 1992. Relationship between insulin injection regimen and metabolic control in young Danish type 1 diabetic patients. Diabetic Medicine 9: 834–9.
Mowbray CT, Moxley DP, Thrasher S, et al. 1996. Consumers as community support providers: issues created by role innovation. Community Mental Health Journal 32(1): 47–67.
Mullett J. 2000. Partnerships for Better Health: A self-care pilot project: Final evaluation report, May 2000. Victoria: Ministry of Health and Ministry Responsible for Seniors. URL: http://www.healthservices.gov.bc.ca/cpa/publications/evalfin.pdf
Murray E, Burns J, et al. 2005. Interactive health communication applications for people with chronic disease. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD004274/frame.html
Murray E, Lo B, Pollack L. 2003. The impact of health information on the internet on the physician patient relationship: patient perceptions. Archives of Internal Medicine 163: 1727–34.
Nair K, Goodenough B, et al. 2006. Telephone support groups for isolated bereaved parents: a review of the literature and an example from Australian paediatric oncology. Illness, Crisis, and Loss 14(4): 319–36.
National Institute for Health and Clinical Excellence. 2008. Improving the Nutrition of Pregnant and Breastfeeding Mothers and Children in Low-income Households. NICE: London.
National Prescribing Centre. 2000. An introduction to health economics (part 2): applying health economics. MeReC Briefing (no. 14). URL: http://www.npc.co.uk/MeReC_Briefings/2000/briefing_no_14.pdf
National Initiative for Telehealth Guidelines. 2002. Ottawa: The Initiative. URL: http://www.nifte.ca
Nelson E-L. 2004. Cognitive behavioural therapy for childhood depression: a comparison of face-to-face and interactive televideo settings. PhD thesis, University of Kansas, USA.
Nelson, E-L, Barnard M, et al. 2006. Feasibility of telemedicine intervention for childhood depression. Counselling and Psychotherapy Research 6(3): 191–5.
NHS Executive Information for Health. URL: http://www.dh.gov.uk/PolicyAndGuidance/InformationPolicy/InformationForhealth/fs/en
Nielsen-Bohlman L, Panzer A, Kindig D (eds). 2004. Health Literacy: A prescription to end confusion. Washington DC: National Academy of Sciences.
Niemann S, Meer A, et al. 2004. Medical telephone triage and patient behaviour: how do they compare? Swiss Medical Weekly 134(9–10): 126–31.
Nilsen ES, Myrhaug HT, et al. 2006. Methods of consumer involvement in developing healthcare policy and research, clinical practice guidelines and patient information material. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD004563/frame.html
Norris SL, Saadine J, et al. 2005. Interventions to promote screening for diabetic retinopathy. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD005104/frame.html

Parent Information Project 59
Nunn E, King B, et al. 2006. A randomised controlled trial of telephone calls to young patients with poorly controlled type 1 diabetes. Pediatric Diabetes 7(5): 254–9.
Nurse telephone-triage. 2001. Lancet 357(9253): 323.
Nwagwu WE. 2007. The internet as a source of reproductive health information among adolescent girls in an urban city in Nigeria. BMC Public Health 7: 354.
Oberleitner R, Elison-Bowers P, et al. 2007. Optimising the personal health record with special video capture for the treatment of autism. Journal of Developmental and Physical Disabilities 19(5): 513–18.
O’Connell JM, Johnson DA, Stallmeyer J, et al. 2001. A satisfaction and return-on-investment study of a nurse triage service. American Journal of Managed Care 7(2): 159–69.
O’Hanley P. 1997. Triage through technology: New Brunswick Tele-Care service reduces ER visits. Hospital Quarterly 1(2): 46–7.
O’Keefe M, Kirwan C. 2008. Screening for retinopathy of prematurity. Early Human Development 84(2): 89–94.
Omoto AM, Snyder M, Martino SC. 2000. Volunteerism and the life course: investigating age-related agendas for action. Basic and Applied Social Psychology 22(3): 181–97.
Ortolon K. 2004. The baby blues. Texas Medicine 100(1): 33–6.
Oxman AD, Thomson MA, Davis DA, et al. 1995. No magic bullets: a systematic review of 102 trials of interventions to improve professional practice. CMAJ: Canadian Medical Association Journal 153: 1423–31.
Ozuah PO, Reznik, M. 2004. The role of telemedicine in the care of children in under-served communities. Journal of Telemedicine & Telecare 10(Suppl 1): 78–80.
Pagliari C, Gregor P, Sloan D. 2005. Literature review and conceptual map of the area of e-health. London NHS Service Delivery and Organisation Programme. URL: www.sdo.Ishtm.ac.uk/ehealth.htm#pagliari
Pappano D, Humiston S, et al. 2004. Efficacy of a pediatric emergency department-based influenza vaccination program. Archives of Pediatrics and Adolescent Medicine 158(11): 1077–83.
Parker DR, Windsor RA, et al. 2007. Feasibility, cost, and cost-effectiveness of a telephone-based motivational intervention for underserved pregnant smokers. Nicotine and Tobacco Research: Official Journal of the Society for Research on Nicotine and Tobacco 9(10): 1043–51.
Pattinson RC, Say L, et al. 2005. Critical incident audit and feedback to improve perinatal and maternal mortality and morbidity. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD002961/frame.html
Pemberton PJ, Goldblatt J. 1998. The internet and the changing roles of doctors, patients and families. Medical Journal of Australia 169: 594–5.
Pert JC, Furth TW, Katz HP. 1996. A 10-year experience in pediatric after hours telecommunications. Current Opinion in Pediatrics 8: 181–7.
Petousis-Harris H, Goodyear-Smith F, et al. 2005. The New Zealand national immunisation hotline – what are callers seeking? Vaccine 23(42): 5038–44.

Parent Information Project 60
Pettinari CJ, Jessopp L. ‘Your ears become your eyes’: managing the absence of visibility in NHS Direct. Journal of Advanced Nursing 36(5): 668–75.
Philip C. 2003. Nurses on call. Nursing BC October.
Piazza-Waggoner C, Ferguson KS, et al. 2006. Case study: providing evidence-based behavioral and nutrition treatment to a toddler with cystic fibrosis and multiple food allergies via telehealth. Pediatric Pulmonology 41(10): 1001–4.
Picot J, Cradduck T. 2000. The Telehealth Industry in Canada: Industry profile and capability analysis. Edmonton: The Keston Group and InfoTELMED Communications. URL: http://strategis.ic.gc.ca/epic/internet/inen-ts.nsf/vwapj/0100016e.pdf/$FILE/0100016e.pdf
Pinnock H, Slack R, Pagliari C, et al. 2006. Professional and patient attitudes to using mobile phone technology to monitor asthma: questionnaire survey. Primary Care Respiratory Journal 15: 237–45.
Pless IB, Hagel B, et al. 2007. Preventing product-related injuries: a randomised controlled trial of poster alerts. Canadian Journal of Public Health: Revue canadienne de santé publique 98(4): 271–5.
Polaschek L, Polaschek N. 2007. Solution-focused conversations: a new therapeutic strategy in well child health nursing telephone consultations. Journal of Advanced Nursing 59(2): 111–9.
Pong RW, Hogenbirk JC. 2000. Reimbursing physicians for telehealth practice: issues and policy options. Health Law Review 9(1): 3–12. URL: http://www.laurentian.ca/cranhr/pdf/telehlth/th_reimb.pdf
Poole SR. 1999. Pediatric care. In: M Green et al (eds) Ambulatory Pediatrics (5th edition). Philadelphia: WB Saunders Co.
Poole SR, Schmitt BD. 1993. After hours telephone coverage: the application of an area-wide telephone triage and advice system for pediatric practices. Pediatrics 92: 670–9.
Price Waterhouse Coopers, Ontario Ministère de la santé et des soins de longue durée. 2001. Evaluation of Primary Care Reform Pilots in Ontario: Phase I, final report. [Ontario]: Price Waterhouse Coopers.
Ralston ME. 2005. This issue: managing emergencies part 2. Pediatric Annals 34(12): 921–3.
Rasmussen LM, Phanareth K, Nolte H, et al. 2005. Internet-based monitoring of asthma: a long-term randomised clinical study of 300 asthmatics. Journal of Allergy Clinical Immunology 115: 1137–42.
Regalado M, Halfon N. 2001. Primary care services promoting optimal child development from birth to age three years. Archives of Pediatrics and Adolescent Medicine 155: 1311–22.
Reisinger KS, Bires JA. 1980. Anticipatory guidance in pediatric practice. Pediatrics 66: 889–92.
Reznik M, Ozuah PO. 2005. Educational videoconferences for parents in the Bronx. In: R Wootton and J Batch (eds) Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press Ltd.
Richards DA, Godfrey L, et al. 2004. NHS Direct versus general practice based triage for same day appointments in primary care: cluster randomised controlled trial. British Medical Journal 329(7469): 774.
Richards DA, Meakins J, Tawfik J, et al. 2002. Nurse telephone triage for same day appointments in general practice: multiple interrupted time series trial of effect on workload and
Parent Information Project 61
costs. British Medical Journal 325(7374): 1214–9. URL: http://bmj.com/cgi/reprint/325/7374/1214.pdf
Ring F, Jones M. 2004. NHS Direct usage in a GP population of children under five years: is NHS Direct used by people with the greatest health need? British Journal of General Practice 54(500): 211–3.
Risk A, Dzenowagis J. 2002. Review of internet health information quality initiatives (WHO 2001). Journal of Medical Internet Research 3(4): e28. URL: http://www.jmir.org/2001/4/e28/#ref16
Roberto AJ, Zimmerman RS, et al. 2007. A computer-based approach to preventing pregnancy, STD, and HIV in rural adolescents. Journal of Health Communication 12(1): 53–76.
Robinson C. 1998. Telecare/Télésoins: evaluation of New Brunswick’s 1-800 dial-a-nurse service (region 1 pilot). Fredericton: Program Analysis and Evaluation Unit, Department of Health and Community Services.
Roland M. 2002. Nurse-led telephone advice: a useful additional service? Editorial. Medical Journal of Australia 176(3): 96. URL: http://www.mja.com.au/public/issues/176_03_040202/rol10686_fm.html
Romanow RJ, Commission on the Future of Health Care in Canada. 2002. Building on Values: The future of health care in Canada – final report. Saskatoon: Commission on the Future of Health Care in Canada. URL: http://www.hc-sc.gc.ca/english/pdf/care/romanow_e.pdf
Rosenstock IM. 1985. Understanding and enhancing patient compliance with diabetic regimens. Diabetes Care 8: 610–16.
Ross VM, Smith CE. 2008. Longitudinal trends in quality of life after starting home parenteral nutrition: a randomised controlled study of telemedicine. Comment. Clinical Nutrition 27(2): 314; author reply 315–6.
Rush JP, Kitch TL. 1991. A randomised, controlled trial to measure the frequency of use of a hospital telephone line for new parents. Birth (Berkeley, CA) 18(4): 193–7.
Ryan D, Cobern W, Wheeler J, et al. 2005. Mobile phone technology in the management of asthma. Journal of Telemedicine and Telecare 11: 43–6.
Ryan R, Prictor M, et al. 2008. Audio-visual presentation of information for informed consent for participation in clinical trials. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD003717/frame.html
Sanghavi DM. 1999. Taking well-child care into the 21st century. Archives of Pediatrics and Adolescent Medicine 153: 482–5.
Sanner T. 2004. Using telehealth to address the nursing shortage. Home Healthcare Nurse 22(10): 695–9.
Saqui O, Chang A, et al. 2007. Telehealth videoconferencing: improving home parenteral nutrition patient care to rural areas of Ontario, Canada. JPEN: Journal of Parenteral and Enteral Nutrition 31(3): 234–9.
Satherley P, Lawes E, Sok S. 2008. The Adult Literacy and Life Skills (ALL) Survey: Overview and International Comparisons. Ministry of Education: Wellington.
Scalvini S, Glisenti F. 2005. Centenary of tele-electrocardiography and telephonocardiography – where are we today? Journal of Telemedicine and Telecare 11(7): 325–30.

