page 1 -2: contacts & important notices page 3 -7...
TRANSCRIPT

Note: This Comparison Is To Be Used As A Guide Only. Actual Benefits Will Be Governed by The Terms And Conditions of the Master Contract.
Page 1 - 2: Contacts & Important Notices
Page 3 - 7: Retiree without Medicare
Page 8- 11: Retiree with Medicare
Page 11 - 15: Rx Benefits, Vision Schedule & Basic Life Insurance
10/2/2013
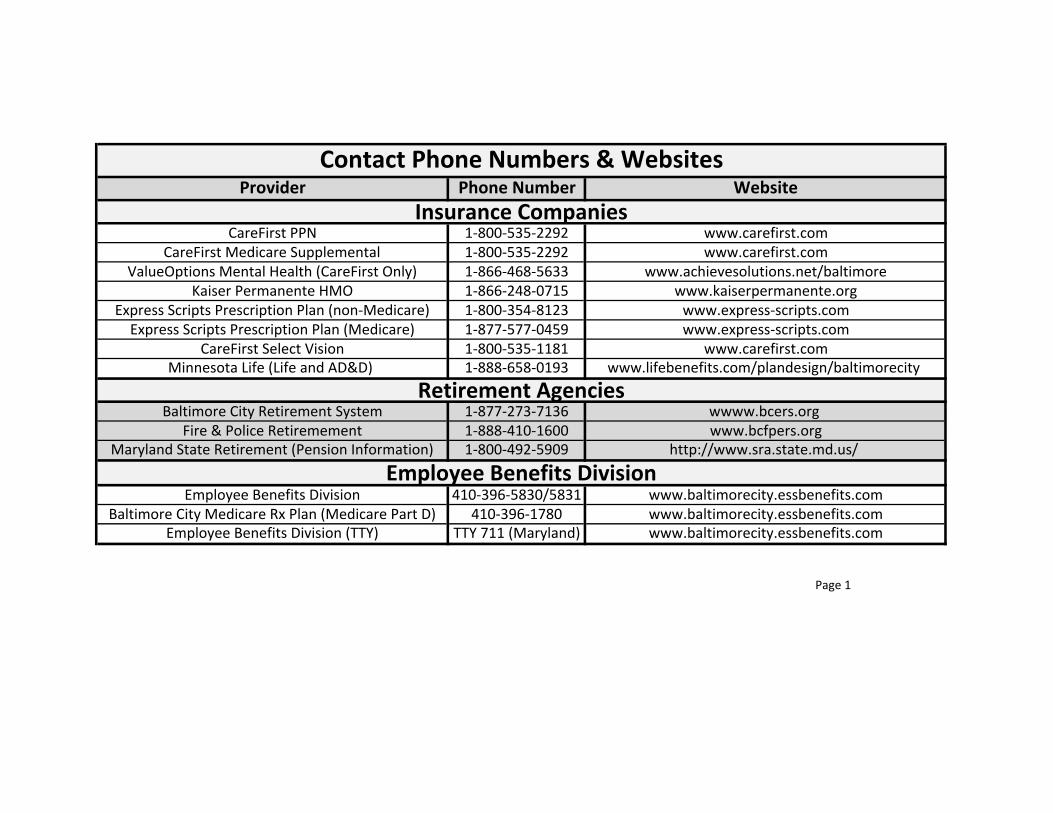
Provider Phone Number Website
CareFirst PPN 1-800-535-2292 www.carefirst.com
CareFirst Medicare Supplemental 1-800-535-2292 www.carefirst.com
ValueOptions Mental Health (CareFirst Only) 1-866-468-5633 www.achievesolutions.net/baltimore
Kaiser Permanente HMO 1-866-248-0715 www.kaiserpermanente.org
Express Scripts Prescription Plan (non-Medicare) 1-800-354-8123 www.express-scripts.com
Express Scripts Prescription Plan (Medicare) 1-877-577-0459 www.express-scripts.com
CareFirst Select Vision 1-800-535-1181 www.carefirst.com
Minnesota Life (Life and AD&D) 1-888-658-0193 www.lifebenefits.com/plandesign/baltimorecity
Baltimore City Retirement System 1-877-273-7136 wwww.bcers.org
Fire & Police Retiremement 1-888-410-1600 www.bcfpers.org
Maryland State Retirement (Pension Information) 1-800-492-5909 http://www.sra.state.md.us/
Employee Benefits Division 410-396-5830/5831 www.baltimorecity.essbenefits.com
Baltimore City Medicare Rx Plan (Medicare Part D) 410-396-1780 www.baltimorecity.essbenefits.com
Employee Benefits Division (TTY) TTY 711 (Maryland) www.baltimorecity.essbenefits.com
Page 1
Contact Phone Numbers & Websites
Retirement Agencies
Employee Benefits Division
Insurance Companies
Page 2
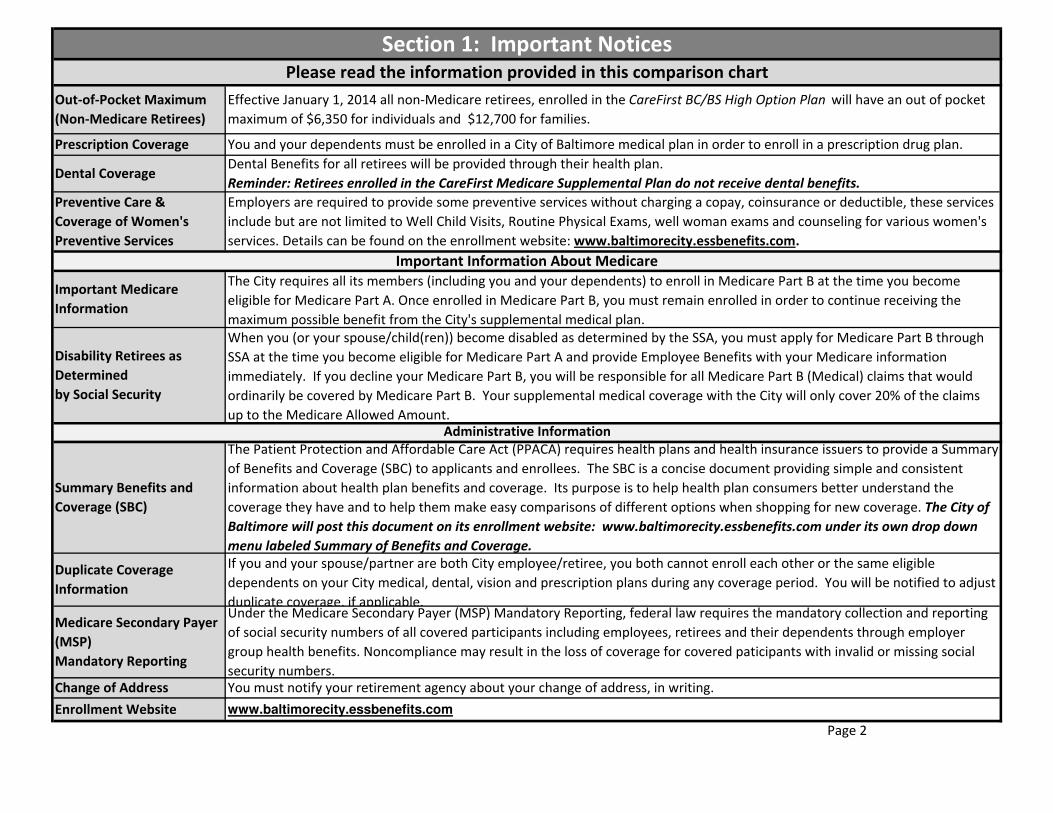
Out-of-Pocket Maximum
(Non-Medicare Retirees)
Effective January 1, 2014 all non-Medicare retirees, enrolled in the CareFirst BC/BS High Option Plan will have an out of pocket
maximum of $6,350 for individuals and $12,700 for families.
You and your dependents must be enrolled in a City of Baltimore medical plan in order to enroll in a prescription drug plan.Prescription Coverage
Section 1: Important Notices
Please read the information provided in this comparison chart
Dental Coverage
Important Information About Medicare
Dental Benefits for all retirees will be provided through their health plan.
Reminder: Retirees enrolled in the CareFirst Medicare Supplemental Plan do not receive dental benefits.
Important Medicare
