pain management initial evaluation patient name ......8/9/19 jvogel, revised 2/10/20 relieving and...
TRANSCRIPT
8/9/19 jvogel, revised 2/10/20
PAIN MANAGEMENT INITIAL EVALUATION
Patient name: _______________________________
Date of Birth: ___________ Date: ______________
How long have you been having SEVERE problems with pain? _______________________
Was it the result of an injury or accident? _____ If so, what happened?
_____________________________________________________________________________
Where is your pain MOST SEVERE most of the time? ______________________________
Timing of Pain:
How often do you have your pain? (please check one)
[ ] Constantly/continuous. Present most of the time.
[ ] Intermittently. The pain comes and goes for periods of time.
Pain Quality:
How would you describe the pain? (choose as many adjectives as are applicable)
[ ] burning [ ] sharp [ ] cutting [ ] throbbing [ ] cramping [ ] numb
[ ] dull, aching [ ] pressure [ ] pins & needles [ ] shooting [ ] electric-like
Does the pain radiate anywhere? Where? ___________________________________________
_____________________________________________________________________________
Rate your Pain Intensity:
“0” = No pain “10” = worst pain imaginable
Circle the number below that best describes the WORST your pain level gets:
0_______1_______2_______3_______4_______5_______6_______7_______8_______9_______10
Circle the one number that best describes the BEST your pain level gets:
0_______1_______2_______3_______4_______5_______6_______7_______8_______9_______10

8/9/19 jvogel, revised 2/10/20
RELIEVING AND AGGRAVATING FACTORS
Activity Improves Pain Worsens Pain
Sitting
Standing
Walking
Driving
Bending
Turning
Twisting
Stretching
Looking up
Looking Down
Lying on back
Reclining
Laying on side
Support w/pillows
Ice application
Heat application
Changing position
Distraction
Relaxation/meditation
Doing something pleasant or fun
Resting
PREVIOUS PAIN TREATMENTS: Please check all of the treatments you have tried for your pain and then complete the appropriate column at the
right to the best of your ability.
Treatment Description Last time tried
Chiropractic
Physical Therapy
Biofeedback
Acupuncture
Dry Needling
Psychotherapy
Massage therapy
Ketamine infusion
Injections:
Joint
Spine
Radio Frequency Ablation
Trigger Point
Surgery: (list)
Other:
8/9/19 jvogel, revised 2/10/20
PREVIOUS DIAGNOSTIC STUDIES: Please indicate approximate date of most recent, if known:
MRI, CT scan, or X-rays:_______________________________________________________________________
EMG/NCV Studies:____________________________________________________________________________
MEDICATIONS: Check any medications you have EVER been on or are CURRENTLY taking:
NSAIDs Muscle Relaxant Adjuncts Short-Acting
Opiates
Long-Acting
Opiates
Migraine
Tylenol Flexeril
/cyclobenzaprine
Gabapentin
/Neurontin
Tramadol Tramadol ER Topamax
Ibuprofen Tizanidine
/Zanaflex
Lyrica Hydrocodone MS Contin Propranolol
Naproxen Baclofen amitriptylene Vicodin Morphabond Maxalt
Meloxicam Robaxin
/methocarbamol
Nortriptyline Norco Embeda Imitrex
/sumatriptan
Celebrex Norflex
/orphenadrine
Cymbalt
a/duloxetine
Percocet Avinza Amerge
Etodolac Skelaxin
/metalazone
Savella Oxycodone Oxycontin Zomig
