pancreas (amiloidosi laini flavia vittoria)
TRANSCRIPT

Regulation of Carbohydrate Metabolism
http://www.fisiokinesiterapia.biz/NewDownload/Pancreasendocrino.pdf
VEDI ANCHE POWER POINT DA PAGINE
WEB

Pancreatic Anatomy
Gland with both exocrine and endocrine functions
15-25 cm long 60-100 g Location: retro-peritoneum, 2nd lumbar
vertebral level Extends in an oblique, transverse position Parts of pancreas: head, neck, body and tail
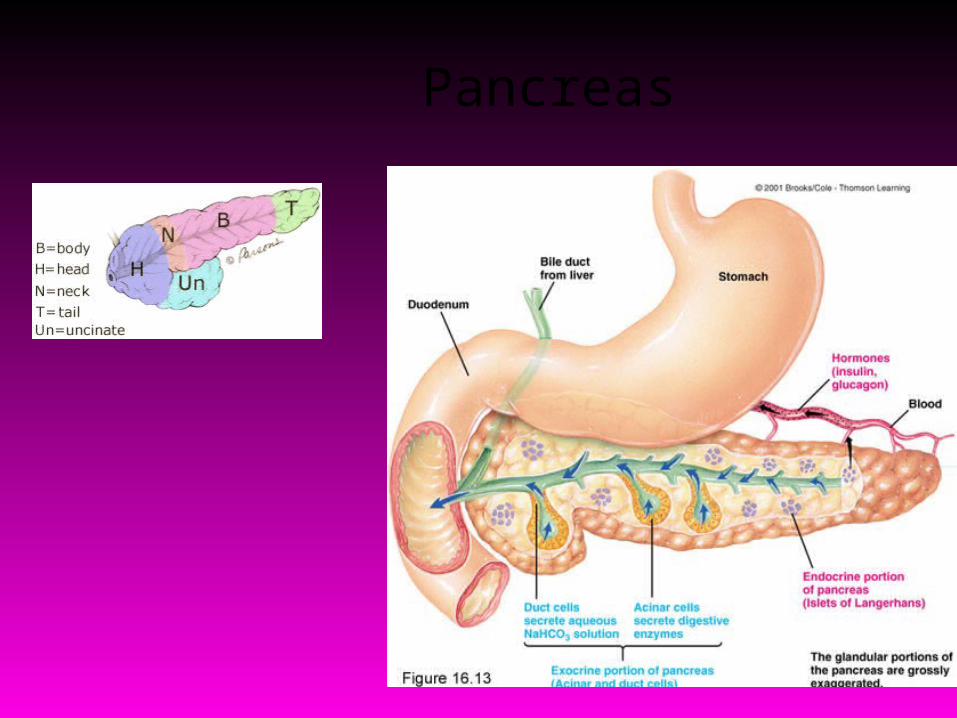
Pancreas

Head of Pancreas
Includes uncinate process Flattened structure, 2 – 3 cm thick Attached to the 2nd and 3rd portions of
duodenum on the right Emerges into neck on the left Border b/w head and neck is determined
by GDA insertion SPDA and IPDA anastamose between the
duodenum and the right lateral border

Neck of Pancreas
2.5 cm in length Straddles SMV and PV Antero-superior surface supports the
pylorus Superior mesenteric vessels emerge from
the inferior border Posteriorly, SMV and splenic vein
confluence to form portal vein Posteriorly, mostly no branches to pancreas
Body of Pancreas
Elongated, long structure Anterior surface, separated from
stomach by lesser sac Posterior surface, related to aorta, lt.
adrenal gland, lt. renal vessels and upper 1/3rd of lt. kidney
Splenic vein runs embedded in the post. Surface
Inferior surface is covered by transverse mesocolon

Tail of Pancreas
Narrow, short segment Lies at the level of the 12th thoracic
vertebra Ends within the splenic hilum Lies in the splenophrenic ligament Anteriorly, related to splenic flexure of
colon May be injured during splenectomy
(fistula)