Information
Enrollment Website www.baltimorecity.essbenefits.com
Change of Address You must notify your retirement agency about your change of address, in writing.
If you and your spouse/partner are both City employee/retiree, you both cannot enroll each other or the same eligible
dependents on your City medical, dental, vision and prescription plans during any coverage period. You will be notified to adjust
duplicate coverage, if applicable.
Medicare Secondary Payer
(MSP)
Mandatory Reporting
Under the Medicare Secondary Payer (MSP) Mandatory Reporting, federal law requires the mandatory collection and reporting
of social security numbers of all covered participants including employees, retirees and their dependents through employer
group health benefits. Noncompliance may result in the loss of coverage for covered paticipants with invalid or missing social
security numbers.
Duplicate Coverage
Information
Preventive Care &
Coverage of Women's
Preventive Services
Summary Benefits and
Coverage (SBC)
The Patient Protection and Affordable Care Act (PPACA) requires health plans and health insurance issuers to provide a Summary
of Benefits and Coverage (SBC) to applicants and enrollees. The SBC is a concise document providing simple and consistent
information about health plan benefits and coverage. Its purpose is to help health plan consumers better understand the
coverage they have and to help them make easy comparisons of different options when shopping for new coverage. The City of
Baltimore will post this document on its enrollment website: www.baltimorecity.essbenefits.com under its own drop down
menu labeled Summary of Benefits and Coverage.
Administrative Information
Disability Retirees as
Determined
by Social Security
Employers are required to provide some preventive services without charging a copay, coinsurance or deductible, these services
include but are not limited to Well Child Visits, Routine Physical Exams, well woman exams and counseling for various women's
services. Details can be found on the enrollment website: www.baltimorecity.essbenefits.com.
The City requires all its members (including you and your dependents) to enroll in Medicare Part B at the time you become
eligible for Medicare Part A. Once enrolled in Medicare Part B, you must remain enrolled in order to continue receiving the
maximum possible benefit from the City's supplemental medical plan.
