page2/2hus.moh.gov.my/bm/wp-content/uploads/2018/09/6aug2018-sgh-tbic... · 1994. [akta keselamatan...
TRANSCRIPT

44
Page2/2
45
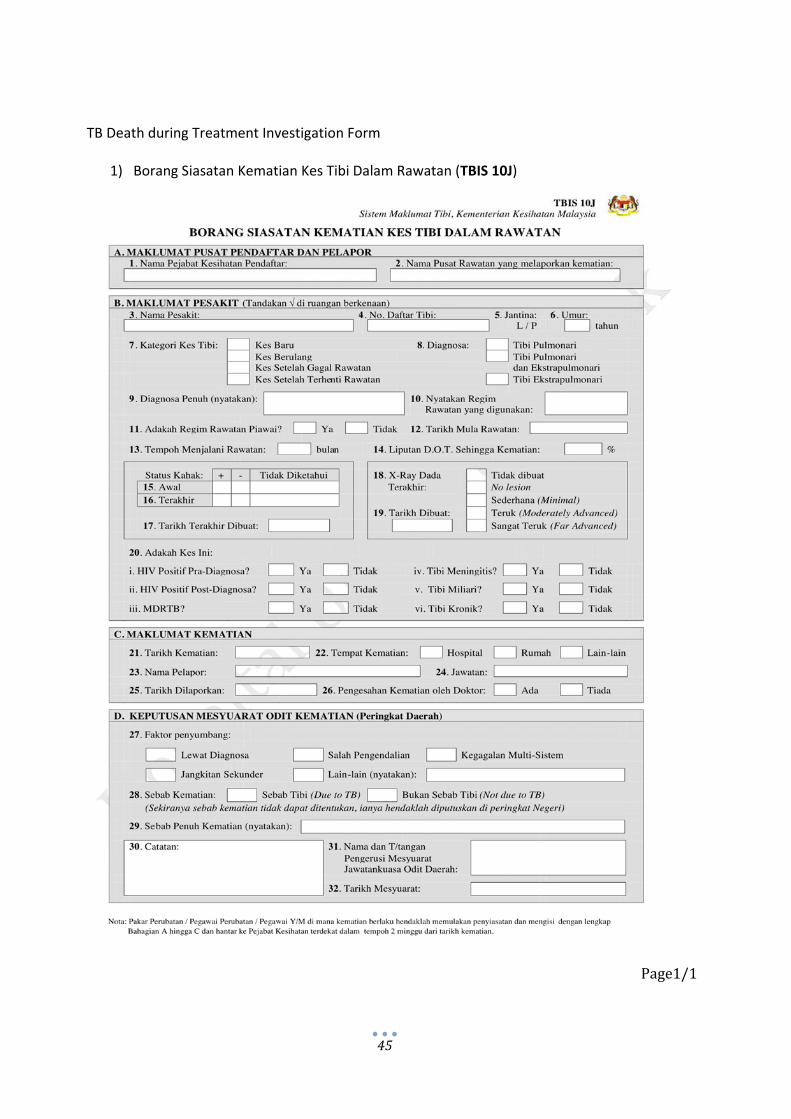
TB Death during Treatment Investigation Form
1) Borang Siasatan Kematian Kes Tibi Dalam Rawatan (TBIS 10J)
Page1/1
46