Pancreatic Duct
Main duct (Wirsung) runs the entire length of pancreas
Joins CBD at the ampulla of Vater 2 – 4 mm in diameter, 20 secondary
branches Ductal pressure is 15 – 30 mm Hg (vs. 7 –
17 in CBD) thus preventing damage to panc. duct
Lesser duct (Santorini) drains superior portion of head and empties separately into 2nd portion of duodenum
Arterial Supply of Pancreas
Variety of major arterial sources (celiac, SMA and splenic)
Celiac Common Hepatic Artery Gastroduodenal Artery Superior pancreaticoduodenal artery which divides into anterior and posterior branches
SMA Inferior pancreaticoduodenal artery which divides into anterior and posterior branches

Arterial Supply of Pancreas
Anterior collateral arcade between anterosuperior and anteroinferior PDA
Posterior collateral arcade between posterosuperior and posteroinferior PDA
Body and tail supplied by splenic artery by about 10 branches
Three biggest branches are Dorsal pancreatic artery Pancreatica Magna (midportion of body) Caudal pancreatic artery (tail)
Pancreatic Arterial Supply

Venous Drainage of Pancreas
Follows arterial supply Anterior and posterior arcades drain
head and the body Splenic vein drains the body and tail Major drainage areas are
Suprapancreatic PV Retropancreatic PV Splenic vein Infrapancreatic SMV
Ultimately, into portal vein

Venous Drainage of the Pancreas
Lymphatic Drainage
Rich periacinar network that drain into 5 nodal groups Superior nodes Anterior nodes Inferior nodes Posterior PD nodes Splenic nodes

Innervation of Pancreas
Sympathetic fibers from the splanchnic nerves
Parasympathetic fibers from the vagus Both give rise to intrapancreatic
periacinar plexuses Parasympathetic fibers stimulate both
exocrine and endocrine secretion Sympathetic fibers have a
predominantly inhibitory effect

Innervation of Pancreas
Peptidergic neurons that secrete amines and peptides (somatostatin, vasoactive intestinal peptide, calcitonin gene-related peptide, and galanin
Rich afferent sensory fiber network Ganglionectomy or celiac ganglion
blockade interrupt these somatic fibers (pancreatic pain)
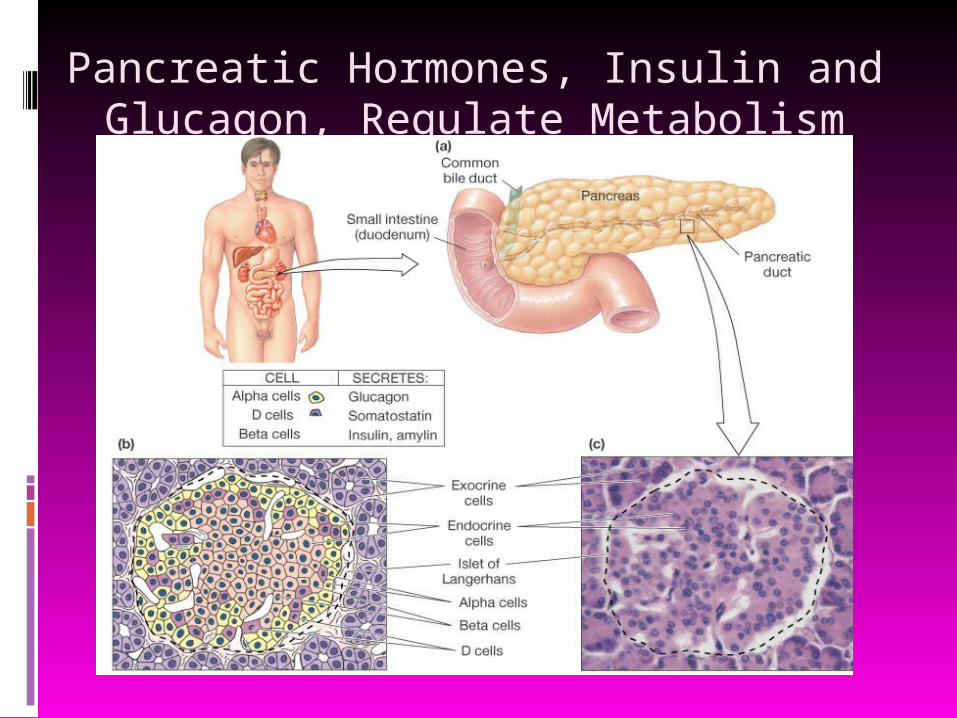
Pancreatic Hormones, Insulin and Glucagon, Regulate Metabolism

Production of Pancreatic Hormones by Three Cell Types
Alpha cells produce glucagon. Beta cells produce insulin. Delta cells produce somatostatin.