Parent Information Project 62
Schmied V, Homer C, Kemp L, et al. 2008. ‘Best for everyone’: a study of the role and nature of universal health services for pregnant women, children and families in Australia. On behalf of the Collaboration for Research into Universal Health Services for Mothers and Children. [email protected]
Schmitt BD. 1998. Pediatric Telephone Protocols. Denver: Decision Press.
Schmitt BD. 2004. Pediatric Telephone Protocols (office version 10th edition). Elkgrove Village: American Academy of Pediatrics.
Schor EL. 2004. Rethinking well-child care. Pediatrics 114: 210–16.
Schulz KF, Chalmers I, Hayes RJ, et al. 1995. Empirical evidence of bias: dimensions of methodological quality associated with estimates of treatment effects in controlled trials. Journal of the American Medical Association 273(5): 408–12.
Schuster MA, Duan N, Regalado M. 2000. Anticipatory guidance. What information do parents receive? What information do they want? Archives of Pediatrics and Adolescent Medicine 154: 1191–8.
Schwartz CE, Sprangers MJ. 1999b. Methodological approaches for assessing response shift in longitudinal health-related quality-of-life research. Social Science and Medicine 48(11): 1531–48.
Scott KE, Kimn DY, et al. 2008. Telemedical diagnosis of retinopathy of prematurity intraphysician agreement between ophthalmoscopic examination and image-based interpretation. Ophthalmology 115(7): 1222–8.e3.
Semere W, et al. 2003. A pediatric surgery study: parent usage of the internet for medical information. Journal of Pediatric Surgery 38(4): 560–4.
Shalitin S, Phillip M. 2007. The role of new technologies in treating children and adolescents with type 1 diabetes mellitus. Pediatric Diabetes 8(Suppl 6): 72–9.
Shaw E, Levitt C, Wong S, et al. 2006. Systematic review of the literature on postpartum care: effectiveness of postpartum support to improve maternal parenting, mental health, quality of life and physical health. Birth 33(3): 210–20.
Shearer BS, Seymour A, Capitani C. 2002. Bringing the best of medical librarianship to the patient team. Journal of Medical Library Association 90: 22–31.
Shekelle P, Roland M. 1999. Nurse-led telephone-advice lines. Lancet 354(9173): 88–9.
Shiffman R, Freudigman K, Brandt C, et al. 2000. A guideline implementation system using handheld computers for office management of asthma: effects on adherence and patient outcomes. Pediatrics 105(4): 767–73.
Sicotte C, Lehoux P, et al. 2004. A cost-effectiveness analysis of interactive paediatric telecardiology (structured abstract). Journal of Telemedicine and Telecare 10(2): 78–83.
Sim NZ, Kitteringham L, Spitz L, et al. 2007. Information on the World Wide Web – how useful is it for parents? Journal of Paediatric Surgery 42(2): 305–12.
Skalet AH, Quinn GE, et al. 2008. Telemedicine screening for retinopathy of prematurity in developing countries using digital retinal images: a feasibility project. Journal of Aapos: American Association for Pediatric Ophthalmology and Strabismus 12(3): 252–8.
Smith AC, Bensink M, et al. 2005. Telemedicine and rural health care applications. Journal of Postgraduate Medicine 51(4): 286–93.

Parent Information Project 63
Smith PC, Brice JH, Lee J. 2007. The relationship between functional health literacy and adherence to emergency department discharge instructions among Spanish speaking patients. Annals of Emergency Medicine 50(3,S1): S55–6.
Solomon LJ, Flynn BS. 2005. Telephone support for pregnant smokers who want to stop smoking. Health Promotion Practice 6(1): 105–108.
Sorum PC, Mallick R. 1997. Physicians’ opinions on compensation for telephone calls. Pediatrics 99: e3.
South M. 2005. Paediatric websites for healthcare professionals. In: R Wootton and J Batch (eds) Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press Ltd.
Spangaro JM. 2007. The NSW health routine screening for domestic violence program. New South Wales Public Health Bulletin 18(5–6): 86–9.
St George I, Cullen M, Gardiner L, et al. 2008. Universal telenursing triage in Australia and New Zealand: a new primary health service. Australian Family Physician 37(6): 476–9.
Stacey D. 2002. Nurse telephone consultation for people facing health-related decisions. Systematic review. Ottawa: Systematic Reviews and Meta-analysis Course, Graduate School of Epidemiology, University of Ottawa.
Stacey D, Noorani HZ, Fisher A, et al. 2004. A clinical and economic review of telephone triage services and survey of Canadian call centre programs. Ottawa: Canadian Coordinating Office for Health Technology Assessment. Technology Overview no. 13.
Stacey D, Noorani HZ, Fisher A, et al. 2003. Telephone triage services: systematic review and a survey of Canadian call centre programs. Ottawa: Canadian Co-ordinating Office for Health Technology Assessment. Technology report no. 43.
Stange KC, Fedirko T, Zyzanski SJ, et al. 1994. How do family physicians prioritise delivery of multiple preventive services? Journal of Family Practice 38: 231–7.
Stange KC, Zyzanski SJ, Jaen CR. 1998. Illuminating the “black box”: a description of 4454 patient visits to 138 family physicians. Journal of Family Practice 46: 377–89.
Stead LF, Perera R, et al. 2006. Telephone counselling for smoking cessation. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD002850/frame.html
Stewart B, Fairhurst R, et al. 2006. Review of calls to NHS Direct related to attendance in the paediatric emergency department. Emergency Medicine Journal 23(12): 911–14.
Stewart S. 2006. Delivering the Goods: Midwives’ use of the internet. Mahwah, NJ: Lawrence Erlbaum Associates Publishers.
Strecher VJ, Greenwood T, Wang C, et al. 1999. Interactive multimedia and risk communication. Journal of the National Cancer Institute Monographs 25: 134–9.
Sulzbacher S, Vallin T, et al. 2006. Telepsychiatry improves paediatric behavioural health care in rural communities. Journal of Telemedicine and Telecare 12(6): 285–8.
Suplee PD. 2007. Women’s Health Case Studies. Philadelphia: Lippincott Williams & Wilkins Publishers.
Sutton D, Stanley P, et al. 2008. Preventing or accelerating emergency care for children with complex healthcare needs. Archives of Disease in Childhood 93(1): 17–22.