47
14. IN‐HOSPITAL ACTION PLAN FOR DELAYED DETECTION OF SMEAR‐POSITIVE TB IN GENERAL WARDS
14.1.1All patients suspectedof infectiousTB should be isolated. In the event ofmissedordelayeddiagnosisofsmear‐positiveTB,whereinisolationandotherairborneinfectioncontrolmeasureshadnotbeeninplace,transmissionriskinthegeneralwardsishigh.
14.1.2 Upondiagnosis,UKAshouldbenotifiedverballyimmediately.14.1.3 ImmediateinvestigationshouldbecarriedoutbyTBICTaskForcewiththe
assistanceoftheaffectedWardSisterandHeadofUnit,todetermineexposurerisk,andscopeofcontactscreen.
14.1.4Closecontacts,egattendingnurses,especiallyifhavingperformedmultiple
aerosolizingprocedures,egendotracheal/ tracheostomysuctioning, shouldbescreenedwithin2weeksofidentification.Screeningshouldbeinclusiveofsymptom,MantouxaswellasCXRscreening,andfollowedup8weeksafterlastexposure,andthen8monthlyfor2years.
14.1.5ExpandedcontactscreenbyMantouxtestforotherasymptomaticHCWin
theunitwillbeperformedafteran8weekswindowperiod.(SeeSection12,page22,SGHHCWContactScreeningWorkFlowfordetails)
14.1.6 The scope of contact screen for other in‐patients and carers will be
determinedbyTBICTaskForcewiththehelpofTBCPKuching,dependingonthepatientcharacteristics,proximityanddurationofexposure.
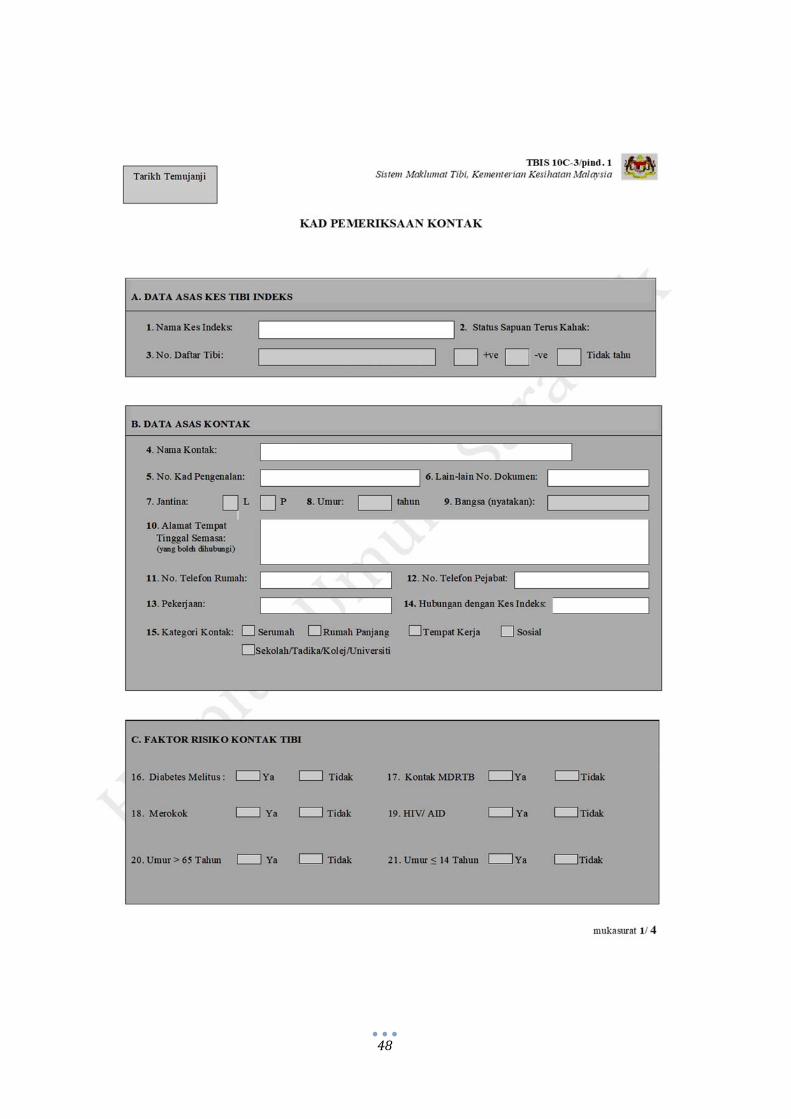
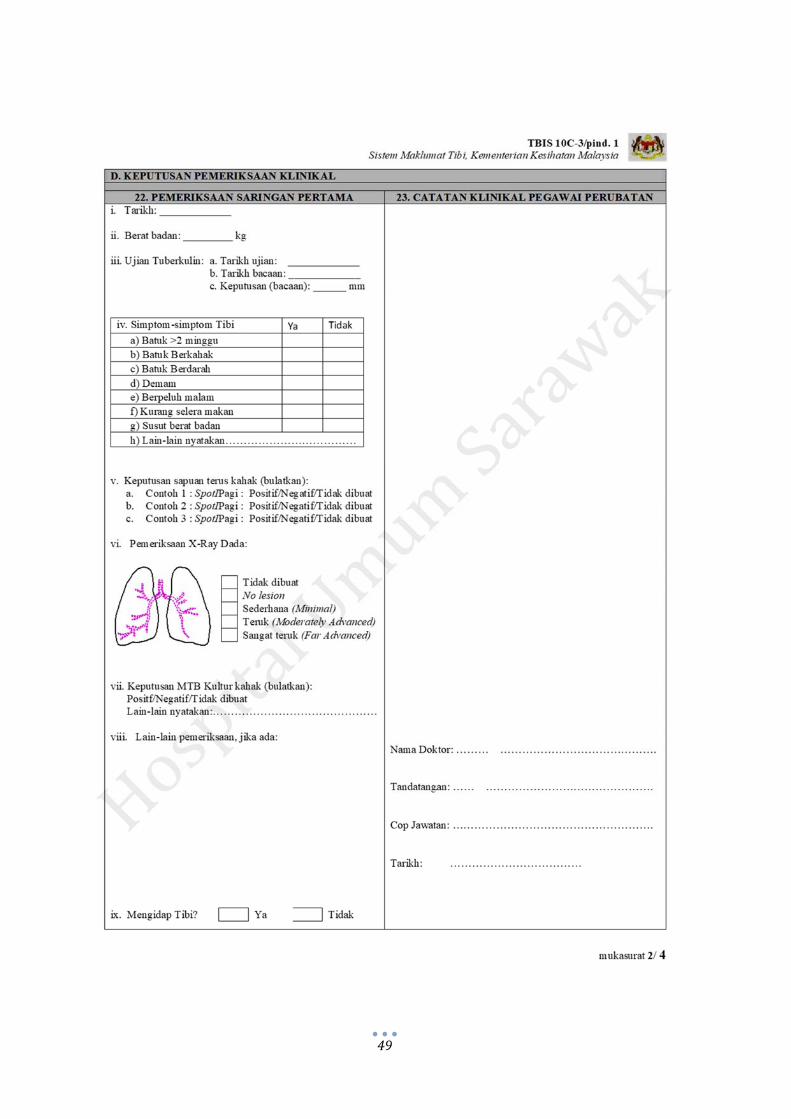
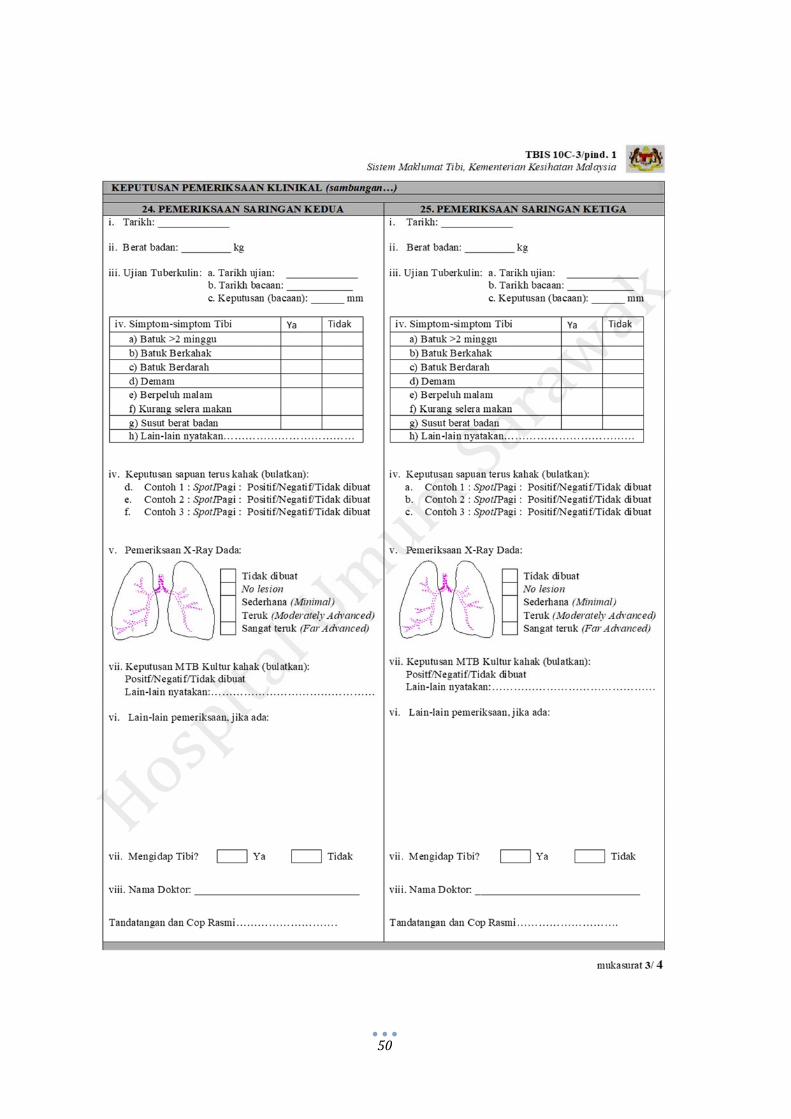
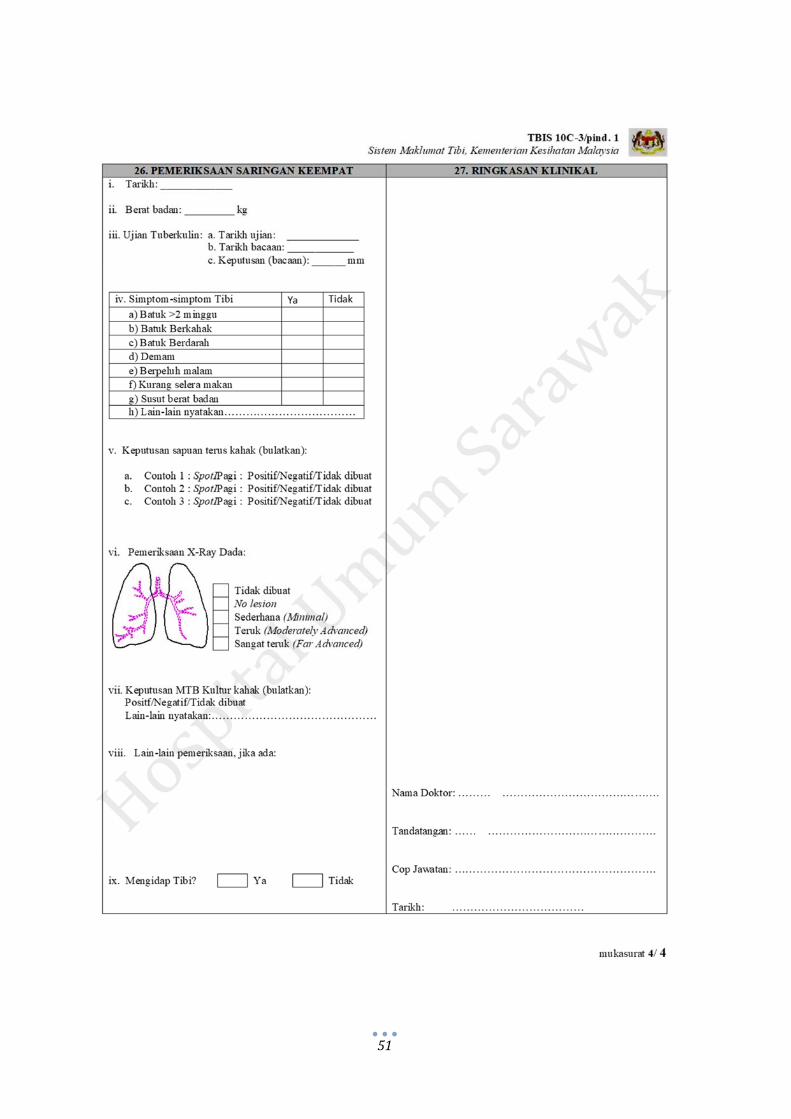
14.1.7TheTBIS10C‐3/pin.1“KadPemeriksaanKontak”willbefilledupbyPPKP,
and handed over to TBCP for contact screening follow‐up of significantlyexposedpatients,andhandedovertoStaffClinic/OHUforcontactscreeningfollow‐upofHCWs.
