pain management- an integral aspect of wound care. glenn bruce. clinical nurse specialist for...
TRANSCRIPT


Pain Management- An integral aspect of Wound Care.Glenn Bruce. Clinical Nurse Specialist for in-patient pain management.
Taunton & Somerset NHS Trust.
http://www.gb42.com/Exeter.html

“Pain is what Sister says it is, and only exists when Sister says it does!”
What is pain?

“Pain is what Matron says it is, and only exists when Matron
says it does!”
What is pain?

The International Association for the Study of Pain. (1986)
'an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage'
What is pain?
Acute pain. Short duration. (<3 months)
A response to tissue damage. Pain decreases/resolves as tissues
heal. Responds well to ‘medical model’ Rx.
Pain, is pain,is pain, is pain,is pain….

Chronic pain.Pain, is pain,is pain, is pain,is pain….

Chronic persistent pain. Longer duration (>3 months)
Not always in response to tissue damage. Persists after tissue healing. Pain management, not pain relief may be
the goal. Multidimensional Responds to Bio-psychosocial model
Pain, is pain,is pain, is pain,is pain….

Nociceptive pain
A normal physiological response to tissue damage
Responds well to ‘traditional’ analgesics
Normally ‘time-limited’

Neuropathic pain Pain experienced as a result of injury to, or malfunction of, the nervous
system. May follow tissue damage. May be of unknown aetiology. Often responds poorly to ‘traditional’ analgesics. May respond to anti-depressants or anti-epileptic drugs (e.g. amitriptyline,
gabapentin, lyrica)

Mixed category pain

Leg Ulcers 83% of patients with arterial ulcers had pain (Lindholm
1999) 65% of patients with venous leg ulcers had pain (Ryan et
al 2003, Briggs and Nelson, Cochrane Review 2003).
Diabetic Foot Ulcers 48% patients reported pain (Ebbeskog et al 1996)
Pressure Ulcers 59% patients report pain (Dallum 1995), nearly half of
patients with Stage 3, 4 ulcers had pain (Lindholm 1999)
Fungating Wounds38% patients report pain (Naylor 2001)

What are the dangers of poor pain relief?
•Anxiety and insomnia
•Delayed healing
•Atelectasis and hypoxia
•Retained secretions and pneumonia
•Increased myocardial work
•Delayed gastric emptying
•Increased cortisol & reduced insulin secretion

What are the causes of poor pain relief?
•Poor pain assessment
•Poor analgesia choice
•Incorrect dose
•Wrong frequency
•Wrong mode of delivery
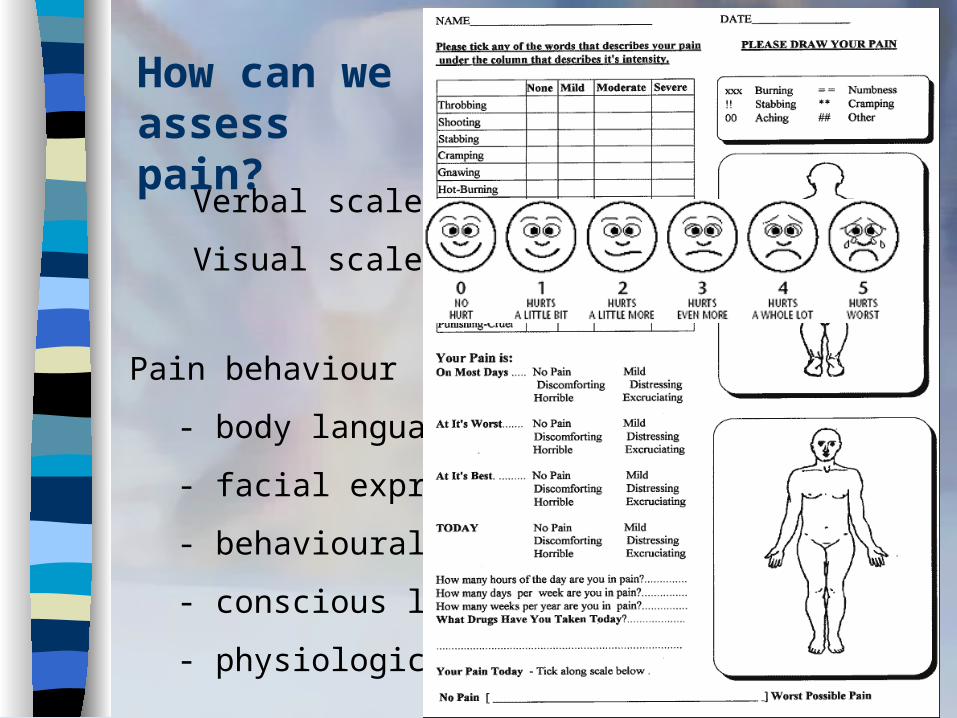
How can we assess pain?
Verbal scales
Visual scales
Pain behaviour
- body language
- facial expression
- behavioural changes
- conscious level
- physiological changes

