pain & its pathways.dr ayesha taha
TRANSCRIPT
Presented by:
Dr.Ayesha Taha
JR I
Department of Pedodontics and
Preventive Dentistry
SPPGIDMS, Lucknow

INTRODUCTION
DEFINITIONS OF PAIN
TAXONOMY
CHARACTERISTIC OF PAIN
CLASSIFICATION
OROFACIAL PAIN
PAIN OF DENTAL ORIGIN.
ASSESSMENT OF PAIN
PAIN RECEPTORS
NEURAL PATHWAYS OF PAIN.
THEORIES OF PAIN
NEURAL PATHWAYS OF PAIN.◦ Neospinothalamic tract.◦ Paleospinothalamic tract.
DIAGNOSIS OF PAIN MANAGEMENT OF PAIN CONCLUSION

Pain is a sensory experience of special significance.
It is considered to be the fifth vital sign.
Pain is the commonest symptom which physicians
are called upon to treat.
It is a cardinal sign of inflammation.
Pain is an intensely subjective experience.
• But it has two features which are nearly universal.
First it is an unpleasant experience; and
Secondly it is evoked by a stimulus which is
actually or potentially damaging to living tissues.
• That is why, although it is unpleasant, pain serves a
protective function by making us aware of actual or
impending damage to the body.

The International Association for the Study of PainPain is "an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage”
[1979 by Harold Merskey]
“An unpleasant emotional experience usually initiated by noxious stimulus and transmitted over a specialized neural network to the CNS where it is interpreted as such.”
[C. Richard Bennett: Monheim’s Local Anesthesia and Pain control in dental practice, 7th edition, CBS Publishers & distributors, 1990]
Allodynia: Pain that occurs without noxious stimulus at the site
of pain.
Analgesia: Absence of sensibility to pain
Anesthesia: Absence of all sensation
Anesthesia dolorosa: Pain In an area that is anesthetic as a
result of differentiation
Arthralgia: Pain that is felt in the joint structures
Causalgia: A syndrome of unremitting burning pain as a result
of differentiation
Dyesthesia: An unpleasant abnormal sensation
Heterotopic pain: A general term to designate pain that is felt
in an area other than its true site of origin
Hypalgesia: Diminished sensitivity to stimulation-evoked pain
Hyperalgesia: Increased sensitivity to stimulation evoked pain
Hyperesthesia: Increased sensitivity to stimulation
Hypoesthesia: Diminished sensitivity to stimulation

1) Threshold and Intensity
• If the intensity of the stimulus is below the threshold (sub-
threshold) pain is not felt. As the intensity increases more
and more, pain is felt more and more according to the
Weber-Fechner’s law.
2) Adaptation – Pain receptors show no adaptation and so the
pain continues as long as receptors continue to be
stimulated.

3) Localization of pain - Pain sensation is somewhat poorly
localized. However superficial pain is comparatively better
localized than deep pain.
4) Influence of the rate of damage on intensity of pain
◦ If the rate of tissue injury (extent of damage per unit time)
is high, intensity of pain is also high.
(A)Based on speed of onset, quality & duration
(1)
Experimental
(2)
Transient
(3)
Acute
(4)
Chronic
Arthur C. Guyton, John E. Hall: Textbook of medical physiology, 11th edition, Elsevier, 2006.

1. Experimental:
noxious stimuli causes a mild uncomfortable or painful sensation .
2. Transient pain:
Short duration
Severe
Self limiting
3. Acute pathological pain :
Sharp, fast, pricking
Occurs very rapidly
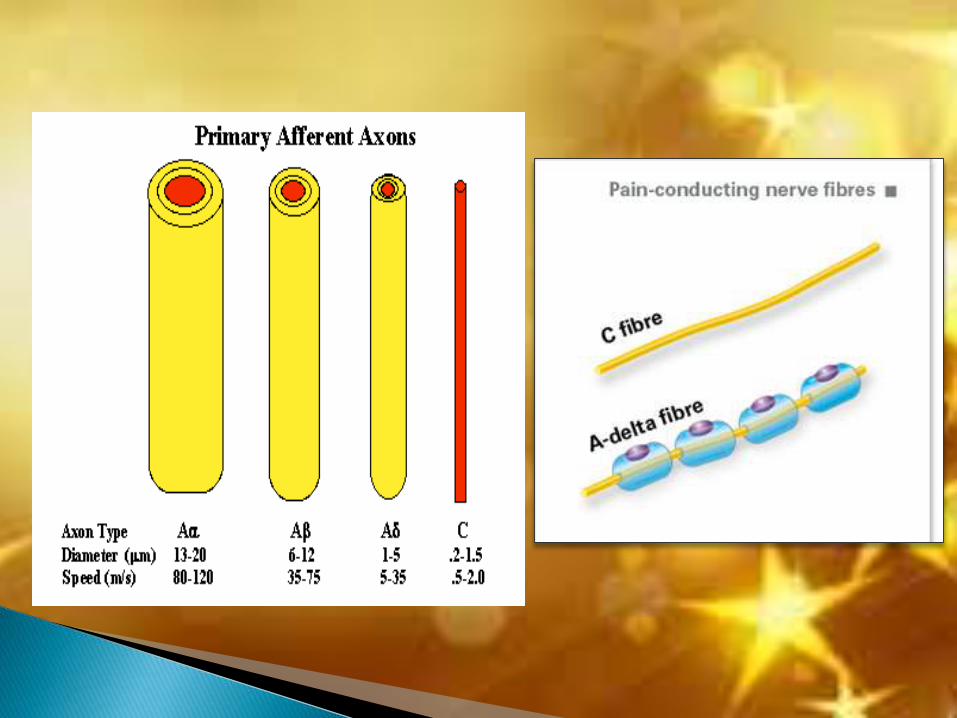
Carried by large diameter myelinated Aδ fibers
Usually alleviated with the help of professional