48
49
50
51
52
15. HEALTH CARE WORKERS AND TB
15.1 Introduction
Healthcare workers (HCWs) are exposed to patients with TB and are at risk of nosocomial
infection. Failure to use personal protection was associated with an almost 3 fold increased risk
of TB among HCWs.
A cost‐effectiveness study among HCWs at different risk of TB exposure showed that regular
tuberculin screening among them is cost‐effective and results in a net cost‐savings. The National
Institute for Health and Care Excellence (NICE), UK recommends reminders of TB symptoms,
and prompt reporting of such symptoms should be included with annual reminders about
occupational health for staff who are at high risk of TB contact.
15.2 Investigation of TB in Health Care Workers 15.2.1 AllHCWsconfirmedtohaveactivepulmonaryTBinfectionshouldbegiven
medicalleaveforatleasttwoweeksoruntilthesputumAFBisnegative.
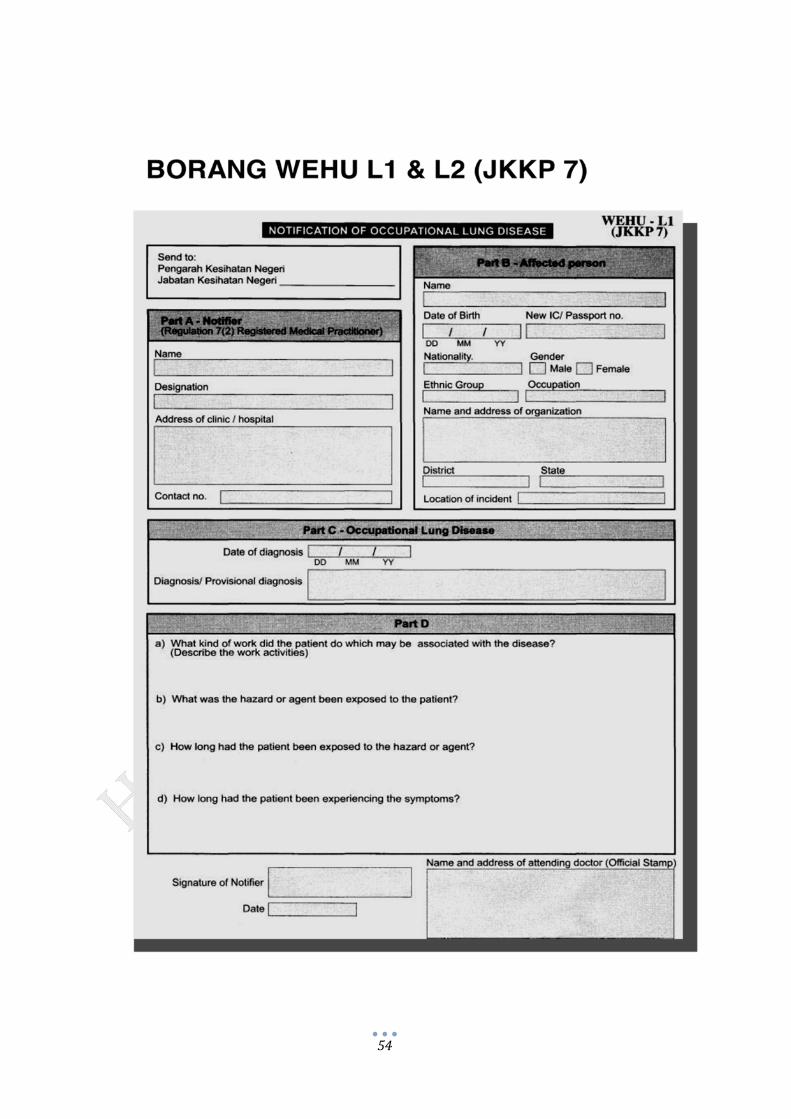
15.2.2 HCWTBistobenotifiedusingWEHUL1&L2(JKKP7)inadditiontotheusualTBIS10A1.
15.2.3 The PPKP of SGHUKA should be notified regarding tuberculosis inHCW,
eitherby theattendingdoctor, ifdiagnosedwithin thishospital, orby theHCW’sHeadofUnit,ifthediagnosishadbeenmadeelsewhere,e.g.inotherhealthcareinstitutions.
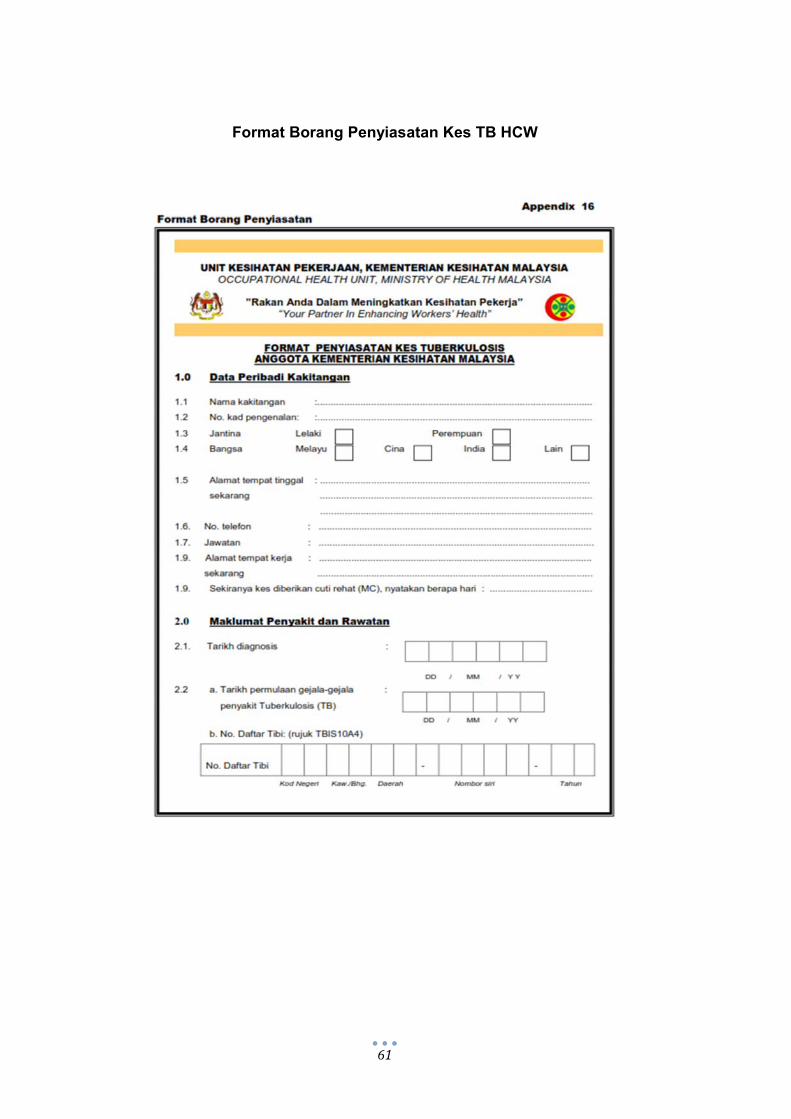
15.2.4Uponnotification,theHealthInspectorwillinterviewtheinfectedHCWusing
FormatPenyiasatanKesTuberkulosisDiKalanganKakitanganKementerianKesihatanMalaysia.
15.2.5 EffortsshouldbemadebytheattendingdoctorandPPKPininterviewingthe
