pain assessment and management in critically ill adultspain assessment and management in critically...
TRANSCRIPT

Pain Assessment and Management in Critically
Louise RoseLawrence S. Bloomberg Professor in Critical Care Nursing, University of Toronto
Adjunct Scientist, Mt Sinai Hospital and Li Ka Shing Institute, St Michael’s HospitalDirector of Research, Provincial Centre of Weaning Excellence, Toronto East General Hospital

BEHAVIOURAL PAIN ASSESSMENT TOOLS

Pain Behaviour Assessment Tool (Puntillo)
Behaviour Pain Score (Payen)
Adult Nonverbal Pain Scale (Odhner) Checklist of Non-Verbal Pain Indicators (Feldt)

Critical-Care Pain Observation Tool

Uni-dimensional�Use single or several domains e.g. behaviour
Multi-dimensional �e.g. behaviour and physiologic signs
Indicate pain presence NOT severity BPS (Payen) and CPOT (Gelinas) valid and reliable Some issues with existing tools�ambiguity of items�lack of specificity for pain�need for further psychometric testing

Patients must be able to exhibit all behaviours�no limb movement will under represent pain
Various scales use different total scores and cutoffs�misinterpretation and confusion
Numeric scale too similar to NRS �which describes pain intensity as well as identifies pain
presence
Available Tools: Cautions

PAIN ASSESSMENT


3711 observation hours
=1213 pain assessment intervals
Total 377 pain assessments
= 223 intervals with pain assessments
Pain assessment in 10.2% of hours
= 18.4% of mandated painassessments documented

PAIs: Behavioural descriptors(N = 679)

PAIs: Behavioural descriptors(N = 679)

3442 surveys sent1251 ON
1251 AB, QC, BC1251 all other
842 surveys receivedResponse rate 24.5%
YT 33%, QC 32%, AB 26%, MB 24%NS 23%, SK 22%, BC 19%, ON 18%,
NF 18%, NB 17%, PEI 17%, NWT/Nu 3%
802 evaluable surveys

Frequent assessment and documentation of pain considered equally important for patients able and unable to communicate (94% vs 94%)
Less likely to use behavioural pain assessment tool compared to self-report tool (33% vs 89% P <0.001)
Behavioural pain assessment tools considered less important in guiding pain assessment compared to self-report tools
(74% vs 88% P <0.001)
61.3% reported pain scores discussed often or routinely during nurse-to-nurse handover
41.5% nurses described targeting of analgesic administration (pain score/other assessment parameters) as prescribed by Drs

Most likely suggestive of pain Least likely suggestive of pain

Use of a behavioural pain tool > 50% of the time was associated with:
awareness of published guidelines odds ratio 2.5 (95% CI 1.7-3.7)
tool availability in the clinical setting OR 2.6 (95% CI 1.6-4.3)
No association with education on pain tools, availability of a protocol, ICU experience, hospital type or province

Knowledge of published guidelines 29% had read any published guidelines or practice
recommendations for pain assessment and management
8% familiar with SCCM Sedation and Analgesia Guidelines (2002)
8% familiar with American Society of Pain Management Nursing (ASPMN) Recommendations (2006)
22% familiar with Registered Nurses Association of Ontario Best Practice Guidelines on pain (2007)

Nurses were less likely to use a behavioural pain assessment tool for patients unable to communicate, rated them less important, and had low awareness of practice recommendations
Suggests inadequate uptake of evidence and practice recommendations for pain assessment and management of critically ill patients, particularly for those unable to communicate pain
Low penetration of practice recommendations may impact availability of pain assessment tools, practice norms and patient outcomes at the local level
Need for novel knowledge-translation interventions to improve routine pain assessment and management practices