Nabumetone soma Lidocaine Oxymorphone
/opana
XTampza ER Relpax
Diclofenac CBD Dilaudid Nucynta ER Amovig
Voltaren gel marijuana Hydromorphone Opana ER Emgality
Flector patch Gralise Nucynta
Exalgo ER Ajovy
toradol Horizant Codeine
Tylenol #3,#4
Fentanyl Botox
tegretol Levorphanol Butrans Fioricet
Subsys Belbuca
morphine Suboxone
methadone
Hysingla ER
Have you been given/prescribed a form of Narcan to use in case of emergency? ____Yes _____No

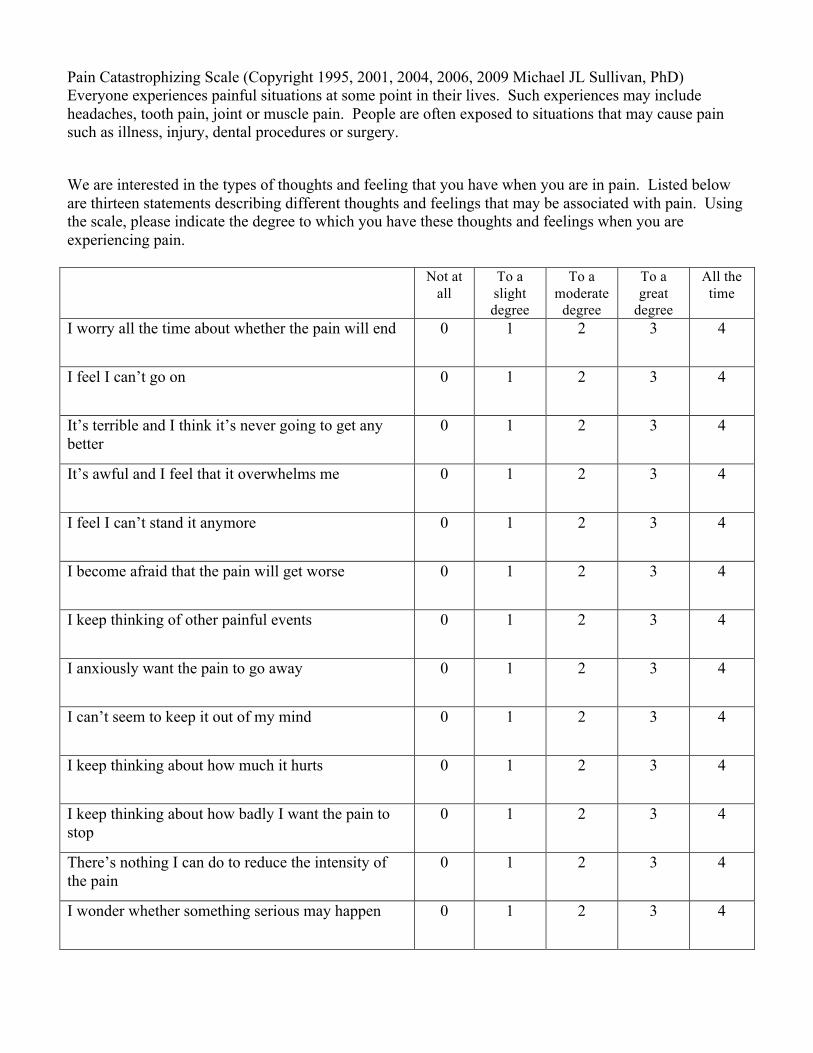
Pain Catastrophizing Scale (Copyright 1995, 2001, 2004, 2006, 2009 Michael JL Sullivan, PhD) Everyone experiences painful situations at some point in their lives. Such experiences may include headaches, tooth pain, joint or muscle pain. People are often exposed to situations that may cause pain such as illness, injury, dental procedures or surgery.
We are interested in the types of thoughts and feeling that you have when you are in pain. Listed below are thirteen statements describing different thoughts and feelings that may be associated with pain. Using the scale, please indicate the degree to which you have these thoughts and feelings when you are experiencing pain. Not at
all To a slight degree
To a moderate
degree
To a great
degree
All the time
I worry all the time about whether the pain will end 0 1 2 3 4
I feel I can’t go on 0 1 2 3 4
It’s terrible and I think it’s never going to get any better
0 1 2 3 4
It’s awful and I feel that it overwhelms me 0 1 2 3 4
I feel I can’t stand it anymore 0 1 2 3 4
I become afraid that the pain will get worse 0 1 2 3 4
I keep thinking of other painful events 0 1 2 3 4
I anxiously want the pain to go away 0 1 2 3 4
I can’t seem to keep it out of my mind 0 1 2 3 4
I keep thinking about how much it hurts 0 1 2 3 4
I keep thinking about how badly I want the pain to stop
0 1 2 3 4
There’s nothing I can do to reduce the intensity of the pain
0 1 2 3 4
I wonder whether something serious may happen 0 1 2 3 4

Matthews Vu Medical Group
PATIENT HEALTH QUESTIONNAIRE (PHQ-9) Name: Date:
Over the last 2 weeks, how often have you been bothered by any of the following problems? (Use "x" to indicate
your answer)
Not at all Several days More than Nearly
half the days every day
0 1 2 3
1) Little interest or pleasure in doing things 2) Feeling down, depressed, or hopeless
3) Trouble falling or staying asleep, or sleeping too
much 4) Feeling tired or having little energy 5) Poor appetite or overeating 6) Feeling bad about yourself or that you are a
failure, or have let yourself or your family down 7) Trouble concentrating on things, such as reading
the newspaper or watching television 8) Moving or speaking so slowly that other people
could have noticed; or the opposite, being so fidgety or restless that you have been moving around a lot more than usual
9) Thoughts that you would be better off dead or of hurting yourself in some way
Total Score:
Interpretation
Minimal Depression
Mild Depression
Moderate Depression
Moderately Severe Depression
Severe Depression
Interpretation of Total Score for Depression Severity 1-4 Minimal depression 5-9 Mild depression 10-14 Moderate depression 15-19 Moderately severe depression 20-27 Severe depression
Powered By eClinicalWorks LLC.