HCWtoidentifypossiblesourcesofexposuretoTB15.2.6TheOHUDirectorwouldconcludewhetheritisacaseofoccupational‐related
TBornotSource:https://www.nice.org.uk
53
15.1.8Simultaneously,theTBICTaskForceshouldbenotifiedregardinginfectedHCWbyStaffClinicorHealthInspector.
15.1.9 TheTBICTaskForcewillreviewthecaseandmay interviewtheHCWfor
furtherinvestigationofanylapseininfectioncontrol.15.1.10TheTBICTaskForcewillconveneameetingtodecideoncontactscreening,
andactionplantocounteranyidentifiedlapseininfectioncontrol.15.1.11 Investigation and contact screening should be completed, and report
submittedtotheHospitalDirectorbyTBICTF,within1monthofnotification.
15.3 Medical Leave AllHCWswithconfirmedactivepulmonaryTBinfectionshouldbegivenmedicalleaveatleast2weeksoruntilsputumAFBisnegative.
15.4 Return to Work Policy
15.4.1 HCWwith TB should be allowed to return toworkwhen a physician hasconfirmedtheHCWisnoninfectious.
15.4.2Thereturntoworkcriteria: i.WorkersreceivesadequateantiTB ii.Coughhasresolved iii.Resultsofthree(3)consecutivesputumAFBsmearsnegative. (sputum
shouldbe8‐24hoursapart).15.4.3Monthly/ regular followupwhen theHCWresumeduty toensureeffective
treatment and DOT should be practised. The HCW should be underRespiratoryUnitfollowupincomplicatedcase.
15.5 Record Keeping 15.5.1AccordingtoNotificationofAccident,DangerousOccurence,OccupationalPoisoningandOccupationalDisease(NADOPOD)Regulations2004,therecordshouldbekeptatleast5yearsfromthedateonwhichitismade.15.5.2 A detailed records on TB of HCW should be kept by facilities inwhich they areworking.OnecopyshouldbesenttoOccupationalHealthUnitMOHthroughStateHealthDepartment.
54