Islet of Langerhans Cross-section
Three cell types are present, A (glucagon secretion), B (Insulin secretion) and D (Somatostatin secretion)
A and D cells are located around the perimeter while B cells are located in the interior
Venous return containing insulin flows by the A cells on its way out of the islets

Pancreatic Hormones, Insulin and Glucagon, Regulate Metabolism
Figure 22-8: Metabolism is controlled by insulin and glucagon
Structure of Insulin
Insulin is a polypeptide hormone, composed of two chains (A and B)
BOTH chains are derived from proinsulin, a prohormone.
The two chains are joined by disulfide bonds.
Roles of Insulin Acts on tissues (especially liver, skeletal
muscle, adipose) to increase uptake of glucose and amino acids.
- without insulin, most tissues do not take in glucose and amino acids well (except brain).
Increases glycogen production (glucose storage) in the liver and muscle.
Stimulates lipid synthesis from free fatty acids and triglycerides in adipose tissue.
Also stimulates potassium uptake by cells (role in potassium homeostasis).

The Insulin Receptor
The insulin receptor is composed of two subunits, and has intrinsic tyrosine kinase activity.
Activation of the receptor results in a cascade of phosphorylation events:
phosphorylation ofinsulin responsive substrates (IRS) RAS
RAF-1
MAP-KMAP-KK Final
actions

Specific Targets of Insulin Action: Carbohydrates
Activation of glycogen synthetase. Converts glucose to glycogen.
Inhibition of phosphoenolpyruvate carboxykinase. Inhibits gluconeogenesis.
Increased activity of glucose transporters. Moves glucose into cells.

Specific Targets of Insulin Action: Lipids Activation of acetyl CoA carboxylase.
Stimulates production of free fatty acids from acetyl CoA.
Activation of lipoprotein lipase (increases breakdown of triacylglycerol in the circulation). Fatty acids are then taken up by adipocytes, and triacylglycerol is made and stored in the cell.
lipoproteinlipase

Regulation of Insulin Release Major stimulus: increased blood glucose
levels- after a meal, blood glucose increases
- in response to increased glucose, insulin is released
- insulin causes uptake of glucose into tissues, so blood glucose levels decrease.- insulin levels decline as blood glucose declines
Insulin Action on Cells: Dominates in Fed State Metabolism
glucose uptake in most cells(not active muscle)
glucose use and storage protein synthesis fat synthesis

Insulin Action on Cells: Dominates in Fed State Metabolism

Insulin: Summary and Control Reflex Loop

Other Factors Regulating Insulin Release Amino acids stimulate insulin release (increased
uptake into cells, increased protein synthesis). Keto acids stimulate insulin release (increased
glucose uptake to prevent lipid and protein utilization).
Insulin release is inhibited by stress-induced increase in adrenal epinephrine- epinephrine binds to alpha adrenergic receptors on beta cells
- maintains blood glucose levels Glucagon stimulates insulin secretion (glucagon
has opposite actions).

Structure and Actions of Glucagon Peptide hormone, 29 amino acids Acts on the liver to cause breakdown of
glycogen (glycogenolysis), releasing glucose into the bloodstream.
Inhibits glycolysis Increases production of glucose from amino
acids (gluconeogenesis). Also increases lipolysis, to free fatty acids for
metabolism. Result: maintenance of blood glucose levels
during fasting.