•Inhalation
•Sublingual
•Oral
•Intramuscular
•Intravenous bolus/infusion/PCA
•Spinal or epidural
•Rectal
•Transdermal
•Topical
What routes of analgesia are there?

Opiates ‘Moderate’ analgesics: e.g.codeine,
tramadol ‘Mild’ analgesics: paracetamol NSAIDS Other drugs Non drug treatments.
What options are there for analgesia?

Where do we, as nurses come in?
Pain assessment. Record keeping. Pre-emptive analgesia administration. Explanations and reassurance. Distraction. Dressing technique & dressing choice.

Dressing technique & dressing choice. Traditional dressings, cleaning
solutions and tapes have been shown to damage healing tissue.
Dressings such as hydrocolloids, gels, alginates and foams are less traumatic for the patient.
But the best dressing may not be the one that causes least pain!
Local infiltration, anaesthetic gels, analgesic dressings.

Some points to ponder…..
Twenty of 39 participants reported
phantom sensations... Nine of the participants
with phantom sensations experienced
phantom pain and 11
non-painful phantom sensations.
(Rothemund 2004)
.When is pain present?
.Is neuropathic pain a factor?
.Aggravating factors
.Relieving factors
.Pain intensity
.Analgesia choice

Analgesia Choice Regular analgesia is more effective than PRN Pre-emptive analgesia is more effective than
reactive analgesia For nociceptive pain follow the W.H.O
analgesia ladder For neuropathic pain consider anti-
depressants or anti-epileptics. Be prepared to balance effects/side-effects.

The analgesia ladder

Percentage of patients achievingat least 50% pain relief over 4-6 hours in patients with
moderate to severe pain
Source: Evidence based health care©Bandolier: 10-Jun-2002

Neuropathic pain
Amitriptyline 10mg nocte Increasing by 10mg every third day in the absence of
effect/unacceptable side-effects up to a maximum of 100mg nocte.
Gabapentin 100mg T.D.S Increasing by 100-300mg every third day in the
absence of effect/unacceptable side-effects up to a typical maximum of 1800mg/day (3600mg absolute max.)

Pain Relief
Ask the following questions:
•Is effective analgesia prescribed?
•Is effective analgesia being given?
•Is the treatment safe and appropriate for the patient?
•Is it working?

Further reading:
Pain at wound dressing-related procedures: a template for assessment. (Hollingworth 2005)
www.worldwidewounds.com
The Best Practice statement on Pain & Trauma in wound management (Cooper et al. 2004)
www.tvna.org

Further reading:
The management of patients’ pain in wound care
(Hollingworth 2005)
www.nursing-standard.co.uk
Pain Talk (www.pain-talk.org.uk)
The national discussion forum and community for UK Healthcare Professionals with an interest in acute, chronic, or palliative Pain Management.

Further reading:Pain and quality of life for patients with venous leg ulcers: proof of concept of the efficacy of Biatain®-Ibu, a new pain reducing wound dressing
Authors: Jørgensen, Bo; Friis, Gitte Juel; Gottrup, FinnSource: Wound Repair and Regeneration,Volume 14, Number 3, May-June 2006 , pp. 233-239(7)Publisher: Blackwell Publishing


Pain Management- An integral aspect of Wound Care.
Clinical Nurse Specialist for in-patient pain management.
Taunton & Somerset NHS Trust.

http://www.gb42.com/Exeter.html