55

56
15.6 Contact Screening of TB in Health Care Workers 15.6.1TheHCWshouldbeadvisedthatcontactscreeningwillbecarriedout.TheinfectedHCW’spreferencesonconfidentialityshouldbeexplored,andrespectedasfaraspossible.However,HCWshouldbewarnedthatinadvertantdisclosureisprobablefromthemedicalleaveandcontactinvestigations.15.6.2Closecontactsarepersonswhosharethesameairspaceinahouseholdorotherenclosedenvironmentforaprolongedperiod–daysorweeks,notminutesorhours–withapersonwithpulmonaryTBdisease.(CDC,2005)15.6.3 Following the guidance of “Garispanduan Pelaksanaan & Penyeliaan ProgramKawalanPenyakitTB,JKNS2017”,thefollowingwouldbescreenedascontacts: 1)Household 2)Allresidentsofthesamelonghouse 3)Exposure>8hoursadayegworkplace 4)Closesocialcontacts
5)Airlinepassengerswithin2rowstothefrontandtothebackofflights>8hours
15.6.3 Identificationand investigationofclosecontacts,outsideofSGH,eghousehold/housematecontacts,willbeperformedbytheHCW’sassignedTBCPcentre,asperroutine,withinoneweek.Onaverage,10contactsarelistedforeachpersonwithacaseofinfectiousTBbyTBCP,andfollowedup8monthlyfor2years.15.6.4 TracingofotherHCWsofcontactwithinSGH,isunderthepurviewofSGHOHU.TBICTask Force will investigate and determine prioritization of contacts within 1week ofnotification.15.6.5Anyidentifiedclosecontactswillbescreenedpromptly,followedup8weeksafterlastexposure,and8monthlyfor2years.15.6.6TheexpandedcontactscreeningofotherHCWsinSGHofcasuallowprioritycontactwillproceedafterthe8weekswindowperiod.15.6.7 HCWs have a responsibility to comply with screening directed by OHU withendorsementoftheHospitalDirector,pursuanttotheOccupationalSafetyAndHealthAct1994.[AktaKeselamatanDanKesihatanPekerjaanDanPeraturan‐Peraturan,Edisi2010.BahagianVI.KewajipanAmPekerja.Seksyen24(1)(d)]
57
15.6.8 For recording of Mantoux testing, HCWwho have been determined to be closecontacts,orHCWinhighriskgroup,i.e.diabetics,immunosuppressed,smokers,etc,willbeconsideredpositiveat>10mm,asperMOHManagementofTuberculosis(3rdEdition)ClinicalPracticeGuidelines,2002.15.6.9WhereasforHCWparticipatinginexpandedscreening,whoareatotherwiselowrisk,Mantouxtestof>15mmprovideshigherspecificity,andistakenasthecut‐offaspertheGuidelinesonPreventionandManagementofTuberculosisforHealthCareWorkersinMinistryofHealthMalaysia2012.15.6.10 AlthoughMantouxtestof10‐14mmareconsiderednegativeby the15mmcutpoint,HCWwhohadpreviousMantoux>10mm,andrequirecontactscreening,shouldbeevaluated by symptoms and CXR. Repeat Mantoux testing should not be performed asresultswouldnotprovideadditionalinformation.(CDC,2005)
58
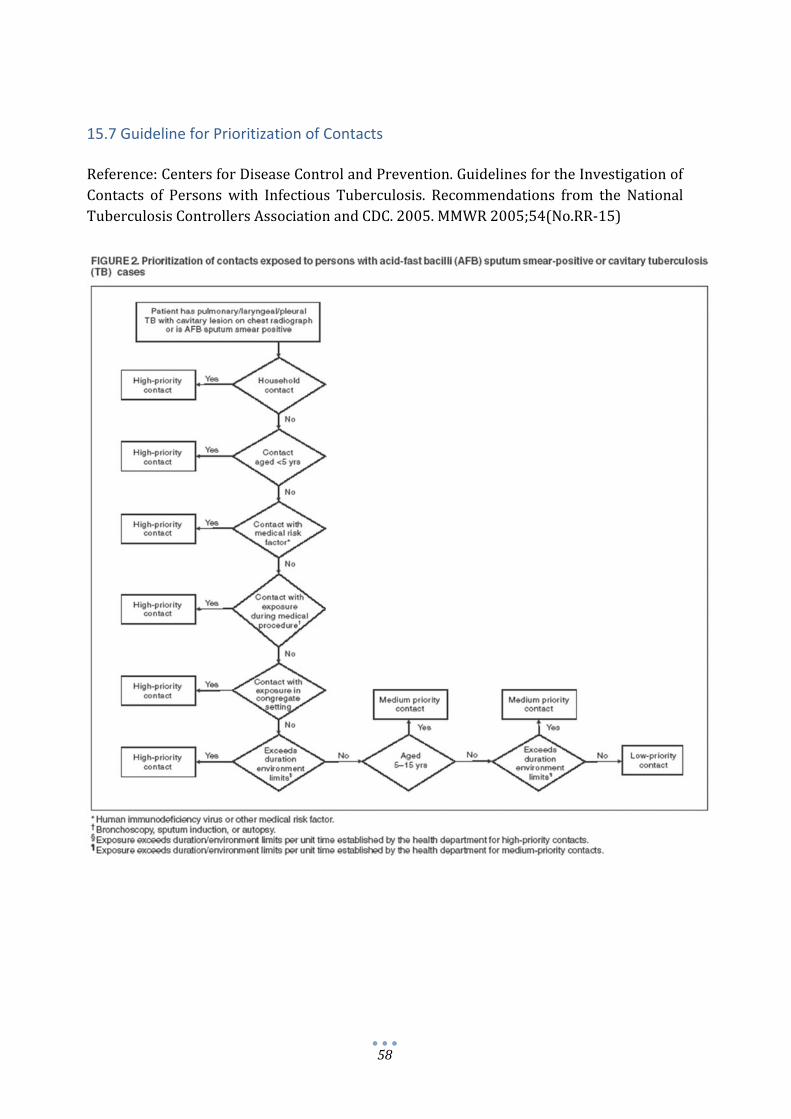
15.7 Guideline for Prioritization of Contacts Reference:CentersforDiseaseControlandPrevention.GuidelinesfortheInvestigationofContacts of Persons with Infectious Tuberculosis. Recommendations from the NationalTuberculosisControllersAssociationandCDC.2005.MMWR2005;54(No.RR‐15)

59
60
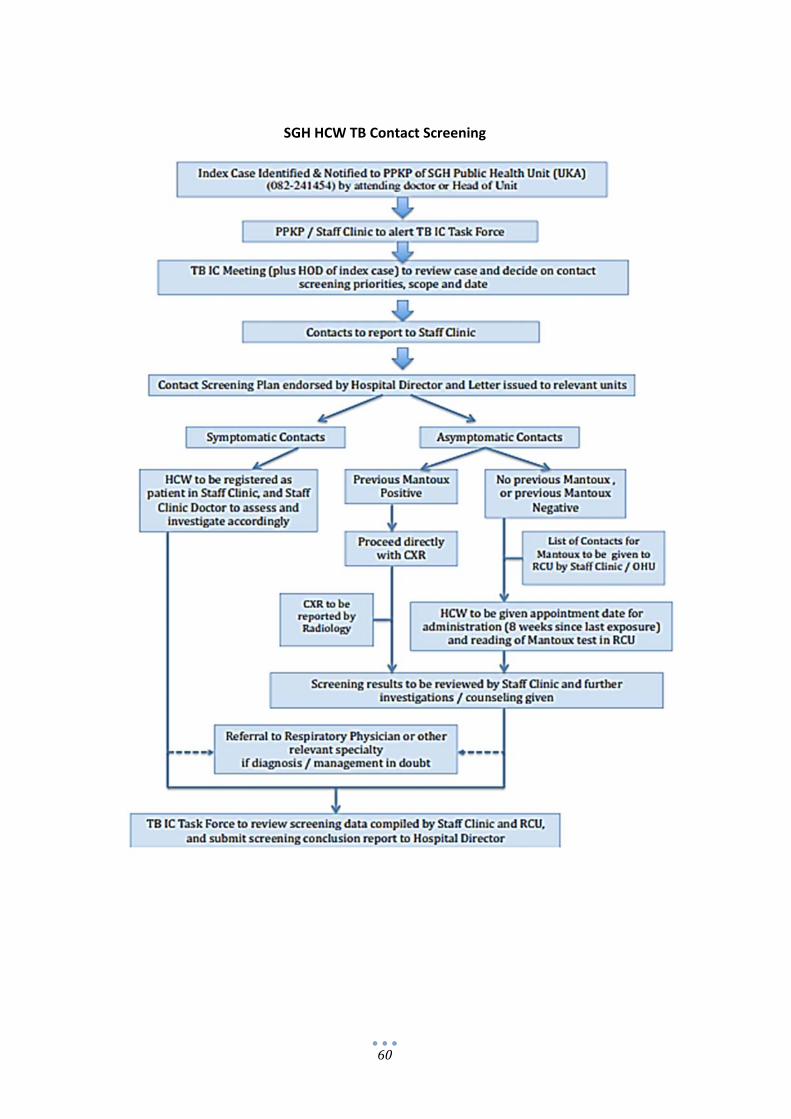
SGH HCW TB Contact Screening
61
Format Borang Penyiasatan Kes TB HCW