4. Chronological pathological pain :
Burning, aching.
Gradually increases.
Carried by small diameter non-myelinated C fibers.
Experience of persistent pain that lasts many months to years.
pain often increases over time & is aggravated by many factors.
(B)Based on level of stimulation
SOMATIC PAIN
Associated with skin
and musculo-skeletal
region.
Superficial Deep
VISCERAL PAIN
Associate with viscera
and
internal organs.
Carried by
unmyelinated type
C fibers.

(C)Based on special consideration
Referred pain Phantom pain

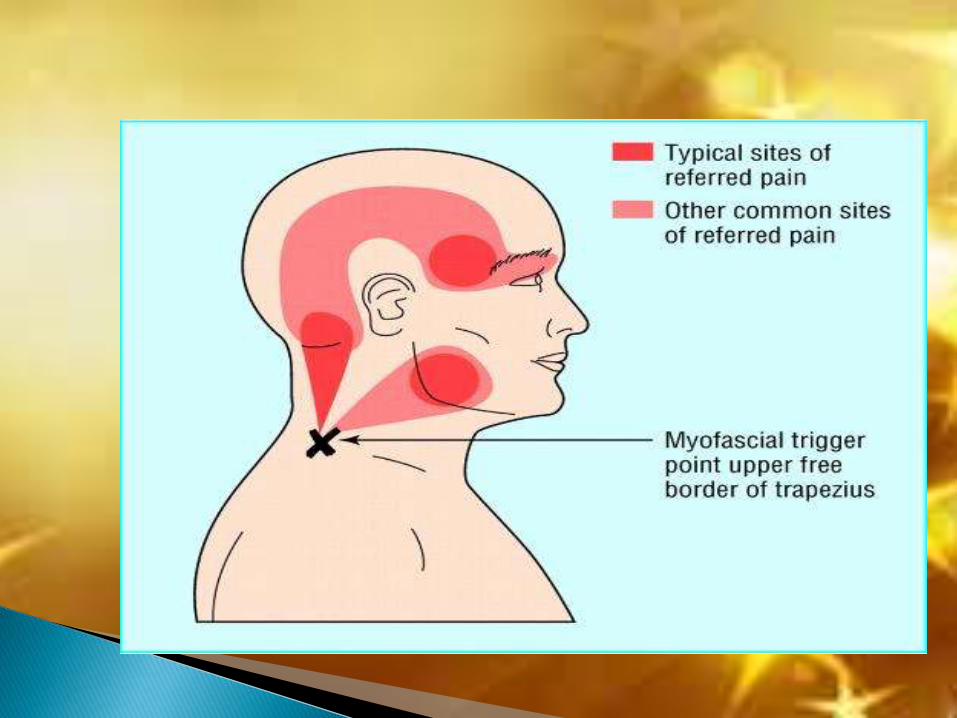
Pain occurring in a visceral structure is usually not felt in the
viscus itself but on the surface of the body or in some other
somatic structure that may be located quite some distance
away. Such type of pain is said to be Referred pain.
It is commonly observed visceral and somatic pain
e.g. the pain of angina pectoris is often felt in the left arm or
the jaw
diaphragmatic pain is often felt in the shoulder or neck.
Arthur C. Guyton, John E. Hall: Textbook of medical physiology, 11th edition, Elsevier, 2006.

It is not accentuated by provocation of the site where the
pain is felt, it is accentuated only by manipulation of the
primary pain source.
It is dependent on continuance of the primary initiating
pain, it ceases immediately if the primary pain is arrested or
interrupted.
Anesthesia of the structure where the referred pain is felt does not arrest the pain.