When you (or your spouse/child(ren)) become disabled as determined by the SSA, you must apply for Medicare Part B through
SSA at the time you become eligible for Medicare Part A and provide Employee Benefits with your Medicare information
immediately. If you decline your Medicare Part B, you will be responsible for all Medicare Part B (Medical) claims that would
ordinarily be covered by Medicare Part B. Your supplemental medical coverage with the City will only cover 20% of the claims
up to the Medicare Allowed Amount.

Kaiser HMO
Out-of-Pocket Maximum$1,500 per individual
$3,000 per family
$3,000 per individual
$6,000 per family
$6,350 per individual
$12,700 per familyN/A
$3,500 per individual
$9,400 per family
Deductible$250 per individual
$500 per family
$500 per individual
$1,000 per familyOnly Under Major Medical Only Under Major Medical N/A
Plan Lifetime Maximum Unlimited Unlimited Unlimited Unlimited Unlimited
Dependent Eligibility
Physician's Office Visit $25 Copay 70% Allowed Benefit
100% of allowed benefit after $20 copay
per medical office visit to a primary care
physician
80% allowed benefit $5 copay per visit
Specialist Office Visit $40 Copay 70% Allowed Benefit100% allowed benefit after
$25 copay 80% allowed benefit $5 copay per visit
Routine GYN - One Yearly 100% Allowed Benefit 100% Allowed Benefit 100% allowed benefit 80% allowed benefit Covered in Full
Hearing Exams 90% allowed benefit 70% allowed benefit
Hearing benefits 100% allowed
benefit with medical diagnosis;
one exam every 36 months
(routine exams excluded)
Hearing benefits 80% allowed
benefit with medical diagnosis;
one exam every 36 months
(routine exams excluded)
$5 copay per visit
Immunizations 100% Allowed Benefit 100% Allowed Benefit100% allowed benefit- when
associated w/a routine physical
80% allowed benefit- when
associated w/a routine physicalCovered in full
Mammography, Colorectal
Screening, Prostate
Screening
100% allowed benefit 100% allowed benefit100% allowed benefit -
yearly after age 40
80% allowed benefit -
yearly after age 40Covered in full
Routine Physical - yearly 100% Allowed Benefit 100% Allowed Benefit 100% allowed benefit 80% allowed benefit Covered in full
Well Baby/Child Care 100% Allowed Benefit 100% Allowed Benefit 100% Allowed Benefit 80% allowed Benefit Covered in full
Page 3
Dependent children, until the end of the calendar year they reach age 26, regardless of student status.
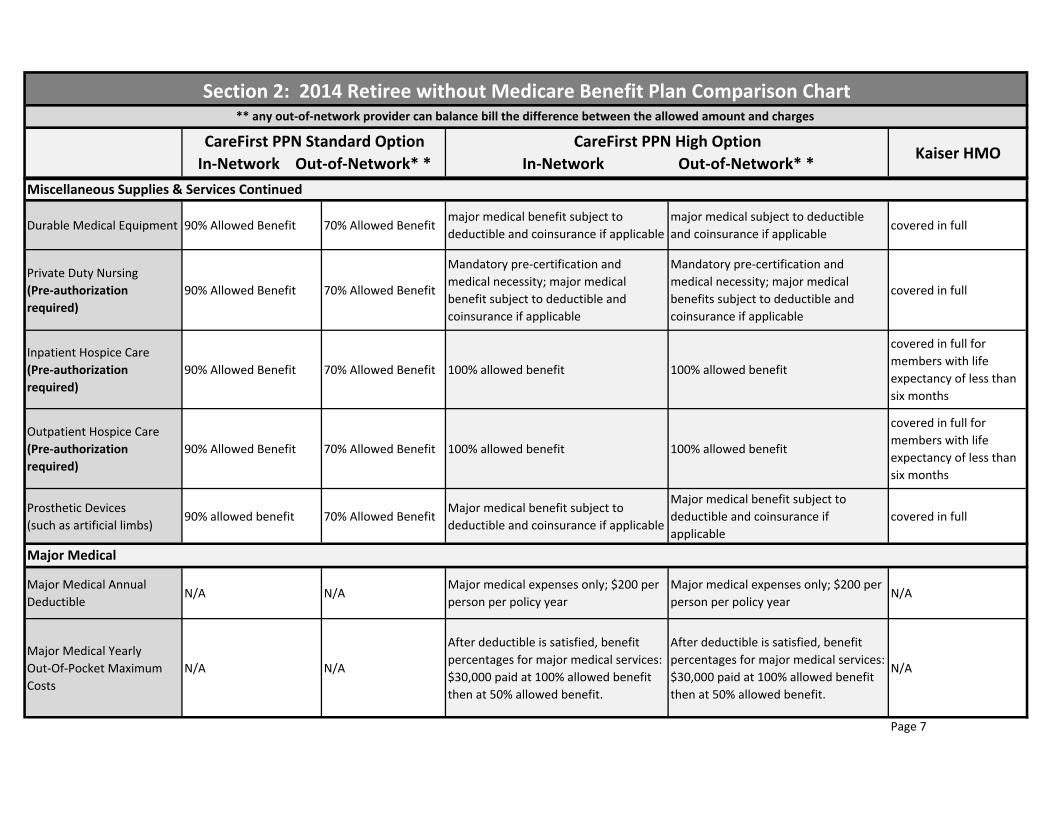
Section 2: 2014 Retiree without Medicare Benefit Plan Comparison Chart ** any out-of-network provider can balance bill the difference between the allowed amount and charges
CareFirst PPN High Option
In-Network Out-of-Network* *
Routine & Preventive Services
CareFirst PPN Standard Option
In-Network Out-of-Network* *

Kaiser HMO
Section 2: 2014 Retiree without Medicare Benefit Plan Comparison Chart ** any out-of-network provider can balance bill the difference between the allowed amount and charges
CareFirst PPN High Option
In-Network Out-of-Network* *
CareFirst PPN Standard Option
In-Network Out-of-Network* *
Ambulance Service
(based on medical
necessity)
90% allowed benefit
(Ground Only)
70% allowed benefit
(Ground Only)
Major medical subject to deductible and
coinsurance if applicable (Ground
Only)
Major medical subject to deductible
and coinsurance if applicable (Ground
Only)