Parent Information Project 64
Tachkara S, Wang XH, Istepanian RSH, et al. 2003. Mobile e-health: the unwired evolution of telemedicine. Telemedicine Journal and e-health 9: 247–57.
Tan K, Lai NM. 2007. Telemedicine for the support of parents of high risk newborn infants. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD006818/frame.html
Taylor BA, Hughes CE, et al. 2004. Teaching teenagers with autism to seek assistance when lost. Journal of Applied Behaviour Analysis 37(1): 79–82.
Telehealth Task Force (ON). 1999. Recommendations for a telephone health education and triage/advisory service: final report to the Ontario Ministry of Health and Long-Term Care. Toronto: Ontario Ministry of Health and Long-Term Care. URL: http://www.health.gov.on.ca/english/public/pub/ministry_reports/telehealth/telehealth.html
Telephone health information systems are popular. 20 March 1991. Hospitals 65: 14.
Thompson F, George S, Lattimer V, et al. 1999. Overnight calls in primary care: randomised controlled trial of management using nurse telephone consultation. British Medical Journal 319(7222): 1408.
Tingen MS, Waller JL, et al. 2006. Tobacco prevention in children and cessation in family members. Journal of the American Academy of Nurse Practitioners 18(4): 169–79.
Tough SC, Johnston DW, et al. 2006. Does supplementary prenatal nursing and home visitation support improve resource use in a universal health care system? A randomised controlled trial in Canada. Birth (Berkeley, California) 33(3): 183–94.
Tsai SH, Kraus J, et al. 2007. The effectiveness of video-telemedicine for screening of patients requesting emergency air medical transport (EAMT) (provisional record). Journal of Trauma 62(2): 504–11.
Tuffrey C, Finlay F. 2002. Use of the internet by parents of paediatrics outpatients. Archives of Disease in Childhood 87: 534–6.
UK Broadband Overview. January 2008. URL: http://point-topic.com/content/operatorSource/profiles2/uk-broadband-overview.htm
Urquhart C, Currell R, et al. 2006. Home uterine monitoring for detecting preterm labour. URL: http://www.mrw.interscience.wiley.com/cochrane/clsysrev/articles/CD006172/frame.html
Van Dijk A, McGuinness D, et al. 2008. Can Telehealth Ontario respiratory call volume be used as a proxy for emergency department respiratory visit surveillance by public health? CJEM: Canadian Journal of Emergency Medical Care 10(1): 18–24.
VanDinter M. 2000. Telephone triage: the rules are changing. American Journal of Maternal/Child Nursing 25(4): 187–91.
Vanelli M, Corchia M, et al. 2006. Outside-hospital assistance for children and adolescents with type 1 diabetes mellitus. Acta Bio-Medica de l Ateneo Parmense 77(3): 163–7.
Wahlberg AC, Wredling R. 1999. Telephone nursing: calls and caller satisfaction. International Journal of Nursing Practice 5: 164–70.
Wahlberg AC, Wredling R. 2001. Telephone advice nursing: callers’ experiences. Journal of Telemedicine and Telecare 7: 272–6.
Wahlberg AC, Cedersund E, Wredling R. 2003. Telephone nurses’ experience of problems with telephone advice in Sweden. Journal of Clinical Nursing 12: 37–45.

Parent Information Project 65
Wainstein BK, Sterling-Levis K, et al. 2006. Use of the internet by parents of paediatric patients. Journal of Paediatrics and Child Health 42(9): 528–32.
Wang S-F, Chen C-H, et al. 2008. Related factors in using a free breastfeeding hotline service in Taiwan. Journal of Clinical Nursing 17(7): 949–56.
Watcher DA, Brillman JC, Lewis J, et al. 1999. Pediatric telephone triage protocols: standardised decision making or a false sense of security? Annals of Emergency Medicine 33: 388–94.
Watson WA, Litovitz TL, et al. 2005. 2004 Annual Report of the American Association of Poison Control Centers Toxic Exposure Surveillance System. American Journal of Emergency Medicine 23(5): 589–666.
Weatherburn G, Dowie R, et al. 2006. An assessment of parental satisfaction with mode of delivery of specialist advice for paediatric cardiology: face-to-face versus videoconference. Journal of Telemedicine and Telecare 12(Suppl 1): 57–9.
Weinstein RS, Lopez AM, et al. 2008. Integrating telemedicine and telehealth: putting it all together. Studies in Health Technology and Informatics 131: 23–38.
Weiss B, Palmer R. 2004. Relationship between health care costs and very low literacy skills in a medically needy and indigent Medicaid population. Journal of the American Board of Family Practice 17(1): 44–7.
Wells GA, Shea B, O’Connell D, et al. 1999. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Ottawa: Clinical Epidemiology Unit, University of Ottawa. URL: http://www.lri.ca/programs/ceu/oxford.htm
Whitten PS, Mair FS, Haycox A, et al. 2002. Systematic review of cost effectiveness studies of telemedicine interventions. British Medical Journal 324(7351): 1434–7. URL: http://bmj.bmjjournals.com/cgi/content/full/324/7351/1434
Wiggins M, Oakley A, et al. 2004. The Social Support and Family Health Study: a randomised controlled trial and economic evaluation of two alternative forms of postnatal support for mothers living in disadvantaged inner-city areas. Health Technology Assessment 8(32): iii, ix–x, 1–120.
Wilkin H, Ball-Rokeach S. 2006. Reaching at risk groups: the importance of health storytelling in Los Angeles Latino media. Journalism 7(3): 299–320.
Williams M, Baker D, Parker R, et al. 1998. Relationship of functional health literacy to patients’ knowledge of their chronic disease. Archives of Internal Medicine 158(2): 166–72.
Williams MD, Gish KW, Giuse NB, et al. 2001. The Patient Informatics Consult Service (PICS): an approach for a patient-centred service. Bulletin of the Medical Library Association 89: 185–93.
Williams S, Crouch R, Dale J. 1995. Providing health-care advice by telephone. Professional Nurse 10(12): 750–2.
Wilson L, Onslow M, et al. 2004. Telehealth adaptation of the Lidcombe Program of Early Stuttering Intervention: five case studies. American Journal of Speech-Language Pathology 13(1): 81-93.
Wilson P. 2002. How to find the good and avoid the bad or ugly: a short guide to tools rating quality of health information on the internet. British Medical Journal 324: 598–600.
Winickoff JP, Tanski SE, et al. 2006. A national survey of the acceptability of quitlines to help parents quit smoking. Pediatrics 117(4): e695–700.

Parent Information Project 66
Winston FK, Erkoboni D, et al. 2007. Identifying interventions that promote belt-positioning booster seat use for parents with low educational attainment. Journal of Trauma – Injury, Infection and Critical Care 63(3 Suppl): S29–38.
Wischmann T. 2008. Implications of psychosocial support in infertility: a critical appraisal. Journal of Psychosomatic Obstetrics and Gynecology 29(2): 83–90.
Wise M, Gustafson DH, et al. 2007. Internet telehealth for pediatric asthma case management: integrating computerised and case manager features for tailoring a web-based asthma education program. Health Promotion Practice 8(3): 282–91.
Woodson KE, Sable CA, et al. 2004. Forward and store telemedicine using Motion Pictures Expert Group: a novel approach to pediatric tele-echocardiography. Journal of the American Society of Echocardiography 17(11): 1197–200.
Woolcott B, Johnson DA, Phillips JS, et al. 1995. Telephone triage safely lessens demand for acute care pediatric services. Managed Care Medicine 2: 22–5.
Wootton R, Batch J (eds). 2005. Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press Ltd.
Yanovski SZ, Yanovski JA, Malley JD, et al. 1992. Telephone triage by primary care physicians. Pediatrics 89: 701–6.
Ybarra ML, Emenyonu N, et al. 2008. Health information seeking among Mbararan adolescents: results from the Uganda Media and You survey. Health Education Research 23(2): 249–58.
Yin HS, Forbis SG, Dreyer BP. 2007. Health literacy and pediatric health. Current Problems in Pediatric and Adolescent Care 37(7): 258–86.
Yogesan K, Kumar S, et al. 2005. Paediatric tele-ophthalmology. In: R Wootton and J Batch (eds) Telepediatrics: Telemedicine and Child Health. London: Royal Society of Medicine Press.
Young KT, Davis K, Schoen C, et al. 1998. Listening to parents: a national survey of parents with young children. Archives of Pediatrics and Adolescent Medicine 152: 255–62.
Young TL, Ireson C. 2003. Effectiveness of school-based telehealth care in urban and rural elementary schools (brief record). Pediatrics 112(5): 1088–94.
Zeman LD. 2005. Hotline tip to probable cause: filling the gap between suspicion and physical abuse findings for mandated reporters. Care Management Journals 6(2): 66–72.