Individuals who have had a limb amputated may
experience pain or tingling sensations that feel as if they
were coming from the amputated limb, just as if that limb
were still present.
Although the mechanism of phantom limb pain is not
understood, the following possible explanations are
offered.
Arthur C. Guyton, John E. Hall: Textbook of medical physiology, 11th edition, Elsevier, 2006.
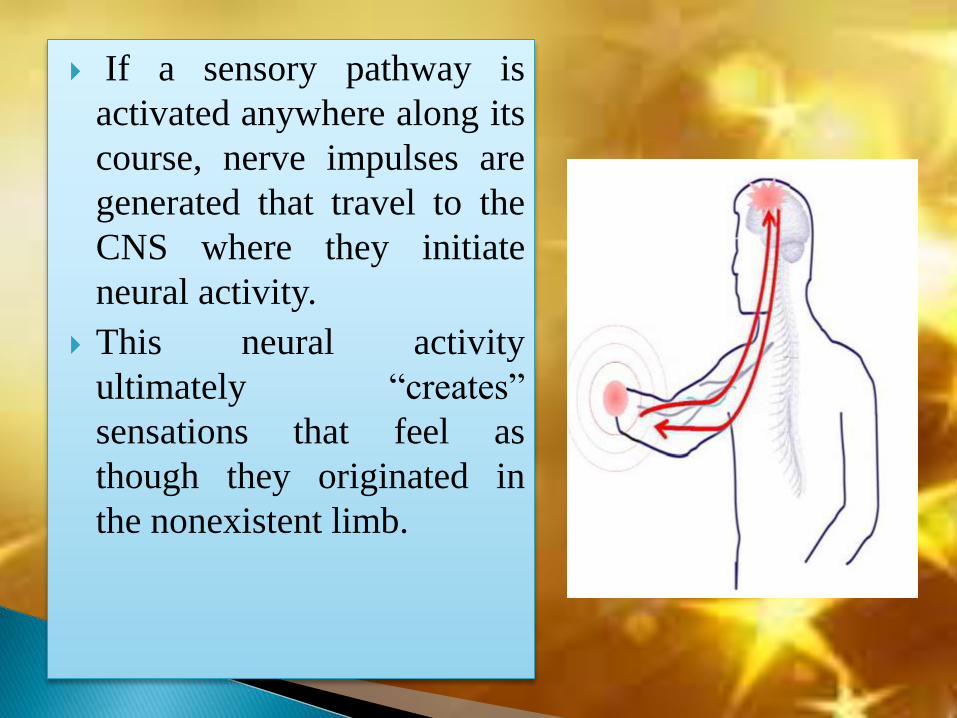
If a sensory pathway is
activated anywhere along its
course, nerve impulses are
generated that travel to the
CNS where they initiate
neural activity.
This neural activity
ultimately “creates”
sensations that feel as
though they originated in
the nonexistent limb.

CLASSIFICATION OF ORO FACIAL PAIN
A. PHYSICAL CONDITIONS
SOMATIC PAIN
NEUROPATHIC
PAIN
B. PSYCHOLOGIC CONDITIONS
1.MOOD DISORDERS
2. ANXIETY DISORDERS
3. SOMATOFORM DISORDERS
4. OTHER CONDITIONS

Type of pain
SLOW
Synonyms: burning pain, aching pain, throbbing pain, nauseous pain, and chronic pain.
Onset: >1 sec.
Tissues involved: Superficial + deep tissues
Cause: Tissue destruction
Results: Unbearable Suffering.
Nerve fibre: C fibre 0.5 – 1 µm, 0.5 – 2 m/s
FAST
Synonyms:sharp pain, pricking pain, acute pain, and electric pain.
Onset: Within 0.1 second.
Tissues involved: All superficial, and not in most of the deeper tissues.
Cause: Tissue damage.
Results: Protective reflex
Nerve fibre: Aδ: 1 – 5 µm, 5 – 15 m/s

ODONTOGENIC PAIN
Pain of Dental Origin
*Most common of all Oro facial pain
*Property to mimic nearly any pain
PULPAL PAIN
PERIODONTAL PAIN
FOOD IMPACTION
DENTINAL HYPERSINSITIVITY
CRACKED TOOTH
SYNDROME
BARODONTALGIA
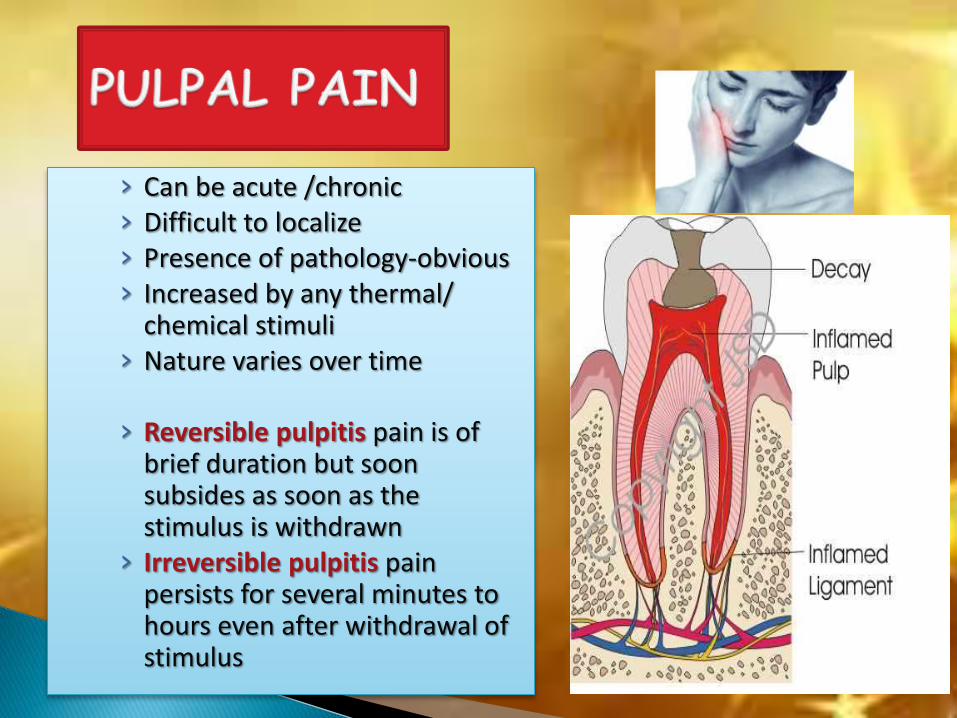
› Can be acute /chronic› Difficult to localize› Presence of pathology-obvious› Increased by any thermal/
chemical stimuli› Nature varies over time
› Reversible pulpitis pain is of brief duration but soon subsides as soon as the stimulus is withdrawn
› Irreversible pulpitis pain persists for several minutes to hours even after withdrawal of stimulus

