para 1000 introduction to paediatrics - flinders learning ... · pdf filegastroenteritis,...
TRANSCRIPT

PARA 1000
Introduction to Paediatrics
Dr John Craven
2015

• The Normal Child
– Ages
– Anatomical and physiological differences
– Stages of development
• The Sick Child
– Presentations
– SIDS
Session outcomes
2

References

The Normal Child

• Newborn
• Neonate (0 - ~6weeks)
• Infant (~6 weeks - ~12 months)
• Toddler (~12months - ~24 months)
• Child (2 yrs ~ 12yrs)
• Adolescent (~12yrs - ~29 yrs)
Ages of Childhood
Newborn

• Transition of fetus to a baby
• Physiological & environmental changes:
– Circulation (placental/umbilical flow, shunting of blood through
heart and through ductus arteriosis)
– Respiration (oxygenation from lungs rather than placenta)
– Exposure to environmental microbes
– Exposure to cold
• Oxygenation and drying of child
• Initiation of feeding
Newborn

• Talk to the parents
– Often new experience for them
– Parental anxiety and expectations
• Look at the child
– Does the child look okay?
• Does the child ‘handle’ well?
Approach to the Newborn

• Establishment of feeding
• Colonisation with commensal bacterial
• Poor immune function
• Poor thermoregulation
• Immobility
Neonate (0-6 weeks)

• Feeding/sleeping/irritability issues
• High risk of bacterial infection
• Sudden Unexplained Death in Infancy (SUDI)
– (previously Sudden Infant Death Syndrome (SIDS)
Neonate (0-6 weeks)

• Develops from minimal movement to rolling,
sitting, crawling, and walking
• Remains highly dependant on environment
Infant (6 weeks – 12months)

• Mobile child 12-24mths
• Exploring, inquisitive, exploring
• Development of language and
communication
Toddler

• High rate of infection (hand to mouth,
infectious contacts)
• Immune system still developing fully
Toddler

• 2 yrs – puberty (~12yrs)
• Further language and social development
• Increased size and physical activity
• Less dependence on the family environment
• Through to beginning of pubertal
development
Child
• Adult size
• Establishment of adult (or pseudo adult)
behaviours
• Pushing of boundaries
– Risk taking (physical activities, drug use)
– Sexual exploration
• Mental health
– Depression
– Eating disorders
– Schizophrenia
Adolescent

Adolescent

Differences between small children
and large children (adults)

Physiological differences
Different body proportions
through & across ages
Smaller children have:
• Larger skin surface
• Higher water volume/kg
• Less total blood volume
• Mature at different rates
• Hyper-metabolic
• Poor heat regulation
• Age related body issues
Childhood growth and development (Ref 74: Children and clinical studies)
Weight variation across an age (Ref62: essential Baby 2011)

Physiological differences
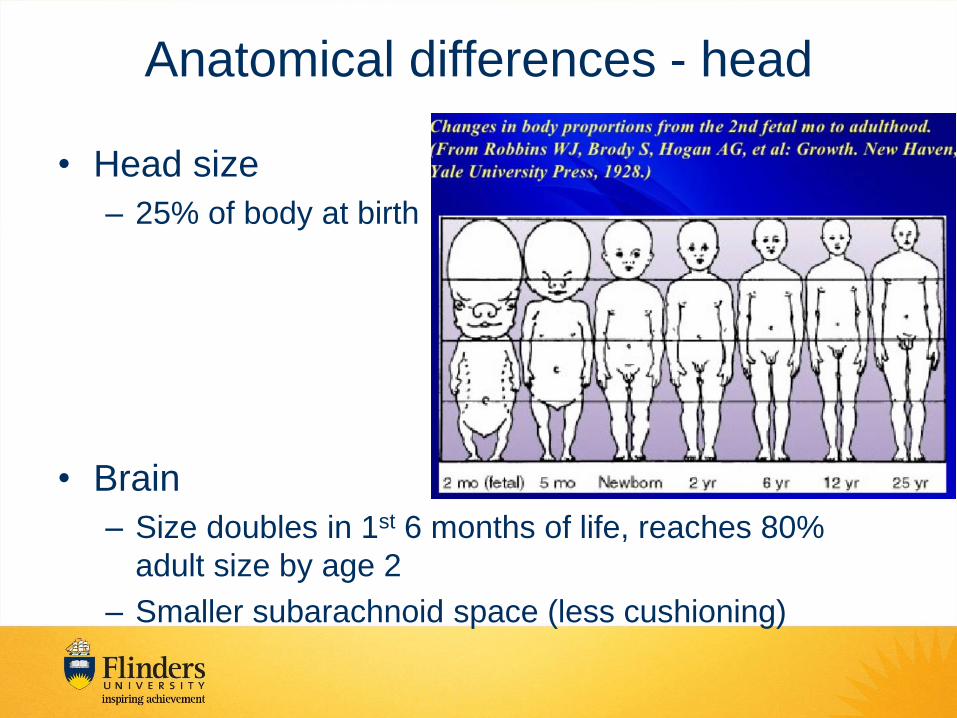
Anatomical differences - head
• Head size
– 25% of body at birth
• Brain
– Size doubles in 1st 6 months of life, reaches 80%
adult size by age 2
– Smaller subarachnoid space (less cushioning)