62

63

64

65
66

67
15.8 Baseline and Periodic Screening of TB in Health Care Workers 15.8.1 All hospital staff need to comply with TB screening outlined in “Guidelines on
PreventionandManagementofTuberculosisforHealthCareWorkersinMinistryofHealthMalaysia2012”.Thisincludes:
1.Pre‐employmentscreeningfornewstaff2.Periodicannualscreeningforexistingstaff3.Pre‐retirement/Pre‐transferscreening
15.8.2AllcategoriesofSGHemployeesneedtoundergoTBscreening.Thisincludesclinical,
aswellasnon‐clinicalstaff.15.8.3AllHCWTBscreeningshouldbeperformedbyStaffClinic,assistedbyRespiratoryDay
CarestaffandOccupationalHealthUnit(OHU).15.8.4HCWshouldNOTperformTBscreeningontheirown.15.8.5AllChest‐Xraysonceperformed,shouldbereportedbySGHRadiologyDepartment.15.8.6SGHHumanResourceUnitshouldinformOHUregardinganystaffnewlyemployed/
transferred/plannedforretirement,withname,unit,post,andcontactnumberforpurposesofTBscreening.
15.8.7 Briefing for new personnel upon reporting for duty, should include instructions to
attendPre‐PlacementMedicalExaminationatStaffClinic.15.8.8The“FormatPemeriksaanKesihatanPraPenempatanAnggotaKementerianKesihatan
Malaysia” OHU TB‐1 form shall be used for the pre‐placement medical screening.(Appendix6ofGuidelinesonPreventionandManagementofTuberculosisforHealthCareWorkersinMinistryofHealthMalaysia,2012)
15.8.9 The OHU TB‐1 forms shall be placed in the Staff Clinic, forwarded to Respiratory
DayCareUnit(RCU)ifdecisionmadeforMantouxtesting,andreviewedbyStaffClinicafterreadingofMantouxtest.
15.8.10Theseproceduresshouldbecompletedwithin2weeksofreportingforduty.15.8.11RCUstaffwillstampandfillindetailsofMantouxadministrationintheOHUTB‐1form.

68

69
5.0 Ujian
MANTOUX X-RAY DADA UJIAN KAHAK Berat
Badan
(Kg)
Tarikh Keputusan
(mm)
Tarikh Keputusan Tarikh Keputusan
Mikroskopi
Keputusan
Kultur
Keputusan
Ujian
Sensitiviti
(Tandatangan & Cop Rasmi)
Tarikh:
Nama Doktor :
No. Pendaftaran MMC:
Alamat Tempat Kerja:
No. Telefon:
70
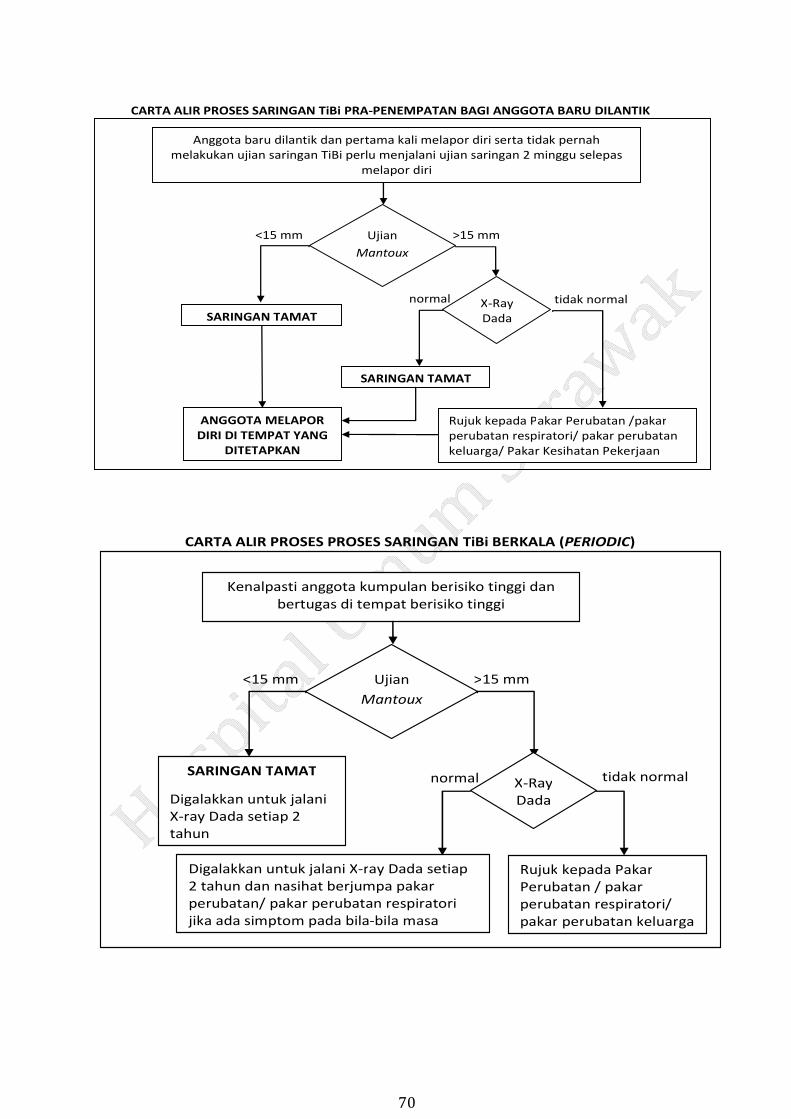
CARTA ALIR PROSES SARINGAN TiBi PRA‐PENEMPATAN BAGI ANGGOTA BARU DILANTIK
Anggota baru dilantik dan pertama kali melapor diri serta tidak pernah melakukan ujian saringan TiBi perlu menjalani ujian saringan 2 minggu selepas
melapor diri
Ujian
Mantoux
>15 mm<15 mm
X‐RayDada
tidak normal normal
Rujuk kepada Pakar Perubatan /pakarperubatan respiratori/ pakar perubatan keluarga/ Pakar Kesihatan Pekerjaan
SARINGAN TAMAT
SARINGAN TAMAT
ANGGOTA MELAPOR DIRI DI TEMPAT YANG
DITETAPKAN
CARTA ALIR PROSES PROSES SARINGAN TiBi BERKALA (PERIODIC)
Kenalpasti anggota kumpulan berisiko tinggi danbertugas di tempat berisiko tinggi
Ujian
Mantoux
>15 mm<15 mm
X‐RayDada
tidak normal normal
Rujuk kepada Pakar Perubatan / pakar perubatan respiratori/ pakar perubatan keluarga
Digalakkan untuk jalani X‐ray Dada setiap2 tahun dan nasihat berjumpa pakar perubatan/ pakar perubatan respiratori jika ada simptom pada bila‐bila masa
SARINGAN TAMAT
Digalakkan untuk jalani X‐ray Dada setiap 2 tahun