covered in full
Emergency Room
(copay waived if admitted)90% allowed benefit 90% allowed benefit 100% of allowed benefit $50 copay 100% of allowed benefit $50 copay $50 copay
Urgent Care$25 Copay 90% allowed
benefit
$25 Copay 70%
allowed benefit$10 copay per visit Will be handled as in-network $5 copay per visit
Anesthesia 90% allowed benefit 90% allowed benefit 100% allowed benefit 100% allowed benefit covered in full
Hospital Services, Including
Room, Board & General
Nursing Services
(Pre-Authorization
required)
90% allowed benefit 70% allowed benefit 100% allowed benefit
$100 deductible per admission, then
plan pays 70% up to $1,500 out of
pocket maximum per admission, then
100% allowed benefit.
covered in full
Medical Surgical
Physician Services90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit covered in full
Physical, Speech &
Occupational Therapy
90% allowed benefit -
limit 60 visits combined
yearly
70% Allowed benefit -
limit 60 visits
combined yearly
100% alowed benefit -100 combined
visits yearly (preauth required after
10th lifetime visit)
80% allowed benefit-100 combined
visits yearly (preauth required after
10th lifetime visit)
covered in full
Organ Transplant
(Pre-Authorization
Required)
90% allowed benefit
70% Allowed Benefit
($30,000 limit per
transplant)**
Kidney, bone marrow, cornea
transplants, liver, heart, heart-lung or
pancreas - 100% allowed benefit
kidney, bone marrow, cornea
transplants, liver, heart,
heart-lung or pancreas - 100% allowed
benefit
covered in full for
non-experimental
transplants
Page 4
Emergency Room and Urgent Care Services
Hospital Inpatient Services

Kaiser HMO
Section 2: 2014 Retiree without Medicare Benefit Plan Comparison Chart ** any out-of-network provider can balance bill the difference between the allowed amount and charges
CareFirst PPN High Option
In-Network Out-of-Network* *
CareFirst PPN Standard Option
In-Network Out-of-Network* *
Chemotherapy & Radiation 90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit $5 copay per visit
Renal Dialysis 90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit $5 copay per visit
Diagnostic Lab Work &
X-rays90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit covered in full
Outpatient Surgery 90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit $5 copay per visit
Cardiac Rehab 90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefitCovered at 100%,
if medically necessary
Allergy Testing 90% allowed benefit 70% allowed benefit 100% allowed benefit 80% allowed benefit $5 copay per visit
Allergy Serum
90% allowed benefit,
max benefit $200 per
year
70% allowed benefit,
max benefit
$200 per year
100% allowed benefit, max benefit $200
per year
80% allowed benefit, max benefit $200
per yearcovered in full
Pre & Post-Natal Physician
Services 100% allowed benefit 80% allowed benefit 100% allowed benefit 80% allowed benefit
copays, deductibles,
or co-insurance may
apply depending on
services rendered
Newborn Care (Inpatient) 100% Allowed Benefit 80% allowed benefit 100% allowed benefit initial & discharge 80% allowed benefit initial & discharge covered in full
Delivery (Inpatient) 100% Allowed Benefit 80% allowed benefit100% allowed benefit
Pe-authorization Required
$100 deductible per admission,
then plan pays 70% up to $1,500
out of pocket maximum per admission,
then 100% allowed benefit.