Jvogel2/10/20
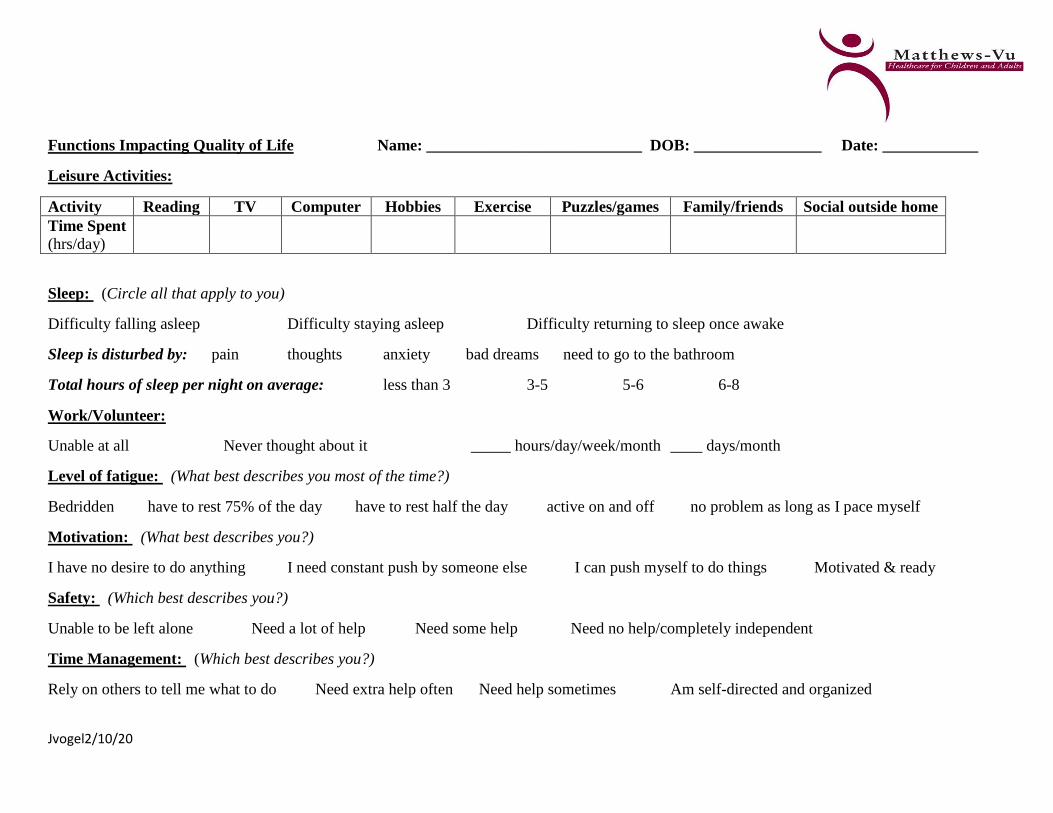
Functions Impacting Quality of Life Name: ___________________________ DOB: ________________ Date: ____________
Leisure Activities:
Activity Reading TV Computer Hobbies Exercise Puzzles/games Family/friends Social outside home
Time Spent
(hrs/day)
Sleep: (Circle all that apply to you)
Difficulty falling asleep Difficulty staying asleep Difficulty returning to sleep once awake
Sleep is disturbed by: pain thoughts anxiety bad dreams need to go to the bathroom
Total hours of sleep per night on average: less than 3 3-5 5-6 6-8
Work/Volunteer:
Unable at all Never thought about it _____ hours/day/week/month ____ days/month
Level of fatigue: (What best describes you most of the time?)