PERIODONTAL PAIN› Can be dull aching› Inflammation along PDL› trauma from occlusion
FOOD IMPACTION› It is the forceful wedging of food into the
periodontium by occlusal forces› Causes dull gnawing type of pain› Cusps that tend to forcibly wedge food into
interproximal embrasures are known as Plunger cusps› Occurs due to open contacts or improper contours.

DENTINAL HYPERSINSITIVITY
› Sharp severe localized pain occurring due to cold, sweet food because of exposed dentine
› Pain lasts for few seconds & disappears after removing stimuli
› Exposure of dentine due to caries, fracture of tooth, attrition, erosion or abrasion, inadequate restorations in form of marginal leakage or improper base

CRACKED TOOTH SYNDROME› Pain on biting & releasing biting pressure
› Pain in particular occlusal position
BARODONTALGIA› Pain in tooth due to change in atmospheric pressure
› Change in the solubility of gases in blood
› Sea divers, decompression chambers
› & Mountaineers

Most pain assessments are done in the form of a scale. The scale is explained to the patient and they give a score. A rating is taken before administering any medication and after the specified time frame to rate the efficacy of treatment.
Number Scale
Patients rate pain on a scale from 0-10, 0 being no pain and 10 being the worst pain imaginable.
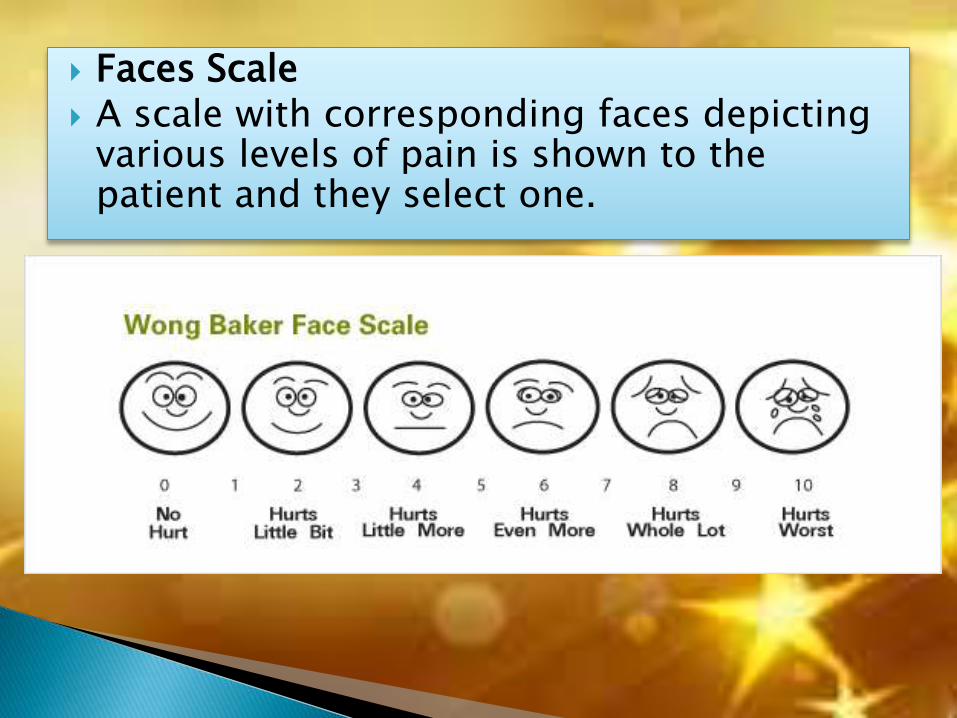
Faces Scale A scale with corresponding faces depicting
various levels of pain is shown to the patient and they select one.

