parent behavioral training to modify child noncompliance: effects on untreated siblings
TRANSCRIPT

ooO5-7YO8/78/oWl-0235 $02.00/O
PARENT BEHAVIORAL TRAINING TO MODIFY CHILD
NONCOMPLIANCE: EFFECTS ON UNTREATED SIBLINGS
LEWIS HUMPHREYS, REX FOREHAND, ROBERT McMAHON and MARK ROBERTS
University of Georgia
Summary-The purpose of the present study was twofold: (a) to examine changes in parent behavior toward an untreated sibling after parent behavioral training to modify a target child’s noncompliance and (b) to examine changes in the untreated sibling’s behavior. Eight clinic- referred children and their mothers served as the subjects. Parent training consisted of the use of a \tandardiled clinic program to modify child noncompliance. The outcome measure was home observation\ of the parent and untreated child’s interactions. The results indicated significant change< in both the parent’s behavior and the untreated sibling’s noncompliance.
Although parent behavior training is an effective method of modifying child problems in the home (Berkowitz and Graziano, 1972; O’Dell, 1974), the effect of such training on the behavior of untreated siblings of the target child has received minimum attention. Resick, Forehand and McWhorter (1976) and Lavigueur, Peterson, Sheese and Peterson (1973) each reported positive changes in a child when a sibling received treat- ment. Unfortunately, both of these studies were case reports involving only one family each. In the only group study, Arnold, Levine and Patter- son (1975) reported decreases in siblings’ deviant
behavior when the target child was treated. However, in two-thirds of the treated families,
one or more of the siblings were actively involved in the treatment program implemented by the parents, thus making it difficult to interpret the results. It has been hypothesized that parent behavior change produces the change in the untreated sibling’s behavior (cf. Arnold et al., 1975). However, the Lavigueur ef al. (1973) study was the only one which reported parent behavior data; consequently, the hypothesis that parent training and, subsequently, parent behavior change produce change in the untreated siblings’ behavior has received minimum sup- port.
The purpose of the present study was to ex-
amine the behavior of an untreated sibling when parents are trained to modify noncompliance of a treated child. Both the sibling’s compliance and the parent’s behavior directed toward the sibling were measured. Furthermore, none of the siblings was involved in treatment. Non- compliance was selected as the target behavior as it is the most frequently reported problem of clinic-referred and non-clinic children (Forehand, 1977). The parent training program that was utilized has been demonstrated effectively to modify selected parent behaviors and child non- compliance in clinic settings (Forehand and King, 1974, 1977; Hanf and Kling, 1973; Peed, Roberts and Forehand, 1977). Furthermore, these changes have generalized to the home (Peed et al., 1977). The change in home behavior has been maintained at a one year follow-up and has not been associated with any adverse child behavior change in school (Forehand, Sturgis, McMahon, Aguar, Green, Wells and Breiner, 1978). Finally, it has been demonstrated that none of the parent and child behavior changes is the result of the passage of time or unspecified environmental factors since Peed et al. (1977) found no changes from pre to post- treatment in any parent or child behaviors in the home over a 30 day period for a waiting list control group. A control group was not viewed
This research was supported in part by a University of Georgia Research Council grant and NIMH grant MH-28859-01. Reprints should be addressed to Rex Forehand, Psychology Department, University of Georgia, Athens, GA 30602.
235

236 LEWIS HUMPHREYS, REX FOREHAND, ROBERT McMAHON and MARK ROBERTS
as necessary in the present study as the treatment
time and demographic characteristics of the present sample were equivalent to Peed et al.‘s control group.
METHOD
Subjects Subjects were eight “family units”, defined as a mother
and two siblings for purposes of this study. One sibling from each family was referred to the University of Georgia Psychology Clinic for treatment of noncompliant behavior problems. Severely retarded, brain damaged, or “autistic” children were excluded from the study.