Anatomical differences - head
• Fontanelles and Sutures
– Anterior closes <18mths
– Posterior closes <3 mths
– Sutures may be palpable
Anatomical differences • Spine
– Hypermobile and incompletely ossified
– Large head + weak neck muscles
• Vision – Pupillary light reflex from 28 wks gestation
– Fix and follow at term
– Visual acuity development • 6/45 at term
• 6/18 at 4mths age
• 6/6 at 6-8 mths
– Colour vision normal from birth

Anatomical differences – Airway
Paediatric and adult airway differences (Ref37: New York State Health)

Anatomical differences – Airway
Paediatric and adult airway differences (Ref37: New York State Health)
• Large tongue
• Soft compressible sub glottic area
• Soft palate
• Initially obligate nasal breather
• High anterior floppy larynx
• Narrowest at the cricoid

Anatomical differences - Chest
• Chest wall more compliant – Blunt chest trauma fracture ribs infant and young child, due to the
increased elasticity and compliance of the chest wall.
– The force may be transmitted through to the underlying structures,
which may sustain significant internal injuries.
• Increased mobility of the mediastinal
structures – The increased mobility of the mediastinum increases the likelihood
that the injured child may develop a tension pneumothorax from a
simple pneumothorax, or transect a small mediastinal vessel as the
mediastinum shifts.

Anatomical differences - Abdomen
• Relatively thin abdominal
wall – Provides less protection to abdominal
organs.
• Abdominal organ proportions
and placement – Flatter diaphragm pushes the liver and
spleen further below the rib cage.
– Liver and spleen are more abdominal and
they are more likely to be injured.
– The infant bladder is an intra-abdominal
organ, increasing the risk of bladder
damage in abdominal trauma.

Anatomical differences - Musculoskeletal
Growth plates not fused
• Epiphyseal plate does not fuse until after the pubertal growth
spurt
Cartilaginous bones
• The bones of children are more cartilaginous and flexible but also
more likely to break than ligaments or tendons
– Green stick fractures are common
– Sprains (ligament or tendon injuries) are less common
– Flexible ribs will transmit force to underlying organs
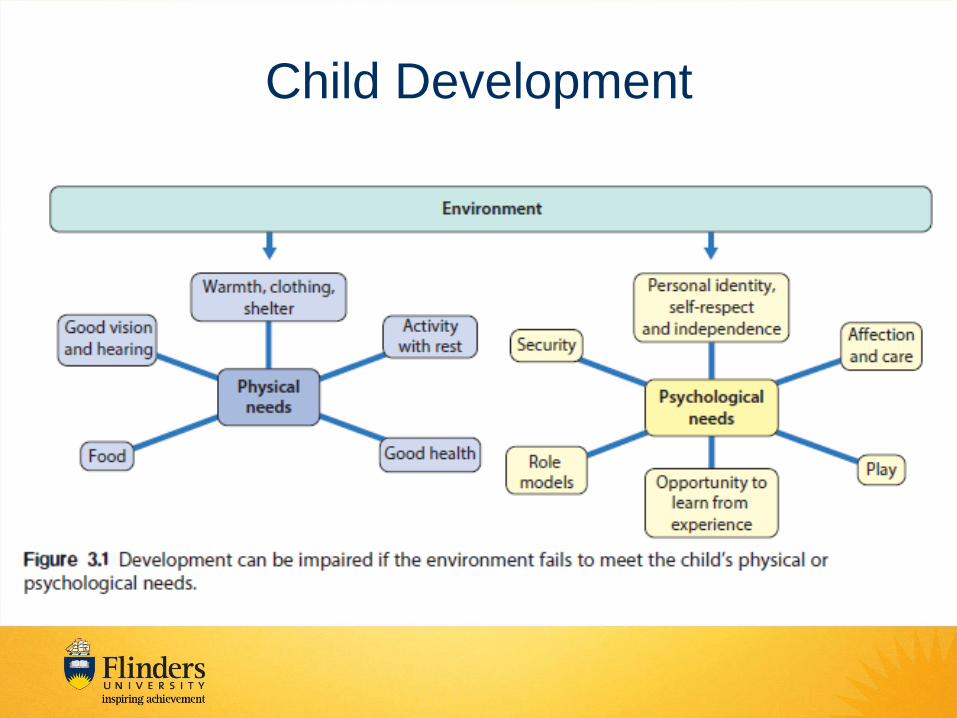
Child Development