FLACC SCALE
Used for neonates/infants or whom cannot verbalize / comprehend
Assessment 0 1 2
FaceSmiling/expressionless Frowning
Clenched jaw/Anguish
LegNormal movement/Relaxed Restless/Tense
Legs drawn up/Kicking
Activity None/Lying quietly Squirming/Tense movements
Arched back/Rigid/Jerking
Cry None Occasional whimper
Crying constantly/Screaming
Consolability RelaxedEasily distracted or reassured
Difficult to distract/reassure
Pain is termed Nociceptive (nocer – to injure or to hurt in Latin), and nociceptive means sensitive to noxious stimuli. Noxious stimuli activate nociceptors.
Nociceptors are sensory receptors that detect signals from damaged tissue or the threat of damage and indirectly also respond to chemicals released from the damaged tissue.
Nociceptors are free (bare) nerve endings found in the skin, muscle, joints, bone and viscera.
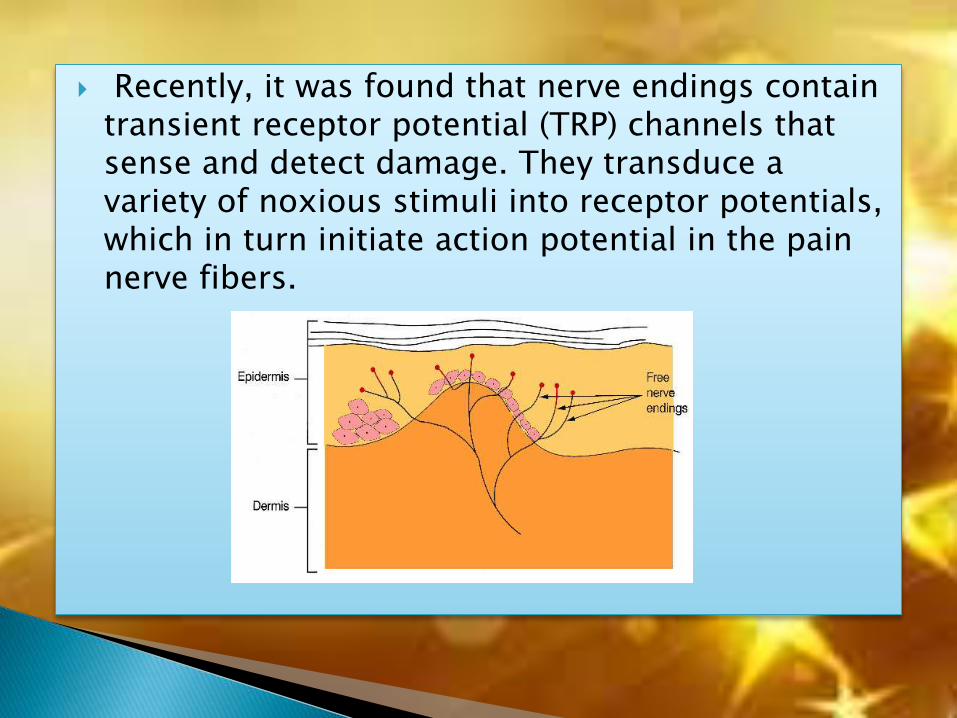
Recently, it was found that nerve endings contain transient receptor potential (TRP) channels that sense and detect damage. They transduce a variety of noxious stimuli into receptor potentials, which in turn initiate action potential in the pain nerve fibers.


The damage of tissue results in a release of a variety of
substances from lysed cells as well as from new substances
synthesized at the site of the injury.
Globulin and protein kinases
Arachidonic acid
Histamine
Nerve growth factor (NGF)
Substance P (SP) and calcitonin gene-related peptide
(CGRP)
Potassium - K+
Serotonin (5-HT), acetylcholine (ACh), low pH (acidic)
solution, and ATP

The nociceptive mechanism (prior to the perceptive event) consists of a multitude of events as follows:
Transduction:
This is the conversion of one form of energy to another. It
occurs at a variety of stages along the nociceptive pathway
from:
– Stimulus events to chemical tissue events.
– Chemical tissue and synaptic cleft events to
- Electrical events in neurones.
– Electrical events in neurones to chemical events at synapses.
Transmission:
Electrical events are transmitted along neuronal pathways,
while molecules in the synaptic cleft transmit information
from one cell surface to another.
Modulation:
The adjustment of events, by up- or down regulation. This can
occur at all levels of the nociceptive pathway, from tissue,
through primary (1°) afferent neuron and dorsal horn, to
higher brain centres.
Thus, the pain pathway as described by Descartes has had to
be adapted with time.

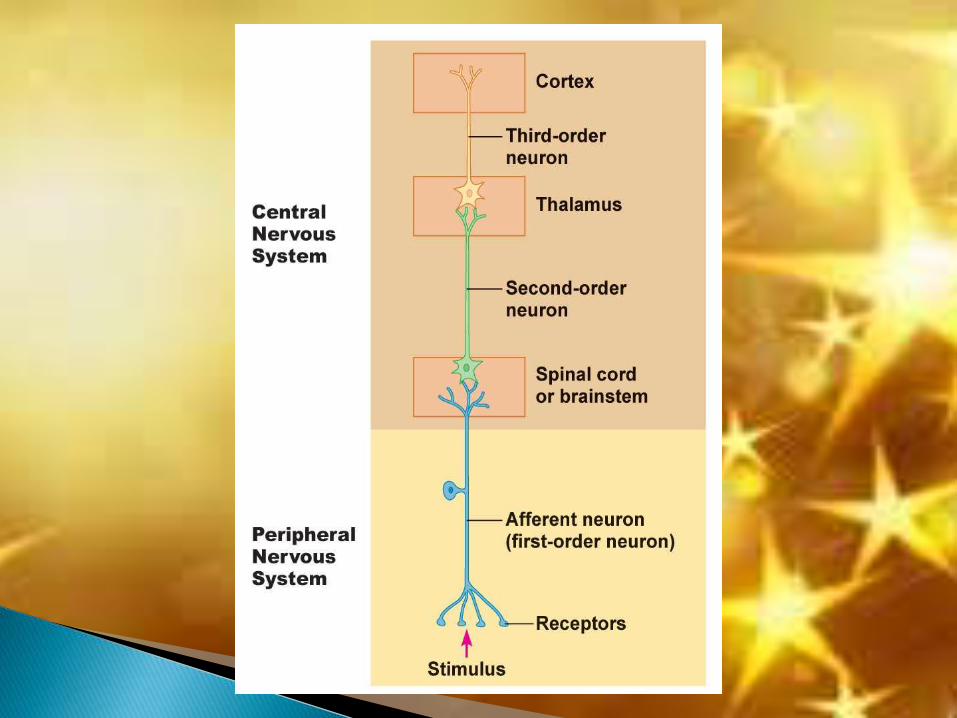
SENSORY NEURONS
First Order Second Order Third Order