At the initial contact, the mean age of the target children was 77.6 months (range: 47-96 months). All target children were males. The mean age of the untreated siblings was 60.6 months (range: 30-128 months). Seven of the untreated siblings were female and one was male. The mean difference in age of the target child and untreated sibling was 39 months (range: 22-51 months), with five of the eight target children older. Six of the families included both parents while the father was absent in two cases.
The index of social status developed by Myers and Bean (1968) was used to determine the socioeconomic status of each family. Using occupation and educational level of the head of the household, each family was assigned a social class standing of I (e.g. professionals) to V (welfare recip- ients). The mean social class status for the eight families was Class III (range: I-IV).
Therapists and observers Two fourth-year clinical psychology graduate students
experienced in treating mother-child pairs with the two- stage parent training program developed by Hanf (Hanf and Kling, 1973) served as the primary therapists. Five undergraduate students served as primary observers in the home and two graduate students served as “calibrating observers”, obtaining reliability checks on the home obser- vers. Therapists collected observation data in the clinic. Four weeks prior to the start of observations on the first family, all observers and therapists received 16 hr of training in use of the coding system. All coders were required to obtain at least 80% agreement with a pre-scored key for a five minute videotape of an actual mother-child interaction. Weekly one hour training sessions were held for all coders throughout the study.
Outcome measure The interactions between the mother and untreated
sibling were coded in the home during four to eight PRE (pre-treatment) observations (X = 6) and during four POST (post-treatment) observations. The mother was instructed to follow her daily routine as much as possible and to interact with the children as she normally would, within the following limitations. She was instructed to limit her activities to two adjoining rooms, to ignore the observer, and to avoid having visitors, telephone calls, or the tele-
lision on during the observation. Other family members were allowed to be present but were not coded.
Observers equipped with a cassette tape recorder, ear- phone, and coding sheets positioned themselves so that they could observe the mother interacting with the untreated sibling. They did not interact with family members during the observation, referred all treatment related questions to the therapist, and did not discuss with the parent whose behavior they were observing. A casette tape recording signalled 30 set intervals via an earphone. Observers collected data in five minute blocks, with one minute rest periods each ten minutes. For each home observation session the interaction between the mother and the untreated sibling was observed for 20 min.
Mothers were informed that observations were to be of typical family interactions so that at least two children were required to be present for all observations. However, until after completion of the study, mothers were not told the untreated sibling’s behavior and the mother’s interaction with this child were coded. Observers were kept blind as to the purposes of the study, the treatment procedures em- ployed, and the reason for the observations of a particular child.
The following parent and sequential sibling-parent behaviors were recoded in each home observation session.
Parent behaviors (1) Rewards. (a) Praise, approval, or positive physical
attention which refers to the child or the child’s activity or (b) descriptive phrases that follow and refer to the child’s ongoing behavior, to objects directly related to his play, to his spatial position, or to his appearance.
(2) Commands, (a) alpha commands. An order, rule, suggestion, or question to which a motoric response is appropriate and feasible.
(b) beta commands. Commands to which the child has no opportunity to demonstrate compliance. Beta commands include parental commands which are (a) so vague that proper action for compliance cannot be deter- mined; (b) interrupted by further parental verbiage before enough time (5 set) has elapsed for the child to comply; or (c) carried out by the parent before the child has an opportunity to comply.
(3) Time-out. A procedure used by the parent that clearly is intended to remove the child from positive rein- forcement because of the child’s inappropriate behaviors (e.g. placing the child in a chair in the corner of the room, sending him to his room).
Sequentialsibling-parent behavior (1) Child compliance. An appropriate motoric response
initiated within five seconds following a parental alpha command.
(2) Child noncompliance. Failure to initiate a motoric response within five seconds following a parental alpha command.
(3) Contingent attention. A reward presented by the parent within five seconds following the initiation of Child Compliances.