Child Development
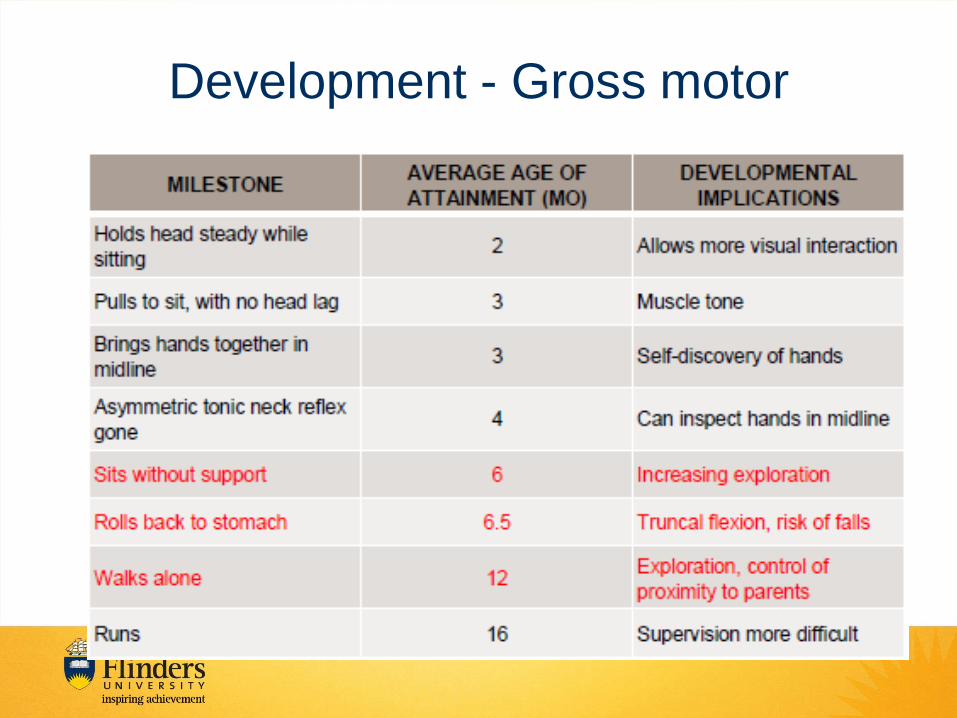
Development - Gross motor