71
Source:TatacaraPerlaksanaanPekelilingKetuaPengarahKesihatanBil.9/2012:ProcesssaringanTiBibagianggotakementeriankesihatan.
CARTA ALIR PROSES SARINGAN TiBi BAGI ANGGOTA PRA PERSARAAN / PRA PERPINDAHAN
Anggota kesihatan yang mendapat arahan untukditukarkan keluar daripada TBT atau akan bersara
X‐RayDada
tidak normalnormal
Rujuk kepada Pakar Perubatan /Pakar perubatan respiratori/ Pakar Perubatan Keluarga
SARINGAN TAMAT
72
15.9 Screening Location 15.9.1Historytaking/symptomscreeningandmedicalexaminationshallbedoneinStaffClinic15.9.2 Tuberculin Skin Test (TST) administration and reading is performed at RespiratoryDaycareUnit(RCU)15.9.3ChestX‐rayshallbeperformedandreportedinRadiologyDepartment.15.9.4InterferonGamaReleaseAssay(IGRA)test,ifdeemednecessarybyphysician,wouldbeoutsourced.
73
15.10 Type of Screening
Symptomscreening
Mantoux/TuberculinSkinTest(TST)SeeSection14.6
ChestX‐ray
IfasymptomaticHCWhadbeenradiographedlessthan6monthsearlier,arepeatCXRisnotnecessary.However,theCXRshouldbereportedbyRadiologyDepartment,andreviewedbyStaffClinic.
InterferonGamaReleaseAssay(IGRA)
WhenrecommendedbyChest/InfectiousDiseasePhysician
15.11 Mantoux Test / Tuberculin Skin Test (TST)
AdaptedfromCanadianTuberculosisStandards.7thedition.Chapter4:DiagnosisofLatentTuberculosisInfection.2014
15.11.1ContraindicationsforTST Previouspositive,severeblisteringTSTreactions ExtensiveburnsoreczemapresentoverTSTtestingsites ActiveTB/TreatedTB(TSTwouldbeofnoclinicalutility) Currentmajorviralinfections(e.g.measles,mumps,varicella) Livevirusimmunization,particularlymeasles,withinthepast4weeks
(possiblefalse‐negativeTST)
15.11.2ThosewiththefollowingconditionscanreceiveTST: BCGvaccination Commoncold Pregnantorbreastfeeding Immunizedwithanyvaccineonthesameday Immunizedwithintheprevious4weekswithvaccinesotherthantheoneslistedearlier HistoryofapositiveTSTreactionthatwasnotdocumented Takinglowdosesofsystemiccorticosteroids,<15mgprednisone(orequivalent)daily.
Itgenerallytakesasteroiddoseequivalentto≥15mgprednisonedailyfor2‐4weekstosuppresstuberculinreactivity