For purposes of analysis, the following parent behaviors were expressed in terms of rate per minute: rewards and beta commands. (Time-outs occurred too infrequently for
PARENT BEHAVIORAL TRAINING TO MODIFY CHILD NONCOMPLIANCE 231
analysis and alpha commands were not of interest as they were not directly manipulated.) Additionally, the following percentage scores were computed: percentage of child compliance to maternal commands = No. of child com- pliances/No. of maternal commands x 100; and percentage of parental contingent attention = No. of contingent attentions/No. of child compliances x 100.
Reliability checks were made on 27% of the home observations (25% for PRE observations; 30% for POST observations) by having a calibrating observer record the entire observation along with the regular observer. A split earplug device was used to synchronize recording intervals for the two observers. For purposes of obtaining observer agreement, all parent and sequential child-parent behaviors were coded in a framework of consecutive 30 set intervals in which a maximum of ten interactions could be recorded. Agreement between the observer and calibrating observer was calculated by dividing the total number of agreements by the total number of calibrator codes for each 30 set segment. The event-by-event analysis required agreement for both category of behavior and sequence. Reliability checks revealed an average agreement of 77% between observers for the mother’s and untreated sibling’s behavior.
Procedure The procedure has been described in detail elsewhere
(Forehand and Peed, 1978; Forehand et al., 1978; Peed et al., 1977) and will only be briefly presented here. Following referral to the Psychology Clinic, each mother was inter- viewed to determine if noncompliance was the primary child problem. Furthermore, a parent-child interaction in a laboratory setting was observed. For children whose primary problem was noncompliance, the parent and child were accepted into the program and PRE home observations were completed. Immediately following treatment POST observations were conducted.
Treatment All treatment took place in clinic playrooms equipped
with one-way mirrors for observation, sound system, and bug-in-the-ear (Farrall Instruments). The treatment was divided into two stages. In Stage 1 of the treatment program the mother learned to be a more effective reinforcing agent by increasing the frequency and range of her social rewards and by reducing the frequency of competing verbal behavior. She first was taught to attend to the child’s behavior and describe the child’s activity. No commands, questions, or criticisms directed to the child were to be used. Next in Stage I the mother was taught to use contingent rewards. Throughout Stage I the principle of increasing compliance through use‘ of contingent attention was stressed. Homework was assigned in the form of daily ten minute practice sessions in which the mother was to practice using the skills taught in the clinic with the child.
Stage II of the treatment consisted of training the mother to use a timeout (TO) procedure to decrease noncompliant behavior exhibited by the child. She was taught to give direct, concise commands and to allow the child sufficient time to comply. She learned to reward compliance which was initiated within five seconds of her command with con- tingent attention. If compliance was not initiated, the mother was trained to implement a TO procedure involving
the child sitting in a chair in a corner (see Forehand et al., 1978, for details). During practice sessions in the clinic the mother was instructed to issue a series of commands designed to elicit noncompliance so that the timeout pro- cedure should be practiced. A list of nonclinic settings in which noncompliance occurred was constructed and use of TO in these settings was discussed with the mother. .’ During treatment the therapist did not initiate discussion of application of the procedures to the untreated child. If the parent stated that she planned to use the procedures with both the target and untreated children, the therapist agreed that the procedures were general ones which were applicable to all children. No further elaboration of this point was made. Specific discussion of behavior problems in the untreated child was deferred until after completion of the POST observations.
Procedure for each treatment session. Each treatment session consisted of the following steps: (a) therapist observing and coding a five minute mother-target child interaction (the observation was of a free play situation during Stage I and of a parent structured situation during Stage II); (b) discussion with the mother about her use of reinforcement (Stage I) or TO (Stage II) during the preceding observation period and at home; (c) modeling of additional reinforcement (Stage I) or TO (Stage II) techniques for the mother by the therapist; (d) practice of the reinforcement (Stage I) or TO (Stage II) techniques in a roleplaying situ- ation with the therapist acting the part of the child; (e) a practice period for the mother with the child in which she wore the bug-in-the-ear and received instructions and immediate feedback from the therapist; (f) a second observation period identical to step (a).