Pre-authorization Required
covered in full
Page 5
Allergy Serum
Outpatient Services
Maternity

Kaiser HMO
Section 2: 2014 Retiree without Medicare Benefit Plan Comparison Chart ** any out-of-network provider can balance bill the difference between the allowed amount and charges
CareFirst PPN High Option
In-Network Out-of-Network* *
CareFirst PPN Standard Option
In-Network Out-of-Network* *
Fertility Testing & Family
Planning
90% allowed benefit
after deductible
70% Allowed Benefit
after Deductible100% allowed benefit 80% allowed benefit
$5 copay per visit for
family planning. Fertility
testing office visit and
any other fertility
services covered at 50%
In-Vitro Fertilization
Pre-authorization required
90% allowed benefit
after deductible up to
$100,000 Lifetime
Maximum
70% allowed benefit
after deductible up to
$100,000 Lifetime
Maximum
100% allowed benefit,
$12,000 lifetime max
80% allowed benefit,
$12,000 lifetime max
50% of allowable
charges; $100,000
maximum lifetime
benefit for up to 3
attempts per live birth
Inpatient Mental
Health/Alcohol &
Substance Abuse Benefits
Pre-Authorization Required
90% allowed benefit
after deductible
Provided by Value
Options
70% allowed benefit
after deductible
Provided by Value
Options
100% allowed benefit;
Provided by Value Options
$100 deductible per admission, then
plan pays 70% up to $1,500 out of
pocket maximum per admission, then
100% allowed benefit. Provided by
Value Options
covered in full
Outpatient Mental
Health/Alcohol &
Substance Abuse Benefits
$25 Copay
Provided by Value
Options
70% Allowed Benefit
Provided by Value
Options
100% allowed benefit after $20 copay.
Provided by Value Options
80% allowed benefit.
Provided by Value Options$5 copay per visit
Nutrition & Health
Education
90% Allowed Benefit
after Deductible
70% Allowed Benefit
after Deductiblecovered at 100% 80% allowed benefit $5 copay per visit
Diabetic Supplies 90% Allowed Benefit
after Deductible
70% Allowed Benefit
after Deductible
100% allowed benefit, including lancets
test strips and glucometers
100% allowed benefit, including
lancets, test strips and glucometersCovered in Full
Page 6
Insulin & syringes are covered by the Rx plan
Fertility Testing & Family Planning
Miscellaneous Supplies & Services
Mental Health & Substance Abuse
Kaiser HMO
Section 2: 2014 Retiree without Medicare Benefit Plan Comparison Chart ** any out-of-network provider can balance bill the difference between the allowed amount and charges
CareFirst PPN High Option
In-Network Out-of-Network* *
CareFirst PPN Standard Option
In-Network Out-of-Network* *
Durable Medical Equipment 90% Allowed Benefit 70% Allowed Benefit major medical benefit subject to
deductible and coinsurance if applicable
major medical subject to deductible
and coinsurance if applicable covered in full
Private Duty Nursing
(Pre-authorization
required)
90% Allowed Benefit 70% Allowed Benefit
Mandatory pre-certification and
medical necessity; major medical
benefit subject to deductible and
coinsurance if applicable
Mandatory pre-certification and
medical necessity; major medical
benefits subject to deductible and
coinsurance if applicable
covered in full
Inpatient Hospice Care
(Pre-authorization
required)
90% Allowed Benefit 70% Allowed Benefit 100% allowed benefit 100% allowed benefit
covered in full for
members with life
expectancy of less than
six months
Outpatient Hospice Care
(Pre-authorization
required)
90% Allowed Benefit 70% Allowed Benefit 100% allowed benefit 100% allowed benefit
covered in full for
members with life
expectancy of less than
six months
Prosthetic Devices
(such as artificial limbs) 90% allowed benefit 70% Allowed Benefit
Major medical benefit subject to
deductible and coinsurance if applicable
Major medical benefit subject to
deductible and coinsurance if
applicable
covered in full
Major Medical Annual
DeductibleN/A N/A
Major medical expenses only; $200 per
person per policy year
Major medical expenses only; $200 per
person per policy yearN/A
Major Medical Yearly
Out-Of-Pocket Maximum
Costs
N/A N/A
After deductible is satisfied, benefit
percentages for major medical services:
$30,000 paid at 100% allowed benefit
then at 50% allowed benefit.
After deductible is satisfied, benefit
percentages for major medical services:
$30,000 paid at 100% allowed benefit
then at 50% allowed benefit.
N/A
Page 7
Major Medical
Miscellaneous Supplies & Services Continued

CareFirst Medicare Supplemental Kaiser HMOAre Referrals Required? no yes
Dependent Eligibility
Plan Lifetime Maximum Benefit Unlimited Unlimited
Physician's Office Visit covered by major medical $5 copay per visit
Specialist Office Visit covered by major medical $5 copay per visit
Routine GYN Examination
For the year Medicare provides the benefit- 100% of balance
after Medicare; for the year Medicare does not provide a
benefit- 100% of BCBS allowed benefit
Covered in full
Hearing Exams no benefit $5 copay, hearing aids not covered
Immunizations no benefitOffice visit copay may apply, then covered in full for influenza,
pnuemococcal and Hepatitis B vaccine
Mammography, Colorectal Screening,
Prostate Screening100% of balance after the Medicare allowed amount $5 copay per visit
Routine PhysicalLimited to 1 visit per calendar year with $100 maximum per
year (no coverage for lab services)Covered in full
Well Baby/Child Care no benefit Covered in full
Ambulance Service
(based on medical necessity)covered by major medical Covered in full according to Medicare guidelines
Emergency Room
(copay waived if admitted)
100% of balance after the Medicare allowed amount up to the
Medicare allowed amount, if within 72 hours of the accident
or injury.