Parent Information Project 67
Appendix 1: Questionnaire Used in Telephone Survey of Parents
S1 How many children do you have [they may not necessarily live with you]? [DO NOT READ] 1 One 2 Two 3 Three 4 Four 5 Five 6 Six or more 7 None/refused [CONCLUDE INTERVIEW]
S2 How old are your children? [DO NOT READ CATEGORIES UNLESS NECESSARY] [ASK FOR AGES FROM YOUNGEST TO OLDEST CHILD]
a Child 1
b Child 2
c Child 3
d Child 4
e Child 5
f Child 6
Newborn to 3 months 1 1 1 1 1 1
4 to 6 months 2 2 2 2 2 2
7 to 9 months 3 3 3 3 3 3
10 to 12 months 4 4 4 4 4 4
13 to 18 months 5 5 5 5 5 5
19 to 23 months 6 6 6 6 6 6
2 years old 7 7 7 7 7 7
3 years old 8 8 8 8 8 8
4 years old 9 9 9 9 9 9
5 years old 10 10 10 10 10 10
6-10 years old 11 11 11 11 11 11
11 to 15 years old 12 12 12 12 12 12
16 to 18 years old 13 13 13 13 13 13
19 years old or older 14 14 14 14 14 14
[If No] Is there anyone in the house with a child under five years old? [If No again: terminate survey] [If Yes: Can I speak with them please – reintroduce] [If Yes] Can I check that you are the parent or guardian that gathers most of the information and advice on your pre-school child’s development? If not ask to speak to that person and re-introduce.
Parent Information Project 68
The research is about what health information parents of pre-school children require. The survey is part of a research project designed to find ways to improve advice and information for parents such as yourself. [IF NECESSARY – IF ASKED HOW TELEPHONE NUMBER WAS OBTAINED: Your telephone number was selected at random from the telephone directory (or from the Māori Electoral Roll).] Is now a convenient time to talk to you? [IF NECESSARY: the survey takes around 20 minutes but this does depend on your answers.] [ARRANGE CALLBACK IF NECESSARY.] [IF NECESSARY: The information you provide will help the Ministry of Health to design appropriate information and advice services for parents of pre-schoolers.] [IF NECESSARY: Your responses will be treated as confidential and no information you provide will be used to identify you.] ** Just to let you know, during the course of this interview my supervisor may listen in to check the quality of my interviewing.**
D5 Which of the following ethnic group or groups do you belong to? Read and code all mentions New Zealand Māori ................................. 1 New Zealand European........................... 2 Other European....................................... 3 Pacific Island ........................................... 4 Chinese ................................................... 5 Indian including Sri Lankan ..................... 6 Other Asian ............................................. 7 Other ....................................................... 8 ***DON’T READ*** Refused.................... 9
D6 [RECORD GENDER – DO NOT ASK] 1 Male 2 Female
A Information sought These next questions are about information, or advice you may have looked for or received about your under five year old’s development. This could include anything you’ve discussed with other people, friends, family, other parents, or medical and health professionals. This also includes information you’ve looked for or received through reading material, on the internet, through the media and so on.

Parent Information Project 69
Q1 I’m going to read out a list of topics relating to the development of under five-year-olds. Only thinking about the last six months, please tell me if you have tried to get or been given any information on each of these. In the last six months have you tried to get or been given information or advice for your under five-year-old on:
(i) What physical development to expect at different ages including for example, toilet training and bed wetting, differences between boys and girls and so on
[IF YES PROBE: Have you tried to get information or advice, been given it, or both?]
[IF STILL NO: Use code 4] 1. Tried to get information 2. Been given information 3. Both (tried to get and been given information) 4. Neither 5. Don’t know [Don’t read out]
Repeat for list of topics, randomise/rotate order of list.
Physical development (ii) Common illnesses and how to deal with them [if necessary: rashes, fevers,
colic, allergies and so on] (iii) Injury prevention and safety [if necessary: fire safety, car seats, preventing
scalds and burns etc] (iv) When to take a child to the doctor, or hospital (v) Breast feeding and/or bottle feeding (vi) Diet and nutrition and what or how much to feed children, or fussy eaters (vii) Sleeping patterns and difficulties (viii) Development milestones such as crawling, walking etc
Emotional and social development (ix) Managing or dealing with behaviour [if necessary: temper tantrums, crying,
anxiety, arguments, fighting], parenting and disciplining (x) What behaviour to expect at different ages (xi) How to promote self-confidence, self-esteem and social skills [if necessary:
playing with others, being nervous or clingy in new situations and making new friends]
(xii) How to manage situations which can affect a child emotionally [if necessary: divorce or separation, grief and loss]

Parent Information Project 70
(xiii) What social interactions to expect at different ages [if necessary: normal relationships with other children of similar age]
(xiv) Separation anxiety/leaving children with others
Intellectual development (xv) How to promote intellectual development and/or learning, including preparing
children for school (xvi) Teaching children to talk [if necessary: how to help speech development] (xvii) Teaching children to read, write or count (xviii) What intellectual development to expect at different ages [if necessary:
speech, ability to count, recognise colours, use a pencil and so on]
Q2 Is there anything that I haven’t mentioned that you have looked for information, or advice on for your under five-year-old in the last six months – or that you feel you need information or advice on, at the moment? Code “other specify” responses (up to five additional)
B Sources used and usefulness of each
Q3 Please can you tell me what sources of information or advice you have used to get information on your child under five in the last six months?
Unprompted – Use Codeframe from Question 4 Prompt: In the last six months which of the following have you used to get information for your child under five?
If necessary: Who did you ask/what did you do or where did you go to find information or advice on your under five year old?
Read out options that have not been selected from Question 4 codeframe Interviewer, please probe to “no more” For each source used at Q3 ask:
Q4 And on a scale very useful, useful, neutral, not useful and not at all useful. How useful or not useful did you find [source] for information on your under five-year-old?
Repeat for next source used [ask for each source only once]:
Very useful
Not at all useful
a Previous experience with your older children 1 2 3 4 5
b Your parents/in-laws, or relatives 1 2 3 4 5
e Friends/other parents 1 2 3 4 5
f Your family doctor (general practitioner/GP) 1 2 3 4 5

Parent Information Project 71
g Your child’s paediatrician 1 2 3 4 5
h Baby or maternal health clinics 1 2 3 4 5
i Nurses or midwives 1 2 3 4 5
j Other health professionals [please specify]
......................................................................
1 2 3 4 5
k Telephone health lines Healthline 1 2 3 4 5 Well Child Advice Line 1 2 3 4 5 Plunket 1 2 3 4 5 Other [please specify] ......................................................................
1 2 3 4 5
l Parent support groups/playgroups 1 2 3 4 5
m Books 1 2 3 4 5
n Magazines 1 2 3 4 5
o Brochures/fact sheets/tip sheets 1 2 3 4 5
p Internet [please specify the (up to three) most useful websites that you can recall]
......................................................................
1 2 3 4 5
q Childcare providers 1 2 3 4 5
r Television programmes 1 2 3 4 5
s Radio programmes 1 2 3 4 5
t Newspaper articles 1 2 3 4 5
u Other [please specify]
......................................................................
1 2 3 4 5
C Preferences for providers/sources
Q5. Which of the following do you have easy access to? a Mobile telephone b Internet
• Internet at home with dial-up access • Internet at home with Broadband access • Internet at a place other than in your home
c TV d DVD player e Video player
We now want to talk about how information on your under five-year0old could be provided to you in the future.
Q6 On a scale of very useful, useful, neutral, not useful and not at all useful, how useful to you would each of the following be as sources of information or advice? Explain scale:

Parent Information Project 72
Very useful
Useful Neutral Not useful
Not at all useful
a Telephone health line
b Telephone healthline provided by Well Child – Tamariki Ora service
c Internet health sites
d Internet sites provided by Well Child – Tamariki Ora service
e DVDs or videos provided by Well Child – Tamariki Ora service
f Brochures generally
g Brochures provided by Well Child – Tamariki Ora service
h DVDs or videos generally
i Internet sites provided by other health professionals (eg, kidshealth)
Q7 And what sources of information on children under five’s development would you prefer to use? IF NECESSARY: Who would you ask/where would you go/what would you do to find information on your under five year olds?
Probe: What others would you prefer to use? [Probe to “nothing else”]
a Previous experience with your older children 1
b Your parents/your partner’s parents 2
c Your partner/spouse 3
d Relatives apart from your partner, your parents or your partner’s parents 4
e Friends 5
f Your family doctor (general practitioner/GP) 6
g Your child’s paediatrician 7
h Baby or maternal health clinics 8
i Nurses or midwives 9
j Other health professionals [please specify] ...................................................................................................................................
10
k Telephone health lines 11 Healthline 12 Well Child Advice Line 13 Plunket 14 Other [please specify] .............................................................................................. 15

Parent Information Project 73
l Parent support groups/playgroups 16
m Books 17
n Magazines 18
o Brochures/fact sheets/tip sheets 19
p Internet websites 20
q Childcare providers 21
r Television programmes 22
s Radio programmes 23
t Newspaper articles 24
u Other [please specify] ............................................................................................... 25
D Plunket/Well Child Tamariki ora If not mentioned Plunket or other Well Child Tamariki Ora provider at Q3, 6, or 7
Q9 Have you had a Well Child Tamariki Ora nurse such as Plunket for your under five-year-old? 1. Plunket 2. Other (specify) 3. None 4. Don’t Know [Interviewer note: this is at any time for their under five year old.]
Ask all those who mentioned, or have a Plunket or other Well Child Tamariki Ora provider:
Q10 Which of the following ways have you received information from [provider] for your under five-year-old: [Interviewer note: this is at any time for their under five-year-old.]
1. [provider] nurse, or staff visiting your home 2. [provider] nurse or staff at Plunket rooms 3. [provider] telephone service 4. [provider] website 5. Brochures or leaflets provided by [provider] 6. Other (please specify)
E Demographics Finally, we need some information about you to help us make sure we’ve surveyed a good mix of people and help with our analysis.