Treatment criteria. Progression through the two treatment stages was based on,behavioral criteria used in the Peed et al. (1977) investigation. The therapist used the data collected during the observations at the beginning and end of each treatment session to determine if the mother- child pair had attained the behavioral criteria necessary for moving to the next segment of treatment (see Peed et al. for details of the criteria). All mothers and target children met criteria, indicating that the desired behavior change was achieved for these individuals. The mean number of treatment sessions was 5.6 and the mean time in treatment was 3 1 days.
RESULTS ANG 2;iSCUSSION
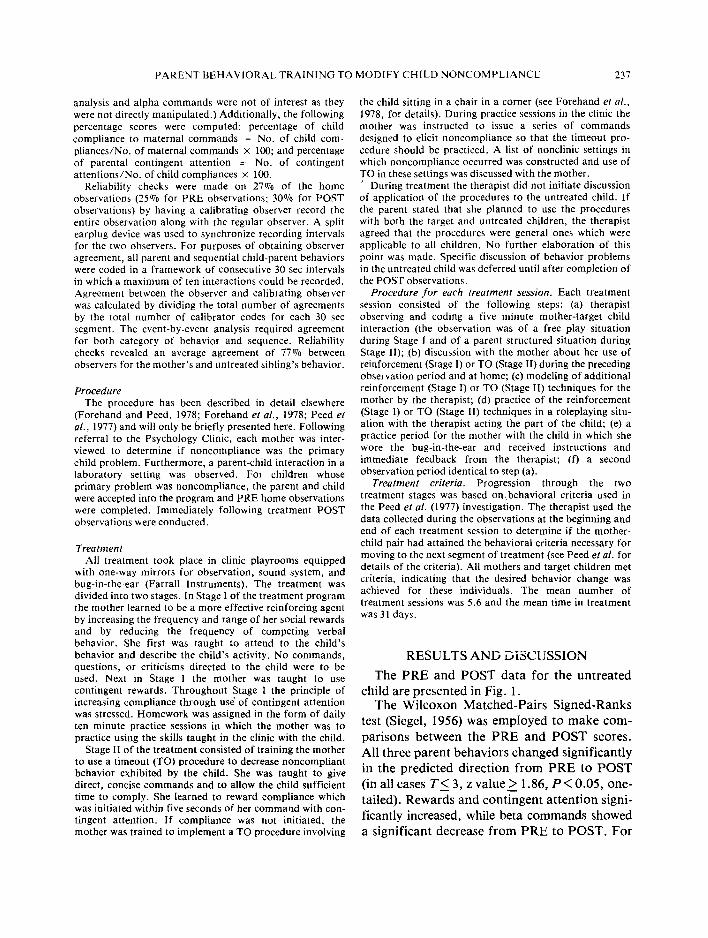
The PRE and POST data for the untreated child are presented in Fig. 1.
The Wilcoxon Matched-Pairs Signed-Ranks test (Siegel, 1956) was employed to make com- parisons between the PRE and POST scores. All three parent behaviors changed significantly in the predicted direction from PRE to POST (in all cases TL 3, z value > 1.86, P< 0.05, one- tailed). Rewards and con&gent attention signi- ficantly increased, while beta commands showed a significant decrease from PRE to POST. For

238 LEWIS HUMPHREYS, REX FOREHAND, ROBERf McMAHON and MARK ROBERTS
.v. :::::
40 ::::: :::::
k .:*:. 2 3:;
5 30 ::::: . . . . . :::;:
E $i
a 20
- :::::
$Q :.:.:
? ::::: . . . . .
2 . . . . .
.I0 3;:;
;g; ::::: . . . . .
0 :::::
0 PRE
m POST
I :.:.: :.:.: ::::: ILL A..
i$$ ::::: I ::::: .:.:. . . . . .
::::: I gi ::::: . ::::: , 3:;. ::::: , :::y
$g , :::y :::::: . . .