Mechanism of Action of Glucagon
Main target tissues: liver, muscle, and adipose tissue
Binds to a Gs-coupled receptor, resulting in increased cyclic AMP and increased PKA activity.
Also activates IP3 pathway (increasing Ca++)
Glucagon Action on Cells: Dominates in Fasting State Metabolism Glucagon prevents hypoglycemia by cell
production of glucose Liver is primary target to maintain blood
glucose levels

Glucagon Action on Cells: Dominates in Fasting State
Metabolism

Targets of Glucagon Action Activates a phosphorylase, which cleaves off a
glucose 1-phosphate molecule off of glycogen. Inactivates glycogen synthase by
phosphorylation (less glycogen synthesis). Increases phosphoenolpyruvate
carboxykinase, stimulating gluconeogenesis Activates lipases, breaking down triglycerides. Inhibits acetyl CoA carboxylase, decreasing
free fatty acid formation from acetyl CoA Result: more production of glucose and
substrates for metabolism
Regulation of Glucagon Release
Increased blood glucose levels inhibit glucagon release.
Amino acids stimulate glucagon release (high protein, low carbohydrate meal).
Stress: epinephrine acts on beta-adrenergic receptors on alpha cells, increasing glucagon release (increases availability of glucose for energy).
Insulin inhibits glucagon secretion.

Other Factors Regulating Glucose Homeostasis Glucocorticoids (cortisol): stimulate
gluconeogenesis and lipolysis, and increase breakdown of proteins.
Epinephrine/norepinephrine: stimulates glycogenolysis and lipolysis.
Growth hormone: stimulates glycogenolysis and lipolysis.
Note that these factors would complement the effects of glucagon, increasing blood glucose levels.
Hormonal Regulation of Nutrients
Right after a meal (resting):
- blood glucose elevated
- glucagon, cortisol, GH, epinephrine low
- insulin increases (due to increased glucose)
- Cells uptake glucose, amino acids.
- Glucose converted to glycogen, amino acids into protein, lipids stored as triacylglycerol.
- Blood glucose maintained at moderate levels.

A few hours after a meal (active):- blood glucose levels decrease- insulin secretion decreases- increased secretion of glucagon, cortisol, GH, epinephrine - glucose is released from glycogen stores (glycogenolysis)- increased lipolysis (beta oxidation)- glucose production from amino acids increases (oxidative deamination; gluconeogenesis)- decreased uptake of glucose by tissues- blood glucose levels maintained
Hormonal Regulation of Nutrients

Turnover Rate
Rate at which a molecule is broken down and resynthesized.
Average daily turnover for carbohydrates is 250 g/day. Some glucose is reused to form glycogen.
Only need about 150 g/day.
Average daily turnover for protein is 150 g/day. Some protein may be reused for protein synthesis.
Only need 35 g/day. 9 essential amino acids.
Average daily turnover for fats is 100 g/day. Little is actually required in the diet.
Fat can be produced from excess carbohydrates. Essential fatty acids:
Linoleic and linolenic acids.

Regulation of Energy Metabolism
Energy reserves: Molecules that
can be oxidized for energy are derived from storage molecules (glycogen, protein, and fat).
Circulating substrates: Molecules
absorbed through small intestine and carried to the cell for use in cell respiration.
Insert fig. 19.2

Pancreatic Islets (Islets of Langerhans)
Alpha cells secrete glucagon. Stimulus is decrease in
blood [glucose]. Stimulates glycogenolysis
and lipolysis. Stimulates conversion of
fatty acids to ketones. Beta cells secrete insulin.
Stimulus is increase in blood [glucose].
Promotes entry of glucose into cells.
Converts glucose to glycogen and fat.
Aids entry of amino acids into cells.VEDI
TRADUZIONE

Cellule alfa secernono glucagone.
Stimolo è Diminuzione del sangue [glucosio].
Stimola la lipolisi e glicogenolisi.
Stimola conversione degli acidi grassi a chetoni.
Le cellule beta secernono insulina.
Stimolo è Aumento nel sangue [glucosio].
Promuove l'ingresso del glucosio nelle cellule.
Converte il glucosio in glicogeno e grasso.
Aids ingresso di aminoacidi nelle cellule.
TRADUZIONE DIAPOSITIVA PRECEDENTE

Energy Regulation of Pancreas
Islets of Langerhans contain 3 distinct cell types: cells
Secreteglucagon. cells
Secreteinsulin. cells
Secrete somatostatin.