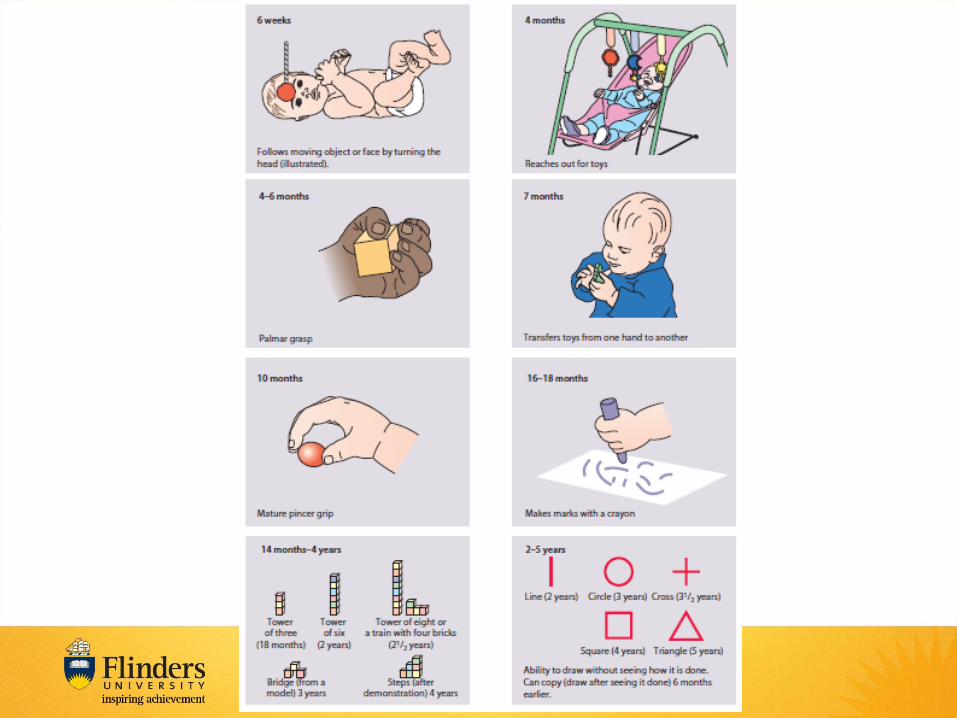
Development - Fine motor
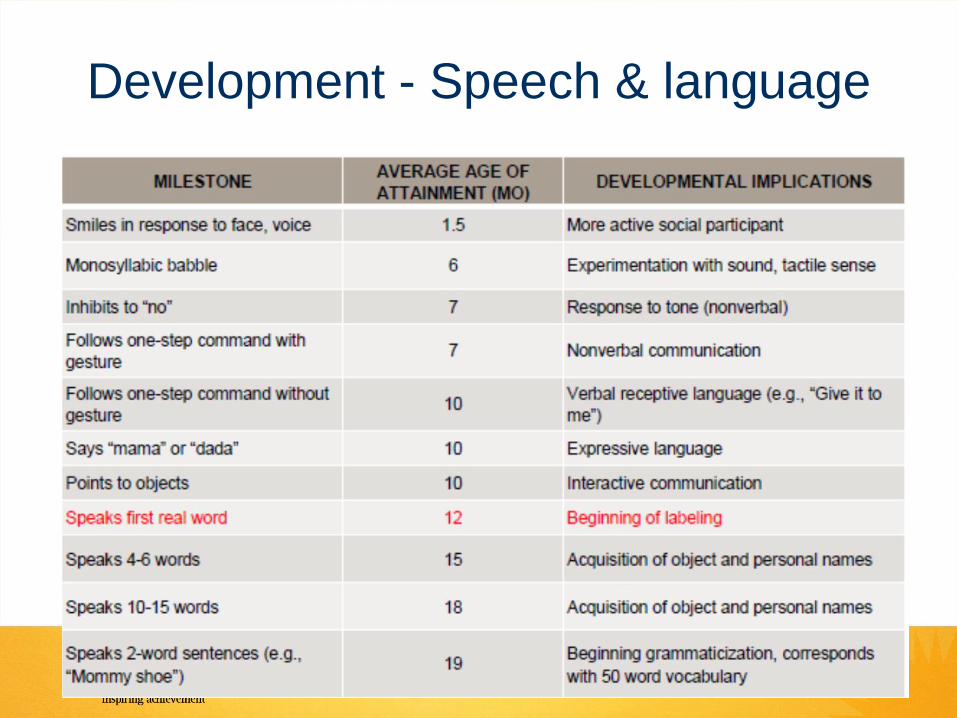
Development - Speech & language
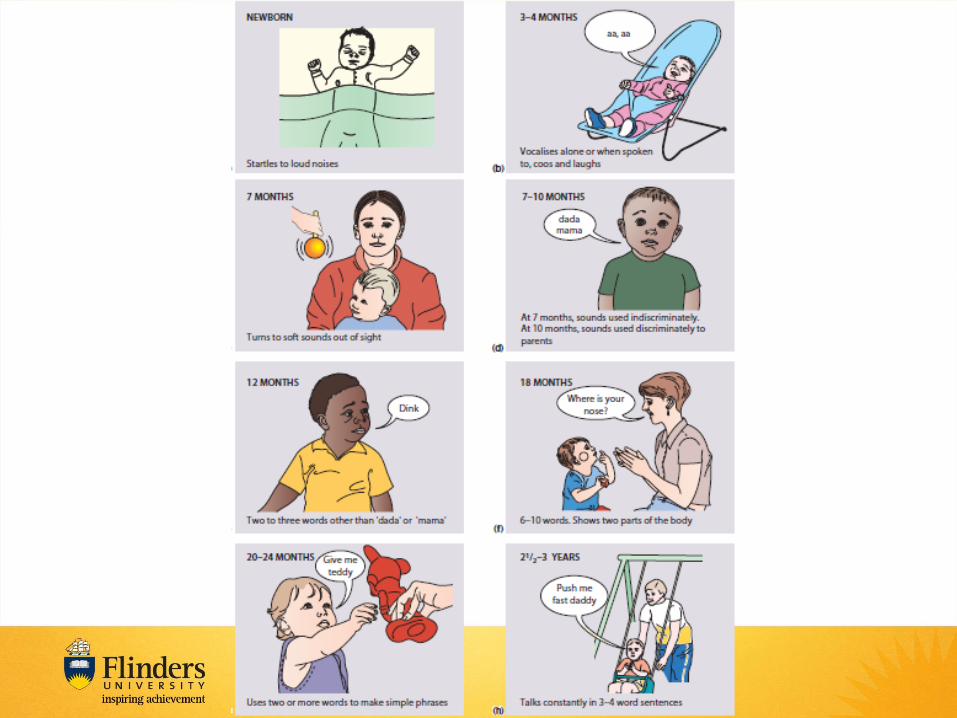