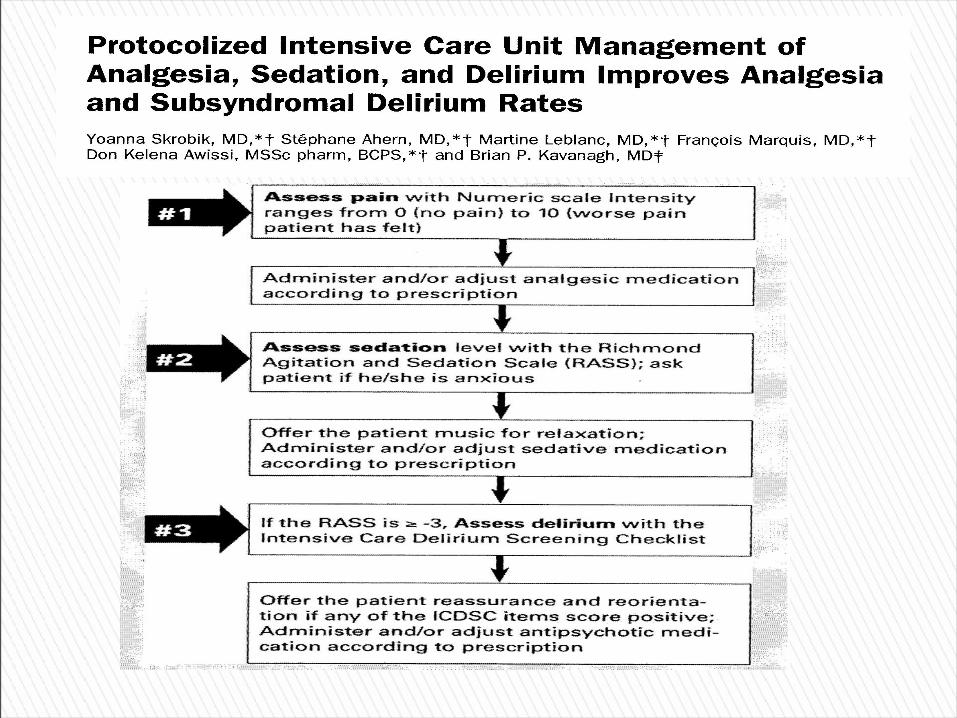
LINKING PAIN ASSESSMENT TO MANAGEMENT

Nurse satisfaction

Nurse satisfaction
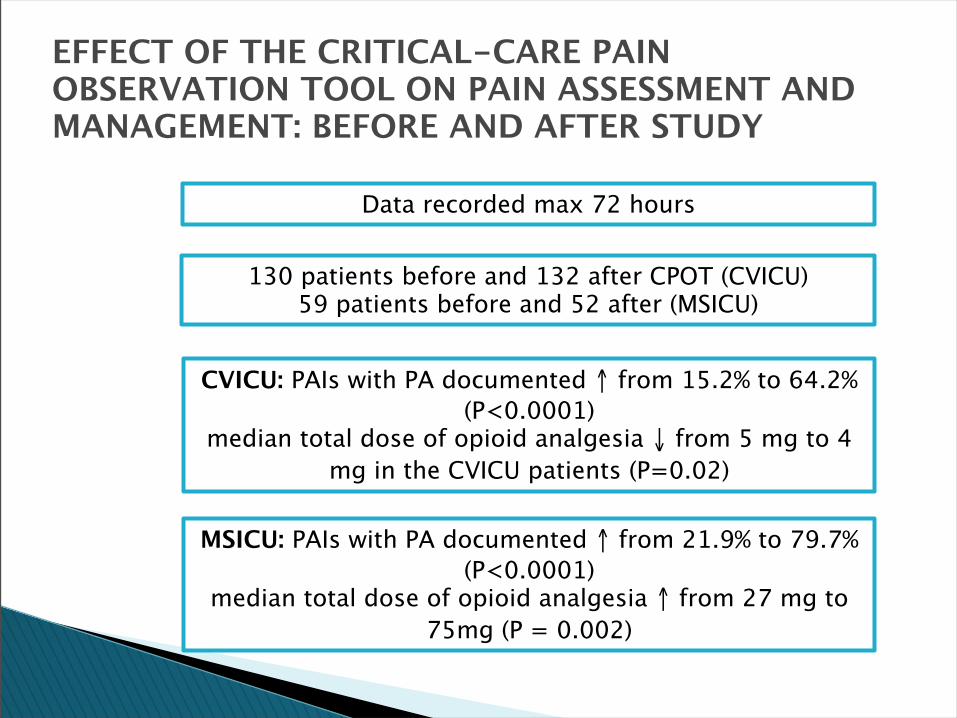
EFFECT OF THE CRITICAL-CARE PAIN OBSERVATION TOOL ON PAIN ASSESSMENT AND MANAGEMENT: BEFORE AND AFTER STUDY
Data recorded max 72 hours
CVICU: PAIs with PA documented ↑ from 15.2% to 64.2% (P<0.0001)
median total dose of opioid analgesia ↓ from 5 mg to 4 mg in the CVICU patients (P=0.02)
MSICU: PAIs with PA documented ↑ from 21.9% to 79.7% (P<0.0001)
median total dose of opioid analgesia ↑ from 27 mg to 75mg (P = 0.002)
130 patients before and 132 after CPOT (CVICU)59 patients before and 52 after (MSICU)








All health professionals should advocate for effective pain control
Ongoing assessment using a systematic approach is essential
Presume pain is present when patients unable to self-report
Early recognition and control = easier to prevent pain escalation
Start analgesia prior to or with sedation that has little to no analgesic effect
Basic Tenets of Pain Management
ERSTAD et al. Chest 135(4) 2009

405 symptom assessments in 171 pts

405 symptom assessments in 171 pts

405 symptom assessments in 171 pts