74
15.11.3BallpointmethodforreadingtransversediameterofTSTinduration
• The TST should be read by a trained health professional. Individuals withoutexperience in reading a TSTmay not feel slight induration, and the TSTwould bemistakenlyrecordedas0mm.
• Self‐readingisveryinaccurateandisstronglydiscouraged.• Reading should be performed 48 to 72 hours after administration, as maximuminduration can take up to 48 hours to develop, but after 72 hours it is difficult tointerpretareaction.Reactionsmaypersistforupto1week,butforasmanyas21%ofindividualswithapositivereactionat48to72hoursthereactionwillbenegativeafter 1 week. If the TST cannot be read within 72 hours because of unforeseencircumstances,itshouldberepeatedataninjectionsitefarenoughfromthatoftheprevioustestthatthereactionsdonotoverlap.Nominimumwaitisrequiredbeforetherepeattest.
• Theforearmshouldbesupportedonafirmsurfaceandslightlyflexedattheelbow.Indurationisnotalwaysvisible.Palpatewithfingertipstocheckwhetherindurationispresent.Ifthereisinduration,marktheborderofindurationbymovingthetipofapenata45°anglelaterallytowardthesiteoftheinjection.Thetipwillstopattheedgeoftheinduration,ifpresent.Repeattheprocessontheoppositesideoftheinduration.Thispenmethodhastheadvantagesofbeingasreliableasthetraditionalpalpationmethod(whichreliesentirelyonfingertips)amongexperiencedreadersandofbeingeasierfornewreaderstolearnanduse.
• Usingaflexibleruler,measurethedistancebetweenthepenmarks,whichreflectsthediameteroftheindurationatitswidesttransversediameter(atarightangletothelongaxisoftheforearm).
• Disregardanddonot recorderythema (redness).Approximately2%‐3%ofpeopletestedwillhavelocalizedrednessorrash(withoutinduration)thatoccurswithinthefirst12hours.Theseareminorallergicreactions,arenotseriousanddonotindicateTBinfection.TheyarenotacontraindicationtofutureTSTs.
• Blistering,which can occur in 3% to 4%of subjectswith positive tests, should berecorded.
• Recordtheresultinmillimetres(mm).Recordnoindurationas"0mm."Recordingsofpositive,negative,doubtful,significantandnon‐significantarenotrecommended.
• Do not round off the diameter of the induration to the nearest 5mm as this caninterferewithdeterminingwhetherTST conversionhasoccurred in the eventof afutureTST.Ifthemeasurementfallsbetweendemarcationsontherules,thesmallerofthetwonumbersshouldberecorded.
75
15.12 Management 15.12.1 After completion of screening, the attending Staff ClinicMedical Officer shall certify
whetherthenewpersonnelhaveactive,latentornoevidenceofTB.15.12.2HCWfoundtohaveactiveTB,willbemanagedaspertheprecedingSection12.1ofthis
policy,andaccordingtoClinicalPracticeGuidelinesfortheControlandManagementofTuberculosis.
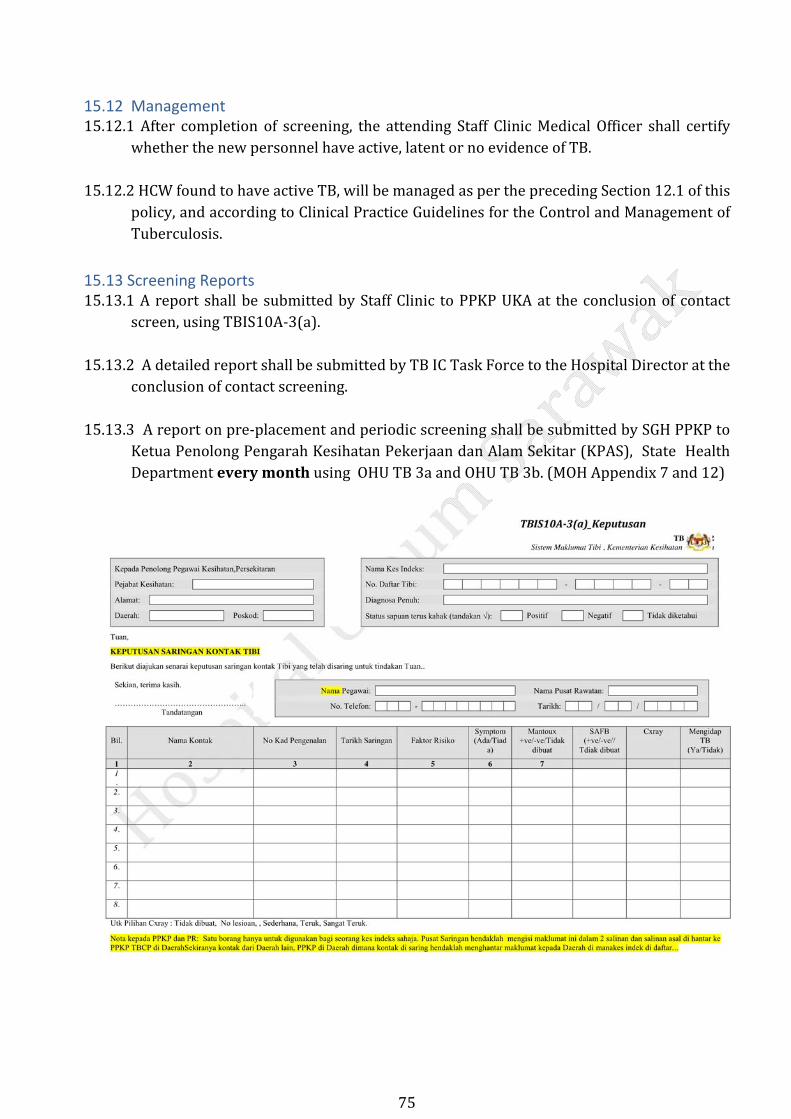
15.13 Screening Reports 15.13.1AreportshallbesubmittedbyStaffClinic toPPKPUKAat theconclusionofcontact
screen,usingTBIS10A‐3(a).15.13.2AdetailedreportshallbesubmittedbyTBICTaskForcetotheHospitalDirectoratthe
conclusionofcontactscreening.15.13.3Areportonpre‐placementandperiodicscreeningshallbesubmittedbySGHPPKPto
KetuaPenolongPengarahKesihatanPekerjaandanAlamSekitar(KPAS),StateHealthDepartmenteverymonthusingOHUTB3aandOHUTB3b.(MOHAppendix7and12)

76

77
15.13.4HCWswillbegivenacopyoftheTBscreeningformfortheirpersonalrecord:
Furtherreading:LobueandMenzies.TreatmentofLatentTuberculosisInfection:AnUpdate.Respirology(2010)15,p604
78
REFERENCES
1. Akta Keselamatan Dan Kesihatan Pekerjaan Dan Peraturan‐Peraturan. 2010.BahagianVI.KewajipanAmPekerja.Seksyen24(1)(d)
2. Asociation of Occupational Health Professionals in Healthcare. Tools for Your Work.
N95 Respirator Training and Fit Testing Verification Card. 2009.
3. Bahagian Kawalan Penyakit. Kementerian Kesihatan Malaysia. PencapaianProgramKawalanTibiKebangsaan(Jan‐Dis,2017).MesyuaratTWGBil1/2018.ProgramKawalanTibi/KustaKebangsaan.5Mac2018.
4. Canadian Tuberculosis Standards. 7th edition. Chapter 4: Diagnosis of LatentTuberculosisInfection.2014
5. Centers for Disease Control and Prevention. Guidelines for Preventing the
Transmission of Mycobacterium tuberculosis in Health‐Care Settings. 2005.MMWR2005;54(No.RR‐17):p4,36,47
6. CentersforDiseaseControlandPrevention.GuidelinesfortheInvestigationof
ContactsofPersonswithInfectiousTuberculosis.Recommendations fromtheNational Tuberculosis Controllers Association and CDC. 2005. MMWR2005;54(No.RR‐15):1‐37
7. Engineering Services Division, Ministry of Health Malaysia, Guideline On
ConceptualDesignAndEngineeringRequirementsForIsolationRoom,2017
8. https://www.nice.org.uk
9. JKNS.GarispanduanPelaksanaan&PenyeliaanProgramKawalanPenyakitTB(Edisi2)Jun2017.
10. Lobue and Menzies. Treatment of Latent Tuberculosis Infection: An Update.
Respirology(2010)15,p604
11. MOH. Guidelines on Prevention andManagement of Tuberculosis for HealthCareWorkersinMinistryofHealthMalaysia.2012.
12. MOH. Management of Tuberculosis (3rd Edition) Clinical Practice Guidelines.
2002

79
13. MOH.TatacaraPerlaksanaanPekelilingKetuaPengarahKesihatanBil.9/2012:Proses Saringan Tibi Bagi Anggota Kementerian Kesihatan. Unit KesihatanPekerjaan.BahagianKawalanPenyakit.
14. NIOSH. CDC. Hospital Respiratory Protection Program Toolkit. Resources for
RespiratorProgramAdministrators.May2015.
15. NIOSH.CDC.RecommendedGuidanceforExtendedUseandLimitedResuseofN95FilteringFacepieceRespiratorsinHealthcareSettings.March13,2014.
16. PreventionandControlofInfectiousDiseasesAct.1988.
17. SarawakHealthDepartment.SarawakWeeklyEpidNews.2017.
18. 3M Personal Safety Division. Particulate Respirator N95.
8210Plus/8210/0748/8110S. User Instructions. Fitting Instructions. 2015.