Regulation of Insulin and Glucagon Mainly regulated by blood [glucose]. Lesser effect: blood [amino acid].
Regulated by negative feedback. Glucose enters the brain by
facilitated diffusion. Normal fasting [glucose] is 65–105
mg/dl.

Regulation of Insulin and Glucagon (continued)
When blood [glucose] increases: Glucose binds to GLUT2 receptor protein
in cells, stimulating the production and release of insulin.
Insulin: Stimulates skeletal muscle cells and
adipocytes to incorporate GLUT4 (glucose facilitated diffusion carrier) into plasma membranes. Promotes anabolism.

Oral Glucose Tolerance Test
Measurement of the ability of cells to secrete insulin.
Ability of insulin to lower blood glucose.
Normal person’s rise in blood [glucose] after drinking solution is reversed to normal in 2 hrs.
Insert fig. 19.8
Regulation of Insulin and Glucagon Parasympathetic nervous system:
Stimulates insulin secretion. Sympathetic nervous system:
Stimulates glucagon secretion. GIP:
Stimulates insulin secretion. GLP-1:
Stimulates insulin secretion. CCK:
Stimulates insulin secretion.

Regulation of Insulin and Glucagon Secretion (continued)
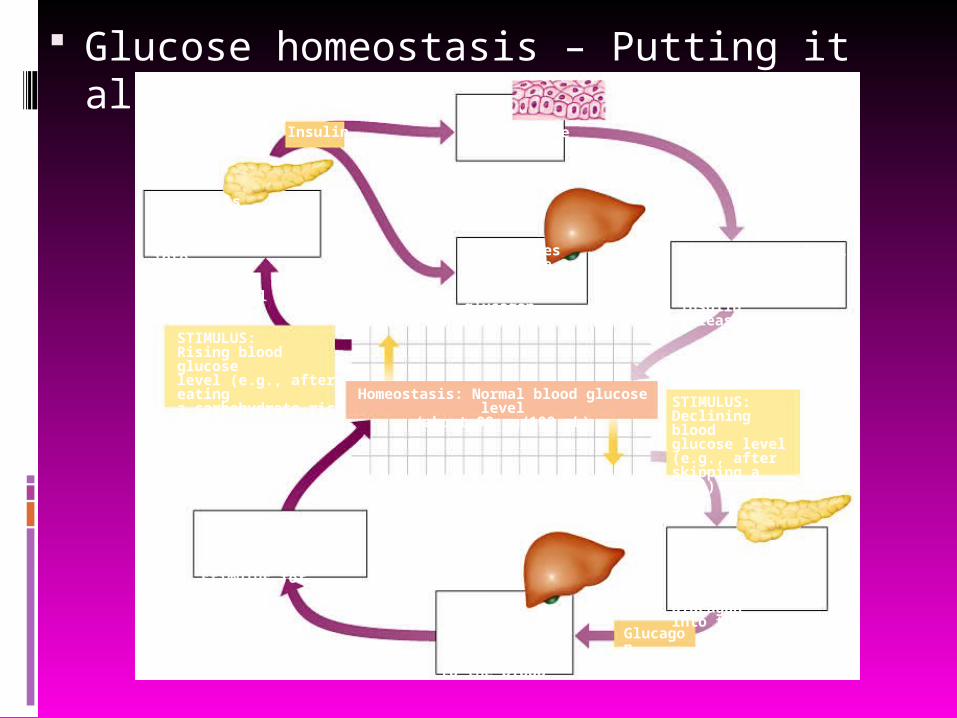
Glucose homeostasis – Putting it all together
Figure 26.8
Insulin
Beta cellsof pancreas stimulatedto release insulin intothe blood
Bodycellstake up moreglucose
Blood glucose leveldeclines to a set point;stimulus for insulinrelease diminishes
Liver takesup glucoseand stores it asglycogen
High bloodglucose level
STIMULUS:Rising blood glucoselevel (e.g., after eatinga carbohydrate-richmeal) Homeostasis: Normal blood glucose level
(about 90 mg/100 mL) STIMULUS:Declining bloodglucose level(e.g., afterskipping a meal)
Alphacells ofpancreas stimulatedto release glucagoninto the blood
Glucagon
Liverbreaks downglycogen and releases glucoseto the blood
Blood glucose levelrises to set point;stimulus for glucagonrelease diminishes
Hormonal Regulation of Metabolism Absorptive state:
Absorption of energy. 4 hour period after eating. Increase in insulin secretion.
Postabsorptive state: Fasting state. At least 4 hours after the meal. Increase in glucagon secretion.