Parent Information Project 74
E1 Which of the following is your age group? [READ OUT] 1. under 20 2. 20–24 3. 25–29 4. 30–34 5. 35–39 6. 40–50 7. over 50 8. Refused
E2 Which of the following is the highest level of formal education you have completed? [IF UNABLE TO ANSWER, OBTAIN AGE PERSON LEFT SCHOOL]
1. Primary school 2. Year 10 or below (Form 4) 3. Year 11 or equivalent (Form 5) 4. Year 12 or equivalent (Form 6) 5. Year 13 or equivalent (Form 7) 6. School Certificate 7. University Entrance 8. Sixth Form Certificate 9. Trade/apprenticeship qualification 10. Other TAFE/Technical certificate, diploma or associate diploma 11. Undergraduate certificate or diploma 12. Degree/postgraduate certificate or diploma/Masters Degree/Doctorate 13. Other school qualifications (eg, overseas qualifications) 14. Other (please specify) 15. Don’t know/can’t say [don’t read out] 16. Age person left school 17. Refused
E3 Is your total annual household income from all sources before tax? [READ] 1. Less than $20,000 2. $20,000–$29,999 3. $30,000–$39,999 4. $40,000–$49,999 5. $50,000–$99,999 6. $100,000 or more 7. Refused

Parent Information Project 75
E4 Which one language do you mainly use at home when speaking to your family and friends? [DON’T READ OUT] [multiple response] 1. English 2. Māori 3. Samoan 4. Tongan 5. Cook Island Māori 6. Niuean 7. Cantonese 8. Mandarin 9. Korean 10. Dutch 11. German 12. Hindi 13. Japanese 14. Vietnamese 15. Afrikaans 16. Punjabi 17. Urdu 18. Farsi 19. Other (specify) 20. [Don’t read] Don’t know/refused
E5 As I mentioned, this survey is about the information needs of parents and guardians of children younger than five. Where a parent or their child has special needs such as a learning or physical disability, it is possible that their information needs may be different or perhaps greater. To help us understand this, can I ask: • Does your (youngest) child under five have any special needs such as a
learning or physical disability? • Do you personally have any special needs such as a learning or physical
disability? 1. Yes 2. No 3. Possibly/still diagnosing/not confirmed
E6 And which of the following best describes your living situation? [Read out single response] 1. One parent family 2. Two parent family 3. Extended family arrangement 4. Two parents in household 5. One parent in household

Parent Information Project 76
6. [Don’t read] Other (specify) 7. [Don’t read] Don’t know 8. [Don’t read] refused
Finally, are there any other comments you’d like to make about information, or advice on the development of your under five-year-old?
Conclusion Thank you very much for your time. In case you missed it, my name is [operator name] from Gravitas Research. If you have any queries about this survey, you can contact Monica Ludolph on our tollfree number 0508 RESEARCH (7373 2724). Have a good morning/afternoon/evening.
Termination Thank you for your help. That’s all the questions I need to ask you today as we are looking for parents with children aged under five years. In case you missed it, my name is [operator name] from Gravitas Research and if you have any questions you can call use tollfree on 0508 7373 2724. IF NECESSARY: We have ended the survey at this point as Ministry of Health have instructed us to speak to parents having children aged under five years. Since you don’t meet the requirements, we are unable to continue with the survey. REFER RESPONDENT TO THE SUPERVISOR IF NECESSARY. [INTERVIEWER PLEASE HANG UP]
Parent Information Project 77
Appendix 2: Results of Telephone Survey of Parents
Parent Information Summary Report – 1 July 2009 This summary report is based on data collected in a telephone survey of parents with children aged under five years.
Methodology The sample size for the survey was n=800, collected nationwide. Surveying was conducted between 9 April and 22 May 2009. The average interview length was 20 minutes. A quota sample was employed to ensure sufficient data was collected for key
groups of interest. The data was then also post weighted to provide a dataset representative of the target population using Census data profiles purchased from Statistics New Zealand for households with at least one child aged under five years.
The quotas collected were:
Ethnicity Māori 217 Pacific Island 128 NZ European 407 Other 48
Urban/Rural Profile Areas Main Urban/Satellite Urban 455 Independent Urban 231 Rural 114
The following sub-samples were also collected by parent type: Single Parents 71 Disadvantaged /Lower Income 93 Disables/Special needs 57 Young parents 50
Sample for the general population was drawn randomly form the Telecom White Pages.
The Māori Electoral Roll was used to sample Māori households to achieve the Māori quota. Additional Pacific Island households were sampled from suburbs with high proportions of Pacific Island residents in Auckland and in Wellington, based on analysis of Census data at Census Area Unit (CAU) level.
Parent Information Project 78
Data has been weighted by ethnicity, location at a regional level and by Statistics New Zealand’s urban/rural profile type, and by educational achievement to produce information that is representative of the target population structure.
Around 1 in 10 households contacted randomly were eligible – that is they contained a parent/guardian of a child aged under 5 years.
The response rate achieved was 30.2 per cent. The data has been provided both as a full dataset and in a set of cross tabulations,
as well as being summarised in this report. Gravitas was commissioned by the Ministry of Health to undertake the telephone
survey of parents. The questionnaire used in the survey was developed by Gravitas in consultation
with the Ministry of Health.
Key Findings Parents cite a range of sources of information on children aged under five years;
with Doctor, telephone health lines - Plunket, friends, childcare staff, books and the
internet most commonly mentioned un-prompted. Over half (52 percent) of respondents nominate internet websites as their preferred
source of information on their child under five’s development. Eighty-eight percent of respondents use Plunket as their Well Child Tamariki Ora
provider. Ten percent of respondents state they speak a language other than English when
they are at home.
Comparisons Sources of information - Unprompted
- Significantly more Māori respondents use Relatives apart from your partner, your parents or your partners parents (34 percent compared to 17 percent of the total sample), television programmes (10 percent compared to 5 percent of the total sample) and their partner/spouse (8 percent compared to 4 percent of the total sample) as a source of advice on their under 5 year old.
- Seven percent of Pacific respondents use newspaper articles as a source of information (compared to 2 percent of the total sample).
- Eighty-four percent of respondents from Other ethnicities mentioned unprompted telephone health lines – Plunket (compared to 45 percent of the total sample ) and nurses or midwives (33 percent – compared to 16 percent of the total sample) as information sources for their under five year old.
- Significantly more respondents located in Independent Urban areas use other parents as an information source (37 percent – compared to 16 percent of the total sample) and nurses or midwives (38 percent – compared to 16 percent of the total sample) as sources of information for their child under five.

Parent Information Project 79
Sources of Information – Prompted - When prompted, Māori respondents say they have used telephone health line -
Plunket (33 percent compared to 21 percent of the total sample), their parents (48 percent – compared to 37 percent of the total sample) and previous experience with their older children (64 percent – compared to 54 percent of the total sample) as an information source for their under five year old.
- Pacific respondents are more likely to have used telephone health lines - Plunket (44 percent – compared to 21 percent of the total sample), childcare providers (47 percent – compared to 33 percent of the total sample), their parents (52 percent – compared to 37 percent of the total sample), relatives apart from your partner, your parents or your partners parents (47 percent – compared to 33 percent of the total sample) and television programmes (48 percent – compared to 33 percent of the total sample) as information sources for their under five year old child..
Usefulness of Sources of Information - Māori respondents rate telephone health line provided by Well Child – Tamariki
Ora service as useful (79 percent – compared to 71 percent of the total sample) and DVDs or videos generally (67 percent – compared to 58 percent of the total sample) as useful sources of information on their under five year old child.
- Respondents from Other ethnicities are less likely to rate internet health sites (73 percent – compared to 83 percent of the total sample), internet sites provided by Well Child – Tamariki Ora service (49 percent – compared to 77 percent of the total sample) as useful and brochures generally (48 percent – compared to 65 percent of the total sample) as useful sources of information for their pre-school child.
- However, Other ethnicities are more likely to rate DVDs or videos generally (79 percent – compared to 58 percent of the total sample) as useful sources of information.
Preferred Source of Information - More Pacific respondents rate family doctor/GP (54 percent – compared to 38
percent of the total sample) as their preferred source for information on their under five year old child and are less likely to prefer Internet websites (37 percent – compared to 52 percent of the total sample).
- Other ethnicities are more likely to rate internet websites (64 percent – compared to 52 percent of the total sample), friends (35 percent – compared to 25 percent total sample), magazines (25 percent – compared to 13 percent of the total sample), your parents, in-laws or relatives (18 percent – compared to 3 percent of the total sample) and other health professionals (14 percent - compared to 6 percent of the total sample) as their preferred choice for information on their under five year old child.
- Other ethnicities are less likely to prefer family doctor/GP (11 percent – compared to 38 percent of the total sample) and telephone health lines – Healthline (4 percent – compared to 20 percent of the total sample).
- Rural respondents are more likely to show preference for family doctor/GP (59 percent – compared to 38 percent of the total sample), their parents (30 percent

Parent Information Project 80
– compared to 20 percent of the total sample) and other parents (20 percent – compared to 9 percent of the total sample) as a source of information on their under five year old child.
Pacific respondents are less likely to have access to a mobile telephone (71 percent – compared to 93 percent of the total sample), television (92 percent – compared to 98 percent of the total sample), DVD player (79 percent – compared to 96 percent of the total sample, and are less likely to have internet at home with broadband access (44 percent – compared to 73 percent of the total sample).