$50 copay
Urgent Care not applicable - see office visit $5 copay per visit
Page 8
Dependent children, until the end of the calendar year they reach age 26, regardless of student status.
Routine & Preventive Services
Emergency Room and Urgent Care Services
Section 3: 2014 Retiree with Medicare Benefit Plan Comparison Chart
** any our-of-network provider can balance bill the difference between the allowed amount and charges
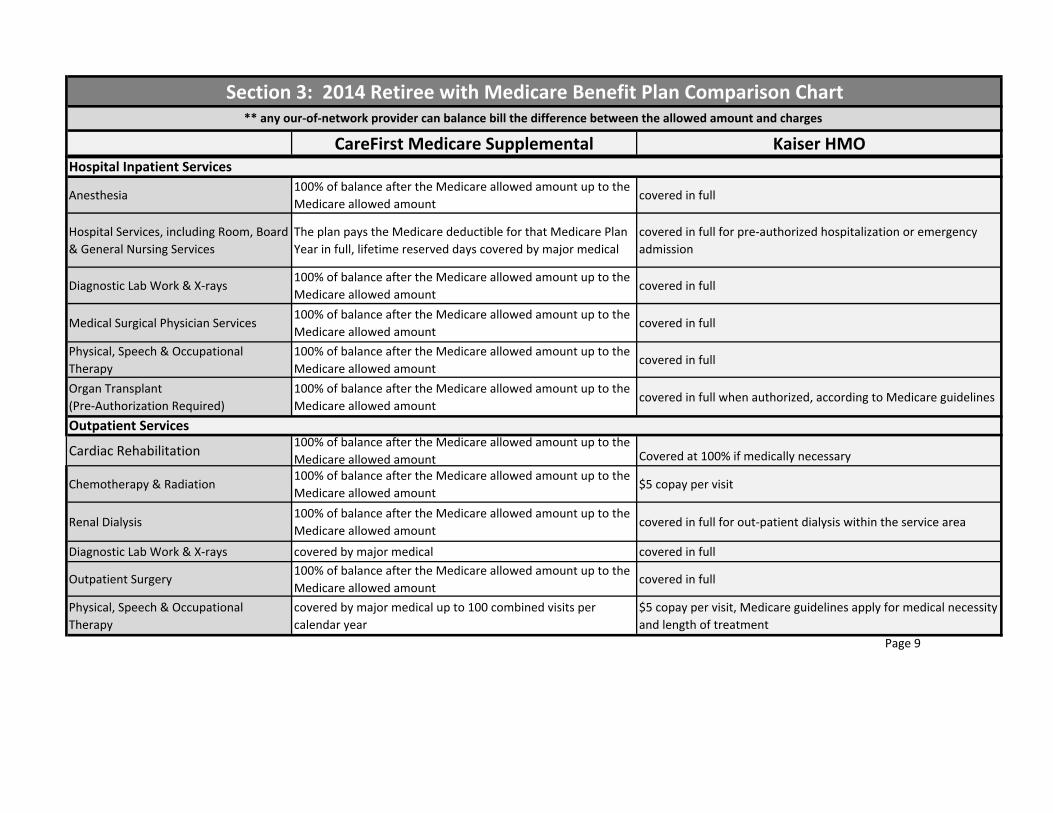
CareFirst Medicare Supplemental Kaiser HMO
Section 3: 2014 Retiree with Medicare Benefit Plan Comparison Chart
** any our-of-network provider can balance bill the difference between the allowed amount and charges
Anesthesia100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full
Hospital Services, including Room, Board
& General Nursing Services
The plan pays the Medicare deductible for that Medicare Plan
Year in full, lifetime reserved days covered by major medical
covered in full for pre-authorized hospitalization or emergency
admission
Diagnostic Lab Work & X-rays100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full
Medical Surgical Physician Services100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full
Physical, Speech & Occupational
Therapy
100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full
Organ Transplant
(Pre-Authorization Required)
100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full when authorized, according to Medicare guidelines
Cardiac Rehabilitation100% of balance after the Medicare allowed amount up to the
Medicare allowed amount Covered at 100% if medically necessary
Chemotherapy & Radiation100% of balance after the Medicare allowed amount up to the
Medicare allowed amount$5 copay per visit
Renal Dialysis100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full for out-patient dialysis within the service area
Diagnostic Lab Work & X-rays covered by major medical covered in full
Outpatient Surgery100% of balance after the Medicare allowed amount up to the
Medicare allowed amountcovered in full
Physical, Speech & Occupational