Bedridden have to rest 75% of the day have to rest half the day active on and off no problem as long as I pace myself
Motivation: (What best describes you?)
I have no desire to do anything I need constant push by someone else I can push myself to do things Motivated & ready
Safety: (Which best describes you?)
Unable to be left alone Need a lot of help Need some help Need no help/completely independent
Time Management: (Which best describes you?)
Rely on others to tell me what to do Need extra help often Need help sometimes Am self-directed and organized
Jvogel2/10/20
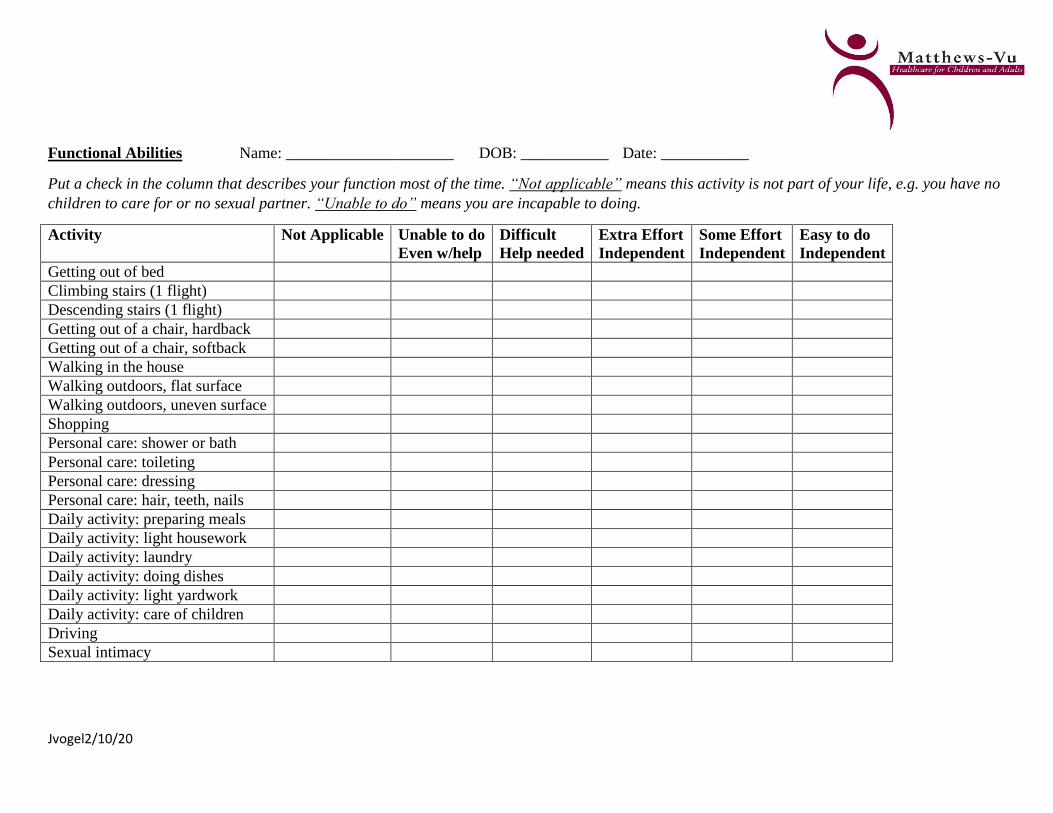
Functional Abilities Name: _____________________ DOB: ___________ Date: ___________
Put a check in the column that describes your function most of the time. “Not applicable” means this activity is not part of your life, e.g. you have no
children to care for or no sexual partner. “Unable to do” means you are incapable to doing.