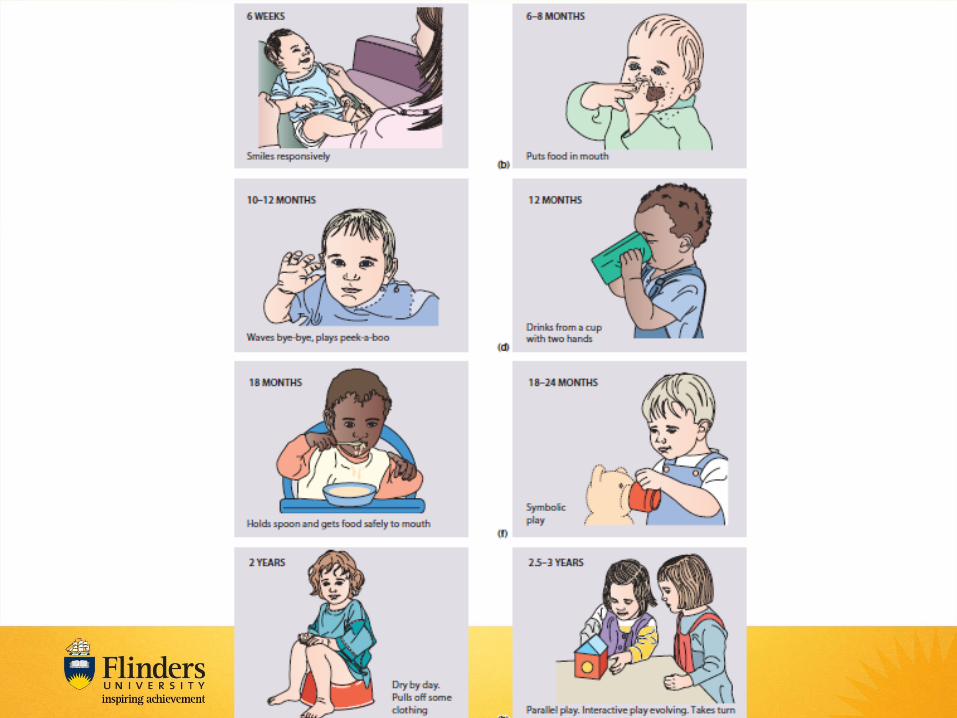
Development - Cognitive and social

• Pick up genetic/congenital/environmental
issues
• Target therapy
• Allows tailoring of the therapeutic approach to
the child
Why child development?