Absorptive State
Insulin is the major hormone that promotes anabolism in the body.
When blood [insulin] increases: Promotes cellular uptake of glucose. Stimulates glycogen storage in the liver and
muscles. Stimulates triglyceride storage in adipose
cells. Promotes cellular uptake of amino acids and
synthesis of proteins.
Postabsorptive State
Maintains blood glucose concentration.
When blood [glucagon] increased: Stimulates glycogenolysis in the liver
(glucose-6-phosphatase). Stimulates gluconeogenesis. Skeletal muscle, heart, liver, and kidneys
use fatty acids as major source of fuel (hormone-sensitive lipase).
Stimulates lipolysis and ketogenesis.

Insert fig. 19.10
Effect of Feeding and Fasting on Metabolism

Diabetes Mellitus
Chronic high blood [glucose]. 2 forms of diabetes mellitus:
Type I: insulin dependent diabetes (IDDM).
Type II: non-insulin dependent diabetes (NIDDM).

Comparison of Type I and Type II Diabetes Mellitus
Insert table 19.6

Type I Diabetes Mellitus
cells of the islets of Langerhans are destroyed by autoimmune attack which may be provoked by environmental agent. Killer T cells target glutamate decarboxylase in
the cells. Glucose cannot enter the adipose cells.
Rate of fat synthesis lags behind the rate of lipolysis. Fatty acids converted to ketone bodies, producing
ketoacidosis. Increased blood [glucagon].
Stimulates glycogenolysis in liver.

Consequences of Uncorrected Deficiency in Type I Diabetes Mellitus

Type II Diabetes Mellitus
Slow to develop. Genetic factors are
significant. Occurs most often in
people who are overweight.
Decreased sensitivity to insulin or an insulin resistance. Obesity.
Do not usually develop ketoacidosis.
May have high blood [insulin] or normal [insulin].
Insert fig. 19.12
Treatment in Diabetes
Change in lifestyle: Increase exercise:
Increases the amount of membrane GLUT-4 carriers in the skeletal muscle cells.
Weight reduction. Increased fiber in diet. Reduce saturated fat. TRADUZIONE: Cambiare stile di vita: Aumentare esercizio: Aumenta la quantità di GLUT-4 vettori nelle cellule
del muscolo scheletrico a membrana. La riduzione del peso. L'aumento di fibre nella dieta. Ridurre i grassi saturi.

Hypoglycemia
Over secretion of insulin.
Reactive hypoglycemia: Caused by an
exaggerated response to a rise in blood glucose.
Occurs in people who are genetically predisposed to type II diabetes.
TRADUZIONE
Oltre la secrezione di insulina.
Ipoglicemia reattiva: Causato da una
risposta esagerata a un aumento del glucosio nel sangue.
Si verifica in persone che sono geneticamente predisposti al diabete di tipo II.
Insert fig. 19.13
Metabolic Regulation
Anabolic effects of insulin are antagonized by the hormones of the adrenals, thyroid, and anterior pituitary. Insulin, T3, and GH can act synergistically to
stimulate protein synthesis. TRADUZIONE
(Effetti anabolizzanti dell'insulina sono antagonizzati dagli ormoni della ghiandole surrenali, tiroide e dell'ipofisi anteriore.
L'insulina, T3 e GH può agire in sinergia per stimolare la sintesi proteica.)