Therapy
covered by major medical up to 100 combined visits per
calendar year
$5 copay per visit, Medicare guidelines apply for medical necessity
and length of treatment
Page 9
Hospital Inpatient Services
Outpatient Services

CareFirst Medicare Supplemental Kaiser HMO
Section 3: 2014 Retiree with Medicare Benefit Plan Comparison Chart
** any our-of-network provider can balance bill the difference between the allowed amount and charges
Allergy Testing covered by major medical $5 copay per visit
Allergy Serum covered by major medical $5 copay per visit
Pre/Post-Natal Physician Services no benefitcopays, deductibles, or co-insurance may apply depending on
services rendered
Delivery (Inpatient) no benefit covered in full
Newborn Care (Inpatient) no benefit covered in full
Fertility Testing & Family Planning no benefit$5 copay per visit- infertility 50% of allowable charges for testing,
lab and x-ray charges
In-Vitro Fertilization no benefit50% of allowable charges; $100,000 maximum lifetime benefit for
up to 3 attempts per live birth
Inpatient Mental Health
Benefits/Alcohol & Substance Abuse100% after Medicare covered in full
Outpatient Mental Health
Benefits/Alcohol & Substance Abusecovered by major medical $5 copay per visit
Nutrition and Health Education Not Covered unlimited visits
Diabetic Supplies100% of balance after Medicare, including test strips, lancets
& glucometers
$5 copay per visit for Medicare covered self-monitoring training;
covered in full for lancets, test strips & glucometers
Page 10
Insulin & Syringes Are Covered By Your Rx Plan
Miscellaneous Supplies & Services
Mental Health & Substance Abuse
Fertility Testing & Family Planning
Maternity
Outpatient Services Continued
CareFirst Medicare Supplemental Kaiser HMO
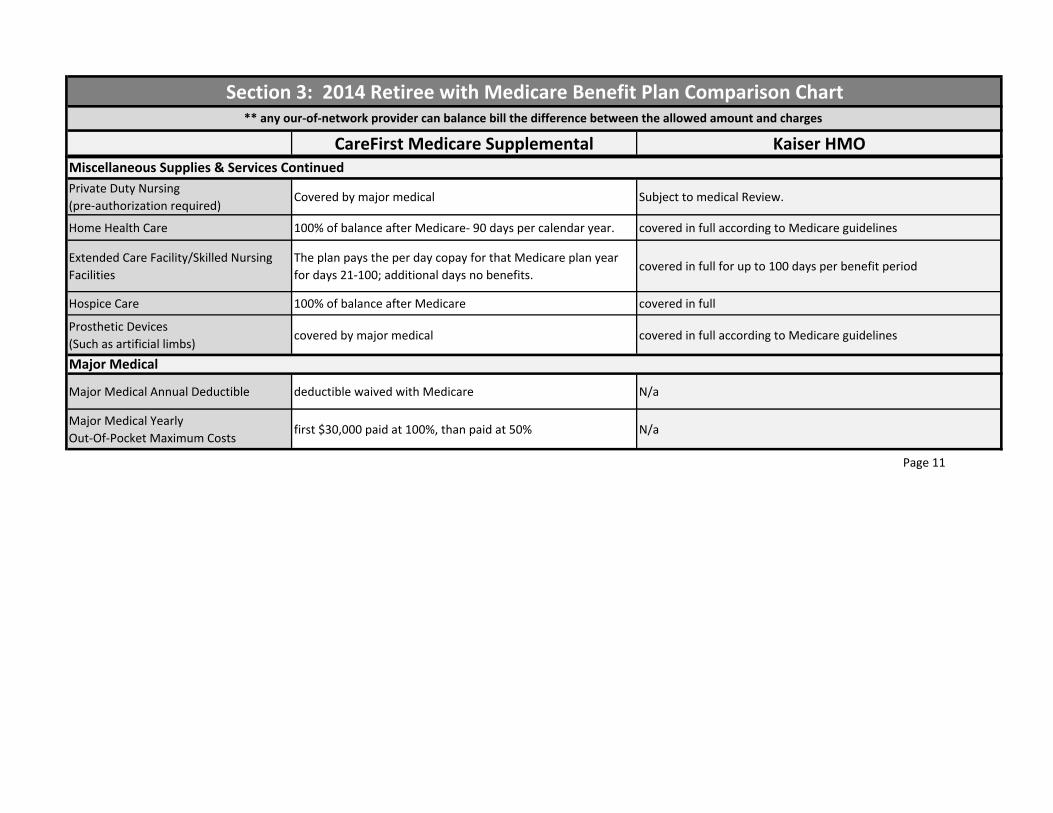
Section 3: 2014 Retiree with Medicare Benefit Plan Comparison Chart
** any our-of-network provider can balance bill the difference between the allowed amount and charges
Private Duty Nursing
(pre-authorization required)Covered by major medical Subject to medical Review.