Each sensory receptor is attached to a first order primary
afferent neuron that carries the impulses to the CNS.
The first order sensory neurons are in the dorsal root ganglia or
the sensory ganglia of cranial nerves.
The axons of these first-order neurons are found to have
varying thickness. It has long been known that a relationship
exists between the diameter of nerve fibers and their conduction
velocities. The larger fibers conduct impulses more rapidly than
smaller fibers.
40

Second Order Neuron
The primary afferent neuron carries impulse into the CNS
and synapses with the second-order neuron.
This second-order neuron is sometimes called a
transmission neuron since it transfers the impulse on to the
higher centers.
The synapse of the primary afferent and the second-order
neuron occurs in the dorsal horn of the spinal cord.
41

Third Order Neuron
Cell bodies of third order neurons of the nociception-
relaying pathway are housed in: the ventral posterior lateral,
the ventral posterior inferior, and the intralaminar thalamic
nuclei
Third order neuron fibers from the thalamus relay thermal sensory information to the somesthetic cortex.
42
It is often assumed that pain is a warning that damage
has occurred. But this is not strictly true.
So these are various theories being put forward on
how nerve impulses give rise to sensation of pain.

According to this view, pain is
produced when any sensory nerve is
stimulated beyond a certain level.
In other words pain is supposed to
be depended only on high intensity
stimulation.
But the Trigeminal system provides
an example against this theory. In
case of trigeminal neuralgia the
patient can suffer excruciating pain
from a stimulus no greater than a
gentle touch provided it is applied to
a trigger zone.
45
INTENSITY THEORY

• According to this view, pain is a specific modality equivalent to vision and hearing etc.
• Just as there are Meissner corpuscles for the sensation of touch,
• Ruffini end organs supposedly for warmth and
• Krause end organs supposedly for cold,
• so also pain is mediated by free nerve endings.
• But concept of specific nerve ending is no long tenable. The Krause and Ruffini endings are absent from the dermis of about all hairy skin, so it is certain that these structures cannot be receptors for cold and warmth.

Head and Rivers (1908) postulated the existence of two
cutaneous sensory nerves extending from the periphery to
the CNS.
The Protopathic system is primitive, yielding diffuse
impression of pain, including extremes of temperature and
is upgraded.
The Epicritic system is concerned with tough
discrimination and small changes in temperature and is phylogenetically a more recent acquisition.

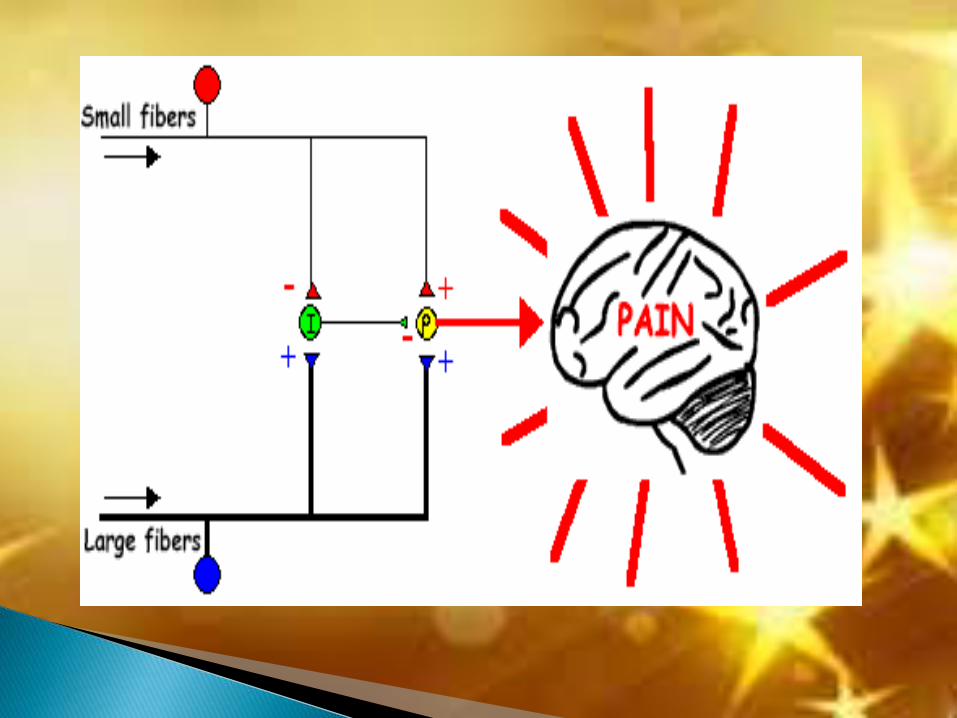
This theory proposed by Melzack and Wall in 1965.
This theory of pain takes into account the relative in put of
neural impulses along large and small fibers, the small nerve
fibers reach the dorsal horn of spinal cord and relay impulses
to further cells which transmit them to higher levels.
The large nerve fibers have collateral branches, which carry
impulses to substantia gelatinosa where they stimulate
secondary neurons.