Activity Not Applicable Unable to do
Even w/help
Difficult
Help needed
Extra Effort
Independent
Some Effort
Independent
Easy to do
Independent
Getting out of bed
Climbing stairs (1 flight)
Descending stairs (1 flight)
Getting out of a chair, hardback
Getting out of a chair, softback
Walking in the house
Walking outdoors, flat surface
Walking outdoors, uneven surface
Shopping
Personal care: shower or bath
Personal care: toileting
Personal care: dressing
Personal care: hair, teeth, nails
Daily activity: preparing meals
Daily activity: light housework
Daily activity: laundry
Daily activity: doing dishes
Daily activity: light yardwork
Daily activity: care of children
Driving
Sexual intimacy

Jvogel2/10/20
My Typical Day Name:________________________ DOB: _________________ Date: _____________
Please record your activities in a typical or average day—not your worst day or your best day.
Time of
Day
Description of Activity Amount of time in
activity
12AM
1
2
3
4
5
6
7
8
9
10
11
12 PM
1
2
3
4
5
6
7
8
9
10
11

8/6/19 jvogel revised 2/10/20
INTEGRATED PAIN CARE @ MATTHEWS-VU
NARCOTIC/OPIOD AGREEMENT
I, ____________________________, agree to the following expectations:
1. I understand that I am being prescribed strong medicine(s) and I have been informed of the common
side effects which I will promptly report to my prescribing provider if they occur.
2. I know I may become dependent or addicted to the medication(s). I agree to take the medicine(s)
exactly as prescribed and to not suddenly stop, increase, or decrease the medication without my
provider’s guidance due to possible life threatening withdrawal symptoms and/or overdose.
3. I have been instructed to avoid driving or operating machinery while taking the medication if it
makes me sleepy or dizzy.
4. I understand that the prescription will not be refilled early and I am responsible for properly taking
and safeguarding the medications. Any signs of misuse of the medication will be reason for the
prescriber to discontinue prescribing to me.
5. I agree that the medication(s) will be prescribed for no more than 30 days at a time by my prescriber
or one covering for him/her and at the time of my clinic/office appointment. Occasionally, an
exception may be made for patients whose insurance allows and demands use of mail order
pharmacy for 90 days prescriptions. Prescriptions will not be written outside of an office visit except
for compelling reasons documented in my medical record.
6. I agree to show up for my appointments at the office as scheduled. If I am late more than 15 minutes,
I will be asked to reschedule. If I cancel less than 24 hours in advance, it will be considered a “no-
show” and I may be charged a no-show fee for the missed visit. If I have more than 3 missed visits
within a six month period, I may be discharged from the program.
7. The treatment will be stopped immediately if I am found to be misusing the medication or using
other controlled substances, licit or illicit, not prescribed by my prescriber, including dentists,
emergency room providers, or surgeons unless authorized by my prescriber in advance.
8. No refills will be made on evenings, weekends, holidays, or by phone unless this has been planned in
advance with the provider.
9. I will use only the following pharmacy to fill all my prescriptions unless that pharmacy is unable to
fill the prescription in a timely manner or I contact my provider regarding a reason for change of
pharmacy:
Pharmacy name: _________________________________________________________________
City: ____________________________ Phone: ________________________________________

8/6/19 jvogel revised 2/10/20
10. I understand that lost, stolen, or damaged medications will not be replaced.
11. I agree not to sell, lend, or share my medications with any other person.
12. I agree to not use any illegal drugs and to use alcohol only in moderation.
13. I agree to submit to drug testing at any time requested.
14. I agree to participate in test, other treatments (exercise, physical therapy, behavioral therapy,
rehabilitation, etc.) or evaluations by other specialists as recommended by my provider and to
cooperate fully in my treatment plan for chronic pain.
15. I am not pregnant at this time and will avoid becoming pregnant while taking this medication as far
as I am able.
16. I agree that I am not currently using illegal drugs and have never been involved in the sale, illegal
possession, diversion, or transport of a controlled substance.
17. I understand I may use marijuana only if I have a license to use medical marijuana and am
responsible for renewing this license annually as long as I use any products containing THC or
cannabis including CBD with THC.
17. If any of the above rules and agreements are broken, my medication(s) may be stopped without
advance notice and I understand I may be discharged from the practice.
Patient Name: __________________________ Signature: _____________________ Date: ________
Provider: __________________________ Signature: _________________________ Date: ________
Witness: __________________________ Signature: _________________________ Date: _________