Parent Information Project 81
Parent Information Survey Results – 1 July 2009 Q1. Tried to get or been given information on the following topics in the last six months (%):
Table 1: Information Sought in the Last Six Months (%)

Parent Information Project 82

Parent Information Project 83
Figure 1: Total of Tried to Get and Tried to Get and Been Given Information on Topics
(%)

Parent Information Project 84
Q2. Is there anything that I haven’t mentioned that you have looked for information, or advice on for your under 5 year old in the last 6 months – or that you feel you need information or advice on at the moment?
Table 2: Other Sources of Information Used (%)

Parent Information Project 85
Q3. Can you tell me what sources of information or advice you have used to get information on your child under 5 in the last six months and how useful that source was?
Figure 2: Ranked List of Sources Used by Respondents (%)
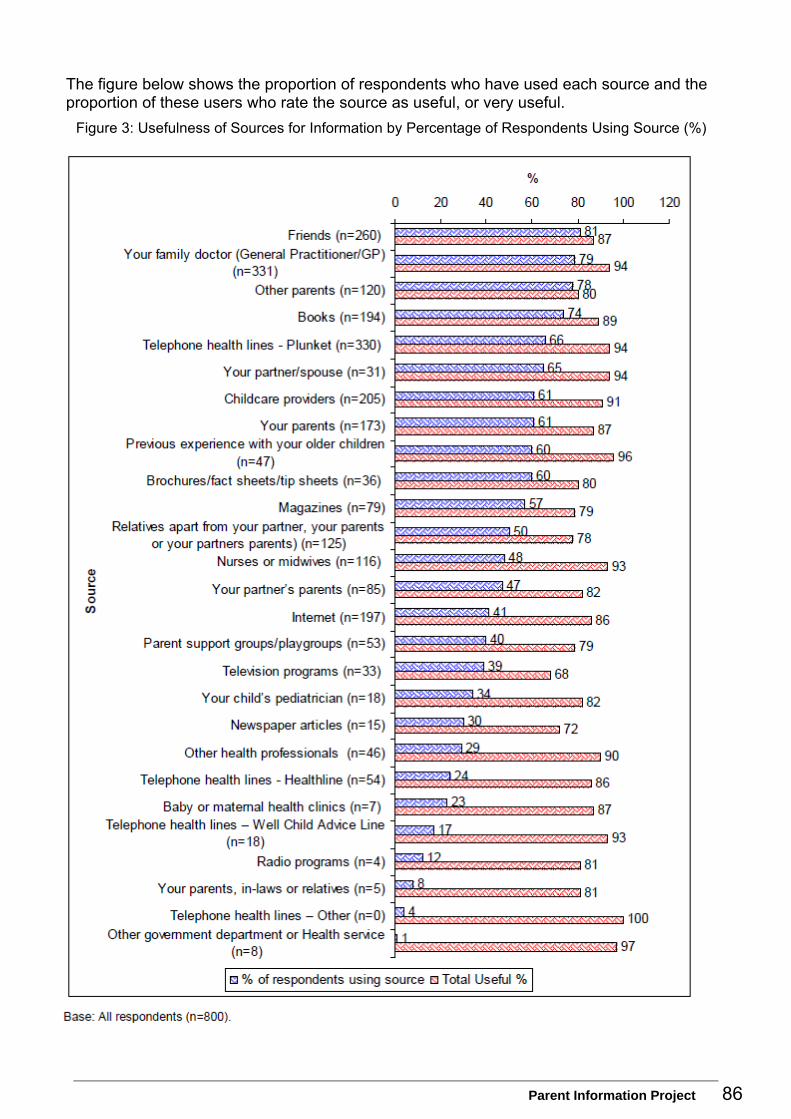
Parent Information Project 86
The figure below shows the proportion of respondents who have used each source and the proportion of these users who rate the source as useful, or very useful.
Figure 3: Usefulness of Sources for Information by Percentage of Respondents Using Source (%)
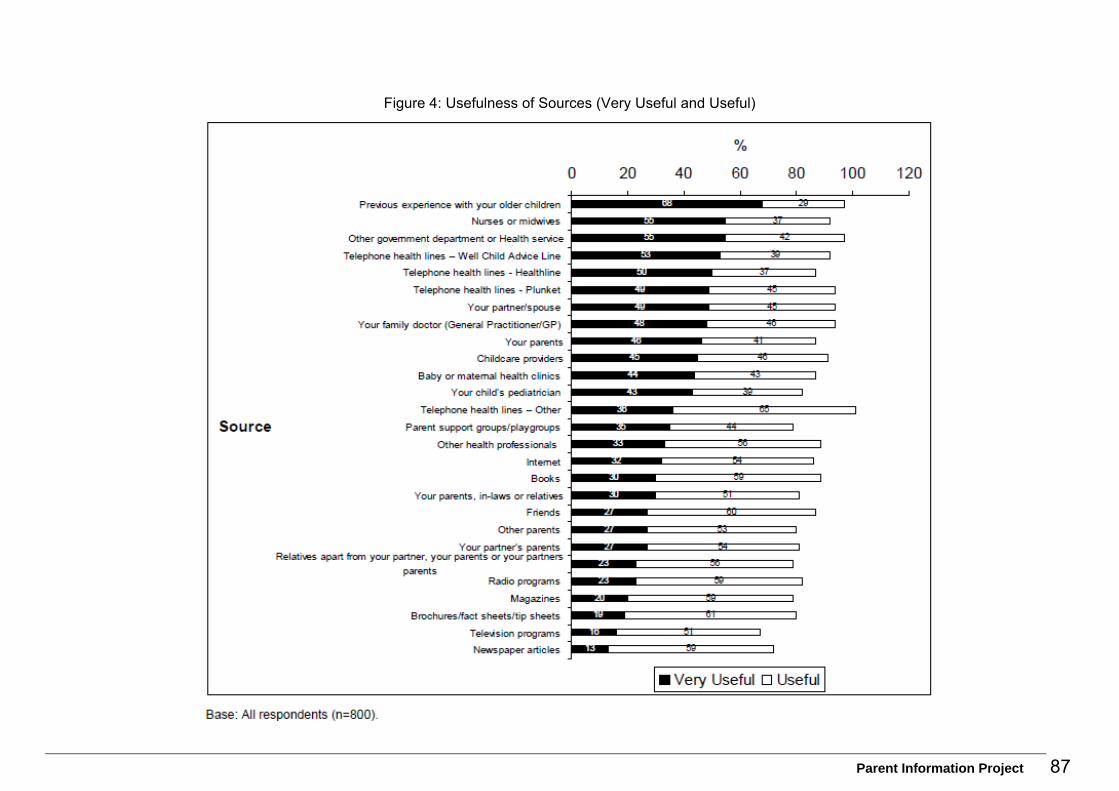
Parent Information Project 87
Figure 4: Usefulness of Sources (Very Useful and Useful)

Parent Information Project 88
Table 3: Prompted and Unprompted mention of Sources and Usefulness of Source by Ethnicity (%)

Parent Information Project 89

Parent Information Project 90

Parent Information Project 91

Parent Information Project 92
Table 4: Prompted and Unprompted mention of Sources and Usefulness of Source by Location (%)

Parent Information Project 93
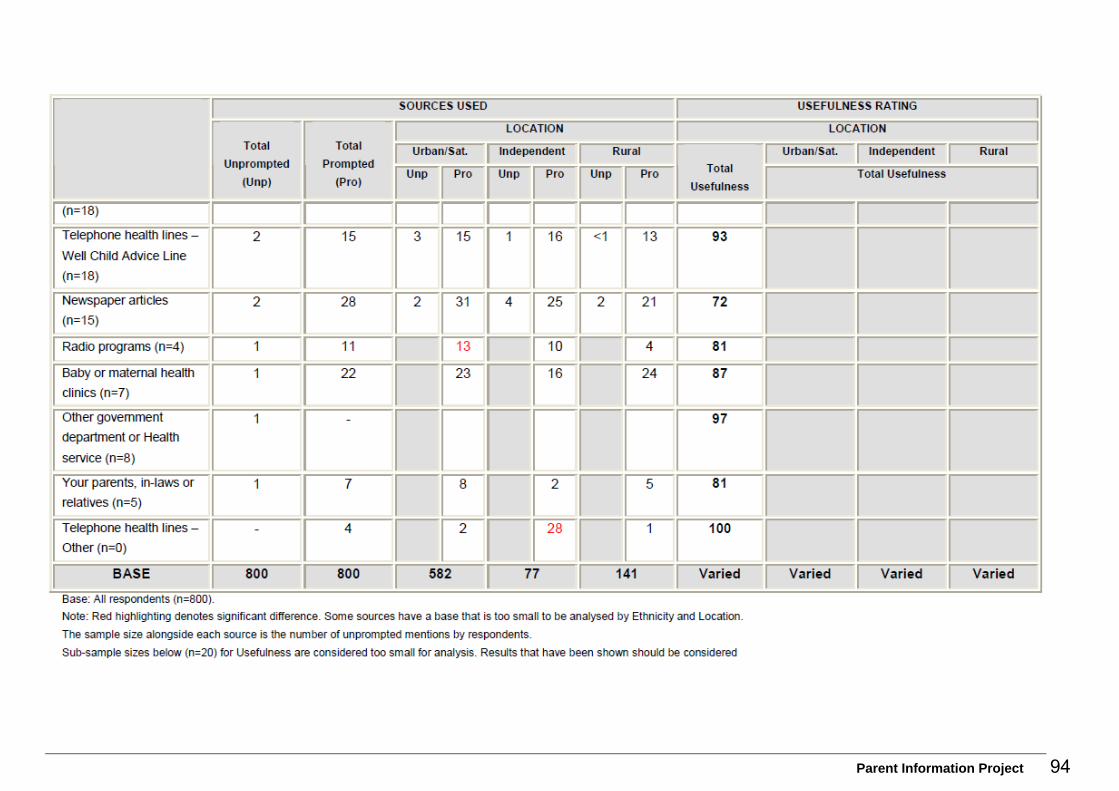
Parent Information Project 94