The substantia gelatinosa cells terminate on the smaller nerve
fibers just as the latter are about to synapse, thus reducing
activity, the result is, ongoing activity is reduced or stopped –
gate is closed, NO PAIN
The theory also proposes that large diameter fiber input has
ability to modulate synaptic transmission of small diameter
fibers within the dorsal horn.
Large diameter fibers transmit signals that are initiated by
pressure, vibration and temperature; small diameter fibers
transmit painful sensations.
Activation of large fiber system inhibits small fiber synaptic
transmission, which closes the gate to central progression of
impulse carried by small fibers.
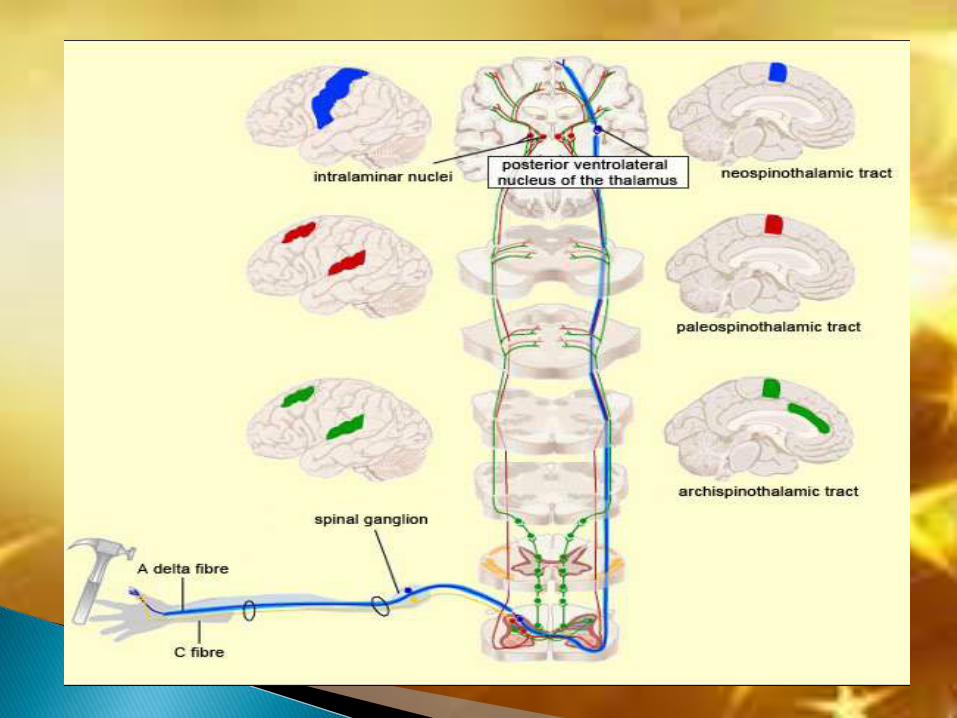
The ascending pathways that mediate pain consist of three
different tracts:
THE NEOSPINOTHALAMIC TRACT,
THE PALEOSPINOTHALAMIC TRACT AND
THE ARCHISPINOTHALAMIC TRACT.
Each pain tract originates in different spinal cord regions
and ascends to terminate in different areas in the CNS.
PATHWAYS OF PAIN IN THE SPINAL CORD AND BRAIN STEM :

The first-order nociceptive neurons (in the DRG) make synaptic connections in Rexed layer I neurons
Axons from layer I neurons decussate in the anterior white commissure, at approximately the same level they enter the cord
And then ascend in the contralateral anterolateral quadrant
Most of the pain fibers from the lower extremity and the body below
the neck terminate in the ventroposterolateral (VPL) nucleus and ventroposteroinferior (VPI) nucleus of the thalamus,
which serves as a relay station that sends the signals to the primary cortex.