1
:
50 the exception of two case reports (Lavigueur et
al., 1973; Resick et al., 1976), the present results 40 are the first to indicate that siblings not involved
?I in treatment demonstrate positive behavior
30 =:
r changes following behavioral training with
2 parents and a problem target child. 20
z
REFERENCES IO Arnold J. E., Levine A. G. and Patterson G. R. (1975)
Changes in sibling behavior following family intervention,
0 J. Consuli. Cl/n. Psycho/ 43,683.688. REWARDS BETA CONTINGENT COMPLIANCE
COMMANDS ATTENTION TO
COMMANDS ’
Fig. 1. Mean occurrence at PRE and POST of parental rewards, beta commands, and contingent attention addressed to the untreated siblings and mean per cent compliance to commands by the untreated siblings. Rewards and beta commands are expressed in rates per minute and should be read from the left vertical axis. The remaining two behaviors are expressed as percentages and should be read from the
right vertical axis.
the child behavior, compliance to commands increased significantly from PRE to POST (T = 6, z = 1.68, P< 0.05, one-tailed).
The changes in three parent behaviors indicate that parents do use the behavioral skills learned in a parent training program with siblings of the treated child. Furthermore, the parent behavior change toward untreated siblings occurred without the aid of direct programming by the therapist (i.e. no prompting or instructions were given to employ the skills learned in the clinic with the treated child in the home with the untreated child). In addition to parent behavior change, sibling compliance to com- mands increased from PRE to POST. This finding indicates that the changes in parent be- havior were associated with increases in the untreated sibling’s compliance without that child being a focus of treatment.
With , the exception of one case report (Lavigueur et al., 1973), the present study is the first to indicate that parent training produces changes in parental behaviors toward children other than the target child. Furthermore, with
Berkowitz B. P. and Graziano A. M. (1972) Training parents as behavior therapists: a review, Behav. Rex & Therapy 10,297-317.
Forehand R. (1977) Child noncompliance to parental commands: behavioral analysis and treatment, In Pro- gress in Behavior Modification (Ed. by Hersen M., Eisler R. M. and Miller P. M.). pp. I1 1.147. Academic Press, New, York.
Forehand R. and King H. E. (1974) Pre- school children’s non-compliance: effects of short- term therapy, J. Commun. Psycho/. 2.42-44.
Forehand R. and King H. E. (1977) Noncompliant children: effects of parent training on behavior and attitude change, Behav. Modificafion 1, 93-108.
Forehand R. and Peed S. (1978) Training parents to modify noncompliant behavior of their children. In Treatment and Re.rearch in Child Psychopathoiogy. (Ed. by Finch A. J. and Kendall P. C.). Spectrum, New York. (In press).
Forehand R., Sturgis E., McMahon R., Aguar D., Green K., Wells K. and Breiner J. (1978) Parent behavioral training to modify child noncompliance: generalization across time and from home to school, Behav. Modification (In press).
Hanf C. and Kling J. (1973) Facilitating parent-child inter- action: a two stage training model. Unpublished manu- script, University of Oregon Medical School.
Lavigueur H., Peterson R. F., Sheese J. G. and Peterson L. W. (1973) Behavioral treatment in the home: effects on an untreated sibling and long term follow-up, Behav. Therapy 4,43 1-441.
Myers J. K. and Bean L. L. (1968) A Decade Later: A Follow-up of Social Class and kental Illness. Wiley, New York.
O’Dell S. (1974) Training parents in behavior modification: a review, Psychol. Bull. 81,418.433.
Peed S., Roberts M. W. and Forehand R. (1977) Evaluation of the effectiveness of a standardized parent training program in altering the interaction of mothers and their noncompliant children, Behav. Modification 1, 223-250.
Resick P. A., Forehand R. and McWhorter A. (1976) The effect of parent treatment with one child on an untreated sibling, Behav. Therapy 1, 544548.
Siegel S. (1956) Nonparametric Statistics for the Behavioral Sciences. McGraw-Hill, New York.