Home Health Care 100% of balance after Medicare- 90 days per calendar year. covered in full according to Medicare guidelines
Extended Care Facility/Skilled Nursing
Facilities
The plan pays the per day copay for that Medicare plan year
for days 21-100; additional days no benefits.covered in full for up to 100 days per benefit period
Hospice Care 100% of balance after Medicare covered in full
Prosthetic Devices
(Such as artificial limbs)covered by major medical covered in full according to Medicare guidelines
Major Medical Annual Deductible deductible waived with Medicare N/a
Major Medical Yearly
Out-Of-Pocket Maximum Costsfirst $30,000 paid at 100%, than paid at 50% N/a
Page 11
Miscellaneous Supplies & Services Continued
Major Medical
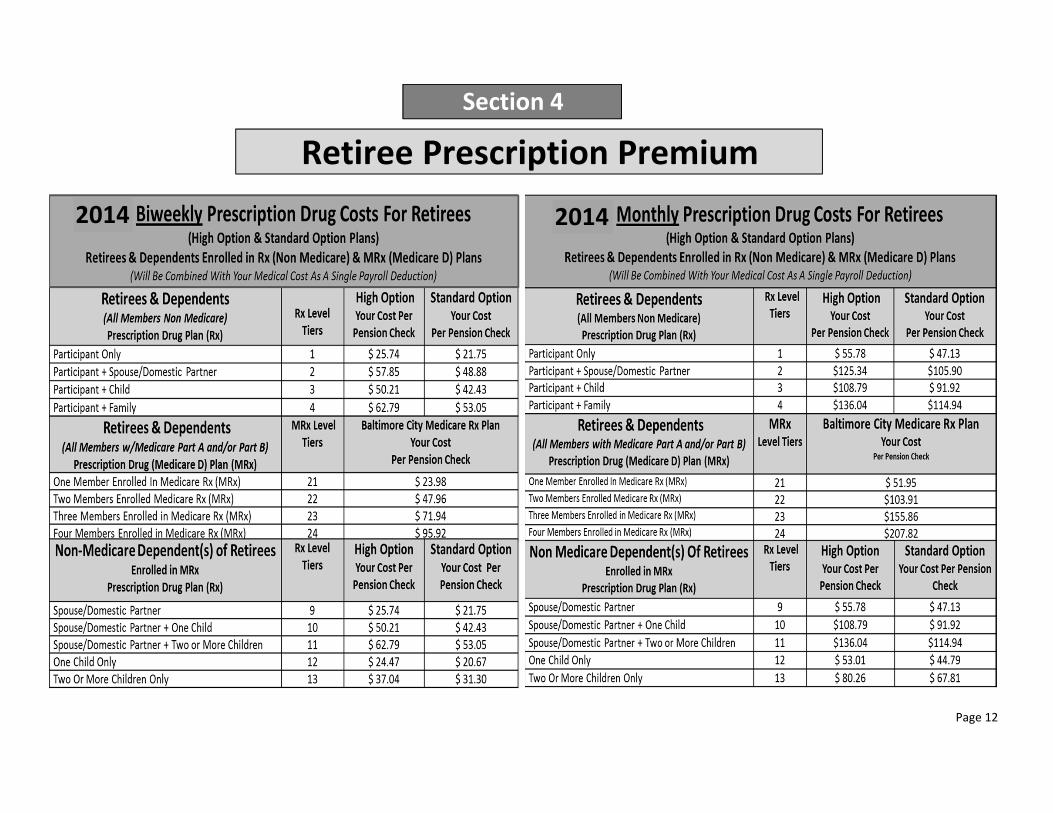
Page 12
Retiree Prescription Premium
Section 4
20142014

Page 13
Section 4: 2014 Express Scripts Copays

You Pay:
Single Vision Single Vision Balance
Bifocal Bifocal Balance
Trifocal Trifocal Balance
Double Bifocal Double Bifocal Balance
Cataract (Aphakic)
Cataract
(Aphakic) Balance
Medically Required*
Not Medically
Required. Single
Vision.**
Not Medically
Required. Bifocal **
Page 14
CareFirst Select Vision- Schedule of Benefits (Retirees: MAPS, Police & Fire Only)If you go to a ….
Participating Provider Non-Participating Provider
Covered Service (Note: Plan allows one pair of glasses or contacts, per member, in a 24 month period.)
Vision Exam Plan Pays 100% of Allowed Benefit.
$41.50 $41.50
Plan Pays 100% of allowed Benefit; you pay the balance.
$67.00$67.00
$100.50 $100.50
$89.50
Plan pays up to: Plan pays up to:
** In place of glasses (frames and lenses)
Frames Per Pair
Plan Pays up to $29.50 and you pay $0 for select
frames. (If you select more expensive frames then
you pay the balance.) Play pays up to $29.50; you pay the balance.
Contact Lenses** Covered only if medically necessary or instead of glasses
Plan pays up to $221.
* Following cataract surgery or when visual acuity of at least 20/70 in the better eye is possible with the use of contact lenses.
$156.50
$89.50
Glasses
Plan pays up to $221; you pay the balance.
$156.50
NOTE: The Only Retirees Eligible for the CareFirst Select Vision Benefits Are MAPS, FIRE & Police
Plan pays up to $71. Plan pays up to $71; you pay the balance.
Plan pays up to $96.50. Plan pays up to $96.50; you pay the balance.
Section 4

Benefit Amount
$8,500
$7,000
$7,000
$1,500
$5,000
$5,000
$5,000
Page 15
AFSCME Local 2202
AFSCME Local 44
CUB
UNION
Retiree Life Insurance
MAPS
Fire
Police
AFSCME Local 558 (Nurses)
Beneficiary forms are available on the City of Baltimore Enrollment website:
www.baltimorecity.essbenefits.com
Section 4

Page 16
NOTES PAGE

CCCCITY OFITY OFITY OFITY OF BBBBALTIMOREALTIMOREALTIMOREALTIMORE
Employee Benefits Division201 E. Baltimore Street- Suite 500
Baltimore, MD 21202Phone: 410-396-5830
TTY 711 (Maryland)website: www.baltimorecity.essbenefits.com