First-order nociceptive neurons make synaptic connections in Rexed layer
II (substantia gelatinosa) and the second-order neurons make synaptic
connections in laminae IV-VIII
Most of their axons cross and ascend in the spinal cord primarily in the
anterior region and thus called the Anterior spinal thalamic tract (AST)
and few remain uncrossed.
The above three fiber tracts are known also as the paleospinothalamic tract.
These fibers contain several tracts. Each of them makes a synaptic connection in different locations
mesencephalic reticular formation (MFR)
periaqueductal gray (PAG) also called as spinoreticular tract
tectum, and these fibers are known as the spinotectal or spinomedullary tractthe PF-CM complex (IL) also known as the spinothalamic tract .
The innervation of these three tracts is bilateral because some of the ascending
fibers do not cross to the opposite side of the cord
From the PF and CM complex, these fibers synapse bilaterally in the
somatosensory cortex (SC II-Brodman area)


The archispinothalamic tract is a multisynaptic diffuse tract or pathway
and is phylogenetically the oldest tract that carries noxious information
The first-order nociceptive neurons make synaptic connections in Rexedlayer II (substantia gelatinosa) and ascend to laminae IV to VII
From lamina IV to VII, fibers ascend and descend in the spinal cord via the
multisynaptic propriospinal pathway surrounding the grey matter to synapse with cells in the MRF-PAG area
Further multisynaptic diffuse pathways ascend to the intralaminar (IL) areas of the thalamus (i.e., PF-CM complex)
and also send collaterals to the hypothalamus and to the limbic system nuclei
These fibers mediate visceral, emotional and autonomic reactions to pain


Three major steps:
◦ Accurately identifying the location of the structure from which the pain emanates
◦ Establishing the correct pain category the is represented in the condition under investigation
◦ Choosing the particular pain disorder that correctly accounts for the incidence and behavior of the patient’s pain problem

I. The chief complaint
•A) location of pain
•B) onset of pain
•C) characteristics of pain
•D) aggravating and alleviating factors
•E) past consultation and/or other treatments
•F) relationship to other complaints
Ii. Past medical history
Iii. Review of systems
Iv. Psychological assessment

Pain sensations may be controlled by interrupting the pain
impulse between receptor and interpretation centers of brain.
This may be done :
1. Chemically
2. Surgically
Most pain sensations respond to pain reducing
drugs/analgesics which in general act to inhibit nerve impulse
conduction at synapses.
Occasionally however, pain may be controlled only by
surgery.

MANAGEMENT OF PAIN:
Pain perception control
1.Removing the cause
2. Blocking the path way
of painful impulses, Ex: GA/LA
3.Analgesics
- non narcotics
- narcotics
- NSAID`s
- muscle relaxants
- antidepressants etc.
Pain reaction control
1.Preventing pain
reaction
by cortical depression.
2.Using psychosomatic
methods.
Ex: Conscious sedation.
Behavior management
Raising the level of pain threshold

The purpose of surgical treatment is to interrupt the pain
impulse somewhere between receptors and innervations
centers of brain, by severing the sensory nerve, its spinal root
or certain tracts in spinal cord or brain.
Sympathectomy – excision of portion of neural tissue from
autonomic nervous system.
Cordotomy – severing of spinal cord tract, usually the lateral
spinothalamic.
Rhizotomy – cutting of sensory nerve roots.
Prefrontal lobotomy – destruction of tracts that connect the
thalamus with prefrontal and frontal lobes of cerebral cortex.

Transcutaneous Neural Stimulation (TNS)
With TNS, cutaneous bipolar surface electrodes are
placed in the painful body regions and low voltage
electric currents are passed.
Best results have been obtained when intense stimulation
is maintained for at least an hour daily for more than 3
weeks.
TNS portable units are in wider spread use in pain clinics
throughout the world and has been proved effective
against neuropathic pain.

• Pain is bad, but not feeling pain can be worse.
• Individuals with a congenital absence of pain receptors are extremely rare but not unknown. Such individuals are very poor at avoiding accidental injuries, and often inflict mutilating injuries on themselves.
• As a result, their life span is usually short. thus pain, although unpleasant, is a protective sensation with enormous survival value.
• The sensation of pain therefore depends in part on the patient past experience, personality and level of anxiety.
• Every day patient seeks care for the reduction or elimination of
pain.
• Nothing is more satisfying to the clinician than the successful
elimination of pain.
• The most important part of managing pain is understanding
the problem and cause of pain.
• It is only through proper diagnosis that appropriate therapy
can be selected.

Arthur C. Guyton, John E. Hall: Textbook of medical physiology, 11th
edition, Elsevier, 2006. C. Richard Bennett: Monheim’s Local Anesthesia and Pain control in
dental practice, 7th edition, CBS Publishers & distributors, 1990 Allan I. Basbaum, Diana M. Bautista, Grégory Scherrer, and David
Julius: Cellular and Molecular Mechanisms of Pain, Cell 139, October16, 2009, 267 -284.
Jeffrey P. Okeson: Bell’s Orofacial Pains The Clinical Management ofOrofacial Pain, 6th edition, Quintessence Publishing Co, Inc, 2005.
Bell’s Orofacial Pain. Fifth edition. Jeffrey P. Okeson Handbook of Pain Management. A clinical companion to Wall and
Melzack’s textbook of pain Mangement of Facial, Head and Neck Pain. Barry C. Cooper. Frank E.
Lucente Monheim’s Local Anesthesia and Pain control in Dental Practise. C.
Richard Bennett Diagnosis & management of facial pain- OMFS clinics of North
America– may 2000