Parent Information Project 95
Other Sources mentioned by respondents:
Table 5: Other Sources Mentioned (%)

Parent Information Project 96
Q5: Which of the following do you have access to?
Table 6: Access to Technology (%)

Parent Information Project 97
Q6: On a scale very useful, useful, neutral, not useful and not at all useful, how useful to you would each of the following be as sources of information or advice?
Figure 5: Usefulness of Potential Sources of Information (%)

Parent Information Project 98
Table 7: Usefulness of Potential Sources (%)

Parent Information Project 99
Q7. And what sources of information on children under five’s development would you prefer to use?
Figure 6: Preferences for Sources of Information (%)

Parent Information Project 100
Table 8: Preferences for Sources of Information(%)

Parent Information Project 101

Parent Information Project 102
Q9. Have you had a Well Child Tamariki Ora nurse such as Plunket for your under 5 year old?
1. Plunket 2. Other (specify) 3. None 4. Don’t Know
Table 9: Well Child – Tamariki Ora Provider (%)
Q10: Which of the following ways have you received information from [provider] for your under 5 year old:
Table 10: Information Received from Well Child – Tamariki Ora Provider (%)

Parent Information Project 103
S1: How many children do you have [they may not necessarily live with you]? Table 11: Number of Children (%)
S2: How old are your children? Table 12: Age of Children (%)

Parent Information Project 104
D2: Gender of respondent. Figure 6: Gender of Respondent (%)
D5. Which of the following ethnic group or groups do you belong to?
Figure 7: Ethnic Group of Respondent (%)

Parent Information Project 105
D3. Which of the following is your age group? Figure 8; Age of Respondent (%)
D6. Which one language do you mainly use at home when speaking to your family and friends?
Table 13: Main Language Spoken at Home (%)

Parent Information Project 106
D3. What is your total annual household income from all sources before tax? Figure 9: Total Household Income (%)

Parent Information Project 107
D2: Which of the following is the highest level of formal education you have completed?
Figure 10: Highest Education Level Achieved (%)

Parent Information Project 108
D7. And which of the following best describes your living situation? Figure 11: Living Situation of Respondent (%)
D8: Do you personally or your youngest child under five have any special needs such as a learning or physical disability?
Table 14: Special Need Requirements of Youngest Child or Respondent (%)

Parent Information Project 109
Appendix 3: Websites Designed for Use by Parents and Children The internet was searched for websites designed for use by parents in Australia, Canada, the USA, England and Scotland. Noted below are those that provide examples to influence the design and execution of a New Zealand maternal and child health website or that contain particular examples of service delivery, or both.
Australia
Nationally http://raisingchildren.net.au/ http://raisingchildren.net.au/articles/smart_population_foundation.html/context/497 http://raisingchildren.net.au/link.aspx?id=2235 http://www.smartpopulation.org/ http://www.healthdirect.org.au/ http://www.parentline.com.au/home_ParentLine.aspx?s=11 http://www.parentline.com.au/template/standard.aspx?s=201 http://www.healthinsite.gov.au/
ACT http://www.parentlink.act.gov.au/index
New South Wales http://www.community.nsw.gov.au/parents_carers_and_families/parenting/general_tips_for_parents_and_carers.html
Queensland http://www.health.qld.gov.au/13health/default.asp
South Australia
Kids health http://www.cyh.com/SubDefault.aspx?p=255
Parent line http://www.parenting.sa.gov.au/helpline/
Child Health – Parent Line http://www.cyh.com/SubContent.aspx?p=102
Victoria
Best Start http://www.beststart.vic.gov.au/ http://www.education.vic.gov.au/ecsmanagement/beststart/

Parent Information Project 110
Early childhood services http://www.education.vic.gov.au/ecsmanagement/default.htm
Centre for Community Child Health http://www.rch.org.au/ccch/index.cfm?doc_id=10556
Parent lines http://www.education.vic.gov.au/earlychildhood/parentline/rpw.htm http://www.education.vic.gov.au/ecsmanagement/beststart/parents.htm http://www.sidsandkids.org/vic/
Health line http://www.health.vic.gov.au/nurseoncall/
Western Australia http://www.health.wa.gov.au/services/detail.cfm?Unit_ID=799
Canada Kidslink – http://www.ndsa.on.ca/ http://www.parentguide.ca/ http://creepublichealth.org/front/about/
England http://www.netmums.com/h/n/SUPPORT/HOME/ALL/464//
NHS Co-branding netmums http://www.netmums.com/h/n/PND/HOME/ALL/
PND http://www.netmums.com/h/f/SUPPORT/pndtest/
Edinburgh scale http://netmums.com/coffeehouse/advice-support-523/advice-support-40/serious-stuff-43/ http://www.mama.co.uk/default.asp?nc=9466&id=31 http://www.ukparentslounge.com/
Centre for parent and child support http://www.cpcs.org.uk/ http://www.nhs.uk/choices/sitemap.aspx http://talk.nhs.uk/ http://talk.nhs.uk/terms/houserules.aspx http://www.nhsdirect.nhs.uk/ http://www.nhs.uk/nhsdirect/Pages/nhsdlanding.aspx http://www.sja.org.uk/sja/first-aid-advice.aspx
New Zealand http://www.kidshealth.org.nz/
Parent Information Project 111
Canterbury webhealth portal– with kids health feed http://canterbury.webhealth.co.nz/information/information_pages/health/useful_links/kids_health?queries_searchfield_query=child%20health,%20parenting,%20parents,%20a-z
Scotland http://www.nhs24.com/content/ http://www.nhs24.com/content/default.asp?page=s29 http://www.nhs24.com/content/default.asp?page=s22_5_18
USA http://www.kidnetic.com/Whatis.aspx http://www.ific.org/kidnetic/
Pregnancy and babies http://parenting.ivillage.com/
Official kids portal for the USA http://www.kids.gov/
American Academy of Family Physicians http://familydoctor.org/online/famdocen/home.html
US Dept of Health & Human Sciences http://www.hhs.gov/kids/
A pediatrician’s guide – HON certified http://www.keepkidshealthy.com/
Am Academy of Peds http://www.aap.org/
Yale Medical Centre http://ymghealthinfo.org/content.asp?pageid=P02284
Podcasting http://www.nih.gov/news/radio/nihpodcast.htm/ http://www.tandemvoicebooth.co.nz/K/Vidcast-Podcast-BigPod-Web-creation-mobile-marketing-radio-television-video-audio-online-audios/_ID.ABC5198D-3048-53A3-B7DEB8DCCBEBCF25
MHSLA health podcasts – library http://mhsla.wordpress.com/2008/12/13/health-podcasts/
John Hopkins podcasts http://www.hopkinsmedicine.org/mediaII/Podcastsinstructions.html
Emerging technologies librarian – health podcasts http://mblog.lib.umich.edu/etechlib/archives/2008/12/health_podcasts.html
Society of critical care medicine http://www.sccm.org/publications/iCritical_Care/Pages/default.aspx