The Sick Child

• Wide range of disorders
that can chronically or
intermittently affect a
child or raise risk of
certain illness developing
• Most parents are experts
in their child’s condition
Congenital/Genetic Problems

• FMC ~18 500 presentations per year
• WCH ~42 000 presentations per year
• Children represent ~2-5% of SAAS transfers
Presentations to hospitals

Patterns of presentation to the Australian and New Zealand Paediatric Emergency
Research Network
Emergency Medicine Australasia
Volume 21, Issue 1, pages 59-66, 17 FEB 2009 DOI: 10.1111/j.1742-6723.2009.01154.x
http://onlinelibrary.wiley.com/doi/10.1111/j.1742-6723.2009.01154.x/full#f1

Patterns of presentation to the Australian and New Zealand Paediatric Emergency
Research Network
Emergency Medicine Australasia
Volume 21, Issue 1, pages 59-66, 17 FEB 2009 DOI: 10.1111/j.1742-6723.2009.01154.x
http://onlinelibrary.wiley.com/doi/10.1111/j.1742-6723.2009.01154.x/full#f2


Age (years) Diagnosis Count Proportion of ED presentations by age
group (%)
<1 yr
(n = 51 753)
1. Bronchiolitis, acute 6214 12.0
2. Gastroenteritis, acute 4610 8.9
3. URTI, acute 4484 8.7
4. Viral illness, acute 3966 7.7
5. Fever without identifiable source 1639 3.2
1–4 yr
(n = 119 610)
1. Gastroenteritis, acute 9393 7.9
2. Viral illness, acute 8405 7.0
3. URTI, acute 8077 6.8
4. Asthma, acute 6148 5.1
5. Croup, acute 5524 4.6
5–9 yr
(n = 59 657)
1. Gastroenteritis, acute 2785 4.7
2. Viral illness, acute 2580 4.3
3. Abdominal pain, non-specific 2489 4.2
4. Asthma, acute 2304 3.9
5. Fractured forearm (radius and/or ulna) 2158 3.6
10–14 yr
(n = 42 596)
1. Abdominal pain, non-specific 2360 5.5
2. Fractured forearm (radius and/or ulna) 1857 4.4
3. Gastroenteritis, acute 1090 2.6
4. Asthma, acute 934 2.2
5. Viral illness, acute 832 2.0
15–18 yr
(n = 10 711)
1. Abdominal pain, non-specific 541 5.1
2. Toxic effect of substance (including alcohol) 308 2.9
3. Psychiatric or behavioural problems 233 2.2
4. Gastroenteritis, acute 216 2.0
5. Asthma, acute 212 2.0
Acworth et al. Patterns of presentation to the Australian and New Zealand Paediatric
Emergency Research Network. Emerg Med Australas. 2009 Feb;21(1):59-66.

• Most paediatric presentations can be divided
into 3 groups:
– Obviously well child
– Obviously sick child
– Potentially sick child
• Severe form of a usually benign illness
• Early subtle signs of a serious illness
• Appear unwell but need investigation to rule out serious
illness
Identification of the sick child

Assessing a sick child -
observation

• Does this child look sick?
• What is it that makes you reach this
opinion?

Summary: Assessment Assessment of the unwell child
Airway and Breathing
• Effort •Respiratory rate •Accessory muscle use •Flaring of the nostrils, head
bobbing, tracheal tug •Child's position
• Efficacy •Chest expansion •Air entry •Pulse oximetry
• Effects of Inadequacy •Respiratory rate •Skin (colour/temperature) •Mental status
Circulation
• Signs: • Heart rate • Capillary refill time • Blood pressure • Skin temperature
• Effects of Inadequacy • Respiratory rate • Skin
(colour/temperature) • Mental status
Disability
• Conscious level
• Posture
• Pupils

• Sudden death of an infant that is not predicted by
medical history and remains unexplained after a
thorough forensic autopsy and detailed death scene
investigation.
• Infants are at the highest risk for SIDS during sleep.
• Typically the infant is found dead after having been
put to bed, and exhibits no signs of having struggled.
Sudden Infant Death Syndrome (SIDS)
Sudden Unexplained Death in Infants
(SUDI)



Sudden Infant Death Syndrome (SIDS)
Sudden Unexplained Death in Infants (SUDI)


• Gaining rapport with the child and the confidence of the
parents is the key to assessing the child
• Address the concerns of the parents/carers – they know
what the child is normally like
• A child needs to be approached according to
chronological and developmental age
• Observation is a vital diagnostic tool
• It is often more important to exclude serious illnesses
than make a definitive diagnosis
• A child should be considered sick until it can be
concluded they are well following a thorough assessment
Paediatrics Tips