Parent Information Project 112
Family Health http://fhradio.org/
Blogs http://www.blogcatalog.com/topic/kids+health/
Nemours Foundation http://www.kidshealth.org.nz/index.php/pi_pageid/5 http://kidshealth.org/parent/kh_misc/about.html http://www.everybody.co.nz/ http://www.sdo.nihr.ac.uk/files/adhoc/appendix-to-jhsrp-review-article.pdf http://www.sdo.nihr.ac.uk/ http://www.erowid.org/general/about/about.shtml http://www.childrenspartnership.org//AM/Template.cfm?Section=Home http://www.urac.org/directory/DirectorySearch.aspx http://www.tommys.org/Page.aspx?pid=247 http://www.intute.ac.uk/about.html http://ec.europa.eu/information_society/eeurope/ehealth/index_en.htm http://www.tmc.edu/tmcnews/05_01_00/page_07.html http://www.babyfriendly.org.nz/page.php?9 http://www.ncbi.nlm.nih.gov/pubmed/18999150?ordinalpos=1&itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_DiscoveryPanel.Pubmed_Discovery_RA&linkpos=1&log$=relatedarticles&logdbfrom=pubmed http://www.bmj.com/cgi/content/short/333/7579/1143/ http://www.ama-assn.org/amednews/2006/12/11/bisb1211.htm http://www.ama-assn.org/ http://www.jpedsurg.org/home http://www.ask.com/bar?q=health+information&page=1&qsrc=1&zoom=%3CKW%3EHealth+Information%3C%2FKW%3E+Management%7C%3CKW%3EHealth+Information%3C%2FKW%3E+Management+Salary%7C%3CKW%3EHealth+Information%3C%2FKW%3E+Management+Jobs&ab=6&u=http%3A%2F%2Fwww.healthinformation.com.au%2F http://www.healthinformation.com.au/ http://www.aboutmyhealth.org/ http://www.eidohealthcare.com/conference/presentations.php http://www.informaworld.com/smpp/content~content=a713817021~db=all http://pandora.nla.gov.au/pan/48322/20050312-0000/www.facs.gov.au/internet/facsinternet.nsf/family/early_childhood_pip.htm
Internet quality criteria http://www.jmir.org/2001/4/e28/ http://www.sigmalist.com/SigmaMathTool/FogIndex.aspx http://simbon.madpage.com/Fog/ http://www.editcentral.com/gwt/com.editcentral.EC/EC.html http://www.online-utility.org/english/readability_test_and_improve.jsp http://www.bmj.com/cgi/content/full/324/7337/598?ijkey=3b84b37a4706a782047e27b1fbce47aead68c052&keytype2=tf_ipsecsha http://www.bmj.com/cgi/reprint/324/7337/569?ijkey=1fb014e8c22fd538fc8df614da91344c5ed019d5
Parent Information Project 113
http://archpedi.ama-assn.org/cgi/content/full/158/9/857 http://www.cche.net/usersguides/main.asp http://archpedi.ama-assn.org/cgi/content/abstract/158/9/857 http://emj.bmj.com/cgi/content/abstract/23/5/345 http://neuro-oncology.dukejournals.org/cgi/content/full/8/2/175 http://scholar.google.com/scholar?hl=en&q=Medical+and+Health+Information+Sites+on+the+Internet+AMA+2006&spell=1 http://www.discern.org.uk/
Well Child http://www.jmir.org/2001/4/e28/#ref16 http://www.hon.ch/HONcode/HON_CCE_en.htm#3.2 http://www.healthpoint.co.nz/search.do?branch=specialists&q= http://www.dohc.ie/ http://fas.org/ota/ http://www.ncchta.org/execsumm/summ536.shtml http://www.ncchta.org/project/1521.asp http://www.roma1.org/documents/CA/matrixmodel.html http://www.cpcs.org.uk/ http://www.livegroup.co.uk/chpp/ http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/DH_083645 http://www.scotland.gov.uk/consultations/health/hfac-00.asp
Australia parent websites http://www.aifs.gov.au/afrc/bibs/research.html http://www.facsia.gov.au/internet/facsinternet.nsf/aboutfacs/programs/sfsc-foundationhouse_factsheet.htm http://www.facsia.gov.au/internet/facsinternet.nsf/family/early_childhood_pip.htm http://www.rch.org.au/ccch/index.cfm?doc_id=10556 http://www.parentlink.act.gov.au/index http://www.community.nsw.gov.au/DOCS/STANDARD/PC_100220.html http://www.education.vic.gov.au/earlychildhood/parentline/rpw.htm http://www.rch.org.au/kidsinfo/index.cfm?doc_id=3665
UK parent websites http://www.everychildmatters.gov.uk/ http://www.netmums.com/h/f/HOME/home/ http://www.fatherhoodinstitute.org/ http://www.bbc.co.uk/parenting/family_matters/you_partner.shtml http://www.raisingkids.co.uk/homepages/homepage_default.asp http://www.kcl.ac.uk/schools/medicine http://www.guysandstthomas.nhs.uk/healthprof/education/gktmedicalschool.aspx http://www.nhsdirect.nhs.uk/Zones/Zone.aspx?zoneId=24 http://www.nhsdirect.nhs.uk/ http://www.familyandparenting.org/

Parent Information Project 114
http://www.equip.nhs.uk/groups/parents.html http://www.parentpages.co.uk/ http://www.thegoodwebguide.co.uk/index.php?rid=2637 http://www.ukparentslounge.com/
New Zealand parent websites http://www.starship.org.nz/ http://www.justbreathe.org.nz/viewforum.php?f=6&sid=ff8e66ac840536c5aa24b5d2086a04ae http://www.ohbaby.co.nz/forum/forum_posts.asp?TID=13059&PN=1&TPN=2 http://www.coffeegroup.org/newsletter_archives/2007-11.htm http://www.adsa.org.nz/coffee.html http://www.howickplunket.org.nz/groups.htm http://www.cleft.org.nz/category/coffee-groups/ http://reflux.cryingoverspiltmilk.co.nz/forum/viewforum.php?f=6 http://maternaljourney.co.nz/coffee-groups.html http://www.buzzonline.co.nz/Plunket-Services/Coffee-Groups/MenuId/177.aspx http://diyfather.com/ http://www.teamup.co.nz/ http://www.maternity.org.nz/links.shtml http://www.ksmidwifery.co.nz/faq.shtml http://www.kiwifamilies.co.nz/about+us.html http://www.bounty.co.nz/articles/baby http://www.nzfamilies.org.nz/parenting/ http://www.littlies.co.nz/ http://www.ohbaby.co.nz/Article.aspx?ContentID=210 http://www.treasures.co.nz/Default.aspx?DN=190971,23071,523,1,Documents http://www.groovybaby.co.nz/forum/viewforum.php?id=10 http://www.coffeegroup.org.nz/ http://www.hauora.com/links/ http://www.phics.org.nz/index.cfm/porirua_health_services/pacific_health_services.html http://www.phics.org.nz/index.cfm/phics_homepage.html http://www.phics.org.nz/ http://www.webhealth.co.nz/page/central_3.php http://www.brainwave.org.nz/ http://www.parentscentre.org.nz/about/default.asp http://www.familyservices.govt.nz/info-for-families/familyweb/connecting-with.html http://www.familyservices.govt.nz/info-for-families/familyweb.html http://www.earlystart.co.nz/ http://www.familyservices.govt.nz/our-work/strong-families/toddlers.html http://www.heartlandservices.govt.nz/locations/waipukurau.html http://www.heartlandservices.govt.nz/ http://www.raukawa.info/ http://www.familyservices.govt.nz/our-work/strong-families/skip/ http://www.plunket.org.nz/ https://www.parentsinc.org.nz/events/ https://www.parentsinc.org.nz/home/

Parent Information Project 115
http://www.kidshealth.org.nz/ http://www.kidshealth.org.nz/index.php/ps_pagename/printpage/pi_targetid/23/pi_id/87 http://wellingtonchildcare.org.nz/links/index.html http://youthline.co.nz/ http://www.parentandfamily.org.nz/ http://www.kiwifamilies.co.nz/ http://www.moh.govt.nz/moh.nsf/indexmh/childhealth-parentresources
Australia parentlines http://www.health.qld.gov.au/13health/default.asp http://www.healthinsite.gov.au/ http://www.healthdirect.org.au/ http://www.health.wa.gov.au/services/detail.cfm?Unit_ID=799 http://www.parentline.com.au/template/standard.aspx?s=201 http://www.parentline.com.au/home_ParentLine.aspx?s=11 http://www.parenting.sa.gov.au/helpline/
McKesson http://www.mckesson.com.au/index.php?option=com_content&task=view&id=87&Itemid=271#Telephone_triage
UK parentlines http://www.birminghamownhealth.co.uk/ http://www.nhs24.com/content/ http://www.nhsdirect.nhs.uk/ http://www.afasic.org.uk/helpline.htm http://www.youngminds.org.uk/parents/ http://www.patient.co.uk/showdoc/26740307/ http://www.gingerbread.org.uk/ http://www.children1st.org.uk/parentline/ http://www.loneparenthelpline.info/ http://www.parentlineplus.org.uk/
USA parent websites http://www.pncgrowupgreat.com/about.html http://www.pncgrowupgreat.com/ http://www.childrenshealthblog.com/about-2/ http://www.mummums.com/contact http://www.ahrq.gov/ppip/childguide/ http://bensguide.gpo.gov/pt/subject.html http://www.winstonswish.org.uk/
New Zealand parentlines http://www.childhelpline.org.nz/
Parent Information Project 116
http://www.phics.org.nz/index.cfm/phics_homepage.html http://www.nzfamilies.org.nz/node/424 http://www.parentline.org.nz/
HTA http://www.crd.york.ac.uk/crdweb/ http://www.hta.hca.wa.gov/ http://nzhta.chmeds.ac.nz/ http://www.ncchta.org/
Canada parentlines http://creepublichealth.org/front/about/ http://www.parentguide.ca/ http://www.parenthelpline.ca/revised_2006/linklibrary_eng.html
Canada parent websites http://www.earlyyearsinfo.ca/ http://www.thecmr.com/resources/links-180.htm http://www.resourceguideforparents.com/ http://www.parentguideblog.blogspot.com/ http://www.canadianparents.com/
USA child health http://www.pubmedcentral.nih.gov/ http://www.nursefamilypartnership.org/index.cfm?fuseaction=home http://www.childhealthdata.org/content/Default.aspx http://mchb.hrsa.gov/ http://www.nlm.nih.gov/medlineplus/childrenshealth.html
USA parentlines http://www.yourmedicaresolutions.com/staying_well/medicareblue_ppo/firsthelp_nurse.html http://www.first5la.org/Programs/First-5-LA-Parent-Helpline http://www.211bigbend.org/hotlines/parent